representation of older patients in clinical trials for drug approval in japan
TRANSCRIPT

IntroductionThe older population is the fastest growing group in many
advanced countries, and this trend is expected to continue forseveral decades (1). Japan is the most rapidly aging country,with the percentage of the population over age 65 projected torise from 23.3% in 2011 to 39.9% in 2060 (2). The populationover age 75 is also increasing in Japan, and within fifty years isestimated to be 26.9%.Older patients are widely treated with drug therapies and
therefore they consume considerable amounts of drugs.However, many aspects of aging complicate the properevaluation of the efficacy and the safety of drugs for the olderpopulation. The pharmacokinetic responses to a drug, such ashepatic metabolism or renal elimination, are well known todiffer in older people as compared with healthy younger adults(3). Moreover, the pharmacodynamic effect (e.g., the affinity ofsome receptors and channels) is sometimes affected by aging(4). As a result of such changes, drug efficacy and safety aresometimes different in older patients compared to youngerpatients (5, 6). A further complication in predicting drug actionin older patients is the heterogeneity of older people, who canrange from frail patients to relatively robust patients (7).Quite a few drugs have been found to be more dangerous in
older patients, as determined in post-marketing settings. Forexample, in February 2012, a warning was issued for apurgative used for bowel cleansing prior to colonoscopy due toa greater risk of acute renal impairment and acute phosphatenephropathy in older patients (8). This purgative is nowcontraindicated in older patients with hypertension in Japan. Itis important to find the proper balance between efficienttreatment of disease and avoiding harm in the older population.
However, extrapolation of clinical results from youngerindividuals sometimes may not provide an adequate risk-benefitestimate for older patients (9, 10). The efficacy and the safetyof a drug should be determined by clinical trials conducted withrepresentatives of the entire target population.Nevertheless, many studies in a range of therapeutic areas
show that drug clinical trials often exclude older patients (11-16). In Europe, where the population is ageing rapidly as well,how to properly conduct researches and developments of a drugfor older patients has been discussed by various partiesinvolving regulators, academia, patient groups andpharmaceutical industry(17-19). In contrast, little studyregarding drug development for older people has been reportedin Japan.To examine the situation for drugs which are authorized and
generally prescribed in Japan, we assessed the representation ofolder patients with several chronic conditions in the clinicaltrials conducted for regulatory approval.
Method
The included drugs studied were launched in Japan by 2012as new molecular entities or drugs with new indications. Theyare prescribed for 6 chronic conditions common among olderpatients: diabetes mellitus (DM), hypertension, rheumatoidarthritis (RA), non-small cell lung cancer (NSCLC),depression, and Alzheimer’s disease (AD). For each drug, weidentified the pivotal, confirmatory clinical trial and/or phaseIII randomized clinical trials conducted with Japanese patientsthat started after Good Clinical Practices (GCP) came into forcein April 1998 and for which information on the ages of all the
REPRESENTATION OF OLDER PATIENTS IN CLINICAL TRIALSFOR DRUG APPROVAL IN JAPAN
Y. ASAHINA, H. SUGANO, E. SUGIYAMA, Y. UYAMAPharmaceuticals and Medical Devices Agency (PMDA). Corresponding author: Yasuko Asahina, Office of New Drug II, Pharmaceuticals and Medical Devices Agency (PMDA), Shin-
Kasumigaseki Building, 3-3-2 Kasumigaseki Chiyodaku Tokyo 100-0013 Japan, Phone: 3-3506-9451, Fax: 3-3506-9453, E-mail address: [email protected]
Abstract: To examine how target patients seen in clinical practice are represented in clinical trials for approveddrugs in Japan, we compared the age distribution of older patients enrolled in confirmatory clinical trials forregulatory approval with that of the estimated actual patient population. Drugs for 6 chronic conditions commonamong older patients (diabetes mellitus, hypertension, rheumatoid arthritis, non-small cell lung cancer,depression and Alzheimer‘s disease) launched by 2012 in Japan were selected. The disparity in age distributionbetween patients in trials and patients seen in clinical practice varied depending on the disease, but older patients,especially those aged 75 or older, were generally underrepresented in clinical trials for regulatory approval inJapan. Under-representation of older patients in hypertension trials was particularly marked compared to otherconditions, despite the similarity in age distribution of patients seen in clinical practice. One factor causing thisdisparity may be an upper age limit in clinical trial protocols. More effort is needed to properly characterize thebenefits and risks of drugs for older patients. This should include the active enrollment of older patients inclinical trials, the establishment of better assessment tools such as pharmacometric approaches, and theappropriate planning and conducting of post-marketing surveys and studies.
Key words: Clinical trial, patient participation, older patient, Japan.
520
The Journal of Nutrition, Health & Aging©Volume 18, Number 5, 2014
Received October 9, 2013Accepted for publication December 16, 2013
subjects was available. We compared the age distribution ofolder patients enrolled in the confirmatory clinical trials withthat of the estimated age and number of patients seen in clinicalpractice. Also, the relative difference in the number of patientsinvolved in clinical trials and patients seen in clinical practiceas a proportion of patients aged 65 or older and 75 or older wasestimated. To assess the age distribution of patients enrolled inclinical trials and the estimated age and number of elderlypatients seen in clinical practice, we obtained data fromcommon technical documents (CTDs) and/or clinical studyreports submitted to PMDA for regulatory review and from thePatient Survey of 2011 published by the Ministry of Health,Labour and Welfare in Japan (20), respectively.
Results and Discussion
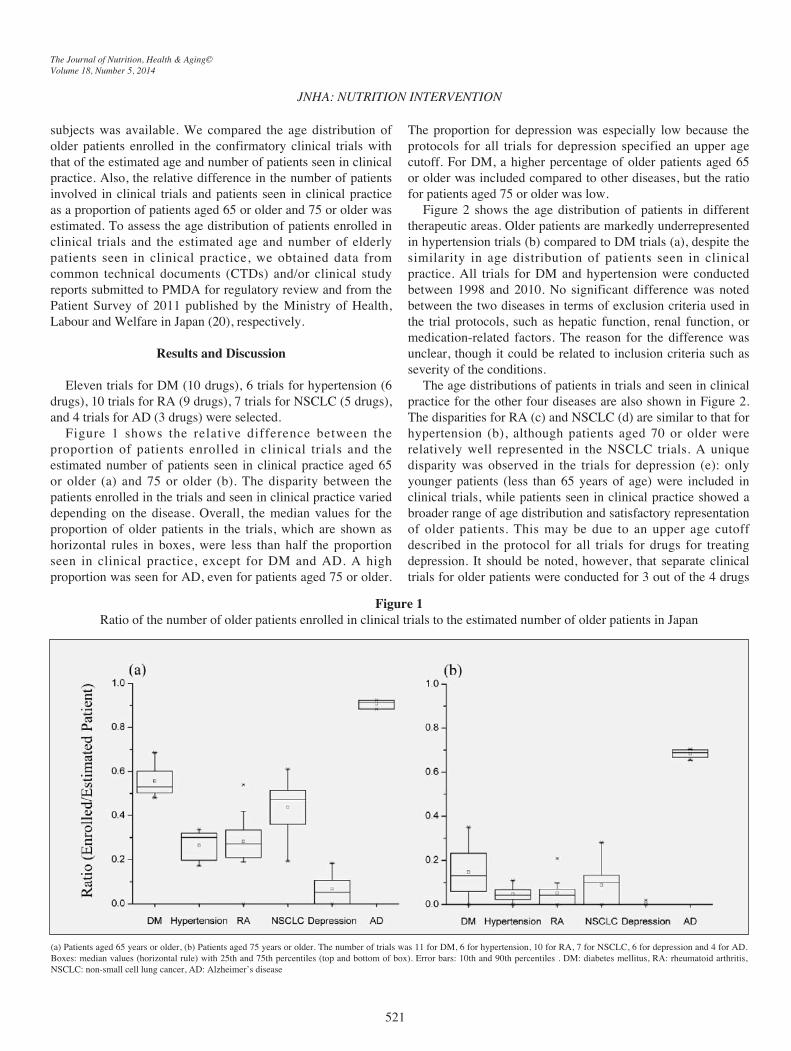
Eleven trials for DM (10 drugs), 6 trials for hypertension (6drugs), 10 trials for RA (9 drugs), 7 trials for NSCLC (5 drugs),and 4 trials for AD (3 drugs) were selected.Figure 1 shows the relative difference between the
proportion of patients enrolled in clinical trials and theestimated number of patients seen in clinical practice aged 65or older (a) and 75 or older (b). The disparity between thepatients enrolled in the trials and seen in clinical practice varieddepending on the disease. Overall, the median values for theproportion of older patients in the trials, which are shown ashorizontal rules in boxes, were less than half the proportionseen in clinical practice, except for DM and AD. A highproportion was seen for AD, even for patients aged 75 or older.
The proportion for depression was especially low because theprotocols for all trials for depression specified an upper agecutoff. For DM, a higher percentage of older patients aged 65or older was included compared to other diseases, but the ratiofor patients aged 75 or older was low.Figure 2 shows the age distribution of patients in different
therapeutic areas. Older patients are markedly underrepresentedin hypertension trials (b) compared to DM trials (a), despite thesimilarity in age distribution of patients seen in clinicalpractice. All trials for DM and hypertension were conductedbetween 1998 and 2010. No significant difference was notedbetween the two diseases in terms of exclusion criteria used inthe trial protocols, such as hepatic function, renal function, ormedication-related factors. The reason for the difference wasunclear, though it could be related to inclusion criteria such asseverity of the conditions.The age distributions of patients in trials and seen in clinical
practice for the other four diseases are also shown in Figure 2.The disparities for RA (c) and NSCLC (d) are similar to that forhypertension (b), although patients aged 70 or older wererelatively well represented in the NSCLC trials. A uniquedisparity was observed in the trials for depression (e): onlyyounger patients (less than 65 years of age) were included inclinical trials, while patients seen in clinical practice showed abroader range of age distribution and satisfactory representationof older patients. This may be due to an upper age cutoffdescribed in the protocol for all trials for drugs for treatingdepression. It should be noted, however, that separate clinicaltrials for older patients were conducted for 3 out of the 4 drugs
JNHA: NUTRITION INTERVENTION
The Journal of Nutrition, Health & Aging©Volume 18, Number 5, 2014
521
Figure 1Ratio of the number of older patients enrolled in clinical trials to the estimated number of older patients in Japan
(a) Patients aged 65 years or older, (b) Patients aged 75 years or older. The number of trials was 11 for DM, 6 for hypertension, 10 for RA, 7 for NSCLC, 6 for depression and 4 for AD.Boxes: median values (horizontal rule) with 25th and 75th percentiles (top and bottom of box). Error bars: 10th and 90th percentiles . DM: diabetes mellitus, RA: rheumatoid arthritis,NSCLC: non-small cell lung cancer, AD: Alzheimer’s disease
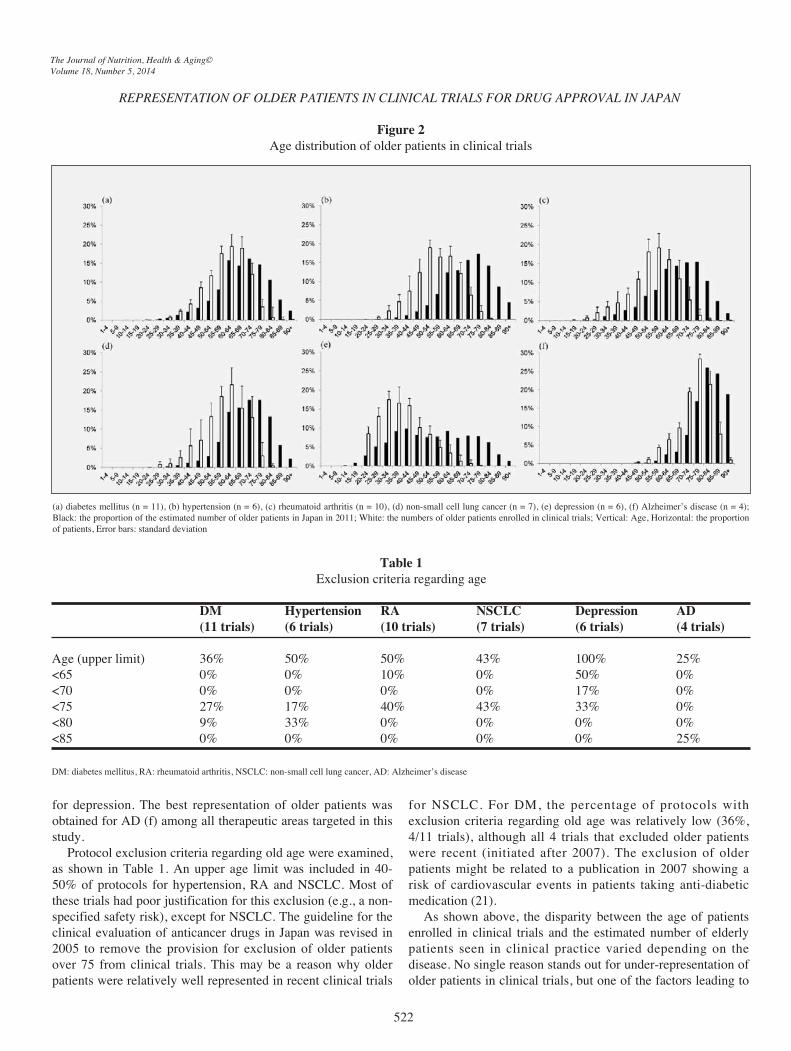
for depression. The best representation of older patients wasobtained for AD (f) among all therapeutic areas targeted in thisstudy.Protocol exclusion criteria regarding old age were examined,
as shown in Table 1. An upper age limit was included in 40-50% of protocols for hypertension, RA and NSCLC. Most ofthese trials had poor justification for this exclusion (e.g., a non-specified safety risk), except for NSCLC. The guideline for theclinical evaluation of anticancer drugs in Japan was revised in2005 to remove the provision for exclusion of older patientsover 75 from clinical trials. This may be a reason why olderpatients were relatively well represented in recent clinical trials
for NSCLC. For DM, the percentage of protocols withexclusion criteria regarding old age was relatively low (36%,4/11 trials), although all 4 trials that excluded older patientswere recent (initiated after 2007). The exclusion of olderpatients might be related to a publication in 2007 showing arisk of cardiovascular events in patients taking anti-diabeticmedication (21).As shown above, the disparity between the age of patients
enrolled in clinical trials and the estimated number of elderlypatients seen in clinical practice varied depending on thedisease. No single reason stands out for under-representation ofolder patients in clinical trials, but one of the factors leading to
REPRESENTATION OF OLDER PATIENTS IN CLINICAL TRIALS FOR DRUG APPROVAL IN JAPAN
The Journal of Nutrition, Health & Aging©Volume 18, Number 5, 2014
522
Figure 2Age distribution of older patients in clinical trials
(a) diabetes mellitus (n = 11), (b) hypertension (n = 6), (c) rheumatoid arthritis (n = 10), (d) non-small cell lung cancer (n = 7), (e) depression (n = 6), (f) Alzheimer’s disease (n = 4);Black: the proportion of the estimated number of older patients in Japan in 2011; White: the numbers of older patients enrolled in clinical trials; Vertical: Age, Horizontal: the proportionof patients, Error bars: standard deviation
Table 1Exclusion criteria regarding age
DM Hypertension RA NSCLC Depression AD(11 trials) (6 trials) (10 trials) (7 trials) (6 trials) (4 trials)
Age (upper limit) 36% 50% 50% 43% 100% 25%<65 0% 0% 10% 0% 50% 0%<70 0% 0% 0% 0% 17% 0%<75 27% 17% 40% 43% 33% 0%<80 9% 33% 0% 0% 0% 0%<85 0% 0% 0% 0% 0% 25%
DM: diabetes mellitus, RA: rheumatoid arthritis, NSCLC: non-small cell lung cancer, AD: Alzheimer’s disease

this disparity might be an unjustified upper age limit presenteven in protocols for trials initiated in 2009. Despite our bestefforts, the inclusion of some kinds of patients in clinical trialsmight be difficult because of their frailty, comorbidity, ormultidrug usage. As mentioned in ICH E7, however, clinicaltrial protocols should not ordinarily include arbitrary upper agecutoffs (22). At the time of approval of many drugs, littleinformation was available about the difference in the magnitudeof risk between older patients and patients younger than 65.This information has mostly been revealed in the post-marketing phase. Regardless, identified differences after drugapproval have sometimes been critical and led to a differentconclusion about benefit/risk balance, resulting in major druglabel revisions regarding the target population or riskdescriptions (4, 8-10). Therefore, it is important to identify thedifference in risk between older and younger patients as muchas possible before marketing.In future clinical trials, more efforts to actively enroll older
patients which represent the target population seen in clinicalpractice will be needed for proper characterization of thebenefit/risk balance of a drug for older patients. At the sametime, methodological tools for better assessing the differencebetween older and younger patients are required. For example,a pharmacometric approach based on pooled data used to assessbenefit/risk in the pediatric population (e.g., modeling &simulation) (23) may also be useful for evaluating safety andefficacy in older patients with multiple risk factors.Furthermore, appropriate planning and conducting of post-marketing surveys/studies are indispensable for the timelydetection and clarification of risks in older patients followingdrug approval.
This views expressed in this article are those of the authorsand do not necessarily reflect the official views of the PMDA.
References
1. United Nations, Department of Economic and Social Affairs, Population Division,2011. World Population Prospects: The 2010 Revision, CD-ROM Edition.http://esa.un.org/wpp/Excel-Data/DB02_Stock_Indicators/WPP2010_DB2_F05_3A_OLD_AGE_DEPENDENCY_RATIO_1564.XLS. Accessed 19 August2013.
2. Cabinet Office. [White paper on aging society (In Japanese)].http://www8.cao.go.jp/kourei/whitepaper/w-2012/zenbun/24pdf_index.html.
Accessed 19 August 2013.3. Corsonello A, Pedone C, Incalzi RA. Age-related pharmacokinetic and
pharmacodynamic changes and related risk of adverse drug reactions. Curr MedChem 2010;17:571-84.
4. Bowie MW, Slattum PW. Pharmacodynamics in older adults: a review. Am J GeriatrPharmacother 2007;5:263-303.
5. Indications for fibrinolytic therapy in suspected acute myocardial infarction:collaborative overview of early mortality and major morbidity results from allrandomised trials of more than 1000 patients. Fibrinolytic Therapy Trialists' (FTT)Collaborative Group. Lancet 1994;343:311-22.
6. Yusuf S, Zhao F, Mehta SR, Chrolavicius S, Tognoni G, Fox KK. Effects ofclopidogrel in addition to aspirin in patients with acute coronary syndromes withoutST-segment elevation. N Engl J Med 2001;345:494-502.
7. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people.Lancet 2013;381:752-62.
8. Information on proper use of Visiclear Combination Tablets. September 2012;http://www.info.pmda.go.jp/iyaku_info/file/kigyo_oshirase_201202_3.pdf.
9. Thiemann DR, Coresh J, Schulman SP, Gerstenblith G, Oetgen WJ, Powe NR. Lackof benefit for intravenous thrombolysis in patients with myocardial infarction whoare older than 75 years. Circulation 2000;101:2239-46.
10. Hylek EM, Evans-Molina C, Shea C, Henault LE, Regan S. Major hemorrhage andtolerability of warfarin in the first year of therapy among elderly patients with atrialfibrillation. Circulation 2007;115:2689-96.
11. Gurwitz JH, Col NF, Avorn J. The exclusion of the elderly and women from clinicaltrials in acute myocardial infarction. JAMA 1992;268:1417-22.
12. Dodd KS, Saczynski JS, Zhao Y, Goldberg RJ, Gurwitz JH. Exclusion of older adultsand women from recent trials of acute coronary syndromes. J Am Geriatr Soc2011;59:506-11.
13. Zulman DM, Sussman JB, Chen X, Cigolle CT, Blaum CS, Hayward RA.Examining the evidence: a systematic review of the inclusion and analysis of olderadults in randomized controlled trials. J Gen Intern Med 2011;26:783-90.
14. Cherubini A, Oristrell J, Pla X, Ruggiero C, Ferretti R, Diestre G, et al. Thepersistent exclusion of older patients from ongoing clinical trials regarding heartfailure. Arch Intern Med 2011;171:550-6.
15. Gill SS, Bronskill SE, Mamdani M, Sykora K, Li P, Shulman KI, et al.Representation of patients with dementia in clinical trials of donepezil. Can J ClinPharmacol 2004;11:e274-85.
16. Murthy VH, Krumholz HM, Gross CP. Participation in cancer clinical trials: race-,sex-, and age-based disparities. JAMA 2004;291:2720-6.
17. European Medicines Agency, Concept paper on the need for a reflection paper onquality aspects of medicines for older people 2013.
18. Diener L, Hugonot-Diener L, Alvino S, Baeyens JP, Bone MF, Chirita D, et al.Guidance synthesis. Medical research for and with older people in Europe: proposedethical guidance for good clinical practice: ethical considerations. The journal ofnutrition, health & aging 2013;17:625-7.
19. Vellas B, Pahor M, Manini T, Rooks D, Guralnik JM, Morley J, et al. Designingpharmaceutical trials for sarcopenia in frail older adults: EU/US Task Forcerecommendations. The journal of nutrition, health & aging 2013;17:612-8.
20. Ministry of Health, Labour and Welfare, 2011. Patient Survey. http://www.e-stat.go.jp/SG1/estat/GL08020101.do?_toGL08020101_&tstatCode=000001031167&requestSender=dsearch. Accessed 19 August 2013.
21. Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardial infarction anddeath from cardiovascular causes. N Engl J Med 2007;356:2457-71.
22. ICH Harmonized Tripartite Guideline. Studies in Support of special populations:GERIATRICS E7 1993. http://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E7/Step4/E7_Guideline.pdf. Accessed 19 August 2013.
23. Manolis E, Osman TE, Herold R, Koenig F, Tomasi P, Vamvakas S, et al. Role ofmodeling and simulation in pediatric investigation plans. Paediatr Anaesth 2011;21:214-21.
JNHA: NUTRITION INTERVENTION
The Journal of Nutrition, Health & Aging©Volume 18, Number 5, 2014
523