report prevention and management diabetes -...
TRANSCRIPT
1of64 | WP7Report
www.chrodis.eu
JA-CHRODISWorkPackage7
Diabetes:acasestudyonstrengtheninghealth
careforpeoplewithchronicdiseases
Surveyonpracticesforpreventionandmanagementof
diabetes
2of64 | WP7Report
www.chrodis.eu
Table of Contents
Executivesummary 3
Acknowledgements 6
Introduction 8
Methods 9
Results 17
GeneralInformation 11
Preventionofdiabetesfocusonpeopleathighrisk 13
Managementofdiabetes 17
Educationprogramsforpersonswithdiabetesandtrainingforprofessionals 24
Educationprogramsforpersonswithdiabetes 24
Trainingprogramsforprofessionals 30
APPENDIX1-DataandnotesbyCountry 35
APPENDIX2-Programs/experiencesreportedinthequestionnaires 52
3of64 | WP7Report
www.chrodis.eu
ExecutiveSummaryThisreportpresentstheresultsofthesurveyonpracticesforpreventionandmanagementof diabetes among the partners of the European Joint Action on Chronic Diseases andPromoting Healthy Ageing across the Life Cycle (JA-CHRODIS), and other countries notinvolvedintheJA.
One of the main objective of JA-CHRODIS is to promote and facilitate a process ofexchange and transfer of good practices between European countries and regions,addressingchronicconditions,withaspecificfocusonhealthpromotionandpreventionofchronicconditions,multi-morbidityanddiabetes.IntheframeoftheJA-CHRODIS,diabetesisconsideredacasestudyonstrengtheninghealthcareforpeoplewithchronicdiseases.
Theworkpackageondiabetes(WP7)focusesonallthemajoraspectsofaseriousdiseaselikediabetes: identificationofpeopleathigh risk,preventionandearlydiagnosis,healthpromotion in people with diabetes, comprehensive multifactorial care, prevention ofcomplications, educational strategies for people with diabetes and training for healthprofessionals. To provide an overview on practices for prevention and management oftype2diabetes,theWP7teamconductedasurveyorganizedintwophases:thefirsthadthe objective to provide a structured overview about current programs (interventions,initiatives, approaches or equivalents) that focus on aspects of primary prevention ofdiabetes,identificationofpeopleathighrisk,earlydiagnosis,preventionofcomplicationsof diabetes, comprehensive multifactorial care, education programs for persons withdiabetes and training for professionals; the second phase is devoted to an in-depthanalysisoftheprogramsidentifiedinthefirstone.
Thisreportpresentstheresultsofthefirstphaseofthesurvey.
Thesurveywasnot intendedtoprovideanexhaustivedescriptionofall theactivitiesondiabetes in the participating countries, in fact the partnerswere asked to report plans,programs, interventions, strategies, experiences that they feltworth tobe reportedandshared.Implicitinthisactivityistheassumptionthatthedescriptionofexperiencesisaneffectivemeans tomake own experience available to others, and to create a capital ofknowledgethatcanbesharedandusedinthefuture.
Summaryresults
A total of nineteen countries,with 63 experts, contributed to the collection of data onprevention and management of diabetes. Seventeen of them were involved in the JA-CHRODIS,RomaniawasreachedthroughEPF,andHungarybyitsrepresentativeintheJAAdvisoryboard.DatawerecollectedintheperiodDecember2014toApril2015.
ThedegreeofcompletenessvariedasafunctionoftheNationalpoliciesondiabetes,ofavailabilityofdata,andofthepartnerwhofilledthequestionnaire.Asanexample,in

4of64 | WP7Report
www.chrodis.eu
BelgiumthequestionnairewasfilledinbytheEuropeanPatientForum,andreflectstheirviewandknowledgeaboutBelgiancontext.InIreland,theEuropeanInstituteofWomen’sHealthgaveitsoverviewonlyonpoliciesandinterventionsonpatienteducation.
Thirteen countries out of the 19 responders have a National Diabetes Plan andmost ofthemhavepoliciesandlegislationatnationallevelthatsupportdiabetesprevention,earlyidentification of people at high risk, education for personswith diabetes and training forprofessionals. Early identification of people at high risk of diabetes too often lacks innational policies. The education of peoplewith diabetes and training for professional aresupportedbynationalpoliciesandlegislationbythe79%ofthecountriesevenif,insomeofthem, theydon’t seemtobe implemented, in factnospecificprograms/interventionsarereported. In about two third of the countries (68.4%), the national information systemprovidesdataonprevalenceorincidenceofdiabetes.
ü PREVENTIONOFDIABETES-FOCUSONPEOPLEATHIGHRISKThe role of prevention in the contrast of diabetes is stated fundamental. Type 2diabetes, in particular, is preventable through lifestyle interventions, aiming atrelativelymodest lifestyle changes, provided for people at high risk to develop thedisease.
In general, the importance of the prevention of diabetes is acknowledged andaddressed in policy level, as 3 out of 4 countries report that diabetes prevention issupportedbynationalpoliciesandlegislations.However,earlyidentificationofpeopleatrisk issupportedonlyby63.2%.Thismight indicatethatpreventionofdiabetes isrecognized at population level (e.g. advocating physical activity and healthy bodyweightasmeanstopreventdiabetes)butspecificactionneedstargetedatpeopleatriskarenotaddressedindiabetespoliciesinallcountries.
ü MANAGEMENTOFDIABETESPersonswithchronicdiseasesrequirenotonlyeffectivetreatment,butalsocontinuityof care, and adequate information and support, so that they can achieve self-managementtothegreatestpossibleextent.
Almostallthecountries,18outofthe19respondents,haveamanagementprogramfordiabetes.About63.2%ofthemarestand-alonenationalprograms,and57.9%areincluded in a more comprehensive national plan. Half of the participant countriesstatedthattheprogramswereimplementedinthelast10years,andabout83%ofalltheimplementedprogramsarecurrentlyrunning.
Onlythe50%oftheprogramstakesintoconsiderationvulnerablegroups,e.g.ethnicminoritiesand lowsocio-economicgroups.Definedcarepathwaysexist todealwithpersons with diabetes, either with or at risk for micro- and macro vascularcomplications,in77.8%ofthecountries.Mostoftheprograms(72.2%)aremonitoredthrough intermediate outcome indicators, 66.7% used process indicators and only
5of64 | WP7Report
www.chrodis.eu
44.4%long-termoutcomeindicators(Fig.B7).The16.7%ofthecountriesdidnotuseanykindofindicator.
ü EDUCATION PROGRAMS FOR PERSONS WITH DIABETES AND TRAINING FORPROFESSIONALS
Educationforpersonswithdiabetesisconsideredanintegralcomponentofdiabetescare,andit'sintendedmainlytodevelopskillsinself-managementandcontributetothe patient empowerment. Effective education provision needs trained healthprofessionals,withexpertiseineducationanddiabetesmanagement.
Onthewhole,15outofthe19participatingcountriesreportededucationprogramsforpersonswithdiabetes.Afewcountriesstatedtohaveaneducationprogramthatexists in a stand-alone national program (15.8%), while 36.8% reported to haveeducation programs that are included in amore comprehensive National plan. Thecore criteria of the quality of education programs are defined, e.g. the goal, therationale, the target group, the setting, the scheduling of the education sessions.Morethanahalfreportedtohaveanevidence-basedcurriculumanddefinedspecificeducation methods and didactics. Only the 60% reported that the curriculum isevaluated, anda lownumberof theparticipatingorganizations (20%) reported thatlong-termeffectindicatorswereused.
Training programs for professionals exist in two out of three of the participatingcountries. The core criteria of the quality of training programs seem to be defined,e.g., the goal, the rationale, the target group, the setting, the scheduling of thetraining sessions.More than a half reported to have an evidence-based curriculumand defined specific training methods and didactics. Only a low number (38.5%)reported that a monitoring of effectiveness and quality of the training program isdefined. Less than a half reported that the training program is based on a theorydrivencurriculumandonlythe30.8%reportedthatintermediateoutcomeindicatorsareappliedtomeasuretrainingprograms.
6of64 | WP7Report
www.chrodis.eu
Acknowledgments
ThisreportderivesfromtheEUJointActiononChronicDiseasesandHealthyAgeingAcrosstheLifeCycle(JA-CHRODIS).
Thefollowingpartnerscontributedtothedevelopmentofthequestionnaire,thecollectionandanalysisofdata,andtodraftingtheReport:
FinlandJaanaLindström,KatjaWikström(THL).GermanyUlrikeRothe,UlfManuwald(TUD).AndreaIcks,SilkeKuske(HHU).ItalyMarinaMaggini,AngelaGiusti,FlaviaLombardo,BrunoCaffari(ISS).NorwayMonicaSørensen(HOD)SloveniaJelkaZaletel(NIJZ)
ThefollowingpartnersandexpertscontributedtothecollectionofdataandtotherevisionoftheReport:
AustriaBrigitteDomittner,SabineHöfler(GÖG),ElisabethRappold,WolfgangGeißler,MartinRobauschBelgiumValentinaStrammiello,VivianedeLavelaye(EPF)CroatiaJosipCulig,MarcelLeppée(STAMPAR)CyprusMyrtoAzina-Chronides(MoH),PaulosPaulou,GeorgiosOympios,MrsViviTreynor,AndreasStylianouFinlandJaanaLindström,KatjaWikström(THL),TiinaLaatikainenFranceAlainBrunot(MoH),PierreGabbach,PierreFontaineGermanyUlrikeRothe(TUD),AndreaIcks(HHU),ChristaScheidt-Nave,EckhardSalzsieder,StefanieGerlach,BerndKulzer,MarionFellmann,StephanMager,Hans-JoachimVerlohren,CorneliaWoitek,JensHofmann,JanSchulze,WolfgangBaier

7of64 | WP7Report
www.chrodis.eu
GreeceTheodoreVontetsianos,PanagiotouThemistoklis(YPE).AlaverasAntonios,NoutsouMarinaHungaryPéterCsizmadia,KrisztinaFeketeIrelandPeggyMaguire,MaeveCusack(EIWH)ItalyMarinaMaggini(ISS),MassimoMassiBenedetti(HIRS),MarcoComaschiLithuaniaZydruneVisockiene(VUHSK),VytautasKasiulevicius,VidaAugustienieneTheNetherlandFrancoisSchellevis(NIVEL)NorwayMonicaSørensen(HOD)PortugalJoséManuelBoavida,CristinaPortugal(DGS)RomaniaCristianAndriciuc,IoanVeresiu,AncaMineaSloveniaJelkaZaletel(NIJZ)SpainAntonioSarríaSantamera,MariadelMarPolodeSantos(ISCIII),JesúsOlivaDomínguez(MSSSI)UKDimitriVarsamis(NHS),NareshKanumilli

8of64 | WP7Report
www.chrodis.eu
Introduction
TheEuropeanJointActiononChronicDiseasesandPromotingHealthyAgeingacrosstheLife Cycle (JA-CHRODIS) addresses the challenge of the increased burden that chronicconditions and diseases place on the health systems and individuals. One of the mainobjectiveofJA-CHRODISistopromoteandfacilitateaprocessofexchangeandtransferofgood practices between European countries and regions, addressing chronic conditions,with a specific focus on health promotion and prevention of chronic conditions, multi-morbidityanddiabetes.
In the frame of the JA-CHRODIS, diabetes is considered a case study on strengtheninghealthcareforpeoplewithchronicdiseases.Diabetesisacommonandseriousdisease:itincreases the risk for many serious health problems (e.g, hypertension, cardiovasculardiseases, eye problems, neuropathy, foot complications, nephropathy), but can beprevented and effectively controlled using available knowledge.With correct treatmentand recommended lifestyle changes,many peoplewith diabetes are able to prevent ordelaytheonsetofcomplications.
Theworkpackageondiabetes(WP7)focusesonallthemajoraspectsofaseriousdiseaselikediabetes: identificationofpeopleathigh risk,preventionandearlydiagnosis,healthpromotion in people with diabetes, comprehensive multifactorial care, prevention ofcomplications, educational strategies for people with diabetes and training for healthprofessionals. JA-CHRODIS isnota researchproject, thus itsmainobjective is touse theknowledgealreadyavailable,toimprovecoordinationandcooperationamongcountriestoact on diabetes, including the exchange of good practices, and to create ground forinnovativeapproachestoreducetheburdenofchronicdiseases.SpecialemphasisisalsogiventosupportthedevelopmentandimplementationofNationalDiabetesPlans.
Toprovideanoverviewonpracticesforpreventionandmanagementoftype2diabetes,theWP7teamconductedasurveyorganizedintwophases:thefirsthadtheobjectivetoprovide a structured overview about current programs (interventions, initiatives,approaches or equivalents) that focus on aspects of primary prevention of diabetes,identification of people at high risk, early diagnosis, prevention of complications ofdiabetes, comprehensive multifactorial care, education programs for persons withdiabetes and training for professionals; the second phase is devoted to an in-depthanalysisoftheprogramsidentifiedinthefirstone.Inthisreportwedescribetheresultsofthefirstphaseofthesurvey.
Thesurveywasnot intendedtoprovideanexhaustivedescriptionofall theactivitiesondiabetes in the participating countries, in fact the partnerswere asked to report plans,programs, interventions, strategies, experiences that they feltworth tobe reportedandshared.Implicitinthisactivityistheassumptionthatthedescriptionofexperiencesisaneffectivemeans tomake own experience available to others, and to create a capital ofknowledgethatcanbesharedandusedinthefuture.
9of64 | WP7Report
www.chrodis.eu
Methods
Thequestionnairewasorganizedin3sections:A-Preventionofdiabetes:focusonpeopleat high risk; B - Management of diabetes; C - Education programs for persons withdiabetesandtrainingforprofessionals.
Eachsectionwasdividedin3parts.Thefirstandsecondpartofeachsectionisdedicatedto a structured description of the main program (intervention, initiative, approach orequivalent) at national, sub-national or local level. The third part of each section isdedicated to a short description of other (up to 3) plans, programs, interventions,strategies,experiencesthattherespondersfeltworthtobereportedandshared.ThelistsofalltheprogramsarereportedintheAppendix2.
Thequestionnairewasdistributedtoallthepartners(associatedandcollaborating)ofJA-CHRODIS.Moreover,theEuropeanPatientForum(EPF,WP7associatedpartner)helpedinfindingexpertsfromcountriesnotinvolvedintheJA.Thepartnerswereinvitedtoidentifyand invite experts working on diabetes (e.g. experts from national, regional and localhealthinstitutesorpublicauthorities,associationsofpersonswithdiabetes,professionalsinvolved in the care of persons with diabetes, …) to contribute in filling in thequestionnaire. A web-based version of the questionnaire was available, thus theresponderscouldchoosewhichversion(pdforweb)touse.
In the countriesweremore thanonepartnerwaspresent,we asked to thepartners toworkonauniquequestionnairetoprovideaCountryoverview.
Datawerecollected in theperiodDecember2014 toApril2015.Dataweresummarizedandreviewedbyeachresponder.
Descriptiveanalysis
A summary descriptive analysis is done for each question indicating the frequency ofcountriesbyeachresponseoption.Blankanswerswereconsideredas“No”.
Percentagesarecalculatedasthetotalofpositiveresponsesonthetotalofthecountriesinvolved in the survey. For thequestions related to specificprograms/interventions, theanalyseswererestrictedonlytocountriesthatreportedsomeofthem.
Each structured question is described by frequency tables and graphs (column and barcharts).
AdetaileddescriptionwithdataandnotesbyCountryisreportedintheAppendix1.
10of64 | WP7Report
www.chrodis.eu
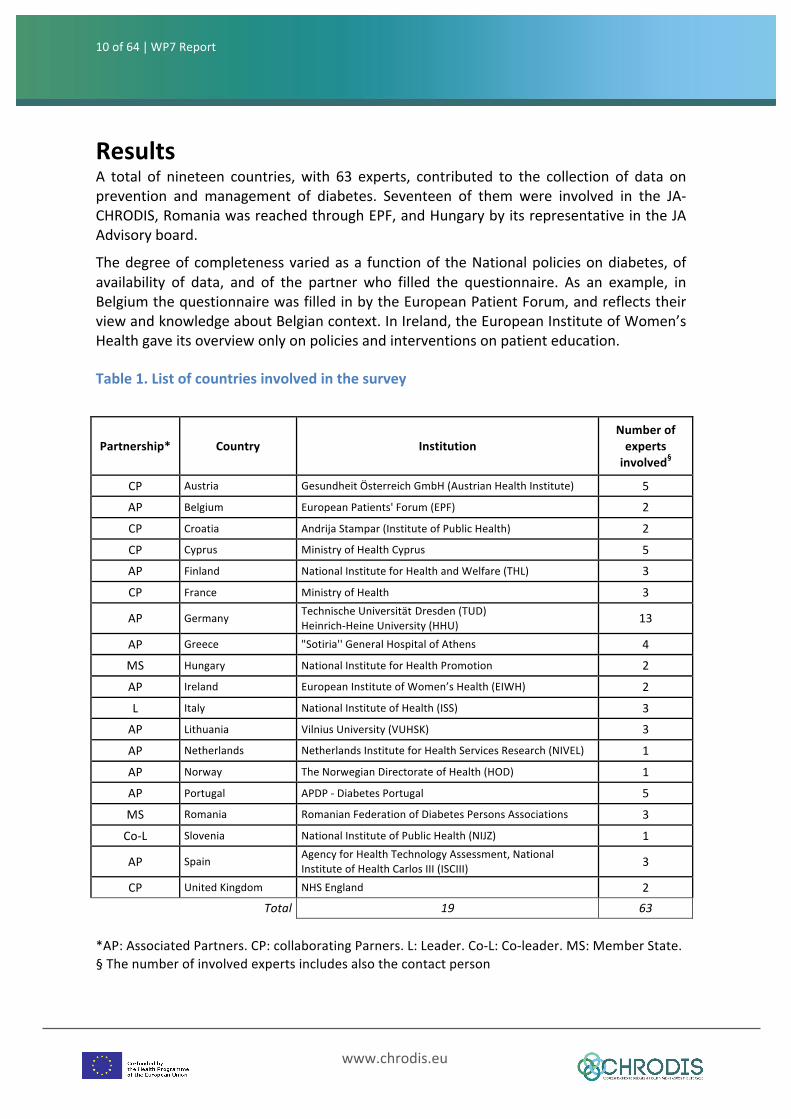
ResultsA total of nineteen countries,with 63 experts, contributed to the collection of data onprevention and management of diabetes. Seventeen of them were involved in the JA-CHRODIS,RomaniawasreachedthroughEPF,andHungarybyitsrepresentativeintheJAAdvisoryboard.
Thedegreeofcompletenessvariedasa functionof theNationalpoliciesondiabetes,ofavailability of data, and of the partner who filled the questionnaire. As an example, inBelgiumthequestionnairewasfilledinbytheEuropeanPatientForum,andreflectstheirviewandknowledgeaboutBelgiancontext.InIreland,theEuropeanInstituteofWomen’sHealthgaveitsoverviewonlyonpoliciesandinterventionsonpatienteducation.
Table1.Listofcountriesinvolvedinthesurvey
Partnership* Country InstitutionNumberofexpertsinvolved§
CP Austria GesundheitÖsterreichGmbH(AustrianHealthInstitute) 5
AP Belgium EuropeanPatients'Forum(EPF) 2
CP Croatia AndrijaStampar(InstituteofPublicHealth) 2
CP Cyprus MinistryofHealthCyprus 5
AP Finland NationalInstituteforHealthandWelfare(THL) 3
CP France MinistryofHealth 3
AP Germany TechnischeUniversitätDresden(TUD)Heinrich-HeineUniversity(HHU) 13
AP Greece "Sotiria''GeneralHospitalofAthens 4
MS Hungary NationalInstituteforHealthPromotion 2
AP Ireland EuropeanInstituteofWomen’sHealth(EIWH) 2
L Italy NationalInstituteofHealth(ISS) 3
AP Lithuania VilniusUniversity(VUHSK) 3
AP Netherlands NetherlandsInstituteforHealthServicesResearch(NIVEL) 1
AP Norway TheNorwegianDirectorateofHealth(HOD) 1
AP Portugal APDP-DiabetesPortugal 5
MS Romania RomanianFederationofDiabetesPersonsAssociations 3
Co-L Slovenia NationalInstituteofPublicHealth(NIJZ) 1
AP Spain AgencyforHealthTechnologyAssessment,NationalInstituteofHealthCarlosIII(ISCIII) 3
CP UnitedKingdom NHSEngland 2 Total 19 63
*AP:AssociatedPartners.CP:collaboratingParners.L:Leader.Co-L:Co-leader.MS:MemberState.§Thenumberofinvolvedexpertsincludesalsothecontactperson
11of64 | WP7Report
www.chrodis.eu
GeneralInformation
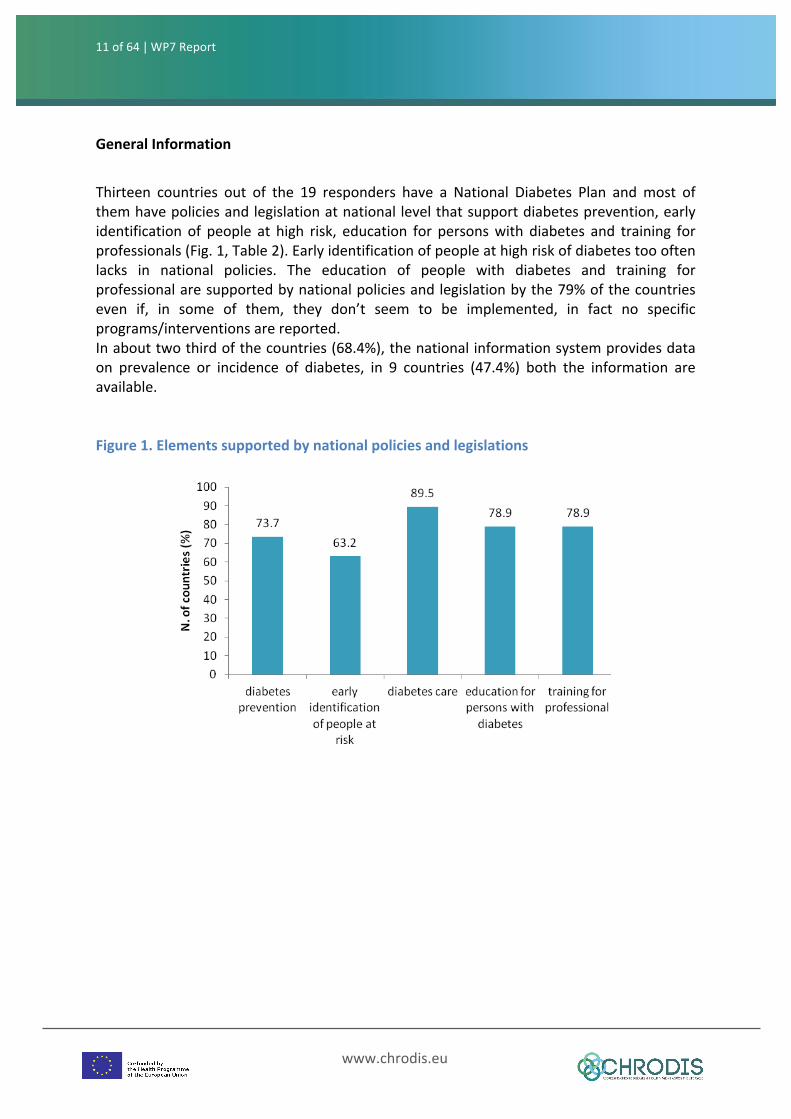
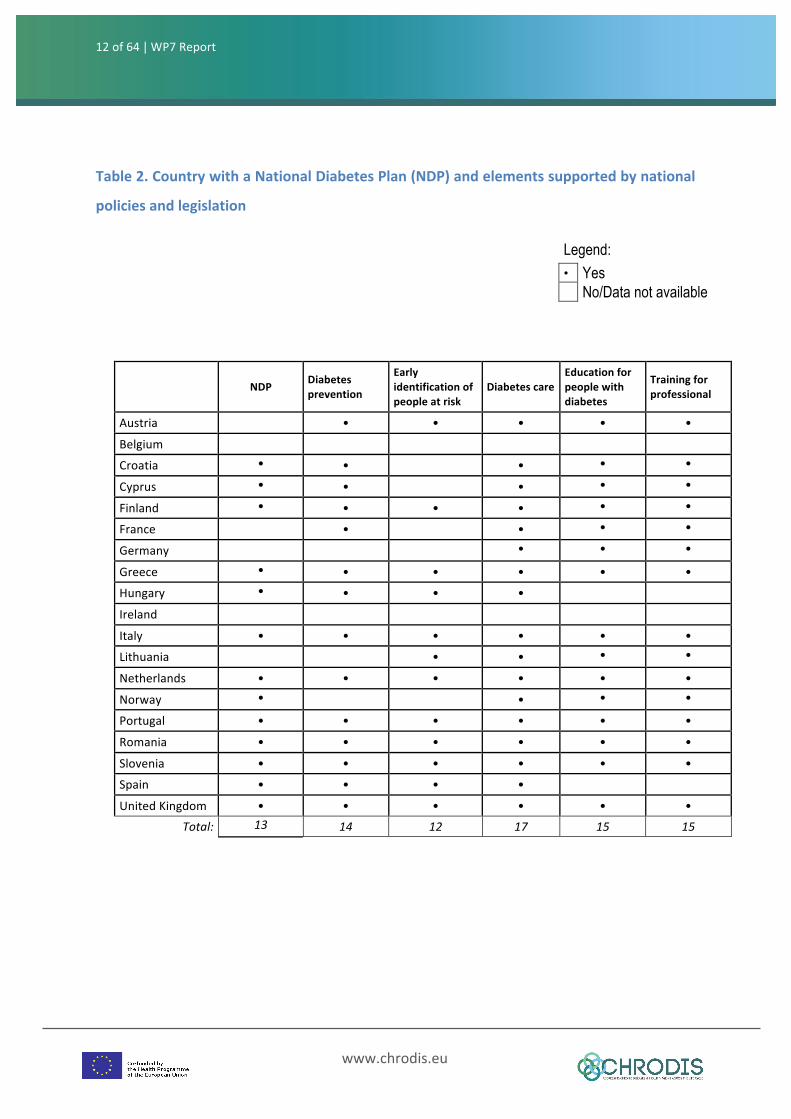
Thirteen countries out of the 19 responders have a National Diabetes Plan andmost ofthemhavepoliciesandlegislationatnationallevelthatsupportdiabetesprevention,earlyidentification of people at high risk, education for personswith diabetes and training forprofessionals(Fig.1,Table2).Earlyidentificationofpeopleathighriskofdiabetestoooftenlacks in national policies. The education of people with diabetes and training forprofessionalaresupportedbynationalpoliciesandlegislationbythe79%ofthecountrieseven if, in some of them, they don’t seem to be implemented, in fact no specificprograms/interventionsarereported.Inabouttwothirdofthecountries(68.4%),thenationalinformationsystemprovidesdataon prevalence or incidence of diabetes, in 9 countries (47.4%) both the information areavailable.Figure1.Elementssupportedbynationalpoliciesandlegislations
12of64 | WP7Report
www.chrodis.eu
Table2.CountrywithaNationalDiabetesPlan(NDP)andelementssupportedbynational
policiesandlegislation
NDP Diabetesprevention
Earlyidentificationofpeopleatrisk
DiabetescareEducationforpeoplewithdiabetes
Trainingforprofessional
Austria • • • • •
Belgium
Croatia • • • • •
Cyprus • • • • •
Finland • • • • • •
France • • • •
Germany • • •
Greece • • • • • •Hungary • • • •
Ireland
Italy • • • • • •
Lithuania • • • •
Netherlands • • • • • •
Norway • • • •
Portugal • • • • • •
Romania • • • • • •
Slovenia • • • • • •
Spain • • • •
UnitedKingdom • • • • • •
Total: 13 14 12 17 15 15
Legend: • Yes No/Data not available
13of64 | WP7Report
www.chrodis.eu
47.4
63.2
47.4
0
10
20
30
40
50
60
70
80
90
100
Stand-alonenationalprogram
includedinamorecomprehensiveNP
sub-national/local level
%A-PREVENTIONOFDIABETES-FOCUSONPEOPLEATHIGHRISK
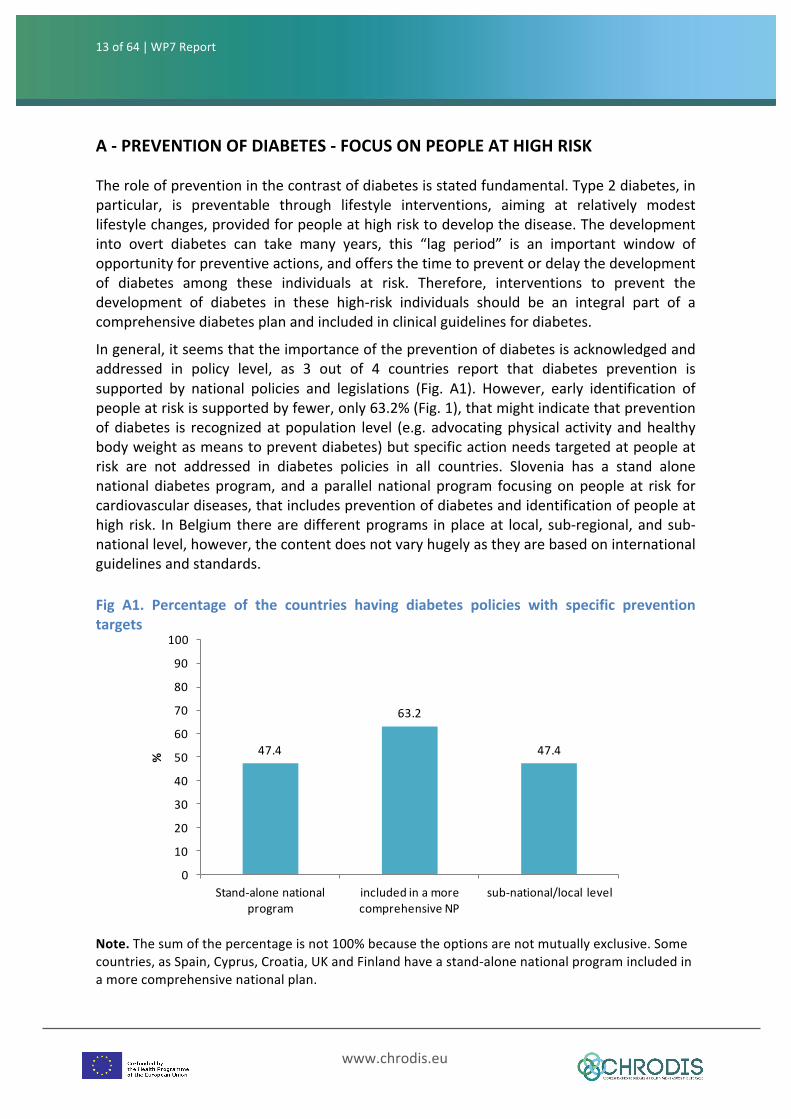
Theroleofpreventioninthecontrastofdiabetesisstatedfundamental.Type2diabetes,inparticular, is preventable through lifestyle interventions, aiming at relatively modestlifestylechanges,providedforpeopleathighrisktodevelopthedisease.Thedevelopmentinto overt diabetes can take many years, this “lag period” is an important window ofopportunityforpreventiveactions,andoffersthetimetopreventordelaythedevelopmentof diabetes among these individuals at risk. Therefore, interventions to prevent thedevelopment of diabetes in these high-risk individuals should be an integral part of acomprehensivediabetesplanandincludedinclinicalguidelinesfordiabetes.
Ingeneral,itseemsthattheimportanceofthepreventionofdiabetesisacknowledgedandaddressed in policy level, as 3 out of 4 countries report that diabetes prevention issupported by national policies and legislations (Fig. A1). However, early identification ofpeopleatriskissupportedbyfewer,only63.2%(Fig.1),thatmightindicatethatpreventionofdiabetes is recognizedatpopulation level (e.g. advocatingphysical activityandhealthybodyweightasmeanstopreventdiabetes)butspecificactionneedstargetedatpeopleatrisk are not addressed in diabetes policies in all countries. Slovenia has a stand alonenationaldiabetesprogram,andaparallel nationalprogram focusingonpeopleat risk forcardiovasculardiseases,thatincludespreventionofdiabetesandidentificationofpeopleathigh risk. InBelgiumtherearedifferentprograms inplaceat local, sub-regional,andsub-nationallevel,however,thecontentdoesnotvaryhugelyastheyarebasedoninternationalguidelinesandstandards. Fig A1. Percentage of the countries having diabetes policies with specific preventiontargets Note.Thesumofthepercentageisnot100%becausetheoptionsarenotmutuallyexclusive.Somecountries,asSpain,Cyprus,Croatia,UKandFinlandhaveastand-alonenationalprogramincludedinamorecomprehensivenationalplan.

14of64 | WP7Report
www.chrodis.eu
72.2 72.2
50.044.4
33.3
16.711.1 11.1 11.1
27.8
0
10
20
30
40
50
60
70
80
90
100
prevalenceofdiabetes
overweightandobesity
physicalactivity recommendationonnutrition
healthcarecostallocated
%
Public
Onrequest
Lithuania has not specific strategies for diabetes prevention, and Ireland (EIWH) didn’tprovideinformationonthistopic.Bothofthemwereexcludedfromthefollowinganalyses,and the percentages are calculated using 17 countries as denominator, except for datareportedinFigA2forwhichLithuaniaanswered.
Diabetes is known to affect disproportionately different social classes: peoplewith lowereducation or income are known to have higher prevalence of diabetes and some ethnicgroupsaremoreatriskthanothers.Thereforeitisofsomewhatconcernthat33.3%ofthecountries respond that these “vulnerable” population groups are not taken intoconsiderationindiabetespreventionstrategies
Prevalenceofdiabetes,overweightandobesityandphysicalactivityarepublicinformationavailableatpopulationlevel(basedoneitherregistersorrepresentativesamples/cohorts),but less frequently the countries have information on health care cost allocated topreventionprograms(FigA2).
FigA2.Availabledataatpopulationlevel
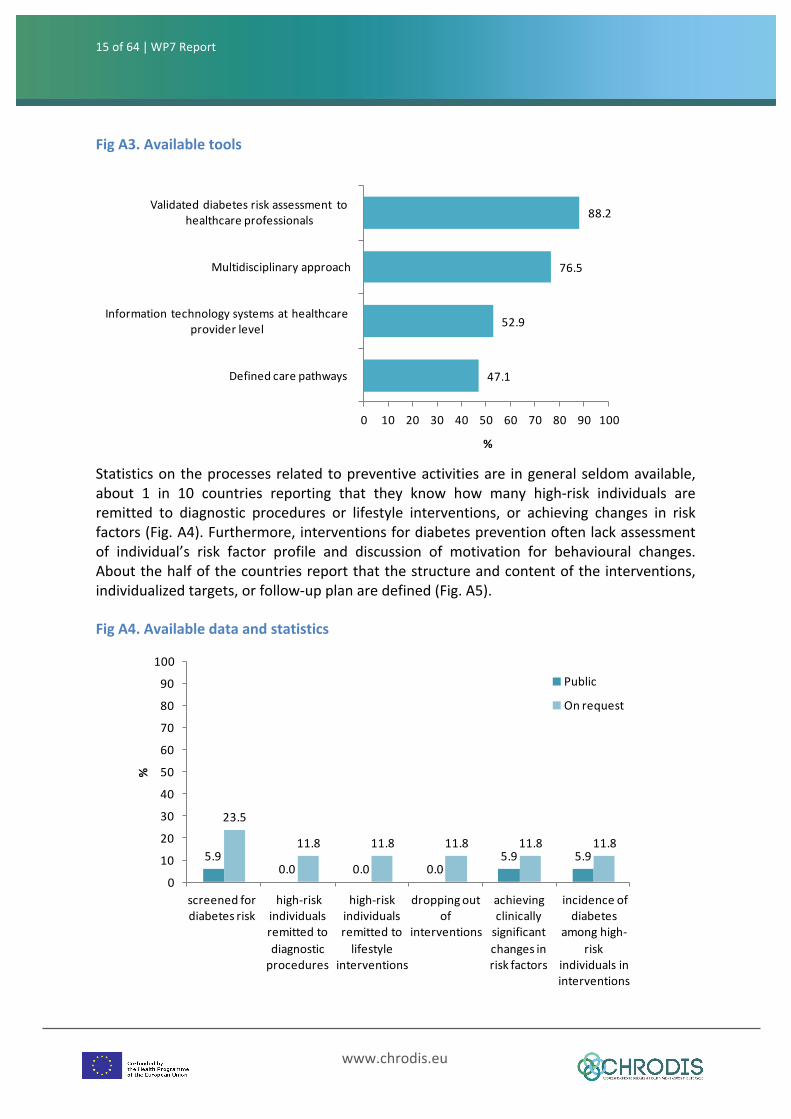
Therespondentsarequiteconfidentthatthehealthcareprofessionalsintheircountriesarewell educated about basics of diabetes prevention, with 94.4% reporting “yes” to thespecific question. However, it is of concern whether this knowledge is implemented inactual work at optimal level. The majority (82.4%) of countries have screeningprotocols/guidelinesavailableforidentificationofhigh-riskpersons,butonlythe29.4%areevaluated at population level. Validated diabetes risk assessment tools are available tohealthcare professionals in almost all (88.2%) the respondent countries.Multidisciplinaryapproach to prevention, which is considered one of the cornerstones of efficaciousprevention, is reported by 76.5%, systems supporting prevention by 52.9%, and definedcare pathways for prevention by only 47.1% of respondents (Fig A3).
15of64 | WP7Report
www.chrodis.eu
47.1
52.9
76.5
88.2
0 10 20 30 40 50 60 70 80 90 100
Definedcarepathways
Informationtechnologysystemsathealthcareproviderlevel
Multidisciplinaryapproach
Validateddiabetesriskassessment tohealthcareprofessionals
%
5.90.0 0.0 0.0
5.9 5.9
23.5
11.8 11.8 11.8 11.8 11.8
0
10
20
30
40
50
60
70
80
90
100
screenedfordiabetesrisk
high-riskindividualsremittedtodiagnosticprocedures
high-riskindividualsremittedtolifestyle
interventions
droppingoutof
interventions
achievingclinicallysignificantchangesinriskfactors
incidenceofdiabetes
amonghigh-risk
individualsininterventions
%
Public
Onrequest
FigA3.Availabletools
Statisticsontheprocessesrelatedtopreventiveactivitiesare ingeneralseldomavailable,about 1 in 10 countries reporting that they know how many high-risk individuals areremitted to diagnostic procedures or lifestyle interventions, or achieving changes in riskfactors(Fig.A4).Furthermore,interventionsfordiabetespreventionoftenlackassessmentof individual’s risk factor profile and discussion of motivation for behavioural changes.Aboutthehalfofthecountriesreportthatthestructureandcontentoftheinterventions,individualizedtargets,orfollow-upplanaredefined(Fig.A5).
FigA4.Availabledataandstatistics
16of64 | WP7Report
www.chrodis.eu
47.1
47.1
52.9
58.8
64.7
0 10 20 30 40 50 60 70 80 90 100
definitionoftheplanforfollow-up
definitionof individualizedtargetsforpreventioninterventions
definitionofthestructureandcontentoftheinterventions
discussionof individual’smotivation forbehaviouralchanges
assessmentofindividual'sriskfactorprofiles
%
41.2
52.9
64.7
76.5
76.5
0 20 40 60 80 100
changeinthequalityofnutrition
changeinwaist circumference
plannedvisitscompleted
changeinglucoselevel
weightchange
%
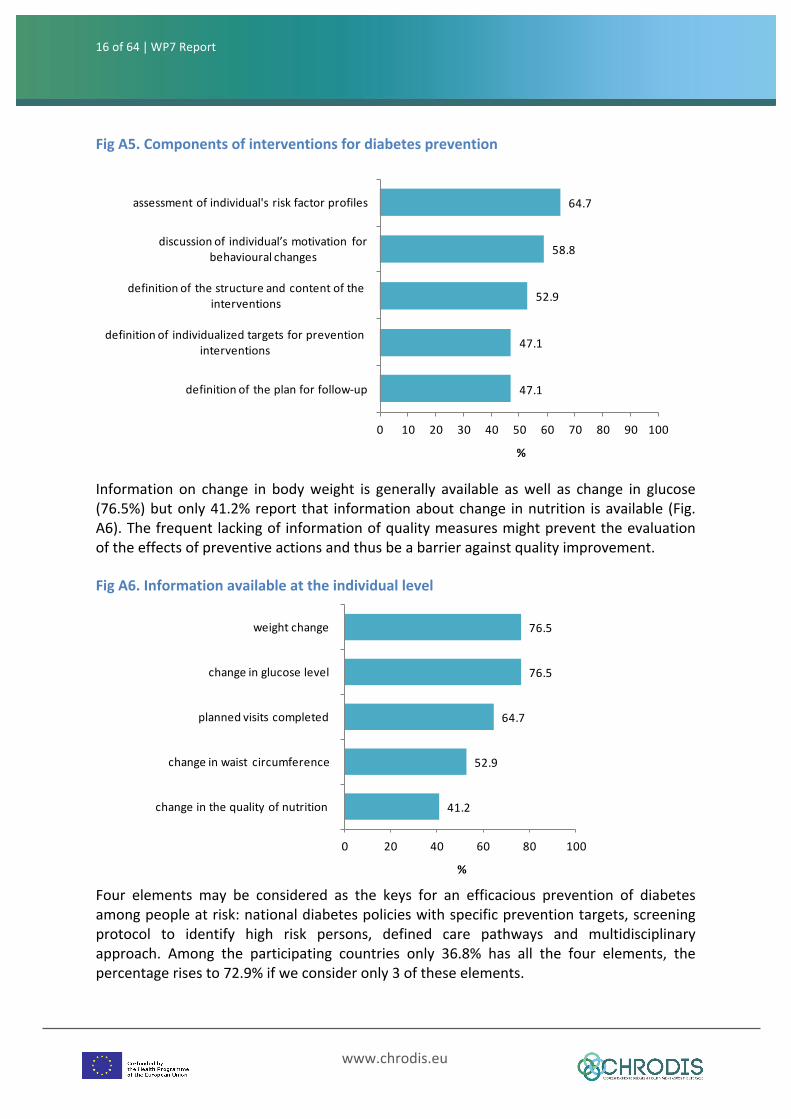
FigA5.Componentsofinterventionsfordiabetesprevention
Information on change in bodyweight is generally available aswell as change in glucose(76.5%)butonly41.2%report that informationaboutchange innutrition isavailable (Fig.A6).Thefrequentlackingof informationofqualitymeasuresmightpreventtheevaluationoftheeffectsofpreventiveactionsandthusbeabarrieragainstqualityimprovement.
FigA6.Informationavailableattheindividuallevel
Four elements may be considered as the keys for an efficacious prevention of diabetesamongpeopleatrisk:nationaldiabetespolicieswithspecificpreventiontargets,screeningprotocol to identify high risk persons, defined care pathways and multidisciplinaryapproach. Among the participating countries only 36.8% has all the four elements, thepercentagerisesto72.9%ifweconsideronly3oftheseelements.
17of64 | WP7Report
www.chrodis.eu
63.257.9
36.8
0102030405060708090
100
Stand-alonenationalprogram
includedinamorecomprehensiveNP
sub-national/local level
%
B-MANAGEMENTOFDIABETES
Personswith chronicdiseases requirenotonly effective treatment, but also continuityofcare,andadequateinformationandsupport,sothattheycanachieveself-managementtothegreatestpossibleextent.Theevidencestronglysuggeststhattoimprovethequalityofcare for people with diabetes, and for most people with chronic diseases, we need toreshapehealthcaresystemstofacilitatethetransitionfromfragmentationtointegrationofcare. A redesigned care system should include an organizedmulti component approach,along with a real partnership between citizens and health professionals, and betweenprimaryandsecondarycare,soastoachievelong-termcoordinatedcarewithandaroundtheneedsofpersonswithdiabetes.
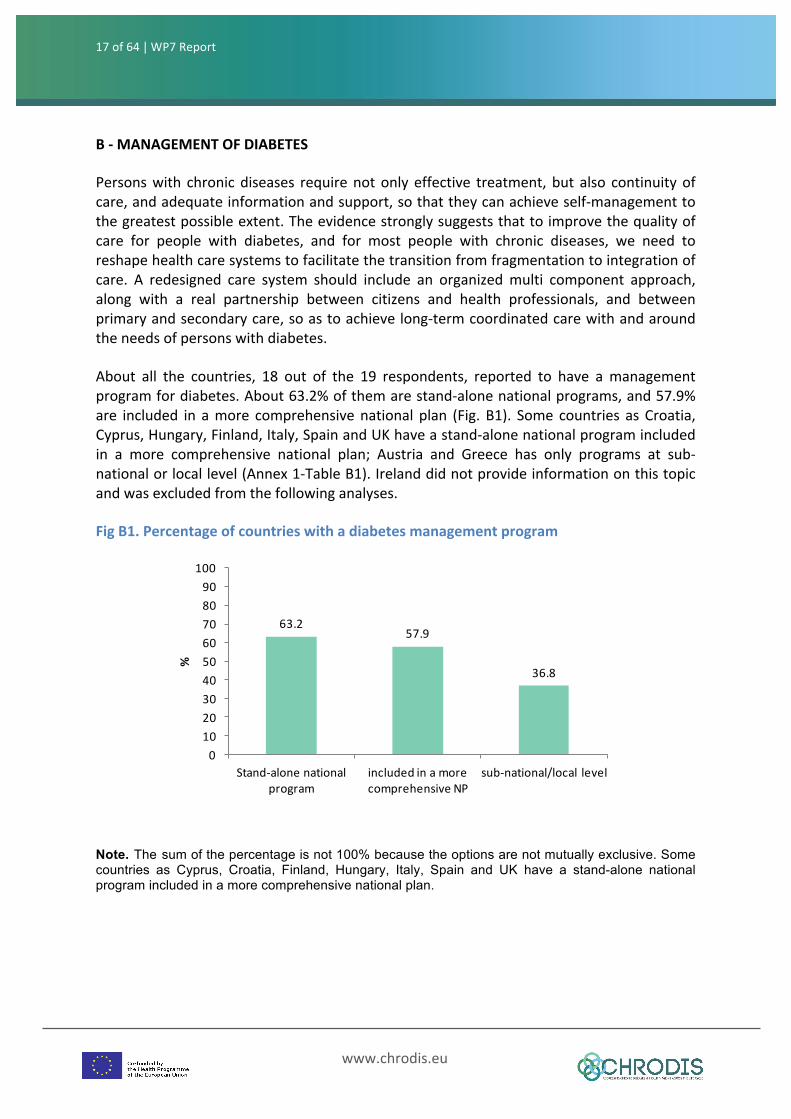
About all the countries, 18 out of the 19 respondents, reported to have amanagementprogramfordiabetes.About63.2%ofthemarestand-alonenationalprograms,and57.9%are included in amore comprehensivenational plan (Fig. B1). Some countries as Croatia,Cyprus,Hungary,Finland,Italy,SpainandUKhaveastand-alonenationalprogramincludedin a more comprehensive national plan; Austria and Greece has only programs at sub-nationalorlocallevel(Annex1-TableB1).Irelanddidnotprovideinformationonthistopicandwasexcludedfromthefollowinganalyses.
FigB1.Percentageofcountrieswithadiabetesmanagementprogram
Note. The sum of the percentage is not 100% because the options are not mutually exclusive. Some countries as Cyprus, Croatia, Finland, Hungary, Italy, Spain and UK have a stand-alone national program included in a more comprehensive national plan.

18of64 | WP7Report
www.chrodis.eu
33.338.9
66.7
77.883.3
0102030405060708090
100
local regional national rural urban
%
Implementationlevel Spread
33.3
72.2
72.2
77.8
83.3
94.4
0 20 40 60 80 100
others
specialistsfordiabeticcomplications
diabetesspecialists inhospital
diabetesspecialists inownpractice
nurses
generalpractitioners
%
The implementation level ismostlynational (66.7%), in 38.9% regional andonly in 33.3%local.Fivecountriesreportedanimplementationatnational,regional,andlocallevel(Annex1-TableB1).Thespreadwasurbanaswellasrural(Fig.B2).
FigB2.Implementationlevelandspread
General practitioners are the health professionals mostly involved in the diabetesmanagement programs (94.4%) followed by nurses (83.3%), diabetes specialists in ownpractices (77.8%), and diabetes specialists in hospitals as well as specialists for diabeticcomplication (72.2%) (Fig. B3). Only 9 countries involve all these health professionalcategories.
FigB3.Healthprofessionalsinvolvedinthediabetesmanagementprogram
Others: diabetes-consultants (Austria); public health specialists (Croatia); dieticians, patient associations, healthcare managers (Italy); governmental decision makers, diabetes organization (Norway); diabetes educators (Spain); pharmacists (Slovenia).
19of64 | WP7Report
www.chrodis.eu
5.644.4
55.655.6
61.161.161.1
66.772.2
77.877.877.877.8
0 20 40 60 80 100
otherreducinginequalitiesinaccesstocare
reducing(public)costspreventing/reducinginappropriatehealthcare
reducinghospitalizationsincreasingmulti-disciplinary/professional collaborationimprovingintegrationoforganizations/careproviders
decreasingmortalityimprovingearlydetectionofco-morbidities
decreasingmorbiditydecreasing/delayingcomplications
improvingqualityofcareimprovingpatientinvolvement
%
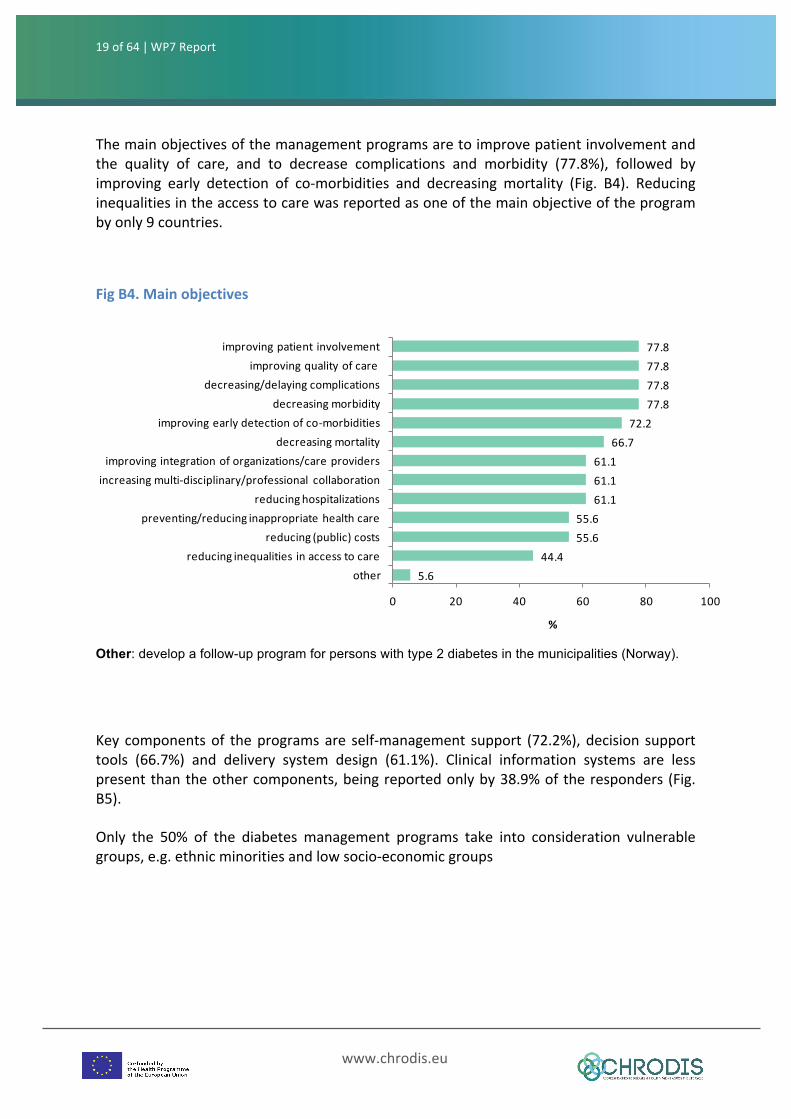
Themainobjectivesofthemanagementprogramsaretoimprovepatientinvolvementandthe quality of care, and to decrease complications and morbidity (77.8%), followed byimproving early detection of co-morbidities and decreasing mortality (Fig. B4). Reducinginequalitiesintheaccesstocarewasreportedasoneofthemainobjectiveoftheprogrambyonly9countries.
FigB4.Mainobjectives
Other: develop a follow-up program for persons with type 2 diabetes in the municipalities (Norway).
Key componentsof theprogramsare self-management support (72.2%),decision supporttools (66.7%) and delivery system design (61.1%). Clinical information systems are lesspresentthantheothercomponents,beingreportedonlyby38.9%oftheresponders(Fig.B5).
Only the 50% of the diabetes management programs take into consideration vulnerablegroups,e.g.ethnicminoritiesandlowsocio-economicgroups
20of64 | WP7Report
www.chrodis.eu
72.266.7
61.1
38.9
0
10
20
30
40
50
60
70
80
90
100
self-management
support
decisionsupporttools
deliverysystemdesign
clinicalinformationsystem
%
11.1
0.0
11.1
11.8
42.1
33.3
44.4
61.1
0 10 20 30 40 50 60 70 80 90 100
other
homecareorganization
insurer
hospitals
patientorganization/association
primarycareorganization/ scientificassociations
diabetologist-endocrinologist/scientificassociations
governmentalbody
%
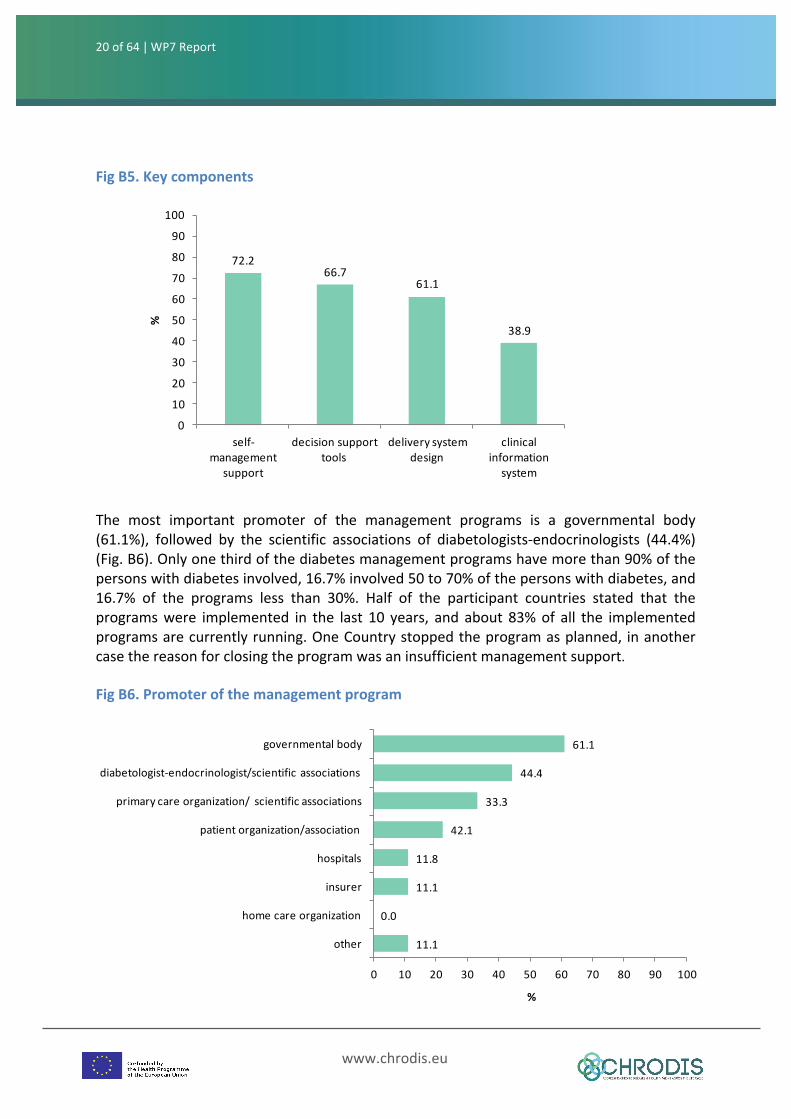
FigB5.Keycomponents
The most important promoter of the management programs is a governmental body(61.1%), followed by the scientific associations of diabetologists-endocrinologists (44.4%)(Fig.B6).Onlyonethirdofthediabetesmanagementprogramshavemorethan90%ofthepersonswithdiabetesinvolved,16.7%involved50to70%ofthepersonswithdiabetes,and16.7% of the programs less than 30%. Half of the participant countries stated that theprogramswere implemented in the last 10 years, and about 83%of all the implementedprogramsarecurrentlyrunning.OneCountrystoppedtheprogramasplanned, inanothercasethereasonforclosingtheprogramwasaninsufficientmanagementsupport.
FigB6.Promoterofthemanagementprogram
21of64 | WP7Report
www.chrodis.eu
66.772.2
44.4
5.6
0
10
20
30
40
50
60
70
80
90
100
processindicators
intermediateoutcomeindicators
long-termeffectindicator
other
%
66.7
38.9
11.15.6
0.0 0.00
10
20
30
40
50
60
70
80
90
100
statutorysystemforhealth
financing
publicinsurers
co-paymentbythepatient
privateinsurers
tradeunions EUstructuralfunds
%Other: public health institutes (Croatia); Steering Committee of National Diabetes Plan (Slovenia).
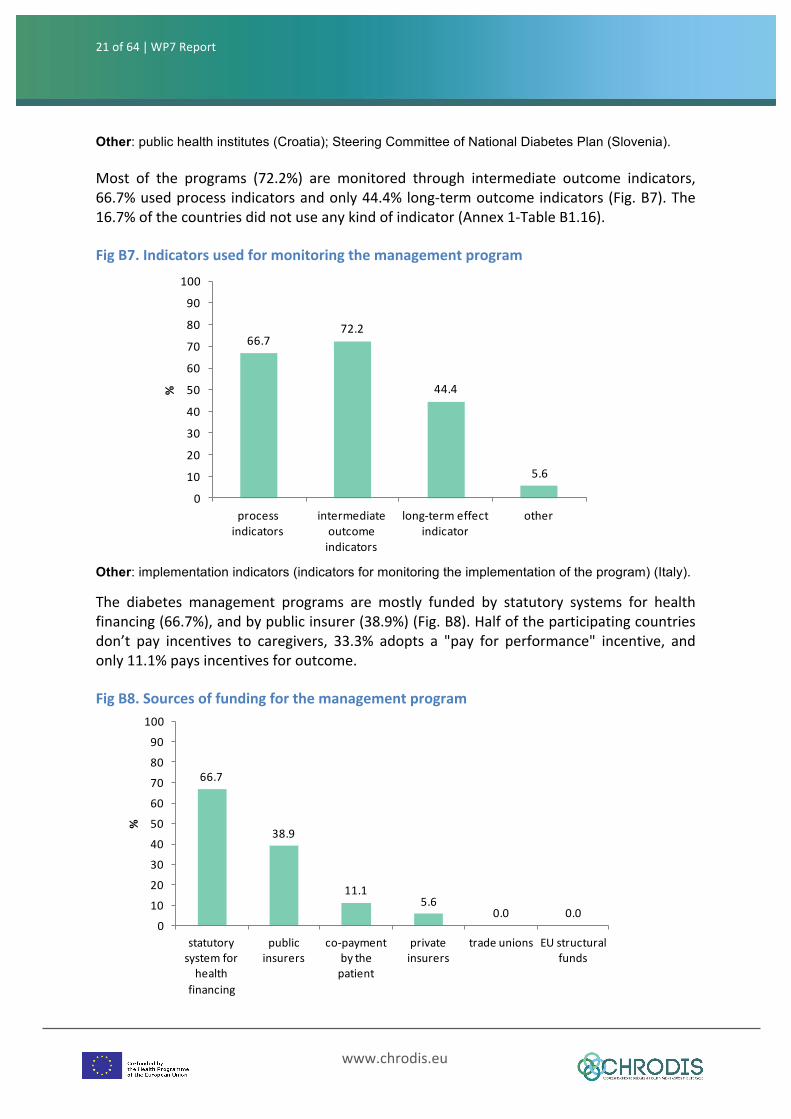
Most of the programs (72.2%) are monitored through intermediate outcome indicators,66.7%usedprocess indicatorsandonly44.4%long-termoutcomeindicators(Fig.B7).The16.7%ofthecountriesdidnotuseanykindofindicator(Annex1-TableB1.16).
FigB7.Indicatorsusedformonitoringthemanagementprogram
Other: implementation indicators (indicators for monitoring the implementation of the program) (Italy). The diabetes management programs are mostly funded by statutory systems for healthfinancing(66.7%),andbypublicinsurer(38.9%)(Fig.B8).Halfoftheparticipatingcountriesdon’t pay incentives to caregivers, 33.3% adopts a "pay for performance" incentive, andonly11.1%paysincentivesforoutcome.
FigB8.Sourcesoffundingforthemanagementprogram
22of64 | WP7Report
www.chrodis.eu
55.6
77.8
83.3
83.3
83.3
94.4
0 20 40 60 80 100
Multidisciplinaryapproachagainst themetabolicsyndrome
Definedcarepathways
Prognosticfactorprofileassessedinpersonswithdiabetes
Cardiovascularriskassessmenttoolsavailable
Screeningprotocolsforearlyidentificationofdiabetes
Curricula/guidelinesofmedicalprofessionals
%
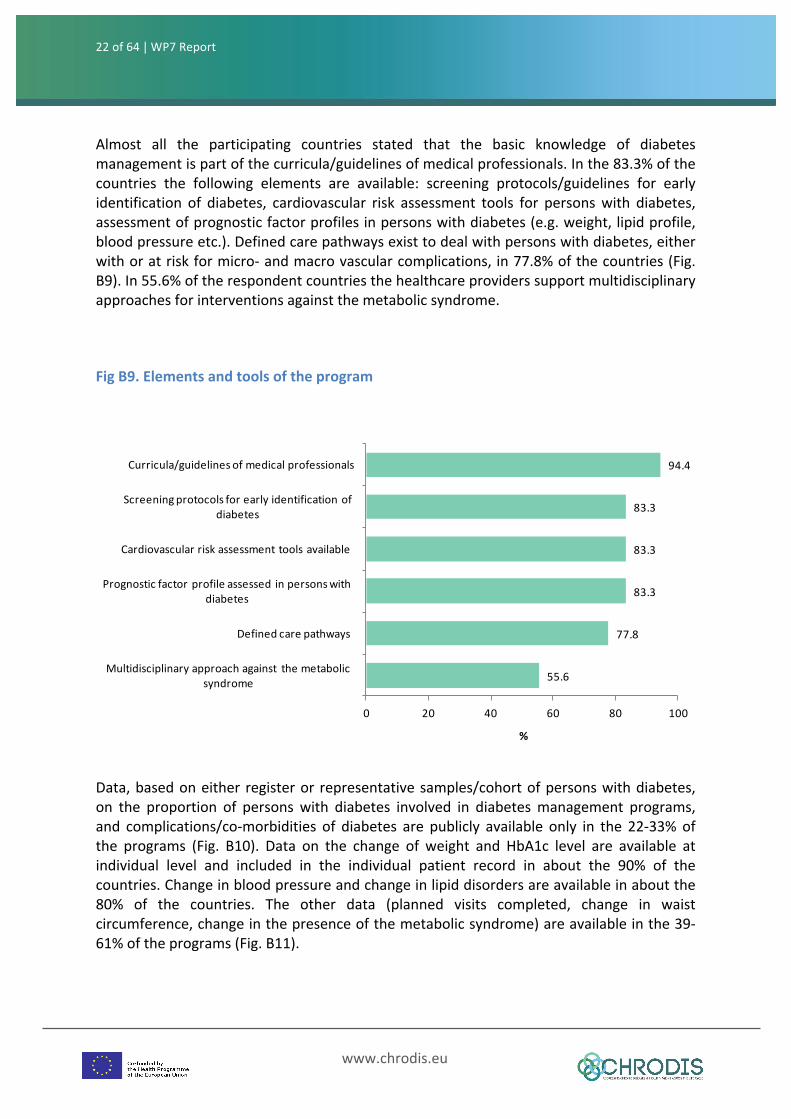
Almost all the participating countries stated that the basic knowledge of diabetesmanagementispartofthecurricula/guidelinesofmedicalprofessionals.Inthe83.3%ofthecountries the following elements are available: screening protocols/guidelines for earlyidentification of diabetes, cardiovascular risk assessment tools for personswith diabetes,assessmentofprognosticfactorprofilesinpersonswithdiabetes(e.g.weight,lipidprofile,bloodpressureetc.).Definedcarepathwaysexisttodealwithpersonswithdiabetes,eitherwithoratriskformicro-andmacrovascularcomplications, in77.8%ofthecountries(Fig.B9).In55.6%oftherespondentcountriesthehealthcareproviderssupportmultidisciplinaryapproachesforinterventionsagainstthemetabolicsyndrome.
FigB9.Elementsandtoolsoftheprogram
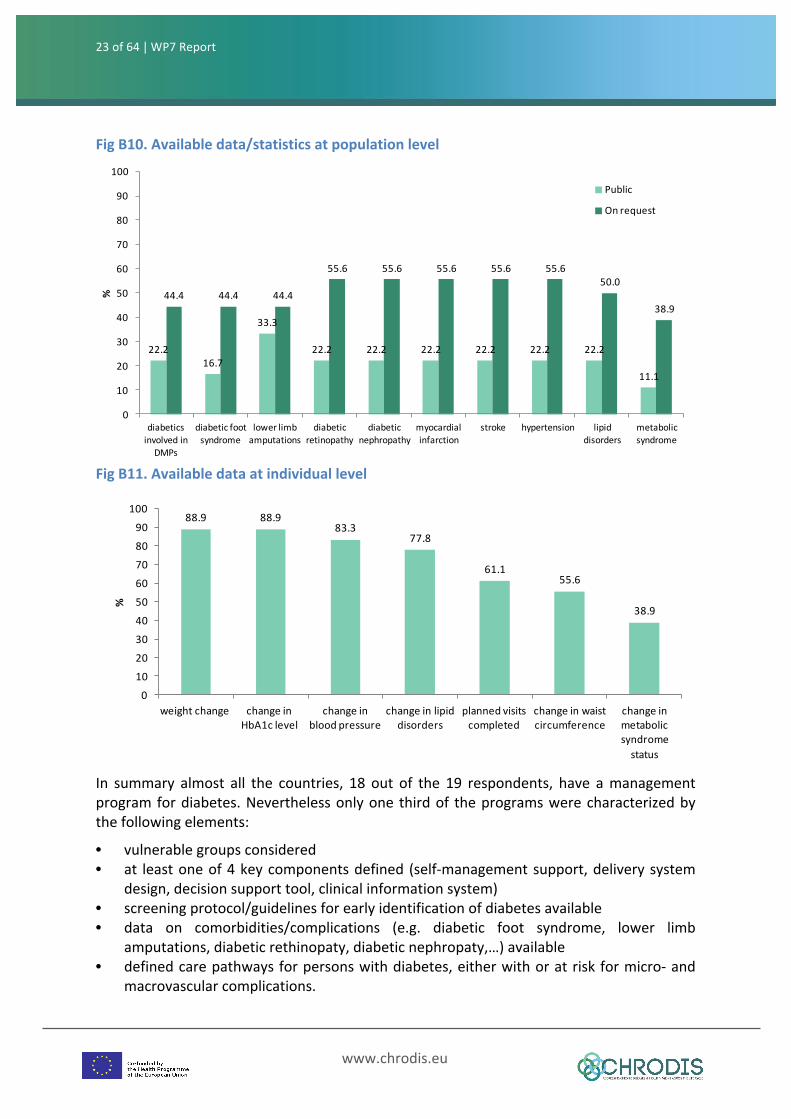
Data,basedoneither registeror representativesamples/cohortofpersonswithdiabetes,on the proportion of personswith diabetes involved in diabetesmanagement programs,and complications/co-morbidities of diabetes are publicly available only in the 22-33%ofthe programs (Fig. B10). Data on the change of weight and HbA1c level are available atindividual level and included in the individual patient record in about the 90% of thecountries.Changeinbloodpressureandchangeinlipiddisordersareavailableinaboutthe80% of the countries. The other data (planned visits completed, change in waistcircumference,changeinthepresenceofthemetabolicsyndrome)areavailableinthe39-61%oftheprograms(Fig.B11).
23of64 | WP7Report
www.chrodis.eu
22.216.7
33.3
22.2 22.2 22.2 22.2 22.2 22.2
11.1
44.4 44.4 44.4
55.6 55.6 55.6 55.6 55.650.0
38.9
0
10
20
30
40
50
60
70
80
90
100
diabeticsinvolvedinDMPs
diabeticfootsyndrome
lowerlimbamputations
diabeticretinopathy
diabeticnephropathy
myocardialinfarction
stroke hypertension lipiddisorders
metabolicsyndrome
%
Public
Onrequest
88.9 88.983.3
77.8
61.155.6
38.9
0
10
20
30
40
50
60
70
80
90
100
weightchange changeinHbA1clevel
changeinbloodpressure
changeinlipiddisorders
plannedvisitscompleted
changeinwaistcircumference
changeinmetabolicsyndromestatus
%
FigB10.Availabledata/statisticsatpopulationlevel
FigB11.Availabledataatindividuallevel
In summary almost all the countries, 18 out of the 19 respondents, have amanagementprogramfordiabetes.Neverthelessonlyone thirdof theprogramswerecharacterizedbythefollowingelements:
• vulnerablegroupsconsidered• at leastoneof4keycomponentsdefined (self-managementsupport,deliverysystem
design,decisionsupporttool,clinicalinformationsystem)• screeningprotocol/guidelinesforearlyidentificationofdiabetesavailable• data on comorbidities/complications (e.g. diabetic foot syndrome, lower limb
amputations,diabeticrethinopaty,diabeticnephropaty,…)available• definedcarepathwaysforpersonswithdiabetes,eitherwithoratriskformicro-and
macrovascularcomplications.

24of64 | WP7Report
www.chrodis.eu
C-EDUCATIONPROGRAMSFORPERSONSWITHDIABETESANDTRAININGFORPROFESSIONALSEducationforpersonswithdiabetesisconsideredanintegralcomponentofdiabetescare,andit'sintendedmainlytodevelopskillsinself-managementandcontributetothepatientempowerment. Effective education provision needs trained health professionals, withexpertiseineducationanddiabetesmanagement.
Inthecontextofpatienteducation,aneducationprogramisaninternationalacceptedandvital interventionwitha targetedstructureofeducation forpeoplewithdiabeteswithanevident effect on the therapy and prognosis of diabetes. Usually, itmeans that the corecontents,goals,methodsanddidacticsaredescribedinacurriculumandmaterialsortoolsfor the educators and participants are provided. Education for persons with diabetes isdescribed as a complex intervention with special requirements on evidence andtransparency regarding its rationale, methodology, performance and outcomerepresentation.
Healthprofessionalsneedtobetrainedtobecomeeffectiveeducators,andthisentailsthattraining programs and curricula are necessary to prepare people for the role of diabeteseducator.Diabeteseducationisaspecialtyandrequiresknowledgeandcompetenceatanadvancedlevelifitistobedeliveredeffectively.
Effectivecurricula, forbotheducatorsandpeoplewithdiabetes,shouldhave instructionalstrategies and approaches based on theories of learning, for example behaviourism,constructivism, social constructivism, that go beyond the cognitive level and addresseshealth determinants, social factors, attitudes, values, norms, and skills that influencespecifichealth-relatedbehaviours.
Educationprogramsforpersonswithdiabetes
On thewhole, 15 out of the 19 participating countries reported education programs forpersonswithdiabetes.Onlyafewcountriesstatedtohaveaneducationprogramthatexistsin a stand-alone national program (15.8%), while 36.8% reported to have educationprograms that are included in amore comprehensiveNational plan. Slightlymore than ahalf(57.9)oftheparticipatingcountriesreportedtohaveeducationprogramsavailableatsub-nationalorlocallevelthatcovereducationactivitiesforpersonswithdiabetes(Fig.C1).Cyprushasastand-alonenationalprogramincludedinamorecomprehensivenationalplan.In Greece, the education of persons with diabetes depends on the diabetic clinics, thediabetesspecialistsortheGPsresponsiblefordiabetesmanagementandcare.Indiabetesclinics there are educational programs in which nurses, psychologists and dieticians areinvolved,butnotaspecificprogramorleadingorganizationcanbedescribed.
25of64 | WP7Report
www.chrodis.eu
100.093.3
100.0 100.0
46.7
66.7
26.7
0
10
20
30
40
50
60
70
80
90
100
healthpromotioninterventions
self-managementeducation
diabetesknowledge
preventionofdiabetes
complications
managementofstress
changeinHbA1clevel
other
%
15.8
36.8
57.9
0
20
40
60
80
100
existsinstand-alonenationalprogram
includedinamorecomprehensiveNP
existsatsub-national/local level
%
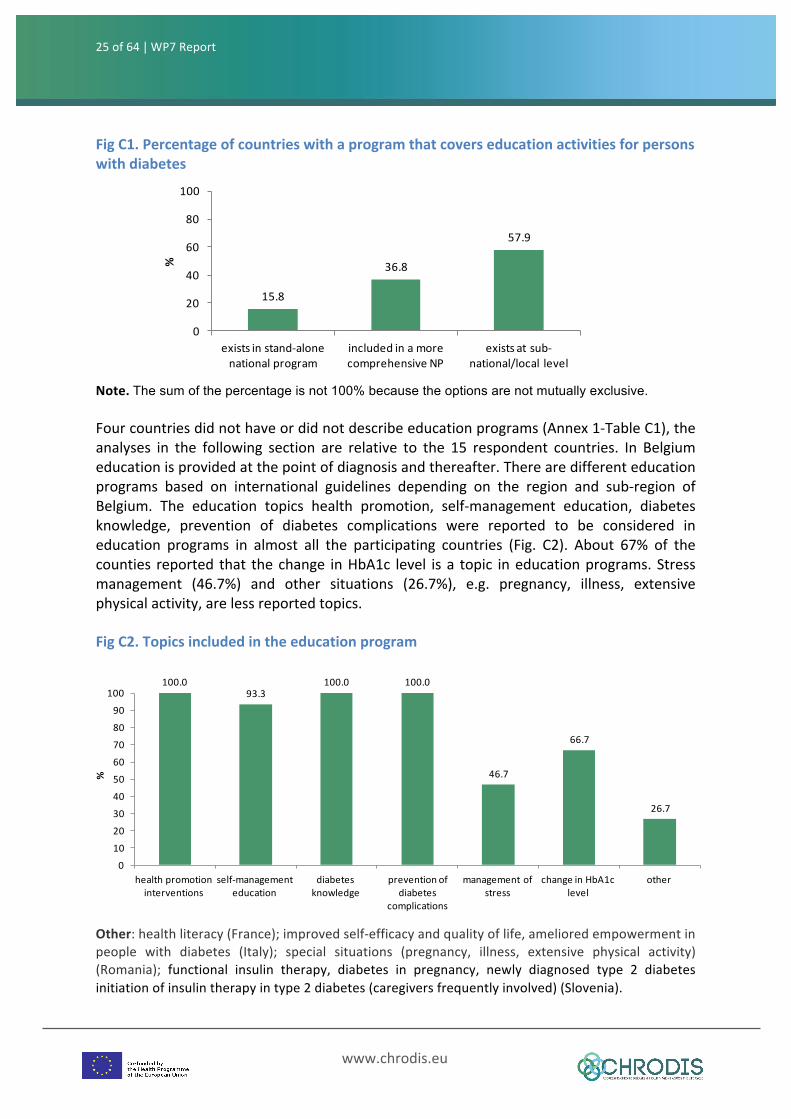
FigC1.Percentageofcountrieswithaprogramthatcoverseducationactivitiesforpersonswithdiabetes
Note.The sum of the percentage is not 100% because the options are not mutually exclusive.
Fourcountriesdidnothaveordidnotdescribeeducationprograms(Annex1-TableC1),theanalyses in the following section are relative to the 15 respondent countries. In Belgiumeducationisprovidedatthepointofdiagnosisandthereafter.Therearedifferenteducationprograms based on international guidelines depending on the region and sub-region ofBelgium. The education topics health promotion, self-management education, diabetesknowledge, prevention of diabetes complications were reported to be considered ineducation programs in almost all the participating countries (Fig. C2). About 67% of thecounties reported that thechange inHbA1c level isa topic ineducationprograms.Stressmanagement (46.7%) and other situations (26.7%), e.g. pregnancy, illness, extensivephysicalactivity,arelessreportedtopics.
FigC2.Topicsincludedintheeducationprogram
Other:healthliteracy(France);improvedself-efficacyandqualityoflife,amelioredempowermentinpeople with diabetes (Italy); special situations (pregnancy, illness, extensive physical activity)(Romania); functional insulin therapy, diabetes in pregnancy, newly diagnosed type 2 diabetesinitiationofinsulintherapyintype2diabetes(caregiversfrequentlyinvolved)(Slovenia).
26of64 | WP7Report
www.chrodis.eu
53.353.353.3
60.060.0
66.766.766.7
73.386.786.7
0 10 20 30 40 50 60 70 80 90 100
sourceoffundingmonitoringeffectivenessandquality
environmentalrequirementsqualificationofthetrainers/educators
numberofparticipantscorecomponentsoftheeducator/trainer'srole
schedulingoftheeducationsessionssetting
targetgrouprationale
goals
%
86.7
60.066.7
40.0
26.7
0102030405060708090
100
allthepersonswithdiabetes
personswithdiabeteswithco-
morbidities
personswithanewdiagnosisofdiabetes
relatives,caregivers
other
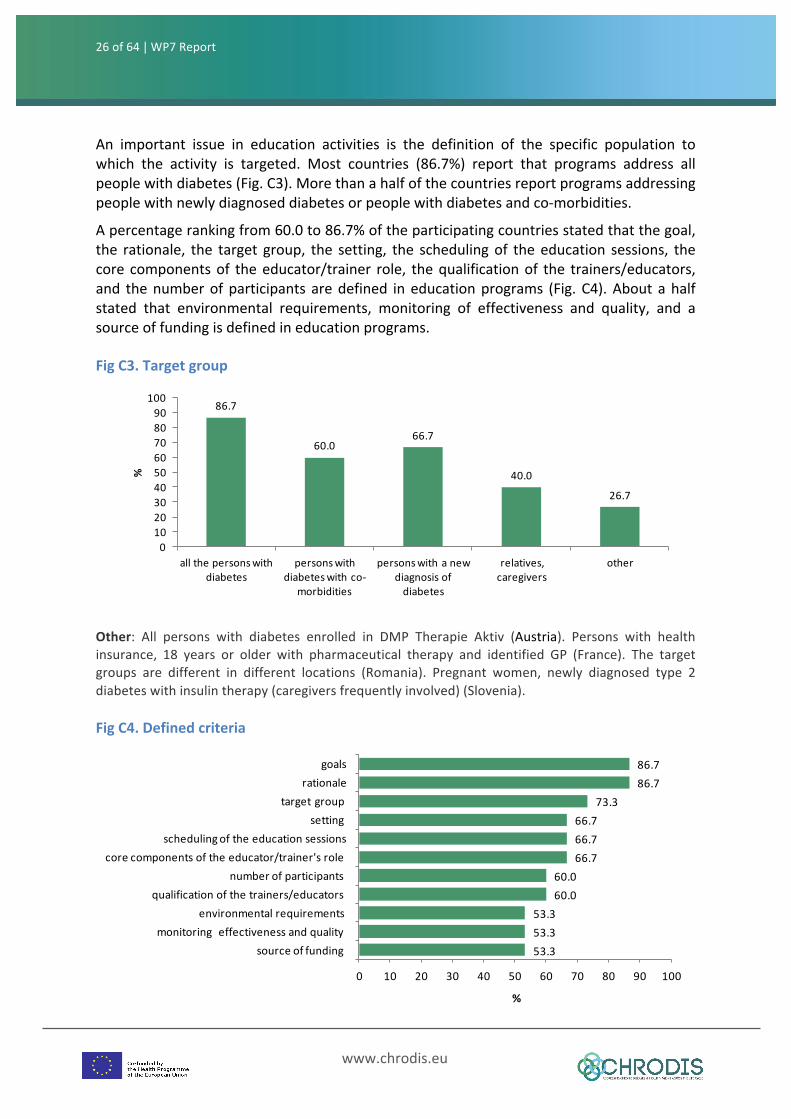
%An important issue in education activities is the definition of the specific population towhich the activity is targeted. Most countries (86.7%) report that programs address allpeoplewithdiabetes(Fig.C3).Morethanahalfofthecountriesreportprogramsaddressingpeoplewithnewlydiagnoseddiabetesorpeoplewithdiabetesandco-morbidities.
Apercentagerankingfrom60.0to86.7%oftheparticipatingcountriesstatedthatthegoal,the rationale, the target group, the setting, the schedulingof theeducation sessions, thecore componentsof theeducator/trainer role, thequalificationof the trainers/educators,and thenumberofparticipants aredefined ineducationprograms (Fig.C4).Aboutahalfstated that environmental requirements, monitoring of effectiveness and quality, and asourceoffundingisdefinedineducationprograms.
FigC3.Targetgroup
Other: All persons with diabetes enrolled in DMP Therapie Aktiv (Austria). Persons with healthinsurance, 18 years or older with pharmaceutical therapy and identified GP (France). The targetgroups are different in different locations (Romania). Pregnant women, newly diagnosed type 2diabeteswithinsulintherapy(caregiversfrequentlyinvolved)(Slovenia).
FigC4.Definedcriteria
27of64 | WP7Report
www.chrodis.eu
46.7
60.066.7
73.366.7
0102030405060708090
100
theorydrivencurriculum
evaluatedcurriculum
evidencebased
curriculum
specificeducationmethods
specificeducationdidactics
60.0 60.0
40.0
93.3100.0
0102030405060708090100
local regional national rural urban
%
Implementationlevel Spread
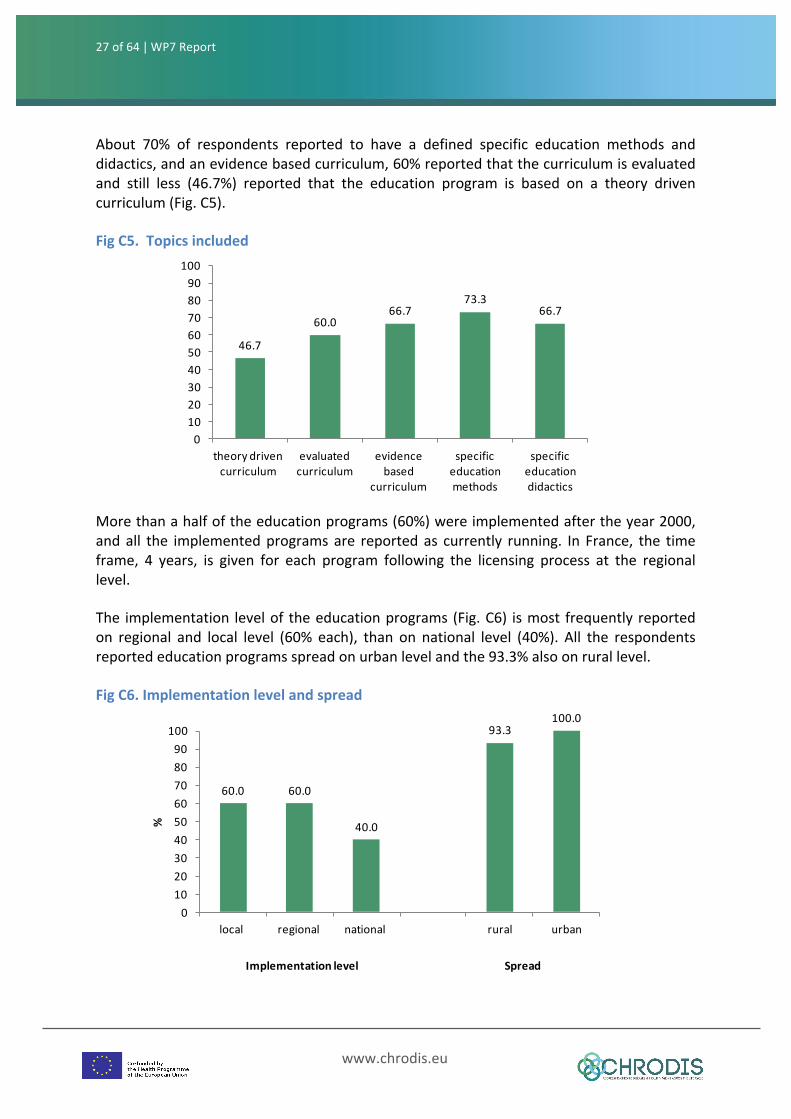
About 70% of respondents reported to have a defined specific education methods anddidactics,andanevidencebasedcurriculum,60%reportedthatthecurriculumisevaluatedand still less (46.7%) reported that the education program is based on a theory drivencurriculum(Fig.C5).
FigC5.Topicsincluded
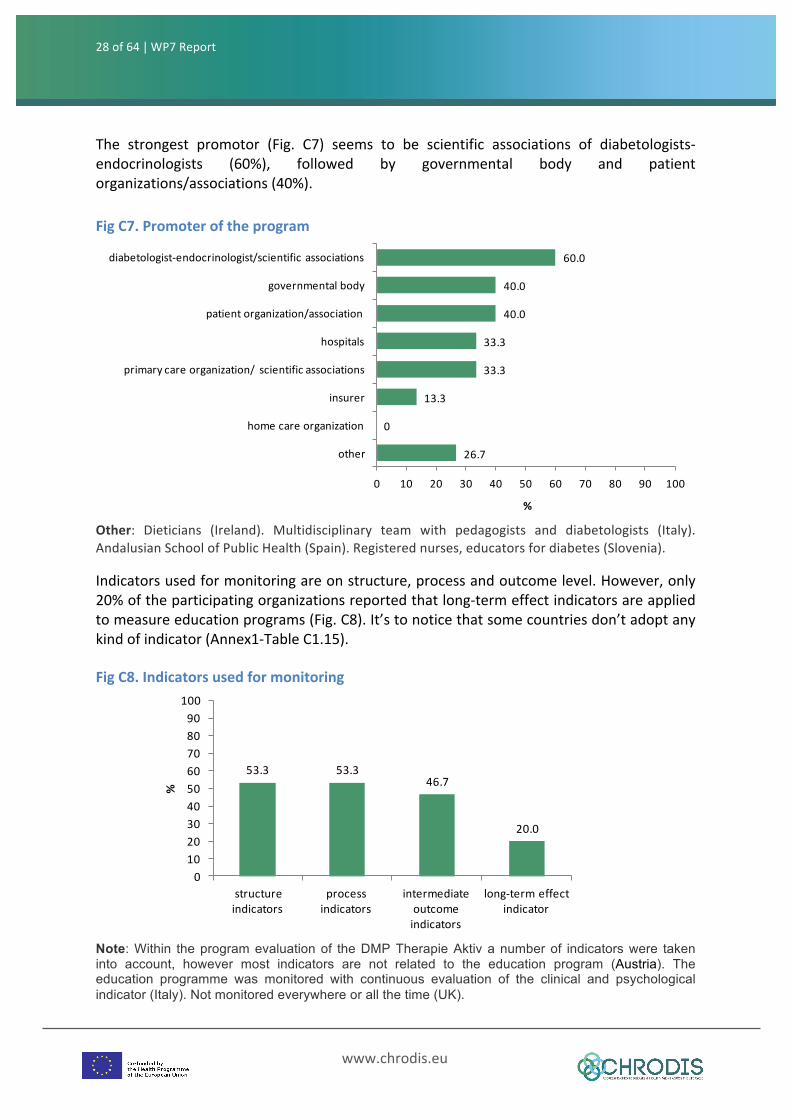
Morethanahalfoftheeducationprograms(60%)wereimplementedaftertheyear2000,andall the implementedprogramsare reportedas currently running. In France, the timeframe, 4 years, is given for each program following the licensing process at the regionallevel.
The implementation levelof theeducationprograms(Fig.C6) ismost frequently reportedon regional and local level (60% each), than on national level (40%). All the respondentsreportededucationprogramsspreadonurbanlevelandthe93.3%alsoonrurallevel.
FigC6.Implementationlevelandspread
28of64 | WP7Report
www.chrodis.eu
26.7
0
13.3
33.3
33.3
40.0
40.0
60.0
0 10 20 30 40 50 60 70 80 90 100
other
homecareorganization
insurer
primarycareorganization/ scientificassociations
hospitals
patientorganization/association
governmentalbody
diabetologist-endocrinologist/scientificassociations
%
53.3 53.346.7
20.0
0102030405060708090100
structureindicators
processindicators
intermediateoutcomeindicators
long-termeffectindicator
%
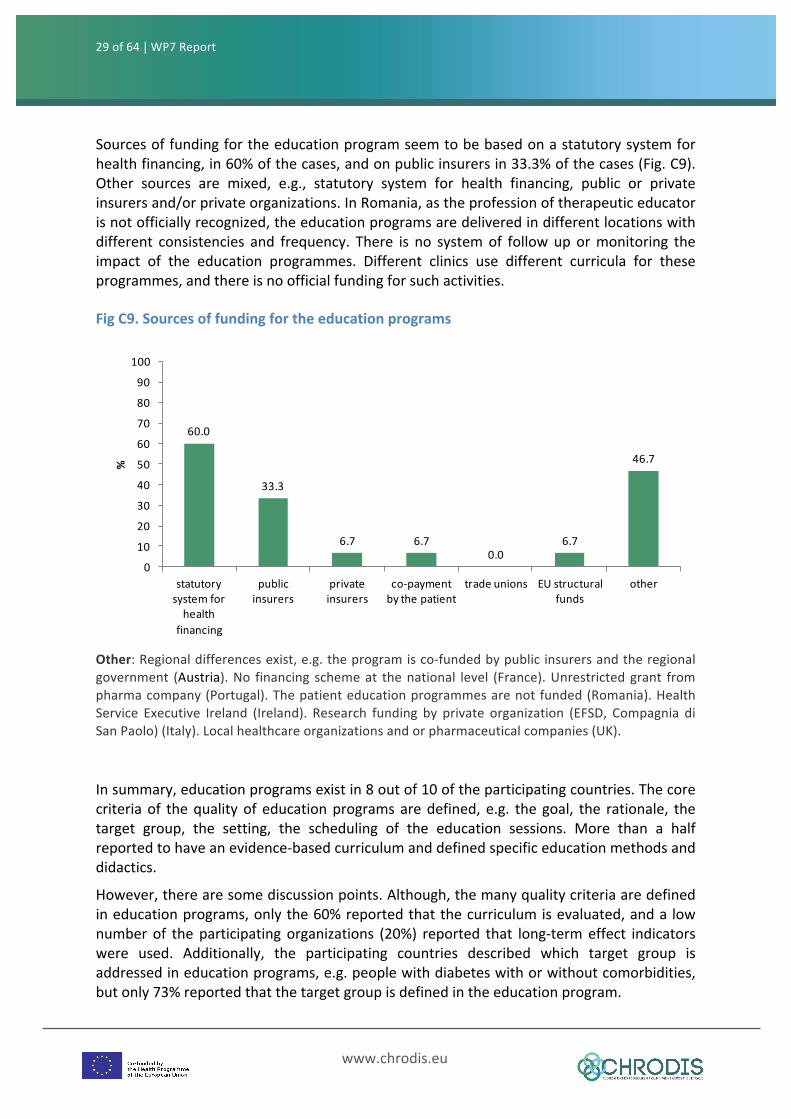
The strongest promotor (Fig. C7) seems to be scientific associations of diabetologists-endocrinologists (60%), followed by governmental body and patientorganizations/associations(40%). FigC7.PromoteroftheprogramOther: Dieticians (Ireland). Multidisciplinary team with pedagogists and diabetologists (Italy).AndalusianSchoolofPublicHealth(Spain).Registerednurses,educatorsfordiabetes(Slovenia). Indicatorsusedformonitoringareonstructure,processandoutcomelevel.However,only20%oftheparticipatingorganizationsreportedthatlong-termeffectindicatorsareappliedtomeasureeducationprograms(Fig.C8).It’stonoticethatsomecountriesdon’tadoptanykindofindicator(Annex1-TableC1.15).
FigC8.Indicatorsusedformonitoring
Note: Within the program evaluation of the DMP Therapie Aktiv a number of indicators were taken into account, however most indicators are not related to the education program (Austria). The education programme was monitored with continuous evaluation of the clinical and psychological indicator (Italy). Not monitored everywhere or all the time (UK).
29of64 | WP7Report
www.chrodis.eu
60.0
33.3
6.7 6.70.0
6.7
46.7
0
10
20
30
40
50
60
70
80
90
100
statutorysystemforhealth
financing
publicinsurers
privateinsurers
co-paymentbythepatient
tradeunions EUstructuralfunds
other
%
Sourcesoffundingfortheeducationprogramseemtobebasedonastatutorysystemforhealthfinancing,in60%ofthecases,andonpublicinsurersin33.3%ofthecases(Fig.C9).Other sources are mixed, e.g., statutory system for health financing, public or privateinsurersand/orprivateorganizations.InRomania,astheprofessionoftherapeuticeducatorisnotofficiallyrecognized,theeducationprogramsaredeliveredindifferentlocationswithdifferent consistencies and frequency. There is no systemof followup ormonitoring theimpact of the education programmes. Different clinics use different curricula for theseprogrammes,andthereisnoofficialfundingforsuchactivities.
FigC9.Sourcesoffundingfortheeducationprograms
Other:Regionaldifferencesexist,e.g.theprogramisco-fundedbypublicinsurersandtheregionalgovernment (Austria).No financing schemeat thenational level (France).Unrestrictedgrant frompharmacompany(Portugal).Thepatienteducationprogrammesarenotfunded(Romania).HealthService Executive Ireland (Ireland). Research funding by private organization (EFSD, Compagnia diSanPaolo)(Italy).Localhealthcareorganizationsandorpharmaceuticalcompanies(UK).
Insummary,educationprogramsexistin8outof10oftheparticipatingcountries.Thecorecriteriaof thequalityof educationprogramsaredefined, e.g. thegoal, the rationale, thetarget group, the setting, the scheduling of the education sessions. More than a halfreportedtohaveanevidence-basedcurriculumanddefinedspecificeducationmethodsanddidactics.
However,therearesomediscussionpoints.Although,themanyqualitycriteriaaredefinedineducationprograms,onlythe60%reportedthatthecurriculumisevaluated,anda lownumberof theparticipatingorganizations (20%) reported that long-termeffect indicatorswere used. Additionally, the participating countries described which target group isaddressedineducationprograms,e.g.peoplewithdiabeteswithorwithoutcomorbidities,butonly73%reportedthatthetargetgroupisdefinedintheeducationprogram.
30of64 | WP7Report
www.chrodis.eu
21.110.5
47.4
0102030405060708090100
existsinstand-alonenationalprogram
includedinamorecomprehensiveNP
existsatsub-national/local level
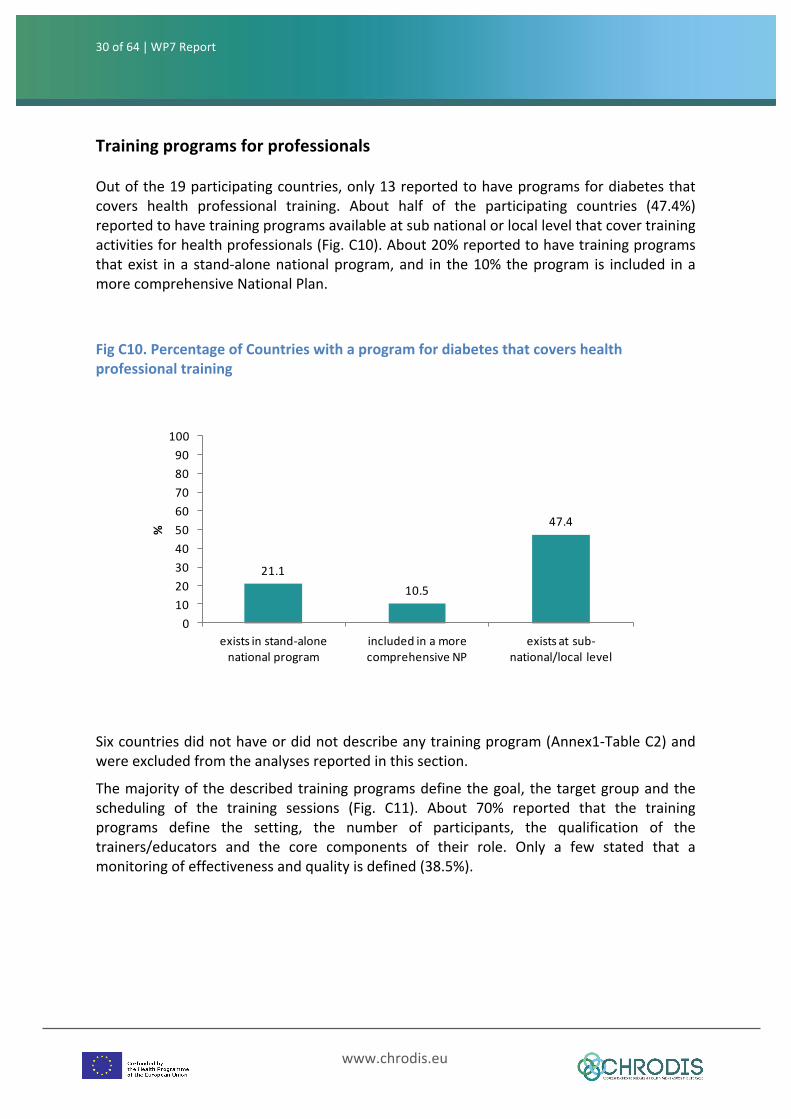
%TrainingprogramsforprofessionalsOutofthe19participatingcountries,only13reportedtohaveprogramsfordiabetesthatcovers health professional training. About half of the participating countries (47.4%)reportedtohavetrainingprogramsavailableatsubnationalorlocallevelthatcovertrainingactivitiesforhealthprofessionals(Fig.C10).About20%reportedtohavetrainingprogramsthatexist ina stand-alonenationalprogram,and in the10%theprogram is included inamorecomprehensiveNationalPlan.
FigC10.PercentageofCountrieswithaprogramfordiabetesthatcovershealthprofessionaltraining
Sixcountriesdidnothaveordidnotdescribeanytrainingprogram(Annex1-TableC2)andwereexcludedfromtheanalysesreportedinthissection.
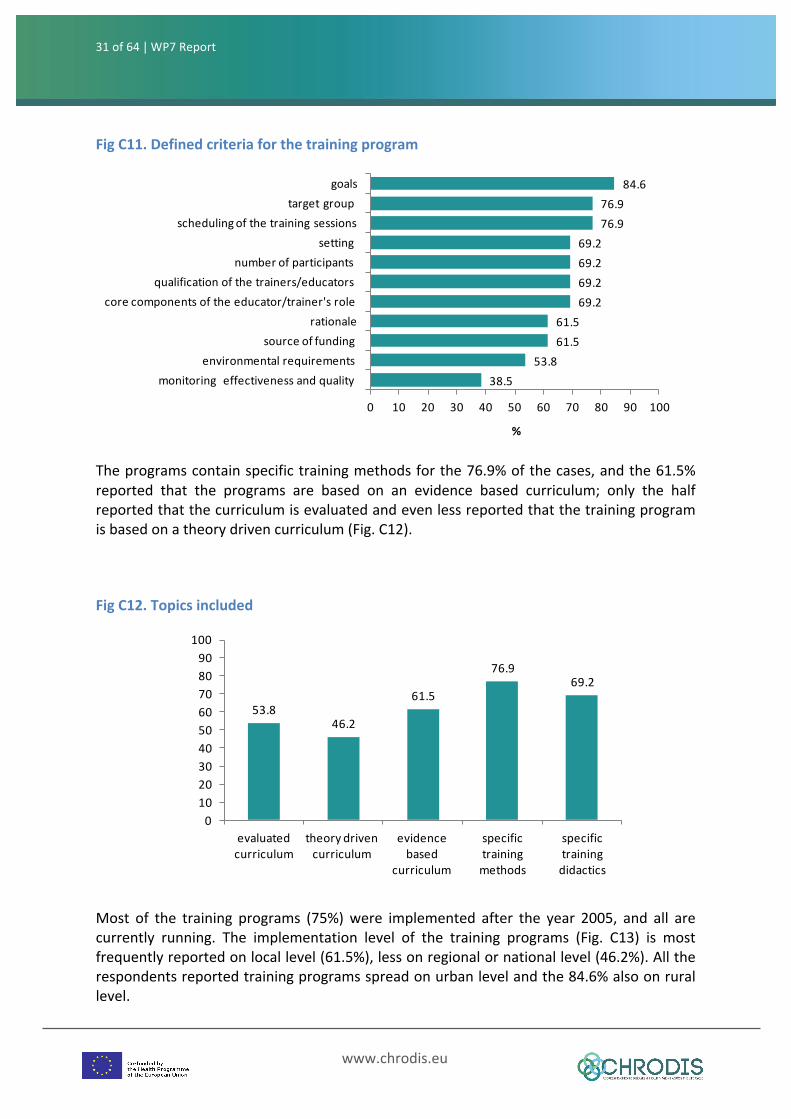
Themajorityofthedescribedtrainingprogramsdefinethegoal, thetargetgroupandthescheduling of the training sessions (Fig. C11). About 70% reported that the trainingprograms define the setting, the number of participants, the qualification of thetrainers/educators and the core components of their role. Only a few stated that amonitoringofeffectivenessandqualityisdefined(38.5%).
31of64 | WP7Report
www.chrodis.eu
38.553.8
61.561.5
69.269.269.269.2
76.976.9
84.6
0 10 20 30 40 50 60 70 80 90 100
monitoringeffectivenessandqualityenvironmentalrequirements
sourceoffundingrationale
corecomponentsoftheeducator/trainer'srolequalificationofthetrainers/educators
numberofparticipantssetting
schedulingofthetrainingsessionstargetgroup
goals
%
53.846.2
61.5
76.969.2
0102030405060708090
100
evaluatedcurriculum
theorydrivencurriculum
evidencebased
curriculum
specifictrainingmethods
specifictrainingdidactics
FigC11.Definedcriteriaforthetrainingprogram
Theprogramscontainspecifictrainingmethodsforthe76.9%ofthecases,andthe61.5%reported that the programs are based on an evidence based curriculum; only the halfreportedthatthecurriculumisevaluatedandevenlessreportedthatthetrainingprogramisbasedonatheorydrivencurriculum(Fig.C12).
FigC12.Topicsincluded
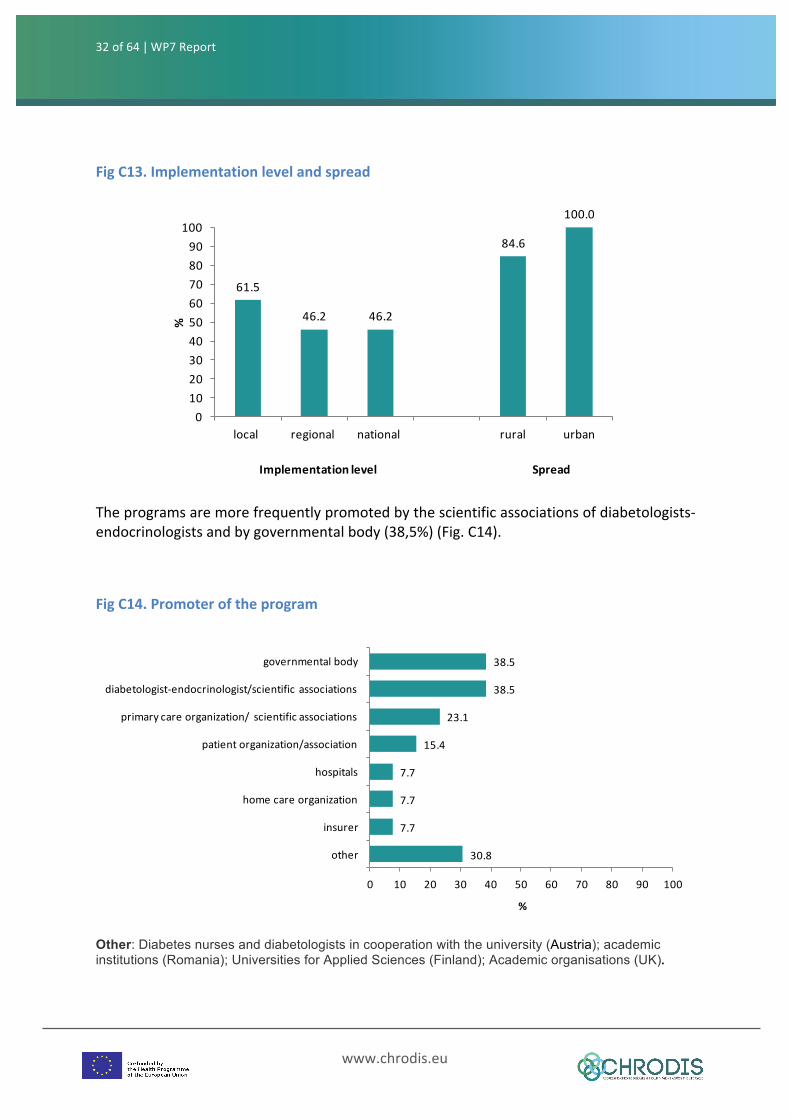
Most of the training programs (75%)were implemented after the year 2005, and all arecurrently running. The implementation level of the training programs (Fig. C13) is mostfrequentlyreportedonlocallevel(61.5%),lessonregionalornationallevel(46.2%).Alltherespondentsreportedtrainingprogramsspreadonurbanlevelandthe84.6%alsoonrurallevel.
32of64 | WP7Report
www.chrodis.eu
61.5
46.2 46.2
84.6
100.0
0102030405060708090
100
local regional national rural urban
%
Implementationlevel Spread
30.8
7.7
7.7
7.7
15.4
23.1
38.5
38.5
0 10 20 30 40 50 60 70 80 90 100
other
insurer
homecareorganization
hospitals
patientorganization/association
primarycareorganization/ scientificassociations
diabetologist-endocrinologist/scientificassociations
governmentalbody
%
FigC13.Implementationlevelandspread
Theprogramsaremorefrequentlypromotedbythescientificassociationsofdiabetologists-endocrinologistsandbygovernmentalbody(38,5%)(Fig.C14).
FigC14.Promoteroftheprogram
Other: Diabetes nurses and diabetologists in cooperation with the university (Austria); academic institutions (Romania); Universities for Applied Sciences (Finland); Academic organisations (UK).
33of64 | WP7Report
www.chrodis.eu
61.5 61.5
30.8
0102030405060708090
100
structureindicators processindicators intermediateoutcomeindicators
%
53.8
15.4
0.07.7
0.0 0.0
23.1
0102030405060708090100
statutorysystemforhealth
financing
publicinsurers
privateinsurers
co-paymentbythepatient
tradeunions
EUstructuralfunds
other
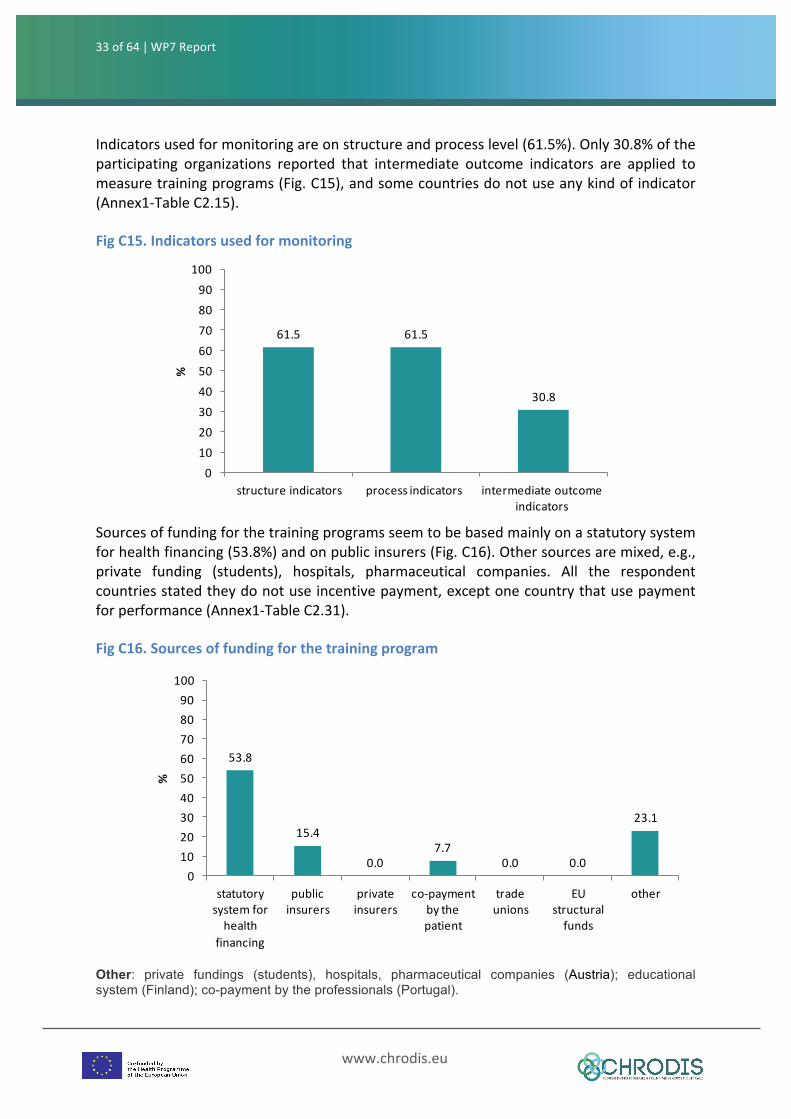
%Indicatorsusedformonitoringareonstructureandprocesslevel(61.5%).Only30.8%oftheparticipating organizations reported that intermediate outcome indicators are applied tomeasuretrainingprograms(Fig.C15),andsomecountriesdonotuseanykindofindicator(Annex1-TableC2.15).
FigC15.Indicatorsusedformonitoring
Sourcesoffundingforthetrainingprogramsseemtobebasedmainlyonastatutorysystemforhealthfinancing(53.8%)andonpublicinsurers(Fig.C16).Othersourcesaremixed,e.g.,private funding (students), hospitals, pharmaceutical companies. All the respondentcountriesstatedtheydonotuseincentivepayment,exceptonecountrythatusepaymentforperformance(Annex1-TableC2.31).
FigC16.Sourcesoffundingforthetrainingprogram
Other: private fundings (students), hospitals, pharmaceutical companies (Austria); educational system (Finland); co-payment by the professionals (Portugal).

34of64 | WP7Report
www.chrodis.eu
In summary, training programs for professionals exist in more than two/third of theparticipating countries. The core criteria of the quality of training programs seem to bedefined, e.g., the goal, the rationale, the target group, the setting, the scheduling of thetraining sessions. More than a half reported to have an evidence-based curriculum anddefinedspecifictrainingmethodsanddidactics.However,therearesomediscussionpoints.Although,themanyqualitycriteriaaredefinedintrainingprograms,onlya lownumberoftheparticipatingorganizationsreportedthatamonitoringofeffectivenessandqualityofthetrainingprogramisdefined.Lessthanahalfreported that the training program is based on a theory driven curriculum and only the30.8% reported that intermediate outcome indicators are applied to measure trainingprograms.