report on rsby-chis utilisation and beneficiary feedback study
TRANSCRIPT

1
CHIAK RSBY-CHIS UTILISATION AND BENEFICIARY FEEDBACK STUDY
Submitted to:
Comprehensive Health Insurance Agency of Kerala (CHIAK)
(A Govt. of Kerala Undertaking-Labour & Rehabilitation Dept.)
Submitted by:
Pratheesh Presannan
MBA-Rural Management,
Xavier University, Bhubaneswar
June,2015
2
ACKNOWLEDGEMENTS
With deep sense of gratitude and appreciation, I acknowledge and appreciate the
contributions of all those who contributed towards the study.
At the very outset, I would like to thank the Comprehensive Health Insurance Agency of
Kerala (CHIAK) for entrusting me with the study. I am grateful to Shri.P. Sukumar,
Executive Director, CHIAK for his support and Guidance, throughout the study period.
I am also thankful to Dr. Raju Sukumaran, Medical Officer of CHIAK, for providing me with
useful and relevant information.
I am also grateful to Mr.Vaishakhan , Manager(IT) for providing all the support .
I am indebted to the Assistant District Coordinators of Thiruvananthapuram, Kottayam ,
Alappuzha and Kozhikode for their full fledged support at the various stages of the study.
My thanks are due to the Hospital authorities, Public Relations Officers, and RSBY
personnel of the hospitals under survey, for providing me with the required information
pertaining to the various aspects of the study.
Special thanks to Mr.Arun.B.Nair of Health Systems Research India Initiative (HSRII) for his
guidance during the course of this study.
Lastly, I owe my unredeemable debt of gratitude to our respondents – the beneficiaries of the
RSBY-CHIS, without whom this study would not have been a reality.
Pratheesh Presannan
MBA-RM,XIMB-XU
MBA-Rural Management,
Xavier University, Bhubaneswar

3
Table of Contents Acknowledgements
List of Tables List of Figures
ABBREVIATIONS ............................................................................................................. 5
1. Introduction: ............................................................................................................. 6
1.1. Unique features of RSBY:..................................................................................... 6
1.2. Salient features of RSBY...................................................................................... 8
2. Rationale for Study ................................................................................................... 8
3. Research Methodology: ............................................................................................ 9
3.1. Key Objective of Study ......................................................................................... 9
3.2. Limitations of the study ...................................................................................... 11
4. Data Analysis and Interpretations ......................................................................... 11
4.1. Key Performance Matrix .................................................................................... 11
5. Beneficiary Response .............................................................................................. 16
5.1. Opinion/Satisfaction on the Experience of RSBY: ............................................ 18
6. Suggestions pertaining to beneficiaries : ............................................................... 19
6.1. Proposed Information Flow diagram ................................................................. 20
6.2. Proposed changes to existing Exit Interview ...................................................... 22
7. Conclusion .............................................................................................................. 23
REFERENCES .................................................................................................................. 24

4
List of Figures Page Number
Figure 1:Geographic locations of the 4 hospitals selected for study 8
Figure 2:Difference between families targeted vs. actual count of families
enrolled in RSBY for the year 2013-14
10
Figure 3: RSBY Enrolment Conversation percentage 10
Figure 4:Overall premium utilization chart for the year 2013-14 11
Figure 5: Gender-wise RSBY utilization in the 4 hospitals for 2014-15 11
Figure 6:Pie- Chart representation of the hospitalisation under RSBY for
Medical and Oncology procedures vs. rest of the procedures for the year
2014-15
12
Figure 7:Distribution of cost and count of admissions under medical
procedure
13
Figure 8: Total amount claimed and admissions under various packages in
Oncology
14
Figure 9:Responses from beneficiaries interviewed in percentage 15
Figure 10:Responses segregated based on type of interview conducted 15
Figure 11:Responses to the type of extra expenses incurred by the patients 16
Figure 12: Info graphics of process flow proposed for streamlining the
RSBY process in hospitals
19
List of Tables
Table 1: Summary of Amount claimed and Number of admissions in 4
Medical colleges for the period of 2014-15
7
Table 2: Summary of amount claimed and also the number of admissions
per procedure under RSBY for the year 2014-15
12

5
ABBREVIATIONS
RSBY : Rashtriya Swasthya Bima Yojana
CHIS: Comprehensive Health Insurance Scheme
CHIAK: Comprehensive Health Insurance Agency of Kerala
NGO : Non Governmental Organization
SHG : Self Help Groups
CAD: Coronary Artery Disease
COPD: Chronic Obstructive Pulmonary Disease (COPD)
CKD: Chronic Kidney Disease
BPL : Below poverty line
OPD : Out Patient Department
OT : Operation Theatre
6
RSBY-CHIS Utilisation and Beneficiary
Feedback Study
1. Introduction:
RSBY has been launched by Ministry of Labour and Employment, Government of India to
provide health insurance coverage for workers in the unorganised sector. Workers in the
unorganized sector constitute about 93 percent of the total workforce in India. One of the
major hindrances faced by these workers in the unorganized sector is the frequent
incidence of illnesses and the need for medical care and hospitalization of such workers
and their family members. Since these workers do not have any kind of social security,
they have to depend on their savings or take loans for treatment. The objective of RSBY is
to provide protection to BPL households from financial liabilities arising out of health
shocks that involve hospitalization.
1.1. Unique features of RSBY:
The RSBY scheme is not the first attempt to provide health insurance to low income
workers by the Government in India. The RSBY scheme, however, differs from these
schemes in several important ways.(Ref. Rashtriya Swasthya Bima Yojana updated on 02
May, 2014,June 2015)
Empowering the Beneficiary : RSBY provides the participating BPL household with
freedom of choice between public and private hospitals and makes him a potential client
worth attracting on account of the significant revenues that hospitals stand to earn through
the scheme.
Business Model for all Stakeholders : The scheme has been designed as a business model
for a social sector scheme with incentives built for each stakeholder. This business model
design is conducive both in terms of expansion of the scheme as well as for its long run
sustainability.
Insurers : The insurer is paid premium for each household enrolled for RSBY. Therefore,
the insurer has the motivation to enroll as many households as possible from the BPL list.
This will result in better coverage of targeted beneficiaries.
Hospitals : A hospital has the incentive to provide treatment to large number of
beneficiaries as it is paid per beneficiary treated. Even public hospitals have the incentive to
treat beneficiaries under RSBY as the money from the insurer will flow directly to the
concerned public hospital which they can use for their own purposes. Insurers, in contrast,

7
will monitor participating hospitals in order to prevent unnecessary procedures or fraud
resulting in excessive claims.
Intermediaries : The inclusion of intermediaries such as NGOs and MFIs which have a
greater stake in assisting BPL households. The intermediaries will be paid for the services
they render in reaching out to the beneficiaries.
Government : By paying only a maximum sum up to Rs. 750/- per family per year, the
Government is able to provide access to quality health care to the below poverty line
population. It will also lead to a healthy competition between public and private providers
which in turn will improve the functioning of the public health care providers.
Information Technology (IT) Intensive : Every beneficiary family is issued a biometric
enabled smart card containing their fingerprints and photographs. All the hospitals
empanelled under RSBY are IT enabled and connected to the server at the district level.
This will ensure a smooth data flow regarding service utilization periodically.
Safe and foolproof : The use of biometric enabled smart card and a key management
system makes this scheme safe and foolproof. The key management system of RSBY
ensures that the card reaches the correct beneficiary and there remains accountability in
terms of issuance of the smart card and its usage. The biometric enabled smart card ensures
that only the real beneficiary can use the smart card.
Portability : The key feature of RSBY is that a beneficiary who has been enrolled in a
particular district will be able to use his/ her smart card in any RSBY empanelled hospital
across India. This makes the scheme truly unique and beneficial to the poor families that
migrate from one place to the other. Cards can also be split for migrant workers to carry a
share of the coverage with them separately.
Cash less and Paperless transactions : A beneficiary of RSBY gets cashless benefit in
any of the empanelled hospitals. He/ she only needs to carry his/ her smart card and provide
verification through his/ her finger print. For participating providers it is a paperless scheme
as they do not need to send all the papers related to treatment to the insurer. They send
online claims to the insurer and get paid electronically.
Robust Monitoring and Evaluation : RSBY is evolving a robust monitoring and
evaluation system. An elaborate backend data management system is being put in place
which can track any transaction across India and provide periodic analytical reports. The
basic information gathered by government and reported publicly should allow for mid-
course improvements in the scheme. It may also contribute to competition during
subsequent tender processes with the insurers by disseminating the data and reports.
8
1.2. Salient features of RSBY
1.Annual hospitalization coverage of up to Rs 30,000/- for a family of five members
through health insurance companies
2. Registration fee of Rs 30/- by a family for accessing empanelled hospitals across the
country
3. Coverage is for hospitalized treatment only.
4.Transportation expenses of upto Rs 1,000/- annually (with a limit of Rs 100 per
hospitalization) are provided in cash for travelling to the hospital (deducted from the
benefit package of Rs 30,000/-)
5.All pre existing diseases are covered from Day 1 .
6. No upper age limit for enrollment into the scheme.
7. 75 % of the premium is borne by the Central Government while 25 percent is the
State’s responsibility (90 percent in case of Jammu & Kashmir as well as North Eastern
States)
8.There is a provision for the State Governments to top up the coverage amount beyond
Rs. 30,000/-
Comprehensive Health Insurance Agency of Kerala - The Nodal Agency, shortly
called CHIAK is the one constituted for the implementation of the RSBY-CHIS health
insurance schemes in Kerala. Labour and Rehabilitation Department is the nodal
department for the implementation of the scheme. The department works in collaboration
with Health & Family Welfare Department and Local Self Government Department.
The chief aims of CHIAK is to provide health insurance cover to the workers and their
families in the unorganized sector under the ‘Rashtriya Swasthya Bima Yojana’(RSBY)
announced by the Central Government and to provide health insurance cover to all
sections of the society under the ‘Comprehensive Health Insurance Scheme’ (CHIS)
announced by the State Government.
2. Rationale for Study
RSBY is one of the programs initiated by the Government that has shown a visible impact
in the life of many people. Since 2008, various studies have been undertaken to evaluate
the performance of RSBY .This study focuses on the performance of RSBY in the state of
Kerala. At present four major district public medical colleges were selected to carry out
the study to get the feedback of the end user and also to find out the major medical
procedures that is being claimed.

9
3. Research Methodology:
Details of the research methodology adopted for this study are described.
3.1. Key Objective of Study
This study was undertaken to assess the implementation process of RSBY in four of the
major public medical colleges across Kerala (Alappuzha, Thrivanthapuram, Kottayam
and Kozhikode) .
The key processes that have been focused upon are:
1. Analyse the medical conditions for which most of the hospitalization happens.
2. Extra expenditure incurred by the patients having RSBY card.
3. To identify the problems experienced by the beneficiaries with respect to RSBY
scheme.
4. To suggest appropriate measures for improving the RSBY scheme.
Target Area: Alappuzha , Kozhikode, Kottayam and Trivandrum districts of the state of
Kerala formed the target area of the study.
Table below shows the summary of Amount claimed and Number of admissions in 4 Medical
colleges for the period of 2014-15.Data shows only the cases that has been claimed so far. A
total of Rs 37,28,38,451 were claimed from these hospitals for an admission of 88,965 cases.
Table 1: Summary of Amount claimed and Number of admissions in 4
Medical colleges for the period of 2014-15
Hospitals
Amount Claimed (In
Rupees)
Number of
Patients
Medical College
Trivandrum 9,50,91,612 20,419
Medical College Kottayam 8,39,72,417 24,873
Medical College Kozhikode 15,24,56,672 33,910
Government TD Medical
College Alappuzha 4,13,17,750 9,763
Grand Total 37,28,38,451 88,965
As per the initial analysis and instruction from the RSBY- CHIAK officials, 4
district public medical colleges mentioned were selected
1. Alappuzha
2. Thiruvananthapuram
3. Kozhikode
4. Kottayam
PRIMARY DATA: The main source of data for this study is the sample survey conducted
among the hospitalized beneficiaries under the scheme.
10
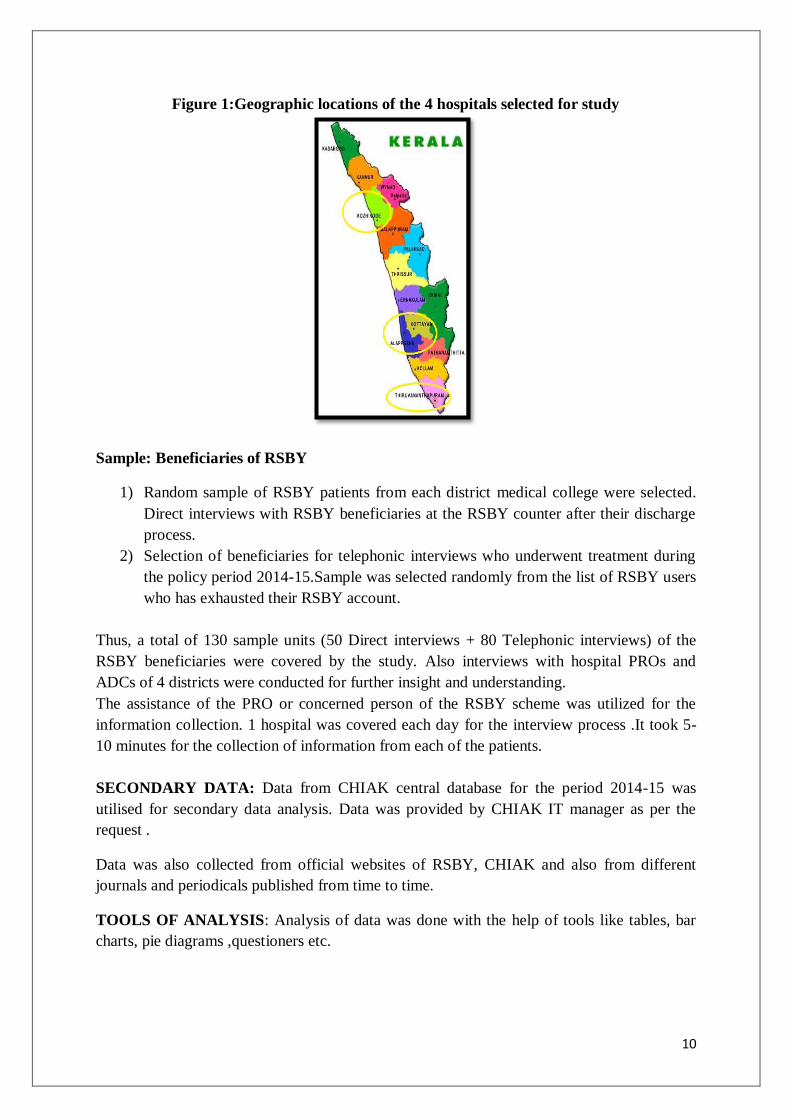
Figure 1:Geographic locations of the 4 hospitals selected for study
Sample: Beneficiaries of RSBY
1) Random sample of RSBY patients from each district medical college were selected.
Direct interviews with RSBY beneficiaries at the RSBY counter after their discharge
process.
2) Selection of beneficiaries for telephonic interviews who underwent treatment during
the policy period 2014-15.Sample was selected randomly from the list of RSBY users
who has exhausted their RSBY account.
Thus, a total of 130 sample units (50 Direct interviews + 80 Telephonic interviews) of the
RSBY beneficiaries were covered by the study. Also interviews with hospital PROs and
ADCs of 4 districts were conducted for further insight and understanding.
The assistance of the PRO or concerned person of the RSBY scheme was utilized for the
information collection. 1 hospital was covered each day for the interview process .It took 5-
10 minutes for the collection of information from each of the patients.
SECONDARY DATA: Data from CHIAK central database for the period 2014-15 was
utilised for secondary data analysis. Data was provided by CHIAK IT manager as per the
request .
Data was also collected from official websites of RSBY, CHIAK and also from different
journals and periodicals published from time to time.
TOOLS OF ANALYSIS: Analysis of data was done with the help of tools like tables, bar
charts, pie diagrams ,questioners etc.

11
3.2. Limitations of the study
An important limitation to be pointed out in telephonic interviews were non-availability of
beneficiary in the contact number provided at the time of RSBY card registration. Almost
34% of sample picked for telephonic interview had their phone disconnected or number
changed. The by standers keep changing for a patient, which restricted them from answering
to many of the queries in the schedule. Further, the respondents were indifferent to answer
because of the stress level they were in because of hospitalization .Similarly, they were
uncomfortable in criticizing the scheme or the treatment facility at the hospital fearing loss of
service.
4. Data Analysis and Interpretations
The data from the central database of CHIAK was used to analyze the general trend in the
admissions. The data gives us an idea of the utilization of the scheme, which on analyses
reveals the most common reason for hospitalization, the most conducted medical procedures
and the amount that has been claimed on this behalf.
Medical Procedures Utilized in the hospitals covered .
• DENTAL
• EAR
• ENDOCRINE
• UROLOGY
• THROAT
• PAEDIATRIC
• OTHER COMMON PROCEDURES
• ORTHOPAEDIC
• OPHTHALMOLOGY
• ONCOLOGY
• NOSE
• NEUROSURGERY
• MEDICAL
• HYSTEROSCOPIC
• GYNAECOLOGY
• GENERAL SURGERY
• ENDOSCOPIC PROCEDURES
4.1. Key Performance Matrix
As per the consolidated data available for the year 2013-14 from the RSBY site the
details of the district-wise premium utilization and the gap in BPL families enrolled
are as follows:
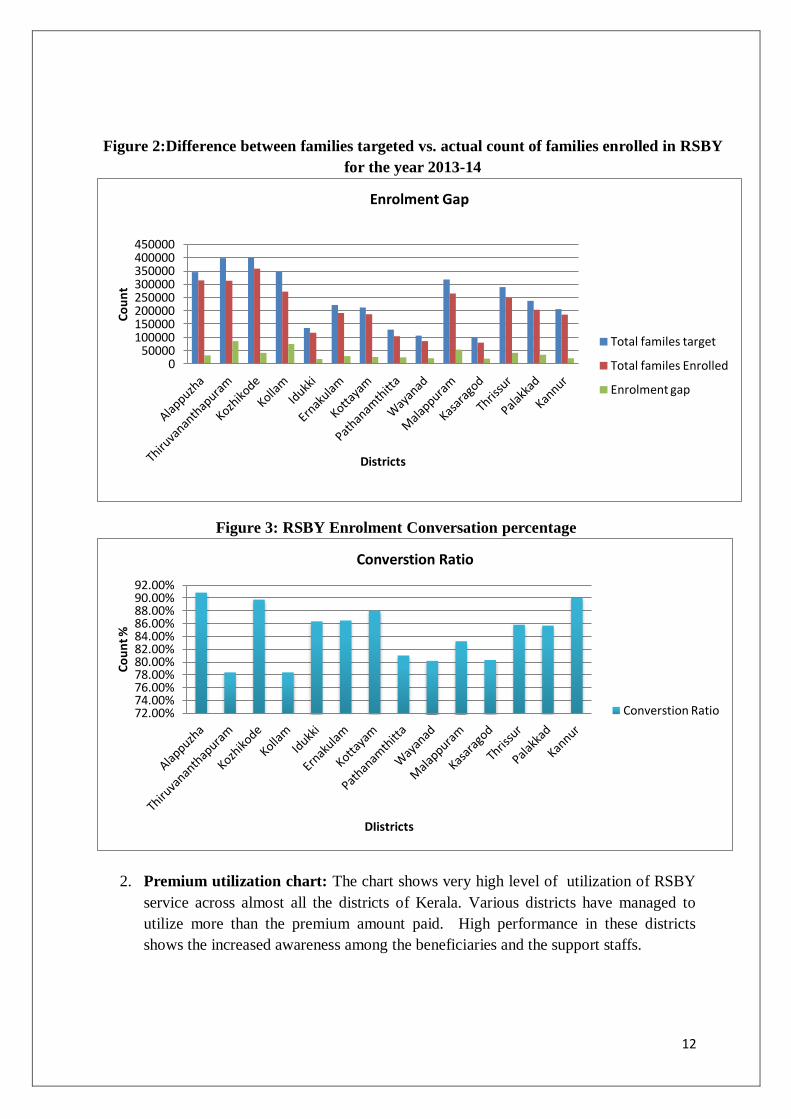
1. Enrolment GAP: The chart below shows the enrolment target achieved in each district
and also the respective conversion percentage.
12
Figure 2:Difference between families targeted vs. actual count of families enrolled in RSBY
for the year 2013-14
Figure 3: RSBY Enrolment Conversation percentage
2. Premium utilization chart: The chart shows very high level of utilization of RSBY
service across almost all the districts of Kerala. Various districts have managed to
utilize more than the premium amount paid. High performance in these districts
shows the increased awareness among the beneficiaries and the support staffs.
0 50000
100000 150000 200000 250000 300000 350000 400000 450000
Co
un
t
Districts
Enrolment Gap
Total familes target
Total familes Enrolled
Enrolment gap
72.00% 74.00% 76.00% 78.00% 80.00% 82.00% 84.00% 86.00% 88.00% 90.00% 92.00%
Co
un
t %
DIistricts
Converstion Ratio
Converstion Ratio

13
Figure 4:Overall premium utilization chart for the year 2013-14
Analysis of 2014-15 data for the 4 hospitals selected: Analysis of data made available for
the period of 2014-15 for four mentioned Medical Colleges gives us insight into major
reasons for availing treatment .It has been identified that of the total admission that took place
during the period of 2014-15, 42% were female and 58% were Male population .
Figure 5: Gender-wise RSBY utilization in the 4 hospitals for 2014-15
-1E+08
-50000000
0
50000000
100000000
150000000
200000000
250000000
300000000
350000000
Am
ou
nt
Districts
Premium Utilization Chart
Hospitalization Value (Rs.) :
Total premium paid (Rs.) :
Difference (Rs.) :
0 10000 20000 30000 40000
50000 60000
Male
Female
51420
37413
Count
Ge
nd
er
Gender Profile

14
Table 2: Summary of amount claimed and also the number of admissions per
procedure under RSBY for the year 2014-15
Figure 6:Pie- Chart representation of the hospitalisation under RSBY for Medical and
Oncology procedures vs. rest of the procedures for the year 2014-15
Of the total number of admissions in the 4 hospitals, Medical procedures account for 45.74%
and Oncology 27.66% of total admissions under RSBY. Rest all combined together comes to
26%.
46%
28%
26%
MEDICAL
ONCOLOGY
REST
Procedures Count of
Admissions Count%
Amount
Claimed
Amount
Claimed
%
MEDICAL 40,697 45.74% 12,10,08,125 32.46%
ONCOLOGY 24,604 27.66% 3,99,07,125 10.70%
OTHER COMMON ROCEDURES 6,328 7.11% 53,08,437 1.42%
GENERAL SURGERY 4,549 5.11% 4,31,54,549 11.57%
ORTHOPAEDIC 4,108 4.62% 5,21,42,800 13.99%
UROLOGY 1,808 2.03% 2,17,98,250 5.85%
Unspecified 1,570 1.76% 3,56,62,640 9.57%
GYNAECOLOGY 1,060 1.19% 89,42,925 2.40%
OPHTHALMOLOGY 872 0.98% 40,02,950 1.07%
ENDOCRINE 829 0.93% 1,21,77,250 3.27%
NEUROSURGERY 695 0.78% 1,19,10,750 3.19%
NOSE 577 0.65% 45,44,900 1.22%
EAR 507 0.57% 50,55,000 1.36%
THROAT 433 0.49% 38,90,000 1.04%
ENDOSCOPIC PROCEDURES 199 0.22% 20,85,250 0.56%
DENTAL 73 0.08% 6,23,500 0.17%
COMBINED PACKAGES 28 0.03% 3,86,500 0.10%
PAEDIATRIC 22 0.02% 1,95,500 0.05%
HYSTEROSCOPIC 6 0.01% 42,000 0.01%

15
Even though GYNAECOLOGY is one of the most utilized schemes under RSBY, 3 out of 4
hospitals selected for this study has Mother and Child department existing as an independent
hospital and data of which was not covered as part of this study.
1. Medical Procedures
The below chart analyses the data for Medical Procedures and its utilization across various
medical procedures such as Cardiac, Renal, Pulmonary and others.
Figure 7:Distribution of cost and count of admissions under medical procedure.
**Rest shows a higher number as many of the descriptions entered by the hospitals are not in standard
terms. REST might include count from COPD,CKD or CAD.
The Observations from the above data are that:
1. Under Medical procedures, around 30% of admissions are related to Coronary Artery
Disease(CAD) and the expense covered is approximately 25% of the amount claimed
under the Medical procedure.
2. Other two major reasons for admission are Chronic Kidney Disease(CKD) and
Chronic Obstructive Pulmonary Disease (COPD)with around 8% admissions for each.
3. This shows a substantial increase in lifestyle induced diseases. The Government could
initiate deeper study into the matter and increase awareness among the people.
2. ONCOLOGY
Here, the study shows the percentage use of scheme among various treatments under
Oncology.
0%
10%
20%
30%
40%
50%
60%
CAD CKD COPD Rest
Cost 27% 10% 7% 55%
Count 33% 8% 8% 51%
Medical Procedures

16
Figure 8: Total amount claimed and admissions under various packages in Oncology
Around 40% of the total amount claimed under oncology is for Radiotherapy and around
20% is for Chemotherapy. Radiotherapy per sitting costs around Rs 1,125 to Rs 1,500
,Chemotherapy per sitting costs Rs 1,000 and Chemotherapy - per sitting plus cost of
injections subject to approval for Insurance administrator costs between Rs.3,750 to Rs 5,000.
5. Beneficiary Response
The reach of the program can be rightly analyzed only by valuing the feedback from the end
user. Hence, feedback from patients were taken by conducting interviews with
patient/bystanders during discharge from hospitals. Opinions and recommendations have
been consolidated after direct interview with over 50 patients and around 80 telephonic
interview.
Main focus of the interviews were their general take on RSBY program and if they incurred
any extra expenses during hospitalisation. Interview was semi-structured approach. This
methodology was useful in getting better insight into their satisfaction. the following were the
response of the members as suggestions and difficulties faced.
7.97%
31.81%
43.46%
24.56%
19.61%
40.19%
Chemotherapy - per siting plus cost of injections subject to approval for Insurance administrator
Chemotherapy - Per sitting
Radiotherapy - Per sitting
Chemotherapy - per siting plus cost of injections subject
to approval for Insurance administrator
Chemotherapy - Per sitting Radiotherapy - Per sitting
Cost % 24.56% 19.61% 40.19%
Count% 7.97% 31.81% 43.46%
Oncology

17
Figure 9:Responses from beneficiaries interviewed in percentage
When enquired about number of patients who incurred extra expenses, were 46% of the
respondents responded that they have incurred no expense so far ,where as 28% claimed yes
and 46% didn’t respond.
Figure 10:Responses segregated based on type of interview conducted.
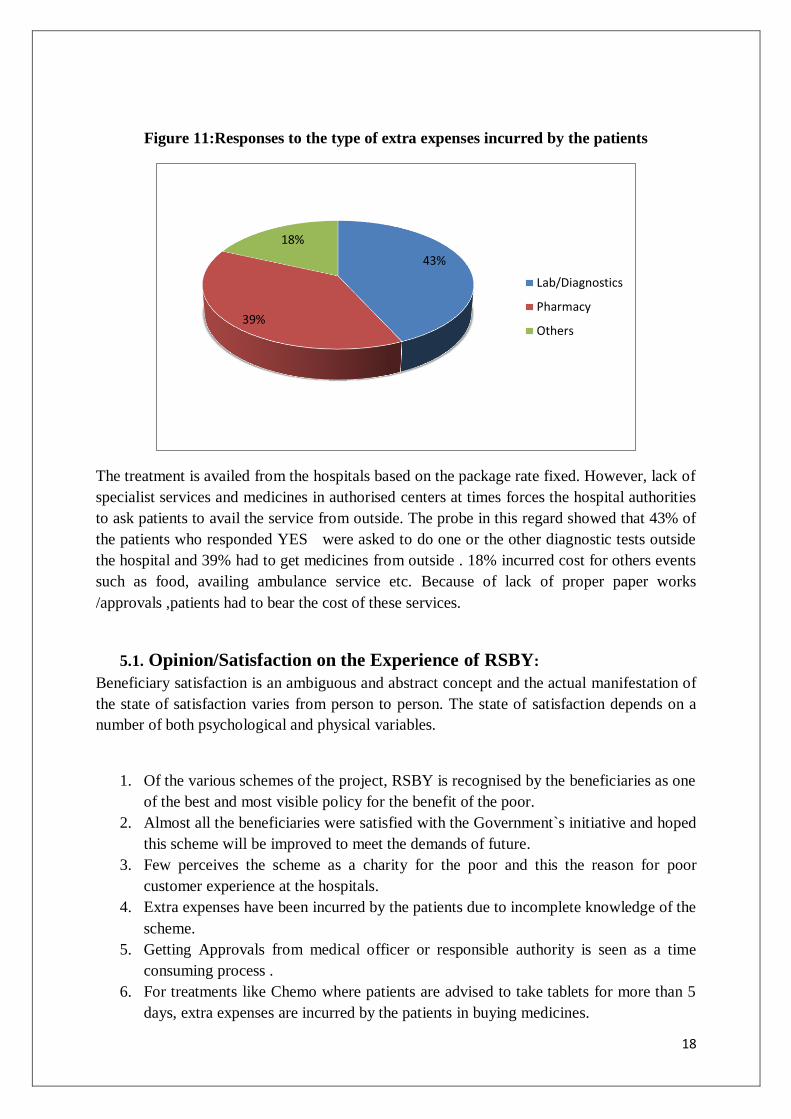
43% of the respondents responded YES incurred expense for Diagnostics and 39% at
pharmacy.18% incurred cost for others events such as food, availing ambulance service etc.
28%
46%
26%
YES NO Didn`t Respond
0
20
40
60
80
100
120
140
Telephonic Interview
Direct Interview Total Responses
Didn`t Respond 27 7 34
NO 34 26 60
YES 19 17 36
Co
un
t
18
Figure 11:Responses to the type of extra expenses incurred by the patients
The treatment is availed from the hospitals based on the package rate fixed. However, lack of
specialist services and medicines in authorised centers at times forces the hospital authorities
to ask patients to avail the service from outside. The probe in this regard showed that 43% of
the patients who responded YES were asked to do one or the other diagnostic tests outside
the hospital and 39% had to get medicines from outside . 18% incurred cost for others events
such as food, availing ambulance service etc. Because of lack of proper paper works
/approvals ,patients had to bear the cost of these services.
5.1. Opinion/Satisfaction on the Experience of RSBY:
Beneficiary satisfaction is an ambiguous and abstract concept and the actual manifestation of
the state of satisfaction varies from person to person. The state of satisfaction depends on a
number of both psychological and physical variables.
1. Of the various schemes of the project, RSBY is recognised by the beneficiaries as one
of the best and most visible policy for the benefit of the poor.
2. Almost all the beneficiaries were satisfied with the Government`s initiative and hoped
this scheme will be improved to meet the demands of future.
3. Few perceives the scheme as a charity for the poor and this the reason for poor
customer experience at the hospitals.
4. Extra expenses have been incurred by the patients due to incomplete knowledge of the
scheme.
5. Getting Approvals from medical officer or responsible authority is seen as a time
consuming process .
6. For treatments like Chemo where patients are advised to take tablets for more than 5
days, extra expenses are incurred by the patients in buying medicines.
43%
39%
18%
Lab/Diagnostics
Pharmacy
Others

19
7. The process was intended to be cashless and paperless. But patients have to go
through a substantial amount of paper works before getting the required approvals
which is in accordance with internal hospital mechanism.
8. Cost for initial lab test such as ECHO and blood tests are borne by the patients, which
is taken 10 to 15 days ahead of a surgery or process. As of now there is no provision
to cover these tests.
9. Extra expenses for supporting drugs that is needed for day treatment has to be taken
up by the patients.
10. Package cost for Plastic surgery is fixed at Rs. 22,000,but in cases which requires
only minor surgeries, entire Rs 22,000 is blocked and it leads to the deduction of the
amount from patient`s health card.
11. Few procedures such as injections for increasing the blood production ,that needs to
be done before day treatment are not covered under RSBY, which is a distress to
patients.
12. There is a major concern over the infrastructure for the support system at RSBY
counter.
13. RSBY counters are small and ill-equipped leading to delays and overcrowding.
14. Patients are not aware of the process to be followed in case of availing services from
unauthorised labs.
15. On transfer of patients from empanelled hospitals to better facility empanelled
hospitals, the cost of ambulance has to be taken up by the patient.
16. Majority of the patients who had exhausted their RSBY card were Cardiac, Renal and
cancer patients and they were covered under CHISPLUS for extra expense incurred.
Patients who exhausted CHIS-PLUS amount availed various schemes such as
Karunya , Suhurtham, Thalolam etc.
6. Suggestions pertaining to beneficiaries :
Given below are few suggestions based on the beneficiary interaction
1. Digitalisation of the entire process to minimise paper works.
2. If process of medicine procurement can be made directly between the pharmacy
and the hospital/department, load on patients can be reduced .
3. Hospital administration should take necessary steps to have display of list of
empanelled pharmacy and labs. And in case the service is not available at these
authorised centres, the procedure to be followed should be listed .
4. Point 2 & 3 are caused due to internal hospital administration problems and
hospitals should strictly follow the guidelines set under RSBY to resolve such
issues .
5. Need more awareness program about the benefits and process to be followed at
the grass route level.
6. Treat every beneficiary as a customer and set customer satisfaction as highest
priority of RSBY to expand its reach.

20
6.1. Proposed Information Flow diagram
Proposed Information Flow to minimise burden on patients/beneficiaries and for greater
transparency .The information flow diagram proposed suggests how information
technology can be used to bring down the paper works and also to minimise the manual
error in the process. Also modernisation of process will help in higher transparency and
customer satisfaction.
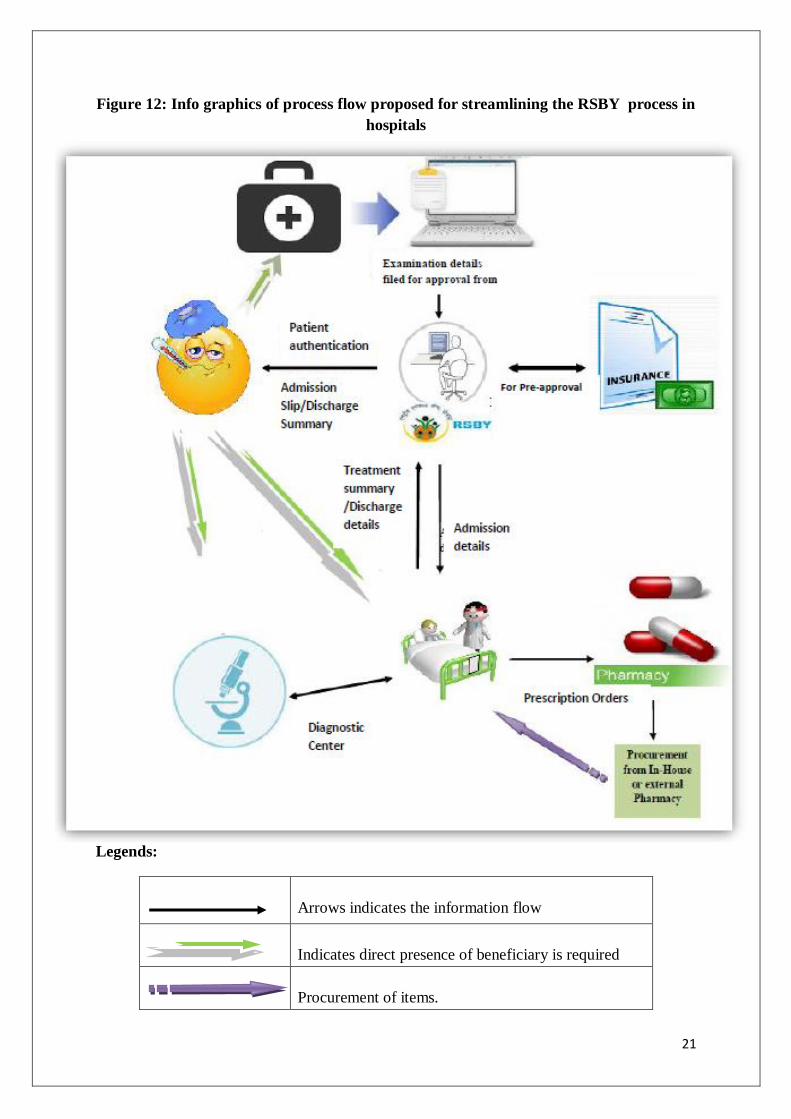
Process Flow:
When patient visits hospital at OP and if required, the doctor refers the patient for
admission. Required Treatment name and Package name under RSBY is identified and
send to RSBY counter for approval.
At RSBY counter, required approval is sought from the insurer. Patient`s finger print
authentication is taken and admission slip is given at the counter.All the required
treatment details are send to hospital ward.Patient is admitted and treatment is provided.
Required medicines are procured directly from pharmacy. All the transaction details are
send to RSBY counter for approval. Pharmacy is responsible for procurement of
medicines and other required equipments. For any diagnostics, the diagnosis details are
send to LAB directly from the ward. If pre approval is required, that can be done directly
in coordination with RSBY counter . Patient or bystanders need not go to RSBY counter
for getting approval for any medicines or diagnostics. Those formalities can be done
directly using an online portal. At the end of the treatment, patient can get discharge slip
from the RSBY counter.
Effective use of information system can reduce the overload on patient or on bystanders .
21
Figure 12: Info graphics of process flow proposed for streamlining the RSBY process in
hospitals
Legends:
Arrows indicates the information flow
Indicates direct presence of beneficiary is required
Procurement of items.
22
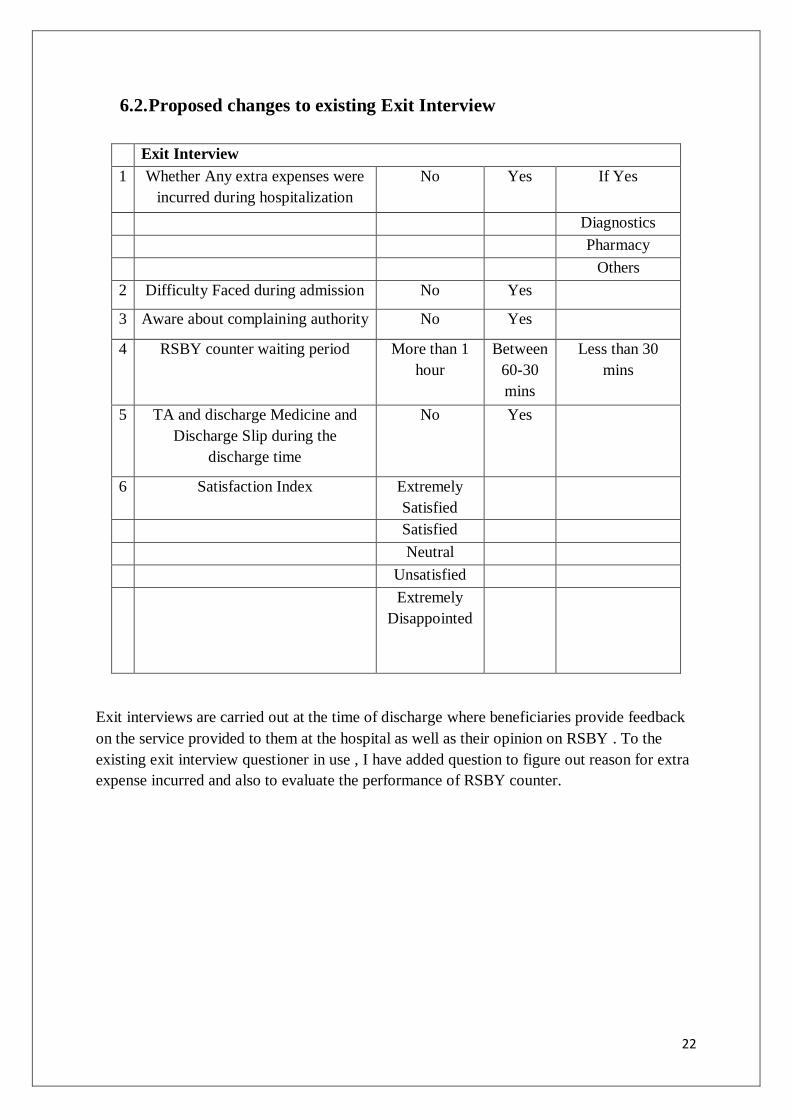
6.2. Proposed changes to existing Exit Interview
Exit Interview
1 Whether Any extra expenses were
incurred during hospitalization
No Yes If Yes
Diagnostics
Pharmacy
Others
2 Difficulty Faced during admission No Yes
3 Aware about complaining authority No Yes
4 RSBY counter waiting period More than 1
hour
Between
60-30
mins
Less than 30
mins
5 TA and discharge Medicine and
Discharge Slip during the
discharge time
No Yes
6 Satisfaction Index Extremely
Satisfied
Satisfied
Neutral
Unsatisfied
Extremely
Disappointed
Exit interviews are carried out at the time of discharge where beneficiaries provide feedback
on the service provided to them at the hospital as well as their opinion on RSBY . To the
existing exit interview questioner in use , I have added question to figure out reason for extra
expense incurred and also to evaluate the performance of RSBY counter.

23
7. Conclusion
It is thus clear from the study that majority of the beneficiaries were happy with the service
with the services provided through RSBY-CHIS. This scheme helps the poor to reduce their
hospitalization expenses . Even though RSBY-CHIS has played a major role in reducing the
hospitalization expenditure among the beneficiaries, there are a few evident problems that
needs to be addressed to make the scheme more effective and satisfactory. This scheme is
moving in right direction to attain the desired objectives of RSBY-CHIS, but the policy
makers should focus on identifying and addressing the gaps to make RSBY-CHIS more
effective and efficient , enhancing its coverage to a wide spectrum of the needy and the
deserved.

24
References
1. Rashtriya Swasthya Bima Yojana updated on 02 May, 2014,June 2015, Retrieved
from http://india.gov.in/spotlight/rashtriya-swasthya-bima-yojana.
2. http://www.rsby.gov.in/Documents.aspx?ID=14 as on June 2015
3. http://Chiak.org as on May 2015
4. Research Institue,RajagiriCollege of Social Sciences, RSBY –CHIS EVALUATION
SURVEY in Kerala ,March 2012(Sponsored by CHIAK,Dep of Labour and
Rehabilitation,Govt of Kerala).
5. Research Institue,RajagiriCollege of Social Sciences, RSBY –CHIS EVALUATION
SURVEY in Kerala ,2009(Sponsored by CHIAK,Dep of Labour and
Rehabilitation,Govt of Kerala).