report on a service delivery inspection of district
TRANSCRIPT

REPORT ON A SERVICE DELIVERY
INSPECTION OF DISTRICT HOSPITALS AND
CLINICS REGARDING AVAILABILITY OF
MEDICINES AND MEDICAL EQUIPMENT AND
THE ROLE OF HEALTH DISTRICT OFFICES
DEPARTMENT OF HEALTH:
NORTH WEST PROVINCE
MAY 2014

Page i Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
TABLE OF CONTENT
FOREWORD ........................................................................................................................................ iii
LIST OF ACRONYMS ........................................................................................................................ iv
1. INTRODUCTION .............................................................................................................. 1
2. OBJECTIVES OF THE INSPECTIONS .......................................................................... 2
3. SCOPE AND METHODOLOGY ...................................................................................... 3
3.1 Scope ................................................................................................................................. 3
3.2 Methodology ...................................................................................................................... 3
4. LIMITATIONS OF THE STUDY ...................................................................................... 4
5. KEY FINDINGS ON ANNOUNCED INSPECTIONS ...................................................... 4
5.1 Contextual background.................................................................................................... 4
5.2 Management of medicines .............................................................................................. 5
5.3 Management of medical equipment ............................................................................ 15
5.4 Governance of health facilities ..................................................................................... 18
5.5 Challenges ....................................................................................................................... 19
6 KEY FINDINGS ON UNANNOUNCED INSPECTIONS ............................................... 20
6.1 Observing facilities ......................................................................................................... 20
6.2 Access to information .................................................................................................... 26
6.3 Talking to citizens ........................................................................................................... 29
7. IMPLEMENTATION OF PSC RECOMMENDATIONS ................................................. 30
8. READINESS OF THE INSPECTED FACILITIES FOR THE ROLL OUT OF THE
NATIONAL HEALTH INSURANCE (NHI) ..................................................................... 30
9. RECOMMENDATIONS ................................................................................................... 31
9.1 ANNOUNCED INSPECTIONS ..................................................................................... 31
9.2 UNANNOUNCED INSPECTIONS ............................................................................... 32
10. CONCLUSION ................................................................................................................. 32
11. ACKNOWLEDGEMENT ................................................................................................. 32

Page ii Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
LIST OF TABLES
Table 1: Objectives of inspections ................................................................................................ 2
Table 2: Sites and dates of inspections ........................................................................................ 3
LIST OF FIGURES
Figure 1: Medicine management cycle .......................................................................................... 6
LIST OF PICTURES
Picture 1: Medicine stored in bulks at the pharmacy of Klerksdorp District Hospital .......... 9
Picture 2: Taung Station Clinic’s pharmacy shelves appeared sufficiently stocked up and
appropriately labelled ................................................................................................... 9
Picture 3: Refrigerators with medicines at Klerksdorp District Hospital ............................... 10
Picture 4: A roster displayed for cleaning of the refrigerators at Klerksdorp hospital ........ 11
Picture 5: Pharmacy of Klerksdorp District Hospital protected with burglar bars ............... 11
Picture 6: A note at Taung Station Clinic instructing personnel to regularly record and
balance stock cards ................................................................................................... 13
Picture 7: Broken equipment found at Unit 9 Clinic ................................................................ 17
Picture 8: One of unsecured broken glass doors at Unit 9 Clinic ......................................... 18
Picture 9: Cracks observed in the walls of Unit 9 Clinic ......................................................... 21
Picture 10: Damaged sanitation pipes at Unit 9 Clinic .............................................................. 22
Picture 11: A dripping water tap at Unit 9 Clinic ........................................................................ 23
Picture 12: Damaged ceiling and exposed electric wires at Unit 9 Clinic .............................. 23
Picture 13: Medical supplies and other equipment stored in the bathroom at Tlapeng ........
Clinic ............................................................................................................................. 24
Picture 14: Back-up generator stored with other items at Dryharts Clinic ............................. 25
Picture 15: Signage at Klerksdorp District Hospital................................................................... 26
Picture 16: Information about baby feeding was displayed in Setswana at Klerksdorp
District Hospital ........................................................................................................... 27
Picture 17: Costs of services clearly displayed at Brits District Hospital ............................... 27
Picture 18: Complaints Mechanism displayed at Klerksdorp District Hospital ..................... 28
Picture 19: Key information about management of Klerksdorp District Hospital .................. 29

Page iii Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
FOREWORD
South Africa’s burden of disease, consisting amongst others of a high rate of HIV/AIDS is
consistent with health challenges affecting many developing countries which are
characterized by high levels of poverty. Thus, health care is one of the key government
priorities as well as an essential service which should be accessible to all the citizens of the
country.
Key to ensuring a long and healthy life for all is having sustainable health care infrastructure
that is responsive to the needs of the citizens. In this regard, primary health care facilities
have been established to ensure that citizens receive health services at the local level.
Furthermore, the National Health Insurance (NHI) has been established to ensure equal
access to quality health care for all citizens. Amongst others, it is important that health care
facilities should at all times have sufficient medicines as well as adequate medical
equipment for timeous and quality treatment, if government is to succeed in mitigating the
burden of disease and ensuring a long and healthy life for all citizens. Furthermore, health
facilities should function in a manner that is in line with the Batho Pele principles of service
delivery.
It is against this background that the Public Service Commission (PSC) deemed it necessary
to conduct inspections to determine the availability of medicines and medical equipment.
Furthermore, the inspections sought to determine the implementation of the PSC’s previous
recommendations in this area and readiness of the health care facilities for the imminent roll-
out of the NHI. Despite supply chain management challenges relating to poor quality of
some of the procured medical equipment and delays by District Offices to attend to
maintenance thereof, medicines and medical equipment were largely available at the sites
visited. It was also found that out of 12 PSC’s recommendations, 7 (58%) were
implemented. Based on the findings and observations, it is the view of the PSC that the
visited health facilities were ready for the roll out of the NHI.
It is a pleasure to present theReport on Service Delivery Inspection of District Hospitals and
Clinics regarding Availability of Medicines and Medical Equipment and the Role of Health
District Offices in the North West. We believe that the inspections remain a valuable
monitoring mechanism whose findings could contribute towards service delivery
improvement.
The PSC wishes to thank officials of the North West Department of Health (NWDoH) for their
cooperation and willingness to share information. We trust that the findings will help the
NWDoH in its efforts to improve service delivery for a sustainable and quality health care.

Page iv Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
LIST OF ACRONYMS
AIDS Acquired Immune Deficiency Syndrome
AO Accounting Officer
ARV Antiretroviral
BP Blood Pressure
CEO Chief Executive Officer
CHC Community Health Centre
DDG Deputy Director-General
DDP District Demand Plans
DEP District Equipment Plans
DHPs District Health Plans
DHS District Health System
EA Executive Authority
EDL Essential Drugs List
EMS Emergency Medical Services
FEFO First In, First Out
GPPSA Good Pharmacy Practice in South Africa
HIV Human Immune Virus
HoD Head of Department
HPCSA Health Professional Council of South Africa
HRP Hospital Revitalization Programme
MEC Member of the Executive Council
MoA Memorandum of Agreement
NDoH National Department of Health
NDP National Development Plan
NDPSA National Drugs Policy of South Africa
NEDLC National Essential Drugs List Committee
NEMLC National Essential Medicine List Committee
NHA National Health Act
NHIS National Health Insurance System
NWDoH North West Department of Health
NW North West
NWDPW North West Department of Public Works
PHC Primary Health Care
PPPFA Preferential Procurement Policy Framework Act
PSC Public Service Commission
PTC Pharmaceutical and Therapeutic Committee
SA South Africa
SCM Supply Chain Management
SLA Service Level Agreement
SMME Small Medium Micro-sized Enterprise
SOPs Standard Operating Procedures
STG Standard Treatment Guidelines
TB Tuberculosis
UV Ultra Violet
WHO Wealth Health Organisation

Page 1 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
1. INTRODUCTION
South Africa (SA)’s burden of disease mainly consists of HIV/AIDs (i.e. Human
Immunodeficiency Virus/Acquired Immune Deficiency Syndrome), communicable diseases,
non-communicable diseases, and trauma emanating from violence and injuries with
consequent high levels of morbidity and mortality1. The impact of this burden of disease is a
shortened life expectancy. To address this burden of disease, government at its Cabinet
Lekgotla held from 20 to 22 January 2010 adopted as one of its twelve Outcomes: A long
and healthy life for all South Africans.
Health care is one of the key government priorities as well as an essential service which
should be accessible to all citizens of the country. The foregoing is predicated on a
sustainable quality health care infrastructure. However, unless sufficient medicines as well
as adequate medical equipment are available at health facilities, government will not
succeed in its key objective of ensuring a long and healthy life for South Africans.
The introduction of the National Drug Policy of South Africa (NDPSA),in line with the World
Health Organization (WHO) guidelines, by the National Department of Health (NDoH) in
1996 aimed at ensuring equal access to medicines for all South Africans. It is the aim of the
NDPSA through the Essential Drugs Programme, which includes an Essential Drugs List
(EDL) and Standard Treatment Guidelines (STG) to ensure that medicines are available at
all health facilities. It is against this background that the citizens expect health facilities to
always have medicines in sufficient quantities as well as the necessary medical equipment.
Furthermore, our constitutional imperatives dictated that government should devolve certain
responsibilities for health services to the provincial and local government 2 . As a
consequence, the District Health System (DHS) was established in terms of section 29(1) of
the National Health Act, 2003 to ensure that communities at local level have access to the
quality health care that they are entitled to3 .Accordingly, the Provincial Departments of
Health created District Health Offices to facilitate the delivery of health services by hospitals
and clinics at district level. District Offices are expected to play a critical supportive role of
ensuring that health facilities are adequately resourced at all times for the optimal provision
of quality health care to citizens.
It is against this backdrop that the Public Service Commission (PSC) deemed it necessary to
conduct service delivery inspections on availability of medicines and medical equipment at
selected health facilities, as well as to determine the role of Health District Offices in this
regard. Inspections are meant to entrench a citizen and service-centred culture, and
reinforce accountability across the Public Service. Furthermore, they provide the PSC with a
first-hand opportunity to experience what is happening at service delivery sites, and thus
strengthen the oversight work of the PSC. The inspections at the selected health facilities
1 Republic of South Africa. National Department of Health. Strategic Plan for Nurse Education, Training and Practice
2012/13 – 2016/17. 2 Republic of South Africa. National Department of Health. White Paper for the transformation of the Health
System in South Africa . 1997. 3 Republic of South Africa. National Health Act. 2003.

Page 2 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
also present an opportunity of determining their readiness for the imminent roll-out of
National Health Insurance (NHI).
Conducting inspections is in line with the Public Service Commission Act, 1997, Section 9,
which provides that “the Commission may inspect Departments and other organizational
components in the Public Service and has access to such official documents or may obtain
such information from Heads of those Departments or organizational components as may be
necessary for the performance of the functions of the Commission under the Constitution or
the Public Service Act4.”
2. OBJECTIVES OF THE INSPECTIONS
According to the PSC’s protocol on announced and unannounced inspections, the broad aim
of inspections is to assess the quality of services rendered by departments, the state of
facilities and the conditions at service delivery sites, in order to ensure adherence to
stipulated regulations and other government frameworks 5 .Table 1 below provides the
objectives of an inspection as defined in the PSC Protocol as well as those pertaining to the
inspection on the availability of medicines and medical equipment.
Table 1: Objectives of inspections
Objectives of an inspection Objectives of inspections on the availability of
medicines and medical equipment
To afford a personal opportunity to
experience the level of service delivery
first-hand and to see what kind of service
delivery challenges are facing staff.
To determine the availability/adequacy of medicines
and equipment at clinics and district hospitals.
To engender a sense of urgency and
seriousness among officials regarding
service delivery.
To establish the role of district health offices in
ensuring the availability of adequate medicines and
equipment at clinics and district hospitals.
To introduce objective mechanisms to
identify both weaknesses and strengths
towards improving service delivery.
To establish whether provincial departments of
Health have developed guidelines and procedures to
manage the selection, procurement, distribution and
use of medicines.
To report serious concerns about the
quality of service delivery and compliance
with Batho Pele requirements.
To establish whether provincial departments of
Health have developed guidelines to manage the
procurement, distribution and maintenance of
medical equipment.
To carry out investigations of serious
failures as pointed out by inspections; and
To determine the plans of the provincial departments
of Health to resolve any identified problems
experienced in relation to the procurement,
distribution and use of medicines as well as
maintenance of medical equipment.
To improve service user care relations in
order to promote a user-oriented public
service.
To establish the specific institution’s compliance with
the implementation of the Batho Pele Framework in
relation to medicines and equipment.
4 Republic of South Africa. Public Service Commission. Public Service Commission Act. 1997. 5. Republic of South Africa. Public Service Commission. Protocol on Announced and Unannounced Inspections. 2007.

Page 3 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
To determine the challenges experienced by the
district offices of health in ensuring that medicines
and equipment are available at the health institutions.
3. SCOPE AND METHODOLOGY
3.1 Scope
The inspections sought to gather first-hand information regarding availability of medicines
and medical equipment at selected hospitals and clinics. A representative sample of both
urban and rural health facilities, which included the sites previously inspected in 2009, was
targeted for inspection to determine the availability of medicines and medical equipment. In
particular, the Dr Kenneth Kaunda was selected on the basis that it has been identified for
the pilot of the NHI.
A brief discussion was held with the officials of the Provincial Head Office, Bonajala and Dr
Kenneth Kaunda district offices in order to obtain an overview of the situation in respect of
the sites visited. For a detailed list of the officials, refer to ANNEXURE A. The table below
shows the inspected sites. Although meetings were not held with district officials of the
Ngaka Modiri and Dr Segomotsi Mompati, the inspection team was assured by the provincial
Head Office that processes for the management of medicines and medical equipment were
largely similar in all districts.
Table 2: Sites and dates of inspections
Inspection Sites Sphere of Government Date of Inspection
Mmabatho Provincial Government 21 October 2013
Ngaka Modiri Molema District
Tlapeng Clinic District 21 October 2013
Unit 9 Clinic District 21 October 2913
Bojanala District
Bojanala District Office District 22 October 2013
Brits District Hospital District 22 October 2013
Dr Kenneth Kaunda District
Dr Kenneth Kaunda District Office District 28 October 2013
Klerksdorp District Hospital District 28 October 2013
Dr Segomotsi Mompati District
Taung Station Clinic District 29 October 2013
Dryhartz Clinic District 29 October 2013
3.2 Methodology
The methodology for conducting the inspections followed both the announced and
unannounced inspections as prescribed in the PSC’s protocol for conducting inspections6.
The inspections sought to understand the challenges experienced by the citizens in
accessing quality health care especially regarding the availability of medicines and medical
equipment at the sites visited and the role of the health district offices in this regard.
6 Republic of South Africa. Public Service Commission. Protocol on Announced and Unannounced Inspections. 2007.

Page 4 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
To initiate the inspection process, letters were forwarded to the Executive Authorities (EAs)
and the Accounting Officers (AOs) of the National and Provincial Departments of Health,
informing them about the PSC’s intention to conduct inspections in the selected hospitals
and clinics.
4. LIMITATIONS OF THE STUDY
The inspections were conducted at selected district offices and health facilities and as such
the findings relate to views and observations made at the said sites. The following limitations
were identified:
The PSC inspection team comprised members who are not experts in the medical
field and relied on the officials of the department to identify the medicines and
medical equipment at the visited sites. It should, however, be mentioned that the
officials appreciated the importance of honesty in this regard as the availability of
these resources will enable them to function optimally.
The inspections did not evaluate the implementation of NHI. However, critical issues
to NHI such as the availability of medicines and medical equipment were inspected to
determine its readiness for roll-out.
5. KEY FINDINGS ONANNOUNCED INSPECTIONS
The findings of the announced inspections are presented into key thematic areas, which are
the management of medicines and the management of medical equipment. It was found that
processes relating to procurement of medicines and medical equipment differ. Detailed
findings of these inspections are attached as ANNEXURE B.
5.1 Contextual background
The inspection team held a meeting with the Deputy Director-General (DDG) for Health
Service in the North West Department of Health (NWDoH) on 21 October 2013. The purpose
of the meeting was to obtain an overview of the province’s District Health System (DHS) as
well as information regarding policies relating to the Primary Health Care (PHC) services,
with specific focus on the distribution of medicines and management of medical equipment.
It emerged during discussions that all pharmaceutical supplies in the province were procured
through national tenders. These were then distributed by the appointed suppliers to the
provincial Medical Depot in Mafikeng and the sub-depot situated in the Tlhabane Sub-District
of the Bojanala District. The inspection team was informed that Bojanala was densely
populated due to labour migration arising from mining development in the area. A
Memorandum of Agreement (MoA) has been entered into between the provincial Medical
Depot and Tlhabane Sub-District, which guides the relationship and operations of these
depots. In terms of the MoA, all health facilities in and around the Tlhabane Sub-District
were serviced by the Tlhabane sub-depot to facilitate the efficient distribution of medicines to
the facilities given their remote locations from the Mafikeng provincial depot.

Page 5 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Furthermore, it emerged that District Offices must develop District Health Plans (DHPs) as
required by section 33(1) of the National Health Act, 2003 (NHA). The inspection team was
provided with the DHP for Bojanala District, which included a situational analysis on the
burden of disease as well as mitigating strategies, in line with the NHA. The DHP for Dr
Kenneth Kaunda District was not produced during the inspections. According to the
Provincial Office, orders for medicines from clinics and district hospitals were consolidated
by District Offices and submitted to the respective depots. The medical depots distribute the
ordered medical supplies weekly to the district hospitals and the latter in turn distribute the
clinics’ orders bi-weekly. It was also noted that during the 2012/13 financial year the NWDoH
had achieved the national target of95%regarding availability of essential medicines,
including the distribution of anti-retroviral drugs (ARVs), at all health facilities in the province.
It was also indicated that the province was on track to maintaining the success rate during
the 2013/14financial year based on its performance of 87.5%by the second quarter.
However, the Provincial Office’s main concern was the lack of regular maintenance of
buildings of health facilities in all the districts. With regard to medical equipment, it emerged
that District Offices submitted annual demand plans for medical equipment items costing
more than R500 000to the Provincial Office, whilst items below the aforesaid threshold were
procured at district and hospital level in line with District Equipment Plans.
Meetings with officials of the Bojanala and Dr Kenneth Kaunda District Offices took place on
22 and 28 October 2013, respectively. It was established at Bojanala District Office that
there were no posts of nursing assistants on its organisational structure. Officials also
indicated that there was a need for additional posts of pharmacy assistants. Furthermore, it
was noted that the district’s human resource plan needed to be revised to align it with the
current population demographics, since the health facilities were unable to meet the
increased demand for health services.
The Handbook for Clinic and Community Health Centre (CHC) Managers7 determines that
supervisors should visit these facilities monthly to ensure effective and efficient service
delivery. District officials indicated that they provide support to health care facilities falling
within their control. It was indicated that District Pharmacists in the respective Districts,
together with hospital pharmacists, play a crucial role in consolidating orders for the districts.
The inspection team found the role of the District Pharmacists to be evidence of the support
the District Offices provide to health facilities in ensuring sustainable quality healthcare to the
public and was in line with the Handbook. Despite human resource capacity challenges,
District officials were confident that the health facilities were ready for the roll-out of the NHI.
The selected health care facilities within these districts were visited to determine the
availability of medicines, medical equipment and the maintenance thereof as well as the
support received from the District Offices.
5.2 Management of medicines
The inspection team visited the selected health care facilities within the District Offices to
determine the availability of medicines as well as the support received from the districts.
7 Republic of South Africa. Department of Health. Handbook for Clinic/Community Health Centres Managers. October
1999.

Page 6 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Scrutiny of the NDPSA indicates that the management of medicines essentially involves five
key functions namely, selection, procurement, management support, distribution, and use.
The availability of medicines at health café facilities is reliant on this process. Therefore,
such is critical in ensuring that medicines reach the patients as and when needed. The
diagram below maps the critical steps of effective and efficient medicine management.(It
should be noted that for the purpose of this report, by medicines, reference is also made to
all pharmaceuticals, medical consumables and medical stationery).In this regard, the
findings on the management of medicines are structured according to this integrated
process.
Figure 1: Medicine management cycle
5.2.1 Product selection
National essential drug lists, together with standard treatment guidelines, serve as the basis
for formal education and in-service training for health professionals and for education about
medication use for the public8. According to the NDPSA, the National Essential Medicines
List Committee (NEMLC) or National Essential Drugs List Committee (NEDLC), appointed
by the Minister of Health, is responsible for the selection and revision of a national list of
essential medicines for three levels of care, i.e. PHC, secondary and tertiary hospitals.The
NEMLC/NEDLC is composed of experts in all spheres of medical and pharmaceutical
practice. As indicated in paragraph 5.1, the selection of medicines is a national competence
and the process is facilitated by the NDoH. Officials informed the inspection team that the
Pharmaceutical and Therapeutic Committees (PTCs) were in place, and were chaired by
pharmacists. It was indicated that the PTCs met regularly to conduct situational analyses on
prevalent diseases with a view to making recommendations on any new medicines for
8. United States of America. The Role of Essential Medicine Lists in Reproductive Health. Volume 36.Jane Hutchings et al.
December 2010.
Product
selection
Rational use,
monitoring and
evaluation
Distribution
and storage
Procurement
Management support:
Information system
Organisation/staffing
Budgeting
Training

Page 7 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
inclusion in the EDL. In addition, the PTCs assess the availability of medicines within their
districts. It was also observed that the PTCs’ specific recommendations relating to the
handling of adverse drug cases were being monitored for implementation by the health
facilities. The PSC found that product selection is well institutionalized and contributes
effectively toward the availability of medicines at health care facilities.
5.2.2 Procurement
The inspection team found that the medical depots were the primary providers of medicines
to the inspected facilities. The signed MoA provided for a routine schedule for ordering of
medicines from the medical depots. It was established at the visited health facilities that
district hospitals order their stock weekly from the depots, whilst clinics order bi-weekly from
their respective District Hospitals.The staff at Tlapeng Clinic informed the inspection team
that the clinic mostly handled cases of diarrhea, chronic hypertension and HIV. Thus, the
clinic ensured that medicines for treatment of these conditions were always available. They
also commended the support they received from the District Offices in ensuring sustainable
service delivery. In instances where patients required special drugs that were not in the
relevant EDL, the visiting doctors would prescribe such medicines, and the patients would be
referred to the district hospital for dispensing of the relevant medicine. It also emerged that
clinics were able to “borrow” out-of-stock medicines from other clinics, and return the
borrowed medicine as soon as their stock was delivered.
The inspection team was also informed that in addition to ordering from the medical depots
through the district offices, District hospitals may use a “buy-out” method. The “buy-out”
method means the hospitals order directly from the suppliers or pharmaceutical companies
on a quotation basis. However, the “buy-out” method was only allowed in the case when the
required medicine was out of stock at the medical depot and the items were urgently
needed. Although District officials found the process to be cumbersome and costly, district
hospitals confirmed that they took advantage of the method when necessary to obtain
medicines. The PSC found this level of flexibility to allow for efficient acquisition of urgently
needed medicines at the health facilities, and thereby ensuring stock availability.
5.2.3 Distribution and storage
The NDPSA aims to ensure the prompt, efficient, timely and equitable distribution of
essential drugs and medical supplies to all institutions. In this regard, provincial departments
are required to develop own standard operating procedures (SOPs) for the distribution
arrangements and storage of medical supplies. The SOPs were found to be in place to
ensure control of access into the facilities’ pharmacies, safety and appropriate labelling of
medicines and medical consumables.
Distribution: In line with the NDPSA, the MoA provided for scheduled deliveries of ordered
stock to district hospitals by the medical depots. In this regard, the medical depots delivered
stock to district hospitals every Tuesdays of the following week from the date of receipt of
orders. District hospitals also undertook to deliver requisitions from clinics on a bi-weekly
basis from the date of receipt of orders. In addition, the MoA requires the depots to ensure

Page 8 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
that emergency orders were ready for collection or distribution by the facilities within four
hours from receipt of such orders, provided the orders were placed before 10h00. The
Department has also contracted a service provider for the transportation of medicines to all
the clinics in the province. Although District officials appeared satisfied with the service by
the service provider, this was not the case at the visited clinics. The nursing staff at the
visited clinics raised concerns that they were forced to use their own vehicles to collect
emergency orders due to the service provider not always being available. While the selfless
efforts of the nursing staff were commendable, the practice cannot be encouraged as it may
result in low morale amongst staff. Furthermore, delays in transporting medicines to facilities
impacted negatively on service delivery, which may have serious consequences. It is the
view of the PSC that the specific provision of the MoA was not adhered to in this regard, and
it was also not in keeping with the NDPSA.
Storage: In terms of the NDPSA measures should be in place for the proper storage and
safeguarding of drugs and medical supplies to ensure the maintenance of quality and
security from the time of receipt into stock up to the time of issue to the patient. In addition,
the Good Pharmacy Practice in South Africa, Fourth Edition, 2010 (GPPSA) sets out the
minimum standards for procurement, storage and distribution of medicines9. The GPPSA
was developed in line with the scope of practice of the pharmacy profession as prescribed in
terms of Section 35A of the Pharmacy Act, 1974 (Act 53 of 1974). Furthermore, pharmacists
must take all reasonable steps to ensure that working conditions are so arranged as to
protect the safety of the public and people working in the pharmacies. The inspection team
was informed that the district hospitals order medicines from depots in bulk quantities, which
are stored at the pharmacies in hospitals. It was observed that the Klerksdorp District
Hospital had sufficient storage space, and boxes of medicines neatly packed. The storage
allowed for easier movement between shelves, including easier evacuation of staff in case of
emergency, which complied with the GPPSA and Occupational Health and Safety
regulations. In addition, the storage was in keeping with the NDPSA. However, the inspected
building at the Brits District Hospital appeared old with very little storage space. The
inspection team was informed that the hospital was in the process of moving to a newly built
facility.
9 Republic of South Africa. South African Pharmacy Council. Good Pharmacy Practice in South Africa, Fourth
Edition, 2010.

Page 9 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Picture 1: Medicine stored in bulks at the pharmacy of Klerksdorp District Hospital
The pharmacies of the visited facilities appeared sufficiently stocked up and the interior
appeared clean with medicines appropriately packed and labelled on the shelves for easier
access by staff in line with the NDPSA and GPPSA.
Picture 2: Taung Station Clinic’s pharmacy shelves appeared sufficiently stocked up and appropriately
labelled

Page 10 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
It was observed that air-conditioning systems were installed and were in good working
condition to maintain the quality of medicines, as well as ensuring that working conditions
were conducive for officials working in the pharmacies. Medicines requiring constant cool
temperature such as vaccines and insulin were stored in refrigerators with thermometers to
regulate the required temperature. Most of the visited sites had sufficient refrigerators and
their temperatures were monitored on a daily basis. However, the inspection team observed
at Tlapeng Clinic that one of its refrigerators was not used despite being new. Officials
indicated that the refrigerator had an electrical fault as it was tripping up power whenever
they connected it.
Picture 3: Refrigerators with medicines at Klerksdorp District Hospital
At Klerksdorp District Hospital an updated roster was displayed for the cleaning of the
refrigerators in order to maintain the quality of medicines. This is a good practice, which was
in line with the NDPSA and GPPSA.

Page 11 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Picture 4: A roster displayed for cleaning of the refrigerators at Klerksdorp hospital
The SOPs also provided for safeguarding measures such as locking facilities to control
access to the pharmacies. In all the visited sites, the pharmacies were adequately secured
with burglar bars and entrance was restricted to authorized personnel as required by the
SOPs. It is also the view of the PSC that the facilities complied with the applicable provisions
of the GPPSA.
Picture 5: Pharmacy of Klerksdorp District Hospital protected with burglar bars

Page 12 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
5.2.4 Rational use, monitoring and evaluation
Rational use: The NDPSA recognizes the key educational role of pharmacists in instructing
patients in the correct use of medicines and to provide preventive health services. It was
found that the NWDoH developed guidelines for district pharmacists who should oversee the
operations of health facilities as well as provide pharmaceutical support to ensure that the
nursing staff adheres to the STGs. Accordingly, clinics must be visited monthly by the
supervisor and written record of the supervisor’s visit should be left with the clinic. Scrutiny of
the attendance registers of the inspected clinics showed that only district officials in the
areas of maintenance, data and asset verification regularly visited the sites. Officials at
Bojanala District Office indicated that the district had a shortage of pharmaceutical staff. As a
result, monthly visits to clinics were not always conducted. However, they informed the
inspection team that District Pharmacists regularly conducted training for Pharmacy
Assistants and Nursing Sisters. The inspection team observed that all the visited health
facilities were provided with copies of the STGs to guide them during dispensing of
medicines. It is the view of the PSC that visits to health facilities by district pharmaceutical
officials provide an opportunity for observing whether health facilities adhered to correct
dispensing practices since errors may have serious health consequences.
Monitoring and evaluation: As required by the NDPSA, District Offices should manage the
availability and safe use of medicines at health facilities. Although officials informed the
inspection team that they provided support to the visited health facilities, they conceded that
regular visits to clinics by District pharmacists were not always conducted due staff shortage
as indicated in 5.2.4.During interaction with staff at the visited facilities it emerged that most
medicines listed in the EDL were available. They informed the inspection team that for
purposes of recording and monitoring pharmaceutical stock levels, hospitals utilise the RX
solution system (i.e. automated medicine management system), whilst the clinics use stock
cards. Scrutiny of the District Health Plan (DHP) for Bojanala District showed that the district
did not have shortage of ARVs and tuberculosis (TB) drugs. The inspection team was not
provided with the DHP for Dr Kenneth Kaunda District. However, officials at Tlapeng and
Dryharts clinics informed the inspection that the clinics had shortage of Ferrous Sulphate
(i.e. treatment for iron deficiency in pregnant mothers), anti-psychotic drugs as well as
surgical supplies. According to the staff, the shortage was as a result of the stock taking
process since health facilities could only place orders once this process was finalised. It was
noted, however, that Taung Station and Unit 9 clinics did not have a similar challenge. The
staff indicated that the District Hospitals issued circulars long before the commencement of
stock taking and thus, they were able to make provision in this regard. The foregoing points
to proper planning by staff at Taung Station and Unit 9 clinics, which officials at Tlapeng and
Dryharts clinics should emulate. It is also the view of the PSC that the challenge at Tlapeng
and Dryharts clinics is due to the inconsistent support by District Offices.

Page 13 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Picture 6: A note at Taung Station Clinic instructing personnel to regularly record and balance stock
cards
The inspection team was informed that there were no expired stocks in pharmacies at all the
inspected health facilities. It was indicated that the stock was regularly checked using the
“first expired, first out” (FEFO) principle. As a result, medicines nearing expiry date were
identified approximately three months before expiry date. These were then either taken to
other sites that may use them before the expiry date or were returned to the District
hospitals’ main dispensaries for incineration. According to staff, the process ensured that
there were no adverse drug events. The inspection team was provided with a copy of the
Department’s policy regarding the adverse drug management. The rationale of the policy is
that the Department should look for ways in which its health care system can be improved,
and managerial and staff behavioural choices adapted, so that the likelihood of a recurrence
of the same adverse/medical error was significantly reduced10. It was found that provincial,
district and hospital PTCs have been established, which review pharmaceutical dosage and
safety of use issues. Scrutiny of the Brits District Hospital minutes dated 1 October 2013
showed that issues discussed in the PTC meetings included medication that should be
discontinued. It was also indicated that the PTCs recommendations relating to the handling
of adverse drug events were being implemented. The foregoing indicated that PTCs were
fully operational and contributed to the safety of medicines and impactful health care.
10Republic of South Africa. North West Provincial Department of Health. Department of Health Adverse Management Policy. 2013

Page 14 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
5.2.5 Management support
On-going support in terms management systems and processes is crucial for the effective
functioning of facilities.
Information technology system: According to the NDPSA computerized inventory control
systems should be established in all hospital pharmacies and clinics, and be linked to
computerized inventory control systems in the medical supply depots. The objective is to
ensure the prompt, efficient, timely and equitable distribution of essential drugs and medical
supplies to all health care institutions11.The inspection team observed that the RX solution
system (i.e automated medicine management system) was only installed at hospitals, whilst
the clinics were still using the manual system of stock cards to record information as well as
monitor stock levels. The inspection team was provided with a report on stock availability in
the Bojanala District12. According to the report information on the inventory management
systems at all hospitals in the district did not match items on the shelf. Furthermore, the
report mentioned that not all the necessary information was recorded on the stock cards.
This suggests weaknesses in the information management systems of the District. It also
raises questions of overstatement of stock availability in its health facilities, and thus
providing misleading information regarding the achievement of the 95% national target by
the NWDoH.
Training: Training plays a central role in ensuring that employees were knowledgeable
about what was expected of them and also to keep them abreast of new developments in
order to provide quality services. The inspection team was informed that all nurses
dispensing medicines were required to complete a dispensing course and were also
registered with the Health Professional Council of South Africa (HPCSA). It was observed at
the time of the inspection team that a similar training was provided to the nursing staff on 27
June 2013. In addition, all officials had received training on the Batho Pele principles in order
to ensure that they prioritised the needs of the citizens.
Staffing: It was noted that there was in general a shortage of medical professionals with
rural areas being worst affected. Staff atUnit 9 Clinic informed the inspection team that the
clinic provided a 24 hour service and approximately 300 patients visited the clinic per day.
The staff raised concern that citizens from areas such as Tlapeng, Mokgosane and Lokaleng
villages were visiting the clinic despite having similar facilities in their areas. The foregoing
was mainly attributed to the fact that the Unit 9 Clinic opened 24 hours per day and thus,
offered uninterrupted services. As a result, staff members were sometimes forced to leave
patients unattended during tea and lunch breaks as they did not anyone to relieve them.
Scrutiny of the post establishment of the clinic showed that the clinic had 16 professional
nurses, of which four performed night duty. Overall, the clinic’s day shift consisted of five
professional nurses, which resulted in one nurse attending to approximately 60 patients and
thus, far exceeding the national norm of 1:40 patient to nurse ratio.
11 Republic of South Africa. Department of Health. National Drug Policy of South Africa. 1996. 12 Republic of South Africa. Department of Health: North West. Stock Availability Report in Bojanala District.
2013

Page 15 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
At Tlapeng Clinic it was indicated that there was only one nursing sister, and when she was
on annual or sick leave the clinic would request the assistance of a nursing sister from
Ramatlabama village, which was approximately 30 kilometres away. The inspection team
also noted that Klerksdorp hospital had a shortage of nursing staff. Officials were concerned
that the shortage of staff impacted negatively on service delivery. It is the view of the PSC
that staff shortages often result in employees being overworked and thus leading to low staff
morale, which may impact negatively on the quality of service.
5.3 Management of medical equipment
Availability of sufficient medical equipment at health facilities is integral to providing quality
health care.Generally, medical equipment or instruments help the medical personnel to
diagnose and/or monitor specific medical conditions as well as to sustain the lives of
patients. As a result, availability of these in good quality is crucial especially in emergency
situations such as when should be put on a life support machine to keep the patient’s heart
beating and to supports his or her weak lungs while awaiting recuperation.
Procurement: According to the provincial Head Office, medical equipment items of a total
value exceeding R500000 were procured at provincial level, whilst items not exceeding the
aforesaid threshold were procured at district and hospital level in line with District Equipment
Plans. According to officials, the processes were undertaken in terms of the Preferential
Procurement Policy Framework Act, 2000 (PPPFA)13. During interaction with senior officials
of the visited the District Offices it emerged that procurement of bulky medical equipment
exceeding the R500 000 threshold was the responsibility of the Provincial Head Office. In
this regard, all health facilities submitted their annual needs to the relevant District Offices at
the beginning of the new financial year for consolidation into District Demand Plans
(DDPs).The District Offices were accordingly expected to make budget provisions based on
the DDPs and forward the plans to the Head of Department (HoD) for approval. Once the
plans were approved and the budget allocated, the purchasing of equipment was dealt with
in terms of the applicable Supply Chain Management (SCM) procedures. However, both
districts raised concerns about the poor quality of the equipment such as blood pressure
(BP) machines being procured for the facilities, which required frequent repairs or
replacement. According to officials, this resulted in poor service delivery as the equipment
often provided incorrect readings. They attributed the poor quality of equipment to the
Supply Chain Management (SCM) process of selecting the cheapest quotations. Officials
suggested that the NWDoH should consider a provincial contract that would provide for
direct procurement from carefully selected and reputable suppliers, to mitigate the risk of
procuring poor quality equipment. The PSC found the Department’s procurement processes
to be in line with the PPPFA. However, it is the view of the PSC that concerns of poor quality
equipment point to weaknesses in the SCM process at District or hospital levels, whose
procurement specifications should be strengthened with input from medical professionals
who have expert knowledge on medical equipment.
13 Republic of South Africa. National Treasury. Preferential Procurement Policy Framework Act, 2000 (PPPFA).

Page 16 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
During interaction with staff at Unit 9 Clinic, they raised concerns of insufficient medical
equipment such as Blood Pressure (BP) machines. In addition, they were concerned about
the quality of the electronic BP machines. According to staff the machines could not handle
the high number of patients visiting the clinic since they frequently stopped working or
provided incorrect readings. It was mentioned that sometimes the nursing staff have to stop
working to allow the equipment to cool down, which resulted in longer waiting times. The
inspection team found that only one blood pressure machine was working at Taung Station
Clinic. At Brits Hospital officials mentioned that the radiology equipment was old and
regularly required repairs.
Asset control: Medical equipment involves the use of state funds and must be safeguarded
to ensure accountability. As a result, section 38(1) of the Public Finance Management Act,
1999, as amended (PFMA) 14 requires the Accounting Officer to ensure the effective
management, including safeguarding, and maintenance of public assets. Accordingly,
Treasury Regulation 10.1.1(a) requires the AO to take full responsibility and ensure that
proper systems exist for assets and that preventative mechanisms were in place to eliminate
theft, losses, wastage and misuse of assets15. At all facilities visited, the inspection team was
informed that supply chain officials from District Offices record all procured equipment on the
asset register; which is updated on a monthly basis. It is the view of the PSC that the asset
control process has been sufficiently devolved to the District Offices, and was in line with the
PFMA.
Maintenance of equipment: In line withsection 38(1) of the PFMA, the applicable asset
management framework requires regular inspection and maintenance of assets, as well as
identification of obsolete for disposal purposes.The inspection team was not provided with
guidelines for the maintenance of equipment. It was established at all the inspected facilities
that medical technologists or technicians stationed at district hospitals were responsible for
the maintenance of medical equipment in accordance with the equipment specification.
These technicians regularly conducted visits to clinics to identify items requiring repairs or
disposal. In addition, it was noted that most large items included maintenance plans
providing for when these were due for service by the suppliers in line with the signed service
level agreements (SLAs).
Officials at Klerksdorp hospital informed the inspection team that the turnaround time for
repairing equipment was too long. At Unit 9 and Dryharts clinics, officials complained that
lack of maintenance of equipment resulted in the clinics being without key equipment for
considerable periods. The inspection team observed that the installed ultra violet (UV) lights
at Unit 9 Clinic for the purpose of quarantining microorganisms that cause tuberculosis (TB)
were not working. This posed a serious health challenge to other patients as they could
contract the germs emitted through coughing by the TB infected patients.
Disposal of medical equipment: Officials at the visited facilities indicated that the disposal
of assets, including medical equipment, was handled by the District Office. The inspection
14 Republic of South Africa. National Treasury. Public Finance Management Act, 1999, as amended (PFMA). 15 Republic of South Africa. National Treasury. Public Finance Management Act, 1999, as amended (PFMA). Treasury
Regulations, 1999.

Page 17 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
team observed that old and broken equipment was left lying around in the Unit 9 Clinic’s
grounds. Officials at the clinic raised concern that despite the necessary documentation
being long forwarded to the District Office, they had not received feedback. Of concern to the
inspection team was that these items could be stolen or further damaged before being their
condition was assessed, and thus result in unnecessary financial loss to the State. The PSC
found this to be a violation of the PFMA.
Picture 7: Broken equipment found at Unit 9 Clinic
Furthermore, among these items were unsecured broken glass doors, which posed a
serious danger to children accompanying parents to the clinic. The neglected items were
also in contravention of the relevant health and safety regulations.

Page 18 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Picture 8: One of unsecured broken glass doors at Unit 9 Clinic
5.4 Governance of health facilities
Public funds are used to provide public services. As a result, citizens as taxpayers have the
right to a responsive public service as well as value for money in how these scarce financial
resources are spent in the delivery of services. It is for this reason that those charged with
the responsibility to provide such services are held to account. Consequently, section
41(6)(a) of the NHA requires of the relevant Member of the Executive Council (MEC) to
appoint a representative board for each public health establishment classified as a hospital
and to prescribe its functions and procedures for meetings. In terms of section 42(1) of the
NHA, provincial legislation must at least provide for the establishment of clinic committees.
Hospital boards: In line with the provisions of the NHA, one of the eight core management
standards of the DHS is that the community acts as a shareholder in hospital management
and its representatives should be on the hospital board 16 . The provincial Head Office
indicated that the hospital boards were in place. It was also indicated that the Department
has, in conjunction with the North West University, developed a curriculum to capacitate the
board members on their roles and responsibilities. During interaction with the District Offices,
the inspection team was informed that hospital boards regularly convened meetings in line
with the applicable governance rules. However, at Brits Hospital officials raised concerns
that the board often involved itself in administration matters, and thus overstepped its
mandate as an oversight institution. It was also observed that board meetings were not
16 Republic of South Africa. A District Hospital Service Package for South Africa. A set of norms and standards. May 2002.

Page 19 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
regularly convened. The foregoing points to lack of clarity on the role of the board, and was
not in line with the relevant provisions of the NHA.
Clinics Committees: The inspection team was informed in all inspected facilities that clinic
committees have been established and were operational. However, the inspection team was
not provided with the minutes of such meetings. The purpose was to have an indication of
the key issues discussed during the meetings as well as the specific recommendations
made. The unavailability of the minutes raised concern whether these meetings were being
regularly held as required by the NHA. It is also the view of the PSC that these committees
could be dormant, and thus depriving the community of a constitutionally enshrined avenue
to contribute to improved service delivery at these clinics.
5.5 Challenges
The following challenges were identified as impacting negatively on effective and efficient
service delivery at the inspected facilities:
Hospital accommodation: It emerged during inspection at the Brits Hospital that there was
no doctors’ quarters. For instance, the Clinical Manager daily travelled a distance of
approximately 100 kilometres per return trip between Brits and his place of residence in
Pretoria. The situation was further exacerbated by lack of residential properties in Brits due
to the area being largely industrial. According staff, this has led to a high turnover of doctors
or challenge in recruiting doctors at the hospital.
Infrastructure: Serious challenges relating to infrastructure were noted at Unit 9 Clinic. The
inspection team observed that owing to lack of space, the room for patients suffering from
TB and waiting to receive treatment was very small, and located next to the data capturer’s
office. Furthermore, the installed ultra violet (UV) lights intended to quarantine TB
microorganisms, especially from seriously coughing patients, were not working, and thus
increasing the risk of the staff and other patients being infected. In addition, the had a
shortage of linen.
The inspection team also observed that Taung Station, Tlapeng, and Unit 9 clinics did not
have back-up generators in case of power failure. There were no telephones in some of the
clinics in rural areas. At Tlapeng Clinic the nursing staff informed the inspection team that
they used their cellular phones in case of emergencies. Although they were provided with
airtime, signal connection to the network was a challenge especially during rainy seasons.
Emergency Medical Services: The inspection was informed that emergency medical
services (EMS) were in all districts generally poor due to insufficient ambulances. It was
noted that response times to calls often varied from an hour to four hours. At times
ambulances failed to arrive following repeated calls which placed the lives of the affected
patients at risk. It emerged that in some cases officials would be forced to transport patients
in their private cars or patients would hire private cars at excessive costs. While the selfless
efforts of officials were commendable, this was a huge risk to take since the vehicles were
not fitted with life-saving apparatus, and had the potential to invite legal challenges.

Page 20 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Budgeting: During discussions with the provincial Head Office it emerged that the
Department was operating under serious budgetary constraints, which impacted negatively
on service delivery. For instance, it was indicated at the Bojanala District Office that although
a new Brits Hospital had been constructed through the Government’s Hospital Revitalization
Programme (HRP), the District’s budget had not been adjusted according to the 36 bed
facility. According to staff, this had the potential to limit availability of beds and other critical
resources at the hospital, and would lead to crowding and thus, defeating the key objectives
of the HRP and the National development Plan (NDP).
6. KEY FINDINGS ON UNANNOUNCED INSPECTIONS
The findings from unannounced inspections are presented below. Batho Pele as a key
strategy for the transformation of Public Service delivery sets out specific principles that
should be adhered to at all times17. It was the purpose of the unannounced inspections to
determine the extent to which the visited health care facilities adhered to these. Detailed
findings of these inspections are attached as ANNEXURE C.
6.1 Observing facilities
Condition of premises: The inspection team observed that the buildings of Unit 9 and
Tlapeng clinics were dilapidated and had cracks as well as paint peeling off the internal
walls. The ceiling of the Unit 9 Clinic was also damaged and its toilet facilities required
urgent refurbishing. For instance, an unbearable smell was noticed that filled the waiting
area and this posed a health risk. On close inspection of the facilities, it was worrying to
observe that sanitation pipes were damaged, and these were wrapped with pieces of plastic
in order to contain spilling. A water tap was damaged and officials used a bucket to trap the
dripping water.
17 Republic of South Africa. Department of Public Service and Administration. The Batho Pele White Paper on the
Transformation of Public Service Delivery, 1997.

Page 21 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Picture 9: Cracks observed in the walls of Unit 9 Clinic

Page 22 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Picture 10: Damaged sanitation pipes at Unit 9 Clinic

Page 23 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Picture 11: A dripping water tap at Unit 9 Clinic
Equally concerning was the exposed electrical wires at the Unit 9 Clinic, which placed the
facility at the risk of fire breaking out or citizens coming into contact with them, and thus
resulting in serious consequences. Overall, the clinic requires complete maintenance.
Picture 12: Damaged ceiling and exposed electric wires at Unit 9 Clinic

Page 24 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Lack of space: Generally, there was a problem of space in all the inspected facilities with
Unit 9 Clinic being worst affected. Officials informed the inspection team that Unit 9 Clinic
had two consultation rooms, which were insufficient considering the high average number of
patients received daily at the facility as indicated in paragraph 5.2.5 above. This resulted in
the staff on occasion using the emergency room reserved mainly for pregnant patients. In
addition, medical equipment items were found at the entrance for medical emergency
deliveries. These may obstruct medical personnel in responding to calls to patients requiring
immediate attention, and result in serious health consequences.
At Tlapeng Clinic, the inspection team observed that boxes of medical supplies and other
equipment were stored in the bathroom due to insufficient space. Officials mentioned that
the challenge had been reported, which was consistent with the concerns of the provincial
Head Office stated in paragraph 5.1 above.
Picture 13: Medical supplies and other equipment stored in the bathroom at Tlapeng Clinic
The challenge of space was also observed at Dryharts Clinic. A back-up generator was
found stored with boxes for disposable items. This raised concern to the inspection team as
the generator can trigger fire and result in serious damage.

Page 25 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Picture 14: Back-up generator stored with other items at Dryharts Clinic
Signage: Despite the aforementioned challenges, the inspection team observed that in all
the inspected health facilities clear signage was provided to guide citizens to the service
points.

Page 26 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Picture 15: Signage at Klerksdorp District Hospital
6.2 Access to information
The Batho Pele principle of access to information requires information to be readily available
to citizens in order to empower them and address their needs.
Service charters: Service standards, patients’ rights charters and other key information
relating to health care services such as payable fees, where applicable, were clearly
displayed in all sites visited. It was even more heartening to observe at Klerksdorp District
Hospital and Taung Station Clinic that the information was available in Setswana. Setswana
is one of the predominantly spoken indigenous languages in the areas serviced by the
visited sites. Using indigenous languages was empowering to the previously disadvantaged
communities and also restored their dignity as enshrined in the Constitution. This was also in
line with the Batho Pele principle of Access.

Page 27 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Picture 16: Information about baby feeding was displayed in Setswana at Klerksdorp District Hospital
Picture 17: Costs of services clearly displayed at Brits District Hospital

Page 28 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Redress: To encourage feedback on the quality of services from citizens on the services
they received, all public institutions are expected to have complaint/suggestion boxes. It is
also required of these institutions to provide the procedure outlining how suggestions or
complaints should be lodged, as well as the manner in which feedback can be expected. In
all the facilities visited the inspection team found that there were complaint/suggestion
boxes. In addition, the suggestions or complaints mechanism was displayed to encourage
citizens to freely make their contributions.
Picture 18: Complaints Mechanism displayed at Klerksdorp District Hospital
Furthermore, it was observed that information regarding management was displayed at most
facilitates to empower citizens in escalating their concerns in instances where they were not
satisfied with the quality of feedback provided.

Page 29 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Picture 19: Key information about management of Klerksdorp District Hospital
6.3 Talking to citizens
Citizens as consumers of the services provided by the institutions are in the best position to
give feedback on the state of service delivery. Their views and comments are important in
any effort meant to improve service delivery. Interviews were conducted with randomly
selected citizens on the quality of services rendered.
Availability of medicines and medical equipment: An insignificant number of citizens
complained about shortage of medicines. For instance, interviewed citizens at Unit 9 Clinic
indicated that there was a shortage of pills for family planning and treatment for epilepsy.
None of the interviewed citizens at all the inspected health facilities raised concerns relating
to availability and quality of medical equipment.
Waiting time: Most citizens were satisfied with the timeliness with which they received their
medication after consultation. At Unit 9 Clinic citizens were mainly unhappy about the waiting
time before being attended to. The foregoing is in line with the findings of shortage of staff
highlighted in paragraph 5.2.5 above. In addition, citizens at Taung Station Clinic complained
about the waiting area since it was small. The inspection team highlighted the challenge of
space at all facilities in paragraph 6.1.

Page 30 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
Consultation: During interaction with citizens in all visited clinics, the inspection team was
informed that there were clinic committees which provided them an opportunity to raise their
concerns with the clinic management to ensure improved quality of services. This finding is
in line with Batho Pele principle of consultation. It is also consistent with the observation
made by the inspection team with regard to redress above.
7. IMPLEMENTATION OF PSC RECOMMENDATIONS
The inspection team followed up on the PSC’s previous recommendations emanating from
the inspections of primary health care facilities conducted in 200918. It was found that 7
(58%) of the 12 recommendations were implemented by the NWDoH. The inspection team
was, however, informed that the erection of ramps and demarcated parking areas fell
outside the responsibility of the Department. It emerged that the provincial Department of
Public Works had been alerted in this regard. Detailed information relating to the
implementation the recommendations is provided as ANNEXURE D.
8. READINESS OF THE INSPECTED FACILITIES FOR THE ROLL OUT OF THE
NATIONAL HEALTH INSURANCE (NHI)
In essence, the NHI is a financing system that aims to ensure that all SA citizens, including
non-citizens who have attained permanent residence, are provided with the necessary
healthcare, regardless of their economic status. The NDoH has committed the first five years
of piloting the system to focus mainly on strengthening the following key priority areas:
Management of health facilities and health districts;
Quality improvement;
Infrastructure development;
Medical devices including equipment;
Human resources planning, development and management; and
Information management and systems support.
It is, therefore, the view of the PSC that streamlining of the operations of the health facilities
and health districts has been identified as critical for the success of the NHI. As the ancillary
aim of the inspections at the selected health facilities, the PSC sought to assess the sites’
readiness for the roll-out of the NHI. The inspection team observed that there were no major
challenges regarding availability of medicines. Concerns relating to medical equipment were
mainly about the poor quality of the procured BP machines as well as delays by District
Officials in attending to requests for maintenance of identified items. However, it was
observed that there was generally a challenge of space at the inspected health facilities. Of
serious concern was the condition of the buildings of Tlapeng and Unit 9 clinics which were
very poor. Equally worrying was the shortage of staff at Unit 9 Clinic, which manifested in the
disruption of service delivery with complaining that they often left unattended during tea and
lunch breaks. It is the view of the PSC that the NWDoH needs to address these challenges
18 Republic of South Africa. Consolidated Report on Inspections of Primary Health Care Delivery Sites: Department of
Health. 2010.

Page 31 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
without delay in order to ensure the readiness of the facilities for the successful
implementation of the NHI.
9. RECOMMENDATIONS
The recommendations contained in 9.1 and 9.2 below emanate from the inspections. These
recommendations should apply to all health facilities in the province that may be
experiencing similar challenges and not only those that were visited by the inspection team.
9.1 ANNOUNCED INSPECTIONS
The NWDoH should, in collaboration with the North West Department of Public
Works (NWDPW), address the shortage of accommodation for medical professionals
at the Brits District Hospital. (A plan of action must be in place by April 2015).
The NWDoH should ensure that all District Offices visit all health facilities, especially
clinics, monthly as required by the Handbook for Clinic/CHC Managers to oversee
their operations and ensure availability of the required medicines and other
resources. In this regard, the visits should be linked to the applicable performance
management system by April 2015.
The NWDoH should immediately ensure that asset management unit of the Ngaka
Modiri Molema DistrictOffice attend to the broken equipment found at Unit 9 Clinic in
terms of the relevant SCM prescripts. In addition, the responsible asset officials
should be held accountable for the delays in addressing the matter. (In this regard,
feedback should be provided to the PSC by 31 December 2014).
The NWDoH should strengthen its SCM process for procurement of medical
equipment and ensure that a system for suppliers of equipment in place to identify
those suppliers found to provide poor quality equipment for blacklisting. (A plan of
action must be in place by 31 March 2015).
Back-up generators should be provided to the Taung Station, Tlapeng and Unit 9
clinics in order to prevent disruption of services in case of power failure.(A plan of
action must be in place by 31 March 2015).
The NWDoH should immediately ensure availability of linen at Unit 9 Clinic.
Computers and network points should be provided at all the health facilities. (A plan
of action must be in place by 31 March 2015).
The NWDoH should review the human resource plan of the Bojanala District to
address the shortage of staff by 31 March 2015.

Page 32 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the
role of Health District Offices in the Department of Health: North West Province
9.2 UNANNOUNCED INSPECTIONS
The NWDoH should engage the NWDPW in order to address the challenge of space
in all the inspected health facilities. This should include the refurbishing of the
buildings of Unit 9 and Tlapeng clinics. (In this regard, a plan of action should be put
in place by April 2015).
10. CONCLUSION
The PSC’s inspections on availability of medicines and medical equipment have found that
there were challenges of availability of medicines at the visited health facilities. With regard
to medical equipment, it emerged that most of the inspected health facilities had the
necessary medical equipment to ensure sustainable service delivery. However, it was found
that the support of the District Offices was not in all instances sufficient. For instance, it was
observed that District Offices did not sufficiently conduct monthly visits, especially to clinics,
as required by the Handbook for Clinic/CHC Managers. As a result, key challenges
experienced by the health facilities such as poor quality and maintenance of medical
equipment, shortage of staff, condition of buildings, were not timeously addressed. It is,
therefore, hoped that the recommendations will assist the NWDoH in ensuring that quality
health care is provided at the inspected facilities.
11. ACKNOWLEDGEMENT
The PSC would like to express the appreciation for the cooperation received from the
officials of the Department in all the visited sites. It is the view of the PSC that the officials
were appreciative of the importance of the inspections in supporting the work of government
in its key objective for a long and healthy life for all South Africans.

Page 33 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the role of Health District Offices in the Department of Health: North West
Province
ANNEXURE A: A LIST OF FACILITIES VISITED AND OFFICIALS THAT WERE ENGAGED
Name of Institution Date Names and designation of interviewed personnel Inspection Team Members
Bojanala District Office Ms Mirriam Mabe, Manager T. Motladiile, Manager
Commissioner Sejosingoe Ms Thato Mohapi Mr Martin Chale Ms Mmapeu De Jenga Mr Patrick Funani Mr Lebogang Mautlwa Ms Mpho Kuane
Tlapeng Clinic Sister Montsho, Nursing Sister
Unit 9 clinic Sister Wechoemang, Nursing Sister
Brits hospital Dr. Pooe, Clinical Manager Ms Heidi Van Rooyen, Pharmacy Manager
Kenneth Kaunda District Office Ms N Mojanaga, Chief Director J. Mbele, Finance Manager
Commissioner Sejosingoe Ms Thato Mohapi Mr Patrick Funani Mr Patrick Funani Mr Lebogang Mautlwa Ms Mpho Kuane
DryhartsClinic Sister Mkenku, Nursing Sister Mr Patrick Funani Mr Lebogang Mautlwa Ms Mpho Kuane Ms Thato Mohapi
Taung Station Clinic Sister Vanqa, Acting Sister-in-Charge Mr Patrick Funani Mr Lebogang Mautlwa Ms Mpho Kuane
Klerksdorp Hospital P. Mokatsane, CEO M Dikging, Manager
Commissioner Sejosingoe Ms Thato Mohapi Mr Patrick Funani Mr Patrick Funani Mr Lebogang Mautlwa Ms Mpho Kuane

Page 34 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the role of Health District Offices in the Department of Health: North West
Province
ANNEXURE B: ANNOUNCED INSPECTIONS ON AVAILABILITY OF EMCICINES AND MEDICALEQUIPMENT IN THE FACILITIES
VISITED
Availability of medicines at inspected clinics
√ Norms and standards adhered to
X Norms and standards not adhered to
Tlapeng Clinic
Me
dic
ine
s
Me
dic
ine
ro
om
with
bu
rgla
r ba
rs
/lo
cka
ble
cu
pb
oard
s
Me
dic
ines a
nd
su
pp
lies s
tock
Me
cha
nis
m f
or
em
erg
ency
su
pp
lies
Ba
tte
ry %
spa
re
glo
be
s fo
r
au
rosco
pe
s
Me
dic
ines a
s p
er
ED
L fo
r P
HC
√ √ √ √ √
Unit 9 Clinic
√ √ √ √ √
Taung Station Clinic
Me
dic
ine
ro
om
with
bu
rgla
r ba
rs
/lo
cka
ble
cu
pb
oard
s
Me
dic
ines a
nd
su
pp
lies s
tock
Me
cha
nis
m f
or
em
erg
ency
su
pp
lies
Ba
tte
ry %
spa
re
glo
be
s fo
r
au
rosco
pe
s
Me
dic
ines a
s p
er
ED
L fo
r P
HC
√ √ √ √ √

Page 35 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the role of Health District Offices in the Department of Health: North West
Province
Dryharts Clinic
√ √ √ √ √

Page 36 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the role of Health District Offices in the Department of Health: North West
Province
Availability of medicines at inspected hospitals
Brits District Hospital
Me
dic
ine
s
Me
dic
ines s
up
ply
acco
rdin
g to
ST
G
an
d E
DL
: H
osp
ita
l le
ve
l
Me
dic
ines s
up
ply
acco
rdin
g to
ST
G
an
d D
L: P
rim
ary
Ca
re leve
l
Me
dic
ines a
nd
su
pp
lies a
lwa
ys in
sto
ck.
Tro
lleys w
ith
em
erg
ency d
rug
s a
nd
resu
scita
tio
n e
qu
ipm
en
t
Ph
arm
ace
utica
l T
he
rap
eu
tic
Co
mm
itte
e in p
lace
√ √ √ √ √
Klerksdorp Hospital
√ √ √ √ √

Page 37 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the role of Health District Offices in the Department of Health: North West
Province
Availability of medical equipment at the inspected hospitals
√ Norms and standards adhered to
X Norms and standards not adhered to
Brits District Hospital*
Me
dic
al e
qu
ipm
en
t
Ba
sic
eq
uip
me
nt fo
r
exa
min
atio
n o
f p
atie
nts
in
OP
D a
nd
wa
rds
Ad
ult a
nd
ch
ild e
lectr
on
ic
we
igh
ing
sca
les, m
easu
ring
rods a
nd
pe
dia
me
ters
Pro
cto
sco
pe
s
La
rynsco
pes
Pe
ak f
low
mete
rs
Glu
co
me
ters
He
am
og
lob
ino
me
ters
Lu
mb
ar
pun
ctu
re k
its
Ca
rdia
c m
on
ito
rin
g u
nit
Ge
ne
ral X
-ra
y r
oom
with
su
pin
e &
bucky u
nit w
ith
scre
en
ing
& ta
ble
ma
ttre
ss
Sn
elle
n c
hart
Ve
no
-pu
nctu
re s
et
Flu
id g
ivin
g s
et
A c
linic
al w
aste
sto
rag
e
Fix
ed
an
d/o
r m
ob
ile o
xyg
en
su
pp
ly
A p
riva
te a
rea
fo
r cou
nse
ling
(e.g
. H
IV/A
IDS
)
Ba
sic
eq
uip
me
nt to
co
ndu
ct
no
rma
l d
eliv
erie
s
EC
G
Em
erg
en
cy e
qu
ipm
en
t fo
r
tra
um
a a
nd
em
erg
ency
Tro
lleys w
ith
em
erg
ency
dru
gs &
re
suscita
tion
eq
uip
me
nt
√ √ √ √ √ √ √ √ √ x √ √ √ √ √ √ √ √ √ √
General X-ray room: Although the X-ray equipment was found to be working, the hospital was concerned that it had almost reached
the end of its lifespan and, therefore, needed to be replaced.
Klerksdorp Hospital
√ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √

Page 38 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the role of Health District Offices in the Department of Health: North West
Province
Availability of medical equipment at inspected clinics
√ Norms and standards adhered to
X Norms and standards not adhered to
Med
ica
l e
qu
ipm
en
t
Tlapeng Clinic
Dia
gn
ostic s
et
Blo
od
pre
ssure
mach
ine
s
Ste
tho
sco
pe
Sca
les f
or
adu
lts &
yo
un
g
ch
ildre
n
Me
asu
rin
g tap
es
Sp
ecu
lum
s o
f d
iffe
ren
t
siz
es
He
am
og
lob
ino
me
ter
Glu
co
me
ter
Pre
gna
ncy test
str
ips
Em
erg
en
cy tro
lley
Oxyg
en
cylin
de
r a
nd
mask
Te
lep
ho
ne
/ tw
o w
ay r
ad
io
Tw
o w
ork
ing
re
frig
era
tors
Sh
arp
s d
isp
osa
l syste
m
Ste
riliz
ation
syste
m
Eq
uip
men
t &
co
nta
ine
rs
for
takin
g b
loo
d &
oth
er
sa
mp
les
Co
nd
om
dis
pe
nse
r p
lace
d
wh
ere
easily
accessib
le
√ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √
Unit 9 Clinic
√ x √ √ √ √ √ √ √ √ √ √ √ √ √ √ √
Blood pressure machines: Gets overheated after prolonged usage then produce incorrect readings.
Taung Station Clinic
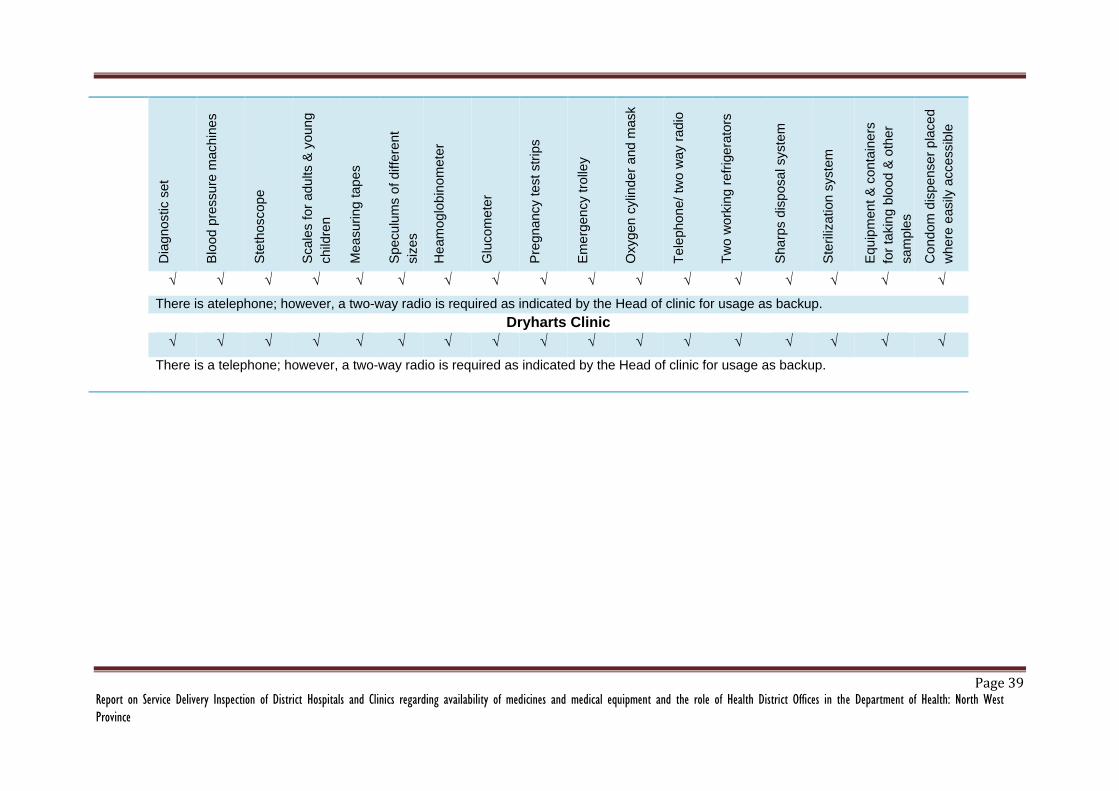
Page 39 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the role of Health District Offices in the Department of Health: North West
Province
Dia
gn
ostic s
et
Blo
od
pre
ssure
mach
ine
s
Ste
tho
sco
pe
Sca
les f
or
adu
lts &
yo
un
g
ch
ildre
n
Me
asu
rin
g tap
es
Sp
ecu
lum
s o
f d
iffe
ren
t
siz
es
He
am
og
lob
ino
me
ter
Glu
co
me
ter
Pre
gna
ncy test
str
ips
Em
erg
en
cy tro
lley
Oxyg
en
cylin
de
r a
nd
mask
Te
lep
ho
ne
/ tw
o w
ay r
ad
io
Tw
o w
ork
ing
re
frig
era
tors
Sh
arp
s d
isp
osa
l syste
m
Ste
riliz
ation
syste
m
Eq
uip
men
t &
co
nta
ine
rs
for
takin
g b
loo
d &
oth
er
sa
mp
les
Co
nd
om
dis
pe
nse
r p
lace
d
wh
ere
easily
accessib
le
√ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √
There is atelephone; however, a two-way radio is required as indicated by the Head of clinic for usage as backup.
Dryharts Clinic
√ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √
There is a telephone; however, a two-way radio is required as indicated by the Head of clinic for usage as backup.

Page 40 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the role of Health District Offices in the Department of Health: North West
Province
ANNEXURE C: UNANNOUNCED INSPECTIONS NORTH WEST CLINICS AND DITRICT HOSPITALS
X Batho Pele requirement adhered to
0 Batho Pele requirement not adhered to
* No fees payable at clinics.
Batho Pele requirements
Re
ce
pti
on
Ou
tsid
e s
ign
Ins
ide
sig
n
Bu
sin
es
s h
ou
rs
Pri
or
req
uir
em
en
ts
Co
st
of
serv
ice
s
Bu
ild
ing
in
go
od
co
nd
itio
n
Ra
mp
s
Cle
an
lin
ess
Sta
ff t
o g
uid
e p
eo
ple
Se
rvic
e c
hart
er
Se
rvic
e c
hart
er
in lo
ca
l
lan
gu
ag
e
vis
ibilit
y o
f se
rvic
e
ch
art
er
Info
rma
tio
n d
es
k
De
sk
wit
h m
ate
ria
l
De
sk
sta
ffe
d
Su
gg
esti
on
bo
x
Co
mp
lain
t p
roc
ed
ure
Na
me
ba
dg
es
Na
me
ba
dg
es
of
ba
ck
off
ice
sta
ff
frie
nd
lin
ess
Pro
fess
ion
alis
m
Air
-co
nd
itio
nin
g
sy
ste
ms
Pa
rkin
g
Dryharts Clinic 0 X X X X -* X X X X X X X X X 0 X X X X X X X X
Taung Clinic 0 X X X X X X X X X X X X X 0 X X X X X X X X
Brits District Hospital
X X X X X X 0 X X X X X X X X 0 X X X X X X X X
Klerksdorp District Hospital
X X X X X X 0 X X X X 0 X X X 0 X X X X X X X X
Tlapeng Clinic X X X X X - 0 0 X 0 X X X 0 0 0 X X X X X X X X
Unit 9 Clinic X X X X X - 0 0 X 0 X X X 0 0 0 X X X X X X X X

Page 41 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the role of Health District Offices in the Department of Health: North West
Province
ANNEXURE D: STATUS OF IMPLEMENTATION OF PSC RECOMMENDATIONS EMANATING FROM INSPECTIONS CONDUCTED IN
2009
The status on the on the implementation of recommendations that was done by the PSC in 2009 is as follows:
Details of the clinic Recommendations Implemented Not implemented
Tlapeng Clinic Ramps for people with disabilities should be erected. (In
this regard a plan of action should be in place by April
2010).
No Not yet implemented.
Demarcated parking areas should be made available (In
this regard a plan of action should be in place by April
2010).
No (District lack capacity).
Not yet implemented.
clinic building should be properly maintained Yes
Reception areas should be erected (In this regard a plan
of action should be in place by April 2010).
No Not yet implemented.
Service Charter should be translated into the local
language (In this regard a plan of action should be in
place by April 2010).
No Not yet implemented.
Staff should be provided with name tags by April 2010
and they must wear them
Yes
Manager should immediately arrange for proper removal
of medical waste
Yes
Clinic should be provided with functional computers, fax, and photocopy machine. (In this regard a plan of action should be in place by April 2010).
Only have functional computer.
Provision of Fax and photocopy
machine still not implemented.
Dryharts Clinic Service Charter should be translated into the local
language (In this regard a plan of action should be in
place by April 2010).
No Not yet implemented.
Clinic should be provided with functional computers, fax,
and photocopy machine. (In this regard a plan of action
Only have functional computer.
Provision of Fax and photocopy

Page 42 Report on Service Delivery Inspection of District Hospitals and Clinics regarding availability of medicines and medical equipment and the role of Health District Offices in the Department of Health: North West
Province
Details of the clinic Recommendations Implemented Not implemented
should be in place by April 2010). machine still not implemented
Clinics should be immediately be provided with sufficient
diesel for generator to ensure that the clinic functions
properly even when there is power failure.
Yes
Clinic should ensure that the clinic facilities remain clean
at all times. This should be done immediately.
Yes