report of the third who stakeholders meeting on
TRANSCRIPT
Report of the third WHO stakeholders meeting
on rhodesiense human African trypanosomiasis
Geneva, Switzerland, 10–11 April 2019
� 789240 012936


Report of the third WHO stakeholders meeting on
rhodesiense human African trypanosomiasis
Geneva, Switzerland, 10–11 April 2019

Report of the third WHO stakeholders meeting on rhodesiense human African trypanosomiasis, Geneva, Switzerland, 10–11 April 2019
ISBN 978-92-4-001293-6 (electronic version) ISBN 978-92-4-001294-3 (print version)
© World Health Organization 2020
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization (http://www.wipo.int/amc/en/mediation/rules/).
Suggested citation. Report of the third WHO stakeholders meeting on rhodesiense human African trypanosomiasis, Geneva, Switzerland, 10–11 April 2019. Geneva: World Health Organization; 2020. Licence: CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis iii
Contents
Abbreviationsandacronyms ........................................................................................................... v
1. Introduction .............................................................................................................................. 1
2. Openingremarks ...................................................................................................................... 2
3. Meetingobjectives ................................................................................................................... 3
4. TheglobalsituationofrhodesienseHAT .................................................................................. 4
5. Reviewoftheconclusionsofthepreviousmeeting ................................................................. 9
6. Countrystatusreports ............................................................................................................ 106.1 Kenya........................................................................................................................................... 10
6.2 Malawi ........................................................................................................................................ 14
6.3 UnitedRepublicofTanzania ........................................................................................................ 17
6.4 Rwanda ....................................................................................................................................... 22
6.5 Uganda ........................................................................................................................................ 24
6.6 Zambia ........................................................................................................................................ 30
6.7 Zimbabwe ................................................................................................................................... 33
7. EliminationofrhodesienseHATaspublichealthproblemin2020 ..........................................367.1 HumanAfricanTrypanosomiasisEliminationTechnicalAdvisoryGroup .................................... 36
7.2 Countrydossierforvalidation ..................................................................................................... 37
7.3 Validationprocess ....................................................................................................................... 38
7.4 Nationalindicators–countrystatus ........................................................................................... 39
7.5 NTDroadmap2030:targetsandindicators ................................................................................ 40
8. StrategiesforeliminationofrhodesienseHAT ........................................................................ 428.1 Overviewofeliminationefforts .................................................................................................. 42
8.2 Strategiesforelimination:case-finding ...................................................................................... 43
8.3 Strategiesforelimination:treatment ......................................................................................... 45
8.4 Strategiesforelimination:epidemiologicalsurveillance ............................................................ 45
8.4 Strategiesforelimination:IEC(information,education,communication) .................................. 46
8.6 Strategiesforelimination:coordination ..................................................................................... 46

iv ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
9. ClinicalmanagementofimportedeastAfricantrypanosomiasisin SouthAfrica:lessonslearnt .................................................................................................... 47
10. ExportedcasesassurveillancetoolforrhodesienseHAT ....................................................... 49
11. ClinicaltrialfortreatmentofrhodesienseHATwithfexinidazole ........................................... 52
12.OneHealth:linkingeliminationofrhodesienseHATwithotherinitiatives ............................ 5512.1 Epidemiologicalstudiesinanimalsandtsetseflies,andnewmolecular
approachesinZambia ................................................................................................................. 55
12.2 Tsetsecontrolandthemanagementofr-HAT ............................................................................ 56
12.3 OverviewofPATTECactivitiesinEastandSouthAfrica .............................................................. 57
12.4 FAOandPATT:theprogressivecontrolpathway(PCP)forAfricananimaltrypanosomosis ....... 59
13. Conclusions ............................................................................................................................. 61
Annexes
1. Agenda .................................................................................................................................... 62
2. Listofparticipants................................................................................................................... 63

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis v
Abbreviationsandacronyms
AAT animalAfricantrypanosomiasis
AU AfricanUnion
CIRAD CooperationInternationaleenRechercheAgronomiquepourleDéveloppement
CIRDES CentreInternationaldeRecherche-Développementsurl’ElevageenZoneSubhumide
CNS centralnervoussystem
CSF cerebrospinalfluid
DNDi DrugsforNeglectedDiseasesinitiative
DVS DirectorateofVeterinaryServices
ECCAS EconomicCommunityofCentralAfricanStates
FAO FoodandAgricultureOrganizationoftheUnitedNations
g-HAT gambiensehumanAfricantrypanosomiasis
HAT humanAfricantrypanosomiasis
HAT-e-TAG HATeliminationTechnicalAdvisoryGroup
IAEA InternationalAtomicEnergyAgency
ICIPE InternationalCentreofInsectPhysiologyandEcology
IEC information,educationandcommunication
MAAIF MinistryofAgriculture,AnimalIndustryandFisheries
NTD neglectedtropicaldisease
OIE WorldOrganisationforAnimalHealth
PAAT ProgrammeAgainstAfricanTrypanosomiasis
PATTEC PanAfricanTsetseandTrypanosomiasisEradicationCampaign
PCP progressivecontrolpathway
PCR polymerasechainreaction
r-HAT rhodesiensehumanAfricantrypanosomiasis
RDT rapiddiagnostictest
UTCC UgandaTrypanosomiasisControlCouncil
VBDCU VectorBorneDiseaseControlUnit
WHO WorldHealthOrganization


ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 1
1. Introduction
2020istheyearsetintheroadmap1onneglectedtropicaldiseases(NTDs),publishedbytheWorldHealthOrganization(WHO)in2012,asthetargetforeliminationofhumanAfricantrypanosomiasis(HAT)asapublichealthproblem.IntheLondonDeclarationonNTDs,2pharmaceuticalcompanies,donors,endemiccountriesandnongovernmentalorganizationsalsocommittedthemselvestomeetingthisgoal.Jointworksince2000resultedin2018infewerthan1000casesreportedglobally,ahistoricallylownumber.ImportantmilestonesarebeingreachedinachievingthegoalofeliminatingHATasapublichealthproblemby2020.
Elimination efforts have focused on gambiense HAT (g-HAT), which is responsible for most (about 98%)reportedcases.RhodesienseHAT(r-HAT)ischronicallyneglected.Thelownumberofreportedcasesfailstoattracttheinterestofdonorsandr-HATisthusoflowpriorityforhealthdecision-makers,despiteitsepidemicpotential.Domesticandwildanimal reservoirsmakethecontrolof r-HATmorecomplex.TheOneHealthapproach involving numerous sectors beyond human health, such as veterinary services, vector control,tourismandmanagementservicesofprotectedareas,isthewayforwardtoreachthesetgoals.
The first WHO stakeholders meeting on r-HAT elimination (Geneva, 20–22 October 2014)3 boosted the multisectoral coordinationmechanismbetweenWHOandpartners to eliminate r-HAT as a public healthproblem.Contributingpartnersincludedmembersofacademia,public–privatepartnerships,nongovernmentaland international organizations, donors and national sleeping sickness control programmes. The secondstakeholdersmeeting(Geneva,26–28April2017)4reviewedprogressandidentifiedessentialactivitiesforthefuturesuchassustainedsurveillance,multisectoralcoordinationandpartnerships,innovativemethodsandtoolsforcontrol,andimprovingcapacity-building.
ThisthirdstakeholdersmeetingtookplaceasthefirstroadmaponNTDs(2015–2020)wasalmostconcludedandthe new roadmap on NTDs (2021–2030)wasbeingprepared.Itwasthetimetosharetheachievements,challengesandviewsonthegoalofeliminationamongparticipatingcountriesandimplementingpartners,andtoadvancetheprocessofvalidationofeliminationandstrengtheningofsurveillancesystemsinordertodetectanyre-emergenceofthediseasebeforereachingepidemiclevelsagain.
1 Acceleratingworktoovercometheglobalimpactofneglectedtropicaldiseases:aroadmapforimplementation.Geneva:WorldHealthOrganization;2012(WHO/HTM/NTD/2012.1.http://www.who.int/neglected_diseases/NTD_RoadMap_2012_Fullversion.pdf).
2 TheLondondeclarationonneglectedtropicaldiseases.UnitingtoCombatNTDs;2012(http://unitingtocombatntds.org/resource/london-declaration).
3 ReportofthefirstWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis.Geneva,20–22October2014.Geneva:WorldHealthOrganization;2015(WHO/HTM/NTD/IDM/2015.2http://who.int/trypanosomiasis_african/resources/9789241508650/en/).
4 ReportofthesecondWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis.Geneva,26–28April2017.Geneva:WorldHealthOrganization;2017(WHO/HTM/NTD/IDM/2017.04 https://who.int/trypanosomiasis_african/resources/WHO_HTM_NTD_IDM_2017.04/en/).

2 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
2. Openingremarks
DrDanielDagne,CoordinatoroftheInnovativeandIntensifiedDiseaseManagementunit,WHODepartmentofControlofNeglectedTropicalDiseases,openedthemeetingandcalleditaturningpoint,asthecurrentroadmaponNTDsisalmostconcludedandthenewRoadmap2021–2030isbeingprepared.HeintroducedDrMweleceleNtuliMalecela, thenewDirectorof theWHODepartmentofControlofNeglectedTropicalDiseases,andDrAugustinKadimaEbeja,NationalProfessionalOfficeroftheWHOCountryOfficeinKinshasa,DemocraticRepublicoftheCongo.
DrEbejawelcomedallparticipantsonbehalfofDrMagaranBagayoko,actingDirectoroftheCommunicableDiseasesCluster,andtheentireNTDteamintheWHORegionalOfficeforAfrica.Hereflectedonthepreviousmeeting and emphasized theOneHealth approach in r-HAT control.Hehighlighted that all stakeholdershavean importantroletoplay intheirareaofcompetencetofacethechallengesof thenationalcontrolprogrammes.Finally,hethankedallthepartners,whosecommitmentisgreatlyappreciatedbytheAfricanregionaloffice.
DrMalecelaemphasizedtheimportanceofthenewNTDroadmap,theproposedgoalsandmilestonesforwhichareaccessibleonline.Endemiccountries,implementingpartners,donorsandstakeholdersareinvitedtocontributeandtheirinputiscrucial.ThegoalsandmilestonesareduetobefinalizedinAugust2019.ShenotedthesignificantprogressofcountriesinwhichHATisendemictowardseliminationandthecontributionoftheDrugsforNeglectedDiseasesinitiative(DNDi)toadvancingdrugdevelopment.However,eliminationmustbevalidatedandsurveillancestrengthened.Governmentcommitmentand investmentareessentialtomaintainthatsuccess,asismultisectoralinvolvementinaOneHealthapproach.DrMalecelaclosedherremarksbyacknowledgingtheinvestmentbyallpartnersparticipatinginthismeeting.
ThemeetingwaschairedbyDrJorgeSeixas,PortugueseInstituteofHygieneandTropicalMedicine,Lisbon.ThemeetingagendaisattachedasAnnex1andthelistofparticipantsasAnnex2.

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 3
3. Meetingobjectives
Theobjectivesofthemeetingwere:
~ to sustain the commitment of national authorities and technical and financial partners to WHO’sobjectivesforr-HAT;
~ to share achievements, challenges and views on the goal of elimination as a public health problemamongcountriesandimplementingpartners;
~ todiscussstrategiesforreinforcingcontrolandsurveillanceofr-HAT;
~ to assess the status of critical technical aspects in research, development and implementation oftherapeuticanddiagnostictools,epidemiologyandvectorcontrol;and
~ toconsolidatethenetworkforcollaborationandcoordinationamongstakeholders.

4 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
4. Theglobalsituationofrhode-siense HAT
WHOhasprioritizedeliminationofHATundertheInnovativeandIntensifiedDiseaseManagementunit.Twoformsofthediseaseexist:g-HAT,theslowlyprogressingform,causedbyTrypanosoma brucei gambiense, foundinwesternandcentralAfrica;andr-HAT,thefasterprogressingform,causedbyT. b. rhodesiense, in easternandsouthernAfrica.HAT is transmittedthroughthebiteof infectedtsetseflies (Glossinagenus).ThegoaloftheHATcontrolandsurveillanceprogrammeistoeliminateHATasapublichealthproblemby2020.Since2001,thiseliminationpriorityhasbeensupportedbyapublic–privatepartnershipwithSanofiandBayer.
EliminationofHAT(g-HATandr-HAT)asapublichealthproblemhasbeendefinedasfewerthan2000casesreportedperyearatacontinentallevel,anda90%reductionofthetotalareaatriskreportingmorethanonecaseper10000peopleannually (from2004baseline levels).Forg-HAT, thenextgoal is to interrupttransmission (i.e.achievesustainableeliminationof zero reportedcases)by2030.For r-HAT, thegoal for2030istomaintaineliminationasapublichealthproblem(i.e.noareaatriskreportingmorethanonecaseper10000peopleannually).Thepursuitofthegoal forr-HAT issignificantlymorecomplexthanthatforg-HATbecauseofthepredominanceofanimalreservoirs.Thelatest(2013)technicalreportofaWHOExpertCommitteeoncontrolandsurveillanceofHAT5statesthatcompleteeliminationisnotatechnicallyfeasiblegoalforr-HATwiththecurrentmeans,butitdoesnotruleoutitseliminationasapublichealthproblem.
Itispossibletoeliminater-HATasapublichealthproblem.Itsoccurrenceisrare,andthecurrentlandscapesuggests thatsomeareasmaybewithin rangeof thisgoal.The incidenceof thedisease iswellmapped,particularlythroughtheAtlasofHAT,6whichisanessentialresourceformonitoringprogressbutwhichmaypresentanincompletepictureduetounderreporting.
Eliminationasapublichealthproblemisarelevantgoalas ithelpstoraiseawarenessofthediseaseandencouragescountriestoinvestinitscontrol.SeveralkeyelementsoftheWHOcontrolprogrammerevolvearound:(i)providingsupportandtechnicalguidancetocountriesendemicforthediseasenationallytoensureaccesstodiagnostictoolsandtreatmentforallpeopleatrisk; (ii)strengtheningsurveillancebygatheringand analysing all the data considered relevant to plan andmonitor interventions; and (iii) coordinatingstakeholdersinvolvedinr-HATelimination.Importantly,reducingthenumberofcasesisnotanend-pointinitselfbutratherthefirststeptowardsanintegrated,sustainablesurveillanceprogramme.Forthisreason,themethodofassessingthisfirststepofeliminationwillbestraightforward.Conversely,theprocesswillbemuchmorecomplexandstringentforassessingtheinterruptionoftransmissionofthedisease.
Sincethereported32850HATcasesin2000,thenumberofcaseshasdecreasedsignificantlyto<2000casesannuallyforthefirsttime:1446caseswerereportedin2017(Figure 4.1).Mostcases(77%)werediagnosedintheDemocraticRepublicoftheCongo. InGuinea,thenumberofcasespeakedat>100 in2016–2017,possiblyduetotheresumptionofcontrolactivitiesaftertheEbolacrises. Thedatafor2018arebeingfinalized
5 ControlandsurveillanceofhumanAfricantrypanosomiasis.Geneva:WorldHealthOrganization;2013(WHOTechnicalReportSeries,No.984(http://apps.who.int/iris/bitstream/10665/95732/1/9789241209847_eng.pdf).
6 SimarroPP,CecchiG,PaoneM,FrancoJR,DiarraA,RuizJAetal.TheAtlasofhumanAfricantrypanosomiasis:acontributiontoglobalmappingofneglectedtropicaldiseases.IntJHealthGeogr.2010;9:57(http://www.ij-healthgeographics.com/content/9/1/57).

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 5
butalreadyshowadecreaseto<1000casesglobally.Nationalcontrolprogrammesarethuswellplacedtoreachtheeliminationgoalsby2020.Whiletheproportionalcontributionofr-HAT(2%ofcases)totheglobalnumberofHATcasesislowcomparedwiththatofg-HAT(98%ofcases),itmustnotbeoverlooked.
Figure 4.1. NumbersofHAT(g-HATandr-HAT)casesreportedannuallysince2000,withthebenchmark(2020)forelimination(expectedcases)
r-HATisendemicinUganda,theUnitedRepublicofTanzania,Malawi,Mozambique,Kenya,Rwanda,ZambiaandZimbabwe.Since2000,therehasbeenacleardecliningtrendinthenumberofreportedr-HATcases:31in2017(fromfiveendemiccountries)and24in2018(fromthreeendemiccountries)(Figure 4.2, Table 4.1).
Figure 4.2. Numbersofr-HATcasesreportedannuallysince2001atgloballevel

6 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Table 4.1. Numbersofr-HATcasesreportedbyendemiccountries,2000–2018
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
Botswana - - - - - - - - - - - - - - - - - - -Burundi - - - - - - - - - - - - - - - - - - -Ethiopia - - - - - - - - - - - - - - - - - - -Kenya 15 10 11 0 0 0 1 0 0 1 0 0 2 0 0 0 0 0 0Malawi 35 38 43 70 48 41 58 50 49 39 29 23 18 35 32 30 35 11 15Mozambique - - 1 - 1 - - - - - - - - - - - - - -Namibia - - - - - - - - - - - - - - - - - - -Rwanda - - - - - - - - - - - - - - - - 0 0 0Swaziland - - - - - - - - - - - - - - - - - - -Uganda(Tbr) 300 426 327 338 335 473 261 119 138 129 112 84 71 43 70 28 10 13 4United Republicof Tanzania 350 277 229 113 159 185 127 126 59 14 5 1 4 1 1 2 4* 3 0
Zambia 9 4 5 15 9 7 6 10 13 4 8 3 6 6 12 8 4 3 5Zimbabwe - - - - - 3 - - 0 3 2 4 9 1 3 3 1 1 0Total reported 709 755 616 536 552 709 453 305 259 190 156 115 110 86 118 71 54 31 24
From2001to2017,Ugandareportedmorethanhalf(58%)ofthe5134r-HATcasesglobally.From2013to2017,twocountries(UgandaandMalawi)reportedthemajorityofcases(46%and39%)andthreecountries(theUnitedRepublicofTanzania,ZambiaandZimbabwe)theremainder(Table 4.1, Figure 4.3).
Figure 4.3. Distributionofr-HATcasesinendemiccountries,2013–2017(includingexportedcases)

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 7
Theoverallpopulationatrisk(i.e.thetotalnumberofpeoplelivinginareasreporting>1caseper10000peopleannually)isconstantlydecreasing,butthereremain4.2millionpeopleforwhomthediseaseremainsapublichealthproblem.Currently, therearenopopulationsathighorveryhigh riskof r-HAT,but someremainatmoderaterisk(Figure 4.4).
Figure 4.4. Populationatriskofr-HATsince2000andprogressionbyfive-yearperiods
While the coverage of the population at risk of infection has improved, a significant proportion still hasdifficultyaccessingdiagnosisandtreatmentforr-HAT.In2017,some124fixedhealthfacilitiesprovidedanydiagnosisofr-HATand44fixedhealthfacilitiesprovidedtreatmentforr-HAT(Table 4.2).
Table 4.2. Healthfacilitiesprovidingr-HATdiagnosisandtreatmentin2017,byendemiccountry
CountryDiagnosis Treatment
TOTAL ΔDxC DxP DxPhTotal
Dx Δ Tx1S Tx2M Total Tx ΔKenya 25 22 16 25 0 15 15 15 14 25 0Malawi 20 6 4 20 0 4 4 4 0 20 0Rwanda 12 12 4 12 12 0 0 0 0 12 12Uganda 37 36 12 37 -1 10 10 10 3 37 -1UnitedRepublicof Tanzania 17 5 2 17 2 4 4 4 -7 17 2
Zambia 12 12 12 12 0 10 10 10 2 12 0Zimbabwe 1 1 1 1 0 1 1 1 0 1 0Total 124 94 51 124 13 44 44 44 12 124 13
DxC,clinicaldiagnosis;DxP,parasitologicaldiagnosis;DxPh,diseasestaging;Tx1S,first-stagetreatmentwithsuramin;Tx2M,second-stagetreatmentwithmelarsoprol;∆,differencefrompreviousyear
Ofthepopulationatmoderateriskofr-HAT in2017,87%lived lessthan3hours (94%lessthan5hours)awayfromahealthfacilitycapableofdiagnosingr-HATand78%livedwithin3hours(89%within5hours)ofafacilitythatprovidestreatment.Ofthepopulationatlowrisk,69%livedlessthan3hours(84%lessthan5hours)awayfromahealthfacilitycapableofdiagnosingr-HAT,and62%within3hours(76%within5hours)ofafacilitythatprovidestreatment.

8 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
One important caveat about the data on r-HAT is underreporting. The disease progresses rapidly,whichmakesitmoredifficulttodetectcasesbecausedeathcanoccurbeforepatientsreachahealthcarefacilitycompetentindiagnosisofHAT,especiallyiftheyliveinasparselypopulatedarea.
Exportedcases(i.e.casesdiagnosedoutsidethecountryofinfection)areinfectedmostlyintouristicareas(e.g.nationalparks,wildlifereserves).Indeed,veryfewcasesarereportedfromthelocalpopulationinthesesameareas.AllexportedcasesarereportedtoWHO,becauseonlyWHOenablesaccesstotreatment.WHOcanuse the reportednumberofexportedcasesasan indicatorof thepresenceof r-HAT transmission ingeographicalareas.
Therearenoappropriate serological screening tools for r-HAT,and thereforedetectionof cases reliesonclinicalsuspicionandparasitologicaldiagnosis.Itwouldlikelybedifficulttofindasponsortodevelopanewserologicalscreeningtool.Thelowawarenessofr-HATandthelackofpreparednessofhealthsystemscouldalsoleadtomisdiagnosisofthedisease.EveninepidemicsituationssuchasinUgandaduring1988–1990,mathematicalmodelsestimatedthat39%ofcaseswentundetected,and92%ofdeathswereunreported.7 Furthermore, the increased use of rapid diagnostic tests (RDTs) for malaria, replacing examination bymicroscopy,hasreducedthenumbersofincidentalr-HATdiagnosesthroughmicroscopy.Itwaspointedoutthatrotationofexperiencedlaboratorystaffalsoreducescapacitiesfordiagnosis.
HealthcareworkersshouldbesensitizedtoreferpatientsformicroscopicexaminationincaseofanegativeRDTformalaria,aswellaspatientswithpositiveRDTwhoareunresponsivetoantimalarialtreatment.
Itwasnotedthatgreatprogresshasbeenmadetowardstheeliminationgoalandinreachingthedefinedmilestones,evenwithdeficienttools.Nonetheless,underdiagnosesandareasthatarenotwellcoveredbycontrolandsurveillanceactivities,andthuswherethesituationisnotwellknown,mustbetakenintoaccount.
7 OdiitM,ColemanPG,LiuWC,McDermottJJ,FèvreEM,WelburnSCetal.Quantifyingthelevelofunder-detectionofTrypanosomabruceirhodesiensesleepingsicknesscases.TropMedIntHealth.2005;10(9):840–9.

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 9
5. Reviewoftheconclusionsofthepreviousmeeting
Box 5.1 summarizes theconclusionsof thesecondstakeholdersmeeting (Geneva,26–28April2017)andjudgestheprogressofitsrecommendations.Thestartofaclinicaltrialtoassesstheefficacyoffexinidazolefortreatmentofr-HATmarksimportantprogress,asdoesthedevelopmentoftoolstoassessandvalidatetheachievementofr-HATelimination.Onlysomecountrieshaveforgedcollaborationandcoordinationofdifferent sectors and reinforced national coordination bodies. Several recommendations have not beenaddressed,notablyonimprovingsurveillance,developingserologicalscreeningtools,tailoringtargetproductprofilesofvectorcontroltoolsandincreasingtheuseofbloodsmearmicroscopy.
Box 5.1. ConclusionsofthesecondWHOstakeholdersmeetingonr-HATelimination in2017andwhethertherecommendationwasfollowed or not followed
CONCLUSIONS MEETING 2017 ~ Itisnecessarytoimprovesurveillancebyexpandingcountrycapacityforcasedetection.
~ Thedevelopmentofbettercontroltoolsisencouraged
¾ Developmentofserologicalscreeningtoolsisneeded. ¾ Strongdemand for extending the clinical trials of fexinidazole as a
treatmentforr-HAT.
¾ Target product profiles of vector control tools tailored to differentenvironments are needed.
¾ The increased use of rapid diagnostic tests (RDTs) for malariahas reduced the use of blood smear microscopy, diminishing thepossibilityofdiagnosingr-HAT.Theuseofbloodsmearmicroscopyinr-HATendemicareasshouldbeencouraged.
~ WHOisrequestedtoprovideguidanceontherequirements,proceduresand criteria for assessing and validating the elimination of r-HAT as apublichealthproblem.
~ r-HATendemic countries express their interest in gainingownershipofandpromoting theuseof theAtlas ofHAT at national level, providingappropriatetrainingmaterialinEnglish.
~ Collaboration and coordination of different sectors including animalhealth, agriculture, conservation of natural areas, tourism and humanhealth is required. The establishment and reinforcement of nationalcoordinationbodiesisrequired

10 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
6. Countrystatusreports
6.1 Kenya
Current situation
Epidemicsofr-HATinKenyahavebeeninterspersedwithlongperiodsoflowendemicityacrossthreemainfoci:theLambweValley,westernKenyaandtheMasaiMaraNationalReserve.Theclusterofcasesdetectedintheearly2000sinwesternKenyawasdrasticallyreducedinsubsequentyearsinresponsetojointworkbythegovernmentsofKenyaandUgandainmobilizinglocalauthoritiesandactingcollaboratively.Thetwolastcasesreportedwerein2012fromtheMasaiMaraNationalReserve.Bothcases(diagnosedinBelgiumandGermany)wereinstage1ofthedisease.Afteramassiveresponsefrommultiplegroups,nomorecaseshavebeendetectedinlocalpeopleortouristssincethen.NocaseshaveoccurredintheLambweValleysince1992andinwesternKenyasince2009.Historically,reportedcasesfromwesternKenyahavebeeninlocalpeople,whereasinMasaiMarathediseasehasbeenexclusivelyreportedintourists.
Endemic foci/regions at risk of r-HAT (Figure 6.1.1) ~ Focus1:LambweValley(RumaNationalParkoccupiesone-thirdofthevalleyfloor);
~ Focus2:WesternKenya(Busia,Teso,Bungoma,MountElgondistricts);
~ Focus3:MasaiMaraarea(MasaiMaraNationalReserveis71kmfromSerengetiNationalParkintheUnitedRepublicofTanzania).
ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 11
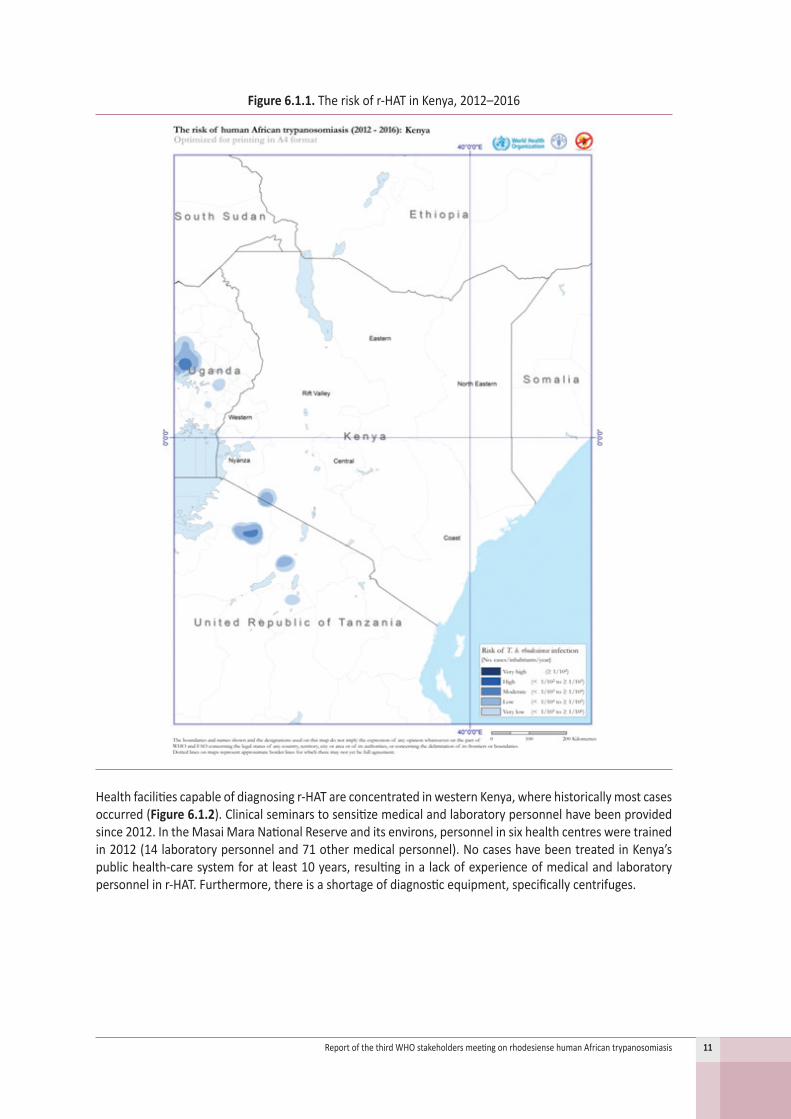
Figure 6.1.1. Theriskofr-HATinKenya,2012–2016
Healthfacilitiescapableofdiagnosingr-HATareconcentratedinwesternKenya,wherehistoricallymostcasesoccurred(Figure 6.1.2).Clinicalseminarstosensitizemedicalandlaboratorypersonnelhavebeenprovidedsince2012.IntheMasaiMaraNationalReserveanditsenvirons,personnelinsixhealthcentresweretrainedin2012(14laboratorypersonneland71othermedicalpersonnel).NocaseshavebeentreatedinKenya’spublichealth-caresystemforatleast10years,resultinginalackofexperienceofmedicalandlaboratorypersonnelinr-HAT.Furthermore,thereisashortageofdiagnosticequipment,specificallycentrifuges.
12 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
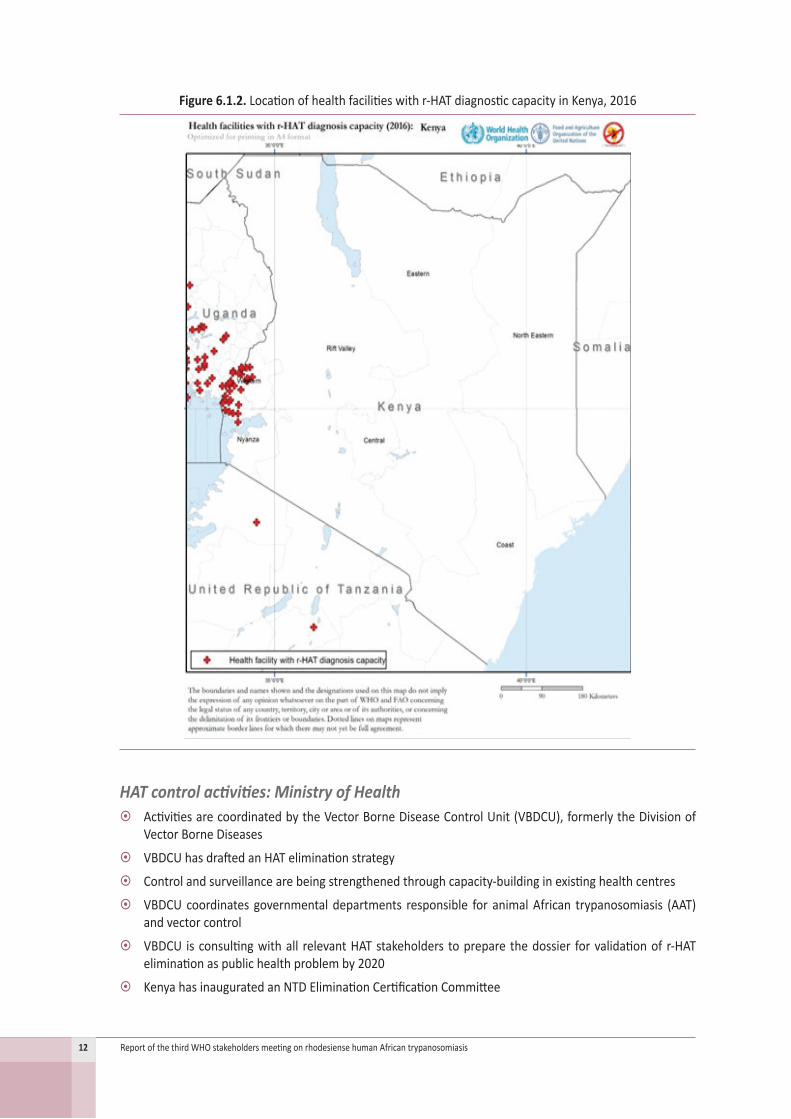
Figure 6.1.2. Locationofhealthfacilitieswithr-HATdiagnosticcapacityinKenya,2016
HAT control activities: Ministry of Health ~ ActivitiesarecoordinatedbytheVectorBorneDiseaseControlUnit(VBDCU),formerlytheDivisionofVectorBorneDiseases
~ VBDCUhasdraftedanHATeliminationstrategy
~ Controlandsurveillancearebeingstrengthenedthroughcapacity-buildinginexistinghealthcentres
~ VBDCUcoordinates governmentaldepartments responsible for animalAfrican trypanosomiasis (AAT)andvectorcontrol
~ VBDCU isconsultingwithall relevantHATstakeholders toprepare thedossier forvalidationof r-HATeliminationaspublichealthproblemby2020
~ KenyahasinauguratedanNTDEliminationCertificationCommittee

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 13
~ Health services have been devolved to County Governments (decentralization reform) since 2014,causingsomelossofstafftrainedinHAT
~ Nationalsupportandfunding:otherhealthneedsareprioritizedduetozeroreportedHATcases
Partners in HAT and funding from partners ~ The Government of Kenya provides human resources, financial and non-financial facilitation andcoordinationofHATactivities
~ WHOprovidesantitrypanosomalmedicinesandsupportssurveillanceofHAT
~ TheUnitedStatesNationalInstitutesofHealthprovidesresearchfunding
~ TheInternationalAtomicEnergyAgency(IAEA)providesresearchcapacity-buildingandfunding
~ TheUnitedStatesCentersforDiseaseControlandPreventionfundsHATresearchandintervention
~ DNDiprovidescapacity-building
~ TheSwissTropicalandPublicHealthInstituteprovidescapacity-building
~ Other sectors active in tsetse and trypanosomiasis control
~ TheKenyaTsetseandTrypanosomiasisResearchCouncil(KENTTEC)conductstsetsecontrolactivities
~ The Kenya Agricultural & Livestock Research Organization (KALRO) supports HAT diagnosis andsurveillance,rapidresponseforsuspectedcasesandoverseesthedevelopmentofnewcontroltools
~ TheKenyaWildlifeServicefocusesonRumaNationalParkandtheMasaiMaraGameReserve
~ TheInternationalCentreofInsectPhysiologyandEcology(ICIPE)conductsresearchonvectorcontroltools
~ TheDirectorateofVeterinaryServicesengagesinveterinaryservicesanddiseasecontrol
Challenges to r-HAT control ~ AccordingtoanassessmentbyVBDCU,99%ofhealthfacilitiesand98%ofhealthworkersincountiesformerlyendemicforr-HAThavenocapacitytodetectordiagnoseHAT
~ Theabsenceofthediseasecontributestolowawarenessamongcommunitiesandhealthworkers
~ Expertiseisbeingprogressivelylostthroughtransfersandnaturalattrition,withnoreplacementofstaff
~ Diagnosisiscomplicated,andthecurrentdiagnostictoolsareinadequate
Future perspectives ~ Completether-HATeliminationstrategydocumentledbyVBDCUandtheMinistryofHealthofKenya
~ Strengthendiagnostic capacity forHAT in existinghealth facilities servingnon-traditional foci (MasaiMara);providetrainingandprogrammesupportvisits
~ Continuetodeveloporadoptnewtoolsfordiagnosisandcontrol
~ Maintain vector control activities in relevant regions and enhance control of AAT (Kenya Tsetse andTrypanosomiasisResearchCouncil,DirectorateofVeterinaryServices)
~ StrengthencoordinationofcontroleffortsamongpartnersthroughtheOneHealthapproach
~ Provideequipmentfordatamanagementandusethesedatatoplanandmonitorinterventions(e.g.HATAtlas)
~ Createandmaintainr-HATawarenessamongcommunitymembers
~ AttendmeetingsofinternationalfocalpointsonHAT
~ Synergizeeffortstosubmitthedossierforvalidationofr-HATelimination

14 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
6.2 Malawi
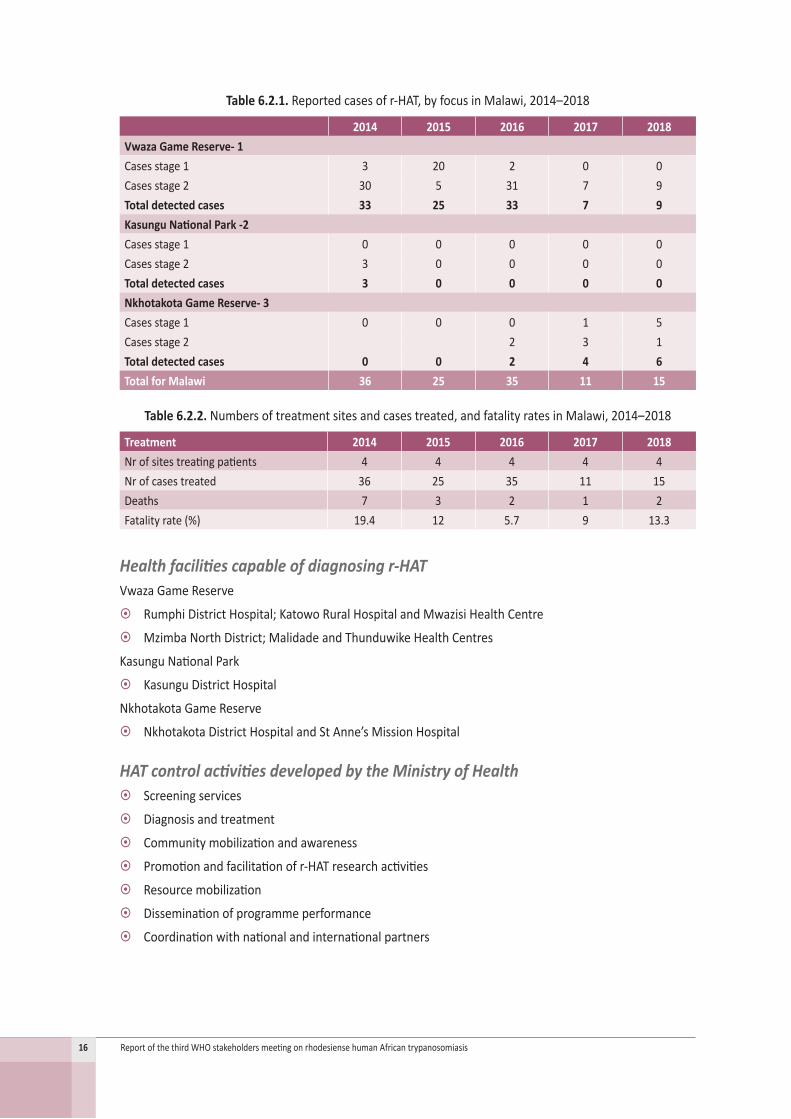
Current situationMalawihasthreefociofr-HATtransmissioninthecentral,westernandnorth-westernregions(Figures 6.2.1–6.2.2).Thenumbersofreportedcasesfellto11in2017and15in2018(Table 6.2.1),mostofwhichwerefromtheVwazaGameReserve(Rumphifocus).Since2016,caseshavebeenreportedinNkhotakotaGameReserveagainafter7consecutiveyearswithoutcases.Itisassumedthatr-HATwasreintroducedbyimportedcattleandelephantsin2014.ThenumberofsitestreatingpatientsandthefatalityratesaregiveninTable 6.2.2.
Figure 6.2.1. Distributionofr-HATcasesinMalawi,2013–2017

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 15
Figure 6.2.2. Theriskofr-HATinMalawi,2012–2016
16 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Table 6.2.1. Reportedcasesofr-HAT,byfocusinMalawi,2014–2018
2014 2015 2016 2017 2018Vwaza Game Reserve- 1Casesstage1 3 20 2 0 0Casesstage2 30 5 31 7 9Total detected cases 33 25 33 7 9Kasungu National Park -2Casesstage1 0 0 0 0 0Casesstage2 3 0 0 0 0Total detected cases 3 0 0 0 0Nkhotakota Game Reserve- 3Casesstage1 0 0 0 1 5Casesstage2 2 3 1Total detected cases 0 0 2 4 6Total for Malawi 36 25 35 11 15
Table 6.2.2. Numbersoftreatmentsitesandcasestreated,andfatalityratesinMalawi,2014–2018
Treatment 2014 2015 2016 2017 2018Nrofsitestreatingpatients 4 4 4 4 4Nrofcasestreated 36 25 35 11 15Deaths 7 3 2 1 2Fatalityrate(%) 19.4 12 5.7 9 13.3
Health facilities capable of diagnosing r-HATVwaza Game Reserve
~ RumphiDistrictHospital;KatowoRuralHospitalandMwazisiHealthCentre
~ MzimbaNorthDistrict;MalidadeandThunduwikeHealthCentres
KasunguNationalPark
~ KasunguDistrictHospital
Nkhotakota Game Reserve
~ NkhotakotaDistrictHospitalandStAnne’sMissionHospital
HAT control activities developed by the Ministry of Health ~ Screeningservices
~ Diagnosisandtreatment
~ Communitymobilizationandawareness
~ Promotionandfacilitationofr-HATresearchactivities
~ Resourcemobilization
~ Disseminationofprogrammeperformance
~ Coordinationwithnationalandinternationalpartners

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 17
Control activities carried out by other sectors ~ MinistryofAgricultureandveterinaryservices:treatmentofsickanimals
~ Wildlifesector:responsiblefortsetsecontrolbysettingtrapsinparksandgamereserves
~ Academicinstitutions:planandconductresearch,anddisseminateresultsforpolicychange
Multisectoral organization and coordination ~ NationalTrypanosomiasisControlCommittee,secretariatisintheMinistryofHealth
~ Ministry ofAgriculture, Irrigation andWaterDevelopment,Ministry of PublicWorks andMinistry ofNaturalResourceschairmeetingsalternatively
~ Academicinstitutionswritereports
~ Goodcollaborationwithdepartmental,inter-ministerialandotherimplementingpartnersanddonors
~ Localpartners:ministries(MinistryofAgriculture,IrrigationandWaterDevelopment,MinistryofPublicWorks, Ministry of Natural Resources); academic institutions (Lilongwe University of Agriculture &NaturalResourcesCollegeofMedicine,KamuzuCollegeofNursing.
~ Implementingpartners:DNDi and WHO
Vector control activities ~ Trapsandtargetscoveronlyafewplacesinthethreeendemicareas
~ InchargeoftheDepartmentofNationalParksandWildlifeChallenges to r-HAT control
~ Inadequatelytrainedhealthworkers
~ Low-techscreeningtools
~ CasesreemerginginNkhotakotaGameReserveafter7yearsofnocases
~ Lackofautilityvehicleatprogrammelevel
~ TheHATprogrammeisinadequatelyfunded
Future perspectives ~ TrainHAThealthworkersinthreedistricts
~ Providehigh-techscreeningtools
~ Increasecommunitymobilizationandawareness–brieftraditionalhealersonHAT
~ Ensureroutinesupportivesupervision
6.3 United Republic of Tanzania
Current situationThefirstrecordedcaseofr-HATintheUnitedRepublicofTanzaniawasin1922inMaswaDistrict,Shinyangaprovince. Largeoutbreaks in thenorth-westernpartof thecountry throughout10endemic regionshavegeneratedmorethan90%ofreportedcases.Thenumberofreportedcaseshasdecreasedsince1995,with≤5casesreportedannuallysince2009andevenzeroreportedcasesin2018(Table 6.3.1).

18 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Figure 6.3.1. Distributionofr-HATcasesintheUnitedRepublicofTanzania,2012–2016
Foci/regions affected by r-HAT (Figures 6.3.1–6.3.2) ~ Tabora:Urambo,Kaliua
~ Katavi: Mpanda
~ Kigoma:Kibondo,Kasulu,Uvinza(Nguruka)
~ Manyara:Magugu,Tarangire
~ Mara:Mugumu,Serengeti
Allhaveprotectedareaswithnearbynationalparks.

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 19
Figure 6.3.2. Theriskofr-HATintheUnitedRepublicofTanzania,2012–2016
Table 6.3.1. Reportedcasesofr-HATbyfocusintheUnitedRepublicofTanzania,2014–2018
2014 2015 2016 2017 2018KigomaCasesstage1 1 0 1 0 0Casesstage2 0 0 1 0 0Total detected cases 0 0 2 0 0TaboraCasesstage1 0 1 2 0 0Casesstage2 0 0 1 0 0Total detected cases 0 0 3 0 0Mara, SerengetiCasesstage1 0 1 0 3 0Casesstage2 0 0 0 0 0Total detected cases 0 0 0 0 0Total for TanzaniaCasesstage1 0 0 3 0 0Casesstage2 0 0 2 0 0Total detected cases 1 2 5 3 0

20 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Health facilities capable of diagnosing r-HAT (Figure 6.3.3) ~ Alldistrictandregionalhospitals
~ Allhealthcentres
~ Afewdispensaries(private,refugeecamps,faithbased)
Figure 6.3.3. Locationofhealthfacilitieswithr-HATdiagnosticcapacityinthe UnitedRepublicofTanzania,2016
Table 6.3.2. Numbersoftreatmentsitesandcasestreated,andfatalityratesinthe UnitedRepublicofTanzania,2014–2018
Treatment 2014 2015 2016 2017 2018Nrofsitestreatingpatients 23 23 23 23 23Nrofcasestreated 1 2 5 3 0deaths 0 0 0 0 0Fatalityrate(%) 0 0 0 0 0
ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 21
HAT control activities: Ministry of HealthCoordination
~ TheepidemiologyunitoftheMinistryofHealth,CommunityDevelopment,Gender,ElderlyandChildrenhasafocalpersonforHAT
~ TheMinistryofHealth,CommunityDevelopment,Gender,ElderlyandChildrenisamemberoftheOneHealthCoordinationUnitinthePrimeMinister’soffice
Strategies
~ HATinterventionsarepartoftheNTDMasterPlan
~ NationalOneHealthStrategy,GuidelineforSurveillanceofZoonoticDiseases
~ NationalStrategyforControlofTsetseandTrypanosomiasis(draft2018)
Fundingfrompartners
~ WHO:forantitrypanosomalmedicines,capacity-buildingandonedesktop
~ FAO:fordevelopmentofadraftstrategyfortsetseandtrypanosomiasiscontrol
Multisectoral organization and coordination ~ TheOneHealthCoordinationDesk,established in thePrimeMinister’sOffice,coordinatescontrolofzoonoses,includingHAT
~ Sixzoonoticdiseasesareprioritized,amongthemHAT
~ Anationalstrategy(guide)hasbeendeveloped;eachsectoractsaccordingly
~ PartnersinHATcoordinationframework(OneHealthCoordinationDesk):MinistryofHealth,CommunityDevelopment,Gender,ElderlyandChildren,MinistryofLivestockandFisheries,TanzaniaNationalParks,NationalInstituteforMedicalResearch,UnitedStatesAgencyforInternationalDevelopment,WHO,FAOandacademia
Vector control activities ~ Generallysmallscale
~ Innationalparks:tourism(Serengeti,Ngorongoro,Tarangire,Katavi)
~ Methodsused
¾ impregnatedtargets(nationalparks)
¾ sprayingoftouristvehicles(nationalparks)
¾ treatmentofanimals,e.g.usingisometamidiumbromide(inpastoralcommunities)
¾ sprayingofanimals(inpastoralcommunities)
¾ researchontsetsefly(vectorsandvector-bornediseases)
~ Responsible institutions: Tanzania National Parks, Ngorongoro Crater Conservation Area Authority,MinistryofLivestockDevelopmentandFisheries,DepartmentofvectorsandvectorsbornediseasesintheMinistryofHealth,VectorControlTrainingCentreTanga
Challenges to r-HAT control ~ Nocoordinatorsatsubnationallevel
~ Verylimitedfinancialsupporttofacilitateactivities

22 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
~ Shortageofskilledstaff(retiredorinexperienced)
~ OveruseofRDTsdecreasestheutilityofmicroscopy,somedispensariesdonothavemicroscopes
~ Enormousassociatedsocialstigmatization
~ Longdurationofhospitalization
~ Hard-to-reachareas
Future perspectivesLaunchandoperationalizethenationaltsetseandtrypanosomiasiscontrolstrategy
~ HATsurveillanceandcontrolactivitiesplanned
¾ rain laboratory technicians and clinicians in remainingHAT foci (includingnew suspectedareas),inviteDistrictmedicalofficersandsensitizeuseofmicroscopes
¾ Advocatefundingfortsetseandtrypanosomiasiscontroltopolicydecision-makers
¾ Conductentomologicalandepidemiologicalsurveysinnewsuspectedareas(Mbeya,Singida)
¾ Initiateapublicawareness-raisingcampaign,includinginschoolsinHAT-endemicareas
~ Partnershipforimplementation
¾ StrengthencollaborationamongHATstakeholdersundertheOneHealthumbrella
¾ Identifyandappointtsetseandtrypanosomiasisfocalpersonsfromkeyplayersinministries
¾ EstablishamultisectoralAdvisoryCommitteeontsetseandtrypanosomiasis
Inthediscussion,itwasacknowledgedthatmanyvectorcontrolprogrammesusepyrethroidinsecticides.
6.4 Rwanda
Current situationAlthoughnocasesof r-HAThavebeen reported inRwandasince1998,monitoringof thedisease shouldcontinue.Historicaldatademonstratethatthediseasewasoncepresentinthepopulation,8thatthevectorisstillpresentinthecountryandthatneighbouringcountriesstillreportr-HATcases.Figure 6.4.1 shows the distributionofhealthfacilitieswithcapacitytodiagnoser-HATasof2016.
8 ClerinxJ,TaelmanH,BogaertsJ,VervoortT.Treatmentoflatestagerhodesiensetrypanosomiasisusingsuraminandeflornithine:reportofsixcases.TransRSocTropMedHyg.1998;92(4):449–50.
ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 23
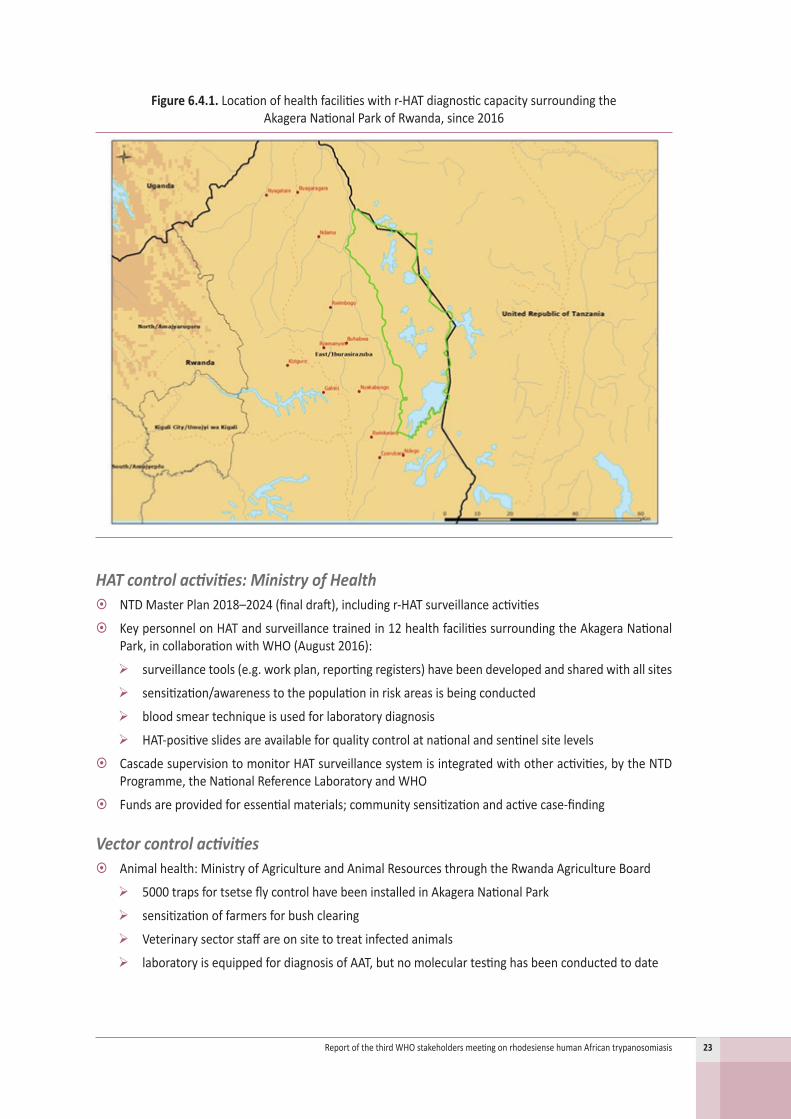
Figure 6.4.1. Locationofhealthfacilitieswithr-HATdiagnosticcapacitysurroundingthe AkageraNationalParkofRwanda,since2016
HAT control activities: Ministry of Health ~ NTDMasterPlan2018–2024(finaldraft),includingr-HATsurveillanceactivities
~ KeypersonnelonHATandsurveillancetrainedin12healthfacilitiessurroundingtheAkageraNationalPark,incollaborationwithWHO(August2016):
¾ surveillancetools(e.g.workplan,reportingregisters)havebeendevelopedandsharedwithallsites
¾ sensitization/awarenesstothepopulationinriskareasisbeingconducted
¾ bloodsmeartechniqueisusedforlaboratorydiagnosis
¾ HAT-positiveslidesareavailableforqualitycontrolatnationalandsentinelsitelevels
~ CascadesupervisiontomonitorHATsurveillancesystemisintegratedwithotheractivities,bytheNTDProgramme,theNationalReferenceLaboratoryandWHO
~ Fundsareprovidedforessentialmaterials;communitysensitizationandactivecase-finding
Vector control activities ~ Animalhealth:MinistryofAgricultureandAnimalResourcesthroughtheRwandaAgricultureBoard
¾ 5000trapsfortsetseflycontrolhavebeeninstalledinAkageraNationalPark
¾ sensitizationoffarmersforbushclearing
¾ Veterinarysectorstaffareonsitetotreatinfectedanimals
¾ laboratoryisequippedfordiagnosisofAAT,butnomoleculartestinghasbeenconductedtodate
24 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
~ Wildlifesector:TheRwandaDevelopmentBoard,throughtheAkageraNationalPark,hasprocuredtrapsfortsetseflycontrol
~ PartnersinHATandfundingfrompartners: apartfromgovernmentalagencies,WHOisthemainpartner
Challenges to r-HAT control ~ Surveillanceactivities:quality controlofhealth centresbyhospitals andofhospitalsby theNationalReference Laboratory not yet systematically conducted. Semester Progress report meetings on HATsurveillanceactivitiesnotregularlyconductedwithin12sentinelsitesandother28surroundinghealthcentres
~ No formal framework for multisectoral coordination to conduct overall evaluation of implementedactivitiesinsurveillanceofAATandHAT
~ Financial:norecentresearchonHATandonvectorandspeciesidentificationofAAT.Operationalcostsforprogressandcoordinationmeetings,mentorship,etc.
~ Humanresources:additionalkeystafffromotherhealthcentressurroundingthe12HATsentinelsitesare not trained
Future perspectives ~ Conductmentorshipsupervisionandlaboratoryqualitycontrol
~ Enhancemonthlyreportingofactivities
~ Createamultisectoralcoordinationframeworkfortrypanosomiasiscontrol(OneHealthapproach)
~ Conductatrainingofotherkeystaffinhealthcentresinat-riskzones
~ Advocatetocreateacommunicationchannelwithneighbouringcountries
~ Advocateforresourcemobilizationforstudiesintrypanosomiasisanditsvectors
~ PrepareavalidationdossierforeliminationofHATasapublichealthproblem
Inthediscussion,itwasacknowledgedthatr-HATappearstohavebeeneliminatedinRwanda.
6.5 Uganda
Current situationThenumbersofreportedcaseshavesignificantlydecreasedinrecentyears,withonly4r-HATcasesreportedin2018(Table 6.5.1).ThemostactivefocuswashistoricallyLango,whichreported3ofthe4casesin2018andwhere Kaberamaido is currently the area of concern. The recent emergence of new reported casesinprotectedareas, albeit in lownumbers, is concerning. Evidence suggests that treatmentof cattlewithinsecticidescontributedtotherapidreductionofr-HATcasesinUganda,althoughadditionalfactorshavenotbeenfullyexplored.
Endemic foci/regions with risk of r-HAT (Figures 6.5.1–6.5.2)Thereare33r-HATendemicdistrictsinUgandainfivemajorfoci,inadditiontoprotectedareas,namely:
~ Ssesefocus/region:LakeVictoriabasin(Kalangala,Mukono,Buvuma,Buikwe,Kayunga)
~ Busogafocus/region(Jinja,Iganga,Mayuge,Luuka,Kaliro,Buyenda,Kamuli,Namutumba)
~ Bukedifocus/region(Tororo,Butaleja,Busia,Namayingo,Paliisa,Kibuku,Budaka,Kibuku)
~ Tesofocus/region(Bukedea,Ngora,Kumi,Serere,Soroti)

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 25
~ Langofocus/region(Dokolo,Kaberamaido,Alebtong,Lira,Kole,Apac,Otuke)
~ Protectedareas(QueenElizabethNationalPark,MurchisonFallsNationalPark)areisolatedfromotherfoci
Figure 6.5.1. Distributionofg-HAT(red)andr-HAT(blue)casesinUganda,2013–2017

26 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Figure 6.5.2. Theriskofg-HAT(red)andr-HAT(blue)inUganda,2012–2016

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 27
Table 6.5.1. Reportedcasesofr-HATbyfocusinUganda,2014–2018
2014 2015 2016 2017 2018KalangalaCasesstage1 0 1 0 0 0Casesstage2 0 0 0 0 0Total detected cases 0 1 0 0 0NamutumbaCasesstage1 0 0 0 0 0Casesstage2 0 0 0 0 0Total detected cases 0 0 0 0 0IgangaCasesstage1 0 0 0 0 0Casesstage2 0 0 0 0 0Total detected cases 0 0 0 0 0KumiCasesstage1 0 0 0 0 0Casesstage2 0 0 0 0 0Total detected cases 0 0 0 0 0BukedeaCasesstage1 0 0 1 0 0Casesstage2 0 0 1 0 0Total detected cases 0 0 2 0 0AlebtongCasesstage1 0 1 2 0 0Casesstage2 0 0 1 0 0Total detected cases 0 1 3 0 0KoleCasesstage1 0 0 0 0 0Casesstage2 0 0 0 0 0Total detected cases 0 0 0 0 0DokoloCasesstage1 10 1 1 0 0Casesstage2 30 6 2 5 1Total detected cases 40 7 3 5 1KaberamaidoCasesstage1 2 6 0 2 1Casesstage2 26 12 2 6 1Total detected cases 28 18 2 8 2LiraCasesstage1 0 0 0 0 0Casesstage2 0 0 0 0 0Total detected cases 0 0 0 0 0Protected areasCasesstage1 2 1 2 0 1Casesstage2 0 0 1 0 0Total detected cases 1 1 3 0 1Total for UgandaCasesstage1 14 10 4 2 2Casesstage2 56 18 6 11 2Total detected cases 70 28 10 13 4

28 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Health facilities capable of diagnosing r-HAT (Figure 6.5.3)The location ofHAT-competent health facilities follows the distribution of historical foci, creating awell-coveredarea:
~ NamungalweHealthCentreIII(Igangadistrict)
~ DokoloHealthCentreIV(Dokolodistrict)
~ SerereHealthCentreIV(Sereredistrict)
~ AlebtongHealthCentreIV(Alebtongdistrict)
~ BudopaHealthCentreIV(Kamulidistrict)
~ LwalaHospital(Kaberamaidodistrict)
~ NsiinzeHealthCentreIV(Namutumbadistrict)
~ BuikweHealthCentreIV(Buikwedistrict)
~ MasafuHospital(Busiadistrict)
~ KitamiroHCIV(Buvumadistrict)
~ KibukuHCIV(Kibukudistrict)
~ MayugeHCIV(Mayugedistrict)
Figure 6.5.3. Locationofhealthfacilitieswithr-HATdiagnosticcapacityinUganda,2016
ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 29
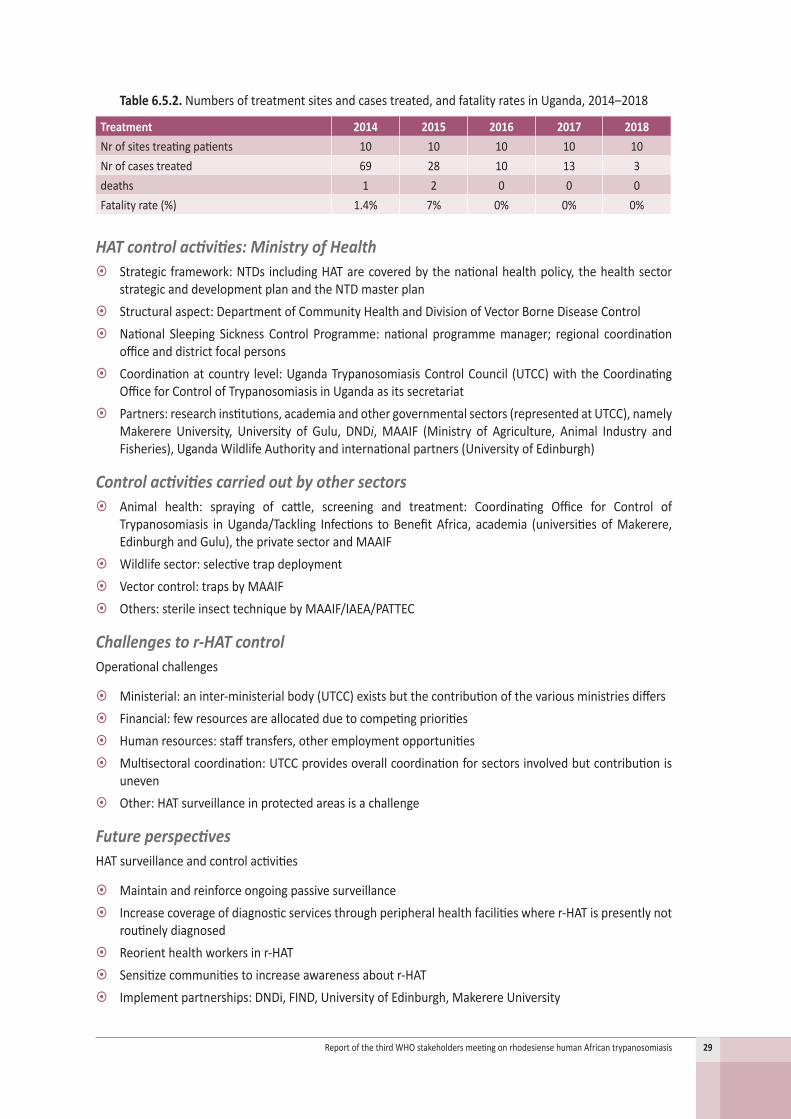
Table 6.5.2. Numbersoftreatmentsitesandcasestreated,andfatalityratesinUganda,2014–2018
Treatment 2014 2015 2016 2017 2018Nrofsitestreatingpatients 10 10 10 10 10Nrofcasestreated 69 28 10 13 3deaths 1 2 0 0 0Fatalityrate(%) 1.4% 7% 0% 0% 0%
HAT control activities: Ministry of Health ~ Strategic framework:NTDs includingHATarecoveredbythenationalhealthpolicy, thehealthsectorstrategicanddevelopmentplanandtheNTDmasterplan
~ Structuralaspect:DepartmentofCommunityHealthandDivisionofVectorBorneDiseaseControl ~ National Sleeping Sickness Control Programme: national programmemanager; regional coordinationofficeanddistrictfocalpersons
~ Coordinationatcountry level:UgandaTrypanosomiasisControlCouncil (UTCC)withtheCoordinatingOfficeforControlofTrypanosomiasisinUgandaasitssecretariat
~ Partners:researchinstitutions,academiaandothergovernmentalsectors(representedatUTCC),namelyMakerere University, University of Gulu, DNDi,MAAIF (Ministry of Agriculture, Animal Industry andFisheries),UgandaWildlifeAuthorityandinternationalpartners(UniversityofEdinburgh)
Control activities carried out by other sectors ~ Animal health: spraying of cattle, screening and treatment: Coordinating Office for Control ofTrypanosomiasis inUganda/Tackling Infections to BenefitAfrica, academia (universities ofMakerere,EdinburghandGulu),theprivatesectorandMAAIF
~ Wildlifesector:selectivetrapdeployment ~ Vectorcontrol:trapsbyMAAIF ~ Others:sterileinsecttechniquebyMAAIF/IAEA/PATTEC
Challenges to r-HAT controlOperationalchallenges
~ Ministerial:aninter-ministerialbody(UTCC)existsbutthecontributionofthevariousministriesdiffers ~ Financial:fewresourcesareallocatedduetocompetingpriorities ~ Humanresources:stafftransfers,otheremploymentopportunities ~ Multisectoralcoordination:UTCCprovidesoverallcoordinationforsectorsinvolvedbutcontributionisuneven
~ Other:HATsurveillanceinprotectedareasisachallenge
Future perspectivesHATsurveillanceandcontrolactivities
~ Maintainandreinforceongoingpassivesurveillance ~ Increasecoverageofdiagnosticservicesthroughperipheralhealthfacilitieswherer-HATispresentlynotroutinelydiagnosed
~ Reorienthealthworkersinr-HAT ~ Sensitizecommunitiestoincreaseawarenessaboutr-HAT ~ Implementpartnerships:DNDi,FIND,UniversityofEdinburgh,MakerereUniversity

30 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
6.6 Zambia
Current situationZambiahasreportedcasesofr-HATsincethe1920sinthreemainfoci,typicallybufferzonesclosetogameparksandprotectedareas(Figure 6.6.1).Atotalof3caseswerereportedin2017and5casesin2018.Thereemergenceofthediseaseinvariousfociisofparticularconcern(Table 6.6.1).
Figure 6.6.1. Distributionofr-HATcasesinZambia,2013–2017
Figure 6.6.2. Theriskofr-HATinZambia,2012–2016

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 31
Table 6.6.1. Reportedcasesofr-HATbyfocusinZambia,2014–2018
2014 2015 2016 2017 2018MpikaCasesstage1 5 2 2Casesstage2 1Total detected cases 6 2 2ChamaCasesstage1 1Casesstage2Total detected cases 1MansaCasesstage1 1 1Casesstage2Total detected cases 1 1NyimbaCasesstage1 1Casesstage2Total detected cases 1LuanoCasesstage1 1Casesstage2Total detected cases 1MambweCasesstage1 1 1Casesstage2Total detected cases 1 1MbalaCasesstage1 1Casesstage2Total detected cases 1RufunsaCasesstage1 4Casesstage2Total detected cases 4UTHCasesstage1 2Casesstage2Total detected cases 2LundaziCasesstage1 1Casesstage2Total detected cases 1ZambiaCasesstage1 9 5 2 3 5Casesstage2 1Total detected cases 10 5 2 3 5

32 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Table 6.6.2. Numbersoftreatmentsitesandcasestreated,andfatalityratesinZambia,2014–2018
Treatment 2014 2015 2016 2017 2018Nrofsitestreatingpatients 2 3 1 1 3Nrofcasestreated 10 5 2 3 3deaths 1Fatalityrate(%) 10%
HAT control activities: Ministry of HealthNationalSleepingSicknessControlProgramme:
~ UndertheCommunicablediseasesunitintheMinistryofHealth,dealingwithNTDs
~ FocalpointpersoninchargeofNTDs
~ NationalCoordinatorappointedbythePermanentSecretaryoftheMinistryofHealth
PartnersinHATcontrol:WHO
Multisectoral organization and coordination ~ Ministry ofHealth andUniversity of Zambia, School ofVeterinaryMedicine, in evaluating the LAMP(loop-mediatedisothermalamplification)testproject
~ OneHealthconcept(MinistryofHealthandSchoolofVeterinaryMedicine)
Vector control activities ~ AerialsprayingofinsecticidesinWesternregionandinsecticide-treatedtargetsinnationalparks
~ Responsible institutions:Ministry of Livestock and ZambiaWildlifeAuthority, PanAfrican Tsetse andTrypanosomiasisEradicationCampaign(PATTEC)/GovernmentofZambia.
Challenges to r-HAT control ~ Frequentchangesinfocalpointpersons
~ Drugdistributionsystem
~ Budgetaryconstraints,dependencyonWHO
~ Frequenttransferoftrainedlaboratorytechnologistsinendemicareas
~ Weakmultisectoralcoordination
~ Lackofqualitycontrol for r-HAT laboratorydiagnosis, lackof regular refreshercourses for laboratorytechnologistsandlackofmoresensitivelaboratorydiagnostictechniquessuchasWoo’smethod(onlyavailableinonehospital)
Future perspectives ~ Cross-bordercollaborationmeetingwithMalawiandZimbabwe(MinistryofHealthfocalpointpersonsandWHOcountryoffices)
~ SensitizationworkshopforDistrictMedicalOfficersfromr-HATendemicdistricts
~ DevelopmentofIEC(information,education,communication)materials
~ Refreshercourseforlaboratorytechnologists,pharmacistsandclinicians
~ Establishqualitycontrolforlaboratorydiagnosisofr-HAT

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 33
~ Annualsupervisoryvisitstohospitalsinendemicareas
~ Restockingofmelarsoprol
~ Communitysensitizationaboutr-HATthroughradiobroadcasts
6.7 Zimbabwe
Current situationr-HATislimitedtooneareaintheZambeziValley(Figures 6.7.1–6.7.2).Since2000,veryfewcaseshavebeenreported,but in2012some9caseswerereported forunknownreasons. In2017,3caseswerereportedwhereasin2018therewerenocases(Table 6.7.1).Historically,caseshavebeenassociatedwithproximitytotheZambeziRiverandwildlife,makingtheinterfacebetweenwildlifeandhumansamajorconcernforriskofr-HAT.Thisisespeciallyimportantastheareaisusedforsafarihuntinggroupsandhostsvisitorstonationalparks.Tsetsefliesarepresentinanareaof20000km2inthenorthernpartofthecountry,andstudiesoftheirdistributionshowapatternthatcloselymatchesthedistributionofcases.Generally,diagnosticcapacityremainspoor inhealth-care facilities,especially in theaffectedarea. Furthermore, there isno treatmentfacilityforr-HATinthefocusarea;casesaretreatedinZambiaorinhospitalsinthecapitalcity.MedicinesareonlydispensedinonepharmacyinHarare(whichis>200kmawayfromendemicareas).Awell-establishedtsetsecontroldivisionisinvolvedinvectorcontrolthroughvariousmethods.
Figure 6.7.1. Distributionofr-HATcasesreportedinZimbabwe,2013–2017

34 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Figure 6.7.2. Theriskofr-HATinZimbabwe,2012–2016
Table 6.7.1. Reportedcasesofr-HATbyfocusinZimbabwe,2014–2018
2014 2015 2016 2017 2018MakutifocusCasesstage1 2 3 1 2 0Casesstage2 1 0 0 1 0Total detected cases 3 3 1 3 0
HAT control activities: Ministry of HealthNationalSleepingSicknessControlProgramme:
~ UnderthecommunicablediseasesunitintheMinistryofHealth,dealingwithNTDs
~ FocalpointpersoninchargeofNTDs
~ NationalCoordinatorappointedbythePermanentSecretaryoftheMinistryofHealth
PartnersinHATcontrol:WHO
Multisectoral organization and coordination ~ TheDirectorateofEpidemiologyandDiseaseControlhousestheNTDsunit
~ Close, sustained collaboration with veterinary services in the Ministry of Agriculture (One Health,integratedvectorcontrol)
~ PrivatephysicianandpharmacistconductingcasemanagementinHararewithsupportfromWHOforsupply(medicinesaredistributedfreeofcharge)
~ TheNationalHealthStrategy2016–2020andtheNationalNTDStrategy2012–2016addressNTDs

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 35
Control activities carried out by other sectors ~ Animalhealth:dippingof livestockusingdeltamethrin,surveillanceandcontrolofAAT inaccordancewiththeProgressiveControlPathway
~ Vectorcontrolinterventions
Vector control activitiesMethodsused:
~ TsetsesurveysusingMan-screenfly-roundsandtraps
~ Odour-baitedinsecticide-treatedtargetsandinsecticide-treatedcattle
~ Groundspraying(2012–2013)
~ Sterileinsecttechnique:entomologicalbaselinedatacollection,dronereleasefeasibilitytrial
Areas/regionscovered
~ MolaareaadjacenttoMatusadonaNationalPark,north-westZimbabwe;sterileinsecttechniqueprojectto be implemented in 1200 km2ofthenationalpark.
~ MakutiHATfocusarea(northerndistrict)
Responsibleinstitutions:DivisionofTsetseControlServices–DepartmentofVeterinaryServices(MinistryofLandsAgriculture,Water,ClimateandRuralResettlement)
Challenges to r-HAT control ~ Lowlevelofawarenessamongmanagement,professionalsandcommunitiesaboutHAT
~ HATprevention,control,managementiscurrentlynotprioritized
~ NodedicatedresourcesareavailableforHAT
~ Notrainingprogrammeandhencenocapacitytodetect,confirmandtreatHATcases
~ The supply of antitrypanosomal medicines by WHO is appreciated, but access is limited throughcentralization
~ Poorsurveillanceforearlydetectionandreportingofcases
~ Nocasemanagementguidelines
Future perspectives ~ EstablishaNationalSleepingSicknessControlProgrammewithintheNTDTaskforce
~ Mapthedistributionofallpartnerswithcapacitytocontrol,detectandmanager-HATinthecountry
~ StrengthentherapiddiseasenotificationsystemforHATsurveillance,managementandcontrolactivities
~ Developajointreportingplatformwithveterinaryservices
~ Re-mapthegeographicalareaofriskbasedonvector,parasiteandhumancasestobettertargetcontroltowardselimination.

36 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
7. EliminationofrhodesienseHATaspublichealthproblemin2020
7.1 Human African Trypanosomiasis Elimination Technical Advisory Group
TheHATeliminationTechnicalAdvisoryGroup(HAT-e-TAG)wasestablishedin2016toassistWHOindefiningthecriteriaandproceduresforthevalidationandverificationofHATelimination.Thetargetfor2020(i.e.eliminationasapublichealthproblem)mustbevalidated.Thetargetfor2030(i.e.zerotransmissionofg-HAT)mustbeverified.Forthat,thestatusofHATeliminationincountriesmustbeassessedagainstobjectivecriteriaandtheachievementformallyrecorded.HAT-e-TAGreviewstheindicatorstoassesstheachievementofHATelimination,devisestemplatesfornationaldossiersonvalidation/verificationandestablishestheprocedurestoreviewthenationaldossiers.Italsodefinestheproceduresforpost-eliminationsurveillanceandrevisesthenationalstatus.Theprocessisperiodicallyreviewed,accordingtoscientificadvancesandtools.
HAT-e-TAGcomprisessevenmembers,withoutconflictof interests,whoareappointedfor2yearsonthebasisoftheirpersonal(notinstitutional)expertise,andsixadvisorswhorepresenttheirorganizations.Theadvisorsdonotparticipateinfinaldecisions.MeetingsareheldannuallyattheinvitationofWHO.
ThefirstHAT-e-TAGmeeting(Geneva,23–25November2016)refinedthetarget/indicatorsforeliminationofHATasapublichealthproblem.Theglobaltargetwasoriginallydefinedas:<1newreportedcase/10000inhabitantsperyearinatleast90%offoci,with<2000reportedcasesperyearatcontinentallevel.Asfociarenotobjectivelymeasurable,andastheareaatriskofHATcanbebettermeasuredinastandardizedway,HAT-e-TAGrefinedthetargetfor2020as:a90%reductionoftheareaatriskreporting≥1case/10000peopleperyear.Theprimaryindicatorsarethusthenumberofcases(asbefore)andtheareaatriskreporting≥1case/10000peopleperyear.ThisnewindicatorwasendorsedbytheWHOStrategicandTechnicalAdvisoryGroup forNeglectedTropicalDiseases at its tenthmeeting (Geneva, 29–30March2017) and is now theofficialmetric.The90%reductionreferstoabaselineoftheareaatriskcalculatedoverthe2000–2004time-period.Thesecondaryindicators(asbefore)aregeographicaldistributionofHAT,levelofriskofpopulation,andcoverageofsurveillanceandcontrol.
Thenewdefinitionoftheindicatorandtargetisappropriateatthegloballevel.However,HAT-e-TAGadvisedthat this particular indicator should not be established at a national level because it requires advancedexpertiseingeographical informationsystemsandsoftware,whichnationalprogrammesoftenlack.Asanoutcome of the second HAT-e-TAGmeeting (Geneva, 26–28 April 2017), national-level indicators of HATeliminationasapublichealthproblemweredefined(seesection7.4).
Forthevalidationofg-HATelimination,atemplatefornationaldossierswasdeveloped.AfirstvalidationdossiersubmittedbyTogoandadraftdossiersubmittedbyCameroonwereusedtoassesstheappropriatenessofthetemplateandtobuildtheassessmentcriteriaduringthethirdHAT-e-TAGmeetingin2018.Thesurveillanceplanforthepost-validationphase(chapter7ofthedossier)isespeciallyimportant.Furthermore,thecountryvalidationdossier for g-HATwas adapted for r-HATandafirst versionwas submitted to thismeeting fordiscussion(seesection7.2).
ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 37
7.2 Country dossier for validationThe validation dossier documents the achievement of elimination of HAT as a public health problem byprovidingtheinformationandrequirementstodemonstratetheabsenceof(orlowlevelof)transmission.Thekeyelementsofthedossieraretoassurethepresenceofafunctionalsurveillancesystemcapableofdetectingpossiblecases.Theversionofthedossieradaptedforr-HAThaseightchapters:
1. Description of the country and its capabilities
1.1 Generalinformationaboutthecountry• Geographical,demographic,economic• Tourismactivitiesinprotectedareas
1.2 Thecountry’shealthsystem• Basicdescription,structures,capabilities• Utilization,attendancerates
2. Historical data and description of endemic areas
2.1 HistoricalHATdata(essential)• Distributionoffoci,controlactivities• Casesperyear,atleastsincethe1960s
2.2 Description/demarcationofcurrentendemicareas(essential)• Howthecountrydefinesendemicareas• Grayareas(potential,butnoinformation)• Annualnumberofvisitors
3. HAT surveillance and control activities
3.1 StructureandcapabilitiestocombatHAT(essential)
3.2 Activescreeningstrategy
3.3 Passivescreeningstrategy(essential)
3.4 Responsetosuspected/confirmedcases(essential)• Concreteactionstaken
3.5 AnalysisSWOT
4. HAT epidemiological data
4.1 Currentdata,nationallevel(essential)
4.2 Dataforthepast5years,byhealthdistrict(essential)• HATcases(S1/S2),malariatesting(bloodsmear/RDT)
4.3 Datafollowingthenationalindicatorofelimination(essential)
4.4 HATinneighbouringcountries
5. Vector control
5.1 Vectorcontrolstrategy• Approach,protocols/toolsandmethodsforevaluatingresults• Time-period,spatialcoverageinrelationtothepresenceofthedisease
5.2 VectorcontrollinkedtoHAT,results
38 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
• Tsetsedistributionmaps,ifpossiblebyspecies• Tsetsedensitydata,trackedovertime• Proportionoffliesinfectedwithtrypanosomespathogenicforhumans
6. Interventions regarding animals
6.1 Data on AAT• Farmingsystems,presenceofTrypanosoma bruceiinanimals,livestockdensity
6.2 CapabilitiestocombatAAT• Actors,methods,coverage,linkswiththehealthsector
6.3 ActivitiesforOneHealth• AnimalinterventionstrategiesforHATcontrol• Linkswiththehealthsector• Partners
7. Plan of post-validation surveillance (essential)
7.1 Eliminationstatusmustbemonitored• Surveillanceandresponseactivities
7.2 Planofsurveillanceforthenext5years• Resourcesavailable,partnersinvolved
7.3 Tomaintaintheacquiredstatus
7.4 Movetowardstheeliminationofthetransmission
8. References and annexes
The dossier allows health ministries to formally submit to WHO the claim of HAT elimination and thesupportingdata.AtemplateisavailableinFrenchandEnglish.Eligiblecountriesareencouragedtoapplyforvalidationandareinvitedalsotoprovideconstructivefeedbacksoastoimprovetheprocess.
7.3 Validation processAnad-hocreviewingvalidationteamwillbeconstitutedtoevaluatethecompleteness,accuracyandreliabilityofagivencountrydossier.TheteamascertainsthelikelihoodthatHATisnolongerapublichealthproblemin thecountry, that the indicatorsestablished for thispurposearemet,and that the surveillance systemproposedisadequateandabletodetectanyre-emergenceofthediseasebeforereachingepidemiclevels.Theteamof1–2expertsisidentifiedfromapanelofexpertsselectedbytheWHORegionalOfficeforAfricaplus1–2expertsfromHATe-TAGandmembersoftheWHOsecretariat(WHORegionalOfficeforAfricaandWHODepartmentofControlofNeglectedTropicalDiseases).Followingthetemplate,eachteammemberpreparesareportthatwillbeshared.TheWHOsecretariatcoordinatestheprocessandpreparesthefinalreport,whichisagreedon.ThefinalreportisalsosubmittedtotheWHORegionalOfficeforreviewAfricaand, ifagreed,endorsedbytheRegionalDirector.Finally, theWHODirector-General formallynotifiestheMinistryofHealth inwriting,andthe information ispublished in theWeeklyEpidemiologicalRecordandtheGlobalHealthObservatory.Areassessmentisforeseenafter5years.Figure 7.3.1showsthepathwayforvalidation.

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 39
Figure 7.3.1. PathwayforvalidationofHATelimination
AFRO,WHORegionalOfficeforAfrica;HQ,headquarters;MoH,MinistryofHealth;PHP,publichealthproblem;SOP,standardoperatingprocedure
Inthediscussion,itwasproposedthattheexperiencesgainedandtheproceduresestablishedforvalidationbe published to serve as an example of good practice for other diseases to follow on the path towardselimination.
7.4 National indicators – country statusThe global targetforeliminationofHATasapublichealthproblemby2020isdefinedasfollows:
~ <2000casesreportedannuallyatcontinentallevel
~ 90%reductionofthetotalareaatriskreporting≥1case/10000peopleperyear(from2004baselinelevels)
Theglobaltargetandtheindicatorsarenotdirectlyapplicableatcountrylevel;theymustbeadaptedinasimpleandeasilymeasurablewaytothenationalcontext.
The target at country levelfortheeliminationofHATasapublichealthproblemby2020wasdefinedbyHAT-e-TAGasfollows:
~ <1case/10000peopleinallhealthdistrictsofthecountryduringthepreviousfive-yearperiod
A health district is the internationally accepted health administrative and operational division (healthmeasuresimplementationunit).Thisgeographicalareaincludesallcomponentsofahealthsystemrequiredtodelivercommunityhealthcare.
Tocalculatethenationalindicators,thenumeratoristhemeannumberofcasesreportedannuallyfortheprevious5yearsinadistrict.Casesarenotifiedbythenationalsleepingsicknesscontrolprogrammeinthehealthdistrictaccordingtothenationalcasedefinition.The5-yearperiodsmoothsanyvariationsofcoverageandreportingfromoneyeartoanother.
40 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Thedenominatoristhepopulationofthehealthdistrictatthemid-yearperiod.Thesourcesforestimatingthehealthdistrictpopulationcouldvary(census,datacollectedbythenationalprogrammeorbythehealthsystem,datafromgeospatialdatasets,etc.)andthereforethesourceshouldbespecifiedinthereporting.
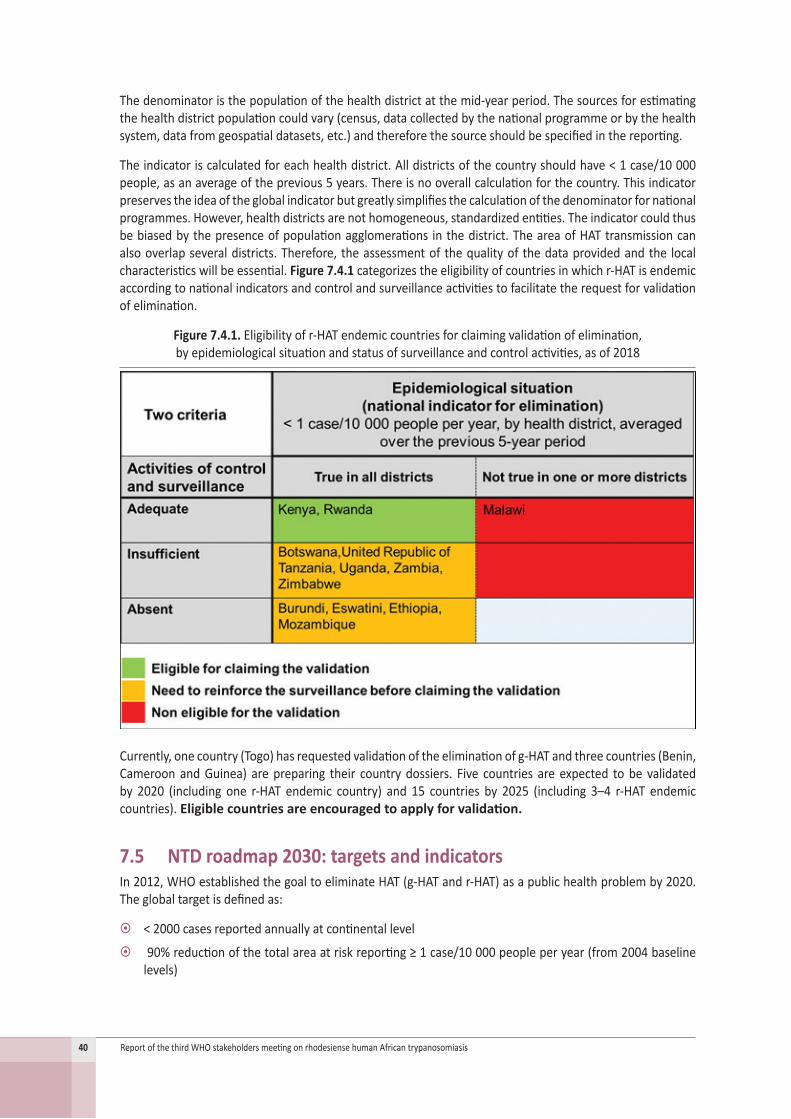
Theindicatoriscalculatedforeachhealthdistrict.Alldistrictsofthecountryshouldhave<1case/10000people,asanaverageoftheprevious5years.Thereisnooverallcalculationforthecountry.Thisindicatorpreservestheideaoftheglobalindicatorbutgreatlysimplifiesthecalculationofthedenominatorfornationalprogrammes.However,healthdistrictsarenothomogeneous,standardizedentities.Theindicatorcouldthusbebiasedbythepresenceofpopulationagglomerations inthedistrict.TheareaofHATtransmissioncanalsooverlapseveraldistricts.Therefore, theassessmentof thequalityof thedataprovidedandthe localcharacteristicswillbeessential.Figure 7.4.1categorizestheeligibilityofcountries inwhichr-HATisendemicaccordingtonationalindicatorsandcontrolandsurveillanceactivitiestofacilitatetherequestforvalidationofelimination.
Figure 7.4.1. Eligibilityofr-HATendemiccountriesforclaimingvalidationofelimination, byepidemiologicalsituationandstatusofsurveillanceandcontrolactivities,asof2018
Currently,onecountry(Togo)hasrequestedvalidationoftheeliminationofg-HATandthreecountries(Benin,Cameroon andGuinea) arepreparing their country dossiers. Five countries are expected tobe validatedby 2020 (including one r-HAT endemic country) and 15 countries by 2025 (including 3–4 r-HAT endemiccountries). Eligible countries are encouraged to apply for validation.
7.5 NTD roadmap 2030: targets and indicatorsIn2012,WHOestablishedthegoaltoeliminateHAT(g-HATandr-HAT)asapublichealthproblemby2020.Theglobaltargetisdefinedas:
~ <2000casesreportedannuallyatcontinentallevel
~ 90%reductionofthetotalareaatriskreporting≥1case/10000peopleperyear(from2004baselinelevels)

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 41
Beyondthat,thegoalsforeliminationofg-HATandr-HATby2030differasfollows:
~ Tointerrupttransmission(sustainableelimination)ofg-HATby2030
¾ Indicator:casesofg-HATdeclaredperyear
¾ Target:zerocasesby2030
~ Tomaintaineliminationofr-HATasapublichealthproblemby2030
¾ Indicator:areaendemicforr-HATreporting≥1case/10000peopleperyear
¾ Target:noareaendemicforr-HATreporting≥1case/10000peopleperyearby2030
Thereliabilityoftheindicatorsisstronglydependentonthecapacitytodetectcases,andunderreportingisaspecialconcernforr-HAT.
Whenmeasuringprogresstowardseliminationofr-HATasapublichealthproblem,milestonesshouldbedefined(e.g.2023,2025,2027)anddifferentindicatorsandtargetsconsidered,namely:
~ Number of r-HAT cases reported.Thisindicatorhasbeenuseduntilnow.Itisexpectedthatthenumberofcaseswilldecrease,butitisdifficulttodefineafigureasatargetandmilestones.In2030,thenumberofcasesofr-HATshouldbesporadic.
~ Areas of high or moderate risk (reporting ≥ 1 case/10 000 people per year).Theseareasareexpectedtodecreaseto0in2030andmilestonesshouldbedefined.
~ A secondary indicator is required to indicate the expected improvement inaccess to diagnosis and treatment for people at risk,namely:
¾ theat-riskpopulationlivingwithin1hour’stravelofacompetentfacility(underdiscussion)
¾ theat-riskpopulationlivingwithin5hours’travelofacompetentfacility(underdiscussion)
¾ theproportionofHATcasesreceivingappropriatetreatment(>99%)
~ Asaprocessindicator,acertainnumberofcountries should be validated progressively for elimination of HAT as a public health problem:
¾ In2021:atleastfivecountries
¾ In2025:atleast15countries(3–4r-HAT)
ThesetargetsareincludedintheframeworkofthenewNTDroadmap(2021–2030).Goal3.3oftheUnitedNationsSustainableDevelopmentGoals is,by2030,“toend theepidemicsofAIDS, tuberculosis,malariaand neglected tropical diseases [including HAT] and combat hepatitis, water-borne diseases and othercommunicablediseases”.Theglobal target forNTDs is,by2030,toreduceby90%thenumberofpeoplerequiring interventionsagainstNTDs.During2019,WHOwilladopt indicatorsandtargets for2030forallNTDsandpublishthemin2020aspartofthenewNTDroadmap.

42 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
8. Strategiesforeliminationof rhodesiense HAT
8.1 Overview of elimination effortsThelife-cycleofr-HATismostlyzoonotic,involvingbothdomesticandwildanimalsasthemainreservoirsoftheparasiteandofthevector Glossinaspp.,commonlyknownasthetsetsefly.Occasionally,humansacquiretheinfectionasaccidentalhosts,whichalthougharelativelyrareeventprovokessevereillness,deteriorationanddeathunlesscasesarediagnosedandtreatedpromptly.Asthelife-cycleofr-HATinvolvesmanyhosts,multipleinterventionsareavailabletargetingdifferentpartsoftheparasitelife-cycle(Figure 8.1.1).
Figure 8.1.1. Life-cycleofr-HATandmethodsofinterventiontargetingdifferentstagesofthedisease
Numeroussectorsareinvolvedinr-HATcontrolbeyondhumanhealth–suchasveterinaryservices,vectorcontrol,tourismandmanagementservicesofprotectedareasaswellaswildlife–allofwhichcontributetoaOneHealthapproach.Eachsectorleadsspecificactivities,whichdifferbycountry,butallsectorscanandshouldactivelycollaborateintheirrespectivefieldsinsurveillanceandIECactivities.Involvementfromlocalauthoritiesisalsoneeded.
Themethodsused to control the vector include tsetse screens and traps, the sterilized insect technique(release of sterile tsetsemales), insecticide impregnated net fencing and large-scale insecticide spraying(groundoraerial).Personalprotectionmethodssuchasuseofinsectrepellentsandminimizingskinexposurearealsopromotedforpopulationsthatmaybeatrisk.

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 43
Approachestor-HATcontrolmayvarybasedonthepresenceofwildlifereservoirsversuscattlereservoirs,forwhichdifferentmonitoringandcontrolmethodsarerequired.Activescreeningisrarelyapplicableforareasinwhichwildanimalsarethemainreservoir,butpassivescreeningcanbeeffective.Protectedareasandparksareavitalsourceofincomeforcountriesandshouldberecognizedashighprioritiesforsurveillancebypolicy-makers.IncorporatingthisOneHealthapproachisimportantecologicallyandforlocalworkers,whoareconstantlyexposed.
Forareasinwhichcattlearethemainreservoir,activeandpassivescreeningisthemethodused.TreatmentofcattleasapreventiveorcurativemeasureisseentocontributesignificantlytotheeliminationofHATand,additionally,protectscattleagainstotherinfections.Treatmentincludessprayingthelegsandbellyofcattlewithinsecticide(restrictedapplicationprotocol).
InterventionsonhumansisthesectorcoveredbyWHOandincludediagnosisofhumancases(case-finding)and treatment. If a surveillance system is in place,WHO can produce pertinent information on diseasedistributionthathelpstotargetinterventionsmoreeffectivelyinallsectors.DatacollectedbythecountryandsubmittedtoWHOareverifiedandenteredintotheAtlasofHAT,whichismadeavailabletocountriesandpartnersonrequest.Itwasnotedthatcountry-levelriskassessmentsshouldtakeintoconsiderationallcomponentsofepidemiologicalinformation,whichcouldhelptowardsachievingthegoalofeliminationandsustainedsurveillance.Forexample,countriesshouldensurethathealth-carefacilitiesrecordthelocationoflikelytransmission,asthisismoreinformativethanthepatient’shometown.Theyshouldalsoensurethatexportedcasesare included in thecountry reports.This isespecially importantnowthat the intensityoftransmissionisreduced.
WHO offers training on diagnostics for clinical and laboratory staff, provides equipment and materials(including treatment) to national programmes and supports the supervision of health facilities offeringHATservices (e.g. refreshingawarenessperiodically,providingadvicewhenrequested).AntitrypanosomalmedicinesaredonatedfreeofchargethankstothepartnershipestablishedwithSanofiandBayerforthepast18years.WHOisresponsibleforforecastingtheamountsneededandwheretheyneedtobeallocated,andprovidesguidanceonhowthesupplyshouldbeusedeffectivelyandbeforeexpiry.
WHOisresponsiblealsoforadvocatingcontinuedsupportfromnationalauthorities,internationalactorsandthescientificcommunity,especiallyastheincidenceofthediseasedeclinesandthushaslimitedappealandawarenesstomany.Raisingawarenessofthediseasealsoappliestoexposedpopulationsandhealth-careworkers.
Whilepromotingtheeliminationofr-HATiscertainlywithinWHO’sremit,itsscopeofactionislimitedtothehumanhealthsector.TheOrganization’sstrengthliesinitsconveningpowerandabilitytocoordinatenationalandinternationalactors,devisecommonstrategiesandplanactivities.Toeliminatethedisease,interactionbetweennationalhealthworkersandveterinaryscientistsmustbestimulated,astheywillberesponsibleforeliminatingthediseasefromtheanimalreservoir.Attheinternationallevel,WHOiscollaboratingwithrelevantorganizations,namelyFAO(theFoodandAgricultureOrganizationoftheUnitedNations),IAEAandOIE(theWorldOrganisationforAnimalHealth).Consolidatingthisinteractionwillbecrucialtoachievingtheeliminationgoal.
8.2 Strategies for elimination: case-findingThemostimportantdecisionforsuccessfulcase-findingisthechoiceofsurveillancesites.Siteselectionistheresponsibilityofthenationalprogrammecoordinator.Surveillancesitesneedtobenearareasoftransmissionandbewellattendedandsufficientlystaffed(alwaysconsiderexistingfacilitiesfirst),withlaboratoryfacilitiespresentandexperiencedstaffandaccessibility/communicationwiththecentral level.CountrieshavesentWHOanexhaustivelistofhealthfacilitiesthatconductclinicaldiagnosis,parasitologicaldiagnosisanddiseasestagingforr-HAT.Thislistwillbeupdatedregularlytotrackchanges,asitisusefulformanagementaswellasformappingthehealthcoverageofendemicareas.
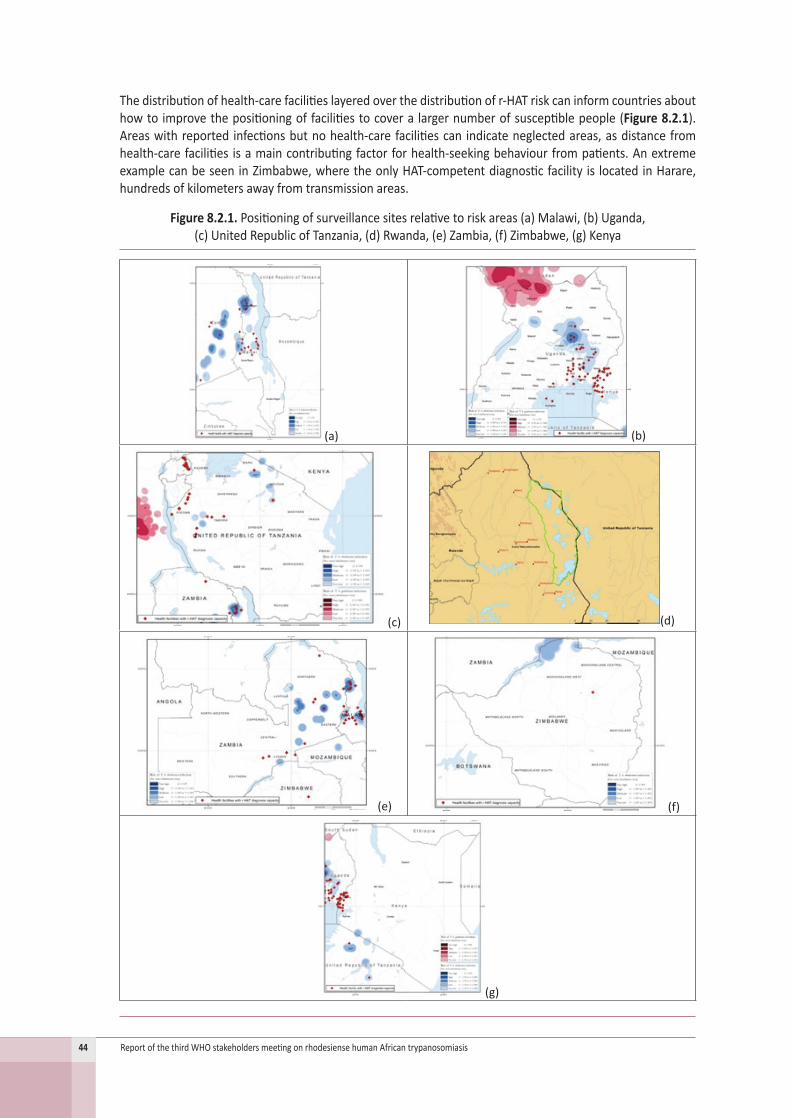
44 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Thedistributionofhealth-carefacilitieslayeredoverthedistributionofr-HATriskcaninformcountriesabouthowto improvethepositioningoffacilitiestocovera largernumberofsusceptiblepeople(Figure 8.2.1).Areaswithreported infectionsbutnohealth-carefacilitiescan indicateneglectedareas,asdistancefromhealth-carefacilities isamaincontributingfactorforhealth-seekingbehaviourfrompatients.AnextremeexamplecanbeseeninZimbabwe,wheretheonlyHAT-competentdiagnosticfacility is locatedinHarare,hundredsofkilometersawayfromtransmissionareas.
Figure 8.2.1. Positioningofsurveillancesitesrelativetoriskareas(a)Malawi,(b)Uganda, (c)UnitedRepublicofTanzania,(d)Rwanda,(e)Zambia,(f)Zimbabwe,(g)Kenya
(a) (b)
(c) (d)
(e) (f)
(g)

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 45
Otherwaysofimprovingcase-findingincludetrainingclinicalstafftobetterrecognizethesignsandsymptomsofr-HAT,withtheuseofsupporttoolssuchaspostersorinformationsheets.Achecklistoffrequentsymptomscanaidclinicalstaffindiagnosingr-HATandhelptohighlightitspresenceinendemicareas.Cascadetrainingforperipheralhealthfacilitiesisawayofbuildingcapacityandcost–effectivelyspreadingknowledgeofthediseaseoutwardsfromsentinelsites.Itisimportanttoexaminehowhealthsystemsworkineachcountry,aseachcountryhasitsownneeds.Decisionsaboutdiagnostictestingrelyontheclinician,soawarenesseffortsandguidanceshouldtargetclinicians.Improvingawarenessofr-HATamongtraditionalhealerscouldalsobebeneficialforsupportingearlyreferraltohealthfacilities.
Training laboratorystaffcanalso improvecase-finding.Forexample,each localnetworkcouldbegivenacustomizeddecision treeofavailablediagnosticmethods, ranging fromsimple tocomplex, inadditiontoposters and information sheets on r-HAT.Often, diagnostics are unavailable due to a lack of equipment,whichshouldbereviewedandreinforcedbythenationalprogrammewhereneeded.Microscopyslidesoflaboratory examinations should be saved for quality control and competency assessment, togetherwithsamples/images/videos of trypanosomes that can be used to refresh staff knowledge and be passed ontonewstaff.Regularsupervision isneededforqualitycontrolandmotivationofstaff. Itwasnotedthatasupervisor’schecklistcouldbeuseful(alreadydevelopedforg-HAT).
Active screening for r-HAT is usually reactive rather than prospective. It targets the family and village oftheinfectedpersonandshouldbedoneimmediately.Currently,activescreeningisbasedonparasitologicalscreeningofaselectedpopulation.Datacollectiononthenumberofsuspected,testedandconfirmedcasescouldhelp inmonitoring trends in the incidenceof thedisease.Aquestionnaire hasbeen introduced insomecountriestargetedatreferringdoctors,relatingtothedetailsofsuspectedcases(patienthistory,travel,activities).
8.3 Strategies for elimination: treatmentTreatmentforr-HATmustberapidandreadilyavailable.Themedicines,availablefreeofcharge,mustbeorderedintimeandthesuppliesmustbeappropriatelymanagedbythenationalprogrammes.WHOprovidesguidanceandtechnicalsupportonmanagingsupplyandhasalsomappedhealth-carefacilitieswhichprovidetreatment,basedondatasubmittedbycountries.Thisinformationisallfedbacktonationalfocalpointsandsummarydataareavailableonline.
8.4 Strategies for elimination: epidemiological surveillanceSurveillanceofr-HATstartswithcollection,validationandconsolidationofdatabythenationalcoordinator,whopreparesthereportsforpartners includingWHO.ThesedataareincludedintheglobalHATAtlasbyWHOinaprocessthatinvolveschecksforcoherenceandconsistency.Anyverificationqueriesaresenttocountrycoordinatorsinordertomaximizedatavalidity.
EmphasisisgiventoestablishingandreportingthemostprobableplaceofinfectionofallHATcases,asthisinformationhasimportantepidemiologicalvalue.Allcasesdiagnosedinnon-endemiccountries(i.e.exportedcases)areincludedandmappedattheirmostprobableplaceofinfection,andthenationalfocalpointsareinformedaccordingly.
Surveillancedataareessential forplanning control andeliminationofHAT. Forexample, themappingoftransmissionareasbystratifiedlevelsofriskallowsthebestlocationofsentinelsitesandidentificationofareasthatarenotwellcovered.
CountrieshavecontributedsignificantlytothedevelopmentandupdatingoftheHATAtlasandhaveexpressedtheirinterestinusingthetoolatcountrylevel.CountrieshaveundergonetrainingandbeenprovidedwithequipmentandsoftwaretousetheAtlasfortheirbenefit.

46 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
8.4 Strategies for elimination: IEC (information, education, communication)
TheIECstrategyaimstoincreaseawarenessofr-HATamong:(i)exposedpopulations(i.e.onwheretoseekhealthcareandwhatprotectivemeasurestouse);(ii)health-careworkersaroundsentinelsites,toremainawareof r-HATasapossiblediagnosisandprovide informationtopatientsbeingreferred; (iii) traditionalhealers,astheyareoftenthefirstpeoplepatientsseekhelpfromandmustthereforebeincludedinapositivewaytoencouragepromptreferralofpatientspresentingHAT-compatiblesymptoms.
Thereisapotentialrolefortheprivatesectorinthisstrategy.Hotelsandparkshavealargestakeinprotectingtheiranimals,theirstaffandtheirvisitors,andhavetheresourcestopromotebetterawarenessofr-HAT.Iftransmissionareasincludenationalparks,messagingshouldberetargetedtothoseareasthattouristsmayvisitandhotelstaffmayfrequent.Astechnologyadvances,anthropologicalsurveyshavedemonstratedthatthecommunicationchannels thatpeopleusecurrentlyareverydifferent frompastmethods,e.g.mobiledevices.Suggestionsincludedasocialmediacampaignonthedangersofr-HATandprotectivemeasures,ortrainingprogrammesonprotectivemeasuresforhotelstaff.
There isalsoaneedtodelineatebetweenmessagingregardingprotectionof livestock (whichwasaverysuccessfulcampaign)andmessagingregardingwildlifereservoirsbecausethepopulationsatriskhaveverydifferent demographics (local residents versus tourists, respectively). Tourists aremore likely to travel tolargerhealth-carefacilitiessuchashospitals forearlydiagnosis,whereas localresidentsmayhave limitedaccesstohealthcareandsomessagingshouldfocusonthem.
8.6 Strategies for elimination: coordinationTheHATeliminationnetworkcoordinates theeffortsofawide rangeof stakeholdersagainstHAT (Figure 8.6.1). Its role is toconvenepartners inorder to identifygaps incontroleffortsand todevelopcommonstrategies forelimination.National coordinationbodiesarevery importantmembersof thenetwork thatevaluateprogressandplanactivitieswithintheendemiccountries.
Figure 8.6.1. TheHATeliminationnetwork
In the discussion, the importance of socio-anthropological aspects of r-HAT at the community level wasrecognized, including for theearlierdetectionof cases. Itwas recommended that this subject shouldbeaddressed.

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 47
9. Clinicalmanagementof importedeastAfrican trypanosomiasisin SouthAfrica:lessonslearnt
SouthAfricaisnotendemicforr-HAT,butcasesareregularlyimportedbymedicalevacuationflightsfromsouthandeastAfricancountries.Withmorethan60patientstreatedforr-HATinthepast18years,importantlessonsaboutclinicalmanagementcouldbelearnt.9Theexperiencewasgatheredinahighresourcesettingwithintensivecaremanagement;however,itcanbealsoadaptedforlesswell-resourcedareas.MostpatientsweretreatedinaprivatehospitalinJohannesburg.Ahospitalpharmacyrepositoryallows24-houraccesstomedicinesfreeofcharge.Telephoneconsultancyordeliveryofmedicinesforothermedicalfacilitiesabroadis also provided.
Moredetaileddataonthe20treatedcaseswerepresented.Mostpatientsweretourists; theothershadanoccupational-relatedexposure(Table 9.1).ThepatientsacquiredtheirinfectioninMalawi,Uganda,theUnitedRepublicofTanzania,ZambiaandZimbabwe(Table 9.2).
Table 9.1. Reasonsforexposureofimportedr-HATcasesinSouthAfrica,2004–2014
Table 9.2. Countrywheretheinfectionwasacquired
No. of cases (%)Foreigntourist 9Expatriate or resident 4Conservationist 2Game farmer 2Foreignsoldier,fieldexercise 1Pilot:touristtransport 1Church-relatedtravel 1TOTAL 20
Country of acquisition Number of cases and sites, 2004-2014Malawi 6(Kasungu3,Nkhotakota3)Zambia 6(LuangwaValley3,Kasanka2,Kafue1)Tanzania 3(Serengeti)Zimbabwe 3(Kariba1,ManaPools2)Uganda 2(QueenElizabethNationalPark,
?MurchesonFalls)TOTAL 20
Thethreekeyelementsforthediagnosiswereidentified:(i)exposureinanendemicarea;(ii)historyofapainfultsetsebite;and(iii)presenceoftrypanosomalchancre.Atrypanosomalchancrehasamarkedandpainfulerythema,butitsappearancevariesconsiderably(Figure 9.1).Achancreisnotalwayspresent(<50%ofcasesaccordingtotextbooks).Chancresareoftenmissed,especially inpartsof thebodythatarenotobviouslyvisibleoraremisinterpretedasinsectbitesorbacterialcellulites.AtrypanosomalchancreisusuallylargerandhasnoobviousnecrosisincontrasttoanescharinAfricantickbitefever.
9 FreanJ,SielingW,PahadH,ShoulE,BlumbergL.ClinicalmanagementofEastAfricantrypanosomiasisinSouthAfrica:Lessonslearned.IntJInfectDis.2018;75:101–8.doi:10.1016/j.ijid.2018.08.012.

48 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Figure 9.1. VariablepresentationsofeastAfricantrypanosomalchancres
Oneofthebiggestproblemsisadelayeddiagnosisthroughpoorhistory-taking,missingkeyclinicalsigns,delayedtransfer,incorrectapplicationofdiagnostictestsandinexperiencedlaboratorypersonnel.Insomeendemiccountries,localorexpatriatedoctorsmaynotbeawareofr-HAT,asitisaveryraredisease.Afterthe onset of symptoms, complicationsmaydevelop in less than 1week.Any extra delaymaybe criticaland result in severe disease,withmultiorgan involvement, severe thrombocytopenia, frequent bleeding,renalfailure,respiratorydistressandhepaticpathology,requiringhighlevelsofclinicalcare. Myocarditis was only observed in an individual case. Anotherratherearlycomplicationwasfluidoverload,whichmustbeconsideredinintravenousfluidmanagement.Onecasewithcomplicatedadrenalinsufficiencywaspresentedthathasbeendescribedonlyoncebefore.Decreasedlevelofconsciousnesswas inmostcasesnotasignofcentralnervoussystem(CNS)involvementandmayhaveotherexplanations,suchasmetabolicderangements.
Initially,trypanosomesmaybescantyanddifficulttodetectbymicroscopicexaminationofperipheralblood;therefore, blood smears should be repeated. Buffy coat filmshave an increased sensitivity, but they canbe technically challenging to produce (e.g. centrifugation needed). Every patient, irrespective of clinicalcondition,musthaveanexaminationofcerebrospinalfluid(CSF).InSouthAfrica,thisisusuallydoneafterafewdaysoftreatmentwithsuramin,whenthepatienthasclinicallyimprovedandtheperipheralbloodsmearisclearofparasites.Otherwise,false–positiveCSFfindingsfroma“bloodytap”maybepossibleandthereisatheoreticalriskofintroducingtrypanosomesintoCSF.TheresultsofCSFshouldbeinterpretednotonlyinisolationbutalsointheclinicalcontext;otherwise,theymayleadtooverdiagnosisofCNSinvolvement.
Treatmentisusuallystartedwithatestdoseofsuramin.Adversereactionsincludingcardiovascularcollapse,skinreactions,peripheralneuropathyandnephrotoxicitymayoccur.Onlytwopatientswereinthesecondstage and had to be treated with melarsoprol. Despite all the common problems described above, themortalityrateinthepresentedcaseserieswaslow(2/20;10%).
Successful case management relies on good laboratory facilities for rapid diagnosis, rapid access toantitrypanosomal treatment and skilled intensive care. Physicians in endemic countries are less and lessexperienced in the management of r-HAT. Besides operational research, recommendations should bedevelopedthatcanbeadaptedtolocalconditionsandespeciallyforlowresourcesettings.

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 49
10.Exportedcasesassurveillancetool for rhodesiense HAT
During2000–2018,atotalof138casesofHATwerereportedfromnon-endemiccountries(Figure 10.1).
Figure 10.1. Numbersofcasesofr-HATdiagnosedannuallyinnon-endemiccountries,2000–2018
Of thesecases,71%corresponded to the rhodesiense formand29%to thegambiense form.Amongther-HATcases,82%werediagnosedinthefirststageand18%inthesecondstage.Thevastmajorityofr-HATcaseswereintouriststravellingtoendemicareas(Table 10.1).
Table 10.1. Casesofr-HATdiagnosedinnonendemiccountriesaccording toactivityofthepatient,2000–2018
ActivityTourists 74Rangers 5Tourismworkers(guidespilots,lodgesstaff) 4Conservationistsworkers 3Soldiers 2Hunters 1Missionary 1Unknown 8Total 98

50 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
HAT cases were diagnosed in nonendemic countries in the five continents. In South Africa, a frequentdestination formedicalevacuationflights fromsouthandeastAfricancountries, thehighestnumber (31ofr-HATimportedcases)wasdiagnosed,followedbytheUnitedStates(20),theUnitedKingdom(12),theNetherlands(8),Belgium(4),Germany,India,Italy(3each),China,Norway,Sweden(2each)andArgentina,Brazil,Canada,France,Israel,PolandandSpain(1each).
The infectionwasmainly contracted inprotectedareas such asnational parks andwildlife reserves. Thecountryexportingthemost(47)r-HATcaseswastheUnitedRepublicofTanzania,mainlyfromtheSerengetiNationalPark.Forexample,aclusterofcasesthatoriginatedintheUnitedRepublicofTanzaniawassuggestiveofachangeinthelocalepidemiologyin2001.Theothercountriesexportingr-HATcaseswereZambia(20),Malawi(15),Zimbabwe(7),Uganda(7)andKenya(2).
During 2000–2018, some 1.7% of all cases was reported from nonendemic countries (Table 10.2). Theproportion of cases in whom r-HAT was diagnosed in nonendemic countries versus those diagnosed inendemiccountriesincreasedinthelastyears(2014–2018).Thevariousfactorsfortheincreasingproportionof r-HAT casesdiagnosed innon-DECswerediscussed.Underreporting inendemic countriesmaybeonefactor.Bettercontrolofthedomesticanimalreservoir,incontrasttoalackofcontrolofthewildlifereservoirintypicaltransmissionzonesfortourists,maybeanotherfactor.
Table 10.2. Casesofr-HATbycountryofinfectionandproportionofcasesdiagnosedinnonendemiccountries(exportedcases)during2000–2018(left)and2014–2018(right)
2000-2018 2014-2018Total Exported % Total Exported %
Kenya 40 2 5.0% 0 0Malawi 695 15 2.2% 119 4 3.4%Mozambique 2 0 0.0% 0 0Tanzania 1,660 47 2.8% 10 5 50.0%Uganda 3,281 7 0.2% 125 5 4.0%Zambia 137 20 14.6% 32 6 18.8%Zimbabwe 30 7 23.3% 8 0 0.0%Total 5,845 98 1.7% 290 20 6.9%
Whiletheriskof infection is lowforthetotalnumberof tourists, itcannotbedisregarded.Awareness inhealthstaffoftravelmedicineservicesoftheriskofHATisthusimportant.
As rapid access to antitrypanosomal treatment is crucial for patients,WHOmaintains strategic stocks invarious non-endemic countries and an emergency stock in Geneva, Switzerland (Figure 10.2). Country-specificregulationsfortheimportofmedicinesmustbeconsidered.TheirdistributionviatheWHOcountryofficesmaybehelpfultoavoiddelays.

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 51
Figure 10.2. AvailabilityofantitrypanosomalmedicinesfortreatmentofHATinnonendemiccountries
~ 1. WHO emergency stock of drugs in Geneva
~ 2. Strategic stocks of anti-trypanosomal medicines
¾ Hospital,RoyalLiverpool&BroadgreenNHSFoundationTrust,Liverpool(United Kingdom)
¾ UniversityCollegeLondon,NHSFoundationTrust,London(United Kingdom)
¾ FMHInnereMedizinundTropen-undReisemedizin,SwissTropical&PublicHealthInstitut,Basel(Switzerland)
¾ CentersforDiseaseControlandPrevention,Atlanta(USA)
¾ DivisionofInfectiousDiseases,InstituteofMedicalScience,Tokyo(Japan)
¾ UniversitairZiekenhuis,Antwerpen(Belgium)
¾ ErasmusMedicalCenter,Rotterdam(The Netherlands)
¾ HospitalClinic,Barcelona(Spain)
¾ NetcareMilparkHospital,Johannesburg(South Africa)
¾ NationalInstituteofParasiticDiseases,ChinaCDC,Shanghai(China)
¾ DepartmentofTropicalMedicine,MissioklinikWürzburg(Germany)
AntitrypanosomalmedicinesaredonatedbySanofiandBayeranddistributedsolelyundertheresponsibilityofWHO.Theycannotbeobtainedcommercially (except forpentamidine,which isused to treatdiseasesother thanHAT).Themedicinesareprovidedtocountries inwhich thedisease isendemic throughWHOcountryoffices,uponrequest,accordingtotheneedsandinformationprovided.TotreatHATcasesdiagnosedin nonendemic countries, pharmaceutical services should request themedicines fromWHOand provideepidemiologicalandclinicaldataoncasesinwhomthediseaseisdiagnosed.ThisinformationenablesWHOtomaintain anHAT surveillance system for nonendemic countries that provides valuable informationon“spots”oftransmissiontocomplementthedatacollectedinendemiccountries.Thisinformationisprovideddirectlytotheendemiccountriesandcanbeusedtotriggerspecificactivities.
52 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
11.Clinicaltrialfortreatment of rhodesiense HAT with fexinidazole
Fexinidazoleisthefirsteffectiveoralmonotherapyagainstbothstagesofg-HAT.ItreceivedapositivescientificopinionbytheEuropeanMedicinesAgencyinNovember2018,andmarketingauthorizationwasgivenintheDemocraticRepublicoftheCongoinDecember2018.
Theclinicaltrial(FEX07)isduetostartinMay2019andwillbeconductedinUgandaandMalawitoassesstheefficacyoffexinidazoleforr-HATpatients.
Fexinidazolecanbeconsideredaprodrugthatismetabolizedintofexinidazolesulfoxide(M1)andfexinidazolesulfone(M2).Theconcentrationof fexinidazolesulfone isdecisive forthetherapeuticeffect.Fexinidazolemustbetakenwithfood.Theplasmalevelsarehighestiftakenwithhighfatfood,buthighplasmalevelsarealsoreachedwithriceorplumpy-nut.ThepredictedCNSconcentrationlevels,with40%freefractionoffexinidazolesulfone,areclearlywithintherapeuticlevels.
Safety data are available from the pooled analysis of the threemain studies (FEX04, FEX05 and FEX06),including619patientswithg-HAT.Gastrointestinaldisorders,mainlyvomitingandnausea,andCNS-relateddisorders(headache,insomnia,tremor)werethemostcommonlyreportedadverseevents.Theincidenceofvomitingwashigherinthepaediatricstudy(FEX06)thanintheadultstudyandwasparticularlyhighintheloadingphaseofthetreatment(36%onday2,thetotalschedulebeing10days).Themajorityofpatientsvomitedmorethan2hafterdrugadministration,likelytriggeredatCNSlevel.Importantly,however,withtheexceptionof2patients,therewerenosevereeventsofvomitingandtreatmentcouldbecontinued.
TheHAT-r-ACCconsortium(ACCstandsforaccess)waspresented.CoordinatedbyDNDi with partners from France,Malawi,Portugal,Switzerland,andUganda,itsaimsare:(i)toextendtheindicationoffexinidazoleforthetreatmentofr-HAT(WP1);(ii)toensureproperexecutionoftheclinicaltrialthroughstrengthenedcapacityfortreatmentandcare(WP2);and(iii)toengagethelocalcommunitytoimproveaccesstotreatmentand extend case detection (WP3). The project management Committee (WP4) includes representativesfrom DNDi,InstitutdeRecherchepourleDéveloppement,theUniversityofLisbon,MakerereUniversityofUganda,MalawiMinistryofHealthandPopulation,theUgandaNationalHealthResearchOrganisation,theSwissTropicalandPublicHealthInstituteandEpicentre.Itwasemphasizedthatthetrainingsnotonlyservethetrialbutalsoenablecommunityengagementthroughlocalstaff.TheprogrammeismainlyfundedbytheEuropean&DevelopingCountriesClinicalTrialsPartnersip.

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 53
Protocolnumber: DNDi-FEX-07-HAT
Study title: Efficacy and safety of fexinidazole in patients with human African trypanosomiasis (HAT) due to Trypanosoma brucei rhodesiense: a multicentre, open-label clinical trial
Design: multicentre,open-label,non-randomized
Recruitmenttarget:34evaluablestage-2r-HATpatients(stage-1patientswillbeincludedbutdonotinfluencethestatisticalanalyses)
Studysites:LwalaHospital(Uganda)andRumphiDistrictHospital(Malawi).
Patients from neighbouring health centres: Kaberamaido/Dokolo districts (Uganda) and Rumphi/Mzimba Northdistricts(Malawi)andChama(Zambia)willbetransportedtothesitesfortreatment
Studyduration:2yearsrecruitmentand1-yearfollow-up
Maininclusioncriteria
~ Signedinformedconsentform
~ ≥6yearsold
~ ≥20kgbodyweight
~ Abilitytoingestatleastonecompletemealperday
~ Karnofskyindex≥40
~ ParasitologicalconfirmationofT. b. rhodesienseinfection
~ Havingapermanentaddressorbeingtraceablebyothersandwillingandabletocomplywithfollow-upvisitschedule
~ Agreementtobehospitalizedforaminimumof11daysandtoreceivethestudytreatment
Mainexclusioncriteria
~ Active clinically relevant medical conditions other than HAT that may jeopardize subject safety or at theinvestigator’sdiscretionmayinterferewithparticipationinthestudy
~ Compromised general health or severely deteriorated general condition, such as severe malnutrition,cardiovascularshock,respiratorydistressorterminalillness
~ Patientswithseverehepaticimpairment
~ Firsttrimesterofpregnancy
~ Anycontraindicationtonitroimidazoleclass(knownhypersensitivity)ortoanyoftheexcipients
~ Patientspreviouslyenrolledinthestudyorhavingalreadyreceivedfexinidazole
Treatment:fexinidazole10days(sameregimenasing-HAT),in2phases ~ 2dosesdependingonthepatient’sageandweight:
~ Alladultsandchildren(≤15yearsold)≥35kg:
¾ D1toD4(1800mg/day)
¾ D5toD10(1200mg/day)
~ Childrenweighing≥20and<35kg:
¾ D1toD4(1200mg/day)
¾ D5toD10(600mg/day)
Followupvisits:after1month,9weeks,6monthsand12monthsTestofcureat6and12monthsincludingthick/thinbloodsmearand/orlymphnodeaspiratemicroscopicexamination,lumbarpunctureforparasitedetectionandCSFwhitebloodcellcount.

54 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Theinitialdataareexpectedforthebeginningof2021anditisenvisagedthatthefinalresultswillbemadeavailableinthesecondquarterof2023.
Inthediscussion,aregularupdateonprogressofthestudywasproposed(e.g.atthenext(fourth)stakeholdersmeeting).Someparticipantssharedtheiroptimisminreachingtherecruitmenttarget,astheclinicaltrialwillraise awareness of the disease.
Thepotentialofacoziborole,asingleoraldosetreatment,wasalsodiscussed.Theclinicaltrialrecruited206patientsinstages1and2ofg-HAT,mostoftheminlatestage2,andwascompletedinMarch2019.InApril2014,about30%ofpatientshadcompletedthefollowupperiodof18months.Theabsorptionofacoziboroleis less dependent on food than that of fexinidazole.

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 55
12.OneHealth:linkingeliminationof rhodesiense HAT with other initiatives
12.1 Epidemiological studies in animals and tsetse flies, and new molecular approaches in Zambia
Luapulaprovince, inthenorthofZambia,borderingtheDemocraticRepublicoftheCongo,wasahistoricfocusof r-HAT,withnoreportedhumancasessince2000.However,after2casesof r-HATwerereported(in2017and2018),abiologicalsurveywasconductedincattleatthelocationofthelastcase(inSamfya).Bloodfrom40cattlewasanalysedwithPCR(LAMP)fortrypanosomes,yieldingpositiveresultsfortsetse-transmittedanimaltrypanosomes,butnotforhumaninfectiveforms.
Astudycombiningmicroscopyandmoleculartechniquesdeterminedthepresenceoftrypanosomespeciesin cattle, goats and tsetseflies in the Luangwavalley, north-easternZambia,butdidnot identify speciesinfectivetohumans.Some10furthertsetsesurveysinnorthernandcentralZambiafoundsamplespositiveforserum-resistanceassociatedprotein(SRA)(invaryingproportions),indicativeforT. b. rhodesiense,mainlyin Glossina morsitans,themainvectorforr-HAT(Figure 12.1.1).Astheseareasarecurrentlyconsideredatlow,verylowornoriskoftransmission,theneedforsurveillanceofHATintheseareaswassuggested.
As the currently available tsetse traps are ineffectiveagainstG. morsitans, anewmobile, carmountabletrap(“SugimotoTrap”)wasdeveloped.Thetrapiseasytoproduceatlowcostandminimizesexposuretofliesduringoperation.ThetrapwastestedinvariousnationalparksinZambiaandMalawiandfoundtobeeffectiveagainstG. morsitans, G. pallidipes and G. brevipalpes.
10 LaohasinnarongD,GotoY,AsadaM,NakaoR,HayashidaK,KajinoKetal.StudiesoftrypanosomiasisintheLuangwavalley,north-easternZambia.ParasitVectors.2015;8:497.doi:10.1186/s13071-015-1112.
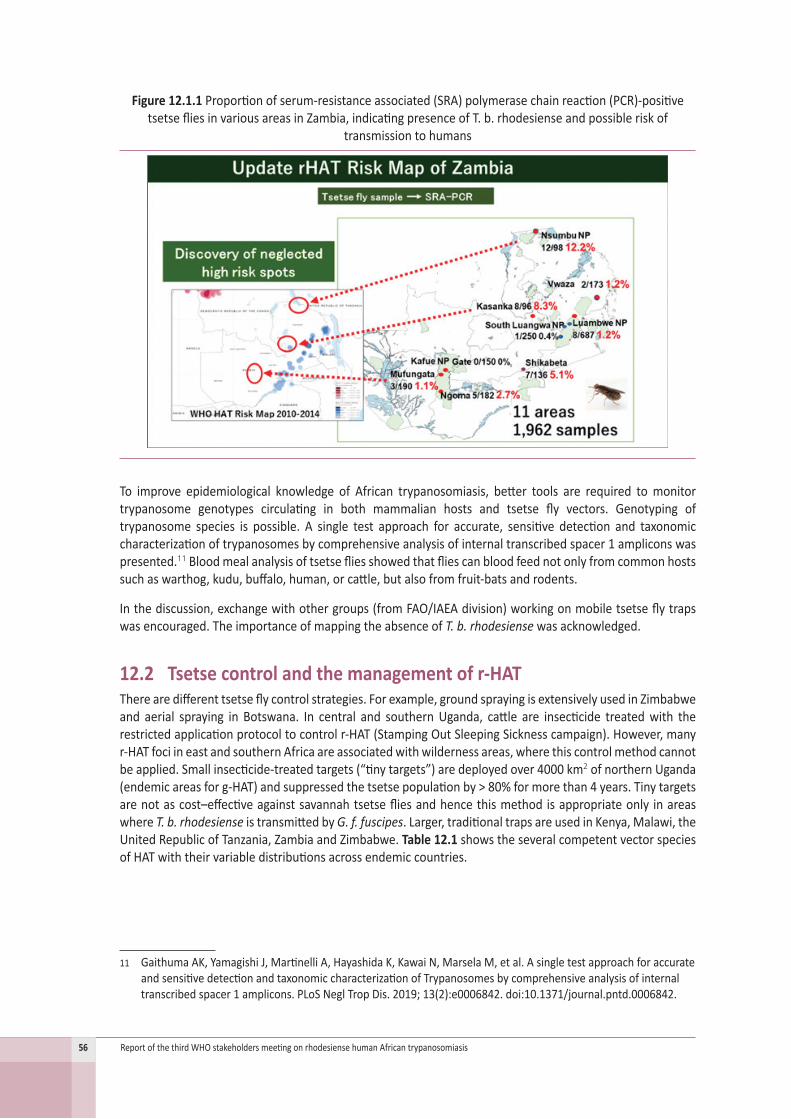
56 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Figure 12.1.1 Proportionofserum-resistanceassociated(SRA)polymerasechainreaction(PCR)-positivetsetsefliesinvariousareasinZambia,indicatingpresenceofT.b.rhodesienseandpossibleriskof
transmissiontohumans
To improve epidemiological knowledge of African trypanosomiasis, better tools are required tomonitortrypanosome genotypes circulating in both mammalian hosts and tsetse fly vectors. Genotyping oftrypanosome species is possible. A single test approach for accurate, sensitive detection and taxonomiccharacterizationoftrypanosomesbycomprehensiveanalysisofinternaltranscribedspacer1ampliconswaspresented.11Bloodmealanalysisoftsetsefliesshowedthatfliescanbloodfeednotonlyfromcommonhostssuchaswarthog,kudu,buffalo,human,orcattle,butalsofromfruit-batsandrodents.
Inthediscussion,exchangewithothergroups(fromFAO/IAEAdivision)workingonmobiletsetseflytrapswasencouraged.TheimportanceofmappingtheabsenceofT. b. rhodesiensewasacknowledged.
12.2 Tsetse control and the management of r-HATTherearedifferenttsetseflycontrolstrategies.Forexample,groundsprayingisextensivelyusedinZimbabweand aerial spraying in Botswana. In central and southernUganda, cattle are insecticide treatedwith therestrictedapplicationprotocoltocontrolr-HAT(StampingOutSleepingSicknesscampaign).However,manyr-HATfociineastandsouthernAfricaareassociatedwithwildernessareas,wherethiscontrolmethodcannotbeapplied.Smallinsecticide-treatedtargets(“tinytargets”)aredeployedover4000km2ofnorthernUganda(endemicareasforg-HAT)andsuppressedthetsetsepopulationby>80%formorethan4years.Tinytargetsarenotascost–effectiveagainstsavannahtsetsefliesandhencethismethodisappropriateonly inareaswhere T. b. rhodesienseistransmittedbyG. f. fuscipes.Larger,traditionaltrapsareusedinKenya,Malawi,theUnitedRepublicofTanzania,ZambiaandZimbabwe.Table 12.1 showstheseveralcompetentvectorspeciesofHATwiththeirvariabledistributionsacrossendemiccountries.
11 GaithumaAK,YamagishiJ,MartinelliA,HayashidaK,KawaiN,MarselaM,etal.AsingletestapproachforaccurateandsensitivedetectionandtaxonomiccharacterizationofTrypanosomesbycomprehensiveanalysisofinternaltranscribedspacer1amplicons.PLoSNeglTropDis.2019;13(2):e0006842.doi:10.1371/journal.pntd.0006842.
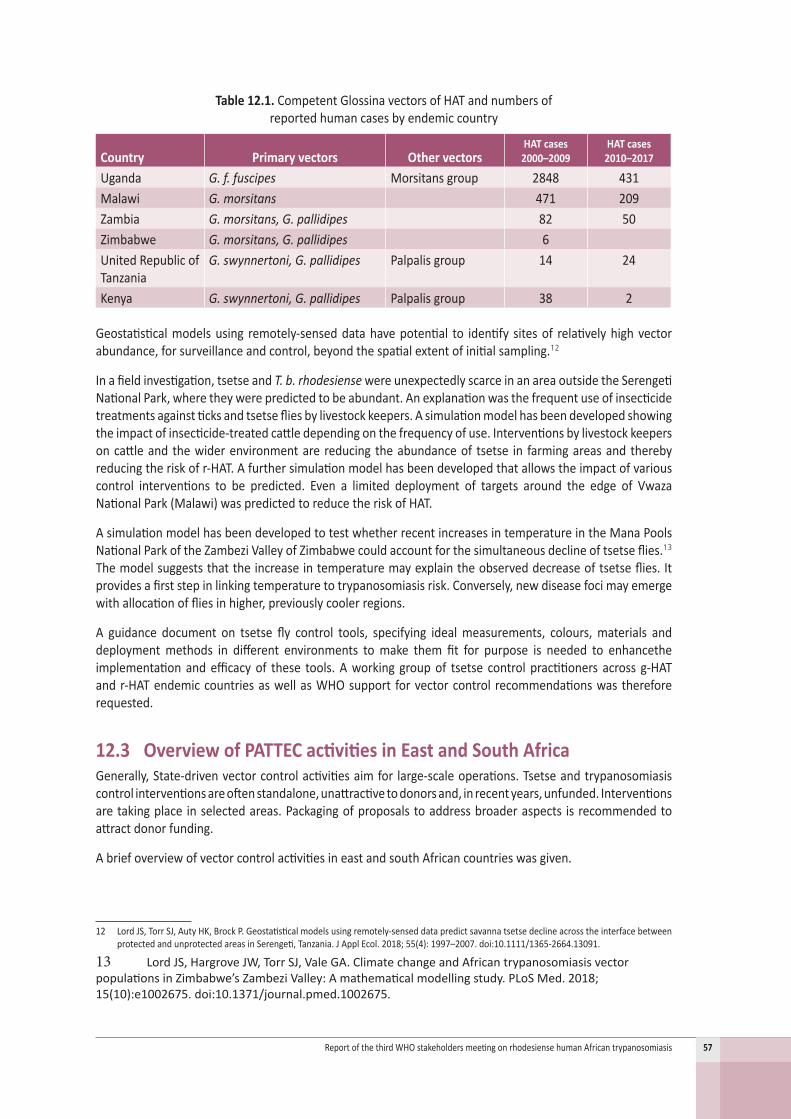
ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 57
Table 12.1. CompetentGlossinavectorsofHATandnumbersof reportedhumancasesbyendemiccountry
Country Primary vectors Other vectorsHAT cases
2000–2009HAT cases
2010–2017
Uganda G. f. fuscipes Morsitansgroup 2848 431Malawi G. morsitans 471 209Zambia G. morsitans, G. pallidipes 82 50Zimbabwe G. morsitans, G. pallidipes 6UnitedRepublicofTanzania
G. swynnertoni, G. pallidipes Palpalisgroup 14 24
Kenya G. swynnertoni, G. pallidipes Palpalisgroup 38 2
Geostatisticalmodelsusing remotely-senseddatahavepotential to identify sitesof relativelyhighvectorabundance,forsurveillanceandcontrol,beyondthespatialextentofinitialsampling.12
Inafieldinvestigation,tsetseandT. b. rhodesiense wereunexpectedlyscarceinanareaoutsidetheSerengetiNationalPark,wheretheywerepredictedtobeabundant.Anexplanationwasthefrequentuseofinsecticidetreatmentsagainstticksandtsetsefliesbylivestockkeepers.Asimulationmodelhasbeendevelopedshowingtheimpactofinsecticide-treatedcattledependingonthefrequencyofuse. Interventionsbylivestockkeepersoncattleand thewiderenvironmentare reducing theabundanceof tsetse in farmingareasand therebyreducingtheriskofr-HAT.Afurthersimulationmodelhasbeendevelopedthatallowstheimpactofvariouscontrol interventions to be predicted. Even a limited deployment of targets around the edge of VwazaNationalPark(Malawi)waspredictedtoreducetheriskofHAT.
AsimulationmodelhasbeendevelopedtotestwhetherrecentincreasesintemperatureintheManaPoolsNationalParkoftheZambeziValleyofZimbabwecouldaccountforthesimultaneousdeclineoftsetseflies.13 Themodelsuggeststhattheincreaseintemperaturemayexplaintheobserveddecreaseoftsetseflies.Itprovidesafirststepinlinkingtemperaturetotrypanosomiasisrisk.Conversely,newdiseasefocimayemergewithallocationoffliesinhigher,previouslycoolerregions.
A guidance document on tsetse fly control tools, specifying idealmeasurements, colours,materials anddeploymentmethods in different environments tomake them fit for purpose is needed to enhancetheimplementationandefficacyof these tools.Aworking groupof tsetse control practitioners across g-HATandr-HATendemiccountriesaswellasWHOsupport forvectorcontrol recommendationswasthereforerequested.
12.3 Overview of PATTEC activities in East and South AfricaGenerally,State-drivenvectorcontrolactivitiesaimfor large-scaleoperations.Tsetseandtrypanosomiasiscontrolinterventionsareoftenstandalone,unattractivetodonorsand,inrecentyears,unfunded.Interventionsaretakingplace inselectedareas.Packagingofproposalstoaddressbroaderaspects isrecommendedtoattractdonorfunding.
AbriefoverviewofvectorcontrolactivitiesineastandsouthAfricancountrieswasgiven.
12 LordJS,TorrSJ,AutyHK,BrockP.Geostatisticalmodelsusingremotely-senseddatapredictsavannatsetsedeclineacrosstheinterfacebetweenprotectedandunprotectedareasinSerengeti,Tanzania.JApplEcol.2018;55(4):1997–2007.doi:10.1111/1365-2664.13091.
13 LordJS,HargroveJW,TorrSJ,ValeGA.ClimatechangeandAfricantrypanosomiasisvectorpopulationsinZimbabwe’sZambeziValley:Amathematicalmodellingstudy.PLoSMed.2018;15(10):e1002675.doi:10.1371/journal.pmed.1002675.
58 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Uganda:thelastlarge-scaleoperationendedin2012.Anumberoffollowupproposalsarenotyetfunded.Trapsandtargets,andcattlesprayingaredeployedinselectedareas.VectorcontrolactivitiesaredonebypartnersinselectedHAThotspots.
South Sudan: thepoliticalinstabilityishinderinginitiationofvectorcontrolactivities.
United Republic of Tanzania:lowlevelvectorcontrolactivities(networkofdiptanks)areundertaken;largescaleoperationsarenotfunded.Anationaltsetseandtrypanosomiasiscontrolstrategyisunderdevelopment.
Kenya: thelastlarge-scaleoperationsconcludedin2012–2013.ICIPEispromotingrepellenttechnologyinselectedareas.KenyaisapparentlyfreeofHAT(butthisstatusisquestionableintheMasaiMara–Serengetiecosystem).
Rwanda:therearelimitedvectorcontrolactivitiesinAkageraNationalPark.ThelastcaseofHATwasin1998.
Burundi:therearevirtuallynovectorcontrolactivities.TheHATstatusisnotdefined.
Zimbabwe: vectorcontrolactivitiesarewelladvanced.
Zambia:vectorcontrolisprogressingwellwithgovernmentalcommitment(e.g.aerialspraying).
Botswana and Namibia:bothcountriesareapplyingforregistrationtobetsetsefree.
Theintensityofvectorcontrolactivitiesvariesgreatlyacrossregions.Large-scalevectorcontroloperationsfacechallengestofunding.GovernmentsshouldconsidertargetingvectorcontrolinareasofHATtransmission,alsotoassessthecontributionofvectorcontroltoHATelimination.Awareness/advocacyforvectorcontrolshouldberaisedatthehighestpoliticallevel.
APATTECcommunication/advocacystrategy,preparedandsupportedbyIAEA,targetspoliticalplayersatthehighestlevel.ThereisincreasedengagementwithRegionalEconomicCommunitiesadvocatingforregionalprogrammes.Recently,meetingshavebeenheldwiththeEastAfricanCommunity,theEconomicCommunityofWestAfricanStatesandtheEconomicCommunityofCentralAfricanStates.
SpecializedTechnicalCommitteesandtheStatutoryMinisterialForumonAgriculture,RuralDevelopment,WaterandEnvironmentareplatformsfromwhichpoliticalawarenesscanbeenhancedandrecommendationsthenmadeto theExecutiveCouncil fordecisionsofAfricanHeadsofStateandGovernment.SideeventsheldduringsummitsoftheAfricanUniononthematicissues,retreatswithpoliticiansonthematicissues,briefingsessionsofthePermanentRepresentativeCommitteeandwithAmbassadorsofMemberStatesoftheCommitteeoftheAfricanUnion,whichreporttonationalcapitalsontheoutcomesofbriefingsessions,offerfurtherpossibilitiestoraiseawareness.
Aproposedway forward is collaborationamongPATTEC,WHOandotherpartnerson thepreparationofpolicybriefs onHATelimination.SummitdecisionsinformedbypolicybriefscouldcommitAfricanHeadsofStateandGovernmenttotheHATeliminationstrategy.
Inthediscussion,thehighlyeffectiveprogrammesinEthiopiaandSenegalwerementioned,whichusethesterileinsecttechniquefortsetsecontrol.ThePATTECdeclarationof2001ontheeradicationofthetsetseflyisbeingreviewed,althoughlimitedstaffinginthePATTECcoordinationofficemakesthistaskchallenging.
ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 59
12.4 FAO and PATT: the progressive control pathway (PCP) for African animal trypanosomosis
TheProgrammeAgainstAfricanTrypanosomosis(PAAT)wasofficiallyestablishedinNovember1997bythe29thSessionoftheFAOConference(resolution5/97).Aninteragencycollaboration,PAATcoordinatestheworkofFAO,WHO,theIAEAandtheInter-AfricanBureauforAnimalResourcesoftheAfricanUnion.
ThevisionofPAATisanAfricancontinentwheretrypanosomosesnolongerconstrainsustainableagricultureandruraldevelopment,northreatenhumanhealth.PAATisfundedbyaregularbudgetfromFAO,anannualcontributionfromWHO(forworkontheHATAtlas)andextrabudgetarycontributionstoFAO(includingfromtheGovernmentofItaly).
PartnersofPAATareAU-PATTEC,AfricanMemberStatesaffectedby tsetseand trypanosomiasis (38sub-Saharancountries),OIE,theInternationalFundforAgriculturalDevelopmentandtheUnitedNationsIndustrialDevelopmentOrganization. There are international cooperations for development and cooperationswithcivilsociety(ItalianCooperation,UnitedKingdomDepartmentforInternationalDevelopment,GlobalAllianceforLivestockVeterinaryMedicines).PartneringresearchinstitutesarebasedinAfrica(CentreInternationalde Recherche-Développement sur l’Elevage en Zone Subhumide, ICIPE, International Livestock ResearchInstitute,NationalAgricultureResearchSystemsandacademia)aswellasinEurope(IRD/CIRAD[CooperationInternationaleenRechercheAgronomiquepourleDéveloppement],ITM).HealthforAnimals(formerlytheInternationalFederationforAnimalHealth)isaprivate-sectorpartner.
FAOpromotestheprogressivecontrolpathway(PCP)forAATasastrategicframeworktoreducethediseaseburden.ItalsopromotesOneHealthinterventions(e.g.livestockprotectivefences).TheAtlasesoftsetseandAAT(i.e.continentalandnational)havebeendeveloped,andWHOissupportedintheAtlasofHAT.Capacitydevelopment and technical support for endemic countries is provided, as well as knowledge products(e.g.publications,website,news,seminars,supporttoresearch,etc.).
WhilegreatstrideshavebeenmadeintheeliminationofHAT,progressinthecontrolofAATlagsbehind.PCPsareusedforthecontrolofanumberofhumanandanimaldiseases,e.g.peste de petits ruminents, brucellosisandrabies.InternationalorganizationssuchasFAO,WHO,OIEandAUrelyonPCPframeworkstoplan,implementandevaluateinterventions.TheoperationaldevelopmentofaPCPforAAT14wasledbyFAO(intheframeworkofPAAT),incollaborationwithIAEA,AU-PATTECandCIRAD,andinconsultationwithOIEandWHO.PCPisastepwiseapproachoffivestagesplusapre-entry(“belowstage1”)level(Figure 12.4.1).Progressionfromonestagetoanother ispossibleonly if thesetgoalsaremetandthefollowingstage isprepared.Anindependentvalidationofstageprogressionisrequired.
At the pre-entry level, political commitment and a functioning specialized national structure with corecapacitiesthatismandatedtodealwithtsetseandAATareessentialrequirementsforenteringPCP.Instage1,affectedcountriesdeveloptechnicalcapacitiesandgainsufficientunderstandingofAATdistribution,riskandimpactforevidence-basedplanningofsubsequentactivities.Pilotfieldinterventionsarealsoconducted.Larger scalefieldactivitiesare implemented in stage2andbeyond. Stage2aims toachieve sustainable,economically-profitable reductions in AAT burden. The intervention strategy is based on integratedmanagementofAAT(acommunity/farmer-basedapproach).Theaimofthefinalstages(3–5)ofPCPistocreatesustainableAAT-freeareas.Stage3 iscompletedwhenAATtransmission is interrupted. Instage4,somecontrolmeasuresaremaintained,whileinstage5theeliminationofAATmustbesustainableintheabsenceofinterventions.
14 DiallO,CecchiG,WandaG,ViljoenGJ,MattioliR,BouyerJ,etal.DevelopingaprogressivecontrolpathwayforAfricananimaltrypanosomosis.TrendsParasitol.2017;33(7):499–509.doi:10.1016/j.pt.2017.02.005.

60 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Figure 12.4.1. Theprogressivecontrolpathway(PCP)forAfricananimaltrypanosomiasis(AAT)
Duringthe17thAU-PATTECCoordinators’Meeting(26–28November2018)itwasrecommendedthatthePCPconceptbestreamlinedintonationalandregionalstrategiesandprojectsagainstAAT.Stakeholdershavebeen engaged in threeAU-PATTECmeetings aswell as in severalworkshops inAAT-affected countries ineasternAfricasince2015.
AAT isanOIEnotifiabledisease.There isnoofficial recognitionbyOIEof “freedomfromAAT”;however,countryself-declarationsoffreedomarepossible.ThefirstAAT-specificchapterintheOIETerrestrialCodewillprovideanopportunitytocloseagapforAAT.FAOsupportsthiseffortandparticipatesinmeetingswithaviewtoensuringconsistencywithPCP.
Inthediscussion,thepossibilityofMemberStatesapplyingforfundingofsmall-scaletechnicalprojectsviatheFAOcountryrepresentativewasraised.

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 61
13.ConclusionsTheparticipantsofthethirdstakeholdersmeetingconcludedasfollows.
1. Thelownumberofreportedr-HATcasesindicatesthatthegoalofeliminationofHATasapublichealthproblemby 2020 iswithin reach.Nevertheless, under-detection remains a concern and surveillanceshould be reinforced in response.WHOmaintains its commitment to supporting countries endemicforthediseaseinensuringaccesstodiagnosisandtreatmentforr-HATpatientsandinmonitoringtheepidemiologicalprogressionofthedisease.
2. Wildlifeanddomesticanimalsconstitutethemainreservoirsofr-HATandplayacentralroleinmaintainingtransmissiontohumansthroughthebiteofinfectioustsetseflies.Inthisepidemiologicalcontext,vectorcontrolshouldbestrengthenedandanimalhealthinterventionsdeployedinaOneHealthframeworkto attain r-HAT elimination. Theuseof theprogressive control pathway approach forAfrican animaltrypanosomiasiscouldbeusefulinpromotingsynergiesforcontroloftheanimalreservoirandthevector.
3. Given the variability in the characteristics and quality of vector control tools, guidelines should bepreparedtoensurethequalityandgooduseofvectorcontroltoolstailoredtodifferentenvironments.
4. New tools for r-HAT diagnosis and surveillance that can be adapted for use in the field should bedevelopedasapriority.
5. Thewidespreaduseofrapiddiagnostictestsformalariahasreducedtheuseofbloodsmearmicroscopyand thereby diminished the probability of diagnosing r-HAT. Therefore, in areas endemic for r-HAT,clinicalandlaboratoryalgorithmsincludingbloodsmearmicroscopyshouldbedesignedandappliedfordiagnosisofr-HAT.
6. Progresshasbeenmadeinthepossibleintroductionofnewtreatmentsforr-HAT.Fexinidazolehasbeenapprovedfortreatmentofgambiense-HATandaclinicaltrialisexpectedtostartshortly.Updatesonthistrial shouldbepresentedat thenext (fourth) stakeholdersmeeting.Anewstage-independent singledoseoraltreatmentwithacoziborolecouldofferotherpossibilitiesfortreatment.
7. Advancesintheprocessofvalidationofeliminationofr-HATasapublichealthproblemhavebeenmade,andeligiblecountriesareencouragedtoapplyforvalidation.WHOshouldmakepubliclyavailablethematerialithasdeveloped,includingtemplatesforcountrydossiers,aswellastheproceduresandcriteriaforassessingthem.ThismaterialcouldalsobeusedtoraiseawarenessofHATandcouldrepresentablueprintforotherdiseasestargetedforeliminationtofollow.
8. Thesignificant fundinggap in control, researchandawareness-raisingactivitiescalls foradvocacybyexternaldonors;nationalappropriationincludingdomesticfinancingiscriticalalsoforsustainabler-HATelimination.
9. Thegapsindiagnostic,treatmentandvectorcontrolcapacities,mainlyintermsoftrainedstaff,togetherwith the loss of expertise and frequent rotation of skilled personnel, areworrisome and should beaddressed.Possiblesolutions includeengaginghealthauthoritiessubnationallyandoptimizingexpertresourcesnationallyandinternationally,includingincascadetraining.
10. Aidmaterialsandmanualsforimprovementofpatientmanagementinendemicareasandofexportedcasesshouldbeprepared.
11. r-HATactivitiesshouldbeintegratedintootherhealthprogrammesasameansofreinforcingcontrolandsurveillanceofr-HAT.
12. The importantsocio-anthropologicalaspectsof r-HATat thecommunity level, includingthepotentialfacilitation of earlier detection of cases and access to treatment, should be addressed alongsidesurveillanceandcontrolactivities.
13. r-HATstakeholdersareencouragedtoengagedintheongoingprocessofdevelopingindicators,targetsand milestones for the new NTD roadmap 2021–2030.

62 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
Annex1.Agenda
Day 1 – Wednesday 10 April 2019: Description of the situation of HAT and progress
09:00–09:30 Welcome WHOAFRORepresentative Director,WHO/CDS/NTD
09:30–09:45 Introduction to the meeting Coordinator,WHO/CDS/IDM Chairperson
10:00–11:00Global situation of r-HAT
WHOReview of the conclusions of the previous meeting
11:00–13:00
Country report on r-HAT–Kenya – Malawi –UnitedRepublicofTanzania – Rwanda –Uganda – Zambia – Zimbabwe
Focalpointsofeachcountry(R.Kisati,M.Lemerani,J.B.Minja,J.B.Mbonigaba,C.Wamboga,V.Mwanakasale,P.Manangazira)
14:00–16:00
Elimination of rhodesiense HAT as a public health problem in 2020
HATeliminationTechnicalAdvisoryGroup(HAT-e-TAG):specificr-HATaspects V.Lejon
Eliminationofr-HATasapublichealthproblembycountries
–Dossierofelimination –Validationofelimination –Countriesstatus
WHO
NTDroadmap2030:target2030(indicatorsandtargets) WHO
16:00–17:00
Strategies for elimination. Reinforced integrated surveillance:
–Selectionofsites –Capacity-buildingindiagnosisandtreatment –Managementofdrugs –Monitoringandevaluation –Reporting
WHO
Day 2 – Thursday 11 April 2019: Control and elimination of r-HAT
09:00–09:30 Clinical management of complicated cases of HAT Case management protocols L.Blumberg
09:30–10:00 Exported cases as a surveillance tool for HAT WHO10:30–12:30 Clinical trial for treatment of r-HAT with fexinidazole NStrub,ATarral,O.Valverde
13:30–15:00
Contribution of other sectors to r-HAT elimination (One Health): linking elimination of r-HAT with other initiatives:
–Vectorcontrol – Animal health –Managementofprotectedareas
FAO/PATTEC/COCTU Openfloor
15:00–16:00 Gaps and challenges Generaldiscussion16:00–17:00 Conclusions, outcomes and closure of meeting Generaldiscussion

ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis 63
Annex2.Listofparticipants
Members
ProfessorM.Barrett,1UniversityofGlasgow,Glasgow,Scotland,UnitedKingdom
DrJ.Bernard,MinistryofHealth,CommunityDevelopment,Gender,ElderlyandChildren,Dodoma,UnitedRepublicofTanzania
DrS.Biéler,FoundationforInnovativeNewDiagnostics,Geneva, Switzerland
ProfessorL.Blumberg,CentreforEmergingandZoonoticDiseases,Johannesburg,SouthAfrica
DrP-MBorne,1CevaSantéAnimaleS.A.,Libourne,France
ProfessorC.Burri,SwissTropicalandPublicHealthInstitute,Basel,Switzerland
ProfessorP.Buscher,1InstituteofTropicalMedicine,Antwerp,Belgium
DrG.Cecchi,FoodandAgricultureOrganizationoftheUnitedNations,Rome,Italy
DrU.Dietmar-Madeja,1BayerHealthCarePharmaceuticals,Berlin,Germany
DrG.Doll,Sanofi,Gentilly,France
DrB.Fatunmbi,1WHORepresentative’sOffice,Kampala,Uganda
ProfessorE.Fèvre,UniversityofLiverpool,Neston,UnitedKingdom
Dr R. Grais,1Epicentre,Paris,France
MrR.ArgilesHerrero,1InternationalAtomicEnergyAgency,Vienna,Austria
Dr G. Hesse,1 BayerEnvironmentalScience,Ecully,France
MrsR.Kasati,1MinistryofHealth,Nairobi,Kenya
DrV.Lameyre,Sanofi,Gentilly,France
DrV.Lejon,ResearchInstituteforDevelopment,Montpellier,France
MrM.Lemerani,MinistryofHealth,Lilongwe,Malawi
DrA.Lidner,InstituteofTropicalMedicineandInternationalHealth,Berlin,Germany
DrP.Managazira,MinistryofHealthandChildWelfare,Harare, Zimbabwe
ProfessorI.Maudlin,1 UniversityofEdinburgh,Edinburgh,Scotland,UnitedKingdom
DrL.Matemba,NationalInstituteforMedicalResearch,DaresSalaam,UnitedRepublicofTanzania
DrE.Matovu,MakerereUniversity,Kampala,Uganda
MrJ.BoscoMbonigaba,MinistryofHealth,Kigali,Rwanda
Mr A. Mortensen,1VestergaardSA,Lausanne,Switzerland
DrK.Msyamboza,1 WHORepresentative’sOffice,Lilongwe,Malawi
DrV.Mwanakasale,CopperbeltUniversitySchoolofMedicine,Ndola,Zambia
ProfessorB.Namangala,UniversityofZambiaSchoolofVeterinaryMedicine,Lusaka,Zambia
Dr A. Nanai, 1 WHORepresentative’sOffice,DaresSalaam,UnitedRepublicofTanzania
ProfessorJ.Ndung’u,FoundationforInnovativeNewDiagnostics,Geneva,Switzerland
DrM.D.Ngamije,WHORepresentative’sOffice,Kigali,Rwanda
Dr E. Hernandez Pando,1MerialRwd,Lyon,France
MrF.Petit,1 MerialRwd,Lyon,France
DrA.Picado,FoundationforInnovativeNewDiagnostics,Geneva, Switzerland
DrC.L.Schumacher,1MerialRwd,Lyon,France
DrJ.B.A.Seixas,UniversidadeNOVAdeLisboa,Lisbon,Portugal
DrW.Shereni,MinistryofAgriculture,MechanizationandIrrigationDevelopment,Harare,Zimbabwe
DrP.Solano,InstitutdeRecherchepourleDéveloppement,Montpellier,France
DrP.Songolo,WHORepresentative’sOfficeforZambia,Lusaka,Zambia
Dr M. Steele,1 Bill&MelindaGatesFoundation,Seattle,UnitedStatesofAmerica
DrN.Strub-Wourgaft,DrugsforNeglectedDiseasesinitiative, Geneva, Switzerland

64 ReportofthethirdWHOstakeholdersmeetingonrhodesiensehumanAfricantrypanosomiasis
ProfessorC.Sugimoto,HokkaidoUniversity,Sapporo,Japan
Dr L. Tano,1MerialSASVeterinary,Lyon,France
DrA.Tarral,DrugsforNeglectedDiseasesinitiative, Geneva, Switzerland
MrI.Tirados,LiverpoolSchoolofTropicalMedicine,Liverpool,UnitedKingdom
ProfessorS.Torr,LiverpoolSchoolofTropicalMedicine,Liverpool,UnitedKingdom
Professor C. Waiswa,1MinistryofAgricultureAnimalIndustryandFisheries,Kampala,Uganda
DrC.Wamboga,MinistryofHealth,Kampala,Uganda
DrG.WisemanWanda,AfricanCommission,AddisAbaba, Ethiopia
ProfessorS.Welburn,1 UniversityofEdinburgh,Edinburgh,Scotland,UnitedKingdom
DrO.Valverde,DrugsforNeglectedDiseasesinitiative, Geneva, Switzerland
DrM.J.B.Vreysen,1InternationalAtomicEnergyAgency,Vienna,Austria
DrW.Zhao,FoodandAgricultureOrganizationoftheUnitedNations,Rome,Italy
DrG.BinghamZivanovic,1VestergaardFrandsenSA,Lausanne,Switzerland
Secretariat
DrB.Abela-Ridder,NeglectedZoonoticDiseases,DepartmentofControlofNeglectedTropicalDiseases,WorldHealthOrganization,Geneva,Switzerland
DrD.ArgawDagne,Innovative&IntensifiedDiseaseManagement,DepartmentofControlofNeglectedTropicalDiseases,Geneva,Switzerland
Dr A. Diarra,1 WHORepresentative’sOffice,Libreville,Gabon
DrA.KadimaEbeja,WHORepresentative’sOffice,Kinshasa,DemocraticRepublicoftheCongo
DrL.Grout,1 Innovative&IntensifiedDiseaseManagement,DepartmentofControlofNeglectedTropicalDiseases,WorldHealthOrganization,Geneva,Switzerland
DrM.NtuliMalecela,DepartmentofControlofNeglectedTropicalDiseases,WorldHealthOrganization,Geneva, Switzerland
DrJ.R.FrancoMinguell,Innovative&IntensifiedDiseaseManagement,DepartmentofControlofNeglectedTropicalDiseases,WorldHealthOrganization,Geneva,Switzerland
DrR.Minghui,HIV/AIDS,Tuberculosis,MalariaandNeglectedTropicalDiseases,WorldHealthOrganization,Geneva, Switzerland
DrG.Priotto,Innovative&IntensifiedDiseaseManagement,DepartmentofControlofNeglectedTropicalDiseases,WorldHealthOrganization,Geneva,Switzerland
DrP.P.Simarro,Consultant,Geneva,Switzerland


Report of the third WHO stakeholders meeting
on rhodesiense human African trypanosomiasis
Geneva, Switzerland, 10–11 April 2019