rehabilitation in ipf
DESCRIPTION
pulmonologyTRANSCRIPT

REHABILITATION IN IPF
DR.S.YUVARAJAN ,M.D,F.C.C.P(U.S.A)

IDIOPATHIC PULMONARY FIBROSIS IPF is characterized by an inexorable progression
of interstitial fibrosis and worsening gas exchange leading to death from respiratory failure within 5 years of diagnosis in the majority of patients.
IPF typically comes to medical attention later in life,beginning in the sixth decade.

PROBLEMS IN IPF Diagnosis often missed at primary care level Usually present to us very late . No promising treatment till now even after
various clinical trials Distressing symptoms ..

REHABILITATION Rehabilitation is the process of helping a person
to reach the fullest physical, psychological, social, vocational, avocational, and educational potential consistent with his or her physiologic or anatomical impairment, environmental limitations, desires and life plans.
ATS/ERS STATEMENT Pulmonary Rehabilitation is an evidence-based,
multidisciplinary, and comprehensive intervention for patients with chronic respiratory diseases who are symptomatic and often have decreased daily life activities.
Integrated into the individualized treatment of the patient, PR is designed to reduce symptoms, optimize functional status, increase participation and reduce health care costs through stabilizing or reversing systemic manifestations of the disease”

Inactivity(avoiding activity)
Decreased work capacity and increased
shortness of breathMuscle weakness
Increased effort to do work
People with chronic lung diseases are often caught in a vicious circle of deconditioning.

Pulmonary Rehabilitation Objectives
Improve Quality of Life. Improve ability to cope with their illness and
health status. Restore the patient to their highest possible
Functional Capacity. To Lead a Satisfying Life.

BENEFITS OF PULMONARY REHABILITATION

EXERCISE CAPACITY Change in exercise capacity following
pulmonary rehabilitation has been subject to a Cochrane Review.
Exercise capacity improves with pulmonary rehabilitation compared with usual care.
Improvement in dyspnoea Based on various randomised controlled trail,A
consistent finding is a small increase in physical activity following pulmonary rehabilitation, though its clinical significance is unknown.
ACTIVITIES OF DAILY LIVING(ADL)
Self-reported measures of ADL have been shown to be reliable and sensitive to change following pulmonary rehabilitation programmes .
27–30 Prospective uncontrolled studies suggest that pulmonary rehabilitation does impact on ADL.

MUSCLE STRENGTH Improvements in muscle strenghth after
rehabilitation eventhough the studies are sparse.
Pulmonary rehabilitation has only a minor effect on body weight.
Nutritional status at the start of rehabilitation does not affect outcomes such as exercise capacity or health status.
Assessment for pulmonary rehabilitation
History smoking status MRC Dyspnoea scale(usually given for
patients with MRC >3) chronic respiratory failure cardiovascular co morbidities. Anxiety and depression

SYMPTOM ASSESSMENT Dyspnoea by borg scale Cough Fever Pedal edema Reflux Fatigue Chest pain

EXERCISE ASSESSMENT Physical limitations Strength,Range of motion, posture,functional
abilities and activities. Orthopedic limitations. Exercise tolerance(six minute walk test) Exercise induced hypoxemia. Gait and balance

PAIN ASSESSMENT Pain needs to be assessed at initial
assessment Pain should also be assessed during all �
exercise sessions Use a 1-10 pain scale�

EXCLUSION Patients with Unstable cardiac
disease,locomotor disease,neurologic(severe arthritis peripheral vascular disease
Patients in terminal phase of illness. Presence of significant cognitive and
psychiatric impairment

STRUCTURE OF AN IDEAL REHABILITATION PROGRAMME
Minimum of twice-weekly supervised sessions in OPD.
Most pulmonary rehabilitation studies showing benefit in the key outcome measures are based on at least two supervised pulmonary rehabilitation sessions a weeK

Each programmes ideally of 6 to 12 weeks.
The reported exercise and health status benefits of pulmonary rehabilitation have been based predominantly on supervised pulmonary rehabilitation programmes.
Home-based pulmonary rehabilitation can lead to similar improvements in walking distance compared with supervised hospital pulmonary programmes.
However, the educational needs, supervision, patient selection and provision of exercise equipment need to be considered.

SETTING A GOAL While generic exercise training is
recommended as opposed to an individually targeted exercise programme, the prescription of exercise is individualised to provide correct intensity.
▸ The term ‘goal setting’ may require discussion with the patient.

ADJUNTS TO PULMONARY REHABILITATION
Inspiratory muscle training (IMT); Nutritional supplements; Non-invasive ventilation (NIV); oxygen; Heliox and neuromuscular electrical
stimulation (NMES). Very few studies to prove it

SUPPLEMENTAL OXYGEN Supplemental oxygen is needed all patients
with hypoxemia

Pulmonary Rehabilitation Components• Medical Management• Education• Breathing Retraining• Anxiety Control• Emotional Support• Exercise

“How does IPF affect your life?”(results of interviews with 20 IPF pts.)
Symptoms: Cough, shortness of breath IPF therapy: Oxygen, side effects of meds Sleep: disturbed sleep Exhaustion: lack of energy, fatigue Forethought: need to always plan ahead Employment: finances, work, security
Swigris et al. Health Qual Life Outcomes 2005

“How does IPF affect your life?” cont’d
Dependence: need to rely on others Family: impact on family relationships Sexual Relations: limitations on activity Socialization/Leisure: social isolation Mental and Spiritual: fear, worry Mortality: feelings about death
Swigris et al. Health Qual Life Outcomes 2005

Managing Symptoms and Improving Function
Learn strategies to manage symptoms of shortness of breath and cough
Keep moving: options for exercise

“If I could just get rid of the cough…”
Effect on family Embarrassment Sick to stomach Retching Incontinence Headache Ache all over Breathlessness Hurts to breathe
Exhausted Unable to do activities Dizziness Rib fractures Sleep interruption Can’t phone, talk, sing,
laugh Decreased
socialization Change in lifestyle
Adapted from: French TF et al. Chest, 2002;121, French TF et al. Chest 2004;125
How to Manage the Cough Manage GERD,UACS,Asthma Eliminate post nasal drip Try medications to suppress cough:
› Inhaled Steroids › Guaifenesin › Benzonatate › Oral Steroids › Nebulized anesthetics (Lidocaine)› Opiates (Codeine, Morphine)› Experimental: baclofen, neurontin,
thalidomide

More on Managing Cough Try lozenges, honey & lemon, hot
water... Avoid irritants, triggers

Managing Shortness of Breath
› Exercise› Fan/cold air› Relaxation› Distraction› Yoga› Oxygen› Opiates

Education Components Anatomy & Physiology Time and Energy Conservation Stress Management Nutrition Sexuality Medications Aerobic Exercise & Weight Training Coping and Panic Control

Benefits of Exercise Builds endurance Strengthens muscles “Desensitizes” you to SOB Improves mood Allows you to maintain an independent life,
to travel, and to socialize Maintains ideal weight Decreases anxiety

Aerobic Exercise Facts
• Two to three weeks to begin improving your fitness level.
• 6 weeks to 3 months to achieve significant improvement.
• 2 days of inactivity is enough to lose your endurance.
• Most of the exercise benefits will be lost within 2 weeks of inactivity.
• PR exercises are traditionally focussed on lower limb exercises with treadmill and cycle ergometer.
• Because improvement is specific to those muscles trained upperlimb exercises should also be incorporated in the program

ENDURANCE TRAINING Endurance training in the form of cycling or
walking exercises is the most commonly applied exercise training modality in pulmonary rehabilitation.
Optimally, the approach consists of relatively long exercise sessions at high levels of intensity (60% maximal work rate). But this is difficult in IPF patients.
.

The total effective training time should ideally exceed 30 minutes .
However, for most of the patients, it may be difficult to achieve this target training time or intensity, even with close supervision . In this situation, interval training may be a reasonable

RESISTANCE TRAINING Strength or resistance training also
appears to be worth while in chronic respiratory diseases.
This type training improves muscle mass and strength than endurance training.

ADDITIONAL STRATEGIES TO IMPROVE THE EXERCISE CAPACITY
Bronchodilators for those with significant airflow limitations.
Oxygen therapy Nutritional supplementation with high
calories

NOVEL METHODS USING A HARMONICA
Controls inhalation/exhalation and prevents airway collapse.
Teaches the patient to breathe slowly. Forces the lungs to expand &recoil Strengthens the diaphragm. Regulates the use of abdominal costal
muscles



DURATION Ideally upto 12 weeks ,can be increased to
3 months/6 months, Longer the duration, the more benefits you
get from it. 4-6 wk. program, 2-3 hr. sessions of
exercise and education, 2-3 x week

VACCINATION Vaccination against influenza and
pneumococcal infection should be encouraged in all patients with idiopathic pulmonary fibrosis.
PULMONARY REHABILITATION –A REAL DIALEMMA IN IPF
Although patients are referred to pulmonary rehabilitation to reduce dyspnoea, it is often the severity of breathlessness that prevents patients gaining more from pulmonary rehabilitation.
.
This dilemma encourages us to revisit a number of questions regarding the optimal duration and frequency of pulmonary rehabilitation programs, how to best prescribe exercise to minimize dyspnoea and how to optimize the volume and intensity of exercise for IPF patients with differing severities of dyspnoea

EXERCISE PRESCRIPTION IN IPF
It is highly possible that patients at any MRC grade may improve more , if we were able to prescribe exercise to optimally balance patient comfort and exertional symptoms ,while still focusing on performing an appropriate intensity and volume of exercise for physiological adaptation.

CTD.. It is highly likely that patients with IPF may
obtain greater benefits by having longer programs or more frequent visits to pulmonary rehabilitation that ease patients into exercise in smaller doses at lower intensities.

This would allow individuals to build up the volume of exercise they can perform more slowly and would potentially lead to greater benefits, more successful behaviour changes and improved long-term activity adherence..
MAKING FRIENDS IN PR
Click icon to add picture

PR in Pulmonary Fibrosis Patients: What Are the Benefits?
Previously, benefits of PR were only studied and documented in patients with COPD (emphysema and chronic bronchitis)
Recently there is increased interest and research data supporting equal benefit of PR for patients with ILD

“Effectiveness of PR in Restrictive Lung Disease (RLD)”
26 pts. with RLD completed 8 wk. PR PFTs, 6MW, QOL at baseline, 8 wks, & 1 yr. Shuttle Walk Test increased by 61 meters Treadmill time increased from 12 to 21
min. Improvements in breathlessness, QOL,
anxiety and depression scores post PR Reduced hospital admissions post PR
Naji, N. et al. JCR.26(4):237, July/August 2006.

“PR Outcomes for Patients Referred from an Interstitial Lung Disease Clinic”
152 pts. from Stanford’s ILD clinic were referred to 19 different California PR programs between 4/02-1/08
About 1/3 (32%) completed PR Reasons for not completing PR included
being too sick, financial reasons, already exercising, distance/transportation and other
Jacobs, S., Hunter,T., Mohabir, P., Rosen., G., Abstract ;American Thoracic Society Mtg, 2007.
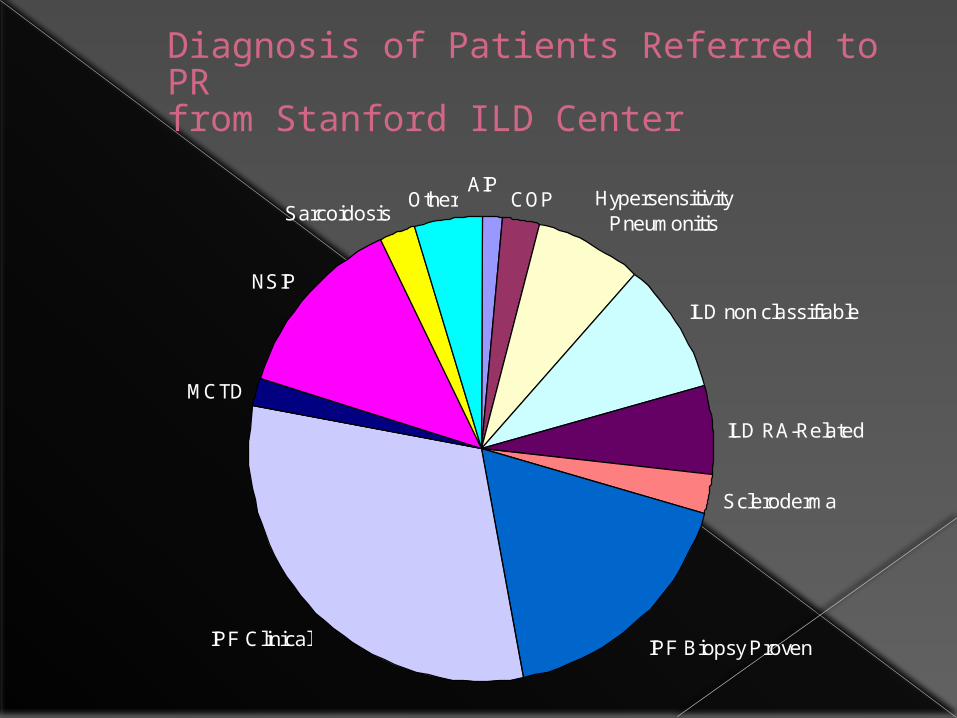
Diagnosis of Patients Referred to PRfrom Stanford ILD Center
COP Hypersensitivity Pneumonitis
ILD non classifiable
ILD RA-Related
Scleroderma
IPF Biopsy Proven
MCTD
NSIP
SarcoidosisOther
IPF Clinical
AIP

“PR Outcomes for Patients Referred from an Interstitial Lung Disease Clinic”
Summary:› 6 minute walk distance and total aerobic
exercise time significantly increased pre to post PR
› Dyspnea measured immediately post-exercise using the modified Borg (0-10 scale ) significantly decreased pre to post PR
› 24hr. oxygen-dependent ILD pts. experienced similar gains in 6MW distance pre to post rehab compared to non-oxygen dependent ILD pts.
Jacobs, S., Hunter,T., Mohabir, P., Rosen., G., Abstract ATS, 2007.

“Effects of PR in patients with idiopathic pulmonary fibrosis”
30 pts. with IPF were randomly assigned to usual care or a 10 week pulm. rehab program
Pulmonary function tests, 6 min. walk test, QOL, and breathlessness scores were measured before and after the program in both groups
RESULTS: – No change in pulmonary function tests before and after PR– Increased 6MW distance of 46 meters in PR group– Improved QOL scores in PR group
Nishiyama,O et al. Respirology , 2008 . V13, 394-399.

“Effects of PR in patients with idiopathic pulmonary fibrosis”
Variable ControlGroup
RehabGroup
DifferenceBetween Groups
P
BDI breathlessness
8.0 (2.2) 6.7 (1.3) +0.4 No difference
SGRQ QOL 40.9 47.3 -6.1 <0.05
6MW, meters 427 (130) 473 (84) +46.3 <0.01
Breathing testFVC (forced Vital Capacity)
2.0 (0.8) 2.1 (0.4) +0.03 No difference
Nishiyama,O et al. Respirology , 2008 . V13, 394-399.

Effect of home-based pulmonary rehabilitation in patients with idiopathic pulmonary fibrosis. Multidisciplinary Respiratory Medicine 2010
A home-based pulmonary rehabilitation program was carried out in 17 IPF patients for 12 weeks..
A significant decrease in perceived dyspnea (p = 0.003) and leg fatigue (p < 0.05) severities, and an increase in the 6MWD (p = 0.04) and general health related quality of life scores..

Exercise limitation and Rehab in IPF(2014)Robert M. Jackson , MD 1 , Carol F. Ramos , MD 2 Am j resp and critical care medicine
Subjects in rehab group when compared to control showed
Increase in Treadmill time, Increase in 6 min walk distance Increase in maximum insp.pressure(MIP)

Exercise Stops the Downward Spiral of Dyspnea - Anxiety - Decreased Activity
Shortness of Breath
Anxiety
Decreased Activity
Shortness of Breath
Anxiety
Shortness of Breath
Interrupt
Inspiration!
Motivation!

THANKS