registry-based quality improvement in anticoagulation geoffrey barnes, md cardiovascular and...
TRANSCRIPT

Registry-based Quality Improvement in Anticoagulation
Geoffrey Barnes, MDCardiovascular and Vascular Medicine
University of Michigan, USA
1st Qatar Conference on Safe Anticoagulation Management
February 28, 2015

Outline
• What is Quality Improvement (QI) in Anticoagulation?
• The case for QI in Anticoagulation Clinics (ACSs)
• Potential targets for QI efforts• Example QI projects• Resources for QI projects

Outline
• What is Quality Improvement (QI) in Anticoagulation?
• The case for QI in Anticoagulation Clinics (ACSs)
• Potential targets for QI efforts• Example QI projects• Resources for QI projects

Quality Improvement
High Quality Anticoagulation• Appropriate Drug
Selection• In-range INRs• Reliable Follow Up
Fewer Unwanted Outcomes
• Bleeding Events
• Strokes• Emergency
Department Visits

Quality Improvement
High Quality Anticoagulation
Fewer Unwanted Outcomes
Time in Therapeutic Range (TTR)

0.0010.00
20.0030.00
40.0050.00
60.0070.00
80.0090.00
100.000
1
2
3
4
Days
INR
Time in the Therapeutic Range
• Rosendaal Method (aka linear interpolation)
0.0010.00
20.0030.00
40.0050.00
60.0070.00
80.0090.00
100.000
1
2
3
4
Days
INR
Rosendaal Thromb Haemost 1993
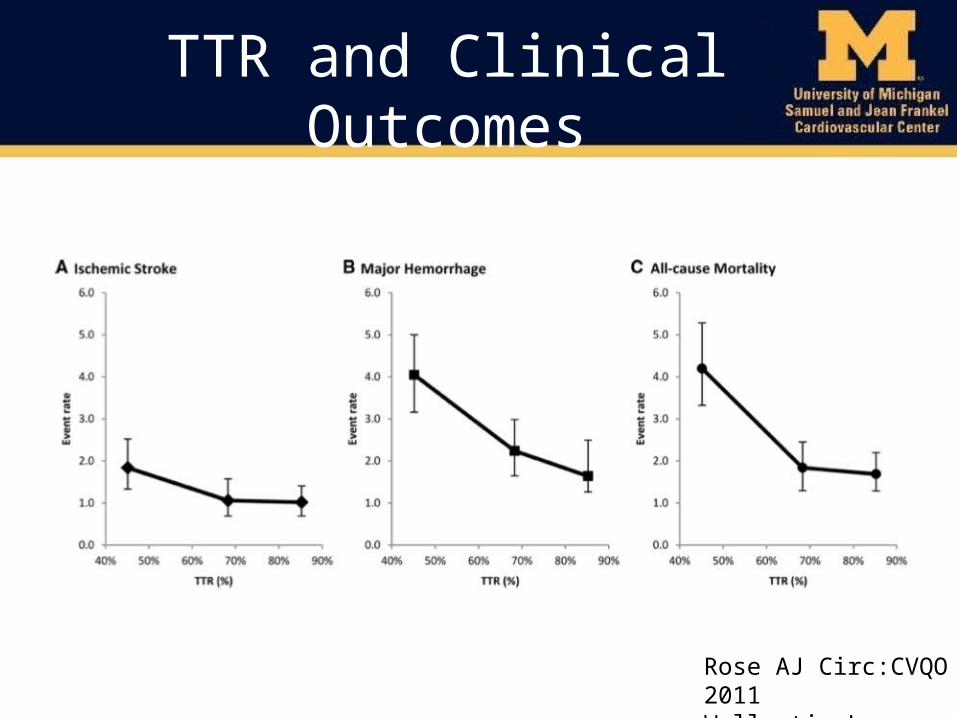
TTR and Clinical Outcomes
Rose AJ Circ:CVQO 2011Wallentin L Lancet 2010

Outline
• What is Quality Improvement (QI) in Anticoagulation?
• The case for QI in Anticoagulation Clinics• Potential targets for QI efforts• Example QI projects• Resources for QI projects

The case for QI
• Common medications– Warfarin– Direct oral anticoagulants (DOACs)
• Highly effective• Potentially devastating side effects

Adverse Drug Events
• Anticoagulants– Up to 10% of all adverse drug events in US– Warfarin #1 cause
• Call for tools to improve care delivery– National Quality Forum
US Dept of Health and Human Services “National Action Plan for Adverse Drug Event Prevention” (2014)National Quality Forum’s 34 Safe Practices (2013) www.hfap.org/pdf/patient_safety.pdf

QI and Cost-Savings
Rose AJ Circ:CVQO 2011

QI and DVT/PE
• Poor Anticoagulation VTE Recurrence– Hospitalization costs– Post Thrombotic Syndrome risk
• Better Anticoagulation Post Thrombotic Syndrome– Economic burden: ~$200 million/year
Kachroo Am J Health Syst Pharm 2012;69:567Lin J Manag Care Pharm 2014;20:174

Quality Improvement
High Quality Anticoagulation• Appropriate Drug
Selection• In-range INRs• Reliable Follow Up
Fewer Unwanted Outcomes
• Bleeding Events
• Strokes• Emergency
Department Visits

Outline
• What is Quality Improvement (QI) in Anticoagulation?
• The case for QI in Anticoagulation Clinics (ACSs)
• Potential Measures of QI efforts• Example QI projects• Resources for QI projects

Quality Measures
• Key Criteria– Commonly occurring events– Linked to important clinical outcomes– Able to be measured
• Two Types– Patient-centered– Provider-centered

Quality MeasuresPatient-Centered
Rose AJ Jt Comm J Qual Patient Saf 2009Witt D J Thromb Thrombolysis 2011Ibrahim S J Thromb Haemost 2013Witt DM Thromb Research 2013
Patients
Intermediate Measures• TTR• % INR In-Range• % Missed INR
Draws• # Extreme INRs
Clinical Outcome• Bleeding Event• Stroke• Emergency Room
Visit

Quality MeasuresProvider-Centered
• Process of Care– # INRs in first 2 weeks– Time from initiation to therapeutic INR– Time from out of range INR to patient contact
• Population-focused– % of patients receiving appropriate anticoagulation
• Guideline-based care• Appropriate drug choice/dose
– % of patients with appropriate INR target range– % receiving appropriate education
Rose AJ Jt Comm J Qual Patient Saf 2009Witt D J Thromb Thrombolysis 2011

Potential QI Targets
• Use guidelines to guide targets (CHEST 2012)– Compliance with specific recommendations
• Other targets in the Literature– Dose adjustment• Agreement between providers• Agreement with nomograms
– Time between INR checks– Workload evaluation
Holbrook A CHEST 2012Witt D J Thromb Haemost 2011

Outline
• What is Quality Improvement (QI) in Anticoagulation?
• The case for QI in Anticoagulation Clinics (ACSs)
• Potential targets for QI efforts• Example QI projects• Resources for QI projects

Michigan Anticoagulation Quality Improvement Initiative
• Six Anticoagulation Management Services
• BCBSM Sponsored CQI• Any indication for
warfarin• Oct 2009-present• ~9200 patients

Atrial Fibrillation
• 1852 AF patients– 24 (1.3%) with CHADS-VASc=0 and no
Cardioversion/Ablation• Potential for harm with overtreatment?
Barnes GD J Thromb Thrombolysis 2014

Atrial Fibrillation
• Screen all AF patients for appropriate anticoagulation– CHADS-VASc=0– No cardioversion or ablation procedure– No other indication for anticoagulation
• Intervention– E-mail, phone call to referring provider– Verify risk elements– Education about guidelines– Ask if warfarin should be discontinued

Provoked DVT Patients
Surgically Provoked
Unprovoked
Non-surgically Provoked
Baglin T Lancet 2003
Provoked DVT Patients
• Patients treated for DVT for 3+ months– Recent surgery (6 wks)– Recent immobilization (6 wks)– No other indication for warfarin
• Intervention– E-mail, phone call to referring provider– Verify provoked nature of DVT– Education about guidelines– Ask if warfarin should be discontinued

Adverse Events Review
• Goal: – Review adverse events in a systematic format
• Structure:– Monthly meeting– MD, RN, PharmD– 2-4 cases
• Format: – Root-cause analysis

Adverse Events Review
• 84yo woman– Paroxysmal AF on warfarin (CHADS2=2)– INR always well controlled (3 yrs)
• Ophthalmology evaluation for “spots in eyes”– Age-related macular degeneration– Treated with AREDS
• Vitamins to slow progression of disease• No feedback to ACS
• 3 weeks later, groin pain– ED eval: retroperitoneal hematoma– INR 10.4

Adverse Events Review
• AREDS – High dose vitamins/minerals– A, C, E, zinc, copper
• Vitamin E potentiates warfarin
• Reviewed by committee• Feedback to Ophthalmology Department– Updated printout given to patients
• Education to all Anticoag RN/PharmDs

Extended INR Testing Interval
• CHEST Guidelines suggests up to 12 week testing intervals (Grade 2B)– Stable patients
• 12 weeks INR in range• No warfarin dose change
• Our clinics– Allow 6-12 week intervals between INR checks
• Initial 6 month data– 222/889 (25%) of eligible patients were “extended”– No difference in safety outcomes
Holbrook, CHEST 2012;144:e152S-184SSchulman, Ann Int Med 2011; 155:653-659

Direct Oral Anticoagulants
• Inappropriate use Bleeding Risk– Up to 25% of dabigatran and rivaroxaban patients– Need adjustment for renal function
• Anticoagulation Clinic Support– Verify dose, drug– Education for patient• 17% without education at Hamad General Hospital -
2008
– Follow up dosing changes (especially VTE)Harper P, NEJM 2012. Larock AS, Ann Pharmacother 2014Steinberg BA, JAHA 2013. Khudair Saudi Med J 2010;31:672

Middle East Example
Only60%
Angiology 2014:1-8

Outline
• What is Quality Improvement (QI) in Anticoagulation?
• The case for QI in Anticoagulation Clinics (ACSs)
• Potential targets for QI efforts• Example QI projects• Resources for QI projects

QI Resources
• Published Guidelines– CHEST 2012 Guidelines– AC Forum Delivery of Optimized Anticoagulant
Therapy• Online References– AC Forum Centers of Excellence Website– MAQI2 Anticoagulation Toolkit
Holbrook A CHEST 2012Garcia DA Ann Pharmacother 2008

QI Resources
www.anticoagulationtoolkit.org

QI Resources
• Need for anticoagulation?– AF Risk assessment tools– VTE Risk assessment tools
• Which anticoagulant to select?– FDA approval list– Comparison between classes– Patient factors that influence
choice
• How to initiate warfarin– Dosing algorithms– Educational tools– Other considerations– Drug-drug interactions– Dietary interactions
• DOAC initiation– Conversion to/from warfarin– Drug-drug interactions– Educational tools
• Long-term warfarin management– Dose adjustment algorithms– Periprocedural management– Key follow up questions
• All available via PDF
• Interactive tool and iPhone app

QI Resources

QI Resources

QI Resources
Excellence.acforum.org

Questions