regis h. turocy, dhce, pt, ecs assistant professor school ... · case study #1 (continued)...
TRANSCRIPT
Strain & Strain & CounterstrainCounterstrain
Regis H. Turocy, DHCE, PT, ECSRegis H. Turocy, DHCE, PT, ECSAssistant ProfessorAssistant Professor
School of Physical TherapySchool of Physical TherapySlippery Rock University of PASlippery Rock University of PA

Concepts of Strain/Concepts of Strain/CounterstrainCounterstrain
Rooted in antiquity:Rooted in antiquity:Body positioningBody positioningUse of tender pointsUse of tender pointsIndirect techniquesIndirect techniques

Origin of Strain/Origin of Strain/CounterstrainCounterstrainFirst Observation First Observation -- The DiscoveryThe DiscoverySecond Observation:Second Observation:> > Missing tender points Missing tender points -- anterior anterior
producing pain posteriorproducing pain posterior> Tender points in extremities were not > Tender points in extremities were not
found in the muscle strained but in the found in the muscle strained but in the antagonistantagonist
> Treating extremities involves greater > Treating extremities involves greater amplitude of movementamplitude of movement

Definition Definition -- 11
A passive positional procedure that places A passive positional procedure that places the body in a position of greatest comfort, the body in a position of greatest comfort, thereby relieving pain by reduction and thereby relieving pain by reduction and arrest of inappropriate arrest of inappropriate proprioceptorproprioceptoractivity that maintains somatic dysfunctionactivity that maintains somatic dysfunction
Definition Definition -- 22
A mild overA mild over--stretching applied in a stretching applied in a direction opposite to the false and direction opposite to the false and continuing message of strain which the continuing message of strain which the body is suffering. body is suffering. –– This is accomplished by shortening the This is accomplished by shortening the
muscle containing the false strain message so muscle containing the false strain message so much that it stops reporting the strain (indirect much that it stops reporting the strain (indirect technique).technique).

Musculoskeletal DysfunctionMusculoskeletal DysfunctionStructural ModelStructural Model–– Associated with anatomic and postural Associated with anatomic and postural
deformation of tissuedeformation of tissue
Functional ModelFunctional Model–– Biomechanical, nonBiomechanical, non--linear somatic disturbance linear somatic disturbance
creating tissue that results in pain, loss of creating tissue that results in pain, loss of motion/tissue extensibility, movement motion/tissue extensibility, movement imbalances, leading to decreased functionimbalances, leading to decreased function

Rationale for Rationale for Strain/Strain/CounterstrainCounterstrain
Based on the work of Irvin Based on the work of Irvin KorrKorr, Ph.D, Ph.D““ProprioceptorsProprioceptors and Somatic Dysfunction”and Somatic Dysfunction”
Journal of The American Osteopathic Association, March Journal of The American Osteopathic Association, March 1975, 1975, VolVol 74 (7)74 (7)
Proposed a neural basis for joint Proposed a neural basis for joint dysfunction incriminating the muscle dysfunction incriminating the muscle spindlespindle

Musculoskeletal System and Musculoskeletal System and ProprioceptiveProprioceptive ReflexesReflexes
RuffiniRuffini ReceptorsReceptors–– Found in joint capsule Found in joint capsule –– Report position, velocity, direction of Report position, velocity, direction of
movementmovement
GolgiGolgi Tendon Organs (GTO)Tendon Organs (GTO) –––– MusculotendinousMusculotendinous junction junction –– Monitors excessive tensionMonitors excessive tension

Muscle SpindleMuscle SpindleLocated between muscle fibers Located between muscle fibers Very sensitive to position, load, and velocityVery sensitive to position, load, and velocity
Korr’sKorr’s RevelationsRevelations
Dysfunction that characterizes the osteopathic Dysfunction that characterizes the osteopathic lesion does not arise in the joint, but are lesion does not arise in the joint, but are imposed by muscles that traverse the jointimposed by muscles that traverse the joint
Blames the primary or Blames the primary or annulospiralannulospiralproprioceptorproprioceptor reflexes in the muscle spindlereflexes in the muscle spindle
Increased gamma discharge exaggerates Increased gamma discharge exaggerates afferent discharge from spindle causing reflex afferent discharge from spindle causing reflex spasm which fixates joint in certain positionspasm which fixates joint in certain position

Jones Neuromuscular ModelJones Neuromuscular Model

Jones’s PostulatesJones’s Postulates
Not a lesion but an onNot a lesion but an on--going going neuromuscular noxious stimulusneuromuscular noxious stimulus
For success hyperFor success hyper--stimulated muscle must stimulated muscle must return to neutral length slowlyreturn to neutral length slowly
In spite of subjective pain and weakness in In spite of subjective pain and weakness in strained muscle, objective evidence in strained muscle, objective evidence in antagonist of painful muscleantagonist of painful muscle

Jones’s PostulatesJones’s Postulates
POC and lasting relief POC and lasting relief –– maximum maximum shortening of antagonist and repeated shortening of antagonist and repeated stretch of painful musclestretch of painful muscle
Treatment does not cure, it decreases or Treatment does not cure, it decreases or eliminates irritation and allows body to eliminates irritation and allows body to heal itselfheal itself

The Facilitated SegmentThe Facilitated Segment
A lesion represents a facilitated segment A lesion represents a facilitated segment of the spinal cord, maintained in that state of the spinal cord, maintained in that state by impulses of endogenous origin entering by impulses of endogenous origin entering the corresponding dorsal root. the corresponding dorsal root.
All structures receiving efferent nerve All structures receiving efferent nerve fibers from that segment are potentially fibers from that segment are potentially exposed to excessive stimulation or exposed to excessive stimulation or inhibition.inhibition.

The Facilitated SegmentThe Facilitated Segment
When these impulses extend beyond their When these impulses extend beyond their normal sensorynormal sensory--motor pathways, the CNS motor pathways, the CNS begins to misinterpret the information due begins to misinterpret the information due to an overflow of neurotransmitter to an overflow of neurotransmitter substance within the involved segmentsubstance within the involved segment

The Facilitated SegmentThe Facilitated Segment

Characteristics of a Facilitated Characteristics of a Facilitated SegmentSegment
HyperHyper--excitabilityexcitability ––A minimal impulse produces excessive A minimal impulse produces excessive responsesresponses
Overflow Overflow ––Impulse may “spill over” to adjacent pathwaysImpulse may “spill over” to adjacent pathways
Autonomic dystrophyAutonomic dystrophy ––Sympathetic ganglia become overSympathetic ganglia become over--stimulated stimulated which decreases healing potentialwhich decreases healing potential

Somatic Dysfunctions Somatic Dysfunctions -- “ART”“ART”
Somatic dysfunction detectable by Somatic dysfunction detectable by physiological manifestations in:physiological manifestations in:
AAsymmetrysymmetry
RRestricted motionestricted motion
TTexture abnormalities and tender pointsexture abnormalities and tender points

Summary Summary -- L.H. Jones, 1995L.H. Jones, 1995

Somatic DysfunctionSomatic Dysfunction
ExtraExtra--articulararticularManifestation of abnormal Manifestation of abnormal proprioceptiveproprioceptiveactivity (muscle spindle)activity (muscle spindle)Inability of muscle spindle to reset is what Inability of muscle spindle to reset is what maintains joint dysfunctionmaintains joint dysfunction

What is a Tender Point?What is a Tender Point?
Small zones of tense, tender, edematous Small zones of tense, tender, edematous muscle and muscle and fascialfascial tissue about 1 cm in tissue about 1 cm in diameterdiameterSensory manifestations of a Sensory manifestations of a neuromuscular or musculoskeletal neuromuscular or musculoskeletal dysfunctiondysfunctionManifestation of facilitated segmentManifestation of facilitated segmentDiagnostic indicatorDiagnostic indicator

Tender PointsTender Points
Jump Sign:Jump Sign: patient / athlete will respond patient / athlete will respond to pressure by moving awayto pressure by moving away
Grimace Sign:Grimace Sign: visual representation of visual representation of tenderpointtenderpoint

Goals of Strain/Goals of Strain/CounterstrainCounterstrain
An indirect technique to restore tissue to An indirect technique to restore tissue to normal physiological functionnormal physiological function
Uses 2Uses 2 3 planes of movement to place 3 planes of movement to place tissue in tissue in position of comfortposition of comfort (POC)(POC)
POC is reached when palpable POC is reached when palpable tenderness of TP softens and or tenderness of TP softens and or decreases (decreases (comfort zonecomfort zone))
Finding the Position of ComfortFinding the Position of Comfort
Patient feedbackPatient feedback
Palpating the mobile point which is the Palpating the mobile point which is the point of maximum ease or relaxation. It is point of maximum ease or relaxation. It is the ideal position for a releasethe ideal position for a release

Mobile PointMobile Point -- L.H. Jones, 1995L.H. Jones, 1995

Effects of Strain/Effects of Strain/CounterstrainCounterstrain
Normalization of muscle Normalization of muscle hypertonicityhypertonicityNormalization of Normalization of fascialfascial tensiontensionReduction of joint Reduction of joint hypomobilityhypomobilityIncreased circulationIncreased circulationDecreased swellingDecreased swellingDecreased painDecreased painIncreased strength, movement, functionIncreased strength, movement, function

Treatment TechniquesTreatment Techniques
Locate the tender point (Locate the tender point (TPTP))Apply subApply sub--threshold pressure on tender threshold pressure on tender point while finding POC or mobile pointpoint while finding POC or mobile pointMonitor point response but take pressure offMonitor point response but take pressure offHold for 90 secondsHold for 90 secondsReturn to neutral slowlyReturn to neutral slowlyRecheck tender point Recheck tender point

General Treatment PrinciplesGeneral Treatment PrinciplesHold POC for no less than 90 secondsHold POC for no less than 90 secondsReturn to neutral slowlyReturn to neutral slowlyAnterior tender points are usually treated in Anterior tender points are usually treated in flexionflexionPosterior tender pints are usually treated in Posterior tender pints are usually treated in extensionextensionTender points on or near the midline are Tender points on or near the midline are treated with more flexion and extensiontreated with more flexion and extensionTender points lateral from the midline are Tender points lateral from the midline are treated with more rotation and sidetreated with more rotation and side--bendingbending

General Treatment PrinciplesGeneral Treatment Principles
With multiple tender points, treat the most With multiple tender points, treat the most severe firstsevere firstIf the tender points are in rows, try treating If the tender points are in rows, try treating the one in the middle firstthe one in the middle firstTreat area with greatest number of Treat area with greatest number of TPsTPs firstfirstTender points in the extremities are usually Tender points in the extremities are usually found on the opposite side of painfound on the opposite side of painMay get sore following treatmentMay get sore following treatment

General Treatment PrinciplesGeneral Treatment Principles
Associated Postural deviations:Associated Postural deviations:Major Posterior TPMajor Posterior TP
Flattened forward curves or accentuated Flattened forward curves or accentuated backward curves backward curves
Major Anterior TPMajor Anterior TPAccentuated forward curves and flattened Accentuated forward curves and flattened backward curves backward curves
Posterior TPPosterior TPPain specific in posterior regionPain specific in posterior region
Anterior TP Anterior TP Diffuse or large areas of painDiffuse or large areas of pain

Scanning EvaluationScanning Evaluation
Evaluate for multiple tender pointsEvaluate for multiple tender points
Record the severity of the tender pointsRecord the severity of the tender points–– + jump sign (extremely severe)+ jump sign (extremely severe)–– + grimace (very tender)+ grimace (very tender)–– moderatemoderate
Contraindications /PrecautionsContraindications /PrecautionsOpen woundsOpen woundsRecent suturesRecent suturesHealing fracturesHealing fracturesHematomaHematomaHypersensitivity of the skinHypersensitivity of the skinSystemic / localized infectionSystemic / localized infectionAcute MI Acute MI -- PrecautionPrecautionTHP THP -- PrecautionPrecaution

IndicationsIndications
Acute injuries Acute injuries (Sports!)(Sports!)Fragile (osteoporosis)Fragile (osteoporosis)PregnantPregnantPediatricsPediatricsChronic painChronic painPostPost--op (e.g. lumbar, knee, shoulder)op (e.g. lumbar, knee, shoulder)NeurologicNeurologic
IndicationsIndications
Used in conjunction withUsed in conjunction with–– ArticularArticular techniquestechniques–– Muscle energyMuscle energy–– MyofascialMyofascial releaserelease–– ExerciseExercise–– ModalitiesModalities

PostPost--TreatmentTreatment
Always return slowly to neutralAlways return slowly to neutral
Recheck TP after you return to neutralRecheck TP after you return to neutral
Warn patient they may experience Warn patient they may experience increased soreness 24increased soreness 24--48 hours post48 hours post

Case Study #1Case Study #1
Patient: 30 y/o male recreational rugby playerPatient: 30 y/o male recreational rugby player
Injury: 2nd degree MCL strain to right kneeInjury: 2nd degree MCL strain to right knee
WeightWeight--bearing status: WBAT with crutches and bearing status: WBAT with crutches and immobilizerimmobilizer
ROM: (ROM: (--)10^ extension; 30^ flexion)10^ extension; 30^ flexion
Pain: constant 5/10; this would increase to 8/10 Pain: constant 5/10; this would increase to 8/10 with increased weightwith increased weight--bearing and movementbearing and movement
Case Study #1Case Study #1 (continued)(continued)
Palpation: Tender over medial aspect of the Palpation: Tender over medial aspect of the kneeknee
Most dominant tender point Most dominant tender point -- right right paraspinalparaspinal muscles at L3, followed by right muscles at L3, followed by right gluteus gluteus minimusminimus
Treatment: Treatment: TP’sTP’s treated and ROM treated and ROM increased to (increased to (--4) extension and 125^ 4) extension and 125^ flexionflexion

Case StudyCase Study #1 (continued)#1 (continued)
WeightWeight--bearing: Increased with much less bearing: Increased with much less painpain
Results: After two treatments patient was Results: After two treatments patient was off crutches, with full ROM and exercising off crutches, with full ROM and exercising without painwithout pain

Case StudyCase Study #2 #2 –– Acute LBPAcute LBP
Patient: 35 Patient: 35 y/oy/o female custodianfemale custodian
Injury: Progressive increase in right sided Injury: Progressive increase in right sided LBP after lifting incident 2 weeks agoLBP after lifting incident 2 weeks ago
Trunk ROM: Limited and painful; Trunk ROM: Limited and painful; flexion>extension>lateral flexion/rotationflexion>extension>lateral flexion/rotation
Neurological: NormalNeurological: Normal

Case Study #2Case Study #2 (continued)(continued)
Pain: constant 5/10; increases to 8/10 Pain: constant 5/10; increases to 8/10 when attempting to lift at workwhen attempting to lift at work
Gait: Gait: antalgicantalgic
Palpation: Palpation: TP’sTP’s over over iliacusiliacus; right L4 and ; right L4 and L5L5
Treatment: Treatment: IliacusIliacus TP with significant TP with significant increase in trunk ROM; L4 and L5 increase in trunk ROM; L4 and L5 TP’sTP’streated with full trunk ROM and no paintreated with full trunk ROM and no pain

SummarySummary
Scan body for TP, grade severityScan body for TP, grade severityFollow general rulesFollow general rulesMonitor TP while finding POCMonitor TP while finding POCMaintain contact with TP while in POCMaintain contact with TP while in POCHold POC until complete releaseHold POC until complete releaseReturn to neutral slowlyReturn to neutral slowlyRecheck TPRecheck TPWarn patient and avoid strenuous activityWarn patient and avoid strenuous activity
That’s All PilgrimsThat’s All PilgrimsQuestions?Questions?

Stain/Stain/CounterstrainCounterstrain LabLab
Posterior Posterior LumbarsLumbarsAnterior Anterior LumbarsLumbarsPosterior PelvisPosterior PelvisAnterior PelvisAnterior PelvisPosterior Posterior SacralsSacrals

Posterior Posterior LumbarsLumbarsD’AmbrogioD’Ambrogio and Roth 1997and Roth 1997

Posterior Posterior LumbarsLumbars
Patient Presentation:Patient Presentation:HyperHyper--lordoticlordotic posturepostureIncreased pain with sittingIncreased pain with sittingDifficulty with flexionDifficulty with flexion

Posterior Lumbar Posterior Lumbar –– LateralLateralD’AmbrogioD’Ambrogio and Roth 1997and Roth 1997

Posterior Posterior LumbarsLumbars 11--55
Location of Tender Points:Location of Tender Points:
Lateral aspect of the Lateral aspect of the spinousspinous processesprocesses
ParaspinalParaspinal sulcussulcus
Posterior aspect of transverse processPosterior aspect of transverse process

Posterior Posterior LumbarsLumbarsD”AmbrogioD”Ambrogio and Roth 1997and Roth 1997

Posterior Posterior LumbarsLumbars 11--55
Position of Treatment:Position of Treatment:Patient lies prone; pillow under chestPatient lies prone; pillow under chest
CAT stands on the side opposite the TPCAT stands on the side opposite the TP
Grasp the anterior aspect of the pelvis on the Grasp the anterior aspect of the pelvis on the TP side; pull TP side; pull posteriorlyposteriorly to create rotation 30 to create rotation 30 --40^40^
Good for severe, acute back painGood for severe, acute back pain

QuadratusQuadratus LumborumLumborum
Position of Tender Point:Position of Tender Point:Lateral aspects of transverse processes Lateral aspects of transverse processes L1L1--L5L5
Pressure Pressure anteriorlyanteriorly then mediallythen medially
Patient PresentationPatient Presentation::–– Limited flexion; tight hamstrings; + SLRLimited flexion; tight hamstrings; + SLR

QuadratusQuadratus LumborumLumborumD”AmbrogioD”Ambrogio and Roth 1997and Roth 1997

QuadratusQuadratus LumborumLumborum
Position of Treatment:Position of Treatment:Patient prone with pillow under chestPatient prone with pillow under chestCAT stands on opposite side and grasps CAT stands on opposite side and grasps iliumilium on affected sideon affected sidePatient then flexes and abducts Patient then flexes and abducts ipsilateralipsilateralhip to 45^hip to 45^

QuadratusQuadratus LumborumLumborum
Position of Treatment:Position of Treatment:Patient prone; sidePatient prone; side--bend trunk toward tender bend trunk toward tender
point; abduct and extend hip and rest on point; abduct and extend hip and rest on operator’s thigh; gently hike hip and fine tune operator’s thigh; gently hike hip and fine tune with rotationwith rotation
Patient lies on unaffected side; hips and knees Patient lies on unaffected side; hips and knees flexed to 90^; CAT stands behind and grasps flexed to 90^; CAT stands behind and grasps ankles and lifts them to induce sideankles and lifts them to induce side--bending; bending; patient protracts or retracts to fine tunepatient protracts or retracts to fine tune
PL 3 (Iliac)PL 3 (Iliac)
Location of Tender Point:Location of Tender Point:3 cm below margin of 3 cm below margin of iliumilium and 7 cm and 7 cm lateral to PSISlateral to PSIS
Pressure applied Pressure applied anteriorlyanteriorly and mediallyand medially

PL 3 (Iliac)PL 3 (Iliac)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997

PL 3 (Iliac)PL 3 (Iliac)
Position of Treatment:Position of Treatment:Patient prone; operator stands on Patient prone; operator stands on opposite side of TPopposite side of TPExtend thigh of affected side and support Extend thigh of affected side and support on thigh of operatoron thigh of operatorOperator then slightly adducts thigh and Operator then slightly adducts thigh and markedly externally rotatesmarkedly externally rotates

PL 4 (Iliac)PL 4 (Iliac)
Location of Tender Point:Location of Tender Point:4 cm below the crest of the 4 cm below the crest of the iliumilium and just and just posterior to the border of the tensor fascia posterior to the border of the tensor fascia latalata
Pressure Pressure anteriomedialanteriomedial

PL 4 (Iliac)PL 4 (Iliac)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
PL 4 (Iliac)PL 4 (Iliac)
Position of Treatment:Position of Treatment:Patient prone and operator stands on the Patient prone and operator stands on the side of the TPside of the TPOperator then extends thigh and supports Operator then extends thigh and supports leg on thighleg on thighLeg then slightly adducted and moderately Leg then slightly adducted and moderately externally rotatedexternally rotated

UPL 5UPL 5
Location of Tender Point:Location of Tender Point:superior medial surface of the PSIS; superior medial surface of the PSIS; pressure applied inferiorly and laterallypressure applied inferiorly and laterallyKEY POINT KEY POINT –– extended L5extended L5
tight hamstringstight hamstrings+ SLR+ SLR

UPL 5UPL 5D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
UPL 5UPL 5
Position of Treatment:Position of Treatment:Patient prone; operator stands on Patient prone; operator stands on opposite side of tender pointopposite side of tender pointOperator extends the hip on affected side Operator extends the hip on affected side and supports leg on thigh; slightly adduct and supports leg on thigh; slightly adduct with mild external rotationwith mild external rotation

LPL 5LPL 5
Location of Tender Point:Location of Tender Point:1.5 to 2 cm inferior to the PSIS in the 1.5 to 2 cm inferior to the PSIS in the sacral notchsacral notchMaverick Point: flexion dysfunction with Maverick Point: flexion dysfunction with TP located TP located posteriorlyposteriorly
If anterior If anterior lumbarslumbars “check out”, look at this “check out”, look at this point; may see with pain on backward point; may see with pain on backward bendingbending

LPL 5LPL 5D”AmbrogioD”Ambrogio and Roth 1997and Roth 1997

LPL 5LPL 5
Position of Treatment:Position of Treatment:Patient pronePatient proneOperator seated on side of tender point; Operator seated on side of tender point; patient moves toward the edge of the table patient moves toward the edge of the table so that leg can be dropped off the table so that leg can be dropped off the table and rest on the operator’s thigh; and rest on the operator’s thigh; Flex hip to 90^, slight adduction and Flex hip to 90^, slight adduction and internal rotation; can retract opposite internal rotation; can retract opposite iliumiliumto fine tuneto fine tune

LPL 5LPL 5
Patient pronePatient proneOperator stands on opposite side of the Operator stands on opposite side of the TP and grasps the TP and grasps the iliumilium at the level of the at the level of the ASIS; ASIS; Patient flexes and abducts leg on affected Patient flexes and abducts leg on affected side; side; iliumilium is retracted and rotated toward is retracted and rotated toward TPTP

Anterior Anterior LumbarsLumbarsD’AmbrogioD’Ambrogio and Roth 1997and Roth 1997

Anterior Anterior LumbarsLumbars
Patient PresentationPatient Presentation::Decreased Decreased lordosislordosisDifficulty with extensionDifficulty with extensionPain with Pain with sidebendingsidebendingIncreased pain with prolonged standing, Increased pain with prolonged standing, walkingwalkingWork on these points before doing EILWork on these points before doing EIL

Anterior Lumbar 1Anterior Lumbar 1
Location of Tender Point:Location of Tender Point:Medial surface of the ASIS; Medial surface of the ASIS;
Press laterally, approximately ¾ inch deepPress laterally, approximately ¾ inch deep

Anterior Lumbar 1Anterior Lumbar 1D”AmbrogioD”Ambrogio and and rothroth 19971997

Anterior Lumbar 1Anterior Lumbar 1
Position of Treatment:Position of Treatment:Patient supine; head of table can be Patient supine; head of table can be raised; raised; Operator stands on side of TP and Operator stands on side of TP and markedly flexes patient’s legs; markedly flexes patient’s legs; Rotate to side of TP and laterally flex Rotate to side of TP and laterally flex toward TP side (or away)toward TP side (or away)
Anterior Lumbar 2Anterior Lumbar 2
Location of Tender Point:Location of Tender Point:InferiorInferior--medial surface of the ASIS; medial surface of the ASIS;
Pressure applied superiorPressure applied superior--lateral (feels like a lateral (feels like a small gland)small gland)

Anterior Lumbar 2Anterior Lumbar 2D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997

Anterior Lumbar 2Anterior Lumbar 2
Position of Treatment:Position of Treatment:Patient is supine; head of table can be Patient is supine; head of table can be raised; raised; Operator stands on opposite side of the Operator stands on opposite side of the TP; TP; Operator flexes patient’s legs to 90^; Operator flexes patient’s legs to 90^; moves knees away from TP side 60^ moves knees away from TP side 60^ (rotation); slightly push feet toward floor to (rotation); slightly push feet toward floor to create side bending away from TP sidecreate side bending away from TP side
AbLAbL 2 (2 (PsoasPsoas))
Location of Tender Point:Location of Tender Point:On the abdomen 5 cm lateral to the On the abdomen 5 cm lateral to the umbilicus and slightly inferior; umbilicus and slightly inferior;
Pressure Pressure posteriorlyposteriorly

AbLAbL 22D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
AbLAbL 22
Position of Treatment:Position of Treatment:Patient is supine with the operator Patient is supine with the operator standing on the side of the TP; standing on the side of the TP; Hips are flexed to 90^; rotates hips 60^ Hips are flexed to 90^; rotates hips 60^ toward TP side and laterally flexes the toward TP side and laterally flexes the hips away from the TP by elevating the hips away from the TP by elevating the feetfeet

AL 3AL 3--44
Location of Tender Point:Location of Tender Point:L3L3
Lateral surface of ASIS; push mediallyLateral surface of ASIS; push mediallyL4 L4
Inferior surface of the ASIS; push Inferior surface of the ASIS; push posteriorlyposteriorlyand then superiorlyand then superiorly

AL 3AL 3--44D”AmbrogioD”Ambrogio and Roth 1997and Roth 1997

AL 3AL 3--44
Position of Treatment:Position of Treatment:Patient is supine with the operator Patient is supine with the operator standing on side opposite the TP; standing on side opposite the TP; Operator flexes patient’s hip 50Operator flexes patient’s hip 50--90^, 90^, laterally flexes hips away from the TP by laterally flexes hips away from the TP by pulling legs toward operator; fine tune by pulling legs toward operator; fine tune by rotating hips toward or away from TProtating hips toward or away from TP

AL 5AL 5
Location of Tender Point:Location of Tender Point:Anterior surface of the pubic boneAnterior surface of the pubic bone
1.5 cm lateral to pubic 1.5 cm lateral to pubic symphysissymphysis

AL 5AL 5D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997

AL 5AL 5
Position of Treatment:Position of Treatment:Patient is supine with the operator Patient is supine with the operator standing on side of TP; standing on side of TP; Patient’s hips are flexed 60Patient’s hips are flexed 60--120^ ; hips 120^ ; hips rotated towards the TP side and laterally rotated towards the TP side and laterally flexes away from TP side (move feet away flexes away from TP side (move feet away from operator)from operator)

Posterior PelvisPosterior PelvisD’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
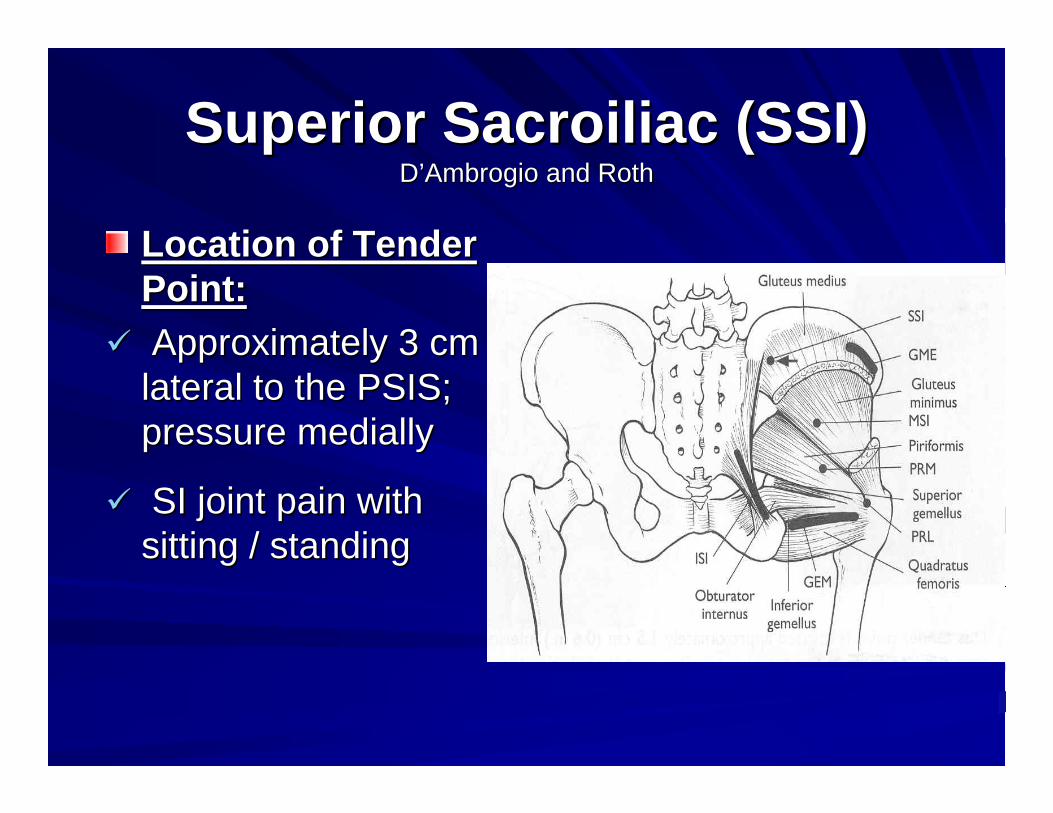
Superior Sacroiliac (SSI)Superior Sacroiliac (SSI)D’AmbrogioD’Ambrogio and Rothand Roth
Location of Tender Location of Tender Point:Point:Approximately 3 cm Approximately 3 cm
lateral to the PSIS; lateral to the PSIS; pressure mediallypressure medially
SI joint pain with SI joint pain with sitting / standingsitting / standing

Superior Sacroiliac (SSI)Superior Sacroiliac (SSI)
Position of Treatment:Position of Treatment:Patient is prone with the operator Patient is prone with the operator standing on the side of the TP; estanding on the side of the TP; eExtend patient’s hip resting leg on Extend patient’s hip resting leg on operator’s thigh; slightly abduct and rotate operator’s thigh; slightly abduct and rotate to fine tuneto fine tuneIf patient has limited hip extension, treat If patient has limited hip extension, treat anteriorsanteriors firstfirst

Middle Sacroiliac (MSI)Middle Sacroiliac (MSI)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point:Tender Point:Middle of the Middle of the
buttocks in a slight buttocks in a slight depression; press depression; press anteriorlyanteriorly and and mediallymedially
Middle Sacroiliac (MSI)Middle Sacroiliac (MSI)
Position of Treatment:Position of Treatment:Patient is prone with the operator Patient is prone with the operator standing on the side of the TPstanding on the side of the TPMarkedly abduct legMarkedly abduct legFine tune with flexion/extension or Fine tune with flexion/extension or internal/external rotationinternal/external rotation

Inferior Inferior ScaroiliacScaroiliac (ISI)(ISI)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Tender Location of Tender Point:Point:Located in a line along Located in a line along the the sacrotuberoussacrotuberousligament from the ligament from the ischialischialtuberositytuberosity to posterior to posterior aspect of the inferior aspect of the inferior lateral angle; lateral angle;
Pressure Pressure anteriorlyanteriorly and and laterallylaterally
Inferior Inferior ScaroiliacScaroiliac (ISI)(ISI)
Position of Treatment:Position of Treatment:Patient prone with the operator on the Patient prone with the operator on the side opposite the TPside opposite the TPOperator reaches across and grasps the Operator reaches across and grasps the leg on the involved side and extends, leg on the involved side and extends, adducts , externally rotates it across the adducts , externally rotates it across the uninvolved leguninvolved leg

PiriformisPiriformis (PRM (PRM –– PRL)PRL)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Tender Location of Tender Point:Point:PRM PRM –– belly of the belly of the piriformispiriformis approximately approximately halfway between the halfway between the inferior lateral angle of the inferior lateral angle of the sacrum and the greater sacrum and the greater trochantertrochanterSI torsions, sciatic SI torsions, sciatic irritation, + SLRirritation, + SLR

PiriformisPiriformis (PRM (PRM –– PRL)PRL)
Position of Treatment:Position of Treatment:Similar to LP5Similar to LP5Patient is prone with operator seated on Patient is prone with operator seated on side of TPside of TPLeg on TP side suspended off table Leg on TP side suspended off table resting on operator’s thighresting on operator’s thighFlex hip from 60 Flex hip from 60 –– 120^, abducted; fine 120^, abducted; fine tune with internal/external rotationtune with internal/external rotation
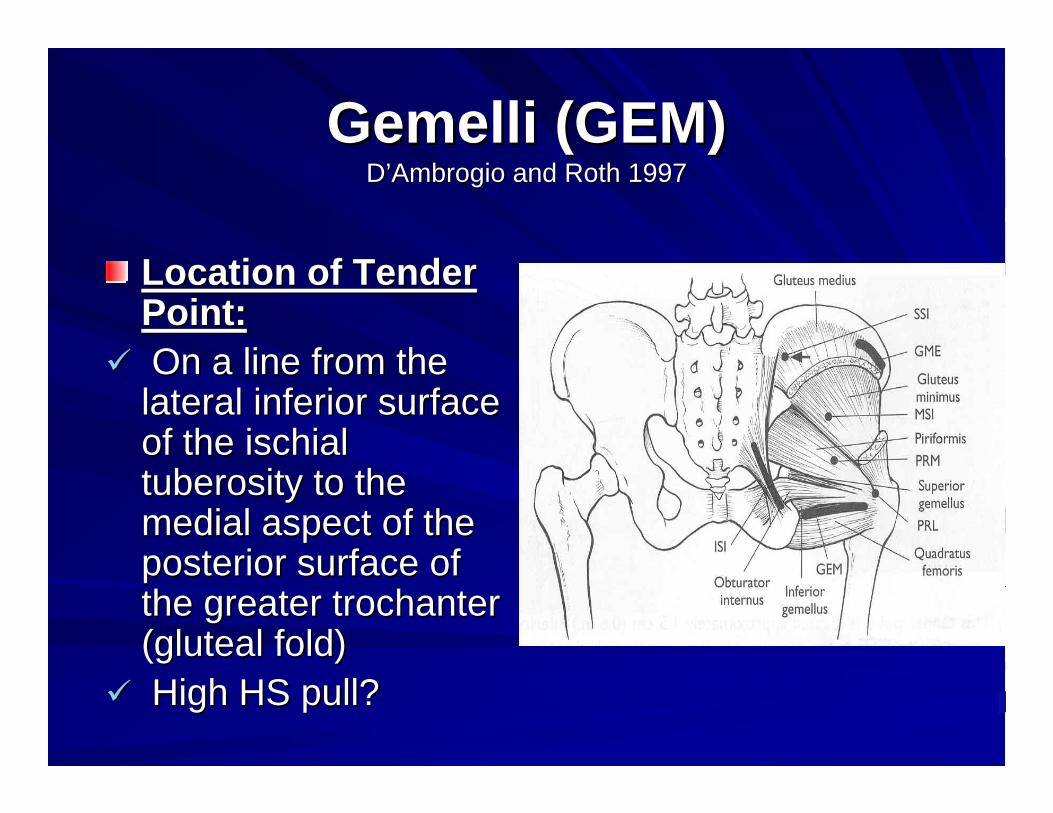
GemelliGemelli (GEM)(GEM)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Tender Location of Tender Point:Point:On a line from the On a line from the
lateral inferior surface lateral inferior surface of the of the ischialischialtuberositytuberosity to the to the medial aspect of the medial aspect of the posterior surface of posterior surface of the greater the greater trochantertrochanter((glutealgluteal fold)fold)High HS pull?High HS pull?

GemelliGemelli (GEM)(GEM)
Position of Treatment:Position of Treatment:Patient is prone, operator on opposite Patient is prone, operator on opposite sidesideOperator pins patient’s ankle in Operator pins patient’s ankle in axillaaxillaLeg is moderately extended, markedly Leg is moderately extended, markedly adducts and externally rotates legadducts and externally rotates leg

Gluteus Gluteus MediusMedius (GME)(GME)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point:Tender Point:On a line 1 cm On a line 1 cm
inferior to the iliac inferior to the iliac crestcrest3 3 –– 5 cm on either 5 cm on either
side of the midside of the mid--axillaryaxillary linelineIliosacralIliosacral dysfunctiondysfunction

Gluteus Gluteus MediusMedius (GME)(GME)
Position of Treatment:Position of Treatment:Patient is prone with operator standing on side Patient is prone with operator standing on side
of TPof TPOperator extends and abducts the leg and rests Operator extends and abducts the leg and rests
the leg in operators thighthe leg in operators thighHip positioned in marked external rotation (Hip positioned in marked external rotation (TPsTPs
posterior to midposterior to mid--axillaryaxillary line) or in internal line) or in internal rotation (rotation (TPsTPs anterior to midanterior to mid--axillaryaxillary lineline

IliotibialIliotibial Band (ITB)Band (ITB)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point:Tender Point:On the On the iliotibialiliotibial band band
along the lateral along the lateral aspect of the thigh on aspect of the thigh on the the midaxillarymidaxillary linelineCheck with hip and Check with hip and
knee dysfunctionknee dysfunction

IliotibialIliotibial Band (ITB)Band (ITB)
Position of Treatment:Position of Treatment:Patient may be prone or supinePatient may be prone or supineOperator stands on the side of the TP and Operator stands on the side of the TP and grasps the patient’s leg and produces grasps the patient’s leg and produces marked abductionmarked abductionInternal/external rotation to fine tuneInternal/external rotation to fine tune

Anterior PelvisAnterior PelvisD’AmbrogioD’Ambrogio and Roth 1997and Roth 1997

Anterior PelvisAnterior Pelvis
Patient PresentationPatient Presentation::Pain with standing and walkingPain with standing and walkingPosture Posture –– anterior pelvisanterior pelvisDysfunction of hip flexors, adductors, Dysfunction of hip flexors, adductors, internal rotatorsinternal rotatorsIliosacralIliosacral dysfunctiondysfunction

IliacusIliacus (IL)(IL)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point:Tender Point:3 cm medial to ASIS 3 cm medial to ASIS
and deep in the iliac and deep in the iliac fossafossa; pressure ; pressure posteriolaterallyposteriolaterallyKey point for chronic Key point for chronic
SI joint dysfunctionSI joint dysfunction

IliacusIliacus (IL)(IL)
Position of Treatment:Position of Treatment:Patient supine with ankles supported on Patient supine with ankles supported on operator’s thigh; operator stands on side operator’s thigh; operator stands on side of TPof TPLegs taken into extreme flexion and Legs taken into extreme flexion and external rotationexternal rotationRotation toward the TP to fine tuneRotation toward the TP to fine tune

Superior Pubis (SPB)Superior Pubis (SPB)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point:Tender Point:Superior aspect of Superior aspect of
lateral lateral ramusramus of the of the pubis and pubis and approximately 2 cm approximately 2 cm lateral to the pubic lateral to the pubic symphysissymphysis; push ; push inferiorlyinferiorly

Superior Pubis (SPB)Superior Pubis (SPB)
Position of Treatment:Position of Treatment:Patient is supine with the Patient is supine with the operatotoperatotstanding on side of TPstanding on side of TPOperator flexes the hip 90 Operator flexes the hip 90 –– 120^ with no 120^ with no abduction or rotationabduction or rotation

Inferior Pubis (IPB)Inferior Pubis (IPB)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point:Tender Point:Medial surface of the Medial surface of the
descending descending ramusramus of of the pubis (find the pubis (find ischialischialtub move medially)tub move medially)

Inferior Pubis (IPB)Inferior Pubis (IPB)
Position of Treatment:Position of Treatment:Patient is supinePatient is supineOperator stands on the side of the TP and Operator stands on the side of the TP and flexes, abducts, and externally rotates the flexes, abducts, and externally rotates the affected hipaffected hip

Lateral Pubis (LPB)Lateral Pubis (LPB)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Tender Location of Tender Point:Point:Lateral surface of pubic Lateral surface of pubic bone just below the bone just below the inquinalinquinal ligament ligament attachment attachment (undergarment line)(undergarment line)SI joint pain, flareSI joint pain, flare--ins, ins, tension in femoral tension in femoral triangle, ant. thigh paintriangle, ant. thigh pain

Lateral Pubis (LPB)Lateral Pubis (LPB)
Position of Treatment:Position of Treatment:Patient is supine and the operator is standing Patient is supine and the operator is standing
on the side of the TPon the side of the TPPatient’s hips flexed to 90^ and rested on Patient’s hips flexed to 90^ and rested on
operator’s thighoperator’s thighUnaffected leg is crossed over the affected legUnaffected leg is crossed over the affected legMove affected leg into internal/external rotationMove affected leg into internal/external rotation

SartoriusSartorius (SAR)(SAR)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point:Tender Point:2 cm lateral to the 2 cm lateral to the
ASIS; hips may be ASIS; hips may be flexed to 45^ to flexed to 45^ to facilitate locationfacilitate location

SartoriusSartorius (SAR)(SAR)
Position of Treatment:Position of Treatment:Patient is supine with the operator Patient is supine with the operator standing on side of TPstanding on side of TPOperator flexes hip to 90^ and adds Operator flexes hip to 90^ and adds moderate abduction and external rotationmoderate abduction and external rotation

Adductors (ADD)Adductors (ADD)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point:Tender Point:Origin of adductors to Origin of adductors to
pubic bone or belly of pubic bone or belly of musclemuscleSI joint flareSI joint flare--outs, outs,
trochanterictrochanteric bursitis, bursitis, ITBITB

Adductors (ADD)Adductors (ADD)
Position of Treatment:Position of Treatment:Patient is supine with the operator Patient is supine with the operator standing on the side opposite of the TPstanding on the side opposite of the TPOperator reaches across and grasps the Operator reaches across and grasps the patient’s distal tibia and adducts the leg patient’s distal tibia and adducts the leg (pulling medially)(pulling medially)

Posterior Posterior SacralsSacralsD’AmbrogioD’Ambrogio and Roth 1997and Roth 1997

Posterior Posterior SacralsSacrals
Present in sacroiliac dysfunction (torsions)Present in sacroiliac dysfunction (torsions)Clear L5 before treating Clear L5 before treating sacralssacrals

Posterior First Sacral (PS 1)Posterior First Sacral (PS 1)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point:Tender Point:Sacral Sacral sulcussulcus, medial , medial
and slightly superior and slightly superior to PSISto PSISBackward sacral Backward sacral
torsionstorsions

Posterior First Sacral (PS 1)Posterior First Sacral (PS 1)
Position of Treatment:Position of Treatment:Patient is pronePatient is proneOperator applies a downward pressure on Operator applies a downward pressure on inferior lateral angle opposite of TPinferior lateral angle opposite of TP

Posterior Second Sacral (PS2)Posterior Second Sacral (PS2)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point:Tender Point:Midline of the sacrum Midline of the sacrum
between the first and between the first and second sacral spinessecond sacral spines

Posterior Second Sacral (PS2)Posterior Second Sacral (PS2)
Position of Treatment:Position of Treatment:Patient is pronePatient is proneOperator applies a downward pressure to Operator applies a downward pressure to apex of sacrum in midlineapex of sacrum in midlineProduces rotation around a transverse Produces rotation around a transverse axisaxis

Posterior Third Sacral (PS3)Posterior Third Sacral (PS3)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point: Tender Point: Midline of sacrum Midline of sacrum
between the second between the second and third sacral and third sacral spinesspines
Posterior Third Sacral (PS3)Posterior Third Sacral (PS3)
Position of Treatment:Position of Treatment:Patient pronePatient proneOperator applies a downward pressure to Operator applies a downward pressure to the apex of the sacrum in midlinethe apex of the sacrum in midline

Posterior Fourth Sacral (PS4)Posterior Fourth Sacral (PS4)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point:Tender Point:Midline of the sacrum Midline of the sacrum
just above the sacral just above the sacral hiatushiatus

Posterior Fourth Sacral (PS4)Posterior Fourth Sacral (PS4)
Position of Treatment:Position of Treatment:Patient is pronePatient is proneOperator applies an anterior pressure on Operator applies an anterior pressure on the sacral base in midlinethe sacral base in midline

Posterior Fifth Sacral (PS5)Posterior Fifth Sacral (PS5)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point:Tender Point:1 cm medial and 1 cm medial and
superior to the inferior superior to the inferior lateral angle of the lateral angle of the sacrumsacrumForward sacral Forward sacral
torsionstorsions

Posterior Fifth Sacral (PS5)Posterior Fifth Sacral (PS5)
Position of Treatment:Position of Treatment:Patient is pronePatient is proneOperator applies a downward pressure on Operator applies a downward pressure on the sacral base on the side opposite the the sacral base on the side opposite the tender pointtender point
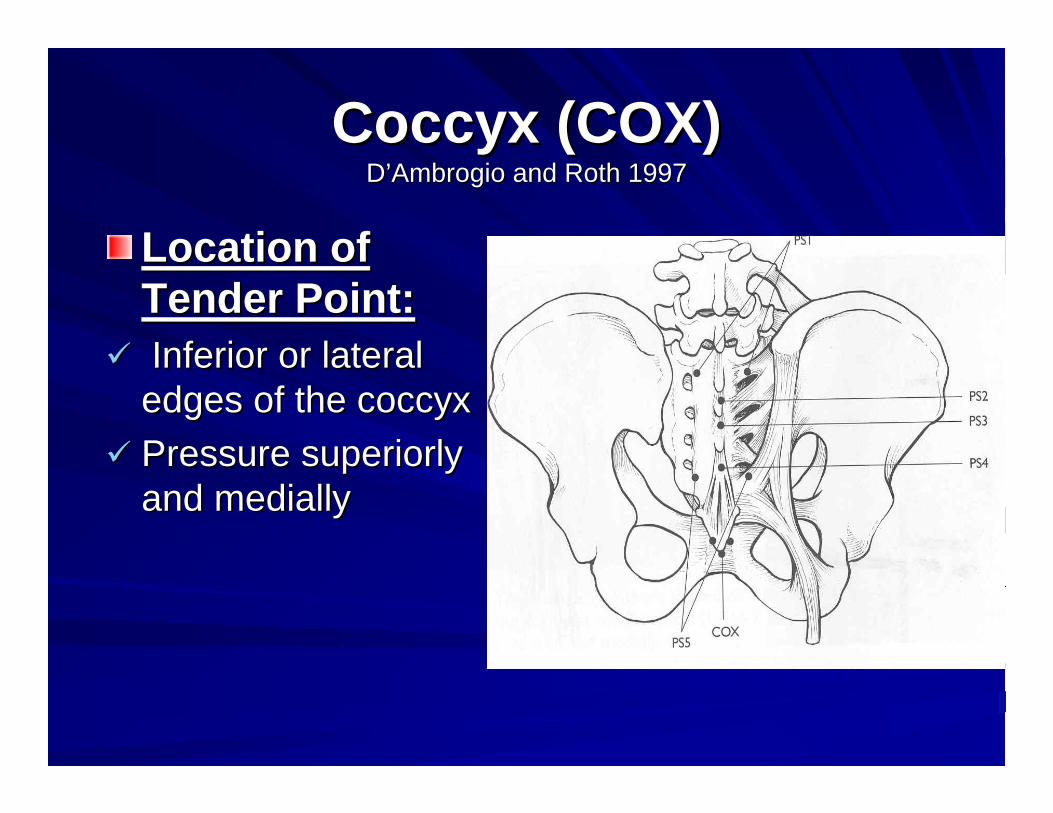
Coccyx (COX)Coccyx (COX)D’AmbrogioD’Ambrogio and Roth 1997and Roth 1997
Location of Location of Tender Point:Tender Point:Inferior or lateral Inferior or lateral edges of the coccyxedges of the coccyxPressure superiorly Pressure superiorly and mediallyand medially

Coccyx (COX)Coccyx (COX)
Position of Treatment:Position of Treatment:Patient is pronePatient is proneApply a downward pressure to the apex of Apply a downward pressure to the apex of the sacrumthe sacrumRotate sacrum toward side of tender pointRotate sacrum toward side of tender point

The End The End –– Questions?Questions?