region 10 and in situ split of the deceased donor liver osotc education conference september 11,...
TRANSCRIPT

Region 10 and In situ Split of the Deceased Donor Liver
OSOTC Education Conference
September 11, 2015

History• In late 1980’s early 1990’s, pediatric waiting list
mortality significant – Development of reduced size liver transplantation
• Both living donor (LDLT) and deceased donor split liver transplantation (DDSLT) evolved from reduced size liver transplantation– Imbalance between recipients and available donors drove the
innovation with the goal of reducing waiting list mortality while maximizing utilization of resources
– DDSLT – 1989, LDLT – 1991– Outcomes following whole organ is best but given imbalance,
alternative techniques must be employed

Anatomic Liver segments

Reduced Size Liver Transplantation

Left Lateral Segment – Extended Right Lobe Split

Left Lobe – Right Lobe Split

In Situ Split – Left Lateral Segment Dissection
Middle Hepatic Vein
Left Portal Vein
Left Hepatic Artery
Left Hepatic Vein

Left Lateral Segment Graft

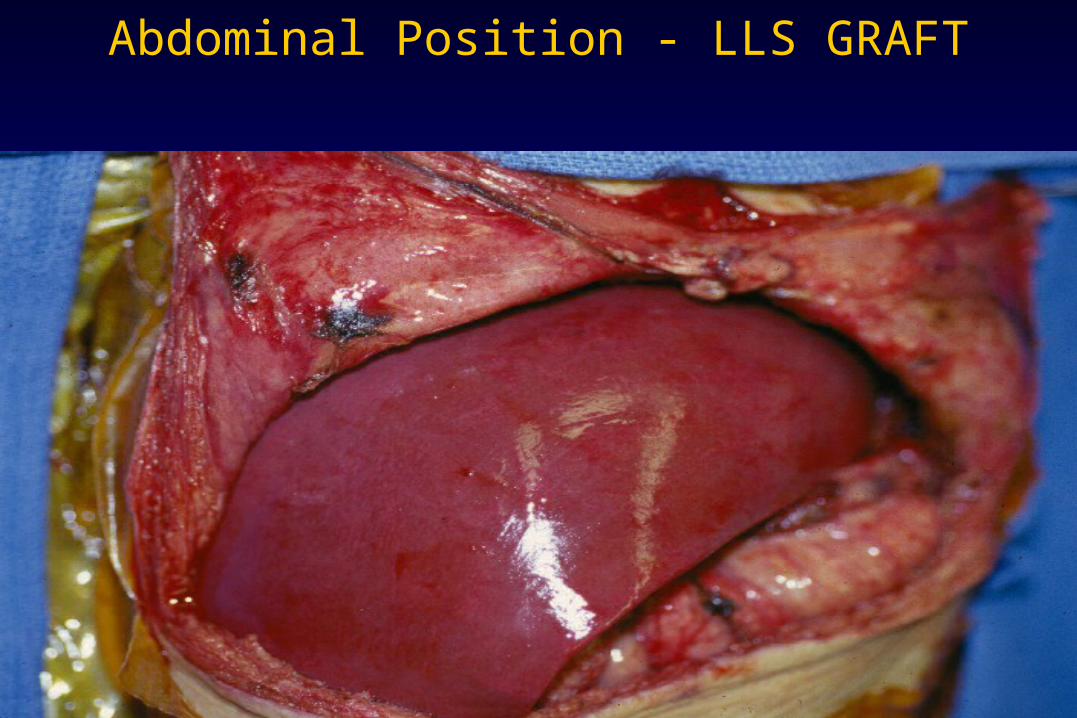
Abdominal Position - LLS GRAFT

Donor Criteria for Split Liver Consideration
• Age < 40
• ICU Stay < 5 days
• Liver biochemical profile within normal limits
• No more than 1 vasopressor agent
• Serum electrolytes within normal limits
Who should get a Split segment? Pediatric Recipient
• Donor : Recipient Weight Ratio– Left Lobe Graft – 2-5 : 1– Left Lateral Segment Graft - 6-10 : 1
• Disease Severity– Status I– PELD>15– Any patient for whom a reduced size graft is being
considered

Who should get a Split segment? Adolescent / Adult Recipient
• Donor : Recipient Weight Ratio– Extended Right Lobe Graft
• Size match
– Right Lobe Graft• Graft weight : Recipient weight (GWRW)
– Living donor > 0.8 %
– Deceased donor > 1%
• Recipient Disease Severity– Lower MELD – Less portal hypertension /hyperdynamic
splanchnic circulation

Where to Split?In situ versus Ex vivo
• In Situ– Benefits
• Clearer sense of both grafts perfusion
• Cut surface controlled• Less cold ischemia time
– Risks• Longer donor OR time• Potential risk of
hemodynamic instability which could effect other organs
• Ex Vivo– Benefits
• Shorter OR time• Less risk to other organs
– Risks• Perfusion of both grafts
unknown• Longer cold ischemia time• Cut surface

Operative Considerations
• Local OPO preparation– Appropriate donor selection and organ allocation– Communication with different donor teams – timing and length
of operation
• OR team – Anesthesia aware with more blood available
• OR Equipment– Essential – Bovie, slush, patience – Helpful – Intra-op cholangiography, laparoscopic staplers,
harmonic, argon beam, experienced scrub tech

Allocation of Vessels and Biliary Tract
• Hepatic artery
• Portal vein
• Hepatic veins / Inferior vena cava
• Bile duct
• Vessels for reconstruction– Iliac artery and vein– Others - Inferior mesenteric and carotid artery
Region 10 Allocation of Structures Working agreement
• The center allocated organ decides vessel distribution– Hepatic artery – Celiac axis– Portal vein - variable– Bile duct – left hepatic duct – Hepatic veins / IVC
• LLS – left hepatic vein
• Left Lobe - Vena cava

Allocation of Hepatic Veins and IVC

Split grafts - Complications• Biliary tract
– Cut surface– Major bile duct
• Vascular – HAT/PVT• Small for size
– Ascites– Jaundice– Failure to thrive
In situ Split – the UCLA experience
• Single Center experience where they mostly split with themselves
• 100 donors yielded 190 grafts transplanted into 105 pediatric patients and 60 adults at UCLA, 25 shared within region
• Compared outcomes with whole organs and living donor grafts for both LLS and right trisegs
Yersiz et al, Ann Surg, 2003

In situ Split – the UCLA experience
Yersiz et al, Ann Surg, 2003

In situ Split – the UCLA experience• Amongst pediatric recipients, biliary and vascular
complications similar between LLS, LD and whole organ recipients
• Amongst adult recipients, increased rate of biliary and vascular complications
• Mechanism to get pediatric recipients transplanted while still giving adults access to a slightly higher risk but viable alternative
• Reduce need for living donor transplantation
Yersiz et al, Ann Surg, 2003

Annual Trend Split Liver Transplantation
0
50
100
150
200C
as
es
88 90 92 94 96 98 00 02 04
Year
C / C
A / A
A / C
Lee KW, Cameron AM, Maley WR et al. Am J Transpl 2008;8:1186-1196.

SPLIT Registry Survival
Diamond IR, Fecteau A, Millis JM et al. Ann Surg. 2007;246:301-310.

Factors affecting graft survival – LLS Split Liver
Risk Factor Hazard Ratio (95%) P value
Recipients Factors
Dx Tumor / No Tumor 1.904 (Tumor +) 0.03
Dialysis 1 wk of Tx 2.935 (Dialysis +) 0.004
Wt < 6 vs > 6 Kg 2.05 (<6Kg) 0.001
Donor Factors
< 30 vs > 30 yrs 1.448 (Age > 30) 0.041
CA post DBD 3.792 (cardiac arrest +) 0.001
Transplant Factors
CIT > 6 hr 1.688 0.008
CIT > 12 hrs 3.003 0.001
Pediatric Specific Ctr 1.0
No share vs share 1.666 vs 2.231 0.009
Lee KW, Cameron AM, Maley WR et al. Am J Transpl 2008;8:1186-1196.
In situ Right Lobe:Left Lobe split – Cleveland Clinic Experience
• Reviewed their experience using a right:left lobe split comparing outcomes to whole organ recipients
• Excluded Right Triseg:LLS in situ splits
• Sixteen donors – 32 grafts– 25 used at CCF, six by other programs in the region, 1
discarded for technical reasons
Hashimoto et al, AJT, 2014
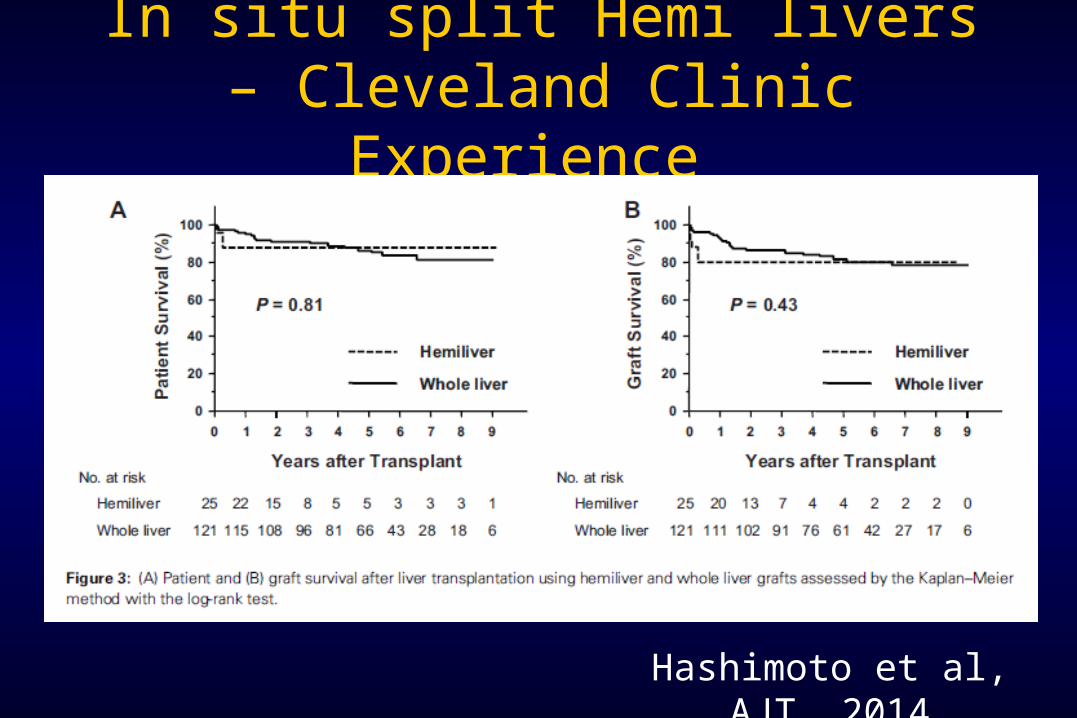
In situ split Hemi livers – Cleveland Clinic Experience
Hashimoto et al, AJT, 2014
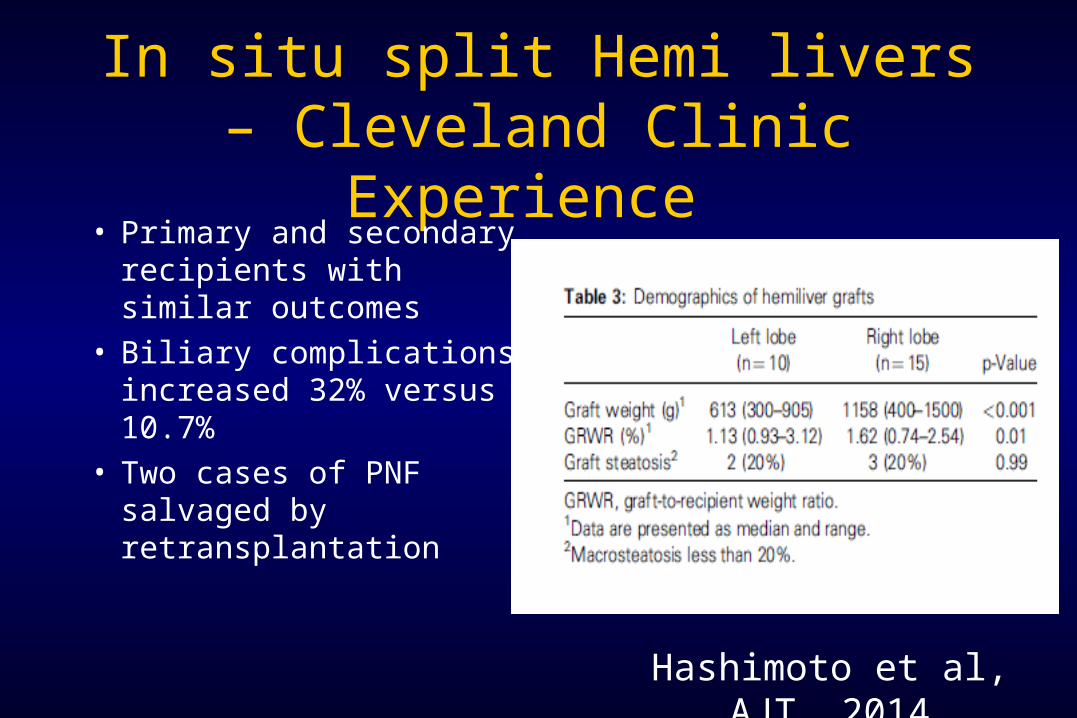
In situ split Hemi livers – Cleveland Clinic Experience
• Primary and secondary recipients with similar outcomes
• Biliary complications increased 32% versus 10.7%
• Two cases of PNF salvaged by retransplantation
Hashimoto et al, AJT, 2014

Meta-analysis of In situ split right lobe grafts
• Review encompassed all articles before December 2014 time period
• PubMed, Embase and Cochrane Library search
• Seventeen studies with a total of 48457 patients utilized in analysis
Wan et al, Liver Transpl, 2015

Meta-analysis of In situ split right lobe grafts
• Patient and graft survival similar
• Complications not identified in study found to be statistically significant– Biliary complications and outflow
obstruction more common in split liver graft
• Ex vivo split worse outcome then in situ split
• Should match appropriate recipient with risk of graft
Outcome Odds Ratio
Confidence Interval
p value
Patient Survival (One year)
0.85 0.62-1.16 0.31
Graft Survival(One year)
0.91 0.76-1.08 0.27
Biliary Complications
1.66 1.29-2.15 <0.001
Bile leaks 4.3 2.97-6.23 <0.001
Vascular complications
1.81 1.29-2.53 <0.001
HAT 1.71 1.17-2.5 <0.005
Outflow Obstruction
4.17 1.75-9.94 0.001
Wan et al, Liver Transpl, 2015

CCHMC Graft use 2004-2015• Increased use of Split segments starting in 2004• Number of transplant 248• Whole – 123, Technical variants - 125• Reduced Size – 90 Split – 25 Living related – 10 • Split – 25
– Extended Right - 2, Right Lobe - 2
– Left Lobe - 10 , LLS - 11
– Donor age range - 7 - 45
– In situ vs ex vivo – 18 in situ, 7 ex vivo
– Local - 2, Region - 23

CCHMC OutcomesGraft Survival Patient Survival

Conclusions
• In situ split livers is an alternative to increase donor pool but should be used in a select population
• In our region, allocation to pediatric patient is logical trigger for in situ split liver consideration
• Requires significant cooperation between OPO, transplant teams

The Risk of any Journey The Risk of any Journey must be appreciated by must be appreciated by
all parties…..all parties…..(Prior to beginning the (Prior to beginning the
Journey !)Journey !)
