reforms in the health care financing the development of health insurance system in albania elvana...
TRANSCRIPT

REFORMS IN THE HEALTH CARE FINANCING The development OF health insurance system in albania
ELVANA HANAGENERAL DIRECTOR
III Balkanic Forum, Montenegro – September 2009
REPUBLIC OF ALBANIAINSTITUTE OF HEALTH INSURANCE

Page 2
Financing fields: Primary Health Care:
414 General and Specialized HC.
Hospital Health Care:
4 University Hospitals
12 Regional Hospitals
23 Municipal Hospitals 11 Unique tertiary
examinations. Drugs reimbursement from the
Reimbursement List.
377 drugs or 944 trading alternatives.
Page 3
Main Issues
I. Deepening in the Financial Reform of the Primary Health Care. Achievements and challenges.
II. The extension of the financing scheme in the hospital health care.
III. Strengthen of HII role as a main purchaser of the health services.

Page 4
BENEFITS FROM THE REFORM ON PHC
Service Providers
Financial
Experience
– Financial management
– Management of H. Resources
– Organization
Medications/medical stuff
Increase of service quality
Conditions for following C.M.E
Strengthen of HC role as gatekeeper.
Insured persons
A better access to obtain health services;
Improvement of conditions to obtain better quality from the services.
Standardized services (Package of services)
Better monitoring regarding the chronic diseases.
Page 5
Reforms achievements in PHC
More founds were allocated to the HC as a consequence of the improvement of their performance and quality indicators.
The HC have a better conceptions regarding the management of the allocated founds.
The level of autonomy of the HC has increased. The contracts with HC have improved and the Boards function.
There have been improvement in the collection of the secondary incomes and better possibilities to manage them by the HC.
Improvement of the information technology It is in process of implementation, supportive supervision, as a new
methodology applied to help in solving the HC problems and improve their performance
HII has provided adequate support in the implementation of professional training programs for the service providers.

Page 6
PHC FINANCING COMPARISON (January - August 2007-2008-2009)
0
200,000
400,000
600,000
800,000
1,000,000
2007 2008 2009
The budget allocated to the HC in 2009 was 13% larger than in 2008
Page 7
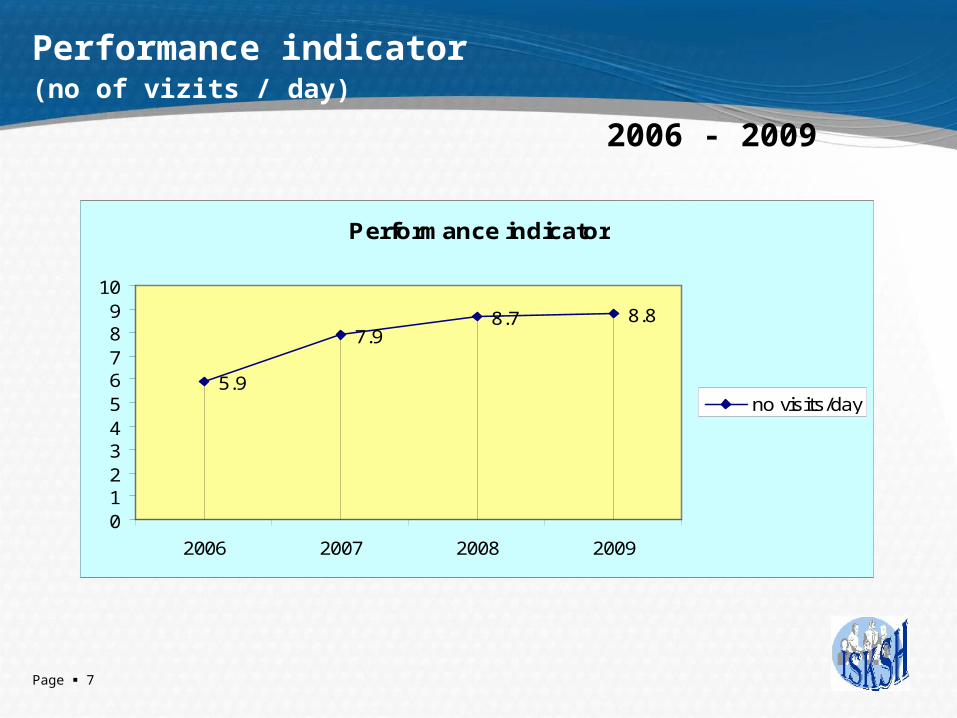
Performance indicator
(no of vizits / day)
2006 - 2009
Performance indicator
5.9
7.98.7 8.8
0123456789
10
2006 2007 2008 2009
no visits/day
Page 8
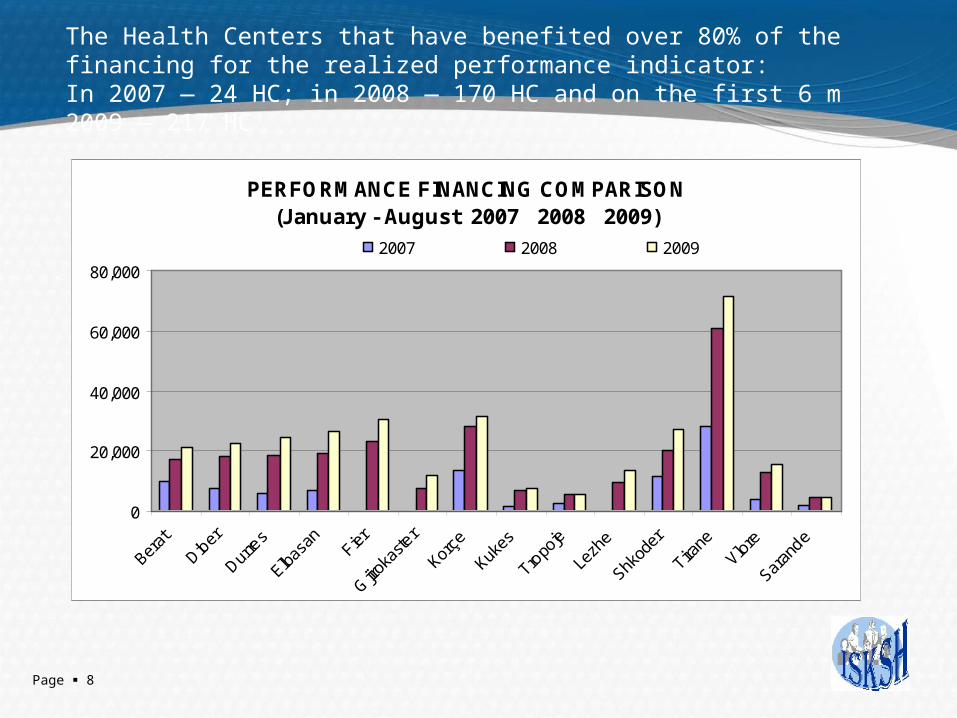
PERFORMANCE FINANCING COMPARISON (January - August 2007 2008 2009)
0
20,000
40,000
60,000
80,000
Berat
Diber
Durre
s
Elbas
an Fier
Gjiro
kaste
r
Korçe
Kukes
Tropo
je
Lezh
e
Shkod
er
Tirane
Vlore
Saran
de
2007 2008 2009
The Health Centers that have benefited over 80% of the financing for the realized performance indicator:In 2007 — 24 HC; in 2008 — 170 HC and on the first 6 m 2009 — 217 HC

Page 9
Quality indicators - Bonus 5%
Quality indicators (2008-2009) Standard - 100 points
68.165.565.259.7
54
0
10
20
30
40
50
60
70
80
I-2008 II-2008 III-2008 IV-2008 6M-2009

Page 10
BONUS FINANCING COMPARISON(January - August 2007 2008 2009)
0
10,000
20,000
30,000
40,000
Berat
Diber
Durre
s
Elbas
an Fier
Gjiro
kaste
r
Korçe
Kukes
Tropo
je
Lezh
e
Shkod
er
Tirane
Vlore
Saran
de
2007 2008 2009
Health Centers that have benefited over 70% of the financing for the realized quality indicators:In 2008 — no HC and in the first 6 m of 2009 — 64 HC

Page 11
The Information Technology achieved:
The application of the standard form for the visits and medical procedures by the medical staff of the HC, which helps in:
- reporting, monitoring and financing the Performance and Services quality
- decision-making to increase the service quality
The electronic registration of the population and the application of the effective payments per capita (still in process)
Page 12
The extension of the financing reform in the hospital service
What do we aim by the reforms in the hospital health care :
Change the method of financing. HII as an active purchaser
Autonomy of Hospitals, which consist of:
– financial: existence of a separate budget, the right to propose it and to manage it financially.
– organizational : relative independence to be self-organized
– normative: the power to issue self-regulatory norms.
– contractual freedom : the possibility to enter in relations freely with the others.

Page 13
Hospital legal status
The hospital is a legal person,
public,
un-budgetary,
non-profitable,
with a separate bank account,
provides medical services approved by the Ministry of Health.

Page 14
Funding of Hospitals by the Health Insurance
HII
Contributions of the active
populationMinistry of Health
ISS – GDT (General Directory
of Taxation)
RDHCI(Branches of HII)
Regional hospital
District hospital District hospital
Contracts
Contracts
Investments
Transfers from the State Budget
(non-Active )
Board

Page 15
The start of the reform in Hospital care in the January 2009 enabled:
Singing of the bilateral contracts with 39 hospitals :
- 4 University hospitals
- 12 Regional hospitals
- 23 Municipal hospitals
Signing of individual contracts between director – staff (in process)
Financing by budgeting according to a Services List
Application of a new method of reporting for the hospital performance:
- Clinical
- Economic and financial

Page 16
(continuation)
Working for the calculation of the actual cost for each hospital according to the clinical services
Defining the cost structure according to the elements of expenditure
Working for the issuance of the actual cost per day/stay for each hospital
Defining of some elements for measuring the hospitals performance like bed utilization etc.
Page 17
Increase of HII role as an active purchaser requires:
I. In the Primary Healthcare
Improvement of the level of autonomy of the HC. Deepening in the process of decentralization.
Efficiency on the information system utilization (the informatization of the HC across the country which is still in process of conclusion
pplication of a system with differential reward for differential work within the HC, depending on the individual fulfillment of the quantitative and qualitative indicators of the job.
Improvement of the method of HC financing to increase the level of their utilization and quality service. (Revision on the actual form of payment 85/ 10 / 5 of the HC’s budget)

Page 18
(continuation)
The cost calculation of the primary service.
Support in the process of drafting guidelines for clinical practice regarding the family doctors.
Implementation of incentive financial policies regarding the health coverage of the vulnerable categories of the population.

Page 19
II. In the hospital healthcare:
Improving the legal framework.Improving the level of autonomy in the hospitals Setting the standards for the costs calculation:
- per service,
- per diagnose case and diagnose group (DRG).
Approving standards for quality and performance indicatorsImplementing a unique informative systemApproving of hospital treatment protocols.Improving and implementing rigorously a referral system in all the
health services levels.
Page 20
( continuation )
Implementing a flexible payment system based on the performance of each provider.
Trainings of the hospital managers and hospital staff regarding the organizational, financial and technical issues.
Increase of access by the population to benefit services. Reducing the level of informality in the services. Promote privatization of specific services at all levels of health care.

Page 21
THANK YOU