reducing preventable hospital readmissions in...
TRANSCRIPT
Reducing Preventable Hospital Readmissions in LTC
Kim Barrows RN BSN

The Affordable Care Act
This Act has brought about many challenges but at the same time has opened opportunities for Skilled
Nursing Facilities to set themselves apart from their competitors.

Session Objectives
This session will help facilities analyze and put proactive steps in place to positively impact their hospital readmission rates.
1. Recognize The implications Of Hospital Readmissions
2. Capture Data & Analyze Your Readmission Rates
3. Build Programs & Create Solutions For Your Facility

Knowing the History
1 in 4 Medicare patients admitted to SNFs from hospitals are readmitted within 30 days
Medicare spending is projected to increase by 79% over the next 7 years to $929.1 billion
Studies indicate that 65% of readmissions to the hospital are unnecessary
Over 50% of avoidable hospitalizations are admitted with:
• Cardiovascular (CHF and Chest Pain)
• Respiratory (Pneumonia and Bronchitis)
• Mental Status Change/Neurological

Why The Focus
• The Patient Protection and Affordable Care Act (March 23, 2010) has several provisions to reduce hospital readmissions
• Medicare is planning financial incentives to reduce potentially avoidable hospital transfers through pay-for-performance, bundled payments, ACOs and other strategies
• CMS implemented financial penalties for hospitals with high 30 day readmission rates for the following diagnoses: CHF, Pneumonia and Acute Myocardial Infarction

What is an ACO?
Groups of volunteer doctors, hospitals, nurses and other care providers who offer coordinated quality care to a specific population of patients.
• Goals:
– Improve the total cost, quality and satisfaction of a specific population, especially chronically ill patients
– Avoid unnecessary duplication of services
– Prevent medical errors
– Transition from volume to value approach

How are ACOs paid?
Efficient delivery of the right care, in the right setting and right time, patients benefit yet we have a cost reduction.
The amount of money saved will be shared between the ACO and the payer source.

ACO - Shared Savings Program
•Accept accountability for the total cost of care for patients
•Create processes to promote evidence-based medicine and patient engagement. Report on quality and cost measures. Coordinate care using telehealth and remote patient monitoring etc...
•The Shared Savings Program will reward ACOs with lower health care costs while meeting performance standards on quality of care and putting patients first.
*2010, Premier Inc.

Critical Components –ACO Model
• Why is it important to know who is participating?
Model
• Develop tightly integrated relationships with specialists, ancillary providers and hospitals in order to achieve high-value outcomes
• Develop provider/payer partnerships and reimbursement models rewarding value over volume *2010, Premier Inc.

ACOs Potential Impact on SNF Quality
American HealthTech www.healthtech.net

Partnership for Care Transformation Implementation Collaborative - Participants
•The Goal:
– To pursue accountability
– Growing from fee-for-service to value-driven business models
– Modify existing payer contracts
• Heartland Health- Saint Joseph, MO
• Saint Francis Health System- Tulsa, OK
• Methodist Medical Center- Peoria, IL
• Website for complete listing: https://www.premierinc.com/quality-safety/tools-services/ACO/aco-implementation-participants.pdf
Premier Inc., 2012

Partnership for Care Transformation Readiness Collaborative Participants
• Responsibilities:
– Develop the organization, skills, team, operational capability and tools to develop a coordinated care delivery model – Will eventually join the Implementation Collaborative
• Adventist Health System-
–Shawnee Mission Medical Center-Kansas City, MO • Phelps County Regional Medical Center- Rolla, MO •St. Anthony’s Medical Center-St. Louis, MO
•Website for complete listing:
–www.premierinc.com/quality-safety/tools-services/ACO/aco-readiness-participants.pdf
Potential Complications with Hospital Admissions
• Transfer Trauma
• Delirium
• Immobility/Deconditioning
• Falls
• Weight Loss
• Incontinence and Foley Catheters
• Hospital Acquired Infections
• Wounds
• Polypharmacy
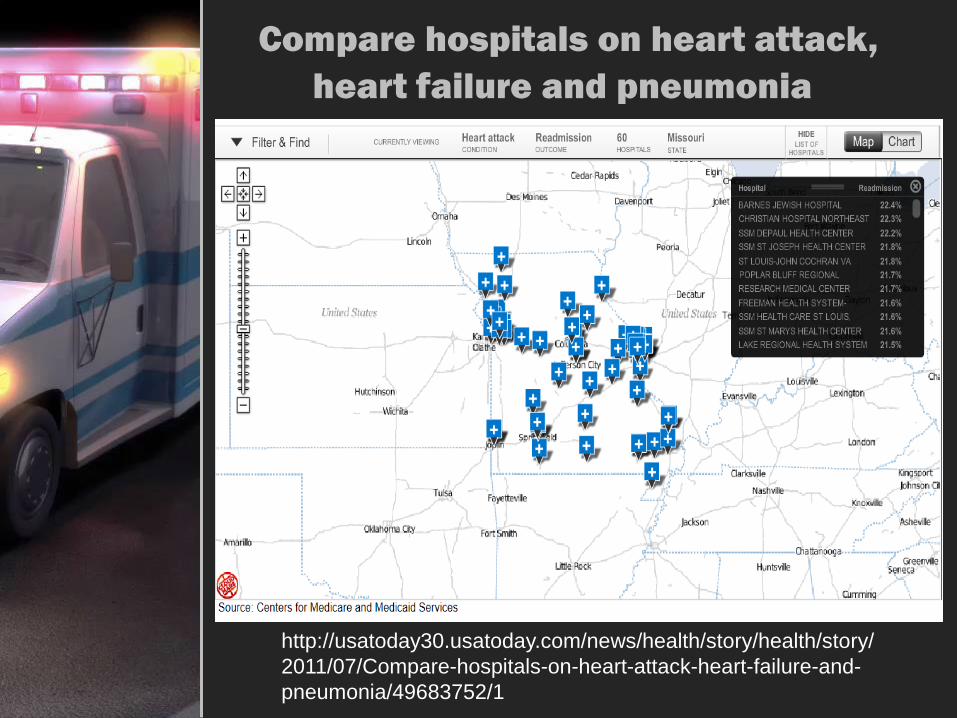
Compare hospitals on heart attack,
heart failure and pneumonia
http://usatoday30.usatoday.com/news/health/story/health/story/
2011/07/Compare-hospitals-on-heart-attack-heart-failure-and-
pneumonia/49683752/1

National Rehospitalization Rates

SNF Days Until Rehospitalization

2013 Medicare Readmission Penalties
Readmission penalties by state and hospital:
http://www.kaiserhealthnews.org/Stories/2013/August/02/readmission-penalties-by-state-year-two.aspx
*Provided by Kaiser Health News. http://www.kaiserhealthnews.org

Readmission Penalties by State
*Provided by Kaiser Health News. http://www.kaiserhealthnews.org

Readmission Penalties by Hospital
*Provided by Kaiser Health News; http://www.kaiserhealthnews.org

Medicare Readmission Penalties by State
State
Total
Hospitals Eligible for
Penalty
# of
Hospitals Penalized
Average Penalty
for Eligible
Hospitals
Missouri 76 55 0.39%
Arkansas 45 37 0.71%
Iowa 34 15 0.20%
Illinois 127 113 0.45%
Oklahoma 91 53 0.34%
Kansas 55 29 0.25%
*Provided by Kaiser Health News; http://www.kaiserhealthnews.org

How Did Medicare Decide On Penalties?
•Policy developed by CMS endorsed by the National Quality Forum (NQF) for heart attack, heart failure and pneumonia
•Three years of discharge data and minimum of 25 cases for each condition were used to develop these ratios
•Adjustment for factors that are clinically relevant including patient demographic characteristics, co- morbidities and patient frailty
*Provided by Kaiser Health News; http://www.kaiserhealthnews.org

Post-Acute Care Reform
The President’s and Other Bipartisan Proposals to Reform Medicare:
1) Reducing market basket updates
2) Neutral payments
3) Modifying criteria required for IRF status
4) Establishing a SNF readmissions programs
5) Creating PAC bundled payments
http://waysandmeans.gov/uploadedfiles/pac_reform_fact_sheet.pdf

Factors Influencing Hospital Readmissions
• Geography
• Demographics (age, gender & race)
• Poverty
• Individuals with disabilities
• 5 or more Co-morbidities double their risk of readmission
• History of readmissions-frequent flyer
• Hospitals that serve low-income patients, will receive higher penalties

Factors Influencing Higher Readmission Rates
•Unsatisfactory discharge planning and follow through
•Noncompliance
•Inadequate follow-up care from post-acute and long-term care providers
•Overestimating family/caregiver’s competency
•Deterioration of a patient’s clinical condition
•Medication errors
•Socioeconomic factors
•Lack of access to a Primary Care Physician
Strategies for Success •Decrease unnecessary rehospitalizations
– Use data tracking log – Analyze data – Monitor for trends – Implement performance improvement plans
•Improve Resident/Family Satisfaction
– QIS (ReadyQ) – Resident/Facility satisfaction survey – Guardian angel program –My InnerView
•Develop partnerships with referral sources
– Become the “Preferred Provider” or Quality Outcome Center –MCOs
•Improve the Quality of Care
– Solid QA Program – Provide clinical education to staff; include competency testing
•Provide efficient yet effective health care
– Outcomes-Share your results

Preventing Avoidable Hospitalizations
Resources
• Evaluated by a physician within 24hrs of
admission
• Physician/NP/PA in the facility 3 days a week
• Knowledgeable nursing staff ; care provided by RN vs LPN
• IV therapy , lab and diagnostic testing on-site
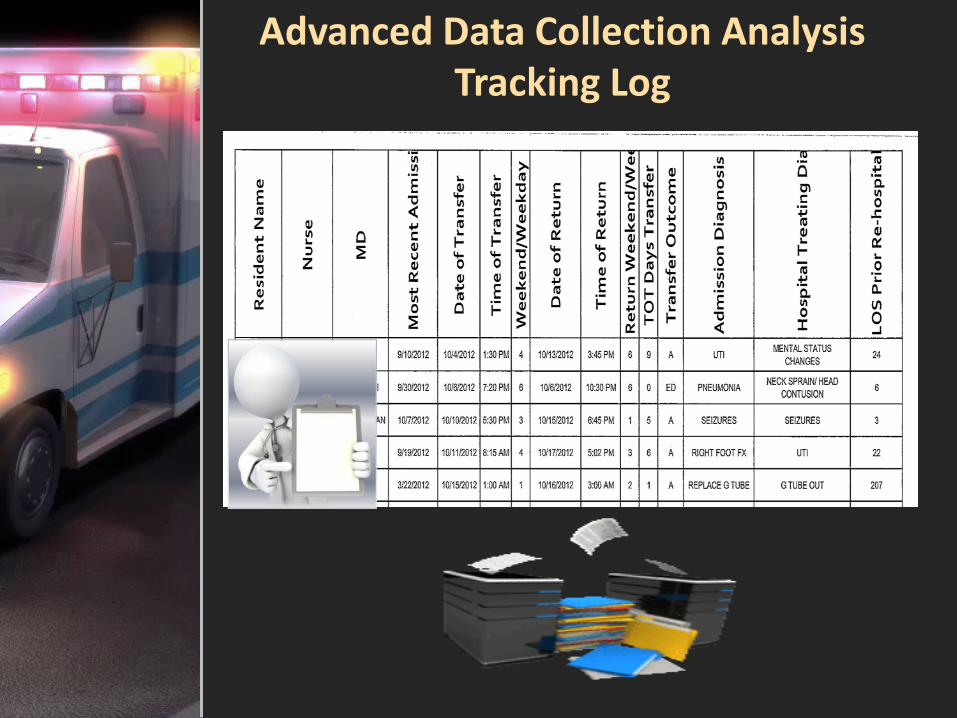
Advanced Data Collection Analysis Tracking Log

Tracking Log Considerations
• Name of the physician discharging. Was it the “On-Call” Physician, PCP or a family/patient request?
• Weekend or evening?
• Time of discharge?
• Staff education? Was education offered to the patient or family on disease management and risk factors?
• Do the Advanced Directives need to be revisited?
• Is Palliative Care appropriate?
• Was the early detection protocol used? Could treatment have been provided in-house?
Tracking Log Considerations
•Discharging Nurse?
•Percentage of residents that are readmitted within the first 30 days for MI, Pneumonia or Heart Failure? Then include all diagnosis.
•Did we fully implement the cardiac program? Joint Replacement Program? Pulmonary Program?
•Is a hospice referral appropriate?
•Who is referring to you? What type of residents are you admitting?

Discharging Nurse
Spreadsheet displaying nurses and how many residents they sent out each month. Allows for tracking trends and which nurses may need additional training and education.

Physician Tracking

Tracking Analysis
•Weekly IDT Committee Meetings
•Monthly Analysis
•Example:
8 acute discharges/ER visits during the month of October.
5 acute discharges resulted in admissions.
3 were ER visits with return after midnight.
Upon review, all three ER visits could have been prevented with proper interventions although two visits were for the same resident and family did request the resident be sent out.

How to Measure Rehospitalization Rates
• Based on claims (hospital & SNF Part A)
• Does not include ER visits and observation stays
• Excludes Medicare Advantage and private insurance
%= numerator
denominator
%= # of persons sent to hospital
# of persons admitted to SNF
• Brown University: http://ltcfocus.org/
• SNF rehosp rates

LTC Trend Tracker
• Available to all American Health Care Association members
– Compare performance in clinical, financial and operational areas with peers
• Provides:
– Survey History
– Resident Characteristics
– Staffing Information
– Cost Report and Medicare Utilization
– CMS Five Star Rating
•Website for additional information
–www.ltctrendtracker.com

Great Emphasis On Quality
Assuring and/or improving quality requires documenting valid metrics and proactively implementing & monitoring systems
How are we being graded?
• Quality Measures
• CMS Five Star Report
• Nursing Home Compare
• Facility Satisfaction Survey
• QIS
• State - Resident Satisfaction Survey
• State - Family Satisfaction Survey
Quality Measures
Who’s watching….
Hospitals
MCOs
ACOs
Survey Agencies

Insurance Scorecard Info
• The transition through the continuum of care
• Length of stay
• Functional rehabilitation progress
• Palliative Care capability
• Rehospitalization rates
• Patient and Family Satisfaction

Humana SNF Scorecard Provider demographics and Services Available

Humana SNF Scorecard Nurse Practitioner, Grijalva Process

Humana SNF Scorecard Communication/Pt Satisfaction Survey/CMS Star Rating

Humana SNF Scorecard Readmissions/Additional Comments/Scoring

Anthem Scorecard

Becoming the Preferred Provider
What do you do best?
• Pick one or two specialties
• Develop a unique program
• Market the outcomes.

HCMG ‘s Collaborative Objectives
Reduce hospital readmissions
Improve patient outcomes without increasing cost
Improve the transition process from the hospital to SNF to home
Become the local hospital’s preferred provider
Cardiac Recovery Program Overview
• Resident Condition Meetings
• In-house Lab and Diagnostic Testing
•Validated Competency Testing performed by Nursing and Therapy departments
• Standardized Patient Education
• Utilize the Teach Back Method
• Early Warning Tool
• Care Coordinator Involvement

Cardiac Approach • ACLS Certification
Education on Cardiac Disease and Management Techniques
• Pharmaceutical Management
• Therapists receive specialized cardiac training
• ACP equipment with measureable outcomes
• Psychosocial Management including Smoking Cessation Classes
• Nutritional Assessment and Counseling with a Registered Dietician

Cardiac Approach
• Wellness coaching on lifestyle changes
• Risk factor management (i.e. HTN, weight loss, lipids, etc.)
•Peer to Peer education
•Assist with developing a home exercise and therapy program
•Follow up call from the Care Coordinator after discharge
• Working hand in hand with home health agencies to provide the continuum of care and prevent readmission.

CHF Standing Orders
Upon Admission:
• Activity Restrictions
• Follow-up appointments with Cardiologist
• Daily Weight: notify MD or weight gain greater than 2 pounds in one day or 5 pounds in a week
• Diet Restriction: No Added Salt or Sodium Controlled
• Head of bed elevated at least 45 degrees
• Monitor Intake and Output
• Follow up labs/diagnostic testing: BMP, BNP, Chest X-ray, Ejection Fraction Ratio, EKG, Renal Panel, Tropin Level
• Vital Signs every shift
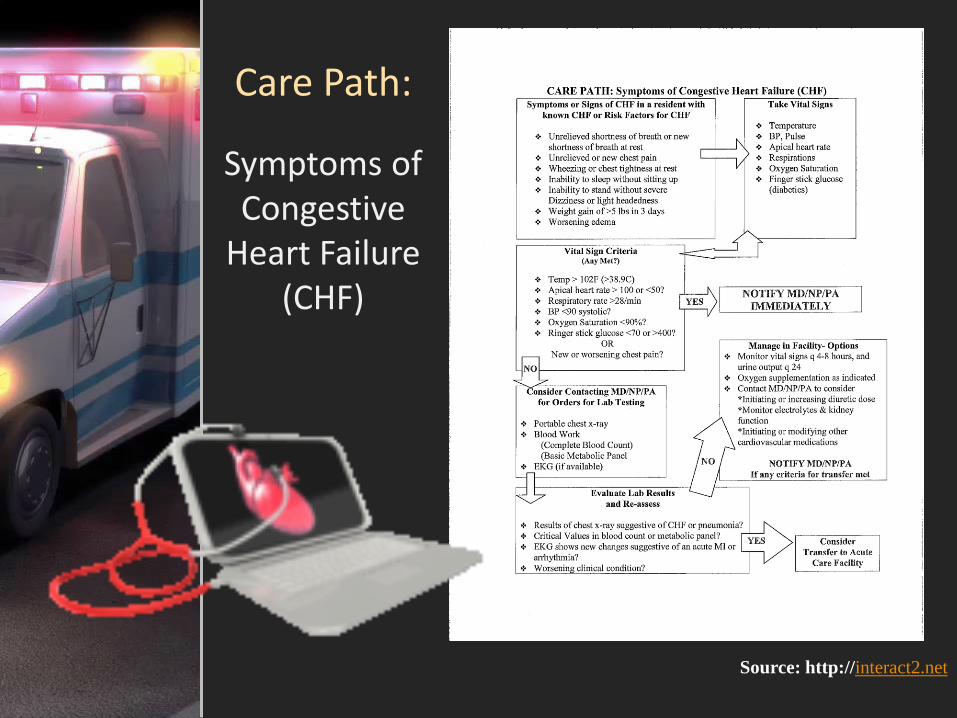
Care Path:
Symptoms of Congestive
Heart Failure (CHF)
Source: http://interact2.net

Resident Condition Meeting Tool
Cardiac Recovery/ Acute CHF Report Tool
Edema - +1/2/3/4 or non present
Lung Sounds - C=clear R=Rales RH=Rhonchi W=Wheezes Date:
Resident's Name Admission Room Prim/Sec Weight Weight O2 Edema Lung Comments
Date # Dx CHF (+)/ (-) Sats Sounds
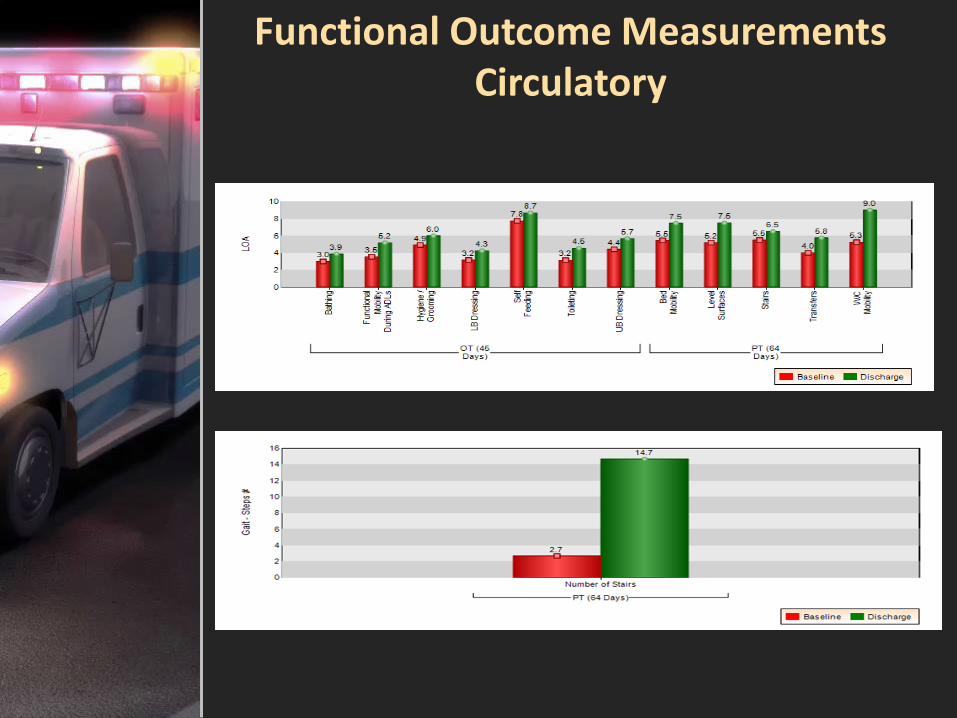
Functional Outcome Measurements Circulatory

SBAR Charting
S= Situation
B= Background
A= Assessment
R= Recommendation
Improves the quality of information that is communicated to the physician resulting in an accurate diagnosis and treatment.
•http://interact2.net/docs/Communication%20Tools/SBAR%20updated%20February%202011.pdf

Evaluation of Resident’s Knowledge
Teach Back Method
• What is the name of the diuretic or water pill you take?
• What amount of weekly weight gain should you report to your doctor?
• Share with me what a low-sodium diet entails?
• Why is it important to take your water pill every day?
• How will you remember to check for symptoms of heart failure every day?

Stop & Watch Tool
• Guides frontline staff through brief review of early, often subtle indicators of change in condition
• Improves communication between frontline staff and the nurse in charge
•http://interact2.net/docs/Communication%20Tools/Early_Warning_Tool_(StopWatch)c.pdf

Electronic Medical Records
Electronic Medical Records (EMRs) with complete, accurate and solid data.
• Software integration with partners to round out EMRs, e.g., labs, pharmacies, EKG reports, etc.
• Specialization programs that focus on reducing length-of-stay and improve the quality of care.
• Outcomes reports showing positive trends for lowering costs, boosting quality and reducing readmissions.

VitelMed: TeleHealthcare Solutions
• Telehealth service solution providing quality video care technology and connectivity between physicians, family and patients.
• Allows physicians to access a patient’s record and complete medical files in real time
• Enables patients to take their own vital health measurements (ex: lung capacity, blood sugars and blood pressure)
• Physicians can perform assessments remotely
• Nurses can assess this data remotely allowing for early detection/prevention
www.vitelmed.com

Telemedicine- Missouri
• New law puts Missouri insurers on the hook for telemedicine costs
• …”If the same service would be covered in an in-person visit, then the same service must be covered if received remotely, the legislation requires. It also prevents carriers from charging higher rates or co-pays for telemedicine visits.”
www.securetelehealth.com/telearticles-a-news.html

Clinical Outcomes
CHF
Discharge Planning
Orthopedic Programs
YOUR RECOVERY AT BROOKWOOD
The primary goal of your stay at Brookwood is for you to safely recover from surgery, participate in therapy, and to put you on the road to recovery. If there is anything we can do to enhance your stay and rehabilitation, please feel free to
ask.
KNEE REPLACEMENT PROGRAM HIP REPLACEMENT

Joint Replacement Program Overview
• Infection/pain monitoring
• Monitoring functional outcomes
• Decreased length of stay
• Staff education including competency testing
• Patient/caregiver education
• Anticoagulant therapy
• Care coordinator involvement
• Standardized education booklet used through the continuum of care
•Outcome measurements

Functional Outcomes Measurement Musculoskeletal

Knee Replacement
Standing Orders
• Avoid crossing legs
• Consider anticoagulant therapy
• CPM as ordered
• Incentive Spirometer 5 times an hour while awake
• Incentive Spirometer at bedside
• Keep knees facing forward
• Monitor for s/s of infection q shift
• Monitor pain q shift
• No deep squatting (lifting, gardening or golf)
• No direct kneeling on the knee cap
• No quick or excessive bending of the knee during any activity
• Place pillows under calf not under knee
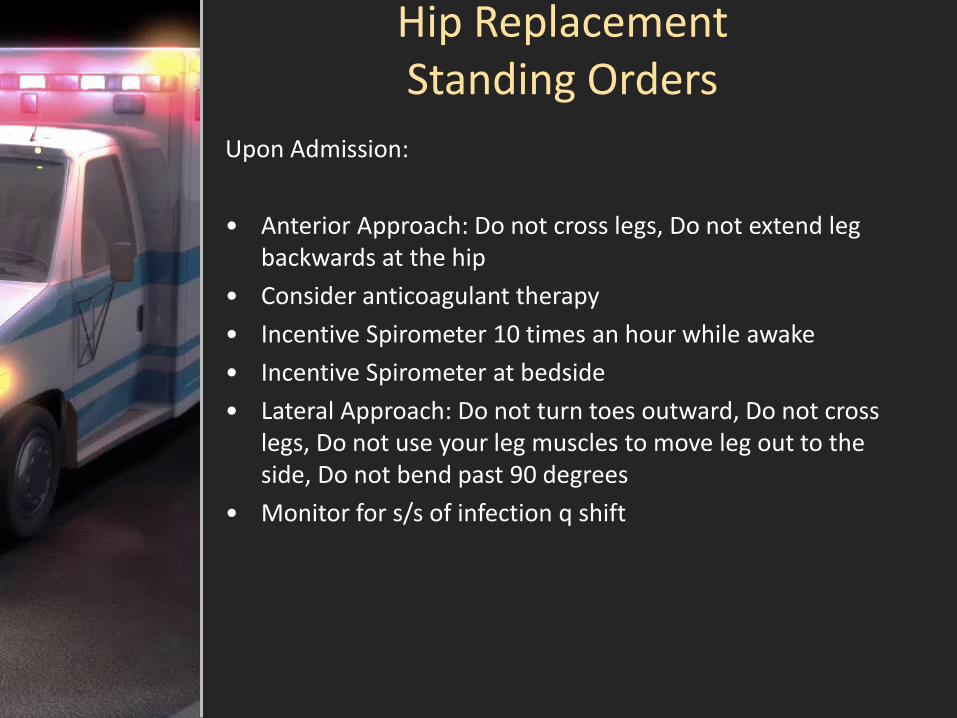
Hip Replacement Standing Orders
Upon Admission:
• Anterior Approach: Do not cross legs, Do not extend leg backwards at the hip
• Consider anticoagulant therapy
• Incentive Spirometer 10 times an hour while awake
• Incentive Spirometer at bedside
• Lateral Approach: Do not turn toes outward, Do not cross legs, Do not use your leg muscles to move leg out to the side, Do not bend past 90 degrees
• Monitor for s/s of infection q shift

Hip Replacement Standing Orders
• Monitor pain q shift
• Posterior Approach: Do not bend the hip past 90 degrees (keep knee always lower than your hips down toward the floor, no bending over or down to pick objects up off the floor, Get help or use a reacher, No sitting on low toilet seats or low/cushy chairs or couches, use a raised toilet seat, higher/firm cushion chair, or sit on 2 pillows, no rocking chairs. Do not cross the knees or ankles, use pillows between the legs, especially if you lie on your side

Clinical Outcomes
• Educational Outcomes
• Joint Replacement Program

Pulmonary Management Program
• Validated nursing and therapy competencies
• Outcome tracking
• Pulmonary rehabilitation
• Educational Booklet
– Signs and symptoms of COPD exacerbation
– Pneumonia-when to call the physician
– Prevention
– Medication management
• Smoking cessation classes
• Care coordinator involvement
• Venous Blood Gas lab draw within facility with quick results

Respiratory Therapist

Pulmonary Management Standing
Orders
•Administer O2 prn to keep sats >92%
•Dietary Consult
•Head of bed elevated at all times
•Incentive Spirometer 5 times an hour while awake
•O2 saturation every shift
•Up daily as tolerated
•Vital Signs every shift

Pulmonary Program Daily Checklist

Pulmonary Disease Care Path

Functional Outcome Measurement Respiratory System

Clinical Outcomes
COPD/Pneumonia Program

The i-STAT System
An advanced handheld diagnostic tool that provides real-time, lab-quality results within minutes.
• Used for the Cardiac and Pulmonary Programs
• Comprehensive Point-of-Care Testing
• Diagnostic Testing (results ranging from 2 min to 17 min)
–Electrolytes and Hematology
–Blood Gas
–Chemistry
–Cardiac Markers
–Coagulation
•www.abbottpointofcare.com

Applications for Apple Products
(CORE) Readmission Risk Calculator (iPad & iPhone)
– Developed by Yale-New Haven Hospital Center for Outcomes Research and Evaluation
– Supported by CMS
– Statistical model based on medical record data that can be used to predict the risk of readmission for heart attack, heart failure and pneumonia within 30 days.
Link to computer website
–http://www.readmissionscore.org/

(CORE) Readmission Risk Calculator

Physician and NP/PA Expectations
• Required presence in facility
• Rounding with nursing staff
• Quarterly Meeting Involvement
• Offer education and In-Services for staff/families
• New admissions seen in a timely manner
• Available for family conferences
• Facility leadership involvement
•Supportive of programs to reduce readmissions

Care Coordinator
Role • Assist with discharge planning from the hospital to SNF to home
• Provide the patient with easy to understand standardized educational material about the disease, using the teach back method to validate understanding
• Monitor the progression of the patient by ensuring program interventions are being followed
• Work collaboratively with the Nurse Practitioner and Primary Care Physician

Care Coordinator
Role (continued) • Medication reconciliation from the Acute Care Setting to the SNF
• Work collaboratively with a reputable Home Health Agency to coordinate a safe and sustainable transition to home
• Monitor clinical status of patient weekly for 4 weeks.
• If at any time the status of the patient is compromised for the first 30 days from hospital discharge, they will be urged to return to an HCMG facility to receive the necessary care unless it is life-threatening.

Nurse Practitioner
• Coordinate patient care with the Primary Care Physician and Interdisciplinary Team while in the SNF
• Continue coordinating care through the transition to home and thereafter
• First home visit 48-72 hours of discharge
• Clinical home data communicated to the Primary Care Physician
• Involve the patient and caregiver in standardized education
• Provide proactive medical management
• Coordinate and monitor medications from the SNF to home

Home Health Agency
• Coordinate and assist patient with their follow up visits to the family physician
• Medication reconciliation within day of discharge
• Promote patient compliance with their treatment program
• Provide standardized education
• Providing proactive medical management
• Proving standardized continuum of care by coordinating care with the HCMG Care Coordinator and Nurse Practitioner

Bridging Connections
Stay Well Home Health

How Often Home Health Patients had to be Admitted to the Hospital
Home Health Compare Website:
http://www.medicare.gov/homehealthcompare-search-html
Unplanned Hospital Readmission
Average (%)
Stay Well Home Health LLC
18%
National Average 17%
Ohio Average 18%


Becoming the Preferred Provider
• Design Unique Programs that are appealing to your local hospital and document outcomes for marketing.
–SNF provider
• Invest in staff training and education
• Invest in equipment
• Implement a system for calculating data
•Identify a champion within your organization to train, monitor and evaluate programs.
• Collect valid data which will allow you to present measureable outcomes.

Becoming the Preferred Provider
•Collaborate
– Monitor your readmission rates and be prepared to present yourself as a solution to the hospital’s problem.
• Consider a Care Coordinator role within your organization and develop partnerships with like-minded companies to ensure a smooth transition of care.

Bridging Connections
The Christ Hospital Health Network
Tri-health Hospitals
Bethesda North
Good Samaritan
Bridging Connections
The Jewish Hospital

Centers of Advanced Quality
Outcomes

The Christ Hospital
Urgent Care
• Retirement and Skilled Facilities
• Treatable Minor Injuries and/or Symptoms
• Twisted Ankle, knee and foot pain
• New joint swelling or pain
• Skin tears, Large liquid bruising, Open areas
• Crushed fingers, swelling and wound with loose nails
• Encrusted inflamed eyes
• Rashes, abscesses, inflammation of skin
• Sore throat, cough, head congestion
• Injuries due to falls (not head injuries)
• Urinary Tract Infection
The Jewish Hospital
Mercy Health
• Outpatient Referral Process for Skilled Nursing Facilities
• Residents have access to an urgent level of services and diagnostic resources without utilizing the emergency room.
• The Goal: reduce inappropriate emergency room utilization, improve emergency department length of stay and reduce inappropriate readmissions.
• Resident will discharge by 11pm; if not status will change to “observation” and contact nursing facility
• The Hospitalist has to see resident within 30 minutes to evaluate and all orders are STAT

Marketing Points
– Improved medical care R/T early identification of change of conditions
– Capitalize on the program’s uniqueness
– Better nursing assessment skills
– Better clinical outcomes
– Reduction in rehospitalizations – Positive reputation among hospitals, MCOs and the community at large
– Improved Customer/Family Satisfaction


“These materials and the intellectual property contained therein are Copyright 2012 and are the
exclusive property of The Health Care Management Group. Any use, reproduction, publication, transfer, display, distribution, copying, dissemination, display,
or adoption of these materials in other works without the express written permission of The Health Care Management Group is strictly prohibited and may give rise to criminal and civil penalties under the federal Copyright Act. All rights reserved by The
Health Care Management Group.”