redesigning the patient pathway for vestibular...
TRANSCRIPT
Redesigning the Patient Pathway for Vestibular
Services
Caroline Rae Vestibular Audiologist

NHS Tayside
Tayside Audiology and Balance Services (TABS)‐Population Covered: 405,721‐Location: Dundee, Scotland

Aims• Establish, using process mapping techniques, if the new audiology
direct access clinic for Labyrinthitis or Vestibular Neuritis leads to quality improvement for this patient demographic.
Objectives• Use a Systems Engineering Initiative for Patient Safety Model as a
framework for system redesign• Carry out a Hierarchical Task Analysis on the patient journey • Use a Systematic Human Error and Reduction and Prediction
Approach to identify any errors in the system• Carry out a clinical audit of the new audiology led direct access clinic
The Project

The human balance system• Even distribution of weight which enables someone to remain stable
and upright• Allows us to focus whilst moving and identify our orientation in space
with respect to gravity• Taken for granted but relies on a complex set of sensorimotor control
systems including, somatosensory, visual and vestibular
The Vestibular System• Bilateral input• Vertigo – illusion of movement• The ‘dizzy patient’
But First...

Vertigo and Dizziness rank among the most common reasons for attending primary care• Lifetime prevalence of 17‐30%• As common as headaches or backaches
Labyrinthitis/Vestibular Neuritis‐ Viral infection which affects the inner ear‐ Rotational Vertigo‐ Nausea/Vomiting‐ Diagnosis
‐ History, Hearing Test, Vestibular Assessment‐ Treatment
‐ Vestibular Rehabilitation ‐ Early intervention
The Dizzy Patient

• Highest quality services to those that require them. • Built around caring compassionate staff and services, clear
communication, effective collaboration between clinicians, patients and others involved
• Safety and efficiency are a high priority• An increasing partnership between health services, human factors and
systems engineering allowing for system redesign• Patient journey can be long
– patients, care givers, family members, healthcare practitioners, GPs, ENT consultants, audiologists, health psychologists, and physiotherapists
• Several handoffs
Quality Improvement

• Patient initially attends GP• Referral to ENT• Triaged for otology dizzy clinic• Attends ENT clinic
• Hearing test by Audiologist• History by ENT• Bedside assessment
• Further tests requested• Attends Audiology clinic for assessment
• Report back to ENT• Attend ENT clinic for diagnosis• Attend Audiology clinic for rehabilitation exercises
Initial Patient Pathway

• MULTIPLE REFERRALS/HANDOFFS
• INCREASED RISK OF REFERRAL BEING MISSED
• MULTIPLE APPOINTMENTS
• LONG WAITS

• Patient initially attends GP• Referral to ENT• Triaged for otology dizzy clinic• Attends ENT clinic
• PTA by Audiologist• History by ENT• Bedside assessment
• Further tests requested
• Attends Audiology clinic for assessment• Report back to ENT
• Attend ENT clinic for diagnosis
• Attend Audiology clinic for rehabilitation exercises

• Patient initially attends GP• Referral to ENT triaged for Audiology• Attends Audiology clinic for assessment
• Hearing Test, History, Vestibular Assessment• Attends Audiology clinic for rehabilitation exercises
How did we get to this point and is the clinic beneficial?
New Pathway
Systems Engineering
• Systems Engineering Initiative for Patient Safety (SEIPS)• Framework for understanding the structures, processes and
outcomes in health care anchored within human factors• Components include person, tasks, tools and technologies, physical
environments and organisational conditions• Interactions between different factors produce different outcomes• LOOK AT THE SYSTEM AS A WHOLE!


Person Tasks Tools and Technologies
Physical Environment
Organisation
Audiologist Physical, Cognitive and Psychosocial aspects described above all come in to play. Audiologist must be strong enough for patient manual handling, experienced enough to be aware of testing inaccuracies or non organic patients and have good motivation and support from Head of Service and ENT
Tasks involve direct patient care, care coordination, indirect patient care and no patient care. Administration tasks are as important as patient handling.
Electronic referral management system, clinical portal online case note system. TOPAS patient management system, AuditBase patient management system, Aurical equipment for pure tone audiometry and tympanometry, Computerised Dynamic Posturography, vHIT
Physical layout of the Audiology department, Soundproof room for pure tone audiometry assessment, Clinical room for vestibular assessment, rooms with black out blinds for vestibular assessment and rehabilitation
Interaction with ENT consultant, Interaction with Audiology Head of Service, BSA protocols for assessment, Local protocols for Audiology and Vestibular assessment and typing up documentation
Patient Patient knowledge, ability to give a good history, present symptoms, ability to cope with assessment, support system
Log of symptoms (diary)Vestibular rehabilitationRelaxation exercises
Patient information leaflets, vestibular rehabilitation exercise booklet
Lighting conditions and falls/tripping hazards at home for carrying out vestibular rehabilitation exercises
Access to department and vestibular rehabilitation

Hierarchical Task Analysis
• “Before improvements can be identified for a process, the process’s anatomy or steps must be understood”
• The HTA is highly structured • easier to produce graphically and • easier to revise as the mapping progresses.
• It offers flexibility in representing goals which did not correspond to specific acts at specific times • represents ongoing issues that could be triggered at any time
such as seeking help from a peer, patient education or tasks that are purely cognitive.
• A flexible tool that can be adapted to a variety of situations and needs. It can be used when modifying an existing design or creating a new design
• In this case used for process mapping the current and redesigned clinics


SHERPA
• The systematic human error reduction and prediction approach (SHERPA)
• It is a human error prediction technique that analyses tasks and identifies potential solutions to errors in a structured manner.
• The technique has been applied to pilot error, the use of consumer products, vending machines being an example and to reduce the risk of errors during surgeries.
• SHERPA uses the bottom level action of the HTA as its inputs. These are the operations or task steps carried out to achieve the higher level goal.

Task Step Error Probability Criticality Remediation
1.3 Referred via online referral management
Communication low low Ensure GPs are aware of Referral Management Protocols
3.4 Patient added to system
Communication low low Check up in place to make sure all appointment added to system
5.1 Notes Requested Communication low low Data stored electronically too
8.1 Referral form filled out
Communication low low Letter also sent
6.2 Marked as arrived on AuditBade
Communication low low Physically check patient has arrived
11.1 Referred back to ENT
Communication low low
17.1 Brief history Communication low low Continuous care form one clinician
Clinical Audit (New Clinic)
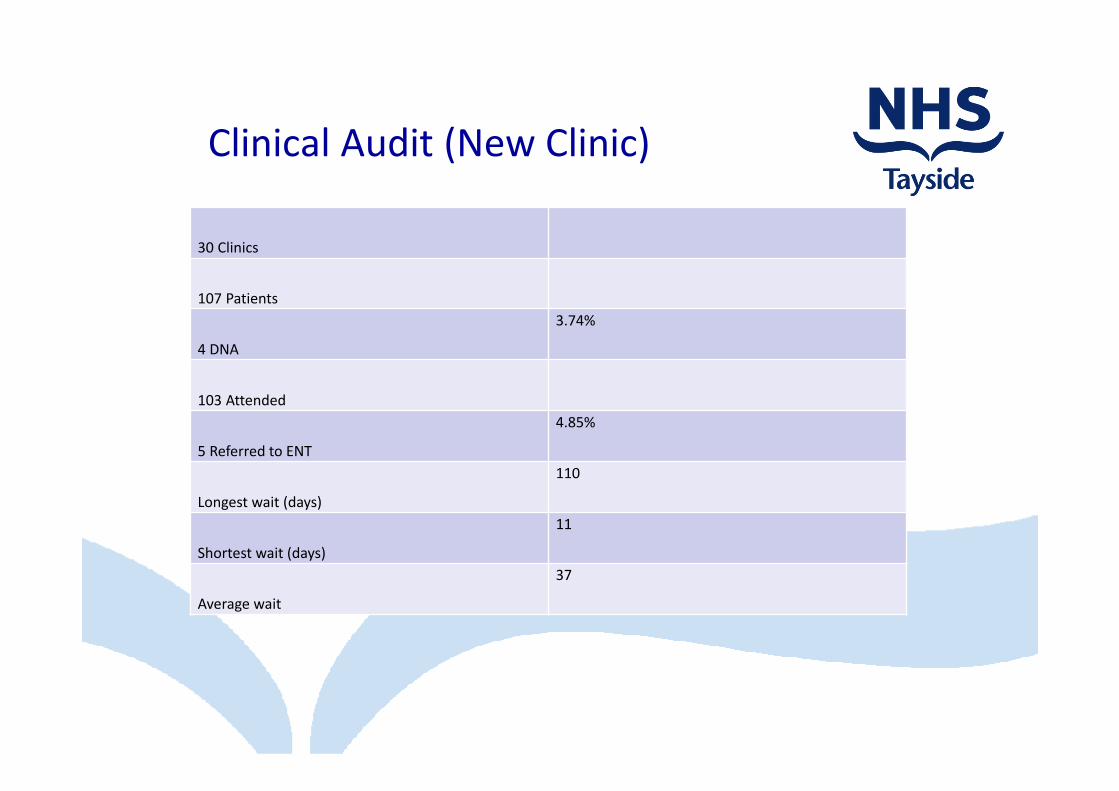
30 Clinics
107 Patients
4 DNA
3.74%
103 Attended
5 Referred to ENT
4.85%
Longest wait (days)
110
Shortest wait (days)
11
Average wait
37

Waiting lists
• The clinical audit data for the audiology led direct access clinic are very positive and promising.
• These patients initially waited just over 100 days for their appointment and towards the end of the trial were waiting just over 20 days. The average wait over the span of this clinic was 37 days.
• Meeting national legislation guidelines• Missing out some of the steps of the original ENT pathway and utilising the
skills sets available has helped to reduce waiting times dramatically and allow patients to be seen and treated quickly.
• The HTA shows that the vestibular patient is added to the waiting lists three times during their pathway. Each time this happens there are inherent risks, particularly with risk of the referral being ‘lost’ in the system or increased patient waits.
• most of the referrals for vestibular assessment are seen within 6‐8 weeks but there is a distinct possibility of a long patient journey for the vestibular patient before they even reach vestibular rehabilitation.

DNA’s• The national average DNA rate for first outpatient appointment is
10%. • Interestingly the highest rate for DNA in national averages was for
ENT. • It is thought that each outpatient DNA costs NHS Scotland £120• The DNA rate for this clinic is a third that of the national average at
3.74%, again showing that altering the patent pathway has proved beneficial.
Referrals• There are only a few patients referred back to ENT, this is generally
linked to inappropriate information on the referral letter or patient request to see an ENT Consultant.

Skills Mix• One of the biggest benefits of the Audiologist led clinic is the better
use of available resources. This means that skilled, well trained Audiologists can be used for this clinic. The average specialist Audiologist will still cost over half that of a newly hired consultant and a quarter of a more senior consultant.

Conclusions
• The results show that vestibular patients with vestibular neuritis or labyrinthitis can be well managed by Vestibular Audiologists.
• This has been shown in the clinical audit and the HTA. • The HTA has been shown to be beneficial in mapping the clinic
pathway even though this is not always used in health care settings. • This is still a new clinic and there are still some aspects that can be
put in place to improve it but this looks very promising for the future and the benefit of the HTA is that this can grow and change as the clinic grows and changes.

Thank you for listening