redefining resuscitation
TRANSCRIPT

Ken Hillman
REDEFINING RESUSCITATION
Don Harrison Perpetual Lecture,
Spark of Life Conference, Perth.
7th-10th April 2011


HISTORY OF
RESUSCITATION
LIFE-SAVING AFTER NEAR-DROWNING
HOLLAND 1767 – Society for resuscitation of the drowned
BRITAIN 1774 – Society for the recovery of persons apparently drowned
Royal Humane Society for the Apparently Dead
2/0179

RESUSCITATION Trespassing the boundary between life
and death
Scientifically possible (sometimes)
Religious - only the Creator could give or
Ethical take life
2/0190

RESUSCITATION – rekindling the
flame of a taper by blowing gently –
MEDICINE’s work
RE-ANIMATION – bringing a corpse
back to life after the spark is fatally
extinct – GOD’s work
2/0161

RESUSCITATION
DOESN’T WORK AFTER
PUTREFACTION HAS SET
IN!!
Royal HUMANE Society 1809
2/0163
REVIVING TEMPORARILY
DEAD PEOPLE
1803 – religiously sound
activity
2/0162

EARLY RESUSCITATION
TECHNIQUES
• Warming
• Rolling body over barrel
• Rubbing the body
• Tickling throat with a feather
2/0191

2/0127

2/0128

UP UNTIL WORLD
WAR II
• Fogging on mirror over mouth –
warm
• No fogging on mirror – SILVESTER
or SCHAFER resuscitation
techniques
2/0165

2/0110

HOLGER NIELSON
TECHNIQUE
Back pressure + arm lift
Started dominating post-World War II
2/0166

2/0111

THE AIRWAY!
Not considered until
Safar 1958
2/0167
CPR
Combination of
• Open airway
• Mouth to mouth respiration
• External cardiac compressions
2/0168

1968 – INCONSISTENT ARTIFICIAL
VENTILATION – GERMAN STUDY 1968
Aim to compare ventilatory effect of:
Howard-Thomsen
Holger Nielsen Chest compression
Silvester-Brosch Arm lift
Mouth-to-nose Exhaled air
Mouth-to-mouth
Acta Anaesth Scand 1968; suppl XXIX

GA – pentobarbitone
Paralysed with methyl-curare
Ventilation with Ambu bag + Ruben valve
Femoral artery catheter
ECG
End exp CO2 %
Pulse rate
Acta Anaesth Scand 1968; suppl XXIX

“LATIN SQUARE” SEQUENCE Volunteers Methods
1+6 A C B E D
2+7 D A E C B
3+8 B D C A E
4+9 C E D B A
5+10 E B A D C
A – Mouth to nose
B – Mouth to mouth
C – Howard-Thomsen
D – Holger Nielsen
E – Silvester-Brosch
Acta Anaesth Scand 1968; suppl XXIX

ABG - normal ventilation
Apnoea - 60 secs
Then one of the 5 ‘methods’
• ABGs/30 sec for 3 min
• The ‘method’ for 9 min
Acta Anaesth Scand 1968; suppl XXIX

ABG - Clark electrode
pH & PaCO2 - Astrup
O2 sat - slide rule designed by
Severinghaus
Acta Anaesth Scand 1968; suppl XXIX
SOME CASES
PaO2 <30 mmHg
O2 sat < 50%
Acta Anaesth Scand 1968; suppl XXIX

CONCLUSION
Manual methods should no
longer be used
Acta Anaesth Scand 1968; suppl XXIX

CPR
• Initially for anaesthesia – induced
cardiac arrest
• “Miraculous, effective, simple”
Kovwenlioven NEJM 1960;173:1064
2/0062

CPR “Anywhere….. Anytime”
Universally applicable to
death and dying – no matter
what the cause
2/0170

CPR LEADS TO:
• Medical personnel in ambulances
• Paramedics
• Coronary Care Units
2/0171

1970’s Widespread community
awareness and education
programmes
2/0193

CPR
• Intimately linked to the practice of
medicine
• Associated with acute medicine through
the media
2/0033

CARDIAC ARREST
TEAM
2/0012
2/0022

HOSPITAL CPR
• Most die in hospital
• Half of all survivors have
significant decrease in
functional status Arch Int Med 2000;160:1969
2/0068

IN-HOSPITAL CARDIAC
ARRESTS
• Extracorporeal CPR
• Better than CPR
Crit Care Med 2011;39:1

PORTRAYAL CPR ON
TELEVISION
UK USA
Survival 16% 77%
2/0045

2/0108

REDEFINING
RESUSCITATION IN ACUTE
HOSPITALS
• Where and why do patients have
cardiac arrests?
• Moving from CPR to patient centered
resuscitation
• The role of DNR?
• The future?
2/0078

REDEFINING
RESUSCITATION
WHERE AND WHY DOES
CPR OCCUR IN HOSPITALS?
2/0013

PATIENTS SUDDENLY
DIE IN GENERAL
HOSPITAL WARDS NOT
IN ICU/OT/ED
ENVIRONMENTS
2/0032

WHY DO PATIENTS HAVE
CARDIAC ARRESTS IN
HOSPITAL?
Up to 80% of all so-called ‘arrests’ are
preceded by at least 8 hours of slow
deterioration in vital signs
2/0013
Schein et al Chest 1990;98:1388

WHY DO PATIENTS HAVE
CARDIAC ARRESTS IN
HOSPITAL?
Silo based hospital function
Medical specialisation
Vital sign measurement
Nurses are trained to measure not act
Doctors act on them in hierarchical way
Poor resuscitation training
2/0013

SICK PATIENT
NURSE OBSERVES BUT CAN’T ACT
TRAINEE DOCTORS ACT BUT NOT
TRAINED
SPECIALIST – TRAINED BUT NOT IN
ACUTE MEDICINE
EVENTUALLY MULTIORGAN
FAILURE/CARDIAC ARREST AND
ADMITTED TO ICU
Systems to
connect first
signs with
acute care
specialists
1.2/0073

2/0026

DOES A MET/RRS
WORK?
2/0017

SINGLE CENTRE STUDIES
ALL SHOW A REDUCTION
IN CARDIAC ARRESTS
AND DEATHS
• System implementation is different from
drug and procedural implementation
• A large Hawthorn effect is essential
2/0017

BEFORE/AFTER
MET
50% reduction in CARDIAC ARRESTS
after casemix adjustment odds ratio
0.5: 95% CI 0.35-0.73
BMJ 2002;324:387
2/0039

BEFORE/AFTER MET STUDY
Before After Difference RR
95% CI 95% CI
Cardiac arrests 63 22 41(23-59) 0.35(0.22-0.57)
Deaths from cardiac
arrests 37 16 21(7-35) 0.43(0.26-0.70)
No. days in ICU>C.arrest 163 33 130(110-150) 0.20(0.13-0.33)
No.days in hospital
>C.arrest 1353 159 1194(1119-1269) 0.11(0.70--.79)
Inpatient deaths 302 222 80(37-123) 0.74(0.70-0.79)
MJA 2003;179(6):283-287
2/0040

THE MEDICAL
EMERGENCY
RESUSCITATION
INTERVENTIONAL TRIAL
(MERIT) STUDY
1.4/0002

EVIDENCE
MERIT
Inconclusive – underpowered
1.4/0340
Lancet 2005;365:2091-2097

REDEFINING
RESUSCITATION
FINDINGS AND INSIGHTS
Lancet 2005;365:2091-2097
1.4/0122

CONFOUNDERS
• Over 30% of calls in control
hospitals were ‘MET’ calls –
contamination
• Large variability in MET
hospitals
2/0017

CONFOUNDERS Less than half of all events
had vital signs criteria
documented in the eight
hours beforehand
Lancet 2005;365:2091-2097

CONFOUNDERS In patients with documented
MET criteria followed by an
event, only a minority of
patients overall had an actual
MET call made
1.4/0122 Lancet 2005;365:2091-2097

PROPORTION OF MISSING VITAL
SIGNS WITHIN 24 h OF SERIOUS
ADVERSE EVENT
Respiratory rate - approx 25%
Heart rate - approx 8%
BP - approx 6%
Resuscitation 2009;80:35

INTERVENTIONS
Emergency Team Calls (ie non-cardiorespiratory arrest)
512 control hospitals
1864 MET hospitals
Only 5 of these were not critical care interventions
Only 1 had an assessment/examination
Resuscitation 2010;81:25

META ANALYSIS
30% reduction in paediatric mortality
and cardiac arrest rates
30% reduction in adult cardiac arrest
rates
Not achieved by any other intervention
Chen et al 2010;170(1):18-26

MERIT STUDY
The MET system reduces
mortality
Crit Care Med 2009;37:148-153

RAPID RESPONSE
SYSTEMS
• Majority of US hospitals – IHI
• Majority of Canadian hospitals
• UK – mandatory outreach and now RRSs
• Scandinavia – spreading
• Holland – national implementation underway
• Sporadic – Mexico, Subcontinent, remainder of Europe

RAPID RESPONSE
SYSTEMS - AUSTRALIA
• NSW – being rolled out in every acute hospital
• Australia – implementation guidelines being developed by the Australian Commission on Safety and Quality in Health Care

REDEFINING
RESUSCITATION
Is about system implementation
as well as
Individual clinical skills
2/0017

EFFECTIVE IMPLEMENTATION
OF RAPID RESPONSE SYSTEMS
1. Triggering criteria
2. Response – 24/7 of at least one person with advanced resuscitation skills
3. Ownership and administration within a hospital
4. Education • Awareness – EVERYONE
• Basic resuscitation – NURSES AND ON-SITE MEDICAL STAFF
• Advanced resuscitation – MINIMUM 1 PERSON 24/7
5. Key performance Indicators (KPIs) • Measure problem
• Track implementation and maintenance
• Measure effectiveness
ALL IMPLEMENTED SIMULTANEOUSLY

REDEFINING RESUSCITATON
MOVE FROM:
CARDIAC ARREST TEAMS
SYSTEM BUILT AROUND AT-RISK PATIENTS – 24/7 system to identify all at-risk patients
– Patient centred triage according to level of illness
– Small 24/7 teams skilled in ALL aspects of managing the seriously ill, including CPR
2/0113

HOSPITAL CARDIAC ARRESTS
ARE SENTINAL EVENTS
- SHOULD BE SUBJECT TO
DETAILED ANALYSIS
• Most are potentially preventable
• Many should have been DNR
• Few are sudden and unexpected

REDEFINING
RESUSCITATION
THE PLACE OF DNR
2/0017

REDEFINING
RESUSCITATION
• CPR has a low survival rate
• CPR works best in witnessed arrests
with sudden arrhythmia
• CPR almost never works at the natural
end of life in a dying person- witnessed
or non witnessed.
2/0017

• IF CPR UNLIKELY TO BE
– appropriate
– successful
• WHY WRITE DNR ORDERS?
• DISCUSS DYING AND HOW IT IS
TO BE MANAGED
2/0090
HOSPITAL - CPR
CRUEL AND DISHONEST
PERIMORTEM RITUAL
2/0059

THINKING DNR?
Catalyst to begin honest discussions:
• Medical condition
• Therapeutic options
• Prognosis
2/0097

DNR = Diagnosis of dying
= Medicine has no more to offer
= Change thrust of care
HONESTY AND PALLIATION
2/0050

REDEFINING
RESUSCITATION
THE FUTURE

SERIOUSLY ILL AT-RISK
PATIENT vs CARDIAC ARREST
PATIENT
“The seriously ill at-risk patient”
is a syndrome similar to the
“coronary artery syndrome”
2/0178
PATIENT-CENTRED
RESUSCITATION
This is not waiting until the
patient’s heart has stopped
and instituting CPR
2/0017

COMMUNITY
EXPECTATIONS
Sophisticated
and well organised systems to
guarantee patient safety at all
times
2/0140

FUTURE OF MONITORING
• Universal
• Non-invasive
• Wireless
Signals not boxes
Algorithms for signals
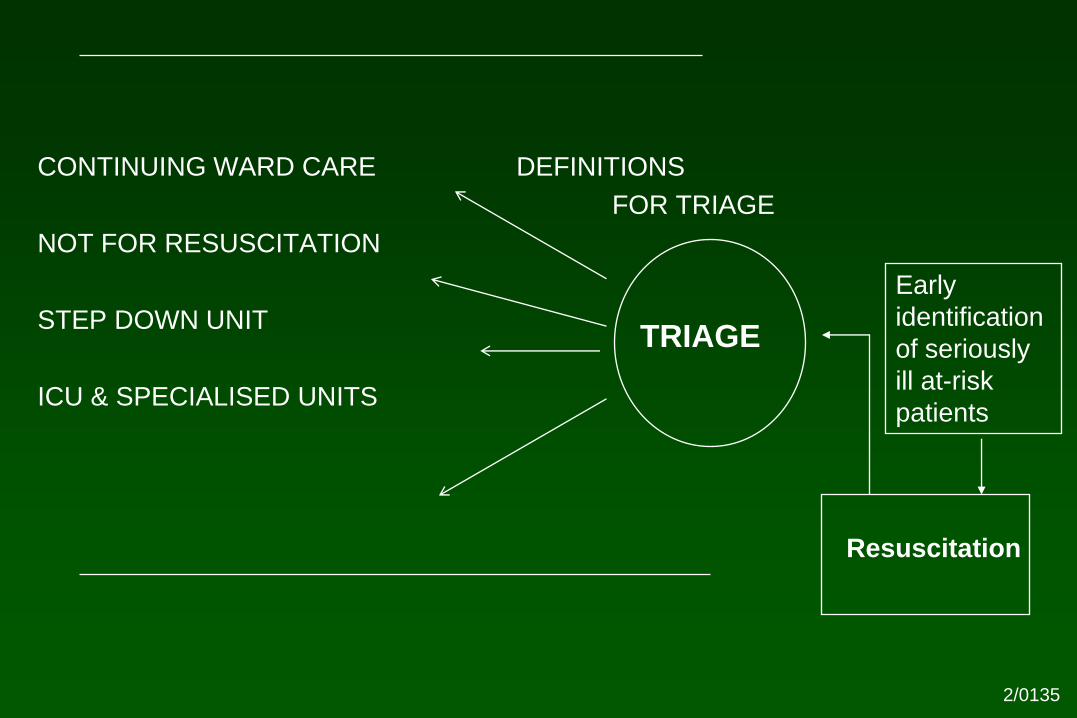
CONTINUING WARD CARE DEFINITIONS
FOR TRIAGE
NOT FOR RESUSCITATION
STEP DOWN UNIT
ICU & SPECIALISED UNITS
TRIAGE
Resuscitation
Early
identification
of seriously
ill at-risk
patients
2/0135

REDEFINING
RESUSCITATION
• Resuscitation is not only CPR
• Resuscitation is a complex set of skills
and experience used to stabilise acutely
ill patients
• Require at least one person at all times
in a hospital with appropriate advanced
skills, knowledge and experience 2/0017

NEED TO CARE FOR
CRITICALLY ILL
PATIENTS
NOT
CRITICAL CARE UNITS