recommendations for well-woman care – a well-woman chart
TRANSCRIPT

Rec
omm
enda
tion
s fo
r W
ell-W
oman
Car
e –
A W
ell-W
oman
Cha
rt
©20
21, C
onte
nt o
wne
d by
the
ACO
G F
ound
atio
n, a
ll M
arks
and
Rig
hts
Rese
rved
. Thi
s pr
ojec
t was
sup
port
ed b
y th
e H
ealth
Res
ourc
es a
nd S
ervi
ces
Adm
inis
trat
ion
(HRS
A) o
f the
U.S
. Dep
artm
ent o
f Hea
lth a
nd H
uman
Ser
vice
s (H
HS)
und
er g
rant
num
ber U
HO
MC
2994
0, B
righ
t Fut
ures
for W
omen
’s H
ealth
: Sta
ndar
d Pr
actic
e G
uide
lines
for
Wel
l Wom
en C
are.
Thi
s in
form
atio
n or
con
tent
and
con
clus
ions
are
thos
e of
the
auth
or a
nd sh
ould
not
be
cons
true
d as
the
offic
ial p
ositi
on n
or p
olic
y of
, nor
shou
ld a
ny e
ndor
sem
ents
be
infe
rred
by
HRS
A, H
HS,
or t
he U
.S. G
over
nmen
t.
a Addi
tiona
l Bri
ght F
utur
es re
com
men
datio
ns in
clud
e: p
erio
dic
visi
on a
nd h
eari
ng te
sts
for a
ges
13-2
1; ri
sk a
sses
smen
t for
ane
mia
for a
ges
13-2
1; an
d flu
orid
e su
pple
men
tatio
n if
need
ed fo
r age
s 13
-16
(htt
ps://
dow
nloa
ds.a
ap.o
rg/A
AP/P
DF/
peri
odic
ity_s
ched
ule.
pdf)
b Imm
uniz
atio
ns sh
ould
be
adm
inis
tere
d ac
cord
ing
to th
e m
ost r
ecen
t AC
IP re
com
men
datio
ns (h
ttps
://w
ww
.cdc
.gov
/vac
cine
s/sc
hedu
les/
inde
x.ht
ml)
.
Abb
revi
atio
ns:
ACIP
= A
dvis
ory
Com
mitt
ee o
n Im
mun
izat
ion
Prac
tices
; BRC
A =
brea
st c
ance
r sus
cept
ibili
ty g
ene;
CRC
= c
olor
ecta
l can
cer;
CVD
= c
ardi
ovas
cula
r di
seas
e; H
IV =
hum
an im
mun
odefi
cien
cy v
irus
; HC
V =
hepa
titis
C v
irus
; HBV
= h
epat
itis
B vi
rus;
STI
= s
exua
lly tr
ansm
itted
infe
ctio
n; U
SPST
F =
U.S
. Pre
vent
ive
Serv
ices
Tas
k Fo
rce;
WPS
I = W
omen
’s P
reve
ntiv
e Se
rvic
es In
itiat
ive.
*Cri
teri
a fo
r se
lect
ive
use
1. Lo
w-d
ose
aspi
rin
to p
reve
nt c
ardi
ovas
cula
r dis
ease
and
col
orec
tal c
ance
r: C
alcu
late
d 10
-yea
r ris
k of
a C
VD e
vent
≥10
%; n
ot a
t inc
reas
ed ri
sk
for b
leed
ing;
hav
e a
life
expe
ctan
cy o
f at l
east
10 y
ears
; and
are
will
ing
to ta
ke lo
w-d
ose
aspi
rin
daily
for a
t lea
st 10
yea
rs.
2. D
iabe
tes
scre
enin
g an
d m
anag
emen
t: O
verw
eigh
t or o
bese
for a
ge 4
0-70
yea
rs; p
revi
ous
gest
atio
nal d
iabe
tes
but n
ot p
revi
ousl
y di
agno
sed
with
dia
bete
s m
ellit
us w
hen
not p
regn
ant f
or a
ge ≥
13 y
ears
.3.
Fol
ic a
cid
supp
lem
enta
tion:
Sex
ually
act
ive
and
plan
ning
or c
apab
le o
f pre
gnan
cy.
4. H
ealth
y di
et a
nd p
hysi
cal a
ctiv
ity c
ouns
elin
g: O
verw
eigh
t or o
bese
and
hav
e ad
ditio
nal C
VD ri
sk fa
ctor
s (h
yper
tens
ion,
dys
lipid
emia
, abn
orm
al
bloo
d gl
ucos
e le
vels
, dia
bete
s). S
peci
fic a
ntic
ipat
ory
guid
ance
for a
ges
13-1
7 m
ay b
e fo
und
in th
e Br
ight
Fut
ures
Gui
delin
es.
5. L
ipid
scr
eeni
ng: F
amili
al d
yslip
idem
ia, r
isk
fact
ors,
or h
igh-
risk
con
ditio
ns fo
r age
13-1
6 ye
ars;
uni
vers
al s
cree
ning
onc
e be
twee
n ag
e 17
-21 y
ears
; cl
inic
al ju
dgem
ent f
or a
ge 2
2-39
yea
rs.
6. O
steo
poro
sis
scre
enin
g: 10
-yea
r fra
ctur
e ri
sk e
quiv
alen
t to
an a
vera
ge-r
isk
65-y
ear o
ld w
oman
bas
ed o
n sp
ecifi
c ri
sk fa
ctor
s (p
aren
tal h
isto
ry
of h
ip fr
actu
re, s
mok
ing,
whi
te ra
ce, e
xces
s al
coho
l con
sum
ptio
n, lo
w b
ody
wei
ght)
.7.
Stat
in u
se to
pre
vent
CVD
: Ag
e 40
to 7
5 ye
ars;
one
or m
ore
CVD
risk
fact
ors
(i.e
., dy
slip
idem
ia, d
iabe
tes,
hyp
erte
nsio
n, o
r sm
okin
g);
and
calc
ulat
ed 10
-yea
r ris
k of
a C
VD e
vent
≥10
%.
8. U
rina
ry in
cont
inen
ce s
cree
ning
: Scr
een
all w
omen
age
18 a
nd o
lder
and
you
nger
wom
en if
pos
tpar
tum
.9.
Gon
orrh
ea a
nd c
hlam
ydia
scr
eeni
ng: N
ew s
ex p
artn
er, m
ore
than
one
sex
par
tner
, a s
ex p
artn
er w
ith c
oncu
rren
t par
tner
s, o
r a s
ex p
artn
er
who
has
an
STI;
inco
nsis
tent
con
dom
use
am
ong
pers
ons
who
are
not
in m
utua
lly m
onog
amou
s re
latio
nshi
ps; p
revi
ous
or c
oexi
stin
g ST
I; an
d ex
chan
ging
sex
for m
oney
or d
rugs
. Pre
vale
nce
is a
lso
high
er a
mon
g in
carc
erat
ed p
opul
atio
ns, m
ilita
ry re
crui
ts, a
nd p
atie
nts
rece
ivin
g ca
re a
t pub
lic S
TI c
linic
s.
10. H
epat
itis
B sc
reen
ing:
Bor
n in
a c
ount
ry w
ith a
pre
vale
nce
of H
BV in
fect
ion
≥2%
; lac
k of
vac
cina
tion
in in
fanc
y in
U.S
.-bor
n pe
rson
s w
ith
pare
nts
from
a c
ount
ry o
r reg
ion
with
pre
vale
nce
≥8%
; HIV
-pos
itive
per
sons
; inj
ectio
n dr
ug u
sers
; and
hou
seho
ld c
onta
cts o
r sex
ual p
artn
ers
of p
erso
ns w
ith H
BV in
fect
ion.
11. H
epat
itis
C s
cree
ning
: One
-tim
e sc
reen
ing
for a
sym
ptom
atic
adu
lts a
ge 18
to 7
9 w
ithou
t kno
wn
liver
dis
ease
. Re
peat
scre
enin
g an
d sc
reen
at o
ther
ag
es if
pas
t or c
urre
nt in
ject
ion
drug
use
.12
. HIV
pre
expo
sure
pro
phyl
axis
(PrE
P): C
andi
date
s fo
r inc
lude
1) h
eter
osex
ually
act
ive
wom
en w
ith a
ser
odis
cord
ant s
ex p
artn
er (i
.e.,
in a
sex
ual
rela
tions
hip
with
a p
artn
er li
ving
with
HIV
); or
inco
nsis
tent
use
of c
ondo
ms
duri
ng s
ex w
ith a
par
tner
who
se H
IV s
tatu
s is
unk
now
n an
d w
ho is
at
hig
h ri
sk; o
r an
STI w
ith s
yphi
lis o
r gon
orrh
ea w
ithin
the
past
6 m
onth
s; 2
) use
s in
ject
ion
drug
s an
d sh
ared
use
of d
rug
inje
ctio
n eq
uipm
ent;
or h
as ri
sk o
f sex
ual a
cqui
sitio
n of
HIV
bas
ed o
n ab
ove;
3) e
ngag
ed in
tran
sact
iona
l sex
, suc
h as
for m
oney
, dru
gs, o
r oth
er.
13. S
exua
lly tr
ansm
itted
infe
ctio
n pr
even
tion
coun
selin
g: R
isk
fact
ors
for S
TIs
incl
ude
havi
ng a
n ST
I cur
rent
ly o
r with
in th
e pa
st y
ear,
not
cons
iste
ntly
usi
ng c
ondo
ms,
hav
ing
mul
tiple
sex
par
tner
s, o
r hav
ing
sex
part
ners
with
in p
opul
atio
ns w
ith a
hig
h pr
eval
ence
of S
TIs.
Incr
ease
d ST
I pre
vale
nce
rate
s ar
e fo
und
amon
g w
omen
see
king
STI
test
ing
or a
tten
ding
STI
clin
ics;
sex
ual a
nd g
ende
r min
oriti
es; a
nd a
mon
g th
ose
with
H
IV, u
sing
inje
ctio
n dr
ugs,
exc
hang
ing
sex
for m
oney
or d
rugs
, or r
esid
ing
in c
orre
ctio
nal f
acili
ties.
14
. Syp
hilis
scr
eeni
ng: W
omen
with
HIV
; hig
h pr
eval
ence
com
mun
ities
or p
opul
atio
ns; h
isto
ry o
f inc
arce
ratio
n; e
xcha
ngin
g se
x fo
r mon
ey o
r dru
gs.
15. T
uber
culo
sis
infe
ctio
n: P
erso
ns fr
om c
ount
ries
with
incr
ease
d tu
berc
ulos
is p
reva
lenc
e; li
ving
in h
igh-
risk
con
greg
ate
sett
ings
(e.g
., ho
mel
ess
shel
ters
, cor
rect
iona
l fac
ilitie
s); e
xpos
ure
to in
divi
dual
s w
ith a
ctiv
e tu
berc
ulos
is, s
uch
as h
ealth
car
e w
orke
rs a
nd w
orke
rs in
hig
h-ri
sk
cong
rega
te s
ettin
gs; i
mm
unos
uppr
esse
d in
divi
dual
s.16
. Bre
ast c
ance
r scr
eeni
ng: N
o sp
ecifi
c cr
iteria
, dec
isio
ns a
bout
scre
enin
g ar
e m
ade
on a
n in
divi
dual
bas
is th
roug
h a
shar
ed-d
ecis
ion
mak
ing
proc
ess.
17. L
ung
canc
er s
cree
ning
: 30
pack
-yea
r sm
okin
g hi
stor
y an
d cu
rren
tly s
mok
e or
hav
e qu
it w
ithin
the
past
15 y
ears
.18
. Med
icat
ions
to re
duce
bre
ast c
ance
r ris
k: M
ajor
risk
fact
ors
for b
reas
t can
cer i
nclu
de in
crea
sing
age
, fam
ily h
isto
ry o
f bre
ast o
r ova
rian
can
cer
(esp
ecia
lly a
mon
g fir
st-d
egre
e re
lativ
es a
nd o
nset
bef
ore
age
50 y
ears
), hi
stor
y of
aty
pica
l hyp
erpl
asia
or o
ther
non
mal
igna
nt h
igh-
risk
bre
ast
lesi
ons,
pre
viou
s br
east
bio
psy,
and
ext
rem
ely
dens
e br
east
tiss
ue. M
odel
s su
gges
t tha
t wom
en w
ith a
n es
timat
ed 5
-yea
r bre
ast c
ance
r ris
k of
3%
or g
reat
er a
re li
kely
to h
ave
mor
e be
nefit
than
har
m, a
lthou
gh th
e ba
lanc
e of
ben
efits
and
har
ms
depe
nds
on a
ge, r
ace
or e
thni
city
, the
m
edic
atio
n us
ed, a
nd w
heth
er th
e pa
tient
has
a u
teru
s.19
. Ski
n ca
ncer
cou
nsel
ing:
Fai
r ski
n, li
ght h
air a
nd e
ye c
olor
, fre
ckle
s, s
unbu
rn e
asily
.20
. Per
inat
al d
epre
ssio
n pr
even
tive
inte
rven
tions
: Cou
nsel
ing
inte
rven
tions
for w
omen
with
one
or m
ore
of th
e fo
llow
ing:
a h
isto
ry o
f dep
ress
ion,
cu
rren
t dep
ress
ive
sym
ptom
s tha
t may
not
reac
h a
diag
nost
ic th
resh
old,
soci
oeco
nom
ic ri
sk fa
ctor
s suc
h as
low
inco
me
or a
dole
scen
t or s
ingl
e pa
rent
hood
, rec
ent i
ntim
ate
part
ner v
iole
nce,
or m
enta
l hea
lth–r
elat
ed fa
ctor
s suc
h as
ele
vate
d an
xiet
y sy
mpt
oms o
r a h
isto
ry o
f sig
nific
ant
nega
tive
life
even
ts.
21. P
reec
lam
psia
pre
vent
ion
with
low
-dos
e as
pirin
: His
tory
of p
reec
lam
psia
, esp
ecia
lly w
hen
acco
mpa
nied
by
an a
dver
se o
utco
me;
mul
tifet
al g
esta
tion;
ch
roni
c hy
pert
ensi
on; t
ype
1 or 2
dia
bete
s mel
litus
; ren
al d
isea
se; a
utoi
mm
une
dise
ase
(sys
tem
ic lu
pus e
ryth
emat
ous,
antip
hosp
holip
id sy
ndro
me)
.22
. Dia
bete
s sc
reen
ing
afte
r pre
gnan
cy: P
revi
ous
gest
atio
nal d
iabe
tes
but n
ot p
revi
ousl
y di
agno
sed
with
dia
bete
s m
ellit
us w
hen
not p
regn
ant.
PREVENTION SERVICESAGE (Years)
13 –17a 18–21a 22–39 40–49 50–64 65–75 >75 GENERAL HEALTH
Alcohol use screening & counseling Anxiety screening
CVD & CRC prevention with aspirin1 50-59 Blood pressure screening Contraceptive counseling & methods Depression screening Diabetes screening2
Fall prevention
Folic acid supplementation3
Healthy diet & activity counseling4
Interpersonal & domestic violence screening
Lipid screening5
Obesity screening & counseling Osteoporosis screening6
Statin use to prevent CVD7
Substance use screening & assessment Tobacco screening & counseling Urinary incontinence screening8
INFECTIOUS DISEASES
Gonorrhea & chlamydia screening9 ≤24 >24Hepatitis B screening10
Hepatitis C screening (at least once)11 <80HIV preexposure prophylaxis12
HIV risk assessmentHIV screening (at least once) >15Immunizationsb
STI prevention counseling13
Syphilis screening14
Tuberculosis screening15
CANCER
Breast cancer screening16
Cervical cancer screening ≥21 ≤65Colorectal cancer screeningLung cancer screening17 55-80 55-80Medications to reduce breast cancer risk18
Risk assessment for BRCA 1/2 testingSkin cancer counseling19 ≤24
PREVENTION SERVICESfor pregnancy provided in addition to age-based services listed above.
PREGNANCYAnxiety screening
Bacteriuria screeningBreastfeeding counseling, services & suppliesContraceptive counseling & methodsDepression screening & preventive interventions20
Folic acid supplementationGestational diabetes screeningGonorrhea & chlamydia screeningHepatitis B screeningHIV screening (each pregnancy)Interpersonal & domestic violence screeningPreeclampsia prevention with low-dose aspirin21
Preeclampsia screeningRh(D) blood typingSubstance use screening & assessment
Syphilis screeningTobacco screening & counseling
PREVENTION SERVICESfor postpartum provided in addition to age-based services listed above.
POSTPARTUMAnxiety screening
Breastfeeding counseling, services & suppliesContraceptive counseling & methodsDepression screening & preventive interventions20
Diabetes screening after gestational diabetes22
Folic acid supplementationInterpersonal & domestic violence screeningSubstance use screening & assessment
Tobacco screening & counseling
KEY: Recommended by the USPSTF (A or B rating), WPSI, or Bright Futures Recommended for selected use
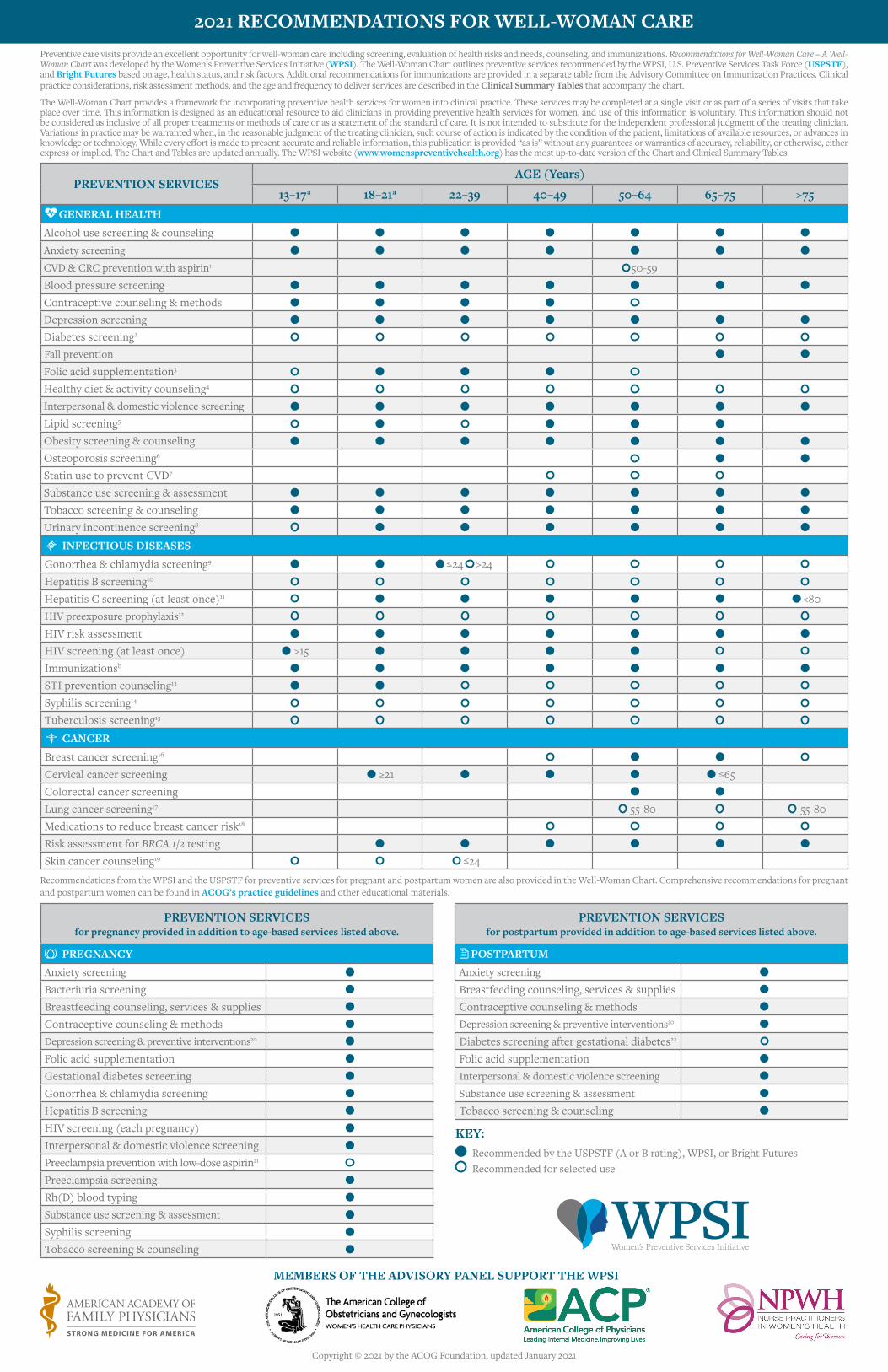
Preventive care visits provide an excellent opportunity for well-woman care including screening, evaluation of health risks and needs, counseling, and immunizations. Recommendations for Well-Woman Care – A Well-Woman Chart was developed by the Women’s Preventive Services Initiative (WPSI). The Well-Woman Chart outlines preventive services recommended by the WPSI, U.S. Preventive Services Task Force (USPSTF), and Bright Futures based on age, health status, and risk factors. Additional recommendations for immunizations are provided in a separate table from the Advisory Committee on Immunization Practices. Clinical practice considerations, risk assessment methods, and the age and frequency to deliver services are described in the Clinical Summary Tables that accompany the chart.
The Well-Woman Chart provides a framework for incorporating preventive health services for women into clinical practice. These services may be completed at a single visit or as part of a series of visits that take place over time. This information is designed as an educational resource to aid clinicians in providing preventive health services for women, and use of this information is voluntary. This information should not be considered as inclusive of all proper treatments or methods of care or as a statement of the standard of care. It is not intended to substitute for the independent professional judgment of the treating clinician. Variations in practice may be warranted when, in the reasonable judgment of the treating clinician, such course of action is indicated by the condition of the patient, limitations of available resources, or advances in knowledge or technology. While every effort is made to present accurate and reliable information, this publication is provided “as is” without any guarantees or warranties of accuracy, reliability, or otherwise, either express or implied. The Chart and Tables are updated annually. The WPSI website (www.womenspreventivehealth.org) has the most up-to-date version of the Chart and Clinical Summary Tables.
Recommendations from the WPSI and the USPSTF for preventive services for pregnant and postpartum women are also provided in the Well-Woman Chart. Comprehensive recommendations for pregnant and postpartum women can be found in ACOG’s practice guidelines and other educational materials.
2021 RECOMMENDATIONS FOR WELL-WOMAN CARE
MEMBERS OF THE ADVISORY PANEL SUPPORT THE WPSI
Copyright © 2021 by the ACOG Foundation, updated January 2021