recognizing shock: diagnosis and management
TRANSCRIPT

Recognizing Shock: Diagnosis and Management
Song Li, MD, FACCAdvanced Heart Failure and Transplant Cardiology
University of Washington
10/18/2019

DISCLOSURESong Li, MD
No relevant financial relationship reported.
Cardiogenic Shock Remains a Deadly Condition
• Complicates 6-10% of STEMI
• In-hospital mortality remains high (27%–51%), especially among patients > 75 years old
• 1-year all-cause and HF rehospitalization rates of 59% and 33%
• NYHA class II to IV symptoms at 1 year: 43%
• Average total hospital cost: $41,774
Van Diepen. Circulation. 2017;136:e232–e268.

Definition of Cardiogenic Shock
• Low cardiac output state resulting in life-threatening end-organ hypoperfusion and hypoxia
• The SHOCK, IABP-SHOCK II trials and ESC HF guidelines definitions based on clinical, hemodynamic, and laboratory criteria
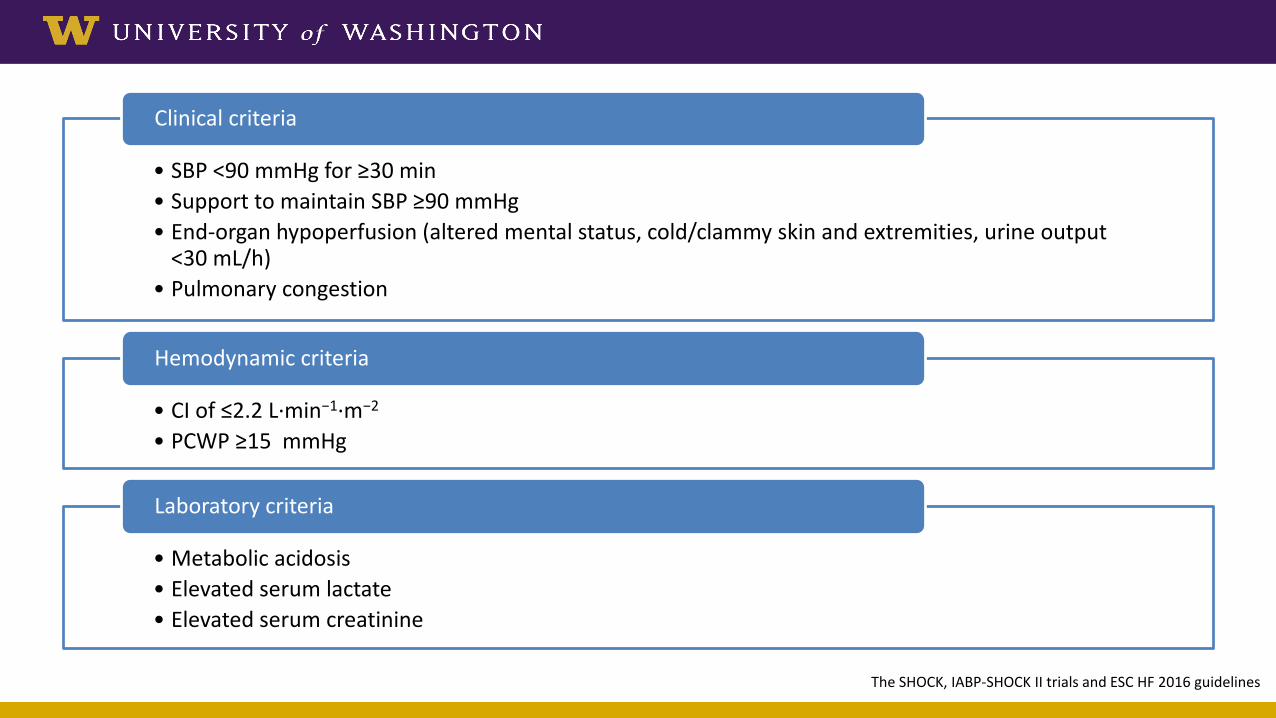
• SBP <90 mmHg for ≥30 min• Support to maintain SBP ≥90 mmHg• End-organ hypoperfusion (altered mental status, cold/clammy skin and extremities, urine output
<30 mL/h)• Pulmonary congestion
Clinical criteria
• CI of ≤2.2 L·min−1·m−2
• PCWP ≥15 mmHg
Hemodynamic criteria
• Metabolic acidosis• Elevated serum lactate• Elevated serum creatinine
Laboratory criteria
The SHOCK, IABP-SHOCK II trials and ESC HF 2016 guidelines

Pathophysiology of Cardiogenic Shock
Van Diepen. Circulation. 2017;136:e232–e268.

Shock Phenotypes
Van Diepen. Circulation. 2017;136:e232–e268.
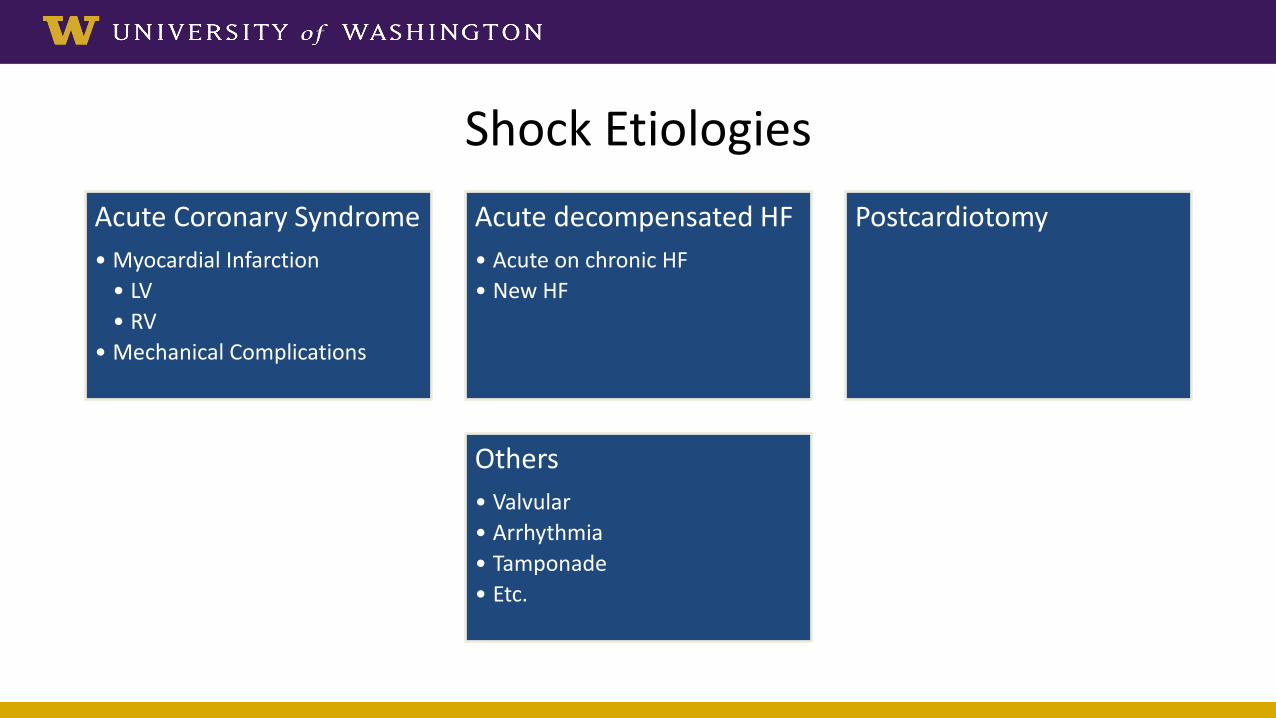
Shock EtiologiesAcute Coronary Syndrome• Myocardial Infarction
• LV• RV
• Mechanical Complications
Acute decompensated HF• Acute on chronic HF• New HF
Postcardiotomy
Others• Valvular• Arrhythmia• Tamponade• Etc.

Management of Cardiogenic Shock

Van Diepen. Circulation. 2017;136:e232–e268.

Vasoactive Drugs
Van Diepen. Circulation. 2017;136:e232–e268.
Tailor to shock etiology. Necessary evil with long-term harm.

Early Revascularization Key For Acute MI and Shock
SHOCK trial, 1999
Hochman, J. et al. JAMA 2006: 295(21), 2511-2515.

CULPRIT-SHOCK, 2018 (MI and Shock) COMPLETE, 2019 (STEMI)
Culprit PCI followed by staged complete revascularization
Culprit vs. Complete Revascularization

Temporary Mechanical Circulatory Support (MCS)

PV Loop and Mechanical Work
Uriel, N. et al. J Am Coll Cardiol. 2018;72(5):569-580

The Spectrum of MCS Options
Atkinson, T. et al. JACC: Cardiovascular Interventions 2016: 9(9), 871-883.
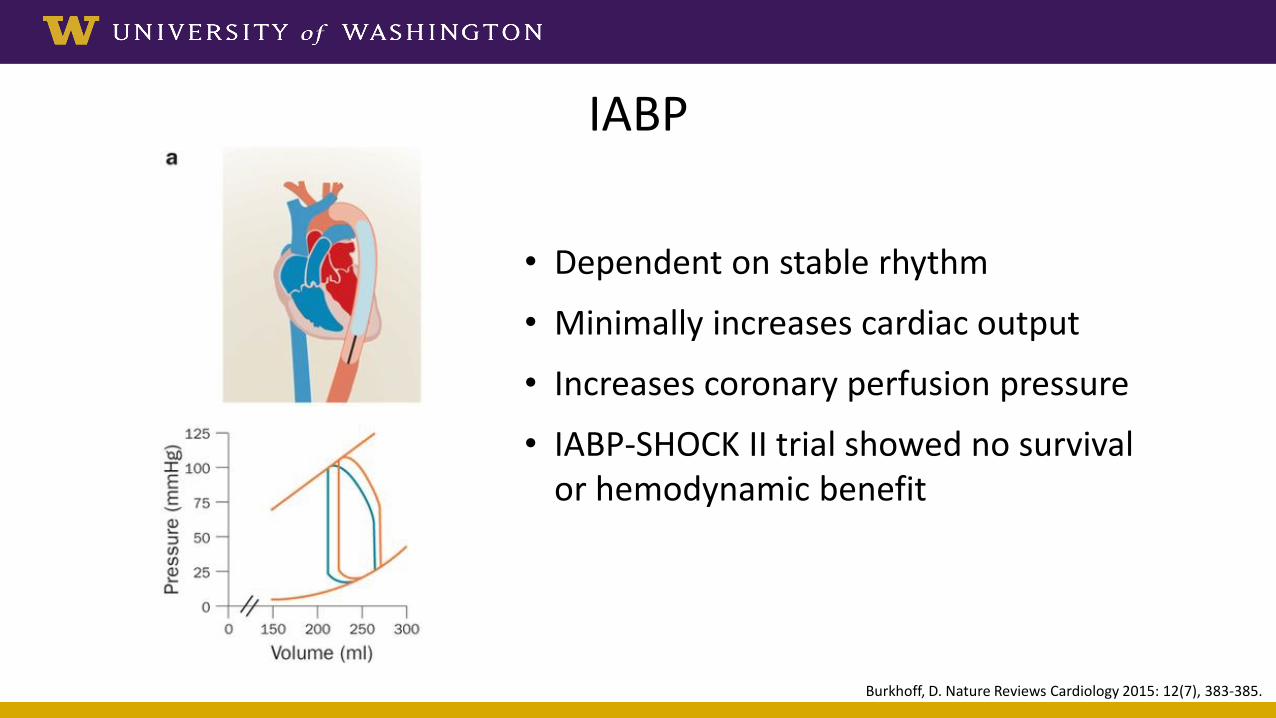
IABP
Burkhoff, D. Nature Reviews Cardiology 2015: 12(7), 383-385.
• Dependent on stable rhythm
• Minimally increases cardiac output
• Increases coronary perfusion pressure
• IABP-SHOCK II trial showed no survival or hemodynamic benefit

VA-ECMO
Burkhoff, D. Nature Reviews Cardiology 2015: 12(7), 383-385. Rao, P., et al. Circulation: Heart Failure 2018: 11(9), e004905.
• Without LV vent, ECMO increases afterload and filling pressure
• Causes LV distention and pulm edema
• Increases mechanical work
• Good for cardiac arrest, BiV failure, and refractory hypoxia

LV Vent is Important for VA-ECMO
Rao, P., et al. Circulation: Heart Failure 2018: 11(9), e004905.

TandemHeart
Burkhoff, D. Nature Reviews Cardiology 2015: 12(7), 383-385.
• Trans-septal puncture
• Provides 3.5 - 5 L/min of flow
• Decreases preload
• Can increase afterload

Impella
Burkhoff, D. Nature Reviews Cardiology 2015: 12(7), 383-385.
• **Directly unloads the LV**
• Reduces LV mechanical work
• Position is key
• LV – AO pressure uncoupling

LV and AO Pressure Uncoupling
Uriel, N. et al. J Am Coll Cardiol. 2018;72(5):569-580

Comparison
Burkhoff, D. Nature Reviews Cardiology 2015: 12(7), 383-385.

Optimizing Cardiogenic Shock Outcomes

Cardiogenic Shock and Timing of MCS
Esposito, M., Kapur, N. F1000Research 2017: 6, 737.

Hemo-Metabolic Shock: Too Late
Morine & Kapur et al. Cardiogenic Shock Working Group

MCS Threshold for Cardiogenic Shock:Too Little or Too Late:

New Concept: Door to Unload
Kapur, N., Davila, C. European Heart Journal 2017: 38(47), 3532-3534

LV unloading before reperfusion may reduce infarct size and LV remodeling
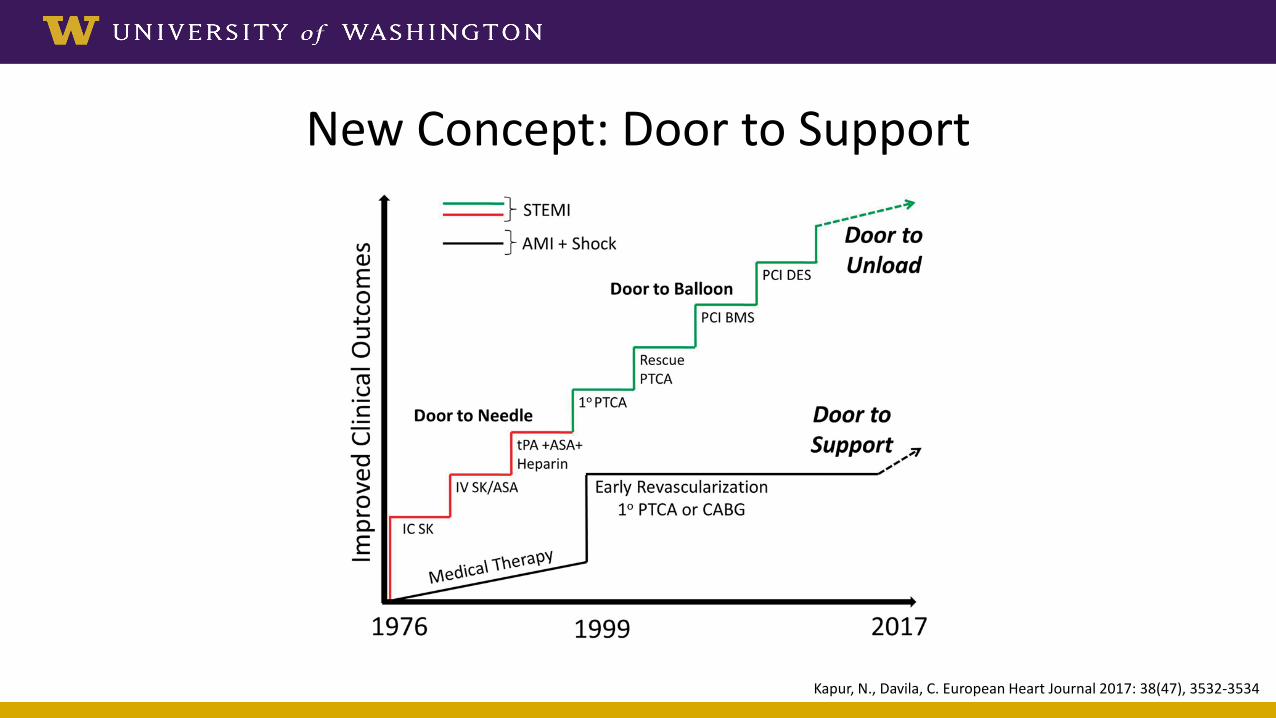
New Concept: Door to Support
Kapur, N., Davila, C. European Heart Journal 2017: 38(47), 3532-3534

Shock Regional Systems of Care
Van Diepen. Circulation. 2017;136:e232–e268.

Shock Team Approach
Taleb, I. et al. Circulation 2019: 140(1), 98-100.
The Cardiogenic Shock Working GroupMulti-Center Acute MCS Registry

Conclusions• Cardiogenic shock remains a condition with high M&M• Early revascularization is key for ACS related cardiogenic shock• “Pumps pump blood; people save lives”
– Understand hemodynamic effects of different MCS platforms– Unload the LV– Initiate MCS before irreversible hemo-metabolic deterioration
• New concepts of “door to unload” and “door to support” are worth studying
• Team-based approach and regional systems of care are promising ways to improve outcomes