recognizing early sepsis signs improves patient care
TRANSCRIPT

Sepsis Inpatient Pilot Project
Recognizing Early Sepsis Signs
Improves Patient Care
C4 | Nipping Infection in the Bud February 25, 2016 Thursday
1430-1530
Sepsis Inpatient Pilot Project
We are unable to identify any
potential conflict of interest
and have nothing to disclose.

Background
• Early recognition and intervention of Sepsis improves patient outcomes.
• Despite significant work done in
Emergency Departments (ED), there is still a gap between early identification of patients who are clinically deteriorating related to Sepsis and timely investigation and treatment.
• It is imperative to expand pivotal work around Sepsis Screening and Treatment from EDs to in-patient units.


Project Goal
• To reduce in-patient Sepsis morbidity and mortality through early identification, timely intervention and appropriate monitoring using best clinical practices and achieving seamless transitions of care.
Purpose
• To standardize care of in-patients developing early sepsis through implementing a Sepsis Screening Tool and piloting a new Early Sepsis Pre-Printed Order Set.

Methods
• Pilot units: CP10CD Acute Medicine units at Vancouver General Hospital (VGH)
– Acute Hospitalist Units
– 24-bed patients
• Pilot period: October 2014 -October 2015
• Sepsis QI Interdisciplinary team formed in collaboration with the British Columbia Safety & Quality Council (BCPSQC)
• Small PDSA cycles, refinement of Sepsis tools

Tools

Assumptions
We’re going to save the world!
“You begin saving the world by saving one man at a time; all else is grandiose romanticism or politics.”
Charles Bukowski

Results
24 in-patients developed Sepsis Oct 2014-Aug 2015
– Group 1: 15 patients: nurse identified early sepsis symptoms AND physicians completed PPO
– Group 2: 4 patients: nurse identified early sepsis, but physician did not use the PPO
– Group 3: 5 patients: nurse missed the early sepsis signs
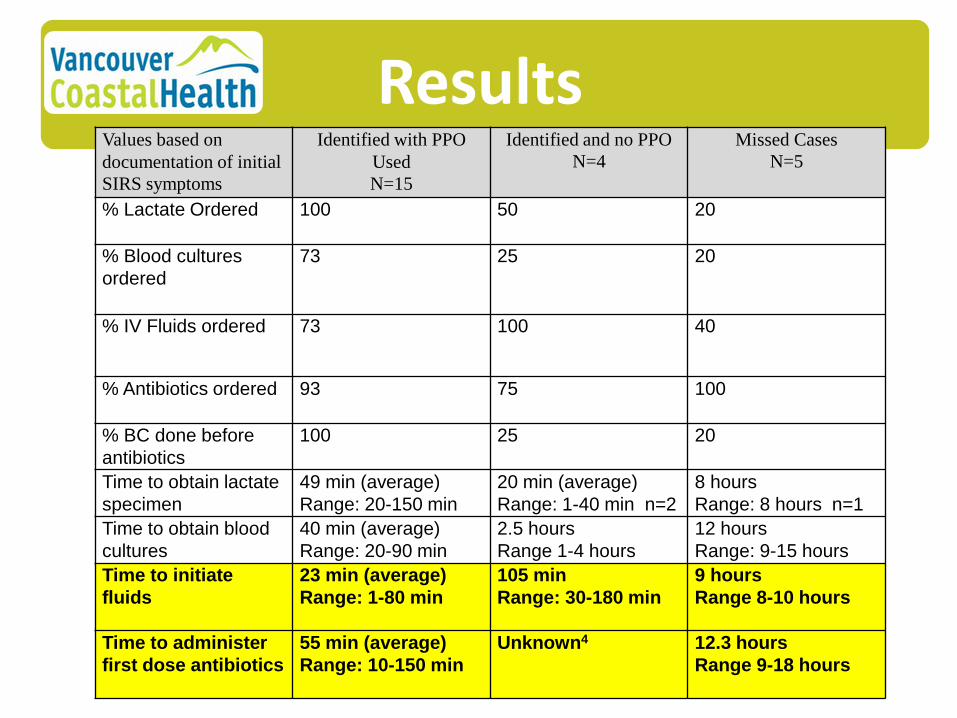
Results
Values based on
documentation of initial
SIRS symptoms
Identified with PPO
Used
N=15
Identified and no PPO
N=4 Missed Cases
N=5
% Lactate Ordered
100 50 20
% Blood cultures
ordered
73 25 20
% IV Fluids ordered
73 100 40
% Antibiotics ordered
93 75 100
% BC done before
antibiotics
100 25 20
Time to obtain lactate
specimen
49 min (average)
Range: 20-150 min
20 min (average)
Range: 1-40 min n=2
8 hours
Range: 8 hours n=1
Time to obtain blood
cultures
40 min (average)
Range: 20-90 min
2.5 hours
Range 1-4 hours
12 hours
Range: 9-15 hours
Time to initiate
fluids
23 min (average)
Range: 1-80 min
105 min
Range: 30-180 min
9 hours
Range 8-10 hours
Time to administer
first dose antibiotics
55 min (average)
Range: 10-150 min
Unknown4 12.3 hours
Range 9-18 hours

Challenges Ongoing engagement of stakeholders and sustainability of program
“Difficult roads often lead to beautiful destinations.”
Anonymous

Biggest Change
Empowerment among staff “You can, you should, and if you’re brave enough to start, you will.” Stephen King

Significant Lesson
The importance of Team "Alone we can do so little, together we can do so much." Helen Keller
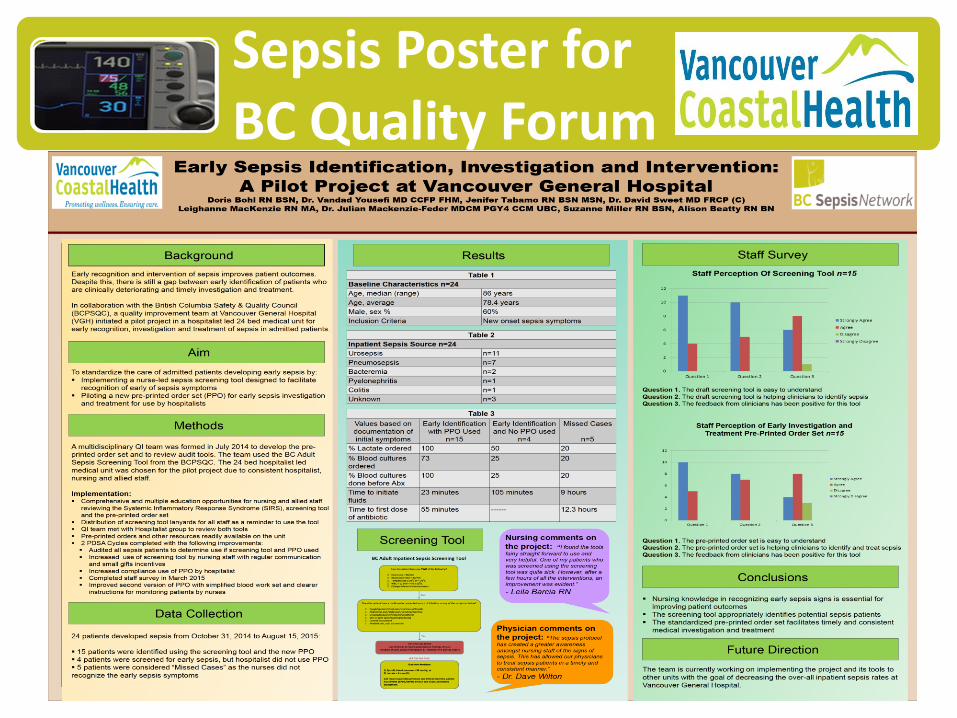
Sepsis Poster for BC Quality Forum

Acknowledgement
• Dr. David Sweet
• Chantelle Pamplin
• Leighanne Mackenzie
• Dr. Vandad Yousefi
• Dr. Julian Mackenzie-Feder
• Alison Beaty
• Suzanne Miller
• Bryn Lander
Jenifer Tabamo, RN, BSN, MSN Clinical Nurse Specialist Medicine Program, Vancouver Acute Vancouver General Hospital Tel: 604-875-4111 Local 64143 BB: 604-803-1862 Email: [email protected]
For more information…
Doris Bohl, RN, BSN Clinical Nurse Educator Units CP 7th Floor and CP 10 CD Vancouver General Hospital Office: 604-875-4111 local 69424 Mobile: 604-809-1279 Email: [email protected]