recent trends in the treatment of primary breast cancer
TRANSCRIPT

RECENT TRENDS IN THE TREATMENT OF PRIMARY BREAST CANCER
SAMUEL ALBERT, MD, PHD,+.~ STEVEN BELLE, MSc HYG,+.§ AND
G. MARIE SWANSON, PHD**"
In response to the continuing controversy over the treatment of primary breast cancer, a review of treatment practices in Metropolitan Detroit for the years 1973 through 1976 has been undertaken to determine what effect, if any, this controversy has had on clinical practice. The study population comprised 6132 females first diagnosed as having breast cancer during this period. Three treat- ment modalities-mastectomy alone, mastectomy plus radiotherapy alone, and mastectomy plus chemotherapy alone, comprising 96.8% of treated cases-were studied. The data indicate that significant changes occurred in surgical treat- ment and adjuvant therapy during this period. The proportion of patients receiving partial and modified radical mastectomy rose, while the use of the simple and radical procedures fell in each year. The use of chemotherapy increased throughout the study period while utilization of radiotherapy ap- peared to be on the decline, after peaking in 1975. In 1976, about 18% of all cases had received adjuvant chemotherapy, compared to 2% in 1973. By 1976, this modality was on an equal footing with radiotherapy as an adjuvant ther- apy. These changes were a function of both stage of disease and age of the patient at diagnosis. Adjuvant chemotherapy was most frequently used for disease staged as regional (30% of cases) and remote (45% of cases). The study shows that, at a time when there is dissatisfaction about the treatment of primary breast cancer, physician attitudes are very sensitive and react quite rapidly to new recommendations.
Cancer 41:2399-2404, 1978.
N THE LAST FEW YEARS, THERE HAS BEEN A I great deal of discussion about the treatment of primary breast cancer in both the lay and medical press. For example, considerable con- troversy exists over the type of mastectomy ap- propriate for obtaining results. 1,8,13 There are those who feel that radical surgery is the proper treatment for primary breast cancer. Others feel that radical mastectomies are unnecessarily mu- tilating and that more conservative surgery is as effective. This debate has become so intense that the American Cancer Society issued a policy
From the *Department of Biometry and Medical So- ciology and 'Department of Epidemiology, Michigan Cancer Foundation, Detroit, Michigan.
Supported in part by the National Cancer Institute's Sur- veillance, Epidemiology and End Results (SEER) program (contract number GP61028).
t Chief, Field Studies Unit. 5 Biostatistician. 'I Chairman. Address for reprints: Samuel Albert, MD, PhD, Chief,
Field Studies Unit, Department of Epidemiology, Michigan Cancer Foundation, 110 E. Warren, Detroit, MI 48201.
The authors thank the Michigan Cancer Foundation (MCF) Cancer Registry staff for their interest and sup- port
Acceptrd for publication September 26, 1977.
statement regarding surgical treatment for oper- able breast cancer. l5
The use of surgery as the sole treatment for breast cancer dropped from 67% to 55% between the intervals 1950-1954 and 1960-1964. During this same period of time, utilization of radio- therapy as the only adjuvant to surgery in- creased slightly from 17% to 22%. However, che- motherapy was the sole adjunct to surgery in 7% of patients in 1960-1964 as compared to only 1% in the earlier interval.' However, the question of the most effective adjuvant therapy is as yet unanswered. Some believe that surgery in con- junction with radiotherapy is effective in con- trolling recurrence and yields better survival than other treatment regimens. ",17 Others refute the effectiveness of radiotherapy. 2,11,1* More re- cently, support is being given for the use of adjuvant Chemotherapy. '*lo
In this atmosphere of controversy over surgery and radiotherapy and anticipation of progress through the use of adjuvant chemotherapy, one must ask what trends have developed in the treatment practices in a community. To this end, a review of treatment of primary breast cancer in the Metropolitan Detroit area, be- tween 1973 and 1976 inclusive, was undertaken.
0008-54X-78-0600-2399-0075 @ American Cancer Society
2399
2400 CANCER June 1978 Vol. 41
TABLE 1. Female Breast Cancers
Microscopically Year of Number of Confirmed
diagnosis cases (percent)
1973 1632 97.6 1974 1962 97.1 1975 1811 97.4 1976* 727 98.5
TOTAL 6132 97.5
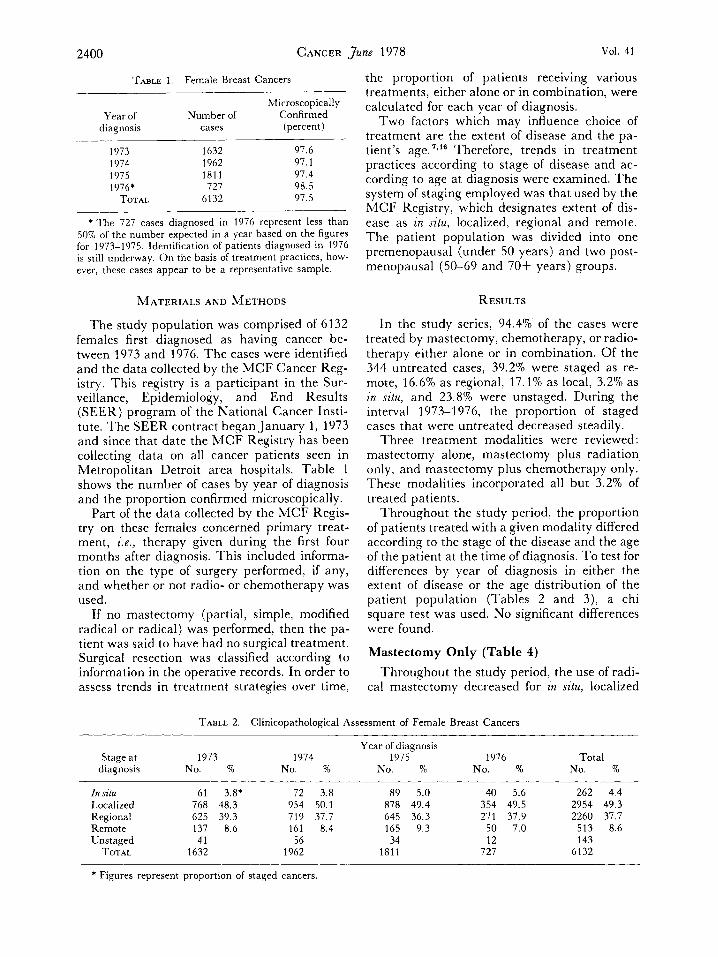
* T h e 727 cases diagnosed in 1976 represent less than 50% of the number expected in a year based on the figures for 1973-1975. Identification of patients diagnosed in 1976 is still underway. On the basis of treatment practices, how- ever, these cases appear to be a representative sample.
MATERIALS AND METHODS
The study population was comprised of 6132 females first diagnosed as having cancer be- tween 1973 and 1976. The cases were identified and the data collected by the MCF Cancer Reg- istry. This registry is a participant in the Sur- veillance, Epidemiology, and End Results (SEER) program of the National Cancer Insti- tute. The SEER contract began January 1, 1973 and since that date the MCF Registry has been collecting data on all cancer patients seen in Metropolitan Detroit area hospitals. Table 1 shows the number of cases by year of diagnosis and the proportion confirmed microscopically.
Part of the data collected by the MCF Kegis- try on these females concerned primary treat- ment, &., therapy given during the first four months after diagnosis. This included informa- tion on the type of surgery performed, if any, and whether or not radio- or chemotherapy was used.
If no mastectomy (partial, simple, modified radical or radical) was performed, then the pa- tient was said to have had no surgical treatment. Surgical resection was classified according to information in the operative records. In order to assess trends in treatment strategies over time,
the proportion of patients receiving various treatments, either alone or in combination, were calculated for each year of diagnosis.
Two factors which may influence choice of treatment are the extent of disease and the pa- tient's age. 'ql' Therefore, trends in treatment practices according to stage of disease and ac- cording to age at diagnosis were examined. The system of staging employed was that used by the MCF Registry, which designates extent of dis- ease as in situ, localized, regional and remote. The patient population was divided into one premenopausal (under 50 years) and two post- menopausal (50-69 and 70+ years) groups.
RESULTS
In the study series, 94.4% of the cases were treated by mastectomy, chemotherapy, or radio- therapy either alone or in combination. Of the 344 untreated cases, 39.2% were staged as re- mote, 16.6% as regional, 17.1% as local, 3.2% as zn situ, and 23.8% were unstaged. During the interval 1973-1976, the proportion of staged cases that were untreated decreased steadily.
Three treatment modalities were reviewed: mastectomy alone, mastectomy plus radiation only, and mastectomy plus chemotherapy only. These modalities incorporated all but 3.2% of treated patients.
Throughout the study period, the proportion of patients treated with a given modality differed according to the stage of the disease and the age of the patient at the time of diagnosis. To test for differences by year of diagnosis in either the extent of disease or the age distribution of the patient population (Tables 2 and 3), a chi square test was used. No significant differences were found.
Mastectomy Only (Table 4) Throughout the study period, the use of radi-
cal mastectomy decreased for in situ, localized
TABLE 2. Clinicopathological Assessment of Female Breast Cancers
Year of diagnosis Stage at 1973 1974 1975 1976 Total
diagnosis No. % No. % No. % No. % No. %
In situ 61 3.8* 72 3.8 89 5.0 40 5.6 262 4.4 Localized 768 48.3 954 50.1 878 49.4 354 49.5 2954 49.3 Regional 625 39.3 719 37.7 645 36.3 271 37.9 2260 37.7 Remote 137 8.6 161 8.4 165 9.3 50 7.0 513 8.6 Unstaged 41 56 34 12 143
TOTAL 1632 1962 1811 727 6132
* Figures represent proportion of staged cancers.
No. 6 BREAST CANCER TREATMENT Albert et al. 2401
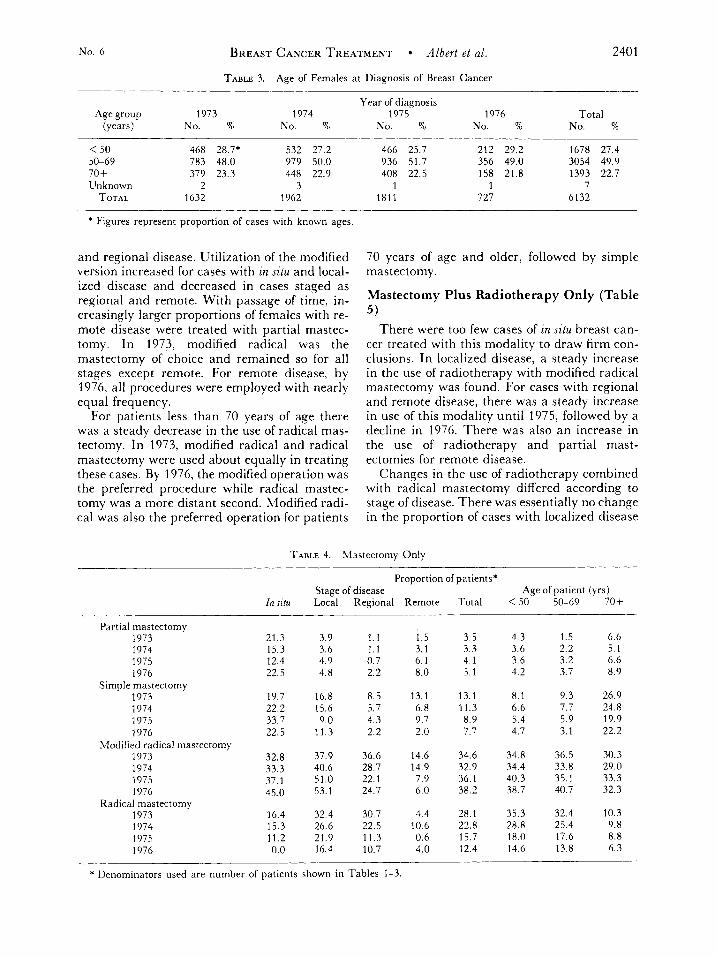
TABLE 3. Age of Females at Diagnosis of Breast Cancer
Year of diagnosis Age group 1973 1974 1975 1976 Total
(years) No. % NO. % No. % NO. 90 No. %
< 50 468 28.7. 532 27.2 50-69 783 48.0 979 50.0 70 + 379 23.3 448 22.9 Unknown 2 3
TOTAL 1632 1962
* Figures represent proportion of cases with known ages
and regional disease. Utilization of the modified version increased for cases with zn sztu and local- ized disease and decreased in cases staged as regional and remote. With passage of time, in- creasingly larger proportions of females with re- mote disease were treated with partial mastec- tomy. In 1973, modified radical was the mastectomy of choice and remained so for all stages except remote. For remote disease, by 1976, all procedures were employed with nearly equal frequency.
For patients less than 70 years of age there was a steady decrease in the use of radical mas- tectomy. In 1973, modified radical and radical mastectomy were used about equally in treating these cases. By 1976, the modified operation was the preferred procedure while radical mastec- tomy was a more distant second. Modified radi- cal was also the preferred operation for patients
466 25.7 212 29.2 1678 27.4 936 51.7 356 49.0 3054 49.9
1393 22.7 408 22.5 158 21.8 1 1 7
1811 727 6132
70 years of age and older, followed by simple mastectomy.
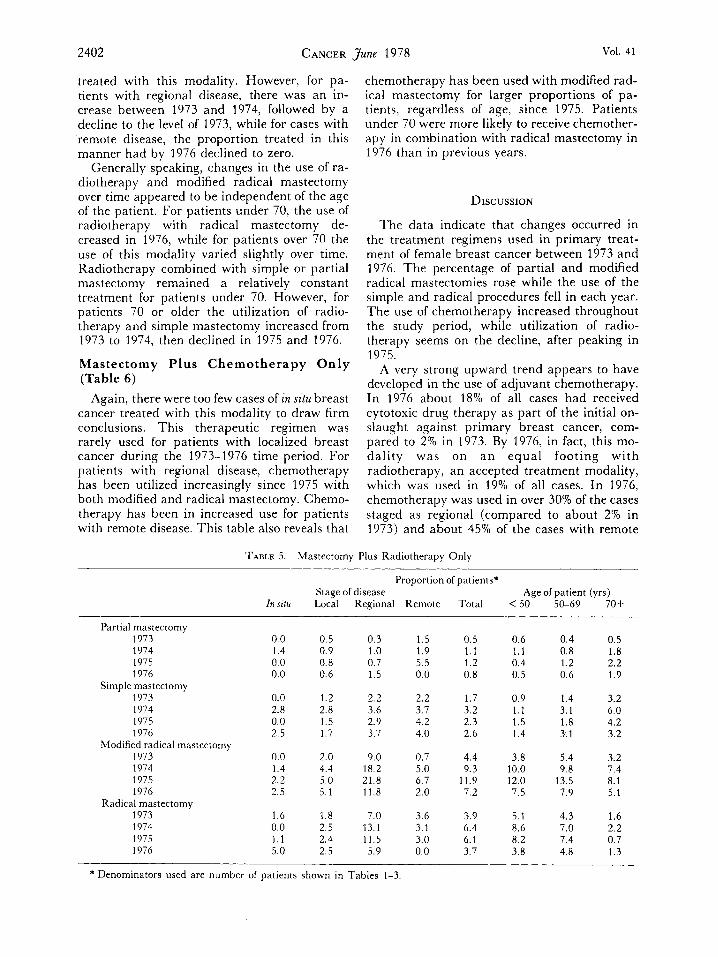
Mastectomy Plus Radiotherapy Only (Table 5 )
There were too few cases of in situ breast can- cer treated with this modality to draw firm con- clusions. In localized disease, a steady increase in the use of radiotherapy with modified radical mastectomy was found. For cases with regional and remote disease, there was a steady increase in use of this modality until 1975, followed by a decline in 1976. There was also an increase in the use of radiotherapy and partial mast- ectomies for remote disease.
Changes in the use of radiotherapy combined with radical mastectomy differed according to stage of disease. There was essentially no change in the proportion of cases with localized disease
TABLE 4. Mastectomy Only
Proportion of patients*
I n ~ z t u Local Regional Remote Total < 50 50-69 70+ Stage of disease Age of patient (yrs)
Partial mastectomy 1973 21.3 3.9 1.1 1.5 3.5 4.3 1.5 6.6 1974 1975 1976
Simple mastectomy 1973 1974 1975 1976
1973 1974 1975 1976
Modified radical mastectomy
15.3 3.6 1.1 3.1 3.3 3.6 2.2 5.1 12.4 4.9 0.7 6.1 4.1 3.6 3.2 6.6 22.5 4.8 2.2 8.0 5.1 4.2 3.7 8.9
19.7 16.8 8.5 13.1 13.1 8.1 9.3 26.9 22.2 15.6 5.7 6.8 11.3 6.6 7.7 24.8
4.3 9.7 8.9 5.4 5.9 19.9 33.7 9.0 22.5 11.3 2.2 2.0 7.7 4.7 3.1 22.2
32.8 37.9 36.6 14.6 34.6 34.8 36.5 30.3 33.3 40.6 28.7 14.9 32.9 34.4 33.8 29.0 37.1 51.0 22.1 7.9 36.1 40.3 35.1 33.3 45.0 53.1 24.7 6.0 38.2 38.7 40.7 32.3
Radical mastectomy 1973 16.4 32.4 30.7 4.4 28.1 35.3 32.4 10.3 1974 15.3 26.6 22.5 10.6 22.8 28.8 25.4 9.8 1975 11.2 21.9 11.3 0.6 15.7 18.0 17.6 8.8 1976 0.0 16.4 10.7 4.0 12.4 14.6 13.8 6.3
* Denominators used are number of patients shown in Tables 1-3.
2402 CANCER June 1978 Vol. 41
treated with this modality. However, for pa- tients with regional disease, there was an in- crease between 1973 and 1974, followed by a decline to the level of 1973, while for cases with remote disease, the proportion treated in this manner had by 1976 declined to zero.
Generally speaking, changes in the use of ra- diotherapy and modified radical mastectomy over time appeared to be independent of the age of the patient. For patients under 70, the use of radiotherapy with radical mastectomy de- creased in 1976, while for patients over 70 the use of this modality varied slightly over time. Radiotherapy combined with simple or partial mastectomy remained a relatively constant treatment for patients under 70. However, for patients 70 or older the utilization of radio- therapy and simple mastectomy increased from 1973 to 1974, then declined in 1975 and 1976.
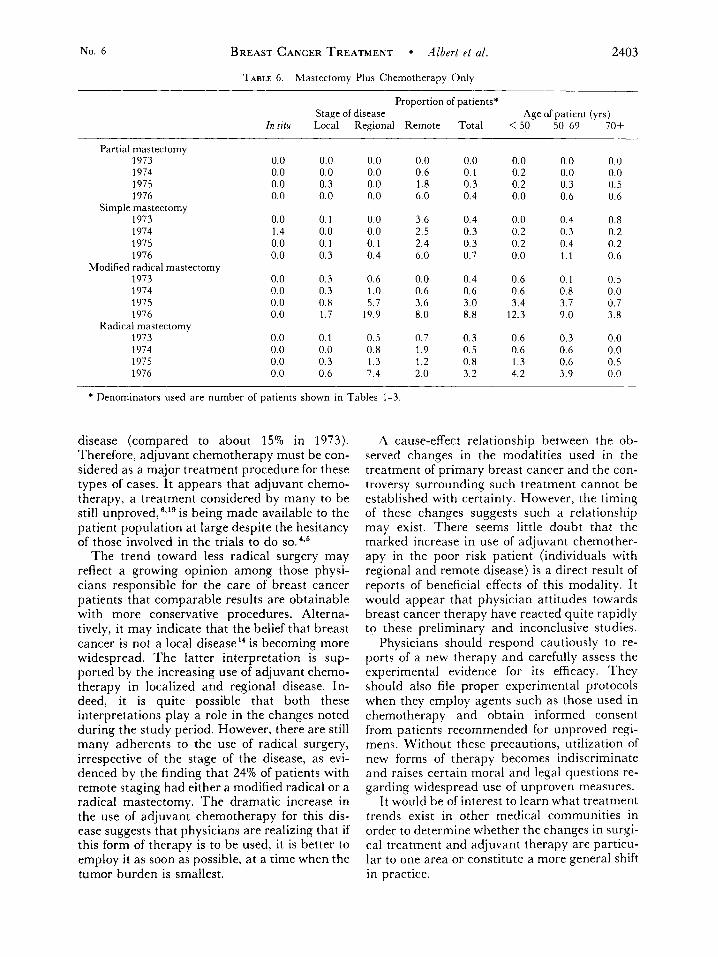
Mastectomy Plus Chemotherapy Only (Table 6)
Again, there were too few cases of in situ breast cancer treated with this modality to draw firm conclusions. This therapeutic regimen was rarely used for patients with localized breast cancer during the 1973-1976 time period. For patients with regional disease, chemotherapy has been utilized increasingly since 1975 with both modified and radical mastectomy. Chemo- therapy has been in increased use for patients with remote disease. This table also reveals that
chemotherapy has been used with modified rad- ical mastectomy for larger proportions of pa- tients, regardless of age, since 1975. Patients under 70 were more likely to receive chemother- apy in combination with radical mastectomy in 1976 than in previous years.
DISCUSSION
The data indicate that changes occurred in the treatment regimens used in primary treat- ment of female breast cancer between 1973 and 1976. The percentage of partial and modified radical mastectomies rose while the use of the simple and radical procedures fell in each year. The use of chemotherapy increased throughout the study period, while utilization of radio- therapy seems on the decline, after peaking in 1975.
A very strong upward trend appears to have developed in the use of adjuvant Chemotherapy. In 1976 about 18% of all cases had received cytotoxic drug therapy as part of the initial on- slaught against primary breast cancer, com- pared to 2% in 1973. By 1976, in fact, this mo- dality was on a n equal footing with radiotherapy, an accepted treatment modality, which was used in 19% of all cases. In 1976, chemotherapy was used in over 30% of the cases staged as regional (compared to about 2% in 1973) and about 45% of the cases with remote
TABLE 5. Mastectomy Plus Radiotherapy Only
Proportion of patients*
Znsitu Local Regional Remote Total < 50 50-69 70+ Stage of disease Age of patient (yrs)
Partial mastectomy 1973 0.0 0.5 0.3 1.5 0.5 0.6 0.4 0.5 1974 1.4 0.9 1.0 1.9 1.1 1.1 0.8 1.8 1975 0.0 0.8 0.7 5.5 1.2 0.4 1.2 2.2 1976 0.0 0.6 1.5 0.0 0.8 0.5 0.6 1.9
1973 0.0 1.2 2.2 2.2 1.7 0.9 1.4 3.2 1974 2.8 2.8 3.6 3.7 3.2 1.1 3.1 6.0 1975 0.0 1.5 2.9 4.2 2.3 1.5 1.8 4.2 1976 2.5 1.7 3.7 4.0 2.6 1.4 3.1 3.2
1973 0.0 2.0 9.0 0.7 4.4 3.8 5.4 3.2 1974 1.4 4.4 18.2 5.0 9.3 10.0 9.8 7.4 1975 2.2 5.0 21.8 6.7 11.9 12.0 13.5 8.1 1976 2.5 5.1 11.8 2.0 7.2 7.5 7.9 5.1
1973 1.6 1.8 7.0 3.6 3.9 5.1 4.3 1.6 1974 0.0 2.5 13.1 3.1 6.4 8.6 7.0 2.2 1975 1.1 2.4 11.5 3.0 6.1 8.2 7.4 0.7 1976 5.0 2.5 5.9 0.0 3.7 3.8 4.8 1.3
Simple mastectomy
Modified radical mastectomy
Radical mastectomy
* Denominators used are number of patients shown in Tables 1-3.
No. 6 BREAST CANCER TREATMENT Albert et al. 2403
TABLE 6. Mastectomy Plus Chemotherapy Only
Proportion of patients*
Znsitu Local Regional Remote Total <SO 50-69 70+ Stage of disease Age af patient (yrs)
~
Partial mastectomy 1973 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 1974 0.0 0.0 0.0 0.6 0.1 0.2 0.0 0.0 1975 0.0 0.3 0.0 1.8 0.3 0.2 0.3 0.5 1976 0.0 0.0 0.0 6.0 0.4 0.0 0.6 0.6
1973 0.0 0.1 0.0 3.6 0.4 0.0 0.4 0.8 1974 1.4 0.0 0.0 2.5 0.3 0.2 0.3 0.2 1975 0.0 0.1 0.1 2.4 0.3 0.2 0.4 0.2 1976 0.0 0.3 0.4 6.0 0.7 0.0 1.1 0.6
1973 0.0 0.3 0.6 0.0 0.4 0.6 0.1 0.5 1974 0.0 0.3 1.0 0.6 0.6 0.6 0.8 0.0 1975 0.0 0.8 5.7 3.6 3.0 3.4 3.7 0.7 1976 0.0 1.7 19.9 8.0 8.8 12.3 9.0 3.8
1973 0.0 0.1 0.5 0.7 0.3 0.6 0.3 0.0 1974 0.0 0.0 0.8 1.9 0.5 0.6 0.6 0.0 1975 0.0 0.3 1.3 1.2 0.8 1.3 0.6 0.5 1976 0.0 0.6 7.4 2.0 3.2 4.2 3.9 0.0
Simple mastectomy
Modified radical mastectomy
Radical mastectomy
* Denominators used are number of patients shown in Tables 1-3.
disease (compared to about 15% in 1973). Therefore, adjuvant chemotherapy must be con- sidered as a major treatment procedure for these types of cases. It appears that adjuvant chemo- therapy, a treatment considered by many to be still unproved, '3 is being made available to the patient population at large despite the hesitancy of those involved in the trials to do ~ 0 . ~ 2 ~
The trend toward less radical surgery may reflect a growing opinion among those physi- cians responsible for the care of breast cancer patients that comparable results are obtainable with more conservative procedures. Alterna- tively, it may indicate that the belief that breast cancer is not a local disease" is becoming more widespread. The latter interpretation is sup- ported by the increasing use of adjuvant chemo- therapy in localized and regional disease. In- deed, it is quite possible that both these interpretations play a role in the changes noted during the study period. However, there are still many adherents to the use of radical surgery, irrespective of the stage of the disease, as evi- denced by the finding that 24% of patients with remote staging had either a modified radical or a radical mastectomy. The dramatic increase in the use of adjuvant chemotherapy for this dis- ease suggests that physicians are realizing that if this form of therapy is to be used, it is better to employ it as soon as possible, at a time when the tumor burden is smallest.
A cause-effect relationship between the ob- served changes in the modalities used in the treatment of primary breast cancer and the con- troversy surrounding such treatment cannot be established with certainty. However, the timing of these changes suggests such a relationship may exist. There seems little doubt that the marked increase in use of adjuvant chemother- apy in the poor risk patient (individuals with regional and remote disease) is a direct result of reports of beneficial effects of this modality. It would appear that physician attitudes towards breast cancer therapy have reacted quite rapidly to these preliminary and inconclusive studies.
Physicians should respond cautiously to re- ports of a new therapy and carefully assess the experimental evidence for its efficacy. They should also file proper experimental protocols when they employ agents such as those used in chemotherapy and obtain informed consent from patients recommended for unproved regi- mens. Without these precautions, utilization of new forms of therapy becomes indiscriminate and raises certain moral and legal questions re- garding widespread use of unproven measures.
It would be of interest to learn what treatment trends exist in other medical communities in order to determine whether the changes in surgi- cal treatment and adjuvant therapy are particu- lar to one area or constitute a more general shift in practice.

2404 CANCER June 1978
REFERENCES
Vol. 41
1. Anglem, T. J . : Management of breast cancer: Radical mastectomy. 3 A M A 30:99-109, 1974.
2. Ansfield, F. ,J.: Adjuvant radiotherapy for breast can- cer. J A M A 235:67-68, 1976.
3. Bonadonna, G., Brusamolino, E., Valagussa, P., and Veronesi, U. : Adjuvant study with combination chemother- apy in operable breast cancer. PYOC. Am. A ~ s o c . Cancer Res.1 Am. Soc. Clin. Oncol. 16:254, 1975.
4. Bonadonna, A., Brusamolino, E., Valagussa, P., Kossi, A,, Brugnatelli, L.; Brambilla, C., DeLena, M., Tancini, A., Bajetta, E., Musumeci, R., and Veronesi, U.: Combination chemotherapy as an adjuvant treatment in operable breast cancer. "4'. Engl. 3. Med. 294:405-410, 1976.
5. Cancer Letter: New Breast Therapies Move into Gen- eral Practice. Feb. 13, 1976.
6. Costanza, H . E.: The problem of breast-cancer pro- phylaxsis. N. Engl. 3. Med. 293:1095-1097, 1975.
7. Cope, D., Wang, C. A., Chu, A,, Wang, C. C., Shulz, M., Castleman, B., Long, J., and Sohier, W. 0.: Limited surgical excision as the hasis of a comprehensive therapy for cancer of the breast. .4m. 3. Surg. 131 :400-407, 1976.
8. Crile, G., Jr.: Management of breast cancer: Limited mastectomy. 3 A h l A 230:95-98, 1974.
9. Cutler, S. J. : Trends in the management of cancer. C 4 18:189-205, 1968.
10. Fisher, B., Carbone, P., Economou, S. G., Frelick, K., Glass, A., Lerner, H., Redmond, C., Zelen, M., Band, P., Katrych, 11. L., Wolmark, N., and Fisher, E, R.: L-Pheny- lalanine Mustard (L-PAM) in the management of primary
breast cancer: A report of early finding. N. Engl. 3. Med. 292:117-122, 1975.
11. Fisher, B., Slack, N. H., Cavanaugh, P. ,J., Gardner, B., and Ravidin, R. G. : Postoperative radiotherapy in the treatment of breast cancer: Results of the NSAB clinical trial. Ann . Surg. 172:711-732, 1970.
12. Fletcher, G. H., Tapley, N. U., Montague, E. D., and Brown, G. R . : Management of localized breast cancer. I n Textbook of Radiotherapy, ed. 2, Philadelphia, Lea & Fehi- ger, 1973; pp. 457-496.
13. Haagensen, C. D.: Editorial: A great leap backward in the treatment of rarcinoma of the breast. J A M A 224: 1 1 81-1 183, 1973.
14. Holland, J. F. : Major advance in breast cancer ther- apy. .,"I. En$ 3. .$led. 294:440-441, 1976.
15. Holleb, A. I . : American Cancer Society Policy State- mrnt on Surgical Treatment of Breast Cancer. (2 23:341- 343, 1973.
16. Leis. H. D., J r . : The surgeon's dilemma in breast cancer. Breast 1:30-34, 1975.
17. Peters, V. hl.: The role of local excision and radiation in early breast cancer. I n Breast Cancer, Early and Late. Chicago, Year Book Medical Publications, 1970; pp. 171- 189.
18. Stjernswlald, J. : Decreased survival related to irradia- tion postoperatively in early operable breast cancer. Lancet 2: 1285-1286, 1974.
19. Tormey, D. C. : Combined chemotherapy and surgery in breast cancer: A review. Cancer 36:881-892, 1975.