recent advances in research and therapy 2 25... · recent advances in research and therapy ......
TRANSCRIPT

"Pain and Suffering”
Recent Advances in Research and Therapy
the K.U.Leuven Center of Excellence ‘Generalization Research
in Ill health and Psychopathology’ (GRIPP*TT)

Pain and suffering: recent
advances in research and therapy
Geert Crombez

Imagine Georges, 47 yrs old, happily married
and three children… He suffers from chronic
severe back pain.….He is on longterm
sickleave… Medical specialists found
nothing “seriously wrong” in his back. He is
however not convinced... He is afraid that his
back problem will worsen, and avoids back
straining activities. He tried several
treatments, but none completely succesful….
What now? As times passes, he starts to
worry about his future. He had a great job, he
was social and sportive, and loved to travel
with wife and children. All have become
impossible because of his pain. He feels
stuck, and uncertain about the future….
However, he won’t give up…
A clinical case

Overview
1. Setting the stage
• Some epidemiological data
• A short history of key constructs
2. Pain and suffering: a multilayered analysis
Pain
Pain-related
fear
Suffering
• Pain: signal of bodily threat
• Pain-related fear: learning
about pain
• Suffering: a threat to identity

Top 10 of most prevalent chronic health problems
Males
(all age groups)
Females
(all age groups)
Back problems 15% Back problems 19%
Allergy 12% Arthrosis 17%
High blood pressure 11% Allergy 14%
Arthrosis 9% High blood pressure 14%
Neck problems 7% Neck problems 12%
Permanently injured by
accident
6% Severe headache 12%
Severe headache 4% Rheumatoid arthritis 8%
Rheumatoid arthritis 4% Depression 6%
Astma 4% Osteoporosis 6%
Chronic pulmonary problems 4% Thyroid gland problems 6%
(Health Interview Survey in Belgium, 2008)

(Health Interview Survey in Belgium, 1997, 2008)

7 days 4 weeks 7 weeks 12 weeks
80%
26%
17%13% 8%
6 months
Based on Spitzer et al. (1987)
Costs
Natural history of non-specific back
problems

Pain DisabilityTissue
Damage
A specificity model of pain

Natural history of back pain
pain after one year in patients with recent onset pain
(Von Korff et al., 1992, 1993)
%

Tissue
Damage Pain
Disability
(Gordon Waddell, 1993)

-
The Gate Control Theory
(Melzack & Wall,1965)

Thermal grill illusion
• Grill with only warm bars (40°C)
• Grill with only cold bars (20°C)
• Grill interlaced with warm and
cold bars
(Thunberg, 1896; Craig & Bushnell, 1994)
Warmth
Coolness
Burning pain

IASP, Subcommittee on pain terms, 1986
Definition of pain
An unpleasant sensory and emotional experience
associated with actual or potential tissue damage,
or described in terms of such damage

Tissue
Damage Pain
Disability

Operant view on pain behavior
• “Pain behavior” instead of “pain” should be the focus of management of chronic pain
• Assumption– Biomedical findings do not eliminate the possibility that psychological
or social factors contribute to the level of pain disability.
– The factors that maintain the pain problem can be different from those that initiated it.
• Application of operant learning principles to problemsof chronic pain– Positive and negative reinforcement of pain behavior
– Avoidance behavior
– Graded activity: reinforcment of well behaviour
(Fordyce ,1976)

“Pain is to disability
as spaghetti to a
brick”
(Fordyce, 1998)

Biopsychosocial perspective
Pain DisabilityTissue
Damage
Disuse
Catastrophizing
Jobsatisfaction
Coping
Socioeconomic status
Central sensitisation
Social Support
Doctor
Shopping
Genetics
Stress
AvoidanceDepression

Pain and suffering: a multilayered
analysis
1. Pain: signal of bodily threat
2. Pain-related fear: learning
about pain
3. Suffering: a threat to identity
Pain
Pain-related
fear
Suffering

• Pain interrupts behaviour,
captures attention & urges escape
• Affective-motivational and not
perceptual characteristics
• Attention to pain is result of
• pain-related characteristics
• other environmental demands
(Eccleston & Crombez, 1999; Crombez, 2006;
Van Damme et al., 2010; Legrain et al., 2009, 2011)

Ss are instructed to ignore pain to complete
an attentionally demanding task. Retardation
and error in task performance are used as
measures of attentional interference by pain.
Primary task paradigm
(Crombez et al., 1994; Eccleston et al., 1994)

(Eccleston, 1995)
Intense chronic pain demands
attention

Thre
High pitch tone
Low pitch tone
(Crombez et al., 1998)

ms
Catastrophizing about pain: students

Summary of findings
(Van Damme et al., 2010; Legrain et. al., 2011; Moriarty et al., 2011)
• Factors amplifying interruption by pain• Pain intensity
• Abrupt onset
• Unpredictability
• Threat value of pain
• Pain catastrophizing
• Pain related fear
• Brain structures involved• Largely multimodal system
Insula, ACC, MCC, (amgydala)
• Saliency (threat) detection system
• Urges action (Moureaux et al., in press)

Clinical implications: a cognitive analysis
• Cognitive control over pain
• Directing attention away from pain is part of many cognitive-
behavioural programs
(Turk & Meichenbaum, 1989; Morley et al., 2004)
• Distraction works,… but when and how…
• Challenges
• Which characteristics of distraction task?
• Attentional set (Van Ryckeghem et al., in preparation)
• Goal value (Verhoeven et al., 2010)
• Works less when pain is intense, novel and threatening,…
(Heyneman et al., 2000; Hadjistravopoulos et al., 2000; Verhoeven
et al., 2010)
• Does not change threat value of pain

Pain and suffering: a multilayered
analysis
1. Pain: signal of bodily threat
2. Pain-related fear: learning
about pain
3. Suffering: a threat to identity
Pain
Pain-related
fear
Suffering

(Gordon Waddell, 1993)
“Fear of pain is more
disabling than pain
itself”

KINESIOPHOBIA
An excessive, irrational and
debilitating fear of physical
movement and activity
resulting from a feeling of
vulnerability to painful injury or
reinjury
(Kori et al., 1990)

Pain Confrontation
Recovery
Disuse
Disability
Depresssion
No fear
Fear of movement,
pain, (re)injury
Catastrophizing
Hypervigilance
Avoidance
Fear-avoidance & kinesiophobia
Injury
(Vlaeyen et al., 1995;Leeuw et al., 2007)
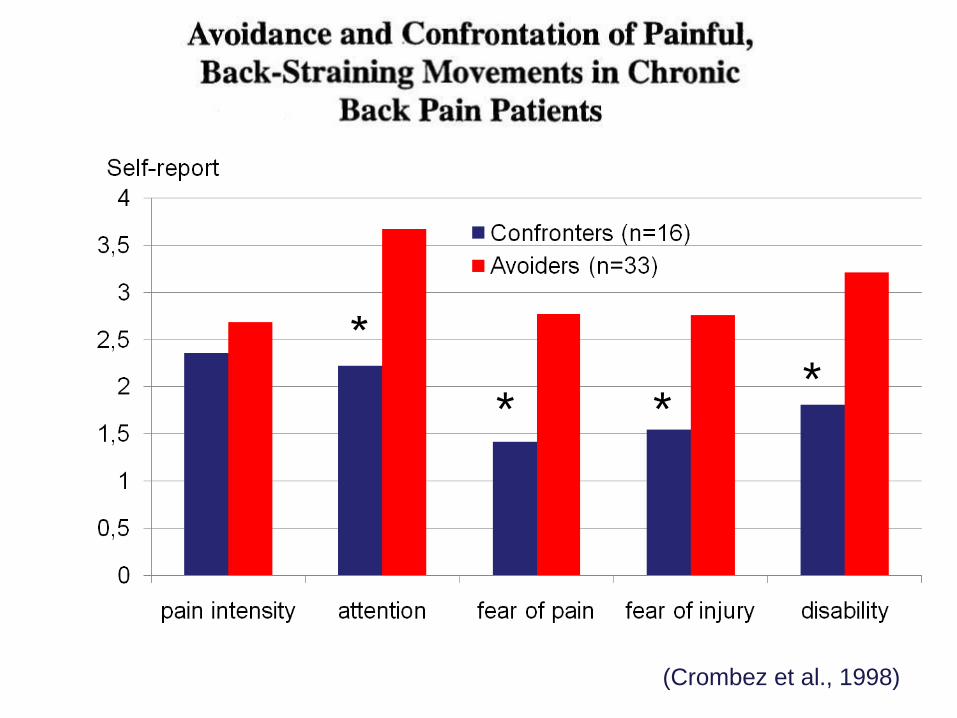
(Crombez et al., 1998)
* **

Hypervigilance for (signals of) pain
(Crombez et al., 2005)

Avoidance behaviour
(Crombez et al., 1996, 1998, 1999)
(Pfingsten et al. 2001; Trost, 2008, in press )

Movement 1 Movement 2Counterbalanced
AABB or BBAA
(Crombez et al., 2002; Goubert et al., 2002; Trost et al., 2008)

Clinical implications: a learning
psychology perspective
• Exposure is clinical analogue of extinction
– Reluctance to generalise corrective experiences
– Overgeneralisation of negative experiences
• Graded exposure (Vlaeyen et al., 2004)
– Idenfication of fearful situations/movements
– Fear hierarchy
– Gradual exposure to movments
• Disconfirming that back pain=injury
• Exposure works
– Reduces the threat value of pain and disability

Challenges
• Psychopathology vs culturally endorsed beliefs
• “Rational” phobia
• Misconceptions about pain also in painfree
• Misconceptions about pain also in health care providers
• “Recovery” does not mean “pain-free”
• Physical movements may remain painful
• Chronic pain may become a threat to identity
• Pain interferes with valued goals
• Pain causes “biographic rupture”
• Pain causes uncertainty about the future


Pain and suffering: a multilayered
analysis
1. Pain: signal of bodily threat
2. Pain-related fear: learning
about pain
3. Suffering: a threat to identity
Pain
Pain-related
fear
Suffering

Suffering: when chronic pain becomes a
threat to identity
action
change
present
state
present
state
present
state
present
state
anticip.
state anticip.
state anticip.
state
anticip.
state
be a good
father
ideal
selfPlay with son
Pick up
ball
system
conceptprinciple program sequence
"be" goals "do" goals motor control goalsgeneral guidelines
(Carver & Scheier, 1998)

Fear-avoidance model is tip of the
iceberg
Fear-avoidance model better
conceptualized as part of
misdirected coping with
disability & suffering

• Classification of coping strategies• Problem focused vs emotion focused (Lazarus & Folkman, 1984)
• Active vs passive coping (Brown & Nicassio, 1987)
• Assumption• Active & problem focused coping = adaptive
• Passive & emotion focused = maladaptive
• Problems• Descriptive but no functional approach of coping (e.g. medication
use)
• Content overlap between coping items and outcome
• Active & problem focused coping, may become part of the
problem
Coping with adversity
(Brandstadter & Renner, 1991;Skinner et al., 2005)

• Ageing literature
• Quality of life increases despite increase in impairments
• Assimilative coping mode
• Goal pursuit
• Solving the obstacle/problem in order to continue
• Accommodative coping mode
• Goal adjustment
• Adjusting personal preferences/goals to
constraints/limitations
Dual process model of coping
(Brandstadter & Renner, 1991; Brandstädter & Rothermund, 2002)

Misdirected problem solving
• No deficit in general problem solving skills
• Problem definition is wrong, or at least too narrow
• Problem: injury=pain, pain=disability
• Search for solution dominated by a tenacious
search for cure/pain relief• Avoidance behavior & bed rest
• Doctor shopping
• Pain medication (e.g. Medication Overuse Headache)
• Invasive techniques with risk of iatrogenic effects
(e.g. Failed Back Surgery Syndrome)
(Aldrich et al., 2000;Vlieger et al., 2006a; 2006b; Lauwerier et al., in press)

Interference by pain
Problem solving
behaviour
Hypervigilance
Worry
Biomedical
Problem
Frame
Problem Solved
Acute pain
Findings in acute pain
• Try to get rid of pain
• Can not accept that pain is insoluble
• Belief that there is a solution
• Meaningful life despite pain
Problem
unsolved
(Eccleston & Crombez, 2007; Brandstadter & Renner, 1990)

(Jamison, 2011)

Interference by pain
Problem solving
behaviour
Hypervigilance
Worry
Biomedical
Problem
Frame
Chronic painMisdirected
problem-solving
Findings in chronic pain
• Try to get rid of pain =
• Can not accept that pain is insoluble =
• Belief that there is a solution ↓
• Meaningful life despite pain ↓
• Distress ↑
• Worrying ↑
• Hypervigilance ↑
Problem
unsolved Perseverance
loop

Pain catastrophizers persevere in
misdirected problem solving…• Solving pain, r=.37***
• Meaningfulness of life despite pain, r=-.46***
• Acceptance of insolubility of pain, r=-.32***
• Belief in a solution, r=-.11*
• Solving pain is necessary to continue with life goals, r=.40**
at the expense of other valued life goals• There are more important things in life than pain, r=-.44***
• I will only be satisfied when I have no pain, r=.45***

• Reassurance
• Communicating bad/good news
• Cognitive behavioural therapy (Turner et al., 2007)
• Δ pain = disability ↓
• Δ pain = injury ↓
• Δ Catastrophizing ↓
• Goal adjustment and acceptance
• Disengage from struggle against pain
• Adapt goals/aspirations to constraints and limitations
• Reengage in valued goals
• Acceptance and committment therapy (McCracken, 2004)
Clinical implications: A self regulation
perspective


Concluding remarks
• Chronic pain is a prototype of chronic illness
• Disability and suffering <> Disease, Illness
• Model of (dis)ability and suffering
• Health psychology model
• “Individuals in abnormal situations” instead of “abnormal
individuals”
• “Medically explained” and “medically unexplained” complaints
• Challenges
• When does search for cure/control becomes too costly
• How to avoid “medicalisation”, but also “psychologisation”
• How to live with chronic illness in a world of healthy

Thank you for your attention
Liesbet Goubert
Stefaan Van Damme
Tine Vervoort
Valéry Legrain
Lies Notebaert
Marieke Dewitte
Chris Eccleston
Ken Craig
Paul Karoly
Stephen Morley
Charles Spence
Johan Vlaeyen
Katrien VerhoevenEmelien Lauwerier
Annabelle CasierDimitri van Ryckeghem
Line CaesKim Helsen
Lies De RuddereSofie Vandenbroucke
Ilse Viane
Acknowledgements