recent advances in arthroscopic repair of traumatic...
TRANSCRIPT

CLINICAL ORTHOPAEDICS AND RELATED RESEARCHNumber 400, pp. 117–122© 2002 Lippincott Williams & Wilkins, Inc.
117
Traumatic anterior instability is the most com-mon type of glenohumeral instability. Althoughsurgical treatment with an open technique hasproduced excellent results, there has been a trendtoward arthroscopic treatment. As understand-ing of instability advances along with improve-ments in surgical techniques and instrumenta-tion, arthroscopic results are fast approachingthose seen with open procedures. Studies done atthe authors’ institution showed a 97% satisfac-tory outcome at short-term followup with 93%stable shoulders in a patient population with highphysical demands. Others recently reported sim-ilar results. As more surgeons become familiarwith the techniques, it is thought that arthro-scopic Bankart reconstructions will be the pre-ferred method in the future.
Traumatic anterior instability is the most com-mon type of glenohumeral instability. Severalstudies have shown the importance of the an-teroinferior capsulolabral structures in main-taining joint stability.2,13,16,20 The anteroinfe-rior labrum serves as the anchor point for the
inferior glenohumeral ligament, the primarystatic restraint to anterior humeral translationin the abducted shoulder.21 An avulsion of thecapsulolabral structures from the glenoid rimand scapular neck was described by Perthes17
and Bankart3 as the essential lesion leading torecurrent instability. More recently, biome-chanical studies and arthroscopic observationshave clarified the incidence of specific pat-terns of capsulolabral injuries that accompanyshoulder instability, with the most commondisorder being the Bankart lesion, occurringapproximately 80% of the time.2,11 The stan-dard form of treatment for the patient withmultiple anterior dislocations has become therepair of the Bankart lesion.
Open techniques for repair of the avulsedanteroinferior capsulolabral structures gener-ally have had recurrence rates reported of fewerthan 10%.18 Although Rowe and coworkers18
reported a 96.5% success rate, only 2⁄3 of thepatients were reexamined, and only 1⁄3 of thoseinvolved in sports returned to a competitivelevel of participation. The open technique alsohas morbidity including scarring from the dis-section required for adequate exposure. Thisoccasionally leads to a limitation of postoper-ative functional ability and is problematic inathletes and laborers because of loss of mo-tion, specifically external rotation. Biglianiand coworkers4 reported that only 67% of ath-
Recent Advances in Arthroscopic Repair of Traumatic Anterior
Glenohumeral Instability
Kenneth S. Weiss, MD; and Felix H. Savoie, III, MD
From the Mississippi Sports Medicine & OrthopaedicCenter, University of Mississippi School of Medicine,Jackson, MS.Reprint requests to Felix H. Savoie, III, MD, Upper Ex-tremity Service, 1325 East Fortification Street, Jackson,MS 39202.

letes who throw return to their normal activitylevel after an open capsular shift despite theirextensive experience.
Although arthroscopic techniques have im-proved, their results must be compared with re-sults of repair with an open technique. Earlyarthroscopic techniques used metal staples andscrews with success rates ranging from 66%to 85%.10 However, significant complicationswere encountered, including loose hardware,articular injury, persistent pain attributable tohardware, and problems with recurrent insta-bility. Later, a transglenoid suturing techniquefor repair of the Bankart lesion was devel-oped.9 In 1987, Morgan and Bodenstab12 re-ported their preliminary results using transgle-noid suture technique for repair in 25 shoulders;a 100% success rate was reported. However, ina long-term study and followup, loosening ofthe repair and redislocation were reported.8The current authors think the anteroinferiorcapsulolabrum was repaired medial to the gle-noid rim and accounted for these poor long-term results. Caspari and Savoie5 later reportedthe importance of repairing the anteroinferiorcapsulolabrum to the glenoid rim.
Snyder and Stafford19 described the use ofanchors and sutures in arthroscopic repair ofthe anteroinferior capsulolabrum to the gle-noid, eliminating transglenoid suturing. Su-ture anchors subsequently were used byWolf,22 Snyder and Stafford,19 and Bacilla andcoworkers1 with excellent preliminary results.More recently, Cole and coworkers6 reportedsimilar results after repair between the openand arthroscopic techniques. However, intheir study the more difficult cases were re-paired with the open technique.
IndicationsAt the authors’ institution, current criteria forarthroscopic treatment of traumatic anterior in-stability includes patients of all ages and all ac-tivity levels with recurrent anterior instabilitywho are impaired functionally and who havenot responded to nonoperative treatment. Cur-rently, patients with first-time, acute shoulderdislocations do not have stabilization.
The Authors Preferred TechniqueThe patient is placed in the lateral decubitusposition for the arthroscopic technique. Theupper extremity is suspended with 5 to 10 lbtraction. A standard posterior portal is estab-lished and a diagnostic arthroscopy is done.When there has been recurrent, traumatic an-terior dislocation, the pathoanatomy usuallyincludes capsulolabral avulsion, the Bankartlesion, and a widened rotator interval (Fig 1).An anterior portal then is established using anoutside-in technique to ensure proper orienta-tion and access to the anteroinferior glenoidfor reconstruction.
The Bankart lesion and anteroinferior cap-sulolabrum are evaluated from the anterior por-tal for associated midcapsular or humeral inser-tion site tears. The arthroscope then is returnedto the posterior portal, and the anterior portal isused for debriding and releasing the anteroinfe-rior capsulolabral complex from the glenoid.The release is extended medially along the gle-noid neck until the subscapularis muscle can beobserved. The release also is done inferiorly tothe 6 o’clock position (straight inferior) of theglenoid. The anteroinferior glenoid then isabraded to a bleeding surface.
Clinical Orthopaedics118 Weiss and Savoie and Related Research
Fig 1. An arthroscopic view of Bankart lesion isshown.
Number 400July, 2002 Arthroscopic Repair Anterior Instability 119
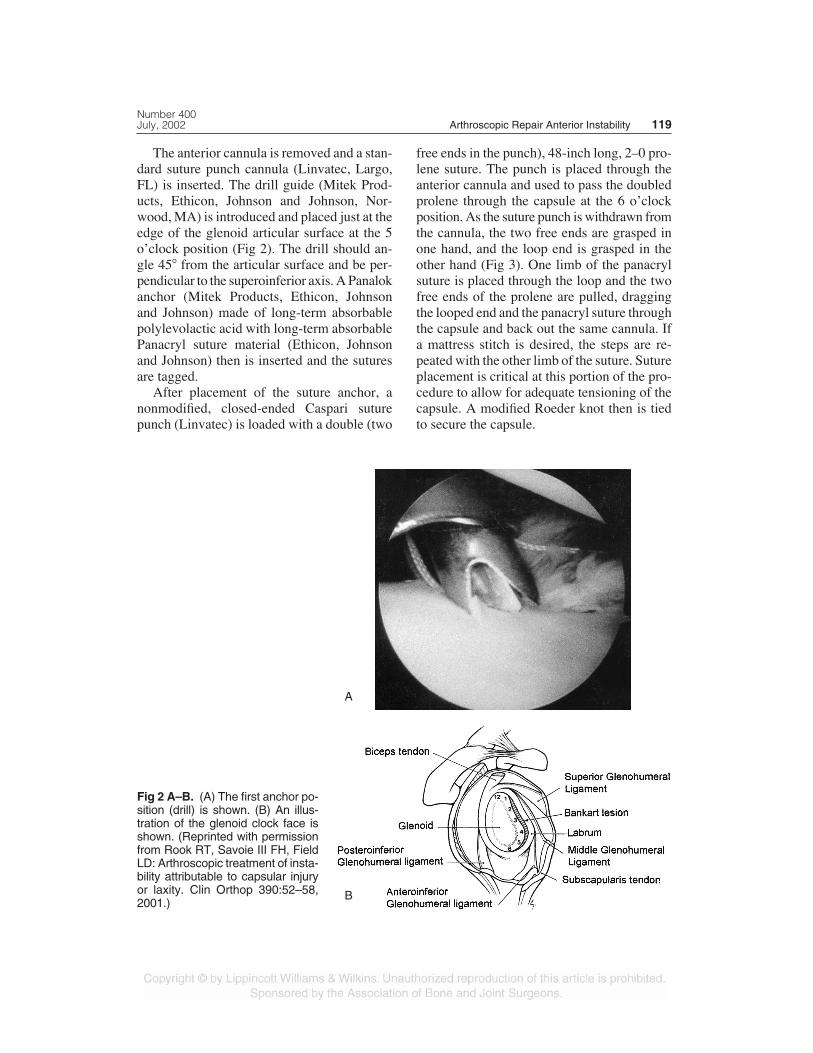
The anterior cannula is removed and a stan-dard suture punch cannula (Linvatec, Largo,FL) is inserted. The drill guide (Mitek Prod-ucts, Ethicon, Johnson and Johnson, Nor-wood, MA) is introduced and placed just at theedge of the glenoid articular surface at the 5o’clock position (Fig 2). The drill should an-gle 45� from the articular surface and be per-pendicular to the superoinferior axis. A Panalokanchor (Mitek Products, Ethicon, Johnsonand Johnson) made of long-term absorbablepolylevolactic acid with long-term absorbablePanacryl suture material (Ethicon, Johnsonand Johnson) then is inserted and the suturesare tagged.
After placement of the suture anchor, anonmodified, closed-ended Caspari suturepunch (Linvatec) is loaded with a double (two
free ends in the punch), 48-inch long, 2–0 pro-lene suture. The punch is placed through theanterior cannula and used to pass the doubledprolene through the capsule at the 6 o’clockposition. As the suture punch is withdrawn fromthe cannula, the two free ends are grasped inone hand, and the loop end is grasped in theother hand (Fig 3). One limb of the panacrylsuture is placed through the loop and the twofree ends of the prolene are pulled, draggingthe looped end and the panacryl suture throughthe capsule and back out the same cannula. Ifa mattress stitch is desired, the steps are re-peated with the other limb of the suture. Sutureplacement is critical at this portion of the pro-cedure to allow for adequate tensioning of thecapsule. A modified Roeder knot then is tiedto secure the capsule.
Fig 2 A–B. (A) The first anchor po-sition (drill) is shown. (B) An illus-tration of the glenoid clock face isshown. (Reprinted with permissionfrom Rook RT, Savoie III FH, FieldLD: Arthroscopic treatment of insta-bility attributable to capsular injuryor laxity. Clin Orthop 390:52–58,2001.)
A
B

Additional anchors are placed in a similarmanner at the 3 o’clock and 1 o’clock posi-tions. A retrograde suture retriever may benecessary above 3 o’clock to retrieve the su-tures through the tissue. The complete repair isassessed from the posterior and anterior por-tals (Figs 4, 5). The posterior capsule also isassessed and tightened if necessary. The rota-tor interval then is plicated, taking care not toincorporate the biceps tendon. This is accom-plished by passing a spinal needle through theanterior edge of the supraspinatus tendon, in-corporating the anterior capsule and occasion-ally the middle glenohumeral ligament. Thesuture limbs then are retrieved through the an-terior cannula and tied blindly using a modi-fied Roeder knot. This completes the repairwith the current arthroscopic technique.
For the first postoperative week, the shoul-der is maintained in a shoulder sling with asmall abduction pillow. The patient begins ahome exercise program of shoulder shrugs,passive forward flexion of the shoulder, andpassive external rotation taking care not toelicit pain. These exercises are continued for 2weeks. At 3 weeks, active internal and exter-nal rotation begin with the arm at the side withslight resistance and continue for 3 additionalweeks. At 6 weeks, physical therapy is started,
emphasizing active range of motion with rota-tor cuff strengthening, without stretching. Plyo-metric exercises may begin at 2 months fol-lowed by return to low velocity throwing at 3months. Return to contact sports and aggres-
Clinical Orthopaedics120 Weiss and Savoie and Related Research
Fig 3 A–B. (A) The Caspari suture punch is shown through the labrum. (B) A representation of theCaspari suture punch through labrum and the free and loop ends coming out of the cannula are shown.
A B
Fig 4. Illustration shows the final repair. (Reprintedwith permission from Noojin FK, Savoie III FH,Field LD: Arthroscopic Bankart repair using long-term absorbable anchors and sutures. TechShoulder Elbow Surg 1:262–267, 2000.)
sive sports specific drilling is determined onan individual basis and usually is delayed un-til 4 months postoperatively.
RESULTS
The results of repair of traumatic anterior insta-bility using an arthroscopic technique with an-chors and sutures in 35 consecutive patientswere studied.15 All patients had sustained atleast two dislocations, were impaired function-ally with activities, and had not responded to anaggressive physical therapy program in an at-tempt to relieve their symptoms. The mean ageof the patients was 27 years, each had a Bankartlesion, and each had an arthroscopic repair us-ing a minimum of three Panalok anchors. Fol-lowup included physical examination and radio-graphic evaluation at a minimum of 2 years(range, 24–36 months). All patients had re-gained a minimum of 170� frontal flexion andabduction and had an average postoperativeBankart score of 93 (range, 50–100). The aver-age external rotation with the shoulder ab-ducted 90� was 110� (range, 95�–135�). Therewas a 97% success rate and one failed result ina patient with a repeat traumatic dislocation thatoccurred 11 months postoperatively.
In a second arthroscopic study from the au-thors’ institution1 the same criteria were used in40 patients; however, all of these patients wereyounger than 23 years and were involved in highdemand athletics. Each patient had a Bankartlesion. The average followup was 30 months(range, 18–36 months). The shoulders in 37 ofthe 40 patients (93%) remained stable, and thepatients returned to normal activities includingparticipation in athletics by 6 months postop-eratively. The average postoperative Bankartscore was 90 (range, 30–100). The shoulders inthree patients redislocated postoperatively.
DISCUSSION
Shoulder stabilization with an arthroscopictechnique was successful in more than 90% ofpatients with traumatic anteroinferior instabil-ity at relatively short-term followup. In addi-tion to repair of the Bankart lesion, the authorsalso did soft tissue tensioning through plica-tion of the rotator interval that may have con-tributed to these favorable results. The resultswere similar to the 96.5% success rate re-ported by Rowe and coworkers.18 Gartsmanand coworkers7 reported 92% good or excel-lent results at 2 to 5 years followup (average,33 months). They also did a soft tissue ten-sioning procedure in addition to repair of theBankart lesion using laser thermal capsulorra-phy of the anteroinferior capsulolabrum in 48of the 53 shoulders. Although these results areencouraging, they may deteriorate with time.Torchia et al19 showed the incidence of recur-rent instability increases for as many as 7 yearspostoperatively. Therefore, although the cur-rent authors are excited with the initial highsuccess rate, it is assumed that the success ratewill decrease with time.
References1. Bacilla P, Field LD, Savoie FH: Arthroscopic
Bankart repair in a high-demand patient population.Arthroscopy 13:51–60, 1997.
2. Baker CL, Uribe JN, Whitman C: Arthroscopic eval-uation of acute initial anterior shoulder dislocations.Am J Sports Med 18:25–28, 1990.
3. Bankart ASB: Recurrent or habitual dislocation ofthe shoulder. BMJ 1:1132–1133, 1923.
4. Bigliani LU, Kurzweil PR, Schwartzbach CC, Wolfe
Number 400July, 2002 Arthroscopic Repair Anterior Instability 121
Fig 5. An arthroscopic view after the entire repairis shown.

IN, Flatow EL: Inferior capsular shift procedure foranterior-inferior shoulder instability in athletes. AmJ Sports Med 22:578–584, 1994.
5. Caspari RB, Savoie FH: Arthroscopic Reconstructionof the Shoulders: The Bankart Repair. In McGinty JB(ed). Operative Arthroscopy. New York, Raven Press507–515, 1991.
6. Cole BJ, L’Insalata J, Irrgang J, Warner JJ: Compar-ison of arthroscopic and open anterior shoulder sta-bilization: A two to six year study. J Bone Joint Surg82A:1108–1114, 2000.
7. Gartsman GM, Roddey TS, Hammerman SM: Arthro-scopic treatment of anterior inferior glenohumeral in-stability: Two to five-year follow-up. J Bone Joint Surg82A:991–1003, 2000.
8. Grana WA, Buckley PD, Yates CK: Arthroscopicbankart suture repair. Am J Sports Med 21:348–353,1993.
9. McIntyre LF, Caspari RB: The rationale and tech-nique for arthroscopic reconstruction of anteriorshoulder instability using multiple sutures. OrthopClin North Am 24:55–58, 1993.
10. Matthews LS, Vetter WL, Oweida SJ, Spearman J,Helfet DL: Arthroscopic staple capsulorraphy for re-current anterior shoulder instability. Arthroscopy4:106–111, 1988.
11. Mohammed KD, Sonnabend DH, Goldberg JA, et al:Biomechanical performance of Bankart repairs in ahuman cadaveric shoulder model. Am J Sports Med26:831–835, 1998.
12. Morgan CD, Bodenstab AB: Arthroscopic bankart su-ture repair: Technique and early results. Arthroscopy3:11–22, 1987.
13. Moseley HF, Overgaard B: The anterior capsular
mechanism in recurrent anterior dislocation of theshoulder: Morphological and clinical studies with spe-cial reference to the glenoid labrum and the gleno-humeral ligaments. J Bone Joint Surg 44B:913–927,1962.
14. Neviaser TJ: The anterior labroligamentous pe-riosteal sleeve avulsion lesion: A cause of anteriorinstability of the shoulder. Arthroscopy 9:17–21,1993.
15. Noojin FK, Savoie FH, Field LD: Arthroscopicbankart repair using long-term absorbable anchorsand sutures. Orthop Today 4:18–19, 2000.
16. O’Brien SJ, Neves MC, Arnoczky SP, et al: Theanatomy and histology of the inferior glenohumeralligament complex of the shoulder. Am J Sports Med18:449–456, 1990.
17. Perthes G: Uber operationen der habituelien schulter-luxation. Dtsch Zeitschrift Chir 56:149–151, 1906.
18. Rowe CR, Patel D, Southmayd WW: The bankartprocedure: A long-term end-result study. J BoneJoint Surg 60A:1–16, 1978.
19. Snyder SJ, Stafford BB: Arthroscopic management ofinstability of the shoulder. Orthopedics 16:993–1002,1993.
20. Torchia ME, Caspari RB, Asselmeier MA, BeachWR, Gayari M: Arthroscopic transglenoid multiplesuture repair: 2 to 8 year results in 150 shoulders.Arthroscopy 13:609–619, 1997.
21. Turkel SJ, Panio MW, Marshall JL, Girgis FG: Sta-bilizing mechanisms preventing anterior disloca-tion of the glenohumeral joint. J Bone Joint Surg63A:1208–1217, 1981.
22. Wolf EM: Arthroscopic capsulolabral repair using su-ture anchors. Orthop Clin North Am 24:59–69, 1993.
Clinical Orthopaedics122 Weiss and Savoie and Related Research