real-world evidence on etanercept biosimilar sb4 in
TRANSCRIPT

REVIEW
Real-World Evidence on Etanercept Biosimilar SB4in Etanercept-Naıve or Switching Patients:A Systematic Review
Hans C. Ebbers . Burkhard Pieper . Amine Issa . Janet Addison .
Ulrich Freudensprung . Mourad F. Rezk
Received: July 2, 2019 / Published online: August 5, 2019� The Author(s) 2019
ABSTRACT
Introduction: In 2016, SB4 (Benepali�) becamethe first etanercept (ETN) biosimilar to obtainmarketing authorisation in Europe. Despiterobust analytical and clinical comparisons,outstanding questions remain on SB4 use inroutine practice.Methods: A systematic search for publicationson real-world evidence of SB4 effectiveness,safety and drug survival was undertaken usingsearch terms (SB4 OR Benepali OR biosimilaretanercept OR innovator etanercept) in theBIOSIS� Toxicology, BIOSIS Previews�, Embase�
and MEDLINE� databases up to 17 January2019.Results: Of 959 articles identified, eight journalarticles, two journal letters and 23 congressabstracts were selected on criteria of original
real-world evidence with a clinical focus. Asexpected with real-world evidence, qualityscoring showed that the evidence had highexternal validity but lower internal validity. Atotal of 13,552 patients were described acrossnine European countries and all approved SB4indications: 2499 were ETN-naıve and 11,053switched from reference ETN to SB4 (switchers).Switch acceptance rates (a combination ofclinicians offering and patients accepting initi-ation on SB4) ranged between 51.6% and99.0%; patient support programmes positivelycontributed to acceptance. Disease activity wasgenerally similar pre- and post-switch (typically3-month timeframe). Retention rates acrossstudies were at least 75% (up to 12 months fol-low-up). No new safety signals were identified.Differences in discontinuation rates versus his-toric controls reported in some studies mayhave been influenced by differences in treat-ment practices, lack of clinician confidence andnocebo effects.Conclusion: Nearly 2500 ETN-naıve patientshave been initiated on SB4 and outcomes aresimilar to those patients receiving referenceETN. Overall this systematic review of real-world evidence provides additional reassurancethat SB4 is as effective and safe as reference ETNin both switched and naıve patients.Funding: Biogen International GmbH.
Enhanced Digital Features To view enhanced digitalfeatures for this article go to https://doi.org/10.6084/m9.figshare.8982353.
Electronic Supplementary Material The onlineversion of this article (https://doi.org/10.1007/s40744-019-00169-4) contains supplementary material, which isavailable to authorized users.
H. C. Ebbers (&) � B. Pieper � A. Issa �U. Freudensprung � M. F. RezkBiogen International GmbH, Baar, Switzerlande-mail: [email protected]
J. AddisonBiogen Idec UK, Maidenhead, UK
Rheumatol Ther (2019) 6:317–338
https://doi.org/10.1007/s40744-019-00169-4

Keywords: Benepali; Biosimilar; ETN; Nocebo;Persistence; Real-world evidence; SB4; Switch;Systematic review
INTRODUCTION
A biosimilar is required by the EuropeanMedicines Agency and the Food and DrugAdministration to demonstrate similarity to thereference (originator) product in terms of qual-ity characteristics and biological activity. Fur-thermore, it must demonstrate bioequivalenceto the reference drug and show comparablesafety and efficacy in comparative clinicalstudies [1, 2]. Real-world evidence to supple-ment that from randomised clinical trials(RCTs) is important to inform and educateprescribers, patients and payers on the actualvalue of a medical intervention in routineclinical practice [3, 4]. Real-world evidence canaddress important questions remaining afterapproval of a biosimilar, including those on itslong-term safety, immunogenicity, outcomes ofswitching from the reference to the biosimilarand the effectiveness and safety of the biosimi-lar in a wider range of clinical indications thantested pre-approval. It can also provide insightsinto nocebo effects, which are the apparentemergence or worsening of symptoms as a resultof negative perceptions and attitudes towardsan intervention, and which have the potentialto adversely affect outcomes [5, 6]. Regulatorsencourage marketing authorisation holders ofbiosimilars to collect and report real-world evi-dence as part of post-approval risk managementplans [7].
Etanercept (ETN) was the first anti-tumournecrosis factor inhibitor to receive marketingauthorisation for the treatment of rheumatoidarthritis (RA), initially from the Food and DrugAdministration [8, 9] and subsequently fromthe European Medicines Agency [10]. ETN (En-brel�, Pfizer Europe) is now also licensed for thetreatment of juvenile idiopathic arthritis, pso-riatic arthritis (PsA), axial spondyloarthritis(AxSpA), ankylosing spondylitis (AS) and plaquepsoriasis (PsO). ETN heralded a new age of bio-logic disease-modifying antirheumatic drugs(bDMARDs); however, the increased efficacy of
treatment came with higher direct drug costscompared with conventional DMARDs(cDMARDs) [11]. This has produced inequalitiesin access to bDMARDs; in Europe, of thosepatients with RA who are eligible for bDMARDsaccording to the clinical recommendations ofthe European League against Rheumatism(EULAR), only 13–86% (dependent on country)can expect to receive these biologics on thebasis of national reimbursement criteria [12].Patent protection for ETN in Europe hasexpired, creating the opportunity for the intro-duction of biosimilars, which may enter themarket at more affordable prices compared tothe reference, potentially reducing healthcarecosts for all approved indications throughincreased market competition, and improvingpatient access.
SB4 is an ETN biosimilar, which was com-pared to ETN in an RCT in patients with mod-erate to severe RA despite methotrexatetreatment [13]. Therapeutic equivalence wasdemonstrated in terms of the American Collegeof Rheumatology 20% response (ACR20) rate atweek 24, with 78.1% of patients in the SB4group demonstrating ACR20 vs. 80.3% ofpatients in the reference ETN group; the 95%confidence interval (CI) for the adjustedbetween-treatment difference was - 9.41% to4.98%, thereby satisfying the predefined equiv-alence margin of - 15% to 15%. The safetyprofiles were similar, but injection site reactionsoccurred in fewer patients treated with SB4compared with reference ETN—3.7% vs. 17.2%(p\ 0.001) up to week 24, potentially due todifferences in the formulation constituents (L-arginine) or the presence of latex in the needleshield of the reference product. SB4 had a lowerincidence of antidrug antibody (ADA) develop-ment than reference ETN with an overall rate of0.7% vs. 13.1% (p\ 0.001) by week 24. TheseADAs were transient and did not affect efficacyand their clinical significance was considered tobe minimal by the European Medicines Agency.In an open-label extension of this trial, in whicha subset of patients either continued to receiveSB4 or were switched from reference ETN toSB4, SB4 continued to be effective and welltolerated with comparable performance to ref-erence ETN up to the end of the study
318 Rheumatol Ther (2019) 6:317–338

(100 weeks) [14, 15]. In January 2016, SB4(Benepali�, Biogen) became the first ETNbiosimilar to gain marketing authorisation inEurope and has the same indications as Enbrel�
[16, 17].The objective of this review is to provide a
systematic review of published real-world evi-dence on the use of SB4, including effectiveness,safety, acceptance rates of the option to switchfrom the reference product to the biosimilar,and retention rates after switching. It includesdata from prospective and retrospective obser-vational studies (non-interventional studies), aswell as analyses from European diseaseregistries.
METHODS
Search Strategy and Selection Criteria
The ProQuest� platform (Ann Arbor, USA) wasused to search for journal articles and confer-ence abstracts in the databases BIOSIS� Toxi-cology, BIOSIS Previews�, Embase� andMEDLINE� covering the period to 17 January2019. The search string was (SB4 OR benepaliOR biosimilar ETN OR innovator ETN) AND(rtype.exact(‘‘Journal Article’’ OR ‘‘ConferenceAbstract’’). Duplicates were automaticallyremoved and screening was undertaken by onereviewer, initially on the basis of titles andsubsequently using abstracts, in order toexclude publications that were reviews ratherthan original data, reported interventionalclinical trials, had no clinical focus (e.g. publi-cations containing only pharmacokinetic,pharmacodynamic or cost modelling data) orlacked identifiable data on SB4. The full publi-cations for the remaining reports were reviewedand additional criteria were applied to obtainthe final list of publications to be appraised inthis review. This was undertaken by onereviewer and validated by a second. The inclu-sion criterion was real-world evidence on theuse of SB4, which was defined as observational/non-interventional retrospective and prospec-tive studies, patient registry data and individualcase reports outside the controlled interven-tional trial setting. Reports of universal non-
medical switches from ETN reference to SB4 as aresult of changes in healthcare policies werepermitted, including studies which incorpo-rated randomised processes to support patientsin making a switch e.g. switch ‘visits’. The fol-lowing were excluded: reviews and meta-anal-yses, interventional clinical trials, open-labelextensions of RCTs, studies based on economicmodelling (as distinct from reports on actualeconomic outcomes) reports from which dataspecific to SB4 could not be extracted frompooled data, encore reports of the same data atdifferent congresses, congress abstracts super-seded by full journal publications and analysesof data from ongoing registries superseded byanalyses at a later data cut-off date, with theexception of those that reported different out-come measures.
Quality Assessment
All eligible publications were scored indepen-dently by two individuals for bias and qualityusing the validated Downs and Black methods[18] modified to remove questions 14 and 15(relating to blinding of subjects and investiga-tors), questions 23 and 24 (relating to ran-domisation) and question 27 (relating to powercalculations), because these were not relevant toobservational studies. Score differences betweenthe two scorers were discussed and resolved.
For each publication, the scores are pre-sented as the grand total from the 22 questions(maximum total score 23), and as the totals foreach aspect of quality assessed i.e. reporting(maximum total score 11 from 10 questions),external validity (maximum total score 3 fromthree questions) and internal validity (maxi-mum total score 9 from eight questions).
Data Extraction
The following data, where available, were sum-marized from each eligible publication: studyobjective or focus, study design, main inclusionand exclusion criteria, indications, patientnumbers (by indication), duration of study,outcomes relating to effectiveness andsafety/tolerability of SB4 and any comparators,
Rheumatol Ther (2019) 6:317–338 319

rates of switches to or from SB4, notable char-acteristics of switchers vs. non-switchers (e.g.disease activity), retention rates of patientsswitching to SB4, reasons for discontinuation ofSB4, outcomes of communication plans tosupport patients switching to SB4, economicoutcomes associated with switching to SB4. Theextraction of data was started on 1 February2019.
Data Synthesis
Summary tables were constructed of outcomes.All congress abstracts were categorised as suchand not as journal publications even if thecongress proceedings had been published in ajournal. Total patient numbers for each indica-tion and by patient SB4 category were calcu-lated across studies. Where different analysesfrom the same registry had overlapping dates,patient numbers were counted from the mostrecent report of the full registry. Patients werecategorised as ETN-naıve patients initiating SB4,patients switching from reference ETN to SB4and patients who initially switched from refer-ence ETN to SB4 and later back-switched fromSB4 to reference ETN. Back-switching patientswere categorised as both switchers and back-switchers. The indications were described asreported. In cases where several indicationswere included in the study but the distributionof patients was not given, these patients werecounted as ‘rheumatology patients notspecified’.
Compliance with Ethics Guidelines
This article is based on previously conductedstudies and does not contain any studies withhuman participants or animals performed byany of the authors.
RESULTS
Overall Evidence Base
Of 951 articles retrieved by the searches therewere six full journal publications [19–24], two
journal letters [8, 25] and 23 congress abstracts[26–48] that were eligible for inclusion in thisreview (Fig. 1). The quality score of the fullpublications ranged from 16 to 19 (median16.5) out of a maximum of 23 using the adaptedDowns and Black methodology (SupplementaryFig. S1) [18]. All had the maximum score forexternal validity; internal validity scores wereproportionately lower, with a median (range)score of 6 (5–7) out of a maximum of 9. Mostcongress abstracts and journal letters had lowerscores than the journal publications, primarilybecause abstract reporting has restrictive wordcount limits (median [range] scores were 13[9–17] total, 3 [1–3] for external validity and 5[3–6] for internal validity) (SupplementaryFig. S2).
Most studies were based upon data from asingle country, including the UK, Germany,Italy, France, Portugal, Sweden, Norway, Den-mark and the Netherlands (Table 1 and Table S1in the supplementary material). The studiesincluded analyses from the following diseaseregistries: BSRBR-RA (British Society forRheumatology Biologics Register—RheumatoidArthritis) [26, 27], the German RABBIT(Rheumatoid Arthritis Observation of BiologicTherapy) cohort [28], the Denmark-wide DAN-BIO registry [21], the Dutch BIO-SPAN study(BIOsimilar switch, Study on Persistence androle of Attribution and Nocebo) [24], the SRQRegistry (Swedish Rheumatology Quality Regis-ter) [8, 19] and the NorArthritis Registry (Nor-wegian National Arthritis Registry) [31].
A total of 13,552 patients were described,including 11,053 patients switching from ref-erence ETN to SB4, of whom 3535 were reportedin full journal publications and 768 back-switchers (also counted as switchers) from SB4to reference ETN, of whom 140 were reported infull journal publications (Fig. 2). Switches formost studies were non-medical i.e. economi-cally driven as part of a clinic-wide policy totransfer patients to a lower priced ETN biosim-ilar. Of the 11,053 patients who initiated SB4without having previously received ETN, 3535were reported in full journal publications. Mostpatients were described as having RA, PsA orAxSpA, but other indications were also repre-sented, including 279 patients with PsO, 12
320 Rheumatol Ther (2019) 6:317–338

patients with juvenile idiopathic arthritis and 4patients with enteropathic arthritis. Most con-gress abstracts did not give separate results fordifferent indications, and consequently manypatients have been summarized here as‘rheumatology patients not otherwisespecified’.
Outcomes covered included the effectivenessof SB4, with a comparison of pre-switch andpost-switch disease activity, retention rates(drug survival) for SB4, reasons for discontinu-ations or back-switches to reference ETN,patients’ acceptability of switching and charac-teristics of those patients switching (Tables 1and S1). Several studies presented data on actualcost savings of switching and Shah et al. focusedexclusively on the economics of switching [32].There was generally little detail provided onsafety outcomes; in most of the congressabstracts these were incomplete owing to thereporting of adverse events (AEs) only in thosepatients discontinuing SB4.
Switching Acceptanceand the Characterization of SwitchingPatients and Clinicians and the Process
Switches from reference ETN to SB4 that weremandatory did not necessarily have higheracceptance rates than non-mandatory switchese.g. in the BIO-SPAN study, 99% of patientsoffered a switch agreed to this [24] comparedwith 79% of patients recorded as switching inthe Danish, country-wide DANBIO registry fol-lowing the adoption of a national guidelinemandating the switch [21]. In the latter study, areason for at least some patients not switchingwas because their dose strength of 25 mg ETNwas not yet commercially available for SB4.That study also reported a higher switch rate forpatients with PsA (86%) than patients with RA(77%) or AxSpA (77%) (Table 1) [21]. Charac-teristics more common in switchers were con-comitant methotrexate (MTX) use (RA and PsA),longer duration of reference ETN treatment and
Fig. 1 Flow chart of systematic publication selection
Rheumatol Ther (2019) 6:317–338 321
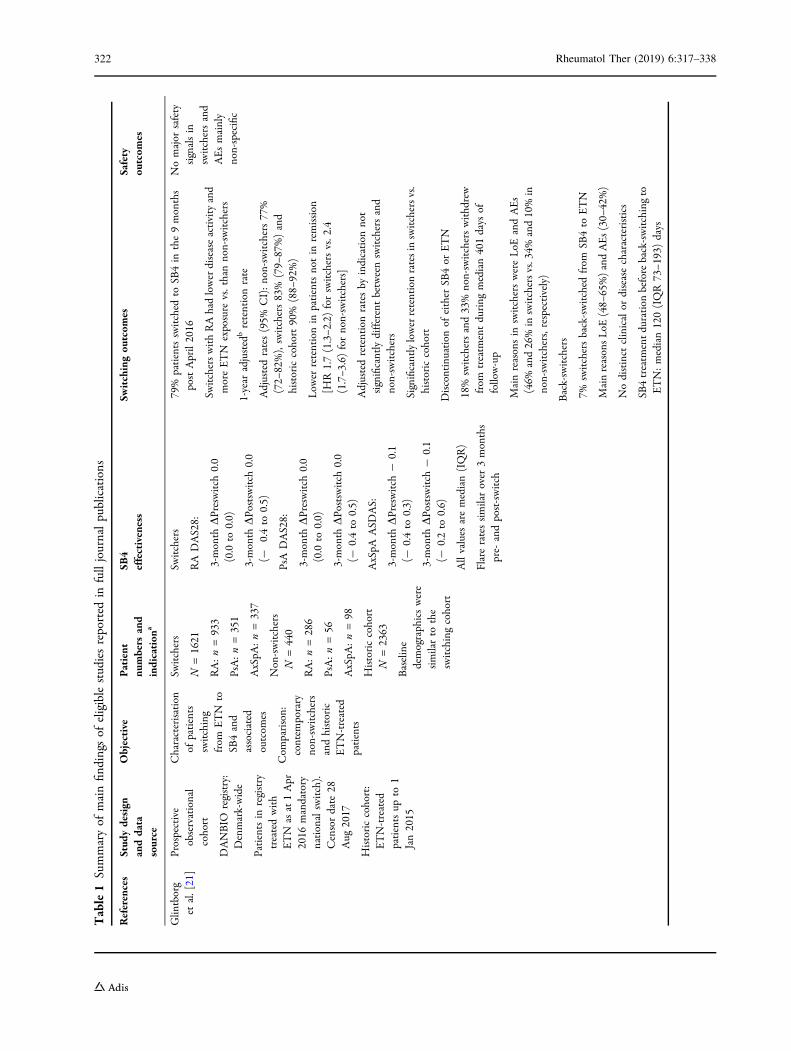
Table1
Summaryof
mainfin
dingsof
eligiblestudiesreported
infulljournalpublications
References
Stud
ydesign
anddata
source
Objective
Patient
numbers
and
indication
a
SB4
effectiveness
Switchingou
tcom
esSafety
outcom
es
Glin
tborg
etal.[21]
Prospective
observational
cohort
DANBIO
registry:
Denmark-wide
Patientsin
registry
treatedwith
ETN
asat1Apr
2016
mandatory
nationalswitch).
Censordate
28Aug
2017
Historiccohort:
ETN-treated
patientsup
to1
Jan2015
Characterisation
ofpatients
switching
from
ETN
toSB
4and
associated
outcom
es
Com
parison:
contem
porary
non-switchers
andhistoric
ETN-treated
patients
Switchers
N=1621
RA:n=933
PsA:n=351
AxSpA
:n=337
Non-switchers
N=440
RA:n=286
PsA:n=56
AxSpA
:n=98
Historiccohort
N=2363
Baseline
demographicswere
similarto
the
switchingcohort
Switchers
RADAS28:
3-month
DPreswitch
0.0
(0.0
to0.0)
3-month
DPo
stswitch
0.0
(-0.4to
0.5)
PsADAS28:
3-month
DPreswitch
0.0
(0.0
to0.0)
3-month
DPo
stswitch
0.0
(-0.4to
0.5)
AxSpA
ASD
AS:
3-month
DPreswitch
-0.1
(-0.4to
0.3)
3-month
DPo
stswitch
-0.1
(-0.2to
0.6)
Allvalues
aremedian(IQR)
Flareratessimilarover
3months
pre-
andpost-switch
79%
patientsswitched
toSB
4in
the9months
postApril2016
SwitcherswithRAhadlowerdiseaseactivityand
moreETN
exposure
vs.thannon-switchers
1-year
adjusted
bretentionrate
Adjustedrates(95%
CI):non-switchers77%
(72–
82%),switchers83%
(79–
87%)and
historiccohort90%
(88–
92%)
Low
erretentionin
patientsnotin
remission
[HR1.7(1.3–2
.2)forswitchersvs.2
.4(1.7–3
.6)fornon-switchers]
Adjustedretentionratesby
indication
not
significantlydifferentbetweenswitchersand
non-switchers
Significantlylowerretentionratesin
switchersvs.
historiccohort
Discontinuation
ofeither
SB4or
ETN
18%
switchersand33%
non-switcherswithdrew
from
treatm
entduring
median401days
offollow-up
Mainreasonsin
switcherswereLoE
andAEs
(46%
and26%in
switchersvs.34%
and10%in
non-switchers,respectively)
Back-switchers
7%switchersback-switched
from
SB4to
ETN
MainreasonsLoE
(48–
65%)andAEs(30–
42%)
Nodistinct
clinicalor
diseasecharacteristics
SB4treatm
entduration
beforeback-switchingto
ETN:median120(IQR73–1
93)days
Nomajor
safety
signalsin
switchersand
AEsmainly
non-specific
322 Rheumatol Ther (2019) 6:317–338

Table1
continued
References
Stud
ydesign
anddata
source
Objective
Patient
numbers
and
indication
a
SB4
effectiveness
Switchingou
tcom
esSafety
outcom
es
Tweehuysen
etal.[24]
Prospective,
controlled
cohort
BIO
-SPA
Nsingle
hospitalstudyin
theNetherlands
Patientstreated
withETN
asat
June
2016
who
wereinvitedto
switch
(non-
mandatory)
from
ETN
toSB
4.Last
6-month
evaluation
May
2017
Randomised
1:1to
receiveor
notto
receive
questionnaires
ontreatm
ent
expectations
and
beliefs
Historiccontrol
groupreceiving
ETN
in2014
(ETN
group)
Toevaluate
effectsof
non-
mandatory
switching
from
ETN
toSB
4on
drug
survivaland
effectiveness
Switchers
N=625
RA:n=433
PsA:n=128
AS:
n=64
Historiccontrol
N=600
RA:n=422
PsA:n=109
AS:
n=69
Mostcharacteristics
similarbetween
switchersand
historiccontrols
withtheexception
ofalonger
treatm
entduration,
alonger
dose
interval,a
lower
CRPlevelanda
lower
DAS28-CRP
scorein
theSB
4switchingcohort
Changeover
6months
Adjusteddifference
forswitchersvs.
historiccontrol:DAS28-CRP
0.15
[95%
CI0.05–0
.25];CRP
1.8[95%
CI0.3–
3.2]
Disease
activity
atbaselin
eand
6monthspost-switch
not
significantlydifferent
99%
ofpatientsswitched
toSB
4
6months’retention
Crude
rates(95%
CI):90%
(88–
93%)forSB
4vs.92%
(95%
CI90–9
4%)forETN
inhistoric
cohort
Switchershadhigher
relative
risk
oftreatm
ent
discontinu
ationvs.historicgroup(adjustedHR
1.57
[95%
CI1.05–2
.36]).Adjusted
discontinu
ationrates:SB
412.5%
vs.h
istoric
group8%
Predictorsof
SB4discontinu
ation:
shorterETN
duration,h
igherpatient’s
globalassessmentof
diseaseactivity
(RA)andhigher
baselin
eCRP
(RA)
Mainreasonsfordiscontinu
ationof
SB4vs.
ETN:LoE
(43%
vs.6
1%),AEs(47%
vs.2
8%)
Retention
ratesnotsignificantlyaffected
bytreatm
entexpectations
Num
berof
AEs
inswitchers
higher
than
inhistoricgroup:
median1.5
(IQR1–
3)versus
1(IQR
1–1);p
=0.01)
MoreAEswere
subjective
inswitchers(84%
)vs.h
istoric
group(40%
,p\
0.001)
AEsleadingto
discontinu
ations
84%
ofthese
weresubjective
inSB
4groupvs.
40%
inhistoric
group
Rheumatol Ther (2019) 6:317–338 323

Table1
continued
References
Stud
ydesign
anddata
source
Objective
Patient
numbers
and
indication
a
SB4
effectiveness
Switchingou
tcom
esSafety
outcom
es
Scherlinger
etal.[23]
Prospectivestudy
ofpatientsin
asinglehospital
(France)
system
atically
offeredanon-
medicalswitch
from
ETN
toSB
4
Inform
ation
supportstrategy
forpatients:oral
andwritten
inform
ationon
biosim
ilars
Recruitment1
May
to31
Oct
2017
with
follow-upto
31Dec
2017
Patientshadto
bestableon
anETN
regimen
forC
6months
andhave
controlled
disease
Toevaluate
switch
acceptance
rate
(primary
outcom
e),
switch
adherenceand
socio-
econom
icinfluenceson
acceptance
N=52
RA:n=20
AS:
n=22
PsA:n=4
Reactivearthritis:
n=2
SAPH
O:n=4
Not
reported
92%
initialswitch
acceptance
rate
Prim
aryrefusalsduemainlyto
fear
ofLoE
,no
confi
dencein
biosim
ilarity,fearof
AEs,will
tokeep
controlon
treatm
ent
Defactoswitch
ratewas85%(4
patientsinitially
agreeing
toswitch
didnotcommence
SB4)
3of
44switchersto
SB4discontinu
edand
returned
toETN:1dueto
objectivemoderate
RAflare-up;1dueto
AxSpA
flare-upand1due
toasym
ptom
aticanti-vitam
inK
overdose
86%
ofswitchersreported
good
experience
ofswitch;15%
feltpressurisedto
accept
switch
3patientsreported
positive
effect
ofswitch
onpain
index
4patientsreported
negative
effect
and2back-
switched
toETN
withgood
outcom
es
Totalback-switch
rate:7%
(3/42)
Discontinuations
ofSB
4
1objective
moderateRA
flare
1AxSpA
flare-up
1asym
ptom
atic
anti-vitam
inK
overdose
324 Rheumatol Ther (2019) 6:317–338

Table1
continued
References
Stud
ydesign
anddata
source
Objective
Patient
numbers
and
indication
a
SB4
effectiveness
Switchingou
tcom
esSafety
outcom
es
DiGiuseppe
etal.[19]
Analysisof
all
patientsin
the
Swedish
Rheum
atology
QualityRegister
(SQR)who
either
initiated
ETN
orSB
4between1April
2016
and31
Decem
ber2016
orwho
wereon
ETN
treatm
ent
by1April2016
Todescribe
the
uptake
ofetanercept
biosim
ilarsin
asetting
without
nationwide
mandatory
switchingand
tocompare
the
characteristics
ofpatients
starting
abiosim
ilar
withthose
starting
the
reference
product
N=249initiated
ETN
N=2691
initiated
SB4
Non-m
edicalswitches
from
ETN
toSB
4
N=1169
RA:n=736
PsA:n=251
SpA:n=93
AS:
n=89
Com
parisongroupof
non-switchingETN
patients:n=5845
Bionaıvepatients
initiating
SB4
N=933
RA:n=502
PsA:n=211
SpA:n=134
AS:
n=86
Patientsstarting
SB4
within6monthsof
discontinu
ingnon-
ETN
bDMARD
N=362
RA:n=197
PsA:n=74
SpA:n=54
AS:
n=37
Not
reported
Atstudyend,
31%
ofallpatientstreatedwith
ETN
orbiosim
ilarweretreatedwithSB
4
There
wereno
significant
differencesbetween
bionaıve
patientsstarting
ETN
andthose
starting
SB4,or
betweenpatientsdiscontinu
ing
anotherbD
MARD
andstarting
ETN
vs.
starting
SB4
Non-m
edicalswitchersfrom
ETN
toSB
4were
similarto
patientscontinuing
ETN,exceptthey
hadashortertimeon
ETN
andhigher
concom
itantuseof
MTX
The
totaln
umberof
patientson
anybD
MARD
increasedaftertheintroduction
ofSB
4
Not
reported
Rheumatol Ther (2019) 6:317–338 325

Table1
continued
References
Stud
ydesign
anddata
source
Objective
Patient
numbers
and
indication
a
SB4
effectiveness
Switchingou
tcom
esSafety
outcom
es
Egeberg
etal.
[20]
Analysisof
patientswith
moderateto
severe
PPtreatedwith
biologicsand
recorded
inthe
DERMBIO
registry,
between1
Janu
ary2007
and31
March
2017
(SB4became
availablein
March
2016
atwhich
timeit
was
national
policyto
initiate
orswitch
tothe
cheapestversion
ofthebiologic
prescribed)
Tocompare
the
safety,efficacy
anddrug
survivalof
bDMARDs
and
biosim
ilarsin
anationwide
Danishcohort
PatientswithPP
treatedwith:
ETN:n=512
SB4:
n=55
(44of
whom
were
switched
from
ETN)
Num
bersareat
first
treatm
entbetween
theanalysisdates
andanyonepatient
couldhave
been
treatedwith
multiplebiologics
SB4data
notreported
separately
from
ETN
Switch
from
ETN
toSB
4occurred
aftera
medianof
2089
days
Nosignificant
impact
ofswitchingon
drug
survival
Nosignificant
differencesin
risk
ofdiscontinu
ationbetweenSB
4vs.E
TN.
HR=0.50,9
5%CI0.11–2
.02,
p=0.317
adjusted
fordifferencesin
sex,MTX
useand
PsA
Incidencerate
ofAEsper100
treatm
entyears
(95%
CI)for
SB4vs.E
TN
Any
AE:34.2
(17.1–
68.3)vs.
32.5
(29.7–
35.6)
Infection:
17.1
(6.4–4
5.5)
vs.
16.4
(14.4–
18.6)
NMSC
:4.3
(0.6–3
0.3)
vs.
0.1(0.1–0
.8)
Cardiovascular:
4.3(0.6–3
0.3)
vs.0
.5(0.2–1
.0)
Neurologic:4.3
(0.6–3
0.3)
vs.
0.8(0.4–1
.4)
Other/
unspecified:4.3
(0.6–3
0.3)
vs.
14.6
(12.7–
16.7)
326 Rheumatol Ther (2019) 6:317–338

Table1
continued
References
Stud
ydesign
anddata
source
Objective
Patient
numbers
and
indication
a
SB4
effectiveness
Switchingou
tcom
esSafety
outcom
es
Pescitelli
etal.[22]
Description
ofexperience
with
ETN
andSB
4in
asingle
centre
(Italy),in
which
therewas
apolicyof
non-
medical
switchingfrom
ETN
toSB
4
Patientswith
moderateto
severe
PsO
and/or
PsA
Patientsswitched
from
ETN
toSB
4:n=32
(PsO
and
13withPsA)
PatientsETN-naıve
andinitiating
SB4:
n=12
(PsO
and2
withassociated
PsA)
Switchingpatients
PASI
scores
mean(SD):baselin
e2.15
(1.88);24
weeks
post-switch
1.20
(1.15)
DAS28mean(SD):baseline1.91
(0.90);24weekspost-switch1.74
(1.07)
Clin
icalremission
(bothPA
SIand/
orDAS28
increase\
10%)of
92%
forPsO
and64%
forPsA
DAS28notsignificantlydifferent
pre-
andpost-switch
PASI
improved
significantlypost-
switch
(p\
0.001)
ETN-naıve
PASI
scores
mean(SD):baselin
e13.09(2.25);24weeks
3.98
(2.42)
2patientsdiscontinu
edat
week16
dueto
PsAreactivation
andPsO
worsening
Improvem
ent[
50%inPA
SIscore
wasobserved
byweek12
in8of12
patients,with
furtherameliorationat
week24
(PASI75
in9of10
patients)
Nothing
reported
otherthan
effectivenessdata
Switchingpatients
ISRsin
4/32
patients
ETN-naıve
3patients
complainedof
diffusepruritus
afterfirst
injection
2reported
mild
fatigueduring
SB4treatm
ent
Studydescriptions
arebasedon
objectives
andoutcom
esrelating
toetanercept
andSB
4anddo
notaccoun
tforparallelanalyses
ofotherbiosim
ilarse.g.infliximab.U
nlessotherwisestated
‘switchers’arepatientschanging
from
ETN
toSB
4therapyand‘back-switchers’arepatientswho
initially
changedfrom
ETN
toSB
4andthen
returned
toETN
therapy.Where
therewere
multipleeffectivenessoutcom
es,D
AS28was
selected
forinclusionin
thetableas
thiswas
themostconsistentlyreported.Inallstudiesetanercept
was
thereference(originator)
product
AEadverseevent,ASankylosing
spondylitis,A
xSpA
axialspond
yloarthritis,B
IO-SPA
Nbiosim
ilartransition
studyon
persistenceandroleof
attributionandnocebo,C
Iconfidence
interval,C
RP
C-reactiveprotein,
DAS28diseaseactivity
calculator
scorein
28joints,D
AS28-CRPdiseaseactivity
score28–C
-reactiveprotein,
ETN
etanercept
referenceproduct,HRhazard
ratio,
IQR
interquartile
range,ISRinjectionsitereaction,L
oElack
ofeffect,M
TXmethotrexate,NMSC
nonm
elanom
askin
cancer,R
Arheumatoidarthritis,PP
plaque
psoriasis,PsApsoriaticarthritis,
PSAIpsoriasisarea
andseverity
index,PsO
psoriasis,SA
PHO
synovitis,acne,p
ustulosis,hyperostosisandosteitis,SpA
spondyloarthritis
aNum
berof
patientsby
indication
was
calculated
from
thepercentagesreported;roun
ding
was
adjusted
ifnecessaryso
that
thenu
mberssummed
tothetotalreported
bAdjustedforgend
er,age,m
ethotrexateuse,remission,com
orbidities,E
TN
startyear
Rheumatol Ther (2019) 6:317–338 327

exposure to fewer previous bDMARDs. Switch-ers with RA also had lower disease activity at thetime of switch than non-switchers at the time ofthe mandated switch. In the Swedish setting ofnon-mandatory switching no significant differ-ences were apparent between switching andnon-switching patients except that the formerhad a higher concomitant use of methotrexate(58.4% vs. 52.8%) and a shorter duration ofreference ETN exposure [mean (standard devia-tion) 5.0 (4.3) years vs. 5.6 (4.4) years] (Table 1)[19].
Some authors highlighted the importance ofsupportive communication with patients andpatient education to achieve high rates ofswitching [23, 32–34]. The only comparison ofpatient support programmes was reported in acongress abstract by Shah et al., who comparedthe switching rate for patients provided witheducation on switching and a specialistswitching clinic (n = 151) with the rate forpatients offered a switch at a routine clinic visit[32]. Full patient support was associated with ahigher switch rate over 12 months than less
Fig. 2 Number of patients receiving SB4 pooled from alleligible publications. Patients who switched from etaner-cept reference to SB4 and subsequently back-switched toetanercept reference are counted both as switchers andback-switchers. Where it was possible to determine thatthe same patients in a database were reported in differentpublications they have been counted once [7, 8]. AS
ankylosing spondylitis, AxSpA axial spondyloarthritis,ETN etanercept, JIA juvenile idiopathic arthritis, PsApsoriatic arthritis, RA rheumatoid arthritis, SpAspondyloarthritis
328 Rheumatol Ther (2019) 6:317–338
intensive support (95% vs. 75%). Scherlingeret al. reported 92% (48/52) initial acceptance ofa non-mandatory switch in patients in a singlehospital in France who were given oral andwritten information on biosimilars [23]. Posi-tive clinician opinions on SB4 were reported tobe the main reason for acceptance of switch in70% of patients. The characteristics of patientswho refused a switch were similar to those whoaccepted, with the exception of those holding anegative opinion of generic drugs (100% vs.11%, p\ 0.001) and a statistical trend towardsolder age and longer disease duration. A studydone in a single hospital in France with a rela-tively low switch acceptance rate (51.6% of eli-gible patients) found that physicians’ behaviourrather than patients’ characteristics were asso-ciated with switching. Older clinicians andthose with full-time academic posts were morelikely to switch patients, but there were noindependent patient characteristics associatedwith switching [35].
There were some data on patient attitudes toswitching. In a French clinic, the experience ofswitching (n = 44) was considered good by 86%of patients, although 15% felt pressure to acceptthe switch [23]. In a UK study of non-medicalswitching managed with education and a dedi-cated biosimilar switching clinic (n = 115), 43%of patients were pleased with the switch and23% were not pleased, with a further 33% eitherbeing indifferent, unsure or failing to answerthe question [36].
Effectiveness of SB4
Three full journal publications reported effec-tiveness outcomes for patients switching to SB4(Table 1) [21, 22, 24]. In the relatively largepopulation from the DANBIO registry that wasanalysed by Glintborg et al., pre- and post-switch changes over 3 months were not clini-cally different for a range of disease activitymeasures in patients with RA, PsA or AxSpA(Table 1) [21]. In the single-hospital BIO-SPANstudy of non-mandatory switches in theNetherlands, Tweehuysen et al. did not find anystatistically significant difference (adjusted forbaseline characteristics) between the 6-month
change in disease activity in a historic referenceETN-treated cohort of patients with RA, PsA andAS (n = 600) and that for switchers to SB4(n = 625), although the switchers had numeri-cally small changes in c-reactive protein (CRP)and Disease Activity Score 28 (DAS28; Table 1)[24]. There was no clinically meaningful changein disease activity between SB4-treated patientspre- and 6 months’ post-switch: median (in-terquartile range [IQR]) CRP level 1 (0–5) mg/lvs. 1 (0–6) mg/l, p = 0.13; median (IQR) DAS28-CRP 1.9 (1.5–2.6) vs.1.9 (1.4–2.6), p = 0.99; andmedian (IQR) Bath Ankylosing Spondylitis Dis-ease Activity Index (BASDAI) score 3.1 (1.8–5.4)vs. 3.3 (1.9–5.3), p = 0.25. A study exclusivelyon patients with moderate to severe PsO and/orPsA (n = 32) observed no difference in rates ofclinical remission (Psoriasis Scalp Severity Indexand/or DAS28 increase\ 10%) before and afterswitch to SB4—92% and 64% for PsO and PsApatients, respectively, p\0.001 [22].
Most of the congress reports with data on SB4effectiveness found no clinically meaningfuldifferences between pre- and post-switch diseaseactivity or changes over time in historic andswitching cohorts of patients (Table S1)[8, 31, 35–42]. In one study of 120 switchers,39.1% (47/120) of patients had increases inDAS28 resulting in 22.5% (27/120) of patientsmoving to a higher disease state [43]. Of patientswith worsening DAS28, 38.3% had disease flares,mainly in the first 4 months’ post-switch. Theauthors concluded that these observations mayhave reflected ‘natural’ fluctuations as increasesin disease activity weremore frequent in patientsnot in disease remission at the time of switching.
Safety
In patients switching from reference ETN to SB4in the DANBIO registry, no major safety signalswere observed, and AEs were mainly non-specific [21]. The overall rate of AEs observed inpatients with PsO in the DERMBIO registry didnot differ for SB4 vs. reference ETN treatment;the incidence rate (95% CI) per 100 treatmentyears was 34.2 (17.1–68.3) vs. 32.5 (29.7–35.6)[20]. In SB4 patients, the incidence rate ofinfections (95% CI) per 100 treatment years was
Rheumatol Ther (2019) 6:317–338 329

17.1 (6.4–45.5), compared with 16.4 (14.4–18.6)for reference ETN-treated patients. Safety dataappertaining to discontinuations is included inthe switching outcomes section above. Addi-tional safety data for switching patients repor-ted in congress abstracts are summarised inTable S1.
In bionaıve patients in the BSRBR-RA registrythe risk of serious AEs was similar betweenpatients initiating SB4 (n = 310) and those ini-tiating ETN (n = 192), as assessed at a 6-monthfollow-up visit, (HR = 0.5, 95% CI 0.3–1.1,p = 0.1) [26]. In the Italian Psobiosimilars reg-istry, the authors concluded that there was nosignificant difference in numbers of AEsbetween switch patients and ETN-naıve patientsinitiating SB4, with AEs reported in 3/158 (1worsening PsA, 1 upper respiratory tract infec-tion,1 melanoma) and 3/39 patients (2 wors-ening PsO and 1 herpes simplex virusinfection), respectively [25]. In the RABBITregistry, the AE profile of bionaıve patients ini-tiating reference ETN differed from that ofpatients initiating SB4 due to a higher rate ofinjection site reactions—7.3% (23/313 patients)vs. 2.6% (7/266 patients).
Immunogenicity as assessed by incidence ofanti-ETN antibodies was generally not reported.
Persistence Following a Switch to SB4
Retention rates (i.e. drug survival) and discon-tinuations were reported as outcomes ofswitching in the majority of studies[8, 20–24, 28, 31, 33, 35–37, 39, 41, 42, 44–48].Glintborg et al. and Tweehuysen et al. distin-guished between all discontinuations of SB4,from which the retention rate could be derived,and a sub-category of discontinuations that ledto a back-switch to reference ETN [21, 24]. Theyadjusted for potential baseline confounders incomparisons of rates with historic referenceETN controls, although this did not includetime-varying confounders such as methotrexateusage. In contrast, most of the congressabstracts did not indicate whether discontinu-ations included back-switches and did notappear to adjust for clinically relevant
confounders [reflected in the Downs and Blackquality scoring (Fig. S1)].
In the BIO-SPAN study, 10% of patientsswitching from reference ETN to SB4 discon-tinued vs. 8% in an historic cohort of referenceETN-treated patients. The relative risk (adjustedhazard ratio, HR) of discontinuing treatment inthe 6 months following the switch was 1.57(95% CI 1.05–2.36), which implied an adjusteddiscontinuation rate of 12.5% in switchers [24].The main reasons for discontinuation of SB4and reference ETN were lack of effect (43% vs.61%) and AEs (47% vs. 28%). These AEs weremore frequently subjective for switch patients:84% (46/55 AEs in 28 patient) vs. 40% (6/15 in13 patients) for the historical reference ETNcohort. Patient questionnaires prior to switch-ing did not show an association betweenpatients’ beliefs about medications or treatmentexpectations and discontinuation. SB4 discon-tinuation was associated with lower reportedself-efficacy with regard to coping with pain andother symptoms related to arthritis and ashorter duration of reference ETN treatment.Analysis of the DANBIO registry also found alower adjusted retention rate over 12 monthsfor switchers compared with historic ETN con-trols, who had similar baseline characteristics,but differences between switchers and contem-porary non-switchers were not significantlydifferent [21]. In both switchers and non-switchers retention rates were lower for patientsnot in remission at switch or baseline (crude HR[95% CI] 1.7 [1.3–2.2] and 2.4 [1.7–3.6],respectively), leading the authors to concludethat patient-related rather than drug-relatedfactors were more important in the decision todiscontinue. The possibility of a nocebo effectcontributing to discontinuation was suggestedby Scherlinger et al., who noted variability inthe pain indexes between patients afterswitches, which might be linked to fluctuationof painful periods in the natural process ofrheumatic disease.
In patients with PsO in the DERMBIO reg-istry discontinuation rate did not differ signifi-cantly between SB4 and reference ETN: adjustedHR adjusted for sex, methotrexate use andpresence of PsA was 0.50 (95% CI 0.11–2.02,p = 0.317) [20].
330 Rheumatol Ther (2019) 6:317–338

Retention rates over 6 months post-switch inanalyses presented in six congress abstracts (asreported or calculated from the number of dis-continuations reported) ranged from 82% to91% (Table S1) [33, 35, 37, 39, 41, 44]. Twostudies found lower retention rates (Table S1).In a small study in the Netherlands (n = 69switchers), the retention rate for SB4 was 75%[42]. In a UK study (n = 72 switchers) retentionrate was 73.6%; the main reasons for SB4 dis-continuation were loss of effect (58%) and AEs(32%); withdrawal in patients with RA wasassociated with duration on reference ETN(odds ratio 1.43 [95% CI 1.02–2.00]) [46]. Theauthors highlighted the fact that there was nosignificant change in disease activity for SpAand PsA, and the loss of effect in RA was due tosubjective measures except for CRP, suggestingthat there were reasons for withdrawal notdetected by the study. An analysis of non-medical switchers in a single rheumatologycentre in Sweden (reported in a journal letter)showed retention rate declining from 90% at6 months to 78% at 12 months and 69% at18 months, which was significantly lowercompared with a historical cohort (p = 0.0015)[8]. This was explained by patient preferencerather than objective worsening of disease.
Back-Switching
A proportion of patients who switched fromreference ETN to SB4 discontinued and back-switched to reference ETN. Some of the smallerstudies highlighted disease flares as a reason forback-switching [23, 30, 43]. This was the casefor 3 out of 44 patients back-switching in asingle-centre French study [23]. In a nationalaudit of Wales, 18 of 120 switching patientsexperienced flares and nine of these back-swit-ched to reference ETN [43].
Evidence from the large DANBIO registrystudy suggests the importance of subjectivereasons for back-switching. Glintborg et al.found that 7% (120/1641) of switchers back-switched after a median duration of SB4 treat-ment of 120 days [IQR (interquartile range)73–193], mainly because of lack of effect of SB4(48–65% depending upon indication) and AEs
(30–42% depending upon indication) [21]. Thebaseline characteristics of back-switchers werenot significantly different from switchers.However, the authors highlighted that changesin disease activity in patients restarting ETNcompared to while receiving SB4 were mainlysubjective. Changes in disease activity at thetime of ETN restart were mainly confined toPatient Global Scores, with little or no changesin CRP and swollen joint counts. Median (IQR)changes for patients with RA, PsA and AxSpAwere as follows: Patient Global Score 30 (12–52)mm, 15 (7–77) mm and 25 (19–35) mm,respectively; swollen joint count 1 (0–4), 0 (0–0)and not applicable (AxSpA), respectively; andCRP 0 (- 1 to 5) mg/l, 1 (0–2) mg/l and 0 (0–4),respectively. Similarly, subjective reasons interms of patient preference were the primaryreason for back-switching in a Dutch single-centre study. At time of censoring in the DAN-BIO study, 104/120 (87%) of patients who back-switched were still being treated with ETN witha median treatment duration of 236 (155–302)days.
Three small studies reported in congressabstracts found AEs to be the most frequentreason for back-switching, accounting for 58%(7/12) [42], 60% (6/10) [48] and 62.5% (6/8) [36]of back-switching, respectively (Table S1). Fourcongress abstracts reported ineffectivenessrather than AEs as the main reason for back-switching, accounting for 50% (7/14) [37], 80%(4/5) [39], 61% (11/18) [47] and 58% (11/19)[46] of back-switching, respectively (Table S1).In the last of these studies, the observed lack ofeffect was mainly subjective (see switchingoutcomes section above).
One study investigated the rate of back-switching in patients switching to SB4 in dif-ferent time periods [44]. Over time, there was aconstant increase in the use of SB4 but theproportion of patients back-switching to refer-ence ETN significantly increased from 7% (53/707) of patients starting SB4 between February2016 and September 2016 (p\0.05) to 10%(153/1607) of those starting between February2016 and March 2017 to 14% (320/2229) ofpatients starting SB4 between February 2016and August 2017 (p\0.05). No reasons forback-switching were reported in this study.
Rheumatol Ther (2019) 6:317–338 331

SB4 Effectiveness and Retention Ratesin ETN-Naıve Patients
Data from the BSRBR-RA registry found that theeffectiveness of SB4 in bionaıve patients was notsignificantly different from reference ETN afteradjusting for baseline characteristics [27]. SB4was also found to be effective in two studies ofETN-naıve patients with PsO. In a study of 39patients from the Psobiosimilars registry, mean(SD) Psoriasis Area Severity Index (PASI) reducedfrom 12.5 (6.2) at baseline to 6.7 (2.2) at month6 [24]. In an Italian study of 12 ETN naıvepatients, PASI score improved by more than50% in eight patients at week 12 of SB4 treat-ment, and by week 2, by which time twopatients had discontinued because of PsA reac-tivation and psoriasis worsening, a 75% reduc-tion in PASI score was achieved by 9 of 10patients [22]. Baganz et al. concluded from theirstudy of the German RABBIT registry that ref-erence ETN and SB4 were equally effective inbionaıve patients initiating these treatments(n = 313 and n = 266, respectively) [28]. Reten-tion was greater for SB4, with 17.3% discontin-uations up to 180 days after drugcommencement compared with 29.4% discon-tinuations in the reference ETN cohort; adjust-ing for disease duration and co-morbiditiesmade no significant difference. AEs were themost frequent cause of discontinuations in bothSB4- (48%) and ETN-treated patients (54%). Themost frequent AEs resulting in discontinuationswere disease flares in SB4 patients (12% of AEs)and skin reactions at the injection site in refer-ence ETN patients (26% of AEs).
Health Economics
Six congress abstracts reported economic out-comes of switching from reference ETN to SB4and these were all cost savings (Table S1)[32, 34, 36, 37, 39, 41]. For example, switching151 patients to SB4 in a UK hospital was esti-mated to result in a total saving of approxi-mately £500,000 per annum [36]. Theinvestment in a high intensity programme ofpatient support for switching saved approxi-mately £9000 per biologic-treated patient over a
year. In another group of hospitals in the UKpotential yearly savings were estimated at£660,000 and enabled the employment of anadditional clinical nurse and secretary.
DISCUSSION
This systematic review provides a comprehen-sive summary of published observational stud-ies on patients in Europe receiving the ETNbiosimilar SB4 in routine practice over the3 years after it gained marketing authorisation.Data from more than 13,500 patients in obser-vational studies and patient registries have beenpublished. As to be expected in the early yearsafter the introduction of a biosimilar into themarket, most studies presented results frompatients switching from reference ETN to SB4.However, large numbers of patients have alsobeen initiated on SB4 therapy without anyprevious exposure to ETN.
Across Europe, different national or localpolicies for the introduction of SB4 have influ-enced its switch acceptance rate; in most of thestudies there was a clinic-wide, non-medicalswitch of patients from reference ETN to SB4.When the acceptance rate was reported, thiswas in a majority of patients, ranging from51.6% to 99% across nine studies; in eight ofthese, the acceptance rate was at least 79%[21, 23, 24, 33–35, 38, 42, 47]. The highest rateof switching reported was in the non-manda-tory setting of the BIO-SPAN study (99%) [24]. Alower acceptance rate (79%) in the DANBIORegistry in Denmark, where switching wasmandated [21], was thought to be influenced bypatient-related factors such as co-morbiditiesand higher disease activity in non-switchers andthe absence of a 25 mg dose of SB4 at the time ofthe study [21]. A higher rate of methotrexateuse was also observed in switchers vs. non-switchers in both the DANBIO registry [21] andthe Swedish Rheumatology Quality register[19]; in the latter this was also seen for switchersto infliximab biosimilar [19]. The studies’ find-ings diverged, however, with respect to dura-tion of treatment with reference ETN, whichwas longer in switchers in the DANBIO registry
332 Rheumatol Ther (2019) 6:317–338

compared with switchers in the SwedishRheumatology Quality register.
The importance of patient education andsupport and clinician attitude towards switch-ing has been highlighted with respect toacceptance rate. The lowest rate of optionalacceptance rate was in a smaller French study(51.6%) and this was attributed to clinicianbehaviour [35]. In a real-world study on theacceptance of biosimilars in Germany, the mostcommon concern of patients was that they didnot know enough about the drug, and this wasmore frequent in patients prescribed a biosimi-lar than a reference product (36–41% vs.25–30%) [49]. Patients in the UK have similarlyreported that better communication by health-care professionals would increase their accep-tance of biosimilars [50]. Experts across Europehave cited lack of education of both cliniciansand patients as the main hurdle for acceptanceof biosimilars [51].
Overall the effectiveness of SB4 was compa-rable with reference ETN in terms of diseaseactivity pre- and post-switch and also in ETN-naıve patients. Results from DANBIO suggestthat SB4 effectiveness did not vary with indi-cation, but most reports did not give sufficientdetails to evaluate this [21]. In patients from thePsobiosimilars registry, switching to SB4 did notresult in any meaningful change in PASI oradditional AEs, and SB4 was also effective inETN-naıve patients [25].
Safety data were incompletely reported inmost of the studies, but there was no indicationfrom the AEs summarised that the safety profileof SB4 was different in routine practice fromthat demonstrated in the controlled clinicaltrial situation. The lack of immunogenicity datawas in line with data from clinical studies thatreported low rates of ADAs without clinicalrelevance and consequently ADAs are notcommonly collected in rheumatology practice[15]. In a non-interventional study of ETN-treated patients, in which all samples wereassessed in a single laboratory using the samemethodology, no ADAs were detected [52].
Retention rates for SB4 were generally high.However, two comparisons between SB4switchers and historic cohorts of ETN-treatedpatients showed lower retention rates in
patients switching to SB4 [21, 24]. The smalldifference in the retention rate in the BIO-SPANstudy might be attributable to calendar timebias, because clinicians were more likely to use a‘treat-to-target’ approach in 2016 than in2014—the time of the historic cohort [24]. SB4retention appeared to be negatively influencedby subjective (symptoms only perceptible to thepatient) [24] or non-specific AEs [21], subjectiveassessment of disease activity (e.g. self-reportedpain, Patient Global Score) [21, 24] and patientcharacteristics such as remission status at base-line (assessed by DAS28 or the AnkylosingSpondylitis Disease Activity Score) [21]. A simi-lar finding was reported by Tweehuysen et al. inseparate study, where a quarter of patientsswitching from infliximab reference to biosim-ilar (CT-P13) discontinued because of subjectiveassessments of disease activity or subjective AEs[53]. Defined nocebo effects have been reportedin 12.8% of patients switching to an infliximabbiosimilar, where a nocebo response wasdefined as ‘‘an unexplained, unfavourable ther-apeutic effect subsequent to a non-medicalswitch from originator infliximab to biosimilarinfliximab with regaining of the beneficialeffects after reinitiating the originator’’ [54].Tweehuysen et al. hypothesized that the higherretention rate they found for SB4 comparedwith that for an infliximab biosimilar in anearlier study could be due to increased confi-dence among clinicians after this previousbiosimilar experience, and the implementationof communication strategies that may havepositively influenced patients and reduced thelikelihood of nocebo effects [24, 53].
SB4 was also as effective as reference ETN inbionaıve patients in the BSRBR-RA registry withrespect to DAS28 and remission status [27].These real-world data indicate that the clinicalequivalence between SB4 and reference ETNthat was demonstrated in bionaıve patients inthe phase 3 RCT [13, 14] and in switchedpatients in the RCT open-label extension to this[15] is also seen in routine clinical practice.Furthermore, analysis of patients in a multi-switching cohort suggested that switching fromreference ETN to SB4 and then back to referenceETN for non-medical reasons does not impactdisease activity [8].
Rheumatol Ther (2019) 6:317–338 333

Back-switching rates across all the reportsreviewed varied from 4.6% to 26.4%[8, 21, 23, 44, 46–48], probably reflecting thediversity in settings and patient numbers. Therewas also one study of a clinic-wide non-medicalback-switch following a reduction in the priceof reference ETN [8]. Some of the data on back-switching and discontinuations were suggestiveof a nocebo effect; notably Glintborg et al.found the reasons given for back-switching weremainly subjective on the part of patients [21].
Real-world data opens the window to what isactually happening in clinical practice. It ben-efits from external validity and can provideinsights into indications not investigated inRCTs. The real-world evidence base presentedhere is rich in terms of overall patient numbers,geography and spread of indications; but itslimitations must be equally recognised. To adegree, high external validity sacrifices internalvalidity, making it difficult to definitively attri-bute differences or similarities in outcomes tothe intervention. Comparisons of retentionrates and drug effectiveness for non-switchersreceiving reference ETN and switchers receivingSB4 are likely to be influenced by selection bias.Some of the analyses by Glintborg et al. andSigurdardottir and Svard extended to follow-updurations of 12 and 24 months, respectively[8, 21]. However, many of the other studies hadfollow-up durations of only 6 months, which islikely to have made their findings more sus-ceptible to the effects of nocebo responses. As aresult of the observational setting, controllingfor bias e.g. selection bias, attrition bias ischallenging. As expected, the quality scoring ofpublications showed the quality of evidencefrom congress abstracts to be generally lowerand more varied than that from full journalpublications. Lower quality was primarily dueto incomplete reporting as a result of wordcount restriction, lack of clarity in themethodology and lack of statistical considera-tion for confounders. Nevertheless, balancingthe strengths and limitations of real-world evi-dence on SB4, the importance of continuedcommitment to generation of post-approvaldata and to maintenance of high-qualitypatient registries is apparent.
Most switches from reference ETN to SB4were made for reasons of cost-saving, and therealisation of these was demonstrated in severalstudies. Savings were reported only briefly incongress abstracts with insufficient detail forcritical appraisal; however, they are an indica-tion of tangible benefits from clinic-wideswitching policies.
Limitations of the Current Review
Systematic reviews are a robust tool for gather-ing, evaluating and summarising data fromexisting studies on a particular topic and draw-ing conclusions from this larger data pool.However, the quality of the subsequent reviewis dependent upon the data available. In thecase of the current review only 6 of the 31selected publications were full articles, with themajority of the remainder being conferenceabstracts. This limited the available data foreach study and the level of analysis that couldbe performed. Thus, while we believe the overallconclusions of the review are robust, it is pos-sible that some of the contributing data couldalter when the full articles are published.
The fact that all of the authors are employeesof the company that markets the product ofinterest could be viewed as introducing poten-tial bias into the review. However, one of themain purposes of a systematic review is toreduce potential bias as much as possible byintroducing clear selection and scoring pro-cesses through the use of checklists as detailedin the ‘‘Methods’’ section. We are confident thatthe conclusions of the current article are a truereflection of the data published.
CONCLUSION
A substantial body of real-world evidence nowexists on the use of SB4, the first subcutaneousanti-tumour necrosis factor biosimilar tobecome available in Europe. While the qualityof the reported evidence is variable, the experi-ence of switching from reference ETN to SB4 hasbeen generally positive, without loss of effec-tiveness or detriment to safety and tolerabilitycompared with the reference ETN, and with
334 Rheumatol Ther (2019) 6:317–338

persistence rates of at least 75%. Reportedacceptance has been mainly high, ranging from51.6% to 99% across nine studies, in eight ofwhich it was at least 79%; patient acceptancehas benefited from a supportive communica-tions programmes. ETN-naıve patients havebeen initiated on SB4 treatment (n = 2499reviewed here) and no differences are reportedin their clinical outcomes compared with thoseof patients treated with ETN. Overall, the bodyof real-world evidence from 13,552 patientspresented here provides additional reassurancethat the biosimilar approval pathway is robustand that SB4 is as effective and safe as ETN ref-erence in both switched and naıve patients.
ACKNOWLEDGEMENTS
Funding. This review and the journal’sRapid Service Fee were funded by Biogen Inter-national GmbH. All authors had full access toall of the data in this study and take completeresponsibility for the integrity of the data andaccuracy of the data analysis.
Medical Writing and Editorial Assis-tance. Medical writing and editorial assistancewere provided by Susanna Ryan of SpringerHealthcare and were funded by Biogen Inter-national GmbH.
Authorship. All named authors meet theInternational Committee of Medical JournalEditors (ICMJE) criteria for authorship for thisarticle, take responsibility for the integrity ofthe work as a whole, and have given theirapproval for this version to be published.
Authorship Contributions. All authors con-tributed to the design of the review methodol-ogy, analysis of the data, and critical review andmodification of the manuscript. All authorshave approved the final version of themanuscript.
Disclosures. Hans C. Ebbers is an employeeof Biogen International GmbH and may holdstock in Biogen. Burkhard Pieper is an employee
of Biogen International GmbH and may holdstock in Biogen. Amine Issa is an employee ofBiogen International GmbH and may holdstock in Biogen. Janet Addison is an employeeof Biogen International GmbH and may holdstock in Biogen. Ulrich Freudensprung is anemployee of Biogen International GmbH andmay hold stock in Biogen. Mourad F. Rezk is anemployee of Biogen International GmbH andmay hold stock in Biogen.
Compliance with Ethics Guidelines. Thisarticle is based on previously conducted studiesand does not contain any studies with humanparticipants or animals performed by any of theauthors.
Data Availability. All data generated oranalysed during this study are included in thispublished article/as supplementary informationfiles.
Open Access. This article is distributedunder the terms of the Creative CommonsAttribution-NonCommercial 4.0 InternationalLicense (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommer-cial use, distribution, and reproduction in anymedium, provided you give appropriate creditto the original author(s) and the source, providea link to the Creative Commons license, andindicate if changes were made.
REFERENCES
1. Committee for Medicinal Products for Human Use.Guideline on similar biological medicinal products.2014. https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-similar-biological-medicinal-products-rev1_en.pdf. Accessed 6 Feb2019.
2. Food and Drug Administration. Biosimilars andinterchangeable products. 2017. https://www.fda.gov/Drugs/DevelopmentApprovalProcess/HowDrugsareDevelopedandApproved/ApprovalApplications/TherapeuticBiologicApplications/Biosimilars/ucm580419.htm. Accessed 7 May 2019.
3. Katkade VB, Sanders KN, Zou KH. Real world data:an opportunity to supplement existing evidence for
Rheumatol Ther (2019) 6:317–338 335

the use of long-established medicines in health caredecision making. J Multidiscip Healthc.2018;11:295–304.
4. Scavone C, di Mauro G, Mascolo A, Berrino L, RossiF, Capuano A. The new paradigms in clinicalresearch: from early access programs to the noveltherapeutic approaches for unmet medical needs.Front Pharmacol. 2019. https://doi.org/10.3389/fphar.2019.00111.
5. Kristensen LE, Alten R, Puig L, et al. Non-pharma-cological effects in switching medication: thenocebo effect in switching from originator tobiosimilar agent. Biodrugs. 2018;32(5):397–404.
6. Rezk MF, Pieper B. Treatment outcomes withbiosimilars: be aware of the nocebo effect.Rheumatol Ther. 2017;4(2):209–18.
7. European Medicines Agency. Summary of the riskmanagement plan (RMP) for Benepali (etanercept).2015. https://www.ema.europa.eu/en/documents/rmp-summary/benepali-epar-risk-management-plan-summary_en.pdf. Accessed 6 Feb 2019.
8. Sigurdardottir V, Svard A. Repeated switchesbetween reference product etanercept and biosimi-lar do not affect disease activity or retention rate ofetanercept over 24 months—a cohort study withhistorical controls. Joint Bone Spine. 2019;86(4):529–30.
9. Amgen. Enbrel Prescribing Information. ThousandOaks: Amgen. 2019. https://www.pi.amgen.com/*/media/amgen/repositorysites/pi-amgen-com/enbrel/enbrel_pi.pdf. Accessed 2 Aug 2019.
10. Pfizer Europe. Enbrel summary of product charac-teristics. Brussels: Pfizer Europe; 2018.
11. Gulacsi L, Brodszky V, Baji P, et al. Biosimilars forthe management of rheumatoid arthritis: economicconsiderations. Expert Rev Clin Immunol.2015;11(Suppl 1):S43–52.
12. Kalo Z, Voko Z, Ostor A, et al. Patient access toreimbursed biological disease-modifying antirheu-matic drugs in the European region. J Mark AccessHealth Policy. 2017;5(1):1345580.
13. Emery P, Vencovsky J, Sylwestrzak A, et al. A phaseIII randomised, double-blind, parallel-group studycomparing SB4 with etanercept reference productin patients with active rheumatoid arthritis despitemethotrexate therapy. Ann Rheum Dis.2017;76(1):51–7.
14. Emery P, Vencovsky J, Sylwestrzak A, et al. 52-weekresults of the phase 3 randomized study comparingSB4 with reference etanercept in patients with
active rheumatoid arthritis. Rheumatol (Oxford).2017;56(12):2093–101.
15. Emery P, Vencovsky J, Sylwestrzak A, et al. Long-term efficacy and safety in patients with rheuma-toid arthritis continuing on SB4 or switching fromreference etanercept to SB4. Ann Rheum Dis.2017;76:1986–91.
16. Charles C. The evolving biosimilar landscape:approval of the first etanercept biosimilar in European interview with Emilio Martin-Mola. Eur Med J.2016;1(3):76–84.
17. European Public Assessment Report for Benepali,European Medicines Agency. 2019. https://www.ema.europa.eu/en/medicines/human/EPAR/benepali.Accessed 2 Aug 2019.
18. Downs SH, Black N. The feasibility of creating achecklist for the assessment of the methodologicalquality both of randomised and non-randomisedstudies of health care interventions. J EpidemiolCommunity Health. 1998;52(6):377–84.
19. Di Giuseppe D, Frisell T, Ernestam S, et al. Uptake ofrheumatology biosimilars in the absence of forcedswitching. Expert Opin Biol Ther. 2018;18(5):499–504.
20. Egeberg A, Ottosen MB, Gniadecki R, et al. Safety,efficacy and drug survival of biologics and biosim-ilars for moderate-to-severe plaque psoriasis. Br JDermatol. 2018;178(2):509–19.
21. Glintborg B, Loft AG, Omerovic E, et al. To switchor not to switch: results of a nationwide guidelineof mandatory switching from originator tobiosimilar etanercept. One-year treatment out-comes in 2061 patients with inflammatory arthritisfrom the DANBIO registry. Ann Rheum Dis.2019;78(2):192–200.
22. Pescitelli L, Lazzeri L, Di Cesare A, Tripo L, Ricceri F,Prignano F. Clinical experience with the etanerceptbiosimilar SB4 in psoriatic patients. Int J ClinPharm. 2019;41(1):9–12.
23. Scherlinger M, Langlois E, Germain V, Schaever-beke T. Acceptance rate and sociological factorsinvolved in the switch from originator to biosimilaretanercept (SB4). Semin Arthritis Rheum.2019;48(5):927–32.
24. Tweehuysen L, Huiskes VJB, van den Bemt BJF,et al. Open-label, non-mandatory transitioningfrom originator etanercept to biosimilar SB4: six-month results from a controlled cohort study.Arthritis Rheumatol. 2018;70(9):1408–18.
25. Gisondi P, Bianchi L, Calzavara-Pinton P, et al.Etanercept biosimilar SB4 in the treatment of
336 Rheumatol Ther (2019) 6:317–338

chronic plaque psoriasis: data from the Psobiosim-ilars registry. Br J Dermatol. 2019;180(2):409–10.
26. De Cock D, Dyball S, Kearsley-Fleet L, Watson K,Hyrich K. Profiling rheumatoid arthritis biosimilarswitchers: data from the British Society forRheumatology Biologics Register for RheumatoidArthritis. Rheumatology (UK). 2018;57(suppl3):iii148.
27. De Cock D, Kearsley-Fleet L, Davies R, Watson K,Hyrich K. SB4 shows comparable short-term effec-tiveness to its etanercept originator as first-linebiologic treatment for patients with rheumatoidarthritis in routine clinical care. Arthritis Rheuma-tol. 2018;70(suppl 10):2539.
28. Baganz L, Meissner Y, Herzer P, Braun J, Grassler A,Strangfeld A, Zink A. Treatment continuation onthe etanercept original in comparison with abiosimilar. Arthritis Rheumatol. 2018;70(suppl10):2512.
29. Rabbitts R, Jewell T, Marrow K-L, Herbison C,Laversuch C. Switching to biosimilars: an earlyclinical review. Rheumatology. 2017;56(suppl2):ii132.
30. Steel L, Marshall T, Loke M. Real world experienceof biosimilar switching at the Norfolk and NorwichUniversity Hospital, United Kingdom. Ann RheumDis. 2018;77(Suppl):321.
31. Haugeberg G, Bakland G, Rødevand E, Fevang BT,Hansen IJW, Diamantopoulos A. Drug survival andreason for drop-out in rheumatoid arthritis patientswith a non-medical switch from originator tobiosimilar etanercept—preliminary data from aNorwegian multicenter study. Ann Rheum Dis.2018;77(suppl 2):1383.
32. Shah K, Flora K, Penn H. Cost effectiveness of a highintensity programme (HIP) compared to a lowintensity programme (LIP) for switching patientswith rheumatoid arthritis to the etanerceptbiosimilar. Rheumatology (UK). 2018;57(suppl3):iii68–9.
33. Holroyd C, Wallis D, Bennett S, Clayton P, EdwardsCJ. Switching from bio-original etanercept tobiosimilar etanercept SB4: patient acceptability andoutcomes in the real world. Ann Rheum Dis.2017;76(supple 2):1180.
34. Szlumper C, Topping K, Blackler L, et al. Switchingto biosimilar etanercept in clinical practice.Rheumatology (UK). 2017;56(suppl 2):ii139.
35. Al Tabaa O, Etcheto A, Miceli-Richard C. Switchfrom innovator etanercept to biosimilar etanerceptin inflammatory rheumatic diseases: the experience
of Cochin University Hospital Paris-France. AnnRheum Dis. 2018;77(suppl 2):960.
36. Shah K, Flora K, Penn H. Clinical outcomes of amulti-disciplinary switching programme tobiosimilar etanercept for patients with rheumatoidarthritis. Rheumatol (UK). 2018;57:iii143–4.
37. Alkoky H, Pakozdi A, Tahir H. Benepali switches inclinical practice—a positive single centre experi-ence. Arthritis Rheumatol. 2018;70(suppl 10):2511.
38. Brites L, Costa F, Freitas J, et al. Impact of blockswitch to biosimilar etanercept in practice, acrossdifferent rheumatic diseases. Arthritis Rheumatol.2018;70(suppl 10):2534.
39. Dyball S, Hoskins V, Christy-Kilner S, Haque S.Effectiveness and tolerability of benepali inrheumatoid arthritis patients switched from enbrel.Arthritis Rheumatol. 2017;69(Suppl 10):2447.
40. Kruger K, Selmi C, Cantagrel A, et al. Benefit study:results of interim analysis of a pan Europeanobservational study to evaluate real-world effec-tiveness of SB4 following transition from originatoretanercept (ETN) in patients with rheumatoidarthritis or axial spondyloarthritis. ArthritisRheumatol. 2018;69(suppl 10):2537.
41. Ma J, Petford S, Jones L, Douglas K, John H. Audit ofthe clinical efficacy and safety of etanerceptbiosimilar to its reference product in patients withinflammatory arthritis: experience from a districtgeneral hospital in the United Kingdom. AnnRheum Dis. 2018;77(suppl 2):1386.
42. Muskens WD, Rongen-van Dartel SAA, Adang E,van Riel PL. The influence of switching from etan-ercept originator to its biosimilar on effectivenessand and the impact of shared decision making onretention and withdrawal rates. Ann Rheum Dis.2018;77(suppl 2):1399.
43. Rajamani K, Choy E. Change in disease activityafter switching etanercept (originator) to biosimilar(Benepali) is associated with active disease at base-line. Arthritis Rheumatol. 2018;70(suppl 10):2513.
44. Alten R, Jones H, Curiale C, Meng T, Lucchese L,Miglio C. Real world evidence on switchingbetween etanercept and its biosimilar in rheumaticdiseases. Ann Rheum Dis. 2018;77(suppl 2):961.
45. De Cock D, Kearsley-Fleet L, Davies R, et al.Biosimilar use in patients with juvenile idiopathicarthritis in a real-world setting in the United King-dom. Ann Rheum Dis. 2018;77(suppl 2):485.
46. Madenidou AV, Jeffries A, Varughese S, et al.Switching patients with arthritis from etanercept(Enbrel) to the biosimilar drug, Benepali: a single-
Rheumatol Ther (2019) 6:317–338 337

center retrospective observational study. ArthritisRheumatol. 2018;70(suppl 10):2533.
47. Patel D, Ahmed TJ, Levy S, Rajak R, SathananthanR, Horwood N. Analysis of rheumatoid arthritispatients who failed the switch from originatoretanercept to biosimilar etanercept in Croydon.Rheumatology (UK). 2018;57:iii199.
48. Smith R, Fawthrop F. Similar experience ofbiosimilars: a review of Rotherham Hospital’sexperience of switching from enbrel to benepali.Rheumatology (UK). 2018;57(suppl 3):iii64.
49. Waller J, Sullivan E, Piercy J, Black CM, Kachroo S.Assessing physician and patient acceptance ofinfliximab biosimilars in rheumatoid arthritis,ankylosing spondyloarthritis and psoriatic arthritisacross Germany. Patient Prefer Adherence.2017;11:519–30.
50. Aladul MI, Fitzpatrick RW, Chapman SR. Patients’understanding and attitudes towards infliximaband etanercept biosimilars: result of a UK web-basedsurvey. Biodrugs. 2017;31(5):439–46.
51. Moorkens E, Vulto AG, Huys I, et al. Policies forbiosimilar uptake in Europe: an overview. PLoSOne. 2017;12(12):e0190147.
52. Moots RJ, Xavier RM, Mok CC, et al. The impact ofanti-drug antibodies on drug concentrations andclinical outcomes in rheumatoid arthritis patientstreated with adalimumab, etanercept, or infliximab:results from a multinational, real-world clinicalpractice, non-interventional study. PLoS One.2017;12(4):e0175207.
53. Tweehuysen L, van den Bemt BJF, van Ingen IL,et al. Subjective complaints as the main reason forbiosimilar discontinuation after open-label transi-tion from reference infliximab to biosimilar inflix-imab. Arthritis Rheumatol. 2018;70(1):60–8.
54. Boone NW, Liu L, Romberg-Camps MJ, et al. Thenocebo effect challenges the non-medical inflix-imab switch in practice. Eur J Clin Pharmacol.2018;74(5):655–61.
338 Rheumatol Ther (2019) 6:317–338