reaching the hard-to-reach
TRANSCRIPT

Reaching the Hard-to-Reach
Migrants, Nomads, IDPs & Border Communities
Lessons from the CORE Group Polio Project in India, South Sudan, and the Horn of Africa

Session Objectives
By the end of this session, participants will have: (1) Examined strategies to reduce inequity in local
health systems by reaching marginalized groups and improving immunization systems
(2) Considered how these strategies can be applied to
other public health initiatives

Current CGPP country Past CGPP country
647
2,710
319
4,296
1,238
9,210 community mobilizers in five countries

CORE Group Spring 2015 Global Health Practitioner Conference
Hilton ,Alexandria , VA
16 April 2015
Reaching the hard – to – reach population Lessons from India Polio Eradication Program.

Presentation outline
• About CORE Group Polio Project India • Inequity • Strategies to reach out to marginalized
groups • Communication Package • Lessons learnt

The CORE Group Polio Project (CGPP)
– Partners : ADRA, PCI and CRS and 10 national
NGOs – The secretariat works in close collaboration with
the Ministry of Health, WHO, UNICEF, Rotary International and USAID.
– In 2003, UNICEF & CGPP started working together as the ‘Social Mobilization Network’ (SM Net) to provide concentrated support in high risk areas (for polio) of Uttar Pradesh state.
– CGPP reaches about 600,000 under 5 children in 12 districts of UP through 1300 + mobilizers

0142
741
559
874
676
66134
225268265
1126
0
300
600
900
1200
1500
1800
2100
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012*
P1 wild P3 wild * data as on 14 September 2012 P2 wild
Polio : Progress in India – A snapshot • 1995: Polio SIAs (campaigns) launched
• 1997: Acute Flaccid Paralysis (AFP) Surveillance initiated
• 1999: Last case of Wild Polio Virus (WPV) type 2 – (U.P)
• 2010: Last case of WPV type 3 - (Jharkhand)
• 2011: Last case of WPV type 1 - ( West Bengal)
• 2012: India removed from list of endemic countries
1600
mOPV 1 bOPV 1 & 3
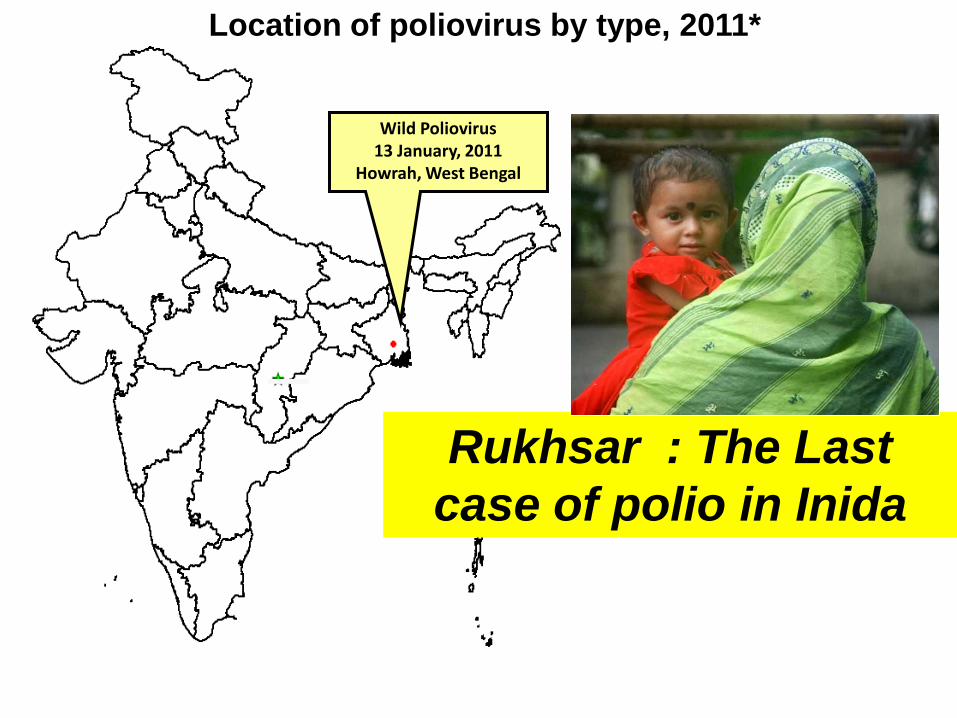
Location of poliovirus by type, 2011*
Wild Poliovirus 13 January, 2011
Howrah, West Bengal
Rukhsar : The Last case of polio in Inida

Dr Poonam Khetrapal Singh, Regional Director, WHO SEARO receiving the polio-free certificate from the Chairperson of Regional Certification
Commission for Polio Eradication
27 March 2014 WHO South-East Asia Region certified polio-free

India/Uttar Pradesh Polio Stats
NIDs started from 1995. 2.3 million vaccinators reach about 175 million <5 children on each
NID. Govt. of India contribution to Polio Eradication 1985- 2012
$1237.28 million
U.P State 75 Districts
Population: 199.6 million Under 5 population: 25 million
33 million houses visited by polio vaccination teams per SIA round

Non-migratory
93%
Migratory7%
Non-migratory
98%
Migratory2%
Uttar Pradesh
(N= 111)
Bihar
(N= 83)
WPV cases by migration status, 07-09*
Non-migratory
58%
Migratory42%
Rest of India
(N= 31) * data as on 30 october 2009
Non-migratory
85%
Migratory15%
Non epidemic UP*
(N= 54)
*Non epidemic UP excludes Moradabad, JP Nagar,Badaun, Kanshi ram nagar, Bareilly and Rampur dists of UP
Inequity : disproportionate number of Polio
cases were reported among
migrant population
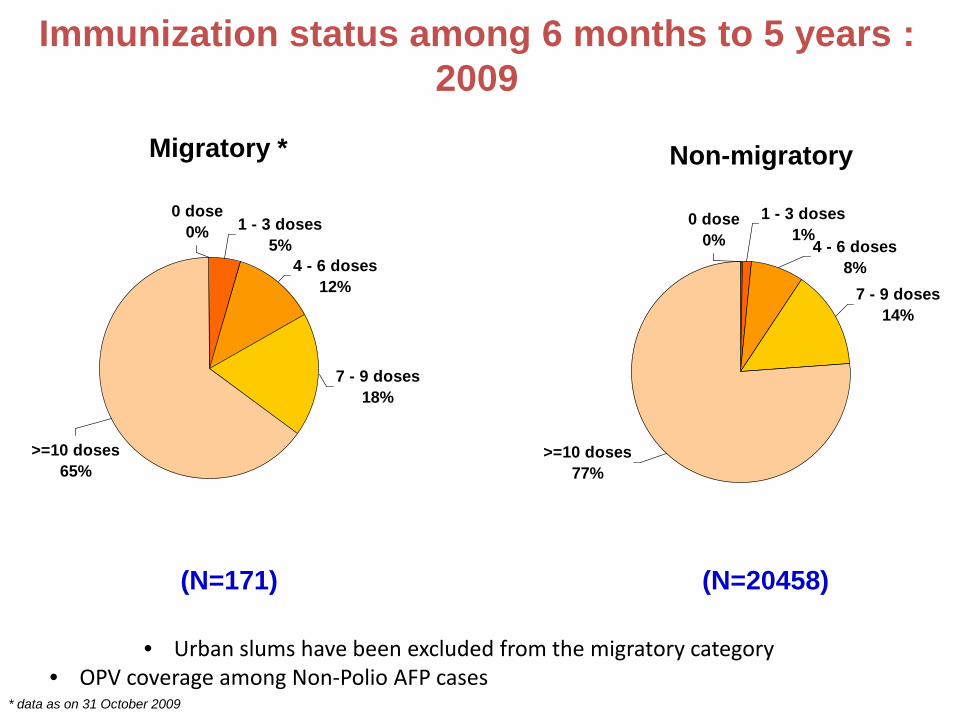
4 - 6 doses12%
>=10 doses65%
1 - 3 doses5%
7 - 9 doses18%
0 dose0%
(N=171)
Migratory * Non-migratory
* data as on 31 October 2009
4 - 6 doses8%
>=10 doses77%
1 - 3 doses1%
7 - 9 doses14%
0 dose0%
(N=20458)
Immunization status among 6 months to 5 years : 2009
• Urban slums have been excluded from the migratory category • OPV coverage among Non-Polio AFP cases

Marginalized Groups Brick Kilns workers
Construction sites
Nomads

Reaching out to marginalized groups: Bringing equity in Health System

Tracking of High Risk Groups
• Mapping of HRGs sites.
• Regularly updating the data
• Joint validation of data with WHO & Govt.

Tracking of High Risk Groups (HRGs)
• Identifying informers
Brick kiln owners/managers
Construction contractors
Barbers
Gate keepers in slums

HRGs Tracking Format

1. Inclusion of > 400,000 high risk settlements with Routine Immunization micro plans
~ 257,000 Migrant sites
Migrant sites High risk areas in settled population
~ 154,000 HR areas in settled population
= 10 Migrant sites = 10 HR sites

Unreached
the

Barbers
Shopkeepers
Brick kiln owners
Small contractors Identification of informers
More than 1000 informers identified

Need to shift from extensive mass awareness
approach to addressing specific conditions/needs
of specific groups
Tailor made strategies

Revised communication package

Focus on skill building of
communicators
Shift from instructive to negotiation approach

A strong MIS supported activity planning and implementation
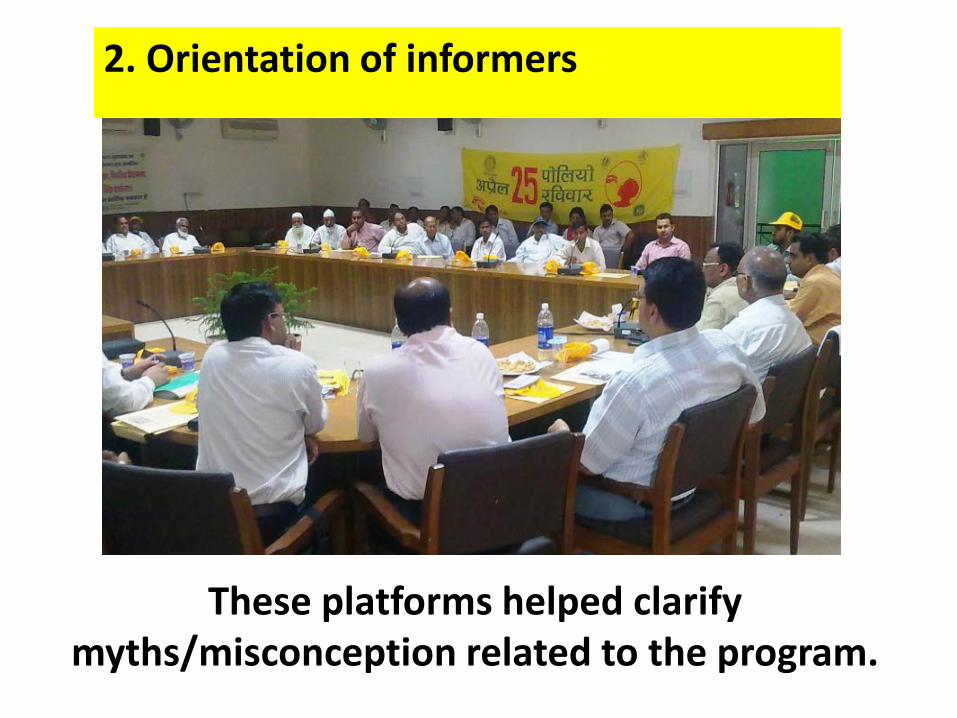
2. Orientation of informers
These platforms helped clarify myths/misconception related to the program.
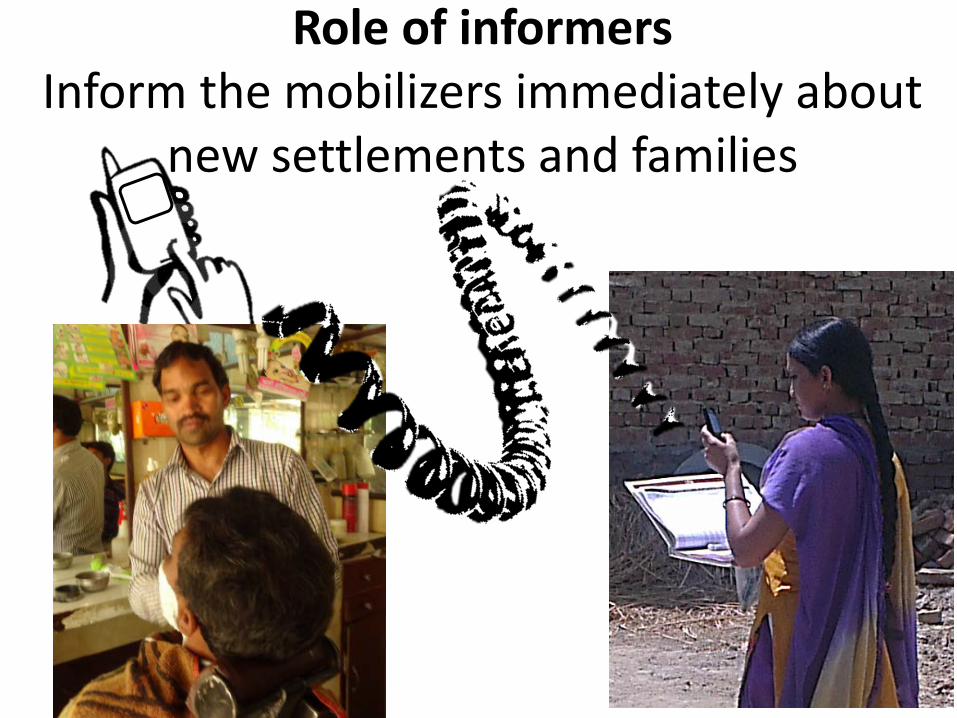
Role of informers Inform the mobilizers immediately about
new settlements and families

3. One to one and group meetings
Went as per their convenience

4. Pictorial materials displayed at strategic locations
Any where you go Give shots & polio drops

5. Health camps/outreach services held

Tapping opportunities for announcements of key messages
Tapping opportunities for announcements of key messages

More than 250000 sites were identified

Lessons learnt • Working in partnership works! • Strong Government ownership at all levels • Synergistic & non-overlapping support by partners
enhances programme effectiveness • Data driven decision making to identify and respond to
unreached areas/populations • Communication strategies need to be tailor made as per
audiences profile • Simple, picture & action oriented communication
materials works better • Tracking system can used in other programs like TB, Ebola.

Thanks

Community volunteers support in strengthening weak
health system in South Sudan to reach the hard to reach population
Core Group Spring Meeting
Presenter: Anthony Kisanga
Core Group South Sudan
April 13-17, 2015

Presentation outline
• Definition of terms • Brief introduction on the health situation in South
Sudan • Background to CGPP Sudan • Contribution of community volunteers • Outcome of community volunteers contribution • Challenges • Lessons learnt • Conclusion

Definition of terms • Community Volunteers: a group of individuals who has
undergone basic or no formal education at all but provides significant community health intervention. They are selected, trained and working for their own communities but not necessarily part of the formal health system, they include vaccinators, cold chain assistants, community mobilizers and independent monitors.
• Hard to reach communities: communities who are not easily accessible to health services due to one or more adverse conditions: distance from the nearest health facility, difficult terrain (mountainous areas, forested areas), flooding, insecurity, poor or unreliable road networks, nomadic lifestyle.

Cont….
• Weak health system: a health system which is unable to meet the basic health needs of its people. Weakness in light of insufficient qualified health workers, diseases surveillance, public awareness, chronic shortage of supplies e.g. vaccines, inequality in distribution of health workers and health facilities, limited or no community outreach programs and engagement of the local population.

Brief introduction on the health situation in South Sudan • South Sudan become independent in July 2011, 10 States
and 79 counties
• Population project (2012) puts the figure for South Sudan at 11,532,241
• Only one third of the country has access to basic health services
• It has 1,090 functional health facilities with 37 of them being hospitals.

Cont….. • It has the worst shortage of health workers put at 1.5
doctors and 2 nurses per every 100,000 population.
• Extreme inequality in distribution of health facilities and health workers with urban areas most favored
• Its maternal mortality ratio stands at 2,054/100,000 and under five mortality rate was estimated at 135/1,000 live births. (Sudan HH Survey 2006/2010)
• 2011 EPI survey shows 16.5% of children under the age of one fully vaccinated and only 22.1% completed OPV3.

Background to Core Group South Sudan
• Started operations in 2011, within eight worst performing counties in immunization mostly based at the Southern borders of South Sudan.
• Core Group South Sudan has three partners: American Refugee Committee, World Vision South Sudan and Amref Health South Sudan.
• It supports comprehensive EPI services that focuses on; 1. Routine immunization both at facility and community level 2. Support Polio National Supplementary Immunization Days 3. Community-based disease surveillance

Cont… • Works in Eight counties ( Western, Central and Eastern
Equatoria States)
• 955 volunteers (358 vaccinators, 54 cold chain assistants, 319 community mobilizers and 224 independent monitors)


Why these counties?
Selected by MoH Criteria of selection: Poor performance routine immunization. Along the border areas to Interrupt transmission Hard to reach
(MOH Administrative Data)

Contribution of community volunteers
• Under this theme we shall be looking into the following areas of health system strengthening that community volunteers have supported:
1. Community-centered planning 2. Service delivery 3. Supply chain 4. Monitoring and evaluation (disease surveillance, monitoring
quality of polio immunization campaigns) 5. Cross border initiatives

Community-centered planning • Engagement of community
leaders in social mapping
• Wealth of knowledge by the community
• Trust in whatever is done
• Acceptance
• Ownership
• Accountability

Service delivery Shortage in professional trained health workers. Only 30% of South Sudanese have access to basic health service. Inequality in health facility and health workers distribution. Outreaches: 5 kms and above Other facilities with no cold chain Vaccination under trees, churches, schools in the villages

Improving knowledge on immunization services using local acceptable means in the community
Mothers group dialogue Drama Local music Community leaders meetings

Overcoming challenges in transport means to reach the unreachable during polio campaign

Improving vaccine stock outs in the remote health facilities Reduced stock out of vaccines from 100% in 2011 to less than 10% in 2014 By using the cost effective means of transport . Delivering vaccines from county Vaccine stores to the most remote areas

Community disease surveillance 319 community mobilizers Conduct active AFP case search Report other diseases e.g. measles Report to the nearest health center or WHO Field assistant for investigation Educate households Refer mothers & children for vaccination Organize for outreach in their villages in Collaboration with vaccinators
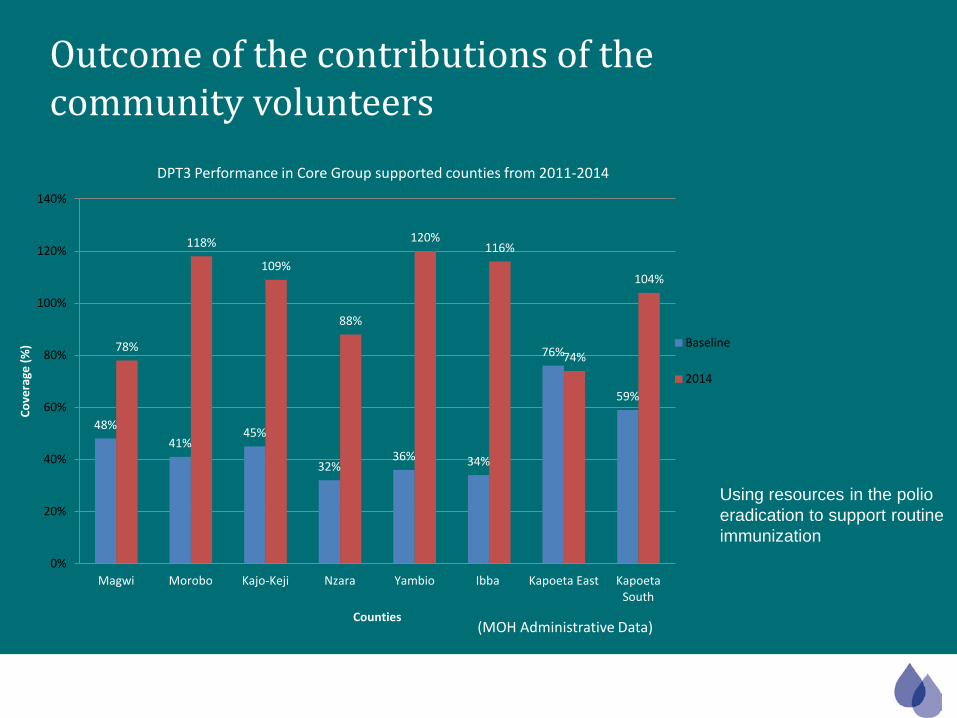
48% 41%
45%
32% 36% 34%
76%
59%
78%
118%
109%
88%
120% 116%
74%
104%
0%
20%
40%
60%
80%
100%
120%
140%
Magwi Morobo Kajo-Keji Nzara Yambio Ibba Kapoeta East Kapoeta South
Cove
rage
(%)
Counties
DPT3 Performance in Core Group supported counties from 2011-2014
Baseline
2014
(MOH Administrative Data)
Using resources in the polio eradication to support routine immunization
Outcome of the contributions of the community volunteers
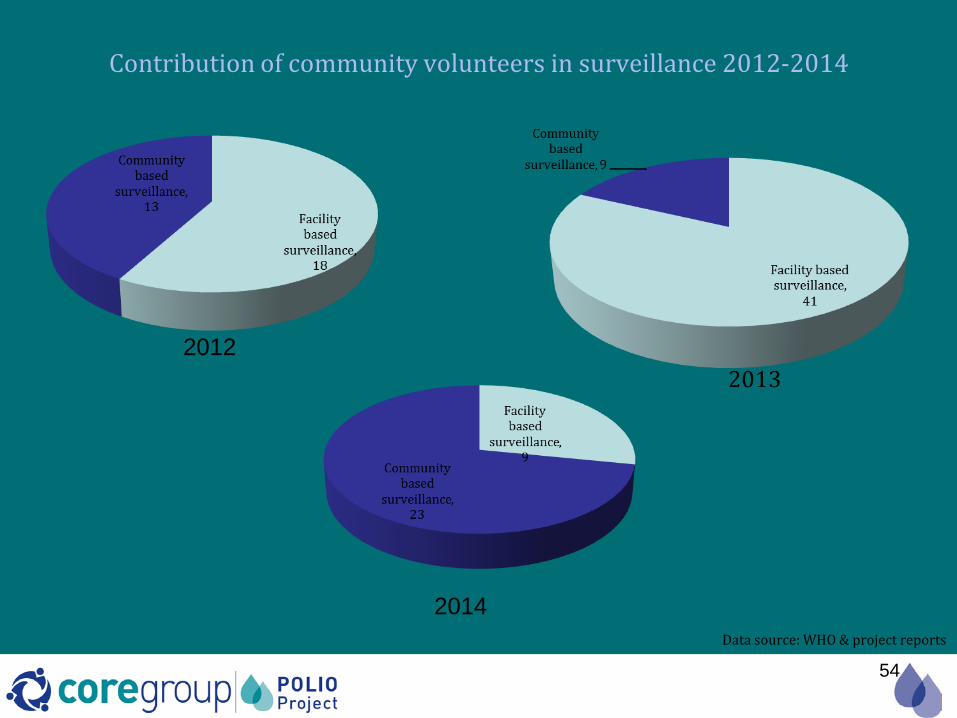
Contribution of community volunteers in surveillance 2012-2014
54
2012
2014 Data source: WHO & project reports

Monitoring of polio campaigns
• 224 independent monitors
• Reaching every town and village
• Focus on hard to reach areas-hard to reach communities.
• Report all missed areas to campaign supervisor-map ups
• Use information for planning
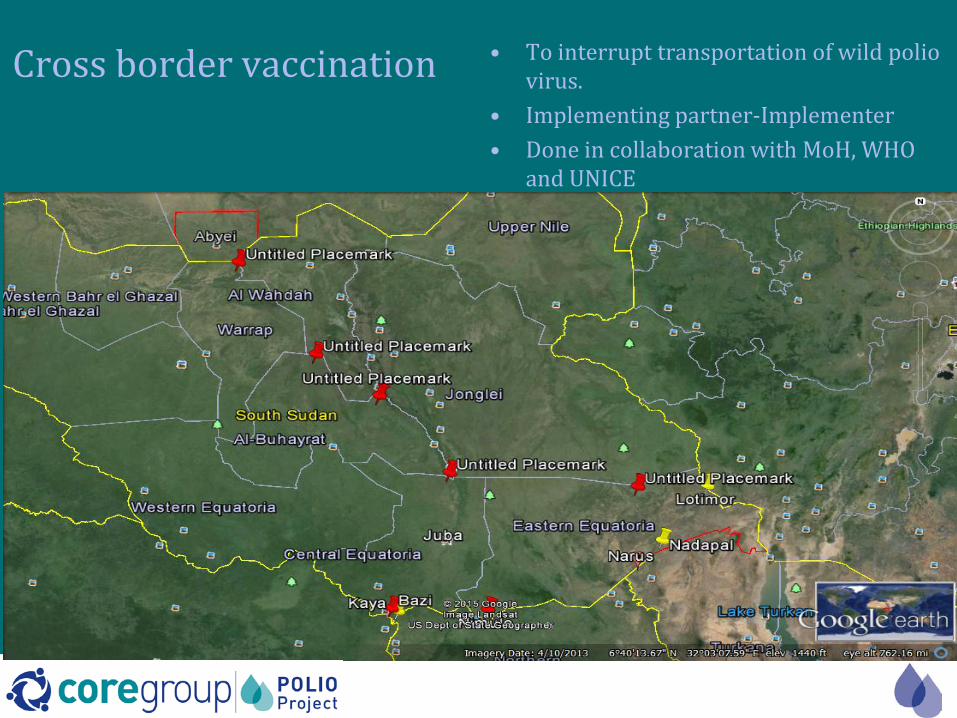
Cross border vaccination • To interrupt transportation of wild polio virus.
• Implementing partner-Implementer • Done in collaboration with MoH, WHO
and UNICE

Challenges
• Inadequate funding to strengthen the already improving services and scaling to other poorly performing counties
• Due to the level of poverty in the community, the expectation of pay among project volunteers
• Poor transport infrastructure- poor roads, flooding, inadequate transport means.
• Insecurity in the remote areas- arrest of volunteers in doing their work in some insecure areas.

Lessons learnt • Integration of the community volunteers’ activities into the
formal health system is critical for the success of the program.
• Collective planning with the community leaders, facility based health workers and volunteers results to ownership of the program
• Community volunteers play a very pivotal role in strengthening the health system through their engagement and participation.

Cont…..
• Working with community volunteers who hail from that community leads to a lot of trust resulting in acceptance of the program and improved uptake of vaccine which culminated in improvement in immunization coverage in most of the counties.
• Strong collaboration between community leaders, the local health authorities and presence of supporting partner on the ground

conclusion • Due to the weak health system in South Sudan resulting in
worsening health indicators, there is no doubt that involving community volunteers and linking them to the formal health system is important if we are to reach the unreached with lifesaving health interventions.

61
Questions?
Photo: Gatesfoundation.org

Reaching Border Communities for Polio Eradication in Horn of Africa
CORE Group Spring Meeting 2015 Virginia, USA
Bal Ram Bhui, CGPP HOA

Presentation Objectives
• To provide an overview of process of Cross Border Initiative for Polio Eradication in Horn of Africa
• To describe various tools for planning, reporting and monitoring.
• Progress, challenges and plans ahead

Outline
• Overview of PEI in HoA • Overview of cross border efforts for polio
eradication in HOA – Cross border issues in HoA for polio eradication – Cross border meeting for SIA in HoA
• Cross border initiative for polio eradication – CORE Group model for reaching hard reach/high
risk and mobile population in along borders
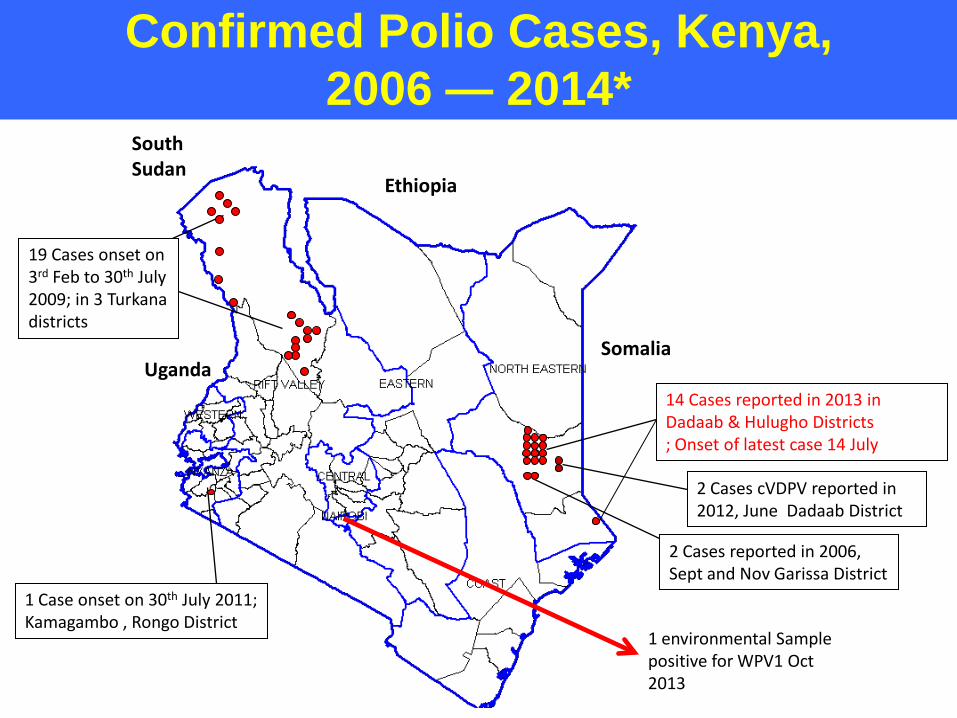
Confirmed Polio Cases, Kenya, 2006 — 2014*
South Sudan
Ethiopia
Somalia Uganda
19 Cases onset on 3rd Feb to 30th July 2009; in 3 Turkana districts
2 Cases reported in 2006, Sept and Nov Garissa District
1 Case onset on 30th July 2011; Kamagambo , Rongo District
14 Cases reported in 2013 in Dadaab & Hulugho Districts ; Onset of latest case 14 July
2 Cases cVDPV reported in 2012, June Dadaab District
1 environmental Sample positive for WPV1 Oct 2013
4/27/2015 66
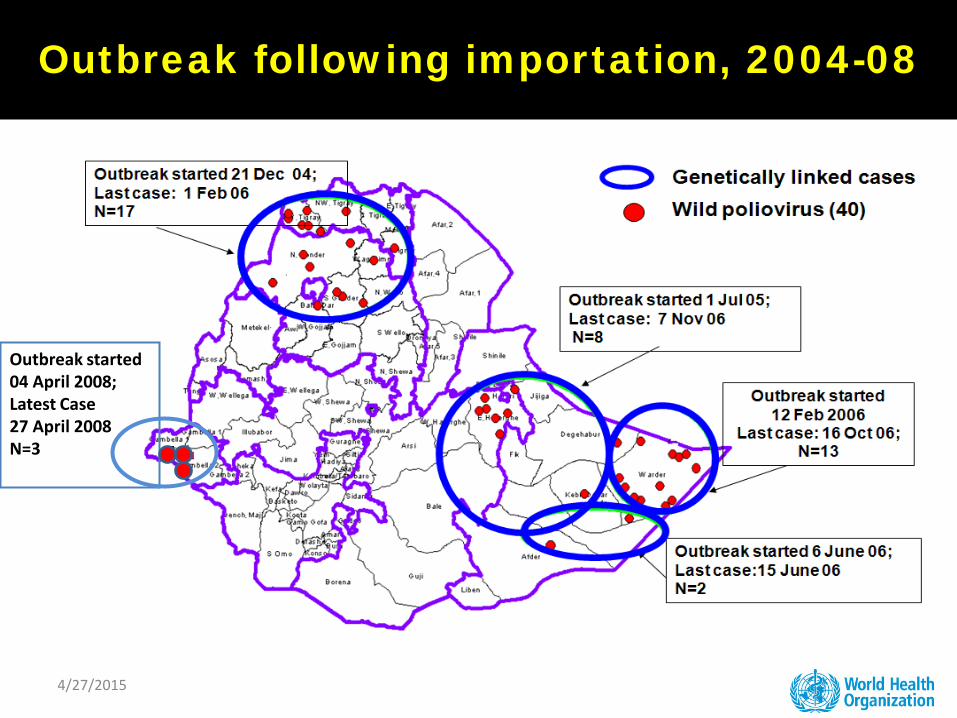
Outbreak following importation, 2004-08
Outbreak started 04 April 2008; Latest Case 27 April 2008 N=3

Somali Region WPV-1 Outbreak Affected Woredas
from July 2014 up to January 14

• The total polio cases during the 2008-09 epidemic were 64 cases – 24 cases in 2008 – 40 cases in 2009
• The last polio case in South Sudan was on 27/6/2009 (Aweil West).
• During the period June 2008 to December 2012 a number of 29 SIAs were conducted
2008 2009
19 Cases onset on 3rd Feb to 30th July 2009; in 3 Turkana districts
1 Case onset on 30th July 2011; Kamagambo , Rongo District
History of polio out break in HOA – 2008-2009 Outbreak in SSD
Exportation of the SSD outbreak to Kenya
(2009)

Border Population at Risk • The cross border community and population at high risk for
outbreak and transmission of infectious diseases including polio • Border communities share ecology, epidemiology, culture and
values • Borders are only politically divided • Borders are likely to be
– Hard to reach – Left out – Socio-economically disadvantaged
• Borders are porous, free movement • People move for trade, pastures, health care, education, cultural
reasons, recreation, migration, conflict and security reasons

Cross border meetings for polio eradication
• 2012 Cross border meetings of Ethiopia, Somalia, South Sudan, Sudan and Kenya
• Cross border meetings by CORE Group South Sudan with Ethiopia, Kenya, DRC, Uganda
• Achievements: – Awareness and commitment of MOH, increased – Synchronized SIAs along the borders
• Challenges: – Meeting was one time before SIA, no follow up – Action plan not implemented – No reporting, monitoring and evaluation – No plan to improve PEI efforts in border communities on
ongoing basis
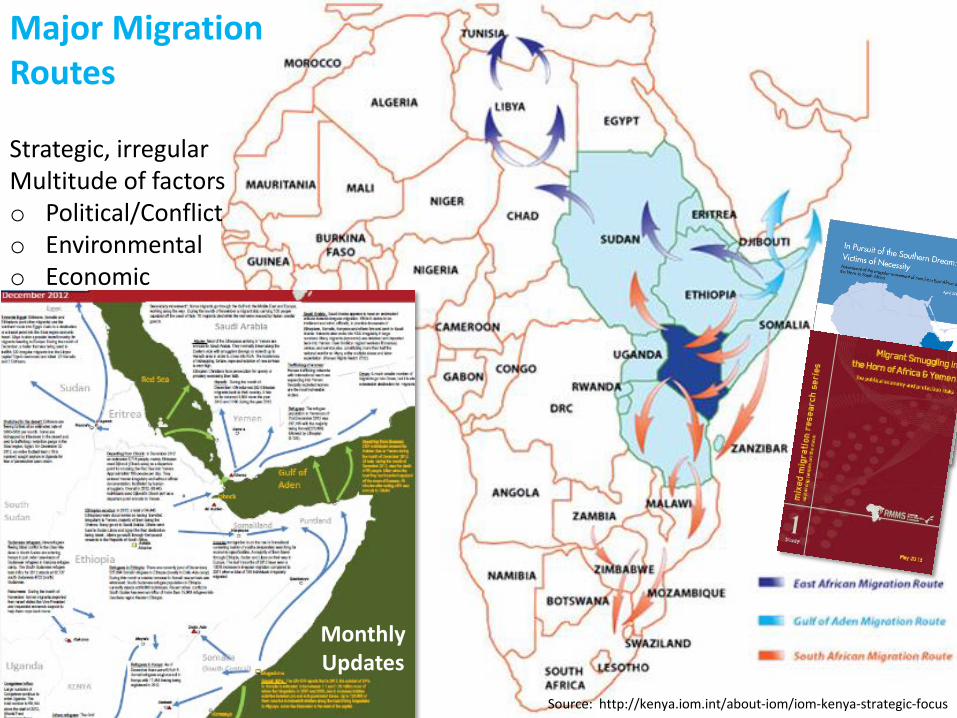
Source: http://kenya.iom.int/about-iom/iom-kenya-strategic-focus
Major Migration Routes Strategic, irregular Multitude of factors o Political/Conflict o Environmental o Economic
Monthly Updates

CORE Group in HoA
• HOA regional secretariat in Nairobi • CGPP Project in Ethiopia since 2001 • CGPP Project in South Sudan since 2010 • CGPP in Kenya and Somalia
– Kenya Border counties – Turkana, Marsabit, Wajir, Mandera, Garissa
– Nairobi – Lower Juba, Gedo, Mudug in Somalia – CORE Group NGOs and National NGOs implement the
project

Cross border initiative (CBI) for Polio Eradication
• What is CBI – Understanding about border
communities, border crossing points and transit hubs and addressing them for polio eradication internally as well as with border counterpart
– Initiative at operational border health authority levels
• Who are involved in CBI – National MOH – County government and health office – Local immigration and security
authorities – Polio Partners and NGOs
• Where is CBI institutionalized – Border between Kenya, Somalia,
Ethiopia, South Sudan and Uganda

Goal and Objectives of CBI • Goal: Contribute to global eradication by improving
population immunity in cross border communities and populations with effective AFP surveillance
• Objectives: Improve cross border collaboration between health, administrative authority of border regions and the partners to – Improve PEI efforts in border communities and populations – Improve coverage and synchronization of SIAs at cross border
points – Establish permanent vaccination points at major crossing points – Improve PEI efforts in transit hubs and routes – Improve communication and collaboration between border
health offices
CORE Group CBI approach
• Country internal approach – Situation assessment of polio eradication in border
health facilities and populations – Polio eradication action plan for cross border
communities and populations • Cross border joint approach
– Identification of populations and areas for cross border collaborations
– Joint action plan – Cross border health committee and TOR – Cross border planning and review meetings

Country internal approach • Situation assessment
– Profiling of border communities, crossing points, transit hubs – Mapping of border communities, crossing points, transit hubs – Capacity assessment of border health facilities – Micro planning for SIA, RI, AFP Surveillance for border areas
• Country action plan to address cross border issues for polio
eradication – Action plan to support border health facility improve SIA
coverage, Routine Immunization Coverage and AFP surveillance sensitivity
– Cross border health committee members designated – Regular review and reporting on implementation of action plan

Show Table data – CBI tools

1. List of Fixed posts, Villages, Markets, Nomadic/Pastoral camps and Border communities and crossing posts by health facility in a Location
NB: List ALL villages in each location with their target populations. Also list markets, seasonal camps (pastoralists, nomadic, etc.), schools, transports stations, re
1 LIBOI Hc-SALAT MOHAMMED 1 DAMAJALEY DISPENSARY.-EVANS ARIAM 1 HAMEY DISPENSARY-SAMUEL CHEPSAIG 1Health Facility (name) (Subsidiary) Health Facility (name) (Subsidiary) Health Facility (name) (Subsidiary) Health Facility (name) (Subsidiary
1.1 1.1 1.1 1.1
1 1.2 1.2 1
Village/Estate - Target populatioon 3484Village/Estate - Target population 925 Village/Estate - Target population 666 Village/Estate (Name/Target 1 Bula safaricom-190 1 Bula sheikh-75 1 Bula borehole-65 12 Bula makabul-210 2 Bula Tuhun-80 2 Bula banaan-70 23 Bula Sambule-220 3 Bula Daidei-90 3 Bula Primary-62 34 Bula Torotoro-210 4 Bula Hodhan-68 4 Bula labi-58 45 Bula Mohamed Zubeir-180 5 Bula Towfiq-74 5 Bula mosque-55 56 Bula Oji-90 6 Bula Primary-85 6 Bula camp-60 67 Bula Celtel-190 7 Bula Labatule-70 7 Bula Sheikh-52 78 Bula Sufi-215 8 8 Bula daidai-58 89 Bula Maseer-200 9 9 9
10 Bula Dana-230 10 10 1011 Bula hursan-210 11 11 1112 Bula Haji-174 12 12 1213 13 13 1314 14 14 1415 15 15 1516 16 16 16
Markets including supermarkets, transport stations, schools and religious places (Day and place): Markets (place & day) Markets (place & day) Markets (place & day)
1 Liboi Primary School 1 Damajaley market centre 1 Hamey market centre 12 Madina Academy 2 Damajaley Primary sch 2 Hamey Primary school 23 Liboi Airstrip 3 Damajaley mosque 3 Hamey animal watering point 34 Liboi Madrssa 4 Damajaley animal watering point 4 Hamey mosque5 Liboi Mosque 5 56 Liboi KDF camp 6 67 Liboi Market centre 7 7 4
Seasonal Settlements Seasonal Settlements / Hard-Reach Seasonal Settlements / Hard-Reach Seasonal Settlements / Hard-R1 Wardaklow-25 1 Abaq dam-10 1 Guba athey-28 12 Ali gabey-30 2 Gari gubane-12 2 Gadable-22 23 Welcadcad-30 3 Tarsis-18 3 34 4 Daryolle-13 4 45 5 Dobale dam-23 5 56 6 6 67 7 7 7
Hard to reach/high risk village/settlements
Hard to reach/high risk village/settlements
Hard to
Hard to reach/high risk village/settlements
Hard
Hard to reach/high risk village/settlements
1 Deg-elema-750 1 Magudo- 65 1 Deq-athey-70 12 Harhar-200 2 Aden santur-72 2 Homijo-65 23 Dat-quran-100 3 Ali dakane-60 3 34 Indatha Dam-30 4 Abdi sugow-110 4 45 5 5 56 6 6 67 7 7 7
Health Facility (name) (Responsible) Health Facility (name) (Responsible) Health Facility (name) (Responsible) Health Facility (name) (Responsible
Mapping of villages

Bordering country(ies): KENYA/SOMALIA Bordering location/districts: LIBOI DIVISION/DADAAB SUB COUNTYDOBLEY/HOSUNGOW
Date: 27/3/2015
Border country Name/area: SomaliSN Name of border
crossing/entry-exit points
Name of village along the border crossing points
Name of health facility that the crossing points belong to
Is crossing point formal or informal? 1-Formal, 0-Informal
Average number of people crossing the border in a day
How will this crossing point be covered during SIA? (A static vaccination team, mobile vaccination team designated for cross border points, none)
Name of border crossing/entry-exit points if different
Name of village along crossing points in other side of border
Name of health facility that the crossing points belong to in other side of border
How will this crossing point be covered during SIA? (A static vaccination team, mobile vaccination team designated for cross border points, none)
Comments
Deg-elema Deg -elema Liboi Hc 0 60 Mobile Deg- elema Deg- elema None
Coverage to be discussed with CB country/WHO
Harhar Harhar Liboi Hc 1 150 Mobile Dobley Dobley Dobley hospital
Coverage to be discussed with CB country/WHO
Magudo Magudo Damajaley disp 0 Mobile Magudo Magudo None
Coverage to be discussed with CB country/WHO
Aden santuir Aden santur Damajaley disp 0 10 Mobile Aden santur Aden santur None
Coverage to be discussed with CB country/WHO
Ali Dakane Ali Dakane Damajaley disp 0 10 Mobile Ali Dakane Ali Dakane None
Coverage to be discussed with CB country/WHO
Abdi sugow Abdi sugow Damajaley disp 0 30 Mobile Abdi sugow Abdi sugow None
Coverage to be discussed with CB country/WHO
Deq-athey Deq-athey Hamey Disp 0 70 Mobile Deg-athey Deg-athey None
Coverage to be discussed with CB country/WHO
Harmujo Homijo Hamey Disp 0 25 Mobile Hosungow Hosungow None
Coverage to be discussed with CB country/WHO
Total
1.2. INTERNATIONAL CROSS BORDER PLAN - Border crosing points
Kenyan villages covered by Kenyan teams are in Kenya's microplan. Other villages will be in border country's microplan
KENYA
Mapping of cross border communities

1.1. INTERNATIONAL CROSS BORDER PLAN - Border communities
Bordering country(ies): KENYA/SOMALIA Bordering location/districts: LIBOI /DAMAJALEY/HAMEY LOCATION
Date:
Border country NamSomalia
Kenyan villagesalong border
Name of Health Facility
Target Pop.(Polio SIAs)
Countrycovering
Date ofvaccinati
on
Border country's villages
to be coveredby Kenyan teams
Border Health facility name
Target Pop(Polio SIAs)
Kenyan Team ID
Date ofvaccinati
on
OPV required(doses)
LIBOI HEALTH CENTRE
Deg-elemaLIBOI HEALTH CENTRE
Kenya 20/4/15 Deg-elema
HarhaarLIBOI HEALTH CENTRE
Kenya 20/4/16 Dobley
Dat-quranLIBOI HEALTH CENTRE
Kenya 21/4/15
DAMAJALEY DISPENSARY
MagudoDAMAJALEY DISPENSARY
Kenya 20/4/15
Aden santurDAMAJALEY DISPENSARY
Kenya 20/4/16
Ali DakaneDAMAJALEY DISPENSARY
Kenya 21/4/15
Abdi sugowDAMAJALEY DISPENSARY
Kenya 21/4/16 Hosingow
HAMEY DISPENSARY
Deq-atheyHAMEY DISPENSARY
Kenya 20/4/15
HomijoHAMEY DISPENSARY
Kenya 21/4/16
Total
KENYA
Kenyan villages covered by Kenyan teams are in Kenya's microplan. Other villages will be in border country's microplan
Mapping of border crossing points

Cross border mapping

Social map of a border health facility

Profiling of border communities

Cross border joint approach
• Cross border initiative operation guide • Joint action planning workshop • Review, reporting and documentation of cross
border activities • Quarterly cross border health committee
meetings • Regular information sharing between border
county/district health office • Engagement of border immigration, security and
other border stakeholders

Implementation • Monthly meeting of cross border health committees on
each side • Joint quarterly meeting of cross border health committee • Semi-annual and annual review meetings • Implement and report on action plan
– Synchronization of vaccination at border crossing points – Actions to improve AFP surveillance of border health facility
catchment areas – Actions to improve routine immunization in border health
facility catchment areas – Permanent vaccination points – Regular communication between parties

Progress to date (1)
• Initiated in October 2014 as a process • Developed necessary assessment, planning and
reporting tools • Microplanning for cross border issue at border health
facility level initiated • Cross border Initiative Operation Guide developed • High level of commitment and support from MOH,
County Health Office, Immigration and Security offices • High level of commitment from polio Partners – WHO
and UNICEF and NGOs
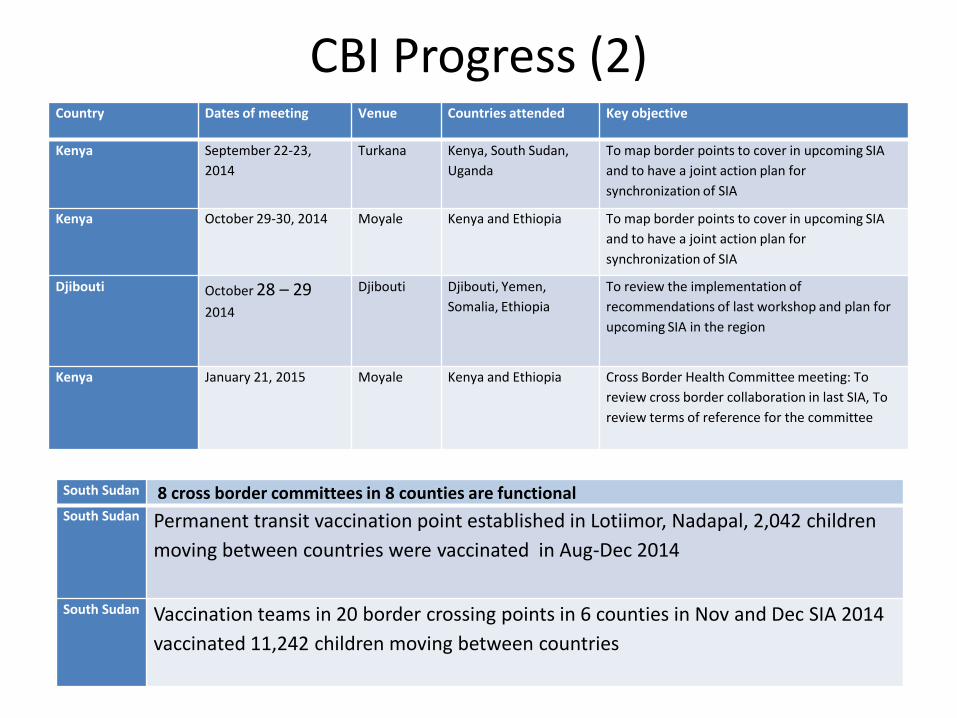
CBI Progress (2) Country Dates of meeting Venue Countries attended Key objective
Kenya September 22-23, 2014
Turkana Kenya, South Sudan, Uganda
To map border points to cover in upcoming SIA and to have a joint action plan for synchronization of SIA
Kenya October 29-30, 2014 Moyale Kenya and Ethiopia To map border points to cover in upcoming SIA and to have a joint action plan for synchronization of SIA
Djibouti October 28 – 29 2014
Djibouti Djibouti, Yemen, Somalia, Ethiopia
To review the implementation of recommendations of last workshop and plan for upcoming SIA in the region
Kenya January 21, 2015 Moyale Kenya and Ethiopia Cross Border Health Committee meeting: To review cross border collaboration in last SIA, To review terms of reference for the committee
South Sudan 8 cross border committees in 8 counties are functional South Sudan Permanent transit vaccination point established in Lotiimor, Nadapal, 2,042 children
moving between countries were vaccinated in Aug-Dec 2014
South Sudan Vaccination teams in 20 border crossing points in 6 counties in Nov and Dec SIA 2014 vaccinated 11,242 children moving between countries

Plans ahead • Plan to expand
– North Horr, Kenya between Kenya and Ethiopia – Mandera, Kenya between Kenya, Ethiopia and Somalia – South Central Zone, Somalia with Kenya
• Provide field support to county health offices for CBI through Sub Grants to NGOs
• Complete profiling and mapping of cross border communities, border crossing points and transit hubs.
• Improve SIA coverage, Synchronization of campaigns, routine immunization , and improved AFP surveillances in border communities
• Regular review and planning meetings on CBI internal and with cross border area
• Improve communication between cross border health facility and authorities
• Improve Polio Partners Collaboration on cross border initiative