reach registry slide kit - clinical trial results
TRANSCRIPT

Updated slide kit, February 2006
1
The REACH Registry
An International, Prospective Observational Study in Subjects at Risk of Atherothrombotic Events in an Outpatient Setting

Updated slide kit, February 2006
2
Outline
Background• Burden of Disease• Risk of Atherothrombosis
REACH Registry Background• Rationale and Objectives• Design
REACH Registry Baseline Results• High Prevalence of Polyvascular Disease• Undertreatment of Patients with Atherothrombosis Worldwide
REACH Registry Today and Beyond• Publications to Date• Upcoming Analyses and Data Availability• Participating Organizations and Scientific Committees

Updated slide kit, February 2006
3
Background
Updated slide kit, February 2006
4
Burden of Disease

Updated slide kit, February 2006
5
Stable angina
Thrombosis
1. Adapted from Libby P. Circulation 2001; 104: 365–372.2. Drouet L. Cerebrovasc Dis 2002; 13(Suppl 1): 1–6.
UA=unstable angina; MI=myocardial infarction; ACS=acute coronary syndrome; TIA=transient ischemic attack
UA MI
Ischemic stroke/TIA
Vascular death
ACS
Atherothrombosis – a Generalized and Progressive Disease Process1,2

Updated slide kit, February 2006
6
Aggregation of platelets into
a thrombus
Platelets
Endothelial cells
Platelets adhering to subendothelial space
Platelet thrombus
Normal platelets in flowing blood
Platelets adhering to damaged endothelium
and undergoing activation
Subendothelial space
1. Adapted from: Ferguson JJ. In: Ferguson JJ, Chronos N, Harrington RA (Eds).
Antiplatelet Therapy in Clinical Practice. London: Martin Dunitz; 2000: 15–35.
Major Role of Platelets in Atherothrombosis1
Updated slide kit, February 2006
7
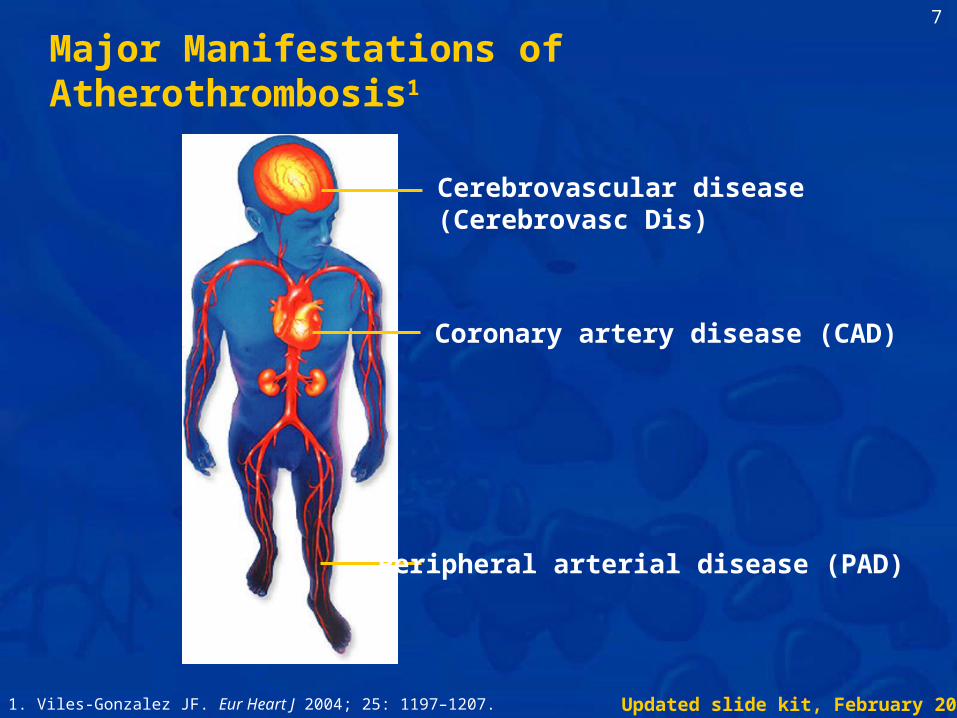
Major Manifestations of Atherothrombosis1
1. Viles-Gonzalez JF. Eur Heart J 2004; 25: 1197–1207.
Coronary artery disease (CAD)
Cerebrovascular disease (Cerebrovasc Dis)
Peripheral arterial disease (PAD)
Updated slide kit, February 2006
8
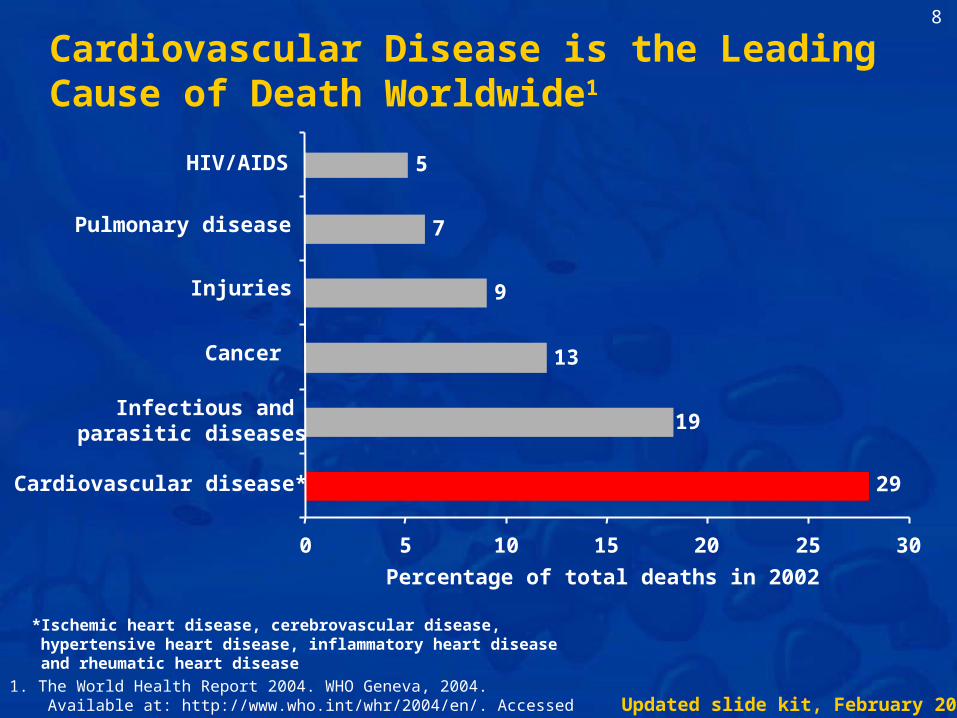
1. The World Health Report 2004. WHO Geneva, 2004. Available at: http://www.who.int/whr/2004/en/. Accessed January 2006.
29
19
13
9
7
5
0 5 10 15 20 25 30
Cardiovascular disease*
Infectious and parasitic diseases
Cancer
Injuries
Pulmonary disease
HIV/AIDS
Percentage of total deaths in 2002
*Ischemic heart disease, cerebrovascular disease, hypertensive heart disease, inflammatory heart disease and rheumatic heart disease
Cardiovascular Disease is the Leading Cause of Death Worldwide1

Updated slide kit, February 2006
9
Analysis of data from the Framingham Heart Study:Average remaining life expectancy for males aged 60 years
Healthy History of any cardiovascular
disease*
History of acute MI
History of stroke
1. Peeters A et al. Eur Heart J 2002; 23: 458466.
*Including coronary heart disease, cerebrovascular accident, congestive heart failure and intermittent claudication
0
4
8
12
16
20
Tim
e (y
ears
)
9.2 years7.7 years 12.0 years
Atherothrombosis Significantly Shortens Life Expectancy1

Updated slide kit, February 2006
10
Risk of Atherothrombosis
Updated slide kit, February 2006
11
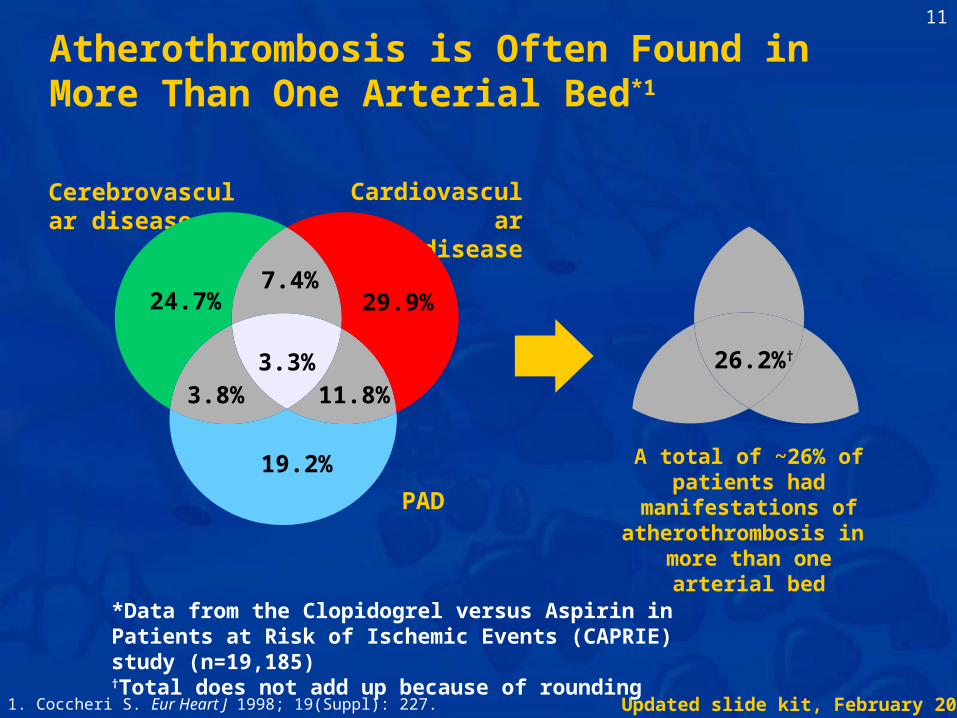
Cardiovasculardisease
Cerebrovascular disease
PAD
24.7%
3.8% 11.8%
29.9%
3.3%
7.4%
19.2%
*Data from the Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events (CAPRIE) study (n=19,185)†Total does not add up because of rounding
A total of ~26% of patients had manifestations of atherothrombosis in
more than one arterial bed
26.2%†
1. Coccheri S. Eur Heart J 1998; 19(Suppl): 227.
Atherothrombosis is Often Found in More Than One Arterial Bed*1

Updated slide kit, February 2006
12
Increased risk versus general population
MI Stroke
MI 5–7 X (includes death)3
3–4 X (includes TIA)1
Ischemic stroke 2–3 X (includes angina and sudden death*)1
9 X2
PAD 4 X (includes only fatal MI and other CHD death†)4
2–3 X (includes TIA)2
*Sudden death defined as death documented within one hour and attributed to coronary heart disease (CHD)†Includes only fatal MI and other CHD death; does not include non-fatal MI
1. Kannel WB. J Cardiovasc Risk 1994; 1: 333–339.2. Wilterdink JI et al. Arch Neurol 1992; 49: 857–863.3. Adult Treatment Panel II. Circulation 1994; 89: 1333–1363.4. Criqui MH et al. N Engl J Med 1992; 326: 381–386.
Patients with Previous Atherothrombotic Events are at Increased Risk of Further Events

Updated slide kit, February 2006
13
1. Bhatt DL et al. Am Heart J 2004; 140: 263–268.
Increased risk of atherothrombotic events
Independent risk factors:
Risk Factors can Create High Risk of MI and Stroke, Even With No History of These Events1
• Male aged 65 yearsor female aged 70 years
• Current smoking>15 cigarettes/day
• Type 1 or 2diabetes
• Hypercholesterolemia• Diabetic nephropathy• Hypertension• ABI <0.9 in either
leg at rest• Asymptomatic carotid
stenosis 70%• Presence of at least
one carotid plaque

Updated slide kit, February 2006
14
*Risk factors: hypertension; hypercholesterolemia; dyslipidemia; diabetes; smoking; left ventricular hypertrophy
1. Kannel WB. Hypertens Res 1995; 18: 181–196.
0
10
20
30
40
50
60
70
0 1 2 3 4 5 6
Estim
ated
10-
yea r
C
HD
rat e
(%)
Number of risk factors*
MenWomen
Risk of CHD Increased in Patients with Multiple Risk Factors1
Updated slide kit, February 2006
15
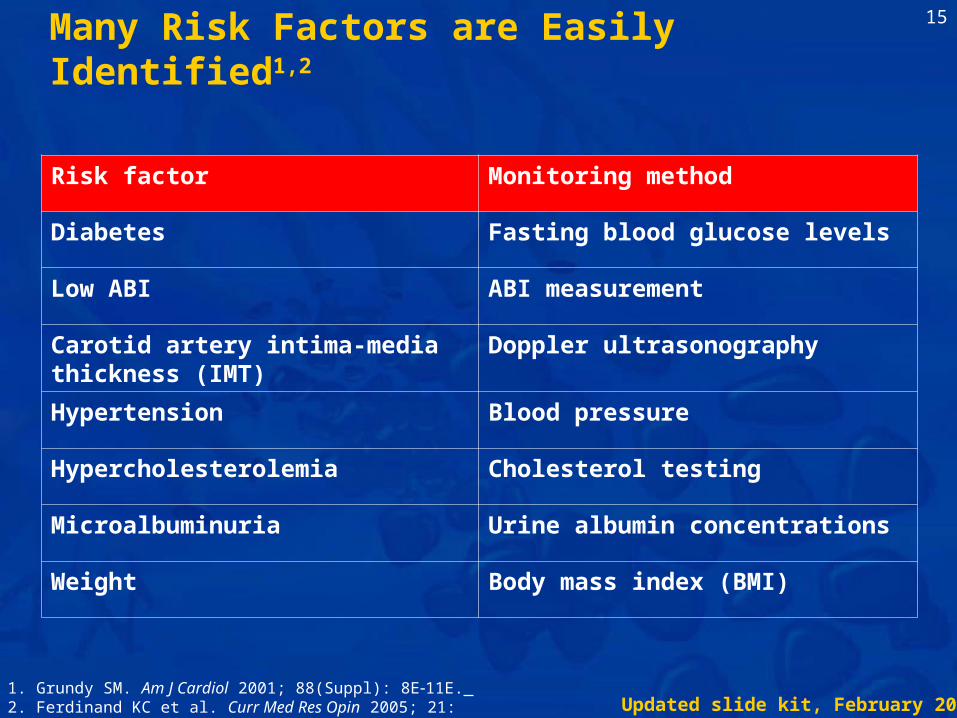
Many Risk Factors are Easily Identified1,2
Risk factor Monitoring method
Diabetes Fasting blood glucose levels
Low ABI ABI measurement
Carotid artery intima-media thickness (IMT)
Doppler ultrasonography
Hypertension Blood pressure
Hypercholesterolemia Cholesterol testing
Microalbuminuria Urine albumin concentrations
Weight Body mass index (BMI)
1. Grundy SM. Am J Cardiol 2001; 88(Suppl): 8E11E. 2. Ferdinand KC et al. Curr Med Res Opin 2005; 21: 10911097.

Updated slide kit, February 2006
16
REACH Registry: Background

Updated slide kit, February 2006
17
REACH Registry: Rationale and Objectives
Updated slide kit, February 2006
18
REACH Registry: a Global Observational Study of around 68,000 Patients in 44 Countries Who Are at High Risk of Atherothrombosis1
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
Rationale• Evaluation of atherothrombosis is still limited because
previous surveys have:1. Focused on studying specific risk factors, or ‘single’
manifestations of the disease (e.g. heart disease)2. Focused mostly on hospitalized or hospital-treated patients
with stringent inclusion criteria3. Been conducted in either North America or Europe

Updated slide kit, February 2006
19
REACH Registry: a Global Observational Study of around 68,000 Patients in 44 Countries Who Are at High Risk of Atherothrombosis1
The REACH Registry should have these added advantages:• The most globally inclusive and geographically extensive
registry of patients at high risk of heart attack and stroke• Includes a broad spectrum of patient types – with or without a
previous history of disease• Provides data from a ‘real world’ setting, reflecting daily
practice
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.

Updated slide kit, February 2006
20
Primary objectives are:
Compile international data set to extend knowledge of atherothrombotic risk factors and ischemic events in the outpatient setting
Provide a better understanding of the prevalence and clinical consequences of atherothrombosis in a wide range of patients from different parts of the world
Important intermediate investigations have included:
Assess use of risk management strategies and 18- to 24-month outcomes in a broad outpatient population encompassing various geographic regions and physician specialties
REACH Registry: Objectives1
1. Ohman EM et al, on behalf of the REACH Registry Investigators.Am Heart J 2006; in press.

Updated slide kit, February 2006
21
Improving the Management of Cardiovascular Disease Risk
Risk factor Recommendation
Blood pressure <140/90 mm Hg1,2 (<130/80 mm Hg for patients with diabetes13)
Total cholesterol <200 mg/dL/<11.1 mmol/L1–4
Triglyceride <150 mg/dL (<1.7 mmol/L)3,4
Diabetes management
Normal fasting plasma glucose (<110 mg/dL [<6.0 mmol/L])1,2 and near-normal HbA1c levels (≤6.1%2 or <7.0%1,3)
Smoking Complete cessation13
Dietary intake An overall healthy eating pattern13
Physical activity Moderate intensity physical activity for 3045 minutes at least 35 times per week13
Weight management
Achieve and maintain desirable weight14 (BMI 18.5–24.9 kg/m2).1 When BMI is ≥25 kg/m2, waist circumference at iliac crest level ≤102 cm (≤40 inches) in men and ≤88 cm (≤35 inches) in women1,2
1. Pearson TA et al. Circulation 2002; 106: 388391.2. De Backer G et al. Eur Heart J 2003; 24: 16011610.3. American Diabetes Association. Diabetes Care 2005; 28: S4S36.4. Adult Treatment Panel III. National Institutes of Health,
Publication No. 02-5215, September 2002.
Guideline recommendations by which REACH Registry patients are benchmarked

Updated slide kit, February 2006
22
REACH is the most geographically and ethnically diverse atherothrombotic population yet surveyed, providing the most accurate view to date of burden of disease and long-term prognosis for patients at high risk for atherothrombotic events
With up to four years of clinical follow-up, the REACH Registry will provide long-term insights into real-world event rates, treatment
patterns and outcomes help to improve assessment and management of stroke, heart
attack and associated risk factors
What do we hope the REACH Registry will achieve?

Updated slide kit, February 2006
23
REACH Registry: Design

Updated slide kit, February 2006
24
*Timelines are for worldwide participation; local timelines will be shorter
Baseline Follow-up at 12 3 months
Follow-up at 24 3 months
REACH Registry extension
REACH Registry extension
Timing* Dec 2003 to June 2004
From baseline time
Last follow-up March 2006
Sept 2006 to March 2007
Sept 2007 to March 2008
Required Data
Subject Data Form:
Section 1
Subject Data Form: Section
2(progression
since baseline)
Subject Data Form: Section 3
(progression since lastfollow-up)
Subject Data Form: Section 4
(progression since lastfollow-up)
Subject Data Form: Section 5
(progression since lastfollow-up)
Patient details, history and
clinical examination
Regular medicationsEmployment
status
Clinical outcomesVascular interventionsRegular medicationsEmployment status
REACH Registry Timeline

Updated slide kit, February 2006
25
Must include:
Signedwritten
informedconsent
Patients aged≥45 years
At least of four criteria1
1. Documented cerebrovascular diseaseIschemic stroke or TIA
2. Documentedcoronary diseaseAngina, MI, angioplasty/stent/bypass
3. Documented historicalor current intermittentclaudication associatedwith ABI <0.9
4. At least atherothrombotic risk factors3
1. Male aged 65 yearsor female aged 70 years
2. Current smoking>15 cigarettes/day
3. Type 1 or 2diabetes
4. Hypercholesterolemia5. Diabetic nephropathy6. Hypertension7. ABI <0.9 in either
leg at rest8. Asymptomatic carotid
stenosis 70%9. Presence of at least
one carotid plaque
REACH Registry Inclusion Criteria1
1. Ohman EM et al, on behalf of the REACH Registry Investigators.Am Heart J 2006; in press.

Updated slide kit, February 2006
26
REACH Registry Exclusion Criteria1
• Anticipated difficulty in patient returning for follow-up visit
• Patient is currently hospitalized
• Patient is currently participating in a clinical trial
1. Ohman EM et al, on behalf of the REACH Registry Investigators.Am Heart J 2006; in press.

Updated slide kit, February 2006
27
Participating physicians
Pre-defined at start of Registry
Based on local practice population• General practitioners (GPs), specialists
Mainly office-based, some hospital representation
Representative of:• Local environment• Country geography
How were they selected?
What is their profile?
1. Ohman EM et al, on behalf of the REACH Registry Investigators.Am Heart J 2006; in press.
Physician Selection: Reflection of Each Country’s Management of Cardiovascular Risk1

Updated slide kit, February 2006
28
Patients
Recruitment at each site
Maximum per site determined at local level (subject to central guidelines)
Within overall Registry timelines
Patient inclusion criteria• Documented atherothrombotic disease, or with at least 3
atherothrombotic risk factors
Real-life setting
How were they selected?
What is their profile?
1. Ohman EM et al, on behalf of the REACH Registry Investigators.Am Heart J 2006; in press.
Patient Selection: Patients Fitting Inclusion Criteria1

Updated slide kit, February 2006
29
REACH Registry:Baseline Results
Data shown may differ slightly from published abstractsowing to a subsequent database lock
Updated slide kit, February 2006
30
Aims of the Baseline Analysis1
Aim:• To determine whether atherosclerosis risk factor prevalence
and treatment would demonstrate comparable patterns in many countries around the world
Conclusion:• Classic cardiovascular risk factors are consistent and common,
but are largely undertreated and undercontrolled in many regions of the world
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.

Updated slide kit, February 2006
31
REACH Registry: Conclusions From Baseline
Cardiovascular risk profiles are common and consistent across different geographic locations and patient types:1
• Treatment goals are consistently not achieved in all patient types worldwide
• Established therapies are consistently underused in high-risk populations
• Women are undertreated despite commonly having more severe disease2
The REACH Registry patients with PAD have:3
• A high prevalence of concomitant disease in other vascular beds• Multiple risk factors for atherothrombosis, including pre-diabetes and
undiagnosed diabetes• Underutilization of appropriate medications to treat cardiovascular risk
The REACH Registry patients with cerebrovascular disease have:4
• A high prevalence of multiple risk factors for atherothrombosis and disease in other vascular beds
• Underutilization of appropriate medications1. Bhatt DL et al, on behalf of the REACH Registry Investigators. JAMA 2006; 295(2):180-189.2. Steg PG et al. Eur Heart J 2005; 26(Suppl): Abstract 1642. 3. Bhatt DL et al. J Am Coll Cardiol 2005; 45(3 Suppl): Abstract 1127–1196.4. Röther J et al. International Stroke Conference 2005; late breaking abstract.

Updated slide kit, February 2006
32
Australia: 2,872
Latin America: 1,931Brazil: 441Chile: 253Mexico: 899Interlatina†: 338
Middle East: 846Israel: 379Kingdom of Saudi Arabia: 198Lebanon: 120United Arab Emirates: 149
Europe: 23,542Austria: 1,588 Lithuania: 99Belgium: 383 The Netherlands: 324Bulgaria: 996 Portugal: 218Denmark: 422 Romania: 2,009Finland: 311 Russia: 999France: 4,592 Spain: 2,515Germany: 5,521 Switzerland: 695Greece: 699 Ukraine: 596Hungary: 957 United Kingdom: 618
North America: 27,746Canada: 1,976USA: 25,770
Thailand: 515Taiwan: 1,057South Korea: 505Singapore: 880Philippines: 1,039Malaysia: 525
Indonesia: 499Hong Kong: 175China: 708Asia: 10,951
Japan: 5,048
†Interlatina includes Panama, Costa Rica, Dominican Republic, Ecuador, Guatemala and Peru
A Large and Far-Reaching International Survey of Atherothrombosis*1
*Data shown may differ slightly from published abstracts owing to a subsequent database lock.
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.

Updated slide kit, February 2006
33
North AmericaEuropeAsia (incl. Japan)AustraliaLatin AmericaMiddle East
40.8%
2.8%
16.3%
4.2%
34.6%
1.2%
Geographic location of patients included in the initial analysis1
*Data shown may differ slightly from published abstracts owing to a subsequent database lock.
Broad Geographic Representation*1
1. Ohman EM et al, on behalf of the REACH Registry Investigators.Am Heart J 2006; in press.

Updated slide kit, February 2006
34
70 67 6863 66 65
73 7062 65
7267
7467 66
74
0
20
40
60
80
100
NorthAmerica
(n=20,750)
LatinAmerica(n=1,681)
WesternEurope
(n=15,053)
EasternEurope
(n=5,375)
MiddleEast
(n=718)
Asia(n=5,137)
Australia(n=2,567)
Japan(n=4,218)
Mean age (years)Male (%)
*Symptomatic refers to patients with documented CAD, Cerebrovasc Dis and/or PAD; data shown may differ slightly from published abstracts owing to a subsequent database lock.
Age and Gender of the Symptomatic Baseline Population*1
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
Age and Gender, Symptomatic Population(years, % of symptomatic population)1

Updated slide kit, February 2006
35
4338 34
26
4941
25
39
8477 78
8581 80
7671
82
59
72
51
81
56
78
45
0
20
40
60
80
100
NorthAmerica
(n=20,750)
LatinAmerica(n=1,681)
WesternEurope
(n=15,053)
EasternEurope
(n=5,375)
MiddleEast
(n=718)
Asia(n=5,137)
Australia(n=2,567)
Japan(n=4,218)
Diabetes (%)Hypertension (%)Hypercholesterolemia (%)
Classic Cardiovascular Risk Factors are Consistent and Common within the Symptomatic REACH Registry Baseline Population*1
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
Risk Factor Prevalence, Symptomatic Population(% of symptomatic population)1
*Symptomatic refers to patients with documented Coronary artery, Cerebro and/or Peripheral Arterial Disease; data shown may differ slightly from published abstracts owing to a subsequent database lock.

Updated slide kit, February 2006
36
69 66 69 65 68 6773 70
4741
56
44
6150
5549
0
20
40
60
80
100
NorthAmerica(n=6,996)
LatinAmerica(n=250)
WesternEurope
(n=2,833)
EasternEurope(n=281)
MiddleEast
(n=128)
Asia(n=766)
Australia(n=305)
Japan(n=830)
Mean age (years)Male (%)
*Data shown may differ slightly from published abstracts owing to a subsequent database lock.
Age and Gender of the Multiple Risk Factor Population at Baseline*1
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
Age and Gender, Multiple Risk Factor Population(years, % of MRF population)1

Updated slide kit, February 2006
37
77 8070
53
71
87 84 8793 89 92 94 94
8883
73
89
7177
68
8777
94
65
0
20
40
60
80
100
120
NorthAmerica(n=6,996)
LatinAmerica(n=250)
WesternEurope
(n=2,833)
EasternEurope(n=281)
MiddleEast
(n=128)
Asia(n=766)
Australia(n=305)
Japan(n=830)
Diabetes (%)Hypertension (%)Hypercholesterolemia (%)
*Data shown may differ slightly from published abstracts owing to a subsequent database lock.
Classic Cardiovascular Risk factors are Consistent and Common within the Multiple Risk Factor REACH Registry Baseline Population*1
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
Risk Factor Prevalence, Multiple Risk Factor Population(% of MRF population)1

Updated slide kit, February 2006
38
43%
29%
13%
2% 1%9%
2%1%
General practitionersInternistsCardiologistsNeurologistsAngiologistsGeneral surgeonsEndocrinologistsOther expertise
REACH Registry Investigators by specialty (% of total)1
*Data shown may differ slightly from published abstracts owing to a subsequent database lock.
1. Ohman EM et al, on behalf of the REACH Registry Investigators.Am Heart J 2006; in press.
Primary Care Practitioners (GPs and internists) Formed the Majority of REACH Registry investigators

Updated slide kit, February 2006
39
High Prevalence of Polyvascular Disease(Disease in More Than One Arterial Bed)

Updated slide kit, February 2006
40
~ 1/4 of the 40,258 patients with CAD also have atherothrombotic disease in other arterial territories
~ 1/4 of Patients with CADHave Polyvascular Disease1
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
Coronary Artery Dis
Periph Art Disease
4.7%
8.4%
1.6% Cerebro-vascular
RISK FACTORS ONLY
44.6%
(%s are of total population)1
Patients with CAD = 59.3% of the REACH Registry population

Updated slide kit, February 2006
41
~ 2/5 of the 18,843 patients with Cerebrovascular Disease also haveatherothrombotic disease in other arterial territories
RISK FACTORS ONLY
8.4%
1.6%
1.2%
~ 2/5 of Patients with Cerebrovascular Disease Have Polyvascular Disease1
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
16.6%
Patients with Cerebrovasc Dis = 27.8% of the REACH Registry population
(%s are of total population)1
Coronary Artery Dis
Cerebro-vascular
Periph Art Disease

Updated slide kit, February 2006
42
~ 3/5 of the 8,273 patients with PAD also haveatherothrombotic disease in other arterial territories
RISK FACTORS ONLY
1.2%4.7%
1.6%
~ 3/5 of Patients with Symptomatic PADHave Polyvascular Disease1
4.7%
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
Patients with PAD = 12.2% of the total REACH Registry
population
(%s are of total population)1
Coronary Artery Dis
Cerebro-vascular
Periph Art Disease

Updated slide kit, February 2006
43
A Large Minority had Polyvascular Disease in the REACH Registry*1
1.61.2
4.78.4
4.716.6
44.6
18.3
15.9
65.9
0 10 20 30 40 50 60 70
Multiple Risk Factors
CAD + Cerebro + PADCerebro + PAD
CAD + PADCAD + Cerebro
OverallPolyvascular Disease
PAD AloneCerebro Alone
CAD AloneOverall
Single Arterial Bed
Patients (%)*Data shown may differ slightly from published abstracts owing to a subsequent database lock.
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
Prevalence of disease in arterial beds(% of total)1
Updated slide kit, February 2006
44
Undertreatment of Patients with Atherothrombosis Worldwide

Updated slide kit, February 2006
45
Undertreatment of Risk Factorsin Patients Worldwide*1
159
65 64
344344 43
17
40
28
5343
17
6048
21
56
15 13
52
24
7
56
0
20
40
60
80
100
Elevated bloodpressure (≥140/90 mm
Hg)
Elevated cholesterol(≥200 mg/dL)
Continued smoking (≥5cigarettes/d)
Patie
nts
not a
chie
ving
targ
et (%
)
North AmericaLatin AmericaWestern EuropeEastern EuropeMiddle EastAsiaAustraliaJapan
*Data shown may differ slightly from published abstracts owing to a subsequent database lock.
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
Patients not achieving target(% of regional population)1

Updated slide kit, February 2006
46
1418 18
46
19
39
3024
44
36
19
28
0
10
20
30
40
50
60
CAD (n=40,258) Cerebrovasc Dis(n=18,843)
PAD (n=8,273) Multiple RiskFactors (n=12,389)
Patie
nts
not r
ecei
ving
pro
ven
ther
apy
(%)
Antiplatelets Lipid-lowering Statin
*Data shown may differ slightly from published abstracts owing to a subsequent database lock.
Established Therapies are Consistently Underused in All Patient Types*1
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
Patients not receiving therapy(% of subpopulation)1

Updated slide kit, February 2006
47
*Data shown may differ slightly from published abstracts owing to a subsequent database lock; **Symptomatic refers to patients with documented CAD, Cerebrovasc Dis and/or PAD
High Prevalence of Overweight and Obesity in Most Regions*1
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
NorthAmerica
LatinAmerica
WesternEurope
EasternEurope
MiddleEast
Asia Australia Japan
Perc
ent o
f pop
ulat
ion
BMI <25BMI 25-<30BMI 30-<35BMI 35-<40BMI ≥40
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
Variation of overweight and obesity in the symptomatic population**(% of regional population)1

Updated slide kit, February 2006
48
*Data shown may differ slightly from published abstracts owing to a subsequent database lock.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
NorthAmerica
LatinAmerica
WesternEurope
EasternEurope
MiddleEast
Asia Australia Japan
Perc
ent o
f pop
ulat
ion
BMI <25BMI 25-<30BMI 30-<35BMI 35-<40BMI ≥40
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
Variation of Overweight and Obesity in theMultiple Risk Factor REACH Registry Population
(% of regional population)1
Overweight and Obesity Highly Prevalent in Multiple Risk Factor Patients in Most Regions*1

Updated slide kit, February 2006
49
44.2
66.7
24.5
81.0
0
20
40
60
80
100
Diabetes Hypercholesterolemia Current smoker Hypertension
Patie
nts†
(%)
†Of the 8,273 patients with symptomatic PAD, the mean age was 69.2 years and 70.7% were male
*Data shown may differ slightly from published abstracts owing to a subsequent database lock.
High Prevalence of Concomitant Risk Factors in Patients with Symptomatic PAD*1
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
Prevalence of risk factors in the PAD population(% of subpopulation)1

Updated slide kit, February 2006
50
97.485.6 82.5 80.9
94.181.8 82.2
61.3
92.481.7 85.6
70.0
0
20
40
60
80
100
Antihypertensives Antiplatelets Oral antidiabeticagents
Lipid-loweringtherapyPa
tient
s re
ceiv
ing
prov
en th
erap
y (%
)
CAD only population CVD only population PAD only population
*Data shown may differ slightly from published abstracts owing to a subsequent database lock.
PAD Patients are Less Likely than Other Patients to Use Established Therapies*1
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
For antihypertensives, % is of pts diagnosed hypertension or elevated blood pressure at initial examination;For oral antidiabetics, % is of pts with history of diabetes or elevated blood glucose at initial examination
Patients receiving established therapy(% of patients)1

Updated slide kit, February 2006
51
80.3 77
38.329.9
13
83.3
58.2
37.4
23.7
14.3
81
66.7
44.2
23.8 24.5
0
20
40
60
80
100
Treatedhypertension
Treated hyper-cholesterolemia
Treated diabetes Obesity (BMI ≥30) Current smoker
Patie
nts
(%)
CAD only populationCVD only populationPAD only population
Risk factors are consistently found across all disease sub-populations*1
1. Bhatt DL et al, on behalf of the REACH Registry Investigators.JAMA 2006; 295(2): 180-189.
*Data shown may differ slightly from published abstracts owing to a subsequent database lock.
Risk Factor Prevalence, By Sub-Population(% of MRF population)1

Updated slide kit, February 2006
52
REACH Registry: Today and Beyond

Updated slide kit, February 2006
53
Publications to Date

Updated slide kit, February 2006
54
REACH Registry Publications Abstracts (I)
Title Lead author
Citation/conference
Undertreatment of atherothrombotic patients worldwide: baseline data from the REACH Registry
Steg PG J Am Coll Cardiol 2005; 45(3 Suppl): Abstract 1070–
121Risk profile and undertreatment of peripheral arterial disease 7,013 patients from the international REACH Registry
Bhatt D J Am Coll Cardiol 2005; 45(3 Suppl): Abstract 1127–
1196Worldwide data from 15,332 stroke patients in 2004 the REACH Registry
Röther J International Stroke Conference 2005; late
breaking abstractSecondary prevention and undertreatment in 16,901 cerebrovascular patients worldwide: data from the REACH Registry
Röther J Cerebrovasc Dis 2005; 19(Suppl 2): Abstract
Undertreatment of women with atherothrombosis: results from the worldwide REACH Registry
Steg PG Eur Heart J 2005; 26(Suppl): Abstract 1642
Correct as of 16th February 2006

Updated slide kit, February 2006
55
REACH Registry Publications Abstracts (II)
Title Lead author
Citation/conference
The prevalence of obesity in the international REACH Registry - a truly global epidemic with the United States leading the world
Bhatt D Eur Heart J 2005; 26(Suppl): Abstract 3925
Attained educational level, hypertension and hypercholesterolemia in persons with atherothrombosis: the experience of >48,000 patients from the international REACH Registry
Wilson PW Eur Heart J 2005; 26(Suppl): Abstract 447
Comparison of risk factors between stroke and transient ischemic attack patients: observations from the international REACH Registry
Röther J World Congress of Neurology 2005 oral
presentationRenal insufficiency is frequent and undertreated among outpatients at high risk of atherothrombotic events: lessons from the REACH Registry
Dumaine R AHA 2005 oral presentation
Quality of secondary prevention: a comparison between stroke and transient ischemic attack (TIA) patients
Röther J AHA-Stroke 2006 poster presentation
Correct as of 16th February 2006

Updated slide kit, February 2006
56
REACH Registry Publications Papers
Title Lead author
Citation
Atherothrombosis and stroke - a lot more to know! Röther J Cerebrovasc Dis 2005;20(2):139-40
Estimating the risk for atherothrombosis – are current algorithms sufficient?
Wilson P Eur J Cardiovasc Prev Rehabil 2005;12(5):427-32
The REduction of Atherothrombosis for Continued Health (REACH) Registry: An international, prospective, observational investigation in subjects at risk for atherothrombotic events – study design
Ohman EM Am Heart J 2006; In Press
International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis
Bhatt D JAMA 2006;295(2):180-9
Correct as of 16th February 2006

Updated slide kit, February 2006
57
Upcoming Analyses and Data Availability
Preliminary 1-year results from participating countriesare available at: www.REACHRegistry.org
Updated slide kit, February 2006
58
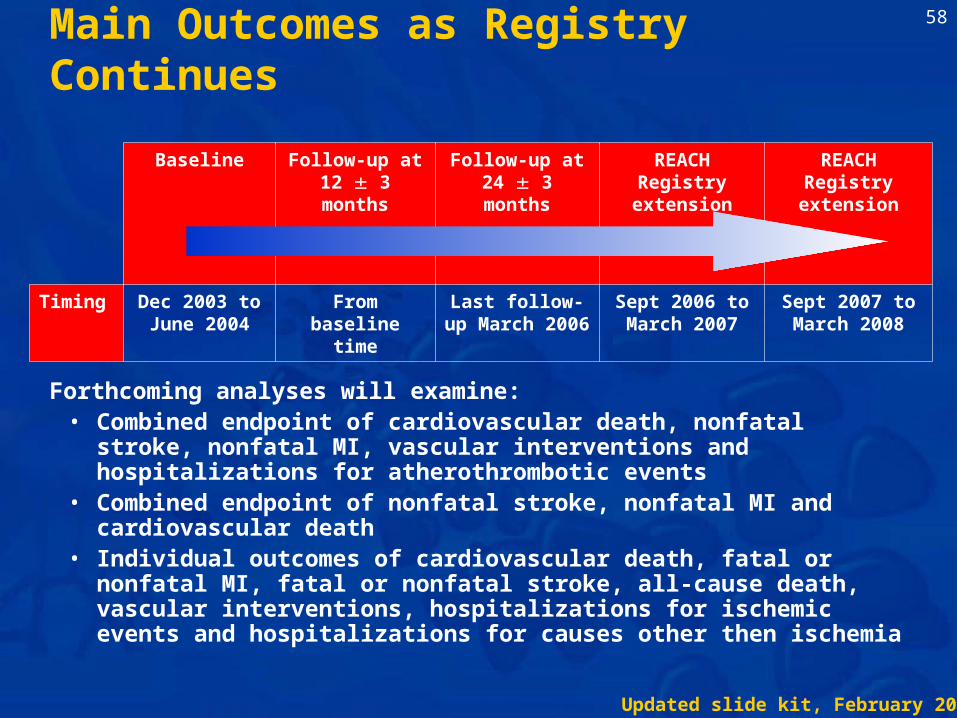
Main Outcomes as Registry Continues
Baseline Follow-up at 12 3 months
Follow-up at 24 3 months
REACH Registry extension
REACH Registry extension
Timing Dec 2003 to June 2004
From baseline time
Last follow-up March 2006
Sept 2006 to March 2007
Sept 2007 to March 2008
Forthcoming analyses will examine:• Combined endpoint of cardiovascular death, nonfatal stroke, nonfatal
MI, vascular interventions and hospitalizations for atherothrombotic events
• Combined endpoint of nonfatal stroke, nonfatal MI and cardiovascular death
• Individual outcomes of cardiovascular death, fatal or nonfatal MI, fatal or nonfatal stroke, all-cause death, vascular interventions, hospitalizations for ischemic events and hospitalizations for causes other then ischemia

Updated slide kit, February 2006
59
Accepted Abstracts
Title Lead author
Conference/Type
Better Guideline Compliance with Medical Therapy seen in Patients with Prior Coronary Revascularization : Results from the REduction of Atherothrombosis for Continued Health (REACH) Registry
Cannon C ACC 2006Oral presentation
REduction in Atherothrombosis for Continued Health (REACH) Registry results: 1-year cardiovascular event rates in a global contemporary registry of over 68,000 outpatients with atherothrombosis
Steg PG ACC 2006Late-breaker
"Global" Risk Factors and Treatment Intensity in Elderly Patients with Atherosclerosis: The Experience of the International REACH Registry
Hirsch AT ACC 2006Poster
Risk factor control among patients with diabetes mellitus in Europe and the rest of the world: the experience of the REACH Registry
Wilson PW
CVDEP 2006 (AHA-Epi 2006)Poster
Correct as of 16th February 2006

Updated slide kit, February 2006
60
Papers in Development (I)
Title Lead author Target journal1-Year Cardiovascular Event Rates in the REACH Registry International Cohort of Over 68,000 Stable Outpatients with Atherothrombosis
Steg PG JAMA
Risk factor profile and management of 18,984 patients in 2004, the REACH Registry - an international prospective observational registry in subjects at risk of atherothrombotic events in an outpatient setting
Roether J,Mas J-L
Stroke TBC
Risk of vascular death and myocardial infarction in patients with stroke or TIA: Results from the REduction of Atherothrombosis for Continued Health (REACH) Registry
Mas J-L TBC
Renal insufficiency according to atherothrombosis location in the REACH Registry
Dumaine R, Montalescot G, YeoT-C, Chan J
TBC
The international morbidity and mortality of peripheral arterial disease: Insights from the REACH Registry
Hirsch AT TBC
Correct as of 16th February 2006

Updated slide kit, February 2006
61
Papers in Development (II)
Title Lead author Target journalSocio-economic status baseline article Wilson PWF TBCAnalysis of the intensity of prevention efforts (at baseline) in CAD patients
Cannon C TBC
CABG manuscript Ohman EM TBCThe risk of abdominal aortic aneurysms: The REACH Registry
Baumgartner I TBC
1-year outcomes in CAD patients Eagle K TBChs-CRP in CAD Cannon C,
Zeymer UTBC
Cardiovascular morbidity of severe peripheral arterial disease: the fate of individuals with ischemic amputations in the REACH Registry
Abola MTB TBC
Baseline control of risk factors according to surgical or medical management of PAD patients in the REACH Registry
Cacoub P TBC
Correct as of 16th February 2006

Updated slide kit, February 2006
62
Participating Organizations and Scientific Committees

Updated slide kit, February 2006
63
Scientific Committee1
1. REACH Registry website. Available at: http://www.REACHRegistry.org. Accessed January 2006.
Name AffiliationP Gabriel Steg, MD Hôpital Bichat-Claude Bernard, Paris, France (Co-chair)Deepak L Bhatt, MD Cleveland Clinic Foundation, Cleveland, OH, USA (Co-chair)E Magnus Ohman, MD Duke University Medical Center, Durham, NC, USAJoachim Röther, MD, PhD Klinikum Minden, Minden, Germany
Peter WF Wilson, MD Medical University of South Carolina, Charleston, SC, USA

Updated slide kit, February 2006
64
Publication Committee1
Name Affiliation
Deepak L Bhatt, MD Cleveland Clinic Foundation, Cleveland, OH, USA
Shinya Goto, MD, DMedSci Tokai University School of Medicine, Kanagawa, Japan
Alan T Hirsch, MD University of Minnesota School of Public Health, Minneapolis, MN, USA
Chiau-Suong Liau, MD, PhD
Taiwan University Hospital and College of Medicine, Taipei, Taiwan
Jean-Louis Mas, MD Centre Raymond Garcin, Paris, France
E Magnus Ohman, MD Duke University, Durham, SC, USA
Joachim Röther, MD, PhD Klinikum Minden, Minden, Germany
P Gabriel Steg, MD Hôpital Bichat-Claude Bernard, Paris, France
Peter WF Wilson, MD Medical University of South Carolina, Charleston, SC, USA
Ralph D’Agostino, PhD Boston University, Boston, MA, USA
1. REACH Registry website. Available at: http://www.REACHRegistry.org. Accessed January 2006.

Updated slide kit, February 2006
65
National Coordinators (I)1
Country Name and affiliationAustralia Christopher Reid, Monash University, VictoriaAustria Franz Aichner, Landes-Nervenklinik Wagner-Jauregg, Linz
Thomas Wascher, Medizinische Universitätsklinik, GrazBelgium Patrice Laloux, Cliniques Universitaires UCL, Mont-GodinneBrazil Denilson Campos de Albuquerque, State University of Rio de Janeiro, Rio de JaneiroBulgaria Julia Djorgova, University Hospital St Ekaterina, SofiaCanada Eric A Cohen, Sunnybrook & Women’s College Health Sciences Center, Toronto, OntarioChile Ramon Corbalan, Hospital Clinico Pontificia Universidad Catolica de Chile, SantiagoChina Chuanzhen LV, Shanghai Huashan Hospital, Shanghai
Runlin Gao, Fu Wai Hospital, BeijingDenmark Per Hildebrandt, H.S. Frederiksberg Hospital, FrederiksbergFinland Ilkka Tierala, Helsinki University Hospital, HelsinkiFrance Jean-Louis Mas, Hôpital Saint-Anne, Paris
Patrice Cacoub, Groupe Hospitalier Universitaire Pitié Salpétrière, ParisGilles Montalescot, Groupe Hospitalier Universitaire Pitié Salpétrière, Paris
Germany Klaus Parhofer, Universitätsklinikum Großhadern, MunichUwe Zeymer, Klinikum Ludwigshafen Medizinische, LudwigshafenJoachim Röther, Klinikum Minden, Minden
1. REACH Registry website. Available at: http://www.REACHRegistry.org. Accessed January 2006.

Updated slide kit, February 2006
66
National Coordinators (II)1
Country Name and affiliationGreece Moses Elisaf, University of Ioannina Medical School, IoanninaGuatemala Romulo López, Centro Diagnostico, Cuidad de GuatemalaHong Kong Juliana Chan, Prince of Wales Hospital, ShatinHungary György Pfliegler, University of Debrecen Medical and Health Science Center, DebrecenIndonesia Bambang Sutrisna, University of Indonesia, JakartaIsrael Avi Porath, Soroka Medical Center, Beer ShevaJapan Yasou Ikeda, Keio University School of Medicine, TokyoLebanon Ismail Khalil, American University Hospital Hamra, BeirutLithuania Ruta Babarskiene, University Hospital, KaunasMalaysia Robaayah Zambahari, Institut Jantung Negara, Kuala LumpurMexico Efrain Gaxiola, Instituto Cardiovascular de Guadalajara, JaliscoThe Netherlands Don Poldermans, Erasmus Medisch Centrum, RotterdamPhilippines M. Teresa B. Abola, Philippine Heart Center, Quezon CityPortugal Victor Gil, Hospital Fernando Fonseca, AmadoraRomania Constantin Popa, Institutul de Boli Cerebro-Vasculare, BucharestRussia Yuri Belenkov, Cardiology Research Complex, Moscow
Elizaveta Panchenko, Cardiology Research Complex, Moscow
1. REACH Registry website. Available at: http://www.REACHRegistry.org. Accessed January 2006.

Updated slide kit, February 2006
67
National Coordinators (III)1
Country Name and affiliationSaudi Arabia Hassan Chamsi-Pasha, King Fahd Military Hospital, JeddahSingapore Yeo Tiong Cheng, National University Hospital, SingaporeSouth Korea Oh Dong-Joo, Korea Hospital, SeoulSpain Carmen Suárez, Hospital Universitario de la Princesa, MadridSwitzerland Iris Baumgartner, Universitätspital Bern, BernTaiwan Chiau-Suong Liau, National Taiwan University Hospital, TaipeiThailand Piyamitr Sritara, Ramathibodi Hospital, BangkokUnited Arab Emirates
Wael Mahameed, Al Jazeera Hospital, Abu Dhabi
UK Jonathan Morrell, The Conquest Hospital, HastingsUkraine Vira Tseluyko, Kharkov Medical Academy of Postgraduate Education, KharkovUSA Mark Alberts, Northwestern University Medical Center, Chicago, IL
Robert M. Califf, Duke University Medical Center, Durham, NCChristopher P. Cannon, Brigham and Women’s Hospital, Boston, MAKim Eagle, University of Michigan Cardiovascular Center, Ann Arbor, MIAlan T Hirsch, Minneapolis Heart Institute Foundation and Division of Epidemiology and Community Health, University of Minnesota School of Public Health, Minneapolis, MN
1. REACH Registry website. Available at: http://www.REACHRegistry.org. Accessed January 2006.

Updated slide kit, February 2006
68
Participating Organizations
The REACH Registry is sponsored jointly by

Updated slide kit, February 2006
69
REACH Registry: Further Information
For further information on the REACH Registry go to:
http://www.REACHRegistry.org