rcts - amcatmpmanufacture.org/wp-content/uploads/2016/10/farzin-farzaneh.pdf · (advanced therapy...
TRANSCRIPT

RCTS
MHRA Manufacturing Authorisation for - Investigational Medicinal Products (MA-IMP) - Specials
• Cells for cellular therapies • Viral vectors for gene therapy • Stem cells for regenerative medicine
Production Manager - Lucas Chan Quality Control Manager - Joti Bhalla Qualified Person - David Farrer
Farzin Farzaneh

The Rayne Cell Therapy Suite MHRA Manufacturing Authorisation for Investigational Medicinal Products (MA-IMP)

KCL/KCH - new Cell & Gene Therapy Unit (Q3, 2011)
• Hepatocyte Transplantation
• Islet Cell Transplantation
• Haematological Stem Cell Transplantation
• Cell and Gene Therapy of Cancer
• Stem cells for regerative medicine applications
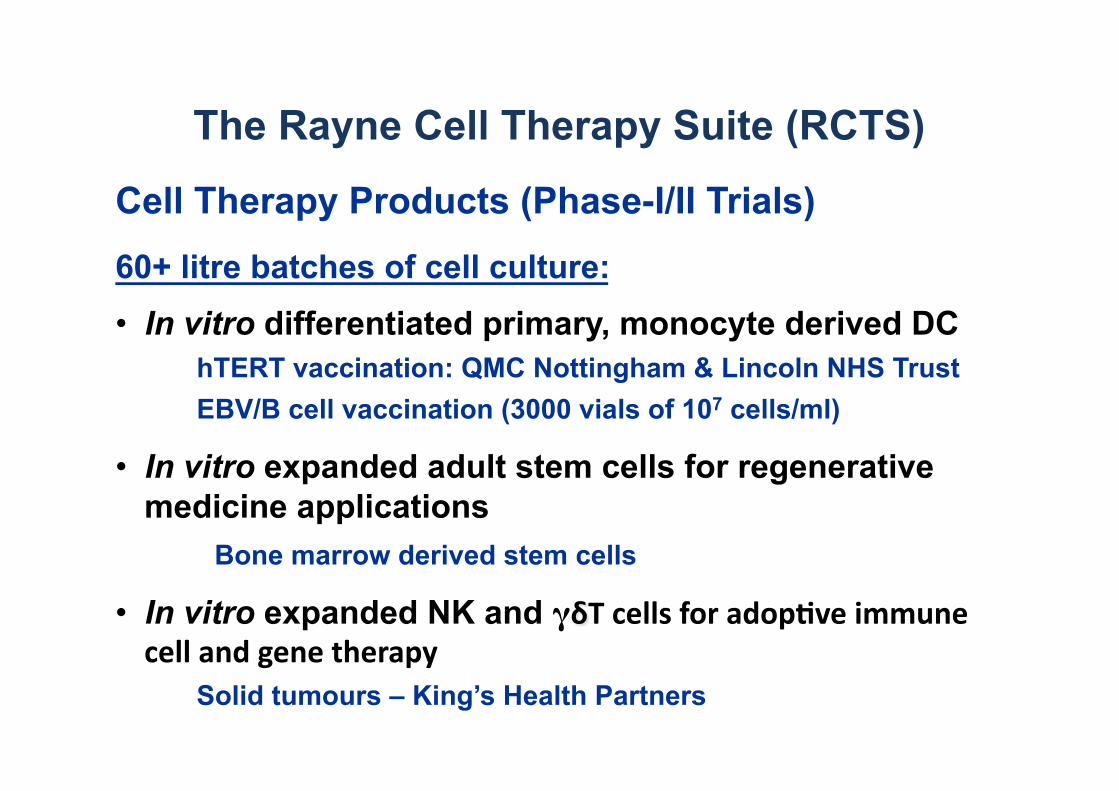
The Rayne Cell Therapy Suite (RCTS)
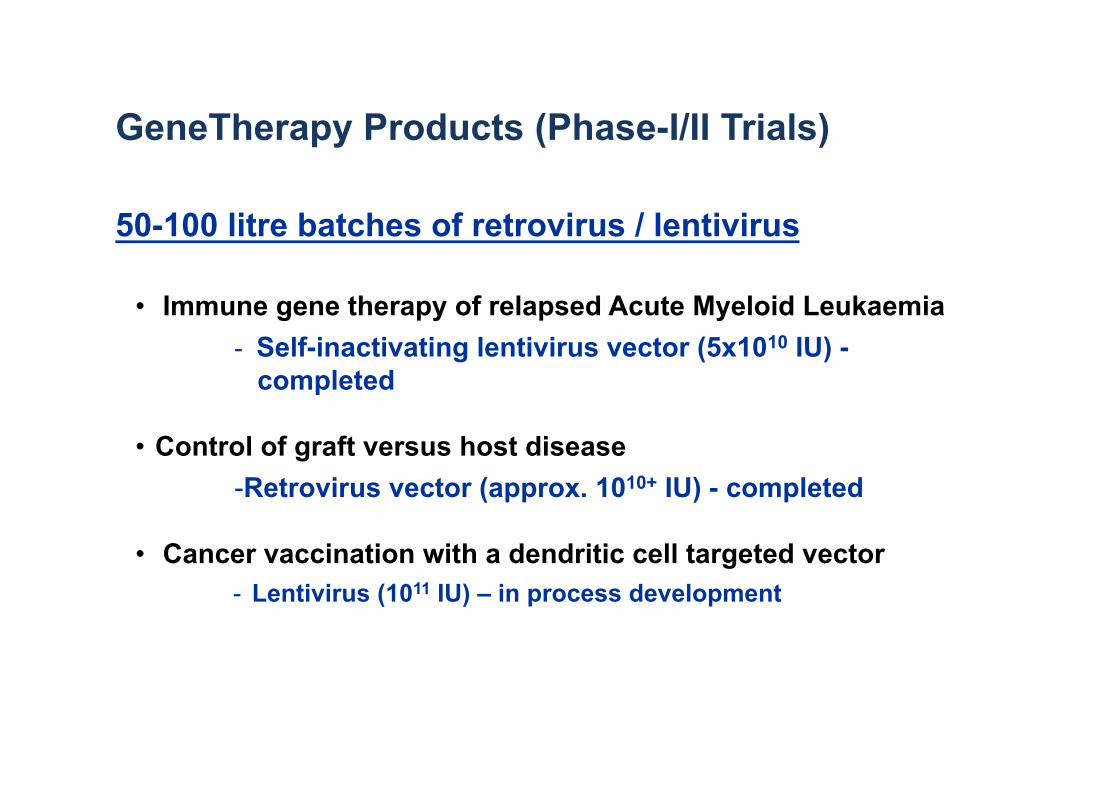
GeneTherapy Products (Phase-I/II Trials)
50-100 litre batches of retrovirus / lentivirus
• Immune gene therapy of relapsed Acute Myeloid Leukaemia - Self-inactivating lentivirus vector (5x1010 IU) - completed
• Control of graft versus host disease - Retrovirus vector (approx. 1010+ IU) - completed
• Cancer vaccination with a dendritic cell targeted vector - Lentivirus (1011 IU) – in process development

AML as a target for cell, gene and peptide based immune therapies
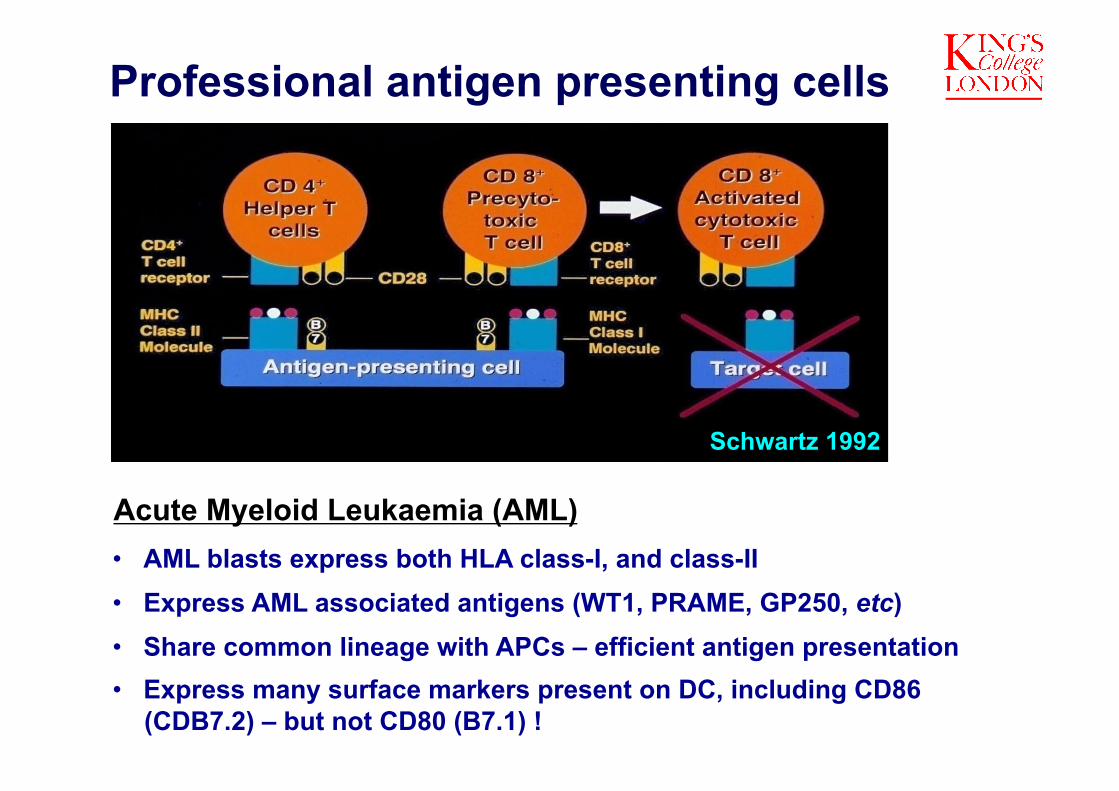
Professional antigen presenting cells
Schwartz 1992
Acute Myeloid Leukaemia (AML) • AML blasts express both HLA class-I, and class-II • Express AML associated antigens (WT1, PRAME, GP250, etc) • Share common lineage with APCs – efficient antigen presentation • Express many surface markers present on DC, including CD86
(CDB7.2) – but not CD80 (B7.1) !

Rejection of established mouse leukaemia, by vaccination with leukemia cells expressing CD80 (B7.1) and IL-2
Leukemia initiation
(105 32Dp210 cells iv)
32D/M3P (Vector)
■
●
■
32D/CD80
32D/IL-2
32D/IL-2/CD80
Cell vaccine ●
100 80
60 40
20
0
% S
urvi
val
■ ■● ●
● ●
■ ■
■ ■
■ ■
■ ■ ■
●
Time (days) 100 20 40 60 80 0
Vaccination (106 irradiated cells)
■
●
● ● ● ● ● ● ■ ■ ■ ■ ■ ■ ■ ■ ■■
In mouse leukaemia and solid tumour models, vaccination with the same tumour cell, modified to express CD80 (B7.1) and IL-2, induces immune mediated tumour rejection.

Autologous CTL activity
Hardwick N et al (2010). Cancer Immunol. Immunther. 59(3): 379-88.
E:T ratio = 50:1
CM
Autologous CTL activity in 3 representative
patients
Remission PBLs, stimulated by autologous IL-2/CD80 (B7.1) AML, display cytolytic activity against unmodified AML blasts

Autologous CTL activity
Hardwick N et al (2010). Cancer Immunol. Immunther. 59(3): 379-88.
E:T ratio = 50:1
CM
Autologous CTL activity in 3 representative
patients
Remission PBLs, stimulated by autologous IL-2/CD80 (B7.1) AML, display cytolytic activity against unmodified AML blasts
- Remission T cells are not defective in cytolytic activity
- AML cells are not resistant to cytotoxicity

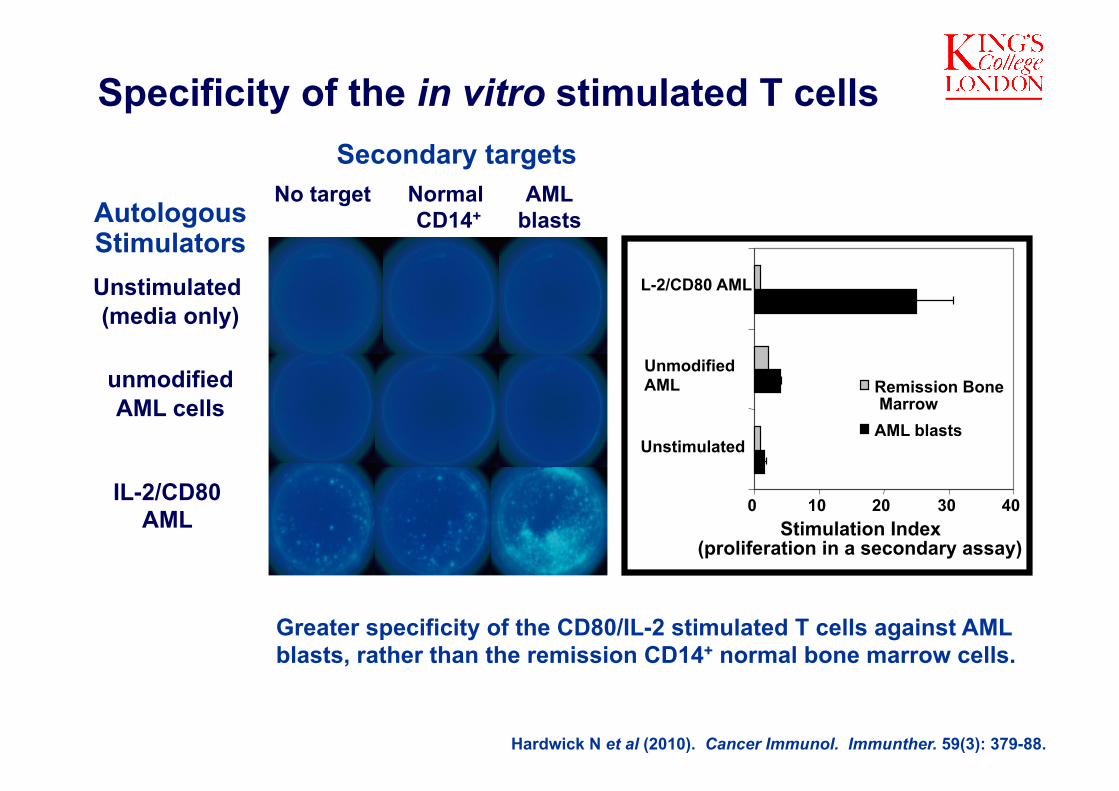
Specificity of the in vitro stimulated T cells
Hardwick N et al (2010). Cancer Immunol. Immunther. 59(3): 379-88.

Specificity of the in vitro stimulated T cells Secondary targets
AutologousStimulators Unstimulated (media only)
unmodified AML cells
IL-2/CD80 AML
Hardwick N et al (2010). Cancer Immunol. Immunther. 59(3): 379-88.
No target Normal AML CD14+ blasts

Specificity of the in vitro stimulated T cells Secondary targets
Hardwick N et al (2010). Cancer Immunol. Immunther. 59(3): 379-88.
No target Normal AML CD14+ blasts Autologous
Stimulators Unstimulated (media only)
unmodified AML cells
IL-2/CD80 AML

Specificity of the in vitro stimulated T cells Secondary targets
Hardwick N et al (2010). Cancer Immunol. Immunther. 59(3): 379-88.
No target Normal AML CD14+ blasts Autologous
Stimulators Unstimulated (media only)
unmodified AML cells
IL-2/CD80 AML
Specificity of the in vitro stimulated T cells
No target Normal AML CD14+ blasts
Secondary targets
Greater specificity of the CD80/IL-2 stimulated T cells against AML blasts, rather than the remission CD14+ normal bone marrow cells.
Hardwick N et al (2010). Cancer Immunol. Immunther. 59(3): 379-88.
AutologousStimulators Unstimulated (media only)
unmodified AML cells
IL-2/CD80 AML

NK cell stimulation by IL-2/CD80 expressing AML cells
CD3
CD
56
PBMC PBMC + AML
PBMC + IL-2/CD80/AML PBMC + CD80/AML PBMC + IL-2/AML
Ingram W et al (2009). Br J Haematol. 145: 749-60.

Enhanced cytotoxicity of NK cells against K562 and autologous AML cells following co-culture with CD80/IL-2 expressing AML cells
• Patient NK cells can be expanded & stimulated to express cytolytic activity
• AML cells not resistant to the cytolytic activity of the stimulated NK cells
Base line +Unmodified + CD80/IL-2 AML modified AML
Base line +Unmodified + CD80/IL-2 AML modified AML
51Cr release assay – isolated NK cells
% S
peci
fic ly
sis
% S
peci
fic ly
sis Target
K562 cells AML Cells
51Cr release assay – isolated NK cells
Target K562 cells AML Cells
Ingram W et al (2009). Br J Haematol. 145: 749-60.

B7.1/IL-2 immune gene therapy for poor prognosis relapsed AML
Chemotherapy
Allo-HSCT RIC
Day 28 Day 56 Day 100
Day 0
Day 100+
Donor Leuckocyte Infusion (DLI) if no evidence of GvHD
reduced leukaemia burden
Reconstituted immune system
(donor chimerism)
Cohort 1
Cohort 2 DLI + AML Cell Vaccine
DLI Alone
105 106 107 108 AML Cell Vaccine
(“autologous”) every 3 weeks
Intensive Chemotherapy but no CR or PR

Advanced Therapy Medicinal Products
EC Regula:on No 1394/2007
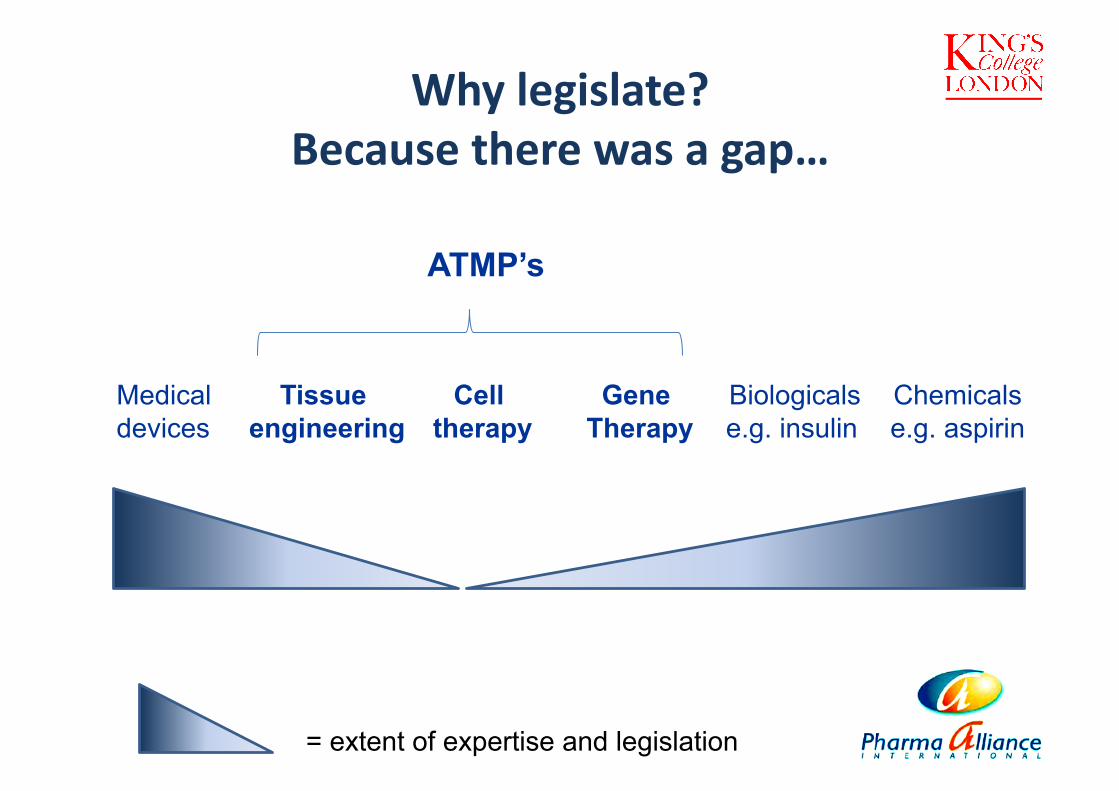
Why legislate? Because there was a gap…
Chemicals e.g. aspirin
Biologicals e.g. insulin
Gene Therapy
Cell therapy
Tissue engineering
Medical devices
= extent of expertise and legislation
ATMP’s

ATMP: Key definitions • Non-viable and viable cells are included
• Products which do not contain viable cells and which do not act principally by metabolic action are excluded
• Where a product contains viable cells, the pharmacological, immunological or metabolic action of those cells shall be considered as the principal mode of action
• The association of cells with a device is no longer considered essential for the cells to be termed “engineered”
• In case of doubt, products will be defined as being in the most tightly regulated category: gene therapy > tissue engineering > somatic cell therapy

Key principles of the legisla<on
• No marketing without prior authorisation
• Demonstration of Quality, Safety and Efficacy
• Post authorisation vigilance
• Centralised procedure mandatory (European Medicines Agency)

“Hospital Exemp<on” scheme
A specific exclusion from EC Regula:on No 1394/2007
Hospital exemption scheme
• Based on Section 6 of EC Regulation 1394/2007 (Advanced Therapy Medicinal Products)
• Allows for unlicensed ATMPs to be used, under very specific conditions: – prepared on a non-routine basis
– with specific quality standards
– used within a hospital in the same Member State
– a custom-made product for an individual patient

“Specials” scheme • Sometimes called “compassionate use” or “named
patient use” • Based on Article 5.1 of Directive 2001/83/EC (the
main directive relating to medicinal products for human use)
• Allows unlicensed medicines to be supplied to meet special needs:
– In response to a bona fide unsolicited order – Formulated in accordance with the specifications of an
authorised health care professional – For use by an individual patient under the health care
professional’s direct personal responsibility
Similarities between the two schemes
• Both cover the supply and use of unlicensed medicines (i.e. those without a Marketing Authorisation)
• A Manufacturer’s Licence, specific to each scheme, is required in order to produce the unlicensed medicines
• Neither scheme requires a QP to certify batches
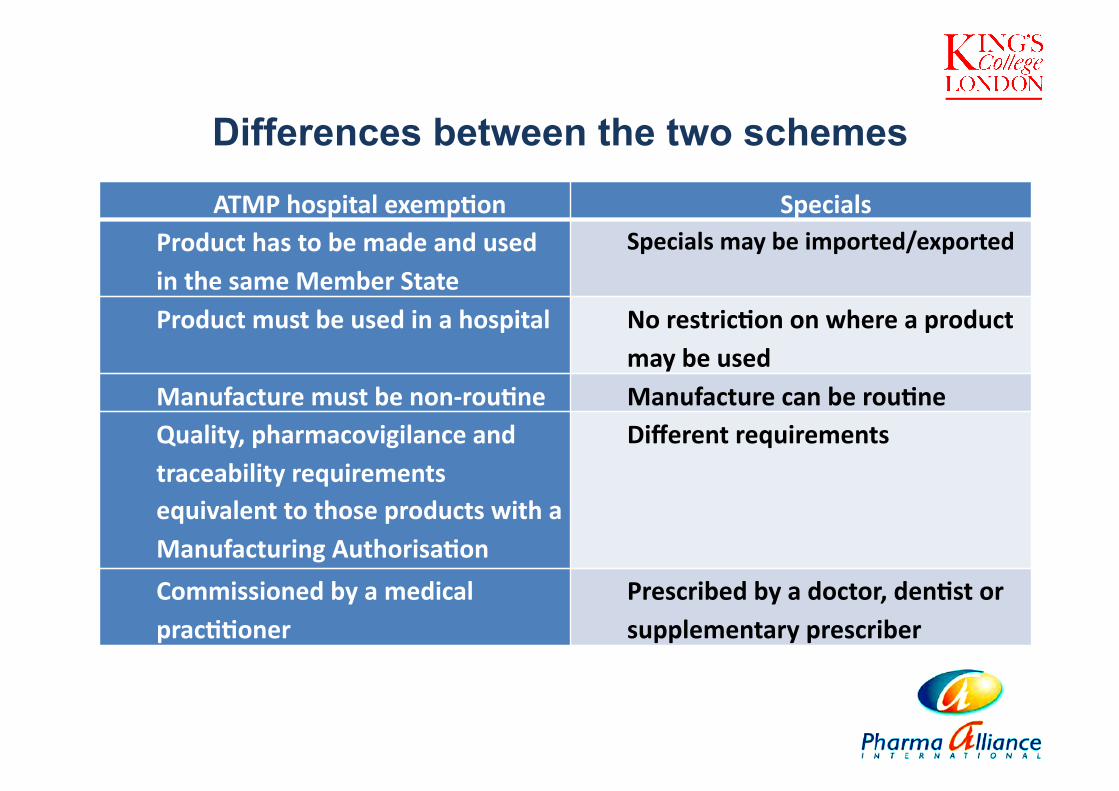
Differences between the two schemes
ATMP hospital exemp<on Specials Product has to be made and used in the same Member State
Specials may be imported/exported
Product must be used in a hospital No restric<on on where a product may be used
Manufacture must be non-‐rou<ne Manufacture can be rou<ne Quality, pharmacovigilance and traceability requirements equivalent to those products with a Manufacturing Authorisa<on
Different requirements
Commissioned by a medical prac<<oner
Prescribed by a doctor, den<st or supplementary prescriber

UK legislation
• As well as incorporating EC Regulation 1394/2007, the MHRA has also included the following provisions in the UK legislation for the hospital exemption scheme: – Pharmacovigilance - notification of adverse reactions
– Possible requirement for a risk management plan
– Traceability records from donor to use/destruction, kept for 30 years
– Specific requirements for patient information on the label and in a leaflet
– An annual return to the MHRA

Qualified Person
Qualifications and requirements

European Directive 2001/83/EC
• A qualified person shall complete a university course of study in one of the following:
– pharmacy
– medicine
– veterinary medicine
– chemistry
– pharmaceutical chemistry and technology
– biology

Directive 2001/83/EC continued…
• The course shall include theoretical and practical study of the following: – Applied physics – General and inorganic chemistry – Organic chemistry – Analytical chemistry – Pharmaceutical chemistry – General and applied biochemistry – Physiology – Microbiology – Pharmacology – Pharmaceutical technology – Toxicology – Pharmacognosy (composition & effects of natural active substances)

Directive 2001/83/EC continued…
• The qualified person shall have acquired practical experience over at least two years at a manufacturing site, including analysis of medicinal products and active substances and of the testing and checking necessary to ensure the quality of medicinal products.
• A person carrying out QP activities before May 1985 shall be eligible to continue to engage in those activities (“grandfather clause”)

To become a QP in the UK…
• The MHRA require the Society of Biology, the Royal Pharmaceutical Society and the Royal Society of Chemistry to assess the eligibility of their members for Qualified Person status.
• These organisations provide guidance notes, study guides and the code of practice, as well as the application forms.

RCTS
Production Manager - Lucas Chan
Quality Control Manager - Joti Bhalla
Qualified Person - David Farrer
Angela Osborne

Asthma and Allergy
Alistair Noble James Wells
Infection & Immunity
Adrian Hayday Mark Peakman

Mayo Clinic Stephen Russell
University College London
Mary Collins Bobby Gaspar Waseem Qasim Adrian Thrasher
UCLA Noriyuki Kasahara
Sharon Williams Nigel Slater
University of Cambridge
Imperial College London Colin Casimir Myrtle Gordon Nagy Habib
Mark Aloysius Lindy Durant Oleg Eremin Adrian Robbins
University of Nottingham / QMC
University of Geneva Didier Trono
San Raffaele Institute, Milan Luigi Naldini

Cytokine profile of human autologous T cells following in vitro stimulation (Cytokine Bead Array – CBA)
• The in vitro stimulated T cells have a predominantly Th1 phenotype
n=3
IFNγ
IL-4
TNF-α
IL-2
IL-6 IL-10
IFNγ
IL-4
TNF-α
IL-2
IL-6 IL-10
IFNγ
IL-4
TNF-α
IL-2
IL-6 IL-10

RCTS