rapidly changing trends in aneuploidy screening … · rapidly changing trends in aneuploidy...
TRANSCRIPT

10/24/2013
1
RAPIDLY CHANGING TRENDS IN ANEUPLOIDY SCREENING
Mary E. Norton MDProfessor, Obstetrics, Gynecology and Reproductive SciencesUniversity of California, San Francisco
Conflict of Interest Disclosure
• I have no personal financial stake in any commercial entity related to this talk
• I am co-PI of a clinical trial supported by AriosaDiagnostics and site PI of clinical studies and unpaid clinical advisor for CellScape.
History of Prenatal Screening
• Maternal age 35 yo 1960’s• MSAFP for NTD 1977• Multiple marker screening 1988
• First trimester markers/NT 1994• ACOG “all tests available” 2007• Universal screening (multiplex panels) 2010• Noninvasive prenatal testing (NIPT) 2011• Fetal whole genome sequencing
2012

10/24/2013
2
0
20
40
60
80
100
120
Detection Rate of Prenatal Screening for Down syndrome has improved over time
Det
ectio
n R
ate
(%)
Multiple marker screening
• Uses a combination of first and second trimester serum analytes and ultrasound markers
• Primary purpose is screening for Down syndrome and neural tube defects
• Can also detect other birth defects and abnormalities
• In absence of fetal anomalies, abnormal levels of some analytes are associated with adverse obstetric outcomes
Fetal Anomalies Associated with Elevated MSAFP
• Open fetal anomalies• Neural tube defects (spina bifida/anencephaly)Ventral wall defects (omphalocele/gastroschisis)
Chromosome abnormalitiesTriploidy
Severe renal abnormalitiesBilateral renal agenesis
Autosomal recessive polycystic kidney disease
Congenital skin disordersUpper GI tract obstruction
Fetal Anomalies Associated with Elevated MSAFP
• Open fetal anomalies• Neural tube defects (spina bifida/anencephaly)• Ventral wall defects (omphalocele/gastroschisis)
• Chromosome abnormalities• Triploidy
• Severe renal abnormalities• Bilateral renal agenesis
• Autosomal recessive polycystic kidney disease
• Congenital skin disorders• Upper GI tract obstruction

10/24/2013
3
UpToDate, 2008
Analyte PatternsNuchal translucency
• Increased NT highly associated with aneuploidy
• Also with several other abnormalities
Nonchromosomal Defects and Increased Nuchal Translucency
• Major cardiac defects • Diaphragmatic hernia• Omphalocele
• Limb body wall defect• Fetal akinesia• Noonan syndrome• Skeletal dysplasias• Other structural and genetic disorders
Euploidfetuses (n)
NT (mm) Genetic disorders and neurodevelopmental delay
Mangione et al., 2001 202 > 3mm 1/202 (0.5%)
Souka et al., 2001 1320 > 3.5 mm 44/1320 (3.3%)
Senat et al., 2002 89 > 4 mm 4/62 (6.4%)
Bilardo et al., 2007 425 > 95th % 23/425 (5.4%)
Total 2271 72/1629 (4.4%) (range 0.5-6.4%)
Genetic Disorders Detected In Fetuses With Enlarged Nuchal Translucency
Bilardo Prenatal Diagnosis 2010

10/24/2013
4
Fetal cardiac defects and enlarged NT
NT Incidence CHD
<2.5mm 0.16%2.4-3.4mm 1%3.5-4.5mm 3%4.5-5.4mm 7%5.4-6.4mm 20%>6.5mm 30%
Souka, 2005
Abnormal Analytes and 3d Trimester Pregnancy Complications
• Several patterns of abnormal analytes have been associated with placental dysfunction
• Low PAPP-A, low uE3, high AFP, hCG, inhibin• 3d trimester pregnancy complications
• Preeclampsia, early fetal loss, late fetal loss, preterm delivery, IUGR
• Risk of adverse outcomes increases with higher levels or with multiple abnormal analytes
Odds Ratios for Outcomes Associated with Abnormal Analytes
Analyte IUFD PTB IUGR PreE
PAPP-A <0.29 MoM 3.0 3.3 4.64 1.79
PAPP-A <0.42 MoM 2.15 1.9 2.81 1.54
hCG >2.0 MoM 1.5-4.7 1.7-2.8 1.8-4.8 2.4
AFP >2.5 MoM 4.4-9.8 1.8-4.8 1.6-4.0 3.8
Inh A >2.0 MoM 2.4 2.4 2.4 2.4
uE3 <0.5 MoM 3.3 2.3
Association between Adverse Outcomes and Serum Analytes
Dugoff, Obstet Gynecol, 2010

10/24/2013
5
Is detection of abnormal analytes helpful?
Disorder ASA No ASA RR (CI)
PreE 9.3% 21.3% 0.47 (0.34-.65)
Severe PreE 7% 15% 0.09 (0.02-.37)
IUGR 7% 16.3% 0.44 (0.30-.65)
Bujold et al, 2010, Obstet GynecolMeta-analysis of studies of aspirin in high risk women
ASA decreased risks only when started at <16 weeks gestation
Is detection of abnormal analytes helpful?
Roberge et al, Ultrasound Obstet Gynecol 2013Meta-analysis of studies of aspirin in high risk women
ASA decreased risks only when started at <16 weeks gestation
Disorder ASA No ASA RR (CI)
Perinatal death 1.1% 4.0% 0.41 (0.19-0.92)
Preeclampsia 7.6% 17.9% 0.47 (0.36-0.62)
Severe PreE 1.5% 12.3% 0.18 (0.08-0.41)
IUGR 8.0% 17.6% 0.46 (0.33-0.64)
Preterm birth 4.8% 13.4% 0.35 (0.22-0.57)
Noninvasive Prenatal Testing (NIPT) using Cell Free DNA
• Tests for aneuploidy by directly sequencing of fetal DNA, largely derived from placenta
• Compared with current screening which uses indirect measurements of protein products
• NIPT for detection of trisomy 21 has greater sensitivity and much greater specificity than multiple marker screening
Analysis of cell free DNA
Zhong, X, Holzgreve, W, Glob. libr. women's med 2009
10/24/2013
6
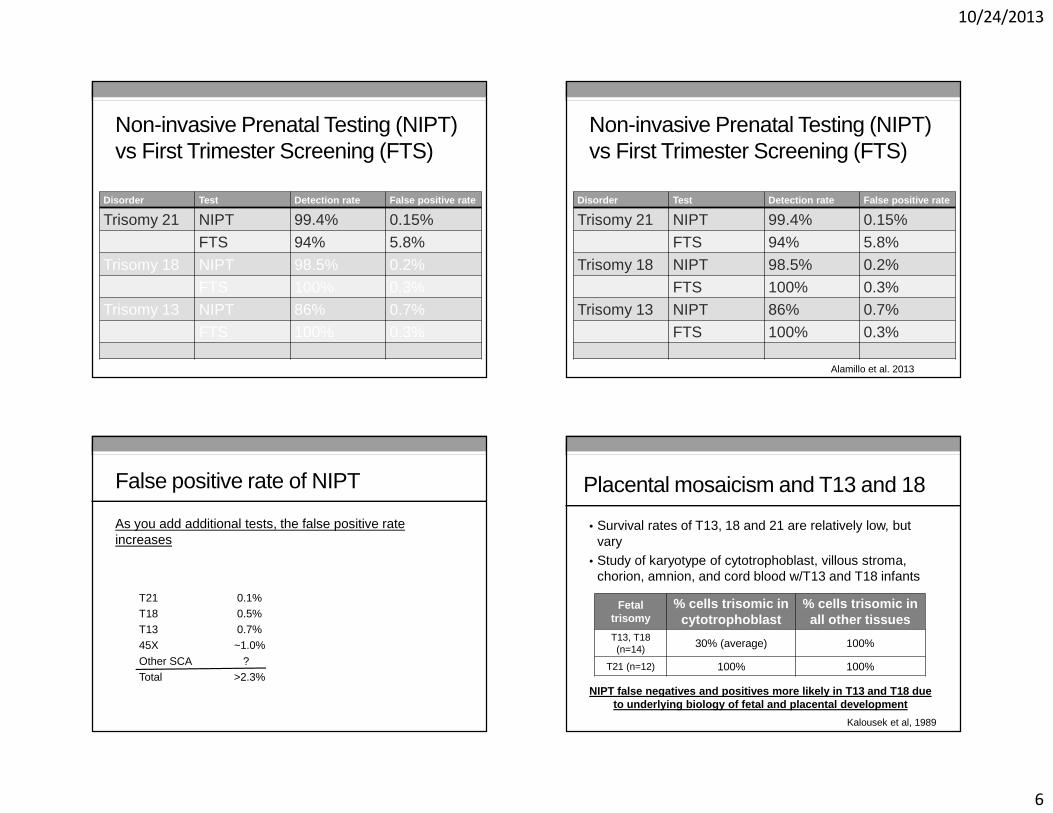
Non-invasive Prenatal Testing (NIPT) vs First Trimester Screening (FTS)
Disorder Test Detection rate False positive rate
Trisomy 21 NIPT 99.4% 0.15%
FTS 94% 5.8%
Trisomy 18 NIPT 98.5% 0.2%
FTS 100% 0.3%Trisomy 13 NIPT 86% 0.7%
FTS 100% 0.3%
Non-invasive Prenatal Testing (NIPT) vs First Trimester Screening (FTS)
Disorder Test Detection rate False positive rate
Trisomy 21 NIPT 99.4% 0.15%
FTS 94% 5.8%
Trisomy 18 NIPT 98.5% 0.2%
FTS 100% 0.3%Trisomy 13 NIPT 86% 0.7%
FTS 100% 0.3%
Alamillo et al. 2013
False positive rate of NIPT
As you add additional tests, the false positive rate increases
T21 0.1%T18 0.5%T13 0.7%45X ~1.0%
Other SCA ? Total >2.3%
• Survival rates of T13, 18 and 21 are relatively low, but vary
• Study of karyotype of cytotrophoblast, villous stroma, chorion, amnion, and cord blood w/T13 and T18 infants
Fetal trisomy
% cells trisomic in cytotrophoblast
% cells trisomic in all other tissues
T13, T18(n=14) 30% (average) 100%
T21 (n=12) 100% 100%
NIPT false negatives and positives more likely in T13 and T18 due to underlying biology of fetal and placental development
Placental mosaicism and T13 and 18
Kalousek et al, 1989

10/24/2013
7
Natural X Chromosome Loss
• 665 women (0-80yrs)
• Lymphocyte cultures on 19,650 cells
• G-banding analysis for presence of 1 or 2 X chromosomes
Russell et al, 2007
NIPT is more precise for T21, T18
NIPT Current NT + serum screen
NIPT is more precise for T21, T18
NIPT Current NT + serum screen
Other abnormalities
NIPT is more precise for T21, T18
NIPT FTSOther abnormalities
8/8 T212/3 T18; 1/3 no result
8/8 T213/3 T187/7 others (45X; triploidy; deletions and duplications)Nicolaides et al, 2012

10/24/2013
8
NIPT is more precise for T21, T18
NIPT FTSOther abnormalities
8/8 T212/3 T18; 1/3 no result
8/8 T213/3 T187/7 others (45X; triploidy; deletions and duplications)
55%(10/18)
100%(18/18)
Nicolaides et al, 2012
“Nearly a third of abnormalities found after first trimester screening are different than expected” Alamillo et al. 2013
• N=23,329 cases of FTS over 10 years• 6.3% screen positive
• 5.7% for T21; 0.4% for T13/18; 0.3% for both
• 97 had a chromosome abnormality (1/240)• 47 Down syndrome (T21) (1/500)• 22 Trisomy 13 or 18
• 29 Other chromosome abnormalities• Range of severity from mild to lethal• Detected by combination of NT and analytes
DS and T18 make up 2/3 of aneuploidies detectable by karyotype
Disorders potentially detectable by serum screening and NIPT
NIPT
• Trisomy 21• Trisomy 18• Trisomy 13
• Some sex chromosomes
Current Screening• Trisomy 21
• Trisomy 18• Trisomy 13• Some sex chromosomes• Triploidy
• Other rare aneuploidies• Congenital heart defects• Noonan syndrome
• Neural tube defects• Ventral wall defects• Congenital adrenal hypoplasia• Smith Lemli Opitz syndrome
• Steroid sulfatase deficiency• Poor OB outcomes (IUGR, PreE, PTB)

10/24/2013
9
Rate of aneuploidy varies by maternal age
• >35 yo 43% of abnormalities will be missed by NIPT• <35 yo 75% of abnormalities will be missed by NIPT
• This includes only those that are detectable by karyotype• Rate is significantly higher if include those detectable by
chromosomal microarray
ACMG, Statement on Noninvasive Prenatal Screening, 2013
Chromosomal Microarray (CMA) for Prenatal Diagnosis
Diagnostic Yield in Cases with Normal Karyotype
Indication for Testing
Clinically Relevant (N=96)
U/S AnomalyN=755
6.0%
AMAN=1,966
1.7%
Positive ScreenN=729
1.7%
OtherN=372
1.3%
Abnormalities detectable per 1000 births
0
5
10
15
20
25
30
35
40
45
20 yo 25yo 30yo 35yo 40yo
NIPT
Amnio/karyotype
Amnio/microarray
Wapner et al 2012; Hook 1983

10/24/2013
10
Detection rate of FTS: Alamillo et al 2013
N=23,329 patients having FTS• N=50 cases of DS
• DR = 47 (94%)• FPR = 1345 (5.8%)
• N=22 cases of T13 or 18• DR = 22 (100%)• FPR = 134 (0.6%)
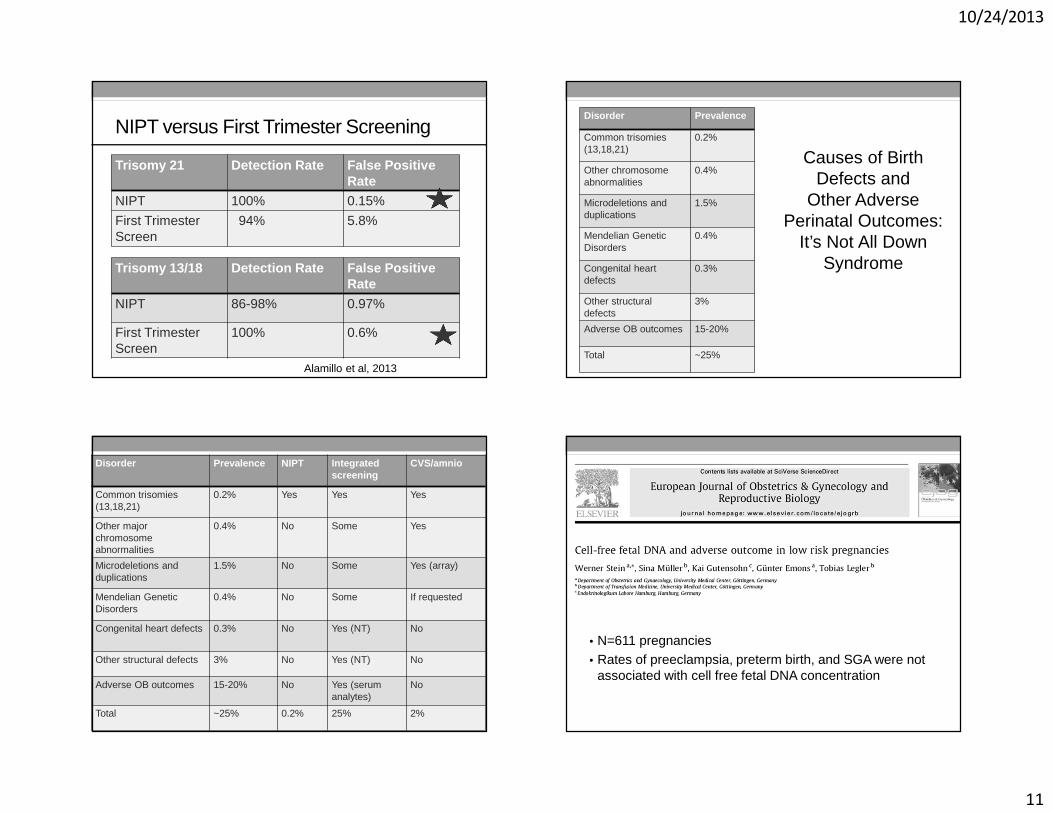
NIPT versus First Trimester Screening
Trisomy 21 Detection Rate False Positive Rate
NIPT 100% 0.15%
First Trimester Screen
94% 5.8%
Alamillo et al, 2013
NIPT versus First Trimester Screening
Trisomy 21 Detection Rate False Positive Rate
NIPT 100% 0.15%
First Trimester Screen
94% 5.8%
Trisomy 13/18 Detection Rate False Positive Rate
NIPT 86-98% 0.97%
First Trimester Screen
100% 0.6%
Alamillo et al, 2013
NIPT versus First Trimester Screening
Trisomy 21 Detection Rate False Positive Rate
NIPT 100% 0.15%
First Trimester Screen
94% 5.8%
Trisomy 13/18 Detection Rate False Positive Rate
NIPT 86-98% 0.97%
First Trimester Screen
100% 0.6%
Alamillo et al, 2013
10/24/2013
11
NIPT versus First Trimester Screening
Trisomy 21 Detection Rate False Positive Rate
NIPT 100% 0.15%
First Trimester Screen
94% 5.8%
Trisomy 13/18 Detection Rate False Positive Rate
NIPT 86-98% 0.97%
First Trimester Screen
100% 0.6%
Alamillo et al, 2013
Disorder Prevalence
Common trisomies(13,18,21)
0.2%
Other chromosomeabnormalities
0.4%
Microdeletions and duplications
1.5%
Mendelian GeneticDisorders
0.4%
Congenital heart defects
0.3%
Other structural defects
3%
Adverse OB outcomes 15-20%
Total ~25%
Causes of Birth Defects and
Other Adverse Perinatal Outcomes:
It’s Not All Down Syndrome
Disorder Prevalence NIPT Integrated screening
CVS/amnio
Common trisomies(13,18,21)
0.2% Yes Yes Yes
Other major chromosomeabnormalities
0.4% No Some Yes
Microdeletions and duplications
1.5% No Some Yes (array)
Mendelian GeneticDisorders
0.4% No Some If requested
Congenital heart defects 0.3% No Yes (NT) No
Other structural defects 3% No Yes (NT) No
Adverse OB outcomes 15-20% No Yes (serum analytes)
No
Total ~25% 0.2% 25% 2%
• N=611 pregnancies• Rates of preeclampsia, preterm birth, and SGA were not
associated with cell free fetal DNA concentration

10/24/2013
12
Prenatal Genetic Screening Comparison
Integrated Screening
- 2 blood tests + NT ultrasound- With sequential screen, patients
get two results over 6+ weeks- Complex counseling
- Stringent GA criteria- Relatively high screen positive
rate and good, not great, detection rate
- NT requires training and on-going QA
- NT very operator dependent+ Detects additional disorders+ Adjusts results by a priori risk
Noninvasive Prenatal Testing
+ Single blood test anytime after 10 weeks GA
+ Excellent performance = more straightforward counseling
+ Fewer invasive procedures+ One result that is highly
reliable- Tests for few conditions- Expensive- High test failure rate, esp.
with high BMI- Not validated in all subgroups- Doesn’t adjust for a priori risk
How Does Test Performance Differ with Risk?
Low Risk (age 25; 1/1000)
N=1000
1 T21 999 not T21
1 TP, 0 FN 2 FP, 998 TN
OAPR = 1/3
High Risk (age 38; 1/100)
N=1000
10 T21 990 not T21
10 TP, 0 FN 2 FP, 988 TN
OAPR = 10/12 or 5/6
(T21: Assume >99% sensitivity and 99.8% specificity)
How Does Test Performance Differ with Risk?
Low Risk (age 25; 1/8,000)
N=10,000
1 T13 9,999 not T13
1 TP, 0 FN 100 FP, 9900 TN
OAPR = 1/100
High Risk (age 38; 1/1000)
N=10,000
10 T13 9,990 not T13
10 TP, 0 FN 100 FP, 9890 TN
OAPR = 10/100 = 1/10
(T13: Assume 99% sensitivity and 99% specificity)

10/24/2013
13
Where does NIPT fit?
�Is this an outstanding screening test or an imperfect diagnostic test?
�Is this best used as a secondary screening test, or as a first tier screening test?
�Are we ready to abandon current screening in favor of NIPT?
Let’s not throw out the baby with the bathwater….. Hype cycle of new technology

10/24/2013
14
• Report on 8 false positive cases of T13 or T18• It is estimated that over 100,000 cases were done last year• Inflated expectations, lack of understanding, aggressive
marketing and competition are problematic

10/24/2013
15
Secretary’s Advisory Committee on Genetics, Health and Society
�Analytic validity: ability of test to measure particular genetic characteristics (eg DNA sequence) accurately and reliably in a given specimen
�Clinical validity: test’s accuracy in detecting the presence of, or predicting risk for, a health condition or phenotype
�Clinical utility: balance between health related benefits and harms that can ensue from a genetic test
Personalized Medicine 2008
Summary• NIPT has great value in detection of common trisomies.
• Multiple marker screening can play a much broader role in evaluating all pregnancies than NIPT.
• First trimester screening addresses not only fetal genetic risk, but also fetal structural abnormalities and pregnancy complications.
• Relative benefits of each test remain unclear, but may vary by patient risk category.
• Further study urgently needed before standard of care is completely changed.
Thank you!