rapid involuting congenital hemangioma in the setting...
TRANSCRIPT

Rapid Involuting Congenital Hemangioma in theSetting of PHACE Association
abstractRapidly involuting congenital hemangioma (RICH) is an uncommon vas-cular tumor that, unlike infantile hemangioma, is largely developed atbirth and undergoes rapid postnatal involution. To date, RICH has oftenbeen described in the setting of an isolated lesion, whereas infantilehemangioma is a well-known feature of numerous syndromes andassociations, including the association of posterior fossa anomalies,hemangioma, arterial anomalies, cardiac anomalies, and eye anoma-lies. The authors report a unique case of RICH in the setting of thisassociation. Pediatrics 2014;133:e1777–e1780
AUTHORS: Lauren M. Patrick, MD,a Christine Oh, BA, MS,a
Nancy Bauman, MD,b Bhupender Yadav, MD,c PhilipGuzetta, MD,d Iris Rubin, MD,e and Albert K. Oh, MDf
aDepartment of Plastic Surgery, Georgetown University Hospital,Washington, District of Columbia; bDivision of Otolaryngology,cDepartment of Radiology, dDepartment of Surgery, eDepartmentof Dermatology, and fDivision of Plastic Surgery, Children’sNational Medical Center, Washington, District of Columbia
KEY WORDShemangioma, PHACE, RICH, infant
ABBREVIATIONSGLUT-1—glucose transporter-1IH—infantile hemangiomaNICH—noninvoluting congenital hemangiomaPHACE—posterior fossa anomalies, hemangiomas, arterial anom-alies, cardiac anomalies, and eye anomaliesRICH—rapidly involuting congenital hemangioma
Dr Patrick conceptualized the study, drafted the initialmanuscript, and reviewed and revised the manuscript; Ms Ohdrafted the initial manuscript and reviewed and revised themanuscript; Drs Baumann, Yadav, Guzetta, Rubin, and Ohconceptualized the study and reviewed and revised themanuscript; and all authors approved the final manuscript assubmitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-2970
doi:10.1542/peds.2013-2970
Accepted for publication Nov 12, 2013
Address correspondence to Albert K. Oh, MD, Department ofPlastic Surgery, Children’s National Medical Center, 111 MichiganAvenue NW, Washington, DC 20010. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicatedthey have no potential conflicts of interest to disclose.
PEDIATRICS Volume 133, Number 6, June 2014 e1777
CASE REPORT
by guest on July 29, 2018www.aappublications.org/newsDownloaded from
PHACE association, a term first coinedby Frieden et al1 in 1996, describesa constellation of combined findingsincluding posterior fossa anomalies,hemangioma, arterial lesions, cardiacabnormalities oraortic coarctation, andabnormalities of the eye. Hemangiomasdescribed in PHACE are invariably thecommon infantile lesions, although theyare often described as plaquelike andmacular, with tendencies toward ulcer-ation.2 Importantly, the infantile hem-angioma (IH) of PHACE follow the classicpattern of minor to no presentation atbirth, with a period of rapid pro-liferation, followed by plateau and pro-longed involutional phases.
Congenital hemangioma is a distinctentity from IH, with 2 subtypes: rapidlyinvoluting congenital hemangioma(RICH) and noninvoluting congenitalhemangioma (NICH). Both types ofcongenital hemangioma are fully de-veloped at birth, unlike IH, and eitherquickly involute (RICH) or remainlargely unchanged with time (NICH).Although there are several other sig-nificant differences between thesecongenital hemangiomas and IH, onecurious finding is that, to date, con-genital hemangiomas have not beendescribed in association with othersyndromic or systemic features. Theauthors present an infant with a largefacial and scalp RICH, cardiac anoma-lies, and significant intracranial arte-riovenous fistulae consistent withPHACE association.
CASE REPORT
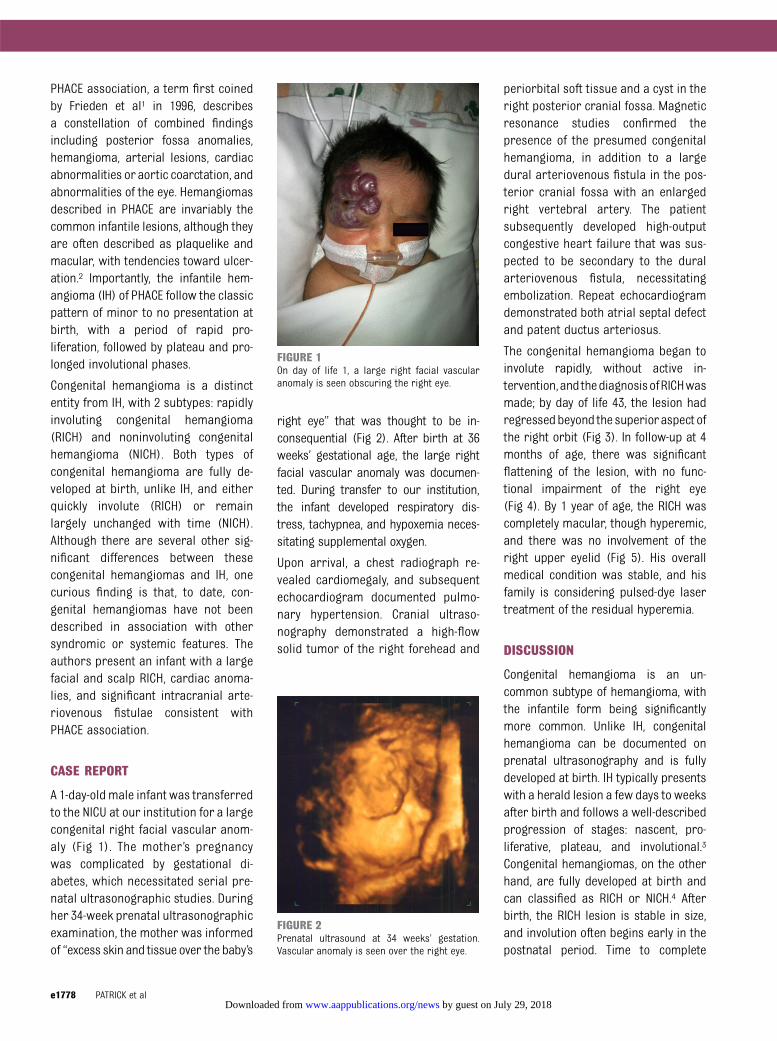
A 1-day-oldmale infant was transferredto the NICU at our institution for a largecongenital right facial vascular anom-aly (Fig 1). The mother’s pregnancywas complicated by gestational di-abetes, which necessitated serial pre-natal ultrasonographic studies. Duringher 34-week prenatal ultrasonographicexamination, the mother was informedof “excess skin and tissue over the baby’s
right eye” that was thought to be in-consequential (Fig 2). After birth at 36weeks’ gestational age, the large rightfacial vascular anomaly was documen-ted. During transfer to our institution,the infant developed respiratory dis-tress, tachypnea, and hypoxemia neces-sitating supplemental oxygen.
Upon arrival, a chest radiograph re-vealed cardiomegaly, and subsequentechocardiogram documented pulmo-nary hypertension. Cranial ultraso-nography demonstrated a high-flowsolid tumor of the right forehead and
periorbital soft tissue and a cyst in theright posterior cranial fossa. Magneticresonance studies confirmed thepresence of the presumed congenitalhemangioma, in addition to a largedural arteriovenous fistula in the pos-terior cranial fossa with an enlargedright vertebral artery. The patientsubsequently developed high-outputcongestive heart failure that was sus-pected to be secondary to the duralarteriovenous fistula, necessitatingembolization. Repeat echocardiogramdemonstrated both atrial septal defectand patent ductus arteriosus.
The congenital hemangioma began toinvolute rapidly, without active in-tervention,and thediagnosisofRICHwasmade; by day of life 43, the lesion hadregressedbeyond the superioraspect ofthe right orbit (Fig 3). In follow-up at 4months of age, there was significantflattening of the lesion, with no func-tional impairment of the right eye(Fig 4). By 1 year of age, the RICH wascompletely macular, though hyperemic,and there was no involvement of theright upper eyelid (Fig 5). His overallmedical condition was stable, and hisfamily is considering pulsed-dye lasertreatment of the residual hyperemia.
DISCUSSION
Congenital hemangioma is an un-common subtype of hemangioma, withthe infantile form being significantlymore common. Unlike IH, congenitalhemangioma can be documented onprenatal ultrasonography and is fullydeveloped at birth. IH typically presentswith a herald lesion a few days to weeksafter birth and follows a well-describedprogression of stages: nascent, pro-liferative, plateau, and involutional.3
Congenital hemangiomas, on the otherhand, are fully developed at birth andcan classified as RICH or NICH.4 Afterbirth, the RICH lesion is stable in size,and involution often begins early in thepostnatal period. Time to complete
FIGURE 1On day of life 1, a large right facial vascularanomaly is seen obscuring the right eye.
FIGURE 2Prenatal ultrasound at 34 weeks’ gestation.Vascular anomaly is seen over the right eye.
e1778 PATRICK et al by guest on July 29, 2018www.aappublications.org/newsDownloaded from

resolution of RICH can vary from 8 to 14months, oftenwith significant dermal andsubcutaneous atrophy.4 The mechanismof resolution is unknown, although it isspeculated to be accelerated apopto-sis.5,6
Pascual-Castroviejo7 initially describedfindings consistent with PHACE in 1978.Both Pascual-Castroviejo7 and Friedenet al1 described cases of large heman-giomas with concurrent Dandy–Walkermalformations and other variabledefects. The IH in PHACE often hasa progressive pattern of growth and
regression and is classically raisedbright red plaques, although there maybe varying patterns of lesion behavior.2
The majority of IH in PHACE is in the cer-vicofacial area and is usually of seg-mental morphology.8,9 Segmental IH hasbeenhypothesized to conform toauniquedevelopmental unit, and there are 4 seg-ments in which they tend to aggregate.9
Our patient had an S1 lesion involving thefrontotemporal region. The maxillary re-gion is analogous with S2, whereas S3 ismandibular and S4 frontonasal.2,9
IH has been well described in patientswith PHACE association, and a pro-spective study revealed that in infantswith large facial hemangiomas, one-third had extracutaneous manifes-tations consistent with PHACE.10 Thedefinition of PHACE consists of thecharacteristic facial IH and at least 1extracutaneous manifestation.11 The2009 consensus statement clarified thediagnostic criteria for PHACE: the pres-ence of a hemangioma greater than 5cm2 of the head (face or scalp) plus 1major criterion or 2 minor criteria.12
Major criteria include an anomaly ofmajor cerebral arteries, Dandy–Walkercomplex, aortic arch anomaly, a poste-rior segment anomaly of the eye, sternaldefect, and others.12 Minor defects in-clude more common congenital cardiac
lesions such as atrial septal defect,ventricular septal defect, patent ductusarteriosus, and others.12
Historically, congenital hemangiomaandIH have been regarded as separate en-tities,13 although more recent reportshave suggested that these lesions maybe on a spectrum of vascular tumors.4,6
A key basis for the distinction betweencongenital and infantile hemangiomas isthe expression of glucose transporter-1(GLUT-1). GLUT-1 expression is limitedto the microvascular endothelium ofblood tissue barriers of the centralnervous system, placental trophoblast,and areas of hypoxia and necrosiswithinother types of vascular tumors.2,14 Im-portantly, GLUT-1 is not present in thevasculature of normal skin and sub-cutaneous tissue, yet it is highlyexpressed in the capillary endotheliumof IH. This has led to the hypothesis of thepossible placental origin of hemangio-mas.14 GLUT-1 expression has also beeninterpreted to be an indicator of a hyp-oxic milieu, and it has been theorizedthat IH develops as a rescue to hypoxictissue in the setting of PHACE syndrome.2,15
To date, RICH and NICH have not beenfound to express GLUT-1.14
Although there is some evidence thatcongenital hemangiomas and infantilehemangiomas are histologically dis-tinct, similarities exist between these2 types of hemangioma. Insulinlikegrowth factor 2,which is upregulated inIH and indirectly linked to expression ofGLUT-1, is found in RICH and NICHspecimens, albeit at very low levels. Thelevelof insulinlikegrowth factor2mRNAexpression in congenital hemangiomaswas comparable to that of IH in the lateinvoluting and involuted phases.16 Adefinitive explanation for such a findingis not yet clear, although it may be ex-trapolated that congenital hemangio-mas are analogous to later-stageinfantile hemangiomas. Mulliken andEnjolras6 described 2 groups ofpatients who embody the “missing
FIGURE 3At day of life 43, the lesion has regressed beyondthe superior aspect of the right orbit.
FIGURE 4At 4 months of age, there is significant flatteningof the lesion, with no impairment of the right eye.
FIGURE 5At 1 year of age, the lesion is completely macular,with no involvement of the right upper eyelid.
CASE REPORT
PEDIATRICS Volume 133, Number 6, June 2014 e1779 by guest on July 29, 2018www.aappublications.org/newsDownloaded from

links” connecting congenital and in-fantile hemangiomas: patients who ei-ther had RICH or NICH along with IH andpatients who were initially diagnosedwith RICH but with incomplete in-volution, persisting as NICH. With thelatter it was hypothesized that RICHmay be an earlier form of NICH, with theNICH having undergone its involutionphase in utero, suggesting a spectrum
of behavior for what were originallydeemed to be distinct lesions.17
Such accounts seem to represent var-iations on a theme, with the implicationthat delineations between vascularlesions are more ambiguous than tra-ditionally believed. The cause of di-verging behaviors has not beendiscovered, although the idea of so-matic mutations leading to varying
phenotypes has been introduced.18,19
Mulliken and colleagues18 introducedthe idea of a unified theory of origin forcongenital and common hemangio-mas; application of this hypothesis, inthe case of our patient, allows a plau-sible explanation for the developmentof the rare RICH as the hemangiomawithin a polymalformative syndromesuch as PHACE association.
REFERENCES
1. Frieden IJ, Reese V, Cohen D. PHACE syn-drome. The association of posterior fossabrain malformations, hemangiomas, arte-rial anomalies, coarctation of the aortaand cardiac defects, and eye abnormali-ties. Arch Dermatol. 1996;132(3):307–311
2. Metry DW, Garzon MC, Drolet BA, et al.PHACE syndrome: current knowledge, fu-ture directions. Pediatr Dermatol. 2009;26(4):381–398
3. Chang LC, Haggstrom AN, Drolet BA, et al;Hemangioma Investigator Group. Growthcharacteristics of infantile hemangiomas:implications for management. Pediatrics.2008;122(2):360–367. doi:doi:10.1542/peds.2007-2767
4. Berenguer B, Mulliken JB, Enjolras O, et al.Rapidly involuting congenital hemangioma:clinical and histopathologic features.Pediatr Dev Pathol. 2003;6(6):495–510
5. Boon LM, Enjolras O, Mulliken JB. Congen-ital hemangioma: evidence of acceleratedinvolution. J Pediatr. 1996;128(3):329–335
6. Mulliken JB, Enjolras O. Congenital heman-giomas and infantile hemangioma: missinglinks. J Am Acad Dermatol. 2004;50(6):875–882
7. Pascual-Castroviejo I. Vascular and non-vascular intracranial malformation associ-ated with external capillary hemangiomas.Neuroradiology. 1978;16:82–84
8. Metry DW, Haggstrom AN, Drolet BA, et al. Aprospective study of PHACE syndrome ininfantile hemangiomas: demographic fea-tures, clinical findings, and complications.Am J Med Genet A. 2006;140(9):975–986
9. Haggstrom AN, Lammer EJ, Schneider RA,Marcucio R, Frieden IJ. Patterns of infantilehemangiomas: new clues to hemangiomapathogenesis and embryonic facial de-velopment. Pediatrics. 2006;117(3):698–703
10. Haggstrom AN, Garzon MC, Baselga E, et al.Risk for PHACE syndrome in infants withlarge facial hemangiomas. Pediatrics. 2010;126(2). Available at: www.pediatrics.org/cgi/content/full/126/2/e418
11. Metry DW, Dowd CF, Barkovich AJ, FriedenIJ. The many faces of PHACE syndrome. JPediatr. 2001;139(1):117–123
12. Metry D, Heyer G, Hess C, et al; PHACESyndrome Research Conference. Consen-sus statement on diagnostic criteria forPHACE syndrome. Pediatrics. 2009;124(5):1447–1456
13. North PE, Waner M, James CA, MizerackiA, Frieden IJ, Mihm MC Jr. Congenitalnonprogressive hemangioma: a distinctclinicopathologic entity unlike infantilehemangioma. Arch Dermatol. 2001;137(12):1607–1620
14. North PE, Waner M, Mizeracki A, Mihm MC
Jr. GLUT1: a newly discovered immunohis-tochemical marker for juvenile hemangio-
mas. Hum Pathol. 2000;31(1):11–22
15. Airley R, Loncaster J, Davidson S, et al.
Glucose transporter GLUT-1 expressioncorrelates with tumor hypoxia and predicts
metastasis-free survival in advanced car-cinoma of the cervix. Clin Cancer Res. 2001;
7(4):928–934
16. Picard A, Boscolo E, Khan ZA, et al. IGF-2 andFLT-1/VEGF-R1 mRNA levels reveal dis-
tinctions and similarities between congen-ital and common infantile hemangioma.
Pediatr Res. 2008;63(3):263–267
17. Krol A, MacArthur CJ. Congenital heman-giomas: rapidly involuting and non-
involuting congenital hemangiomas. ArchFacial Plast Surg. 2005;7(5):307–311
18. Mulliken JB, Bischoff J, Kozakewich HP.Multifocal rapidly involuting congenital
hemangioma: a link to chorangioma. Am JMed Genet A. 2007;143A(24):3038–3046
19. Walter JW, North PE, Waner M, et al. So-
matic mutation of vascular endothelialgrowth factor receptors in juvenile hem-
angioma. Genes Chromosomes Cancer.2002;33(3):295–303
e1780 PATRICK et al by guest on July 29, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2013-2970 originally published online May 26, 2014; 2014;133;e1777Pediatrics
Iris Rubin and Albert K. OhLauren M. Patrick, Christine Oh, Nancy Bauman, Bhupender Yadav, Philip Guzetta,Rapid Involuting Congenital Hemangioma in the Setting of PHACE Association
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/133/6/e1777including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/133/6/e1777#BIBLThis article cites 19 articles, 5 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on July 29, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2013-2970 originally published online May 26, 2014; 2014;133;e1777Pediatrics
Iris Rubin and Albert K. OhLauren M. Patrick, Christine Oh, Nancy Bauman, Bhupender Yadav, Philip Guzetta,Rapid Involuting Congenital Hemangioma in the Setting of PHACE Association
http://pediatrics.aappublications.org/content/133/6/e1777located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1073-0397. 60007. Copyright © 2014 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on July 29, 2018www.aappublications.org/newsDownloaded from