random ecgs 2
TRANSCRIPT
Random ECGs 2
Dr Chris Cresswell
Emergency Physician
2015

62 year old with chest pain

Elderly patient, CP, ST elevation peaked Ts = ischaemia till proved otherwise

10 minutes later
• This is one of the reasons we do repeat ECGs– Another one is Wellen’s syndrome where the ECG with CP can look
normal, but the ECG when the pain has resolved may show marked anterior T wave inversion. Associated with critical LAD stenosis

22 F low GCS, no Hx available

Slightly wide complex. Dominant R in aVR
= Na channel blockade eg tricyclic

Went on to have a seizure then a wide complex tachy
Mx?

NaHCO3 1-2 mmol/kg boluses q5min til QRS < 120ms
Intubate and hyperventilate
(I don’t know if that doc came back to work)

82 F with CP and borderline low BP
How will you manage this, including important negatives?

Inferior MI +/- posterior MI
Aspirin (+/- other anticoagulents)
Fentanyl
Avoid morphine and GTN
May need fluid load to improve LV filling
Revascularisation
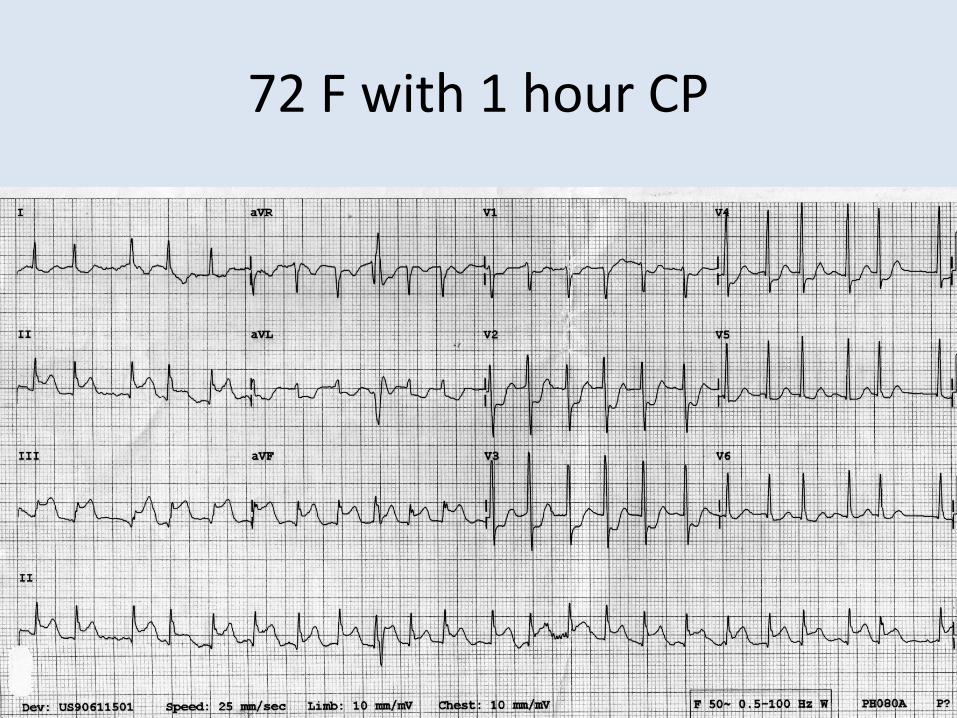
72 F with 1 hour CP

Same patientR sided ECG
Confirms RV infarct
Could also have done posterior leads which may or may not have shown a posterior STEMI

14 year old with CP

Looks like T wave inversion in I and avLBut P waves inverted in IDifferent morphology in I and V6 (look at the same area of heart)= incorrect lead placement

82 M diarrhoea x 8Palpitation
ICD firing repeatedlyTerrified
What is going on?What are you going to do?
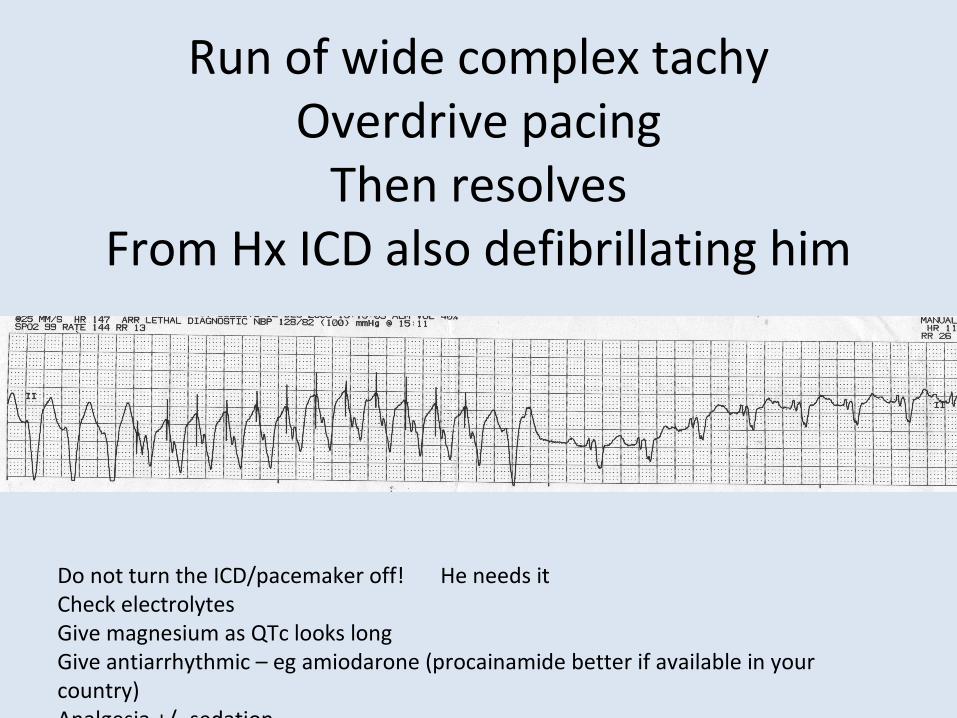
Run of wide complex tachyOverdrive pacing
Then resolvesFrom Hx ICD also defibrillating him
Do not turn the ICD/pacemaker off! He needs itCheck electrolytesGive magnesium as QTc looks longGive antiarrhythmic – eg amiodarone (procainamide better if available in your country)Analgesia +/- sedation

85 M with 1 hour of chest pain

Anterior sepatal STEMI + inferior ischaemia(inferior leads are not the reciprocal leads
of the septal leads)

Aspirin (+/- other anticoagulants/antiplatelet agents)Analgesia
Revascularisation
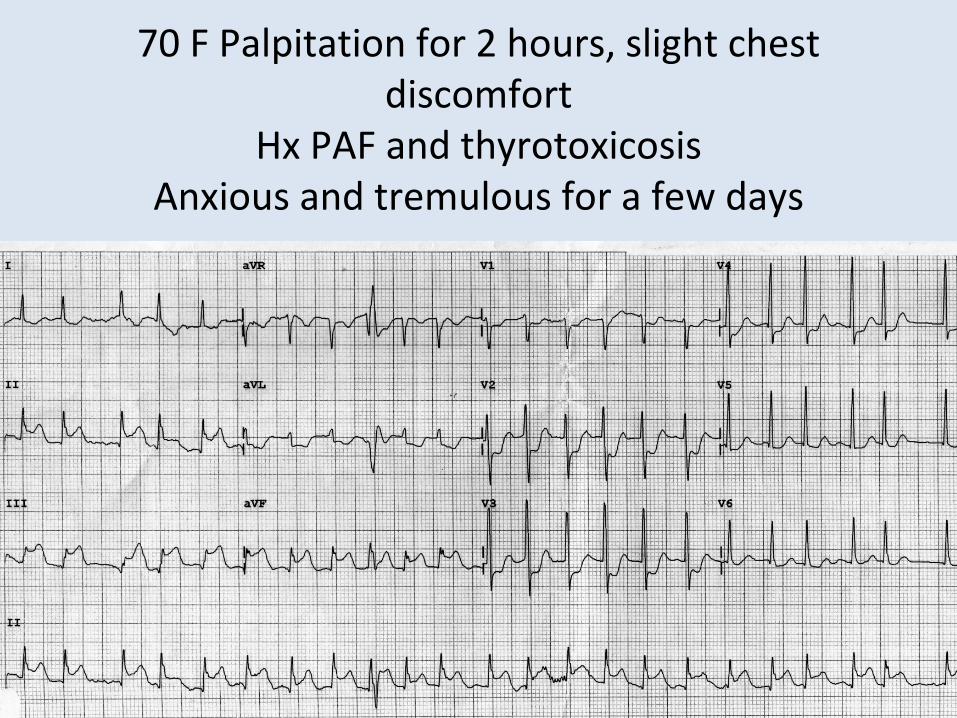
70 F Palpitation for 2 hours, slight chest discomfort
Hx PAF and thyrotoxicosisAnxious and tremulous for a few days

Inferior STEMI and fast AF (AF with RVR)
What are you going to do?

Inferior STEMI and fast AF (AF with RVR)
What are you going to do?
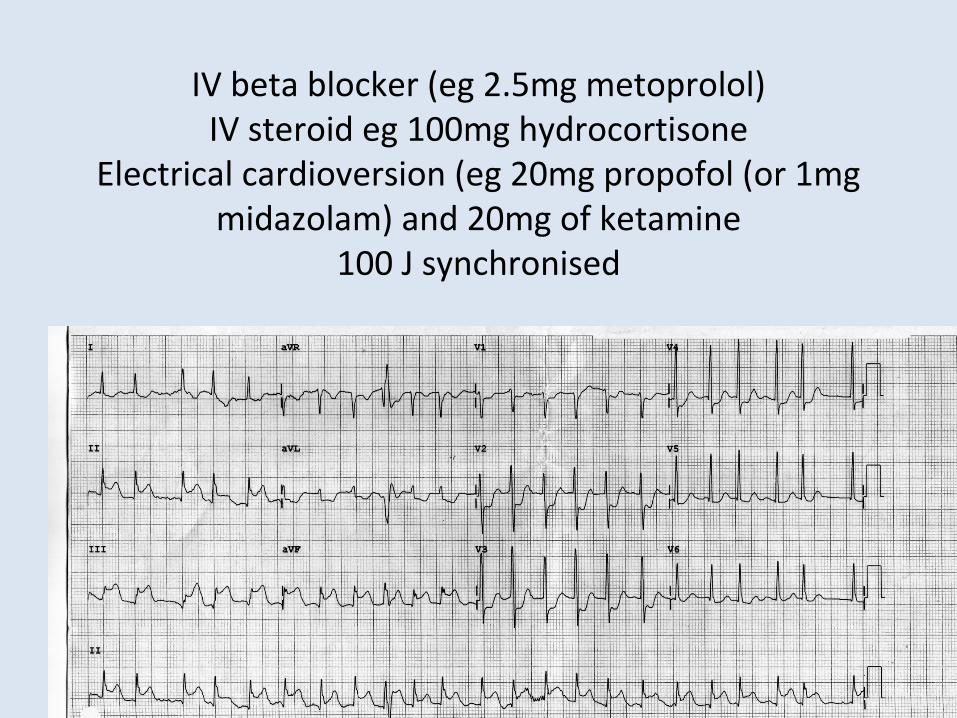
IV beta blocker (eg 2.5mg metoprolol)IV steroid eg 100mg hydrocortisone
Electrical cardioversion (eg 20mg propofol (or 1mg midazolam) and 20mg of ketamine
100 J synchronised

OopsHypoperfusion from tachycardia
Now hypoperfusion from bradycardia
What now?

Support blood pressure with fluids if needed
Aspirin and reperfusion
(had RV infarct also)

18 year old with glandular fever for 2 weeks, dry, sore, miserable HR noted
to be 170

No p wavesregular
Narrow complex

Symptomatically better with IV fluids, and analgesia
No response to vagal manouevresRx adenosine (these days I would use diltiazem)

65 M CP

10 minutes later, pain free
Wellen’s syndrome – critical LAD stenosisDo not put on treadmill – they tend to drop dead

50 F found collapse at supermarketDecr GCS, hypotensive
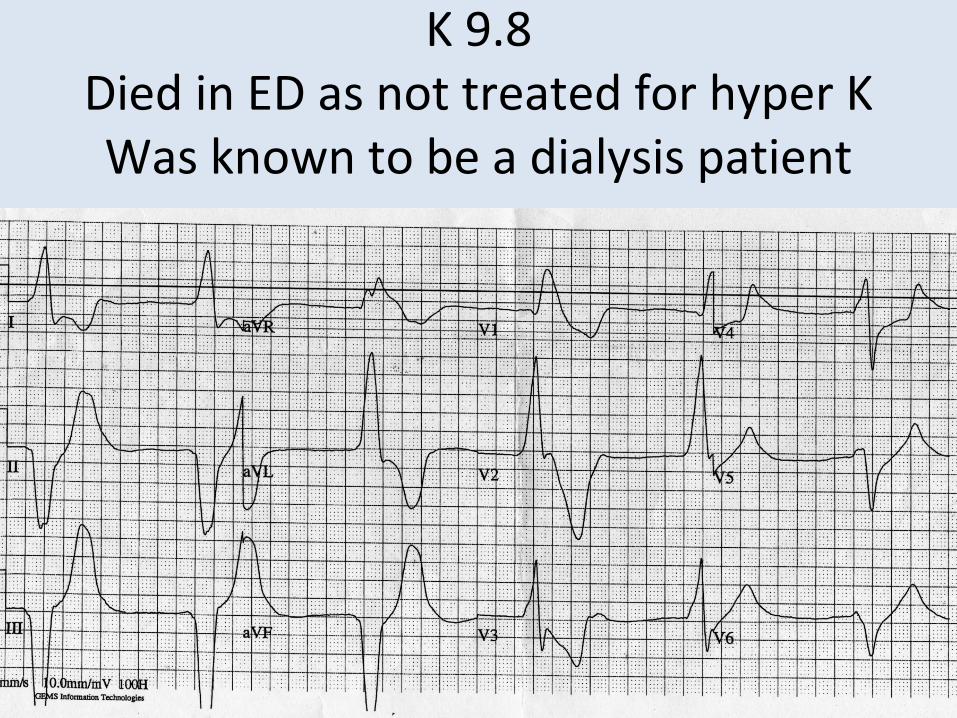
K 9.8Died in ED as not treated for hyper KWas known to be a dialysis patient

81 F palpitation, light headed for 3 hours. BP 110/50
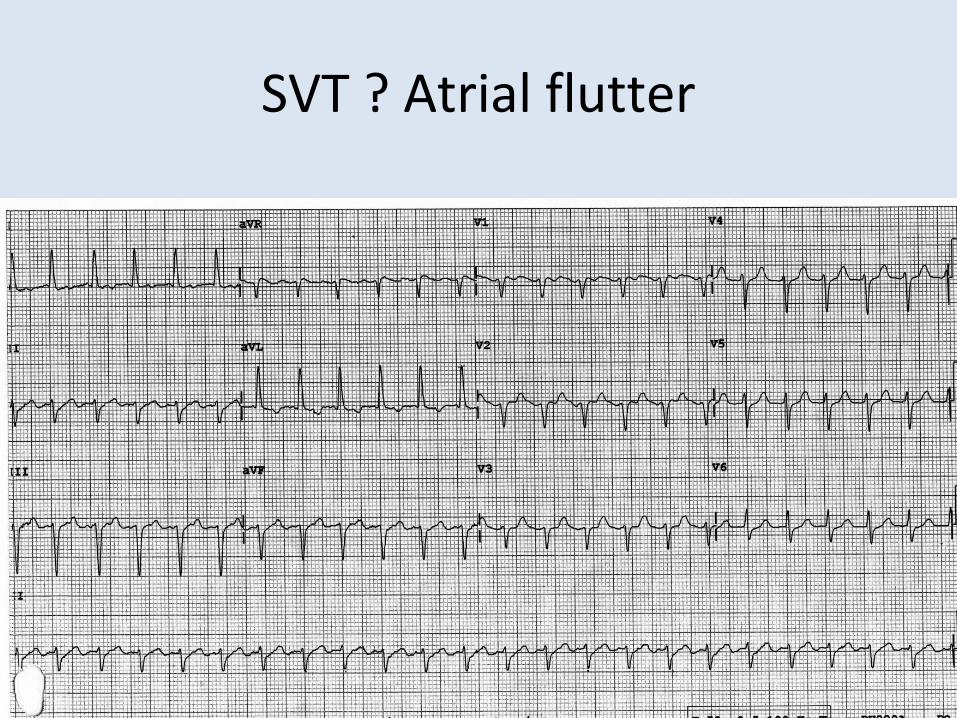
SVT ? Atrial flutter

Electrically cardioverted



Crap
What do you do now?

If conscious and no chest pain: nothing, hope it improves
If decr LOC: CPR +/- electrical or chemical pacing (eg 1mg of adrenalin in 1L saline dripping freely and titrated to effect, change to eg isoprenaline ASAP)
In patient improved spontaneouslyDr sent for clean underwear

45 F dialysis patient10 minutes into cardiac arrest

Assume hyperK
Continue CPR (unless advance directive)Rx Calcium gluconate 1g = 10ml of 1% repeat q 5minNaHCO3 2mmol/kgInsulin (actrapid) 10u and 50ml of 50% dextroseIV salbutamol 250µg
Intubate and PEEP as often pulmonary oedema from volume overload
Urgent dialysis

19 F with CP, no palpitation

Short PRDelta waves
WPWIncidental finding
T wave inversion aVL is concerning

92 F CP -> false teeth + palpitationNo cardiac Hx
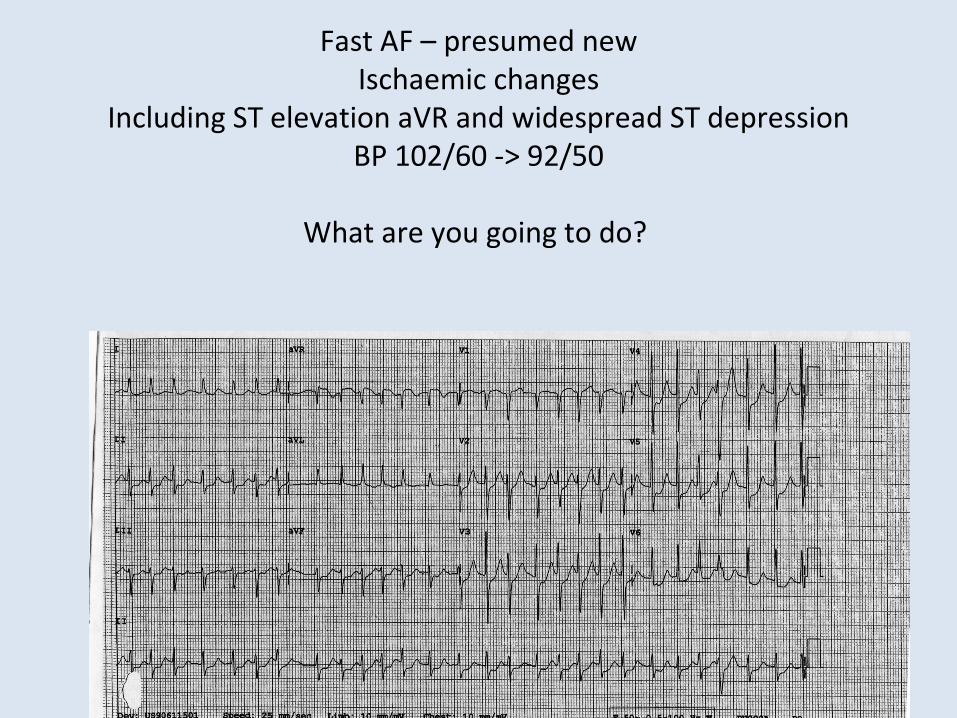
Fast AF – presumed newIschaemic changes
Including ST elevation aVR and widespread ST depressionBP 102/60 -> 92/50
What are you going to do?
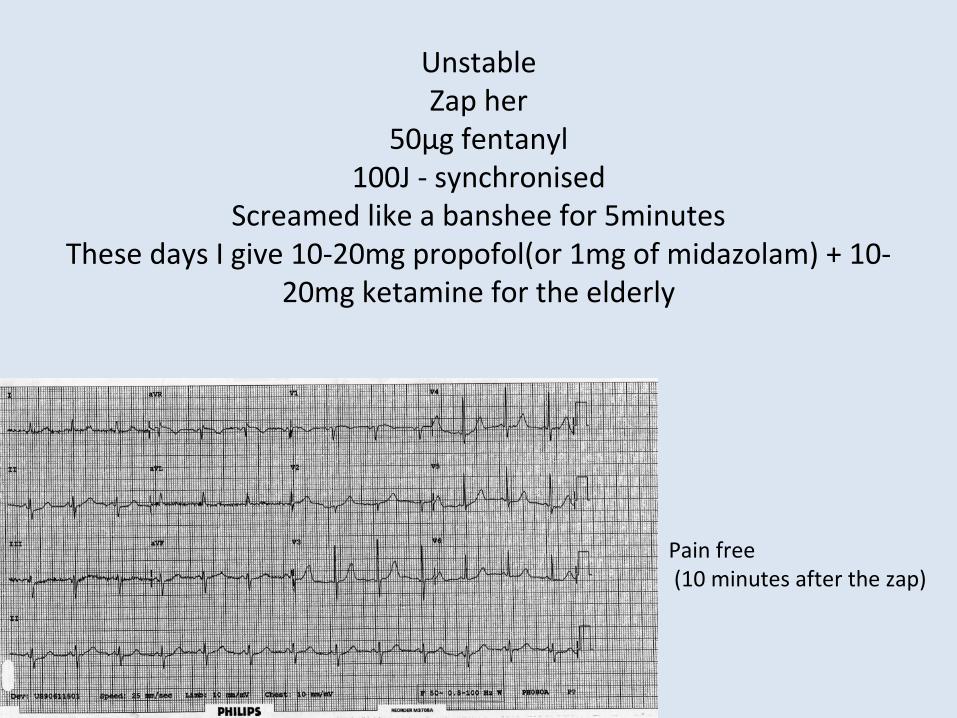
UnstableZap her
50µg fentanyl100J - synchronised
Screamed like a banshee for 5minutesThese days I give 10-20mg propofol(or 1mg of midazolam) + 10-
20mg ketamine for the elderly
Pain free (10 minutes after the zap)

56 M. Hx AF

Atrial flutter with variable block

Post 20mg IV diltiazem

78 F Weakness, collapse, nauseated, dizzy
Diarrhoea for a week. Hx AF. BP 141/52

78 F Weakness, collapse, nauseated, dizzy
Diarrhoea for a week. Hx AF. BP 141/52

Slow, irregular, no p waves, narrow complex= very slow AF
Diarrhoea for a week -> renal impairmentCreat 152 (GFR 29)
K 6.8 (3.4-5.2)Digoxin 3.14 (0.6-2.0)
Mx?

IV fluidDigoxin FAB eg Digibind or DigiFAB2 vials
Indications controversial:Digoxin level > therapeutic range + symptoms and signseg nausea, bradycardia, increased automaticity, hyperK
Don’t retest the digoxin level as assay measures free and bound digoxin -> no use
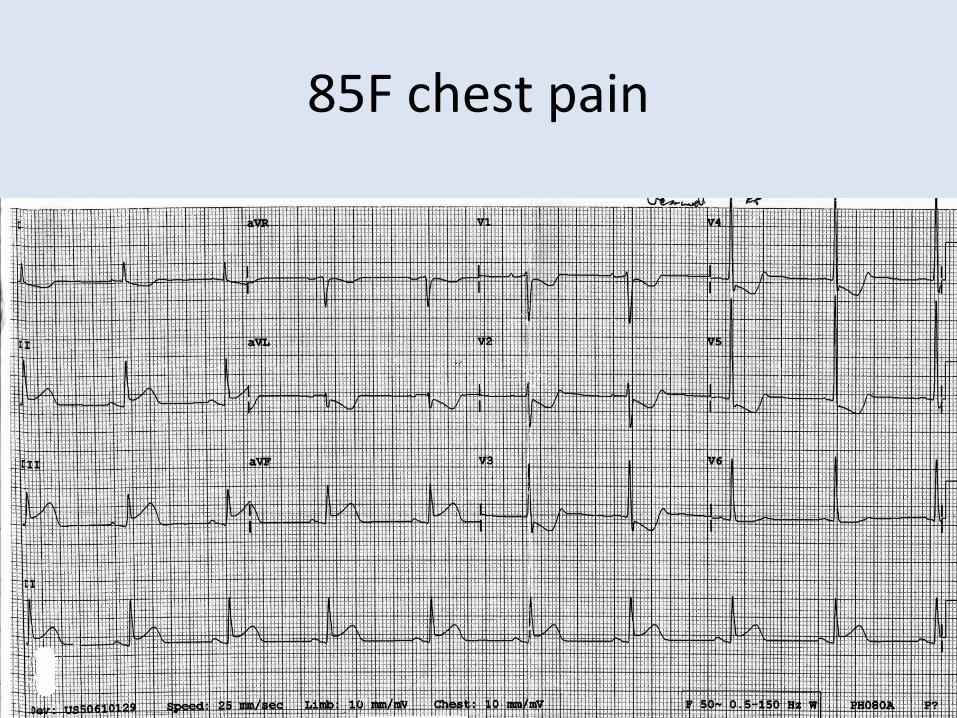
85F chest pain

Inferior STEMI +/- posterior and RV infarct
R sided and posterior ECG didn’t show posterior or RV infarcts

AspirinAnalgesia (still be cautious with GTN
and morphine)Revascularise -> thrombolysed

Chest pain worse, BP OKBugger
What now

Hearts do lots of funky things during or post revascularisation
• Support them through it• Fentanyl for pain• Fluid for hypotension• Electricity for fast VT or VF• Don’t treat idioventricular rhythms (slow VT, wide complex,
rate less than, say, 120

Some ECGs from Life in The Fast Lane