radiologic extranodal spread and matted nodes: important ... · showed evident metastases or if...
TRANSCRIPT

ORIGINAL ARTICLE
Radiologic extranodal spread and matted nodes: Important predictive factors fordevelopment of distant metastases in patients with high-risk head and neck cancer
Remco de Bree, MD, PhD,1,2* Redina Ljumanovic, MD, PhD,3 Marieke J. Hazewinkel, MD,4 Birgit I. Witte, PhD,5 Jonas A. Castelijns, MD, PhD6
1Department of Otolaryngology–Head and Neck Surgery, VU University Medical Center, Amsterdam, The Netherlands, 2Department of Head and Neck Surgical Oncology, UMCUtrecht Cancer Center, UMC Utrecht, Utrecht, The Netherlands, 3Department of Radiology, Advent Hospital Willemstad, Curacao, The Netherlands, 4Department of Radiology,Medisch Spectrum Twente, Enschede, The Netherlands, 5Department of Epidemiology and Biostatistics, VU University Medical Center, Amsterdam, The Netherlands, 6Departmentof Radiology, VU University Medical Center, Amsterdam, The Netherlands.
Accepted 26 August 2015
Published online 13 November 2015 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/hed.24257
Background. Different clinical high-risk factors for the development ofdistant metastases have been identified but not tested in the samecohort of patients with head and neck squamous cell carcinoma(HNSCC).Methods. In 145 patients with previously identified clinical high risk fac-tors, the presence of extranodal spread (ENS) and matted node on pre-treatment CT (n 5 96) and/or MRI (n 5 111) were determined.Results. Of 145 patients, ENS was detected in 87 patients (60.0%) andmatted nodes in 53 patients (36.6%). Kaplan–Meier curves for presenceor absence of ENS (on CT and/or MRI) and matted nodes (on CT) differ
significantly. In a Cox regression analysis, only ENS was a significantrisk factor (hazard ratio [HR] 5 3.3; 95% confidence interval [CI] 5 2.0–5.5; p < .001).Conclusion. In patients with high-risk HNSCC with clinically (palpably orradiologically) ENS and matted nodes, both determined radiologically,are high risk factors for development of distant metastases. VC 2015Wiley Periodicals, Inc. Head Neck 38: E1452–E1458, 2016
KEY WORDS: head and neck squamous cell carcinoma, distantmetastases, extranodal spread, matted nodes, risk factors
INTRODUCTIONHead and neck squamous cell carcinoma (HNSCC) isconsidered a predominantly locoregional disease. Theincidence of distant metastasis in HNSCC is relativelylow but remains a major determinant of prognosis andtherefore an important factor in clinical decision-making.1
Patients with distant metastases are generally not consid-ered curable and almost always receive only palliativetreatment.2 Pretreatment detection of distant metastasesmay avoid futile extensive locoregional treatments withunnecessarily burden to the patient and use and costs ofhealth resources.
The incidence of distant metastases from HNSCC isgenerally too low to warrant an extensive radiologicalstaging for distant metastases.3 In the Surveillance, Epide-miology, and End Results database, distant metastaseswere reported in 2066 of 73,247 patients with HNSCC(2.82%).4 This low number of distant metastases in unse-lected patients with HNSCC emphasizes the need forselection based on risk factors. Selection can be based onclinical factors and biomarkers. In a series on advanced-stage HNSCC only, the percentages are, not surprisingly,higher. Alvi and Johnson5 reported on a cohort of 130
patients with advanced-stage HNSCC of which 30 (23%)developed distant metastasis as the initial site of failure.Leemans et al6 found that patients with HNSCC with atleast 1 lymph node metastasis had twice as much distantmetastases as did those with histopathologic absence(13.6% vs 6.9%). Moreover, patients with HNSCC withmore than 3 lymph node metastases on histopathologicalexamination of their neck dissection specimen had a riskof 46.8% for development of distant metastases. The pres-ence of extranodal spread (ENS), as found histopathologi-cally, meant a 3-fold increase in the incidence of distantmetastases, compared with patients without this feature(19.1% vs 6.7%).6 In a series of 2648 cases using theRadiation Therapy Oncology Group database, Leibelet al7 reported a significant higher distant metastases ratein case of locoregional recurrence: a 21% rate of distantmetastasis at 5 years of follow-up for patients who hadlocoregional disease control at 6 months after the start oftreatment, compared to 38% for patients who had locore-gional failure.
Histopathologically determined risk factors obtainedfrom the surgical specimen are generally not available forprimary treatment planning. Until now, no convincing dis-crimination between metastasizing and nonmetastasizingtumors based on gene expression profiling has beenfound.1,8 Several studies in patients with HNSCC havefound an association between standardized uptake valueof 18F-fluorodeoxyglucose (FDG) in primary tumor orlymph node metastases and the development of distant
*Corresponding author: R. de Bree, Department of Head and Neck SurgicalOncology, UMC Utrecht Cancer Center, University Medical Center Utrecht,Heidelberglaan 100, 3584 CX, Utrecht, The Netherlands.E-mail: [email protected]
E1452 HEAD & NECK—DOI 10.1002/HED APRIL 2016

metastases.9,10 However, because Haerle et al11 could notconfirm this association in patients with advanced-stageHNSCC, it is not clear if this predictive factor is inde-pendent of the aforementioned clinical factors. In addi-tion, an association between FDG standardized uptakevalue and ENS has been reported.12
J€ackel and Rausch13 found that screening is particularlyuseful in patients with advanced-stage disease, local and/or regional recurrences, and second primary tumors. Lohet al14 evaluated screening of patients with HNSCC usingchest CT and found clinically T4 and/or N2/3 to be riskfactors for the development of distant metastases. Leonget al15 found, in their series of 102 patients who under-went screening by chest X-ray and chest CT, that of thepatients with positive screening, 86% had clinically T3 orT4 disease and 71% had clinically N2 or N3 disease. In21% of patients with clinically advanced-stage disease(T3/4 and/or N2/3), Haerle et al11 detected distant metas-tases by positron emission tomography (PET)-CT andfollow-up.
In previous studies, we identified and validated as rele-vant high-risk factors: clinically (palpably and/or radio-logically) 3 or more lymph node metastases, bilaterallymph node metastases, lymph node metastases of 6 cmor larger, low jugular lymph node metastases, locore-gional recurrence, and second primary tumors. Usingthese selection criteria, distant metastases were detectedin 29% to 33% of the patients during initial screening orwithin 12 months’ follow-up after initial screening.16–18
In a previous MRI study at our institute in univariateanalysis, the only significant characteristics in lymphnode-positive patients associated with distant metastases-free survival were ENS and ipsilateral total lymph nodevolume, both determined by MRI. In multivariate analy-sis, ENS remained the only independent predictor withregard to distant metastases-free survival.19 Recently,Kann et al20 found that on CT radiologically, ENS is anindependent prognosticator of poor distant control andsurvival for oropharyngeal carcinoma.
Recently, matted nodes, defined as 3 nodes abuttingone another with loss of intervening fat that is replacedwith evidence of extracapsular spread, were identified asa novel marker of poor prognosis in oropharyngeal squa-mous cell carcinoma independent of established prognos-tic factors.21,22 By definition, all patients with mattednodes have ENS. Spector et al22 showed that ENS withmatted nodes had a worse overall and disease-specificsurvival as compared with patients without ENS andpatients with ENS and nonmatted nodes.
The purpose of this study was to examine if ENS andmatted nodes, both determined radiologically, are predic-tive for the development of distant metastases in patientswith HNSCC who underwent screening on distant metas-tases because of one or more of the aforementioned highrisk factors.
PATIENTS AND METHODSA retrospective study was performed on a consecutive
group of patients with head and neck cancer with highrisk factors who underwent screening on distant metasta-ses by chest CT and/or FDG-PET or FDG-PET-CT and/or whole body MRI between 1997 and 2010 at VU Uni-
versity Medical Center Amsterdam. One hundred forty-five patients with CT (n 5 96) and/or MRI (n 5 111) ofthe head and neck available were included. Institutionalapproval and a waiver for informed consent wereobtained because the daily clinical practice was notaffected in this retrospective study.
Of these 145 patients, 114 patients were men and 31were women. Clinically risk factors were 3 or morelymph node metastasis (n 5 34), bilateral lymph nodemetastasis (n 5 74), lymph node metastasis of 6 cm orlarger (n 5 29), low jugular lymph node metastasis (n 523), a locoregional recurrence (n 5 13), and a second pri-mary tumor (n 5 31), assessed by physical examination,MRI, CT, and/or biopsy. Some patients had more than 1high risk factor. The median age was 59 years (range,32–84 years). The primary HNSCC sites were oral cavity(n 5 26), oropharynx (n 5 69), hypopharynx (n 5 16),and larynx (n 5 35). Six patients had more than 1 pri-mary HNSCC tumor. Three patients had synchronous pri-mary lung cancer and 3 had esophageal cancer.Pathological primary tumor classification was T1 (n 5 9),T2 (n 5 33), T3 (n 5 40), T4 (n 5 47), and unknownprimary tumor (n 5 7). The pathological lymph nodeclassifications were N0 (n 5 20), N1 (n 5 9), N2 (n 582), and N3 (n 5 30) (Table 1). Locoregional recurrenceswere not restaged. All patients were discussed at multidis-ciplinary board meetings. Fifty-four patients underwentsurgery (with adjuvant [chemo]radiation in 26 patients),23 patients had radiotherapy only, 49 patients underwentprimary chemoradiation, and 19 patients had only pallia-tive treatment. Adjuvant radiotherapy varied from 60 to66 Gy and was combined with platinum-based chemother-apy in case of positive surgical margins or histologicalENS (only in recent years and in patients <70 years old).For primary radiotherapy, typically, 70 Gy was deliveredin 2 Gy/fraction and, on indication, combined with (con-current) platinum-based chemotherapy. None of thesepatients received induction chemotherapy.
Extranodal spread and matted nodes
CT and MRI were reviewed by 2 radiologists experi-enced in head and neck radiology (R.L. and M.H.). CTand MRI scans were scored for the presence or absenceof ENS and matted nodes. In a patient, if both CT andMRI scans were available, the results of the MRI wereused in analyses in which the findings of CT and MRIwere combined. The criterion for declaring ENS was aCT-positive or MRI-positive lymph node with capsularcontour irregularity and/or infiltration of adjacent planes.On CT and MRI matted nodes were defined as 3 nodesabutting one another with loss of intervening fat that isreplaced with evidence of ENS.
Distant metastases
Patients were considered to have distant metastases ifdistant metastases were detected during pretreatmentscreening (at the time of chest CT, PET-CT, FDG-PET-CT, and/or whole body MRI) or follow-up. Scoring crite-ria and follow-up were used as described previously.11,12
Histological confirmation was not available in all patients.Lesions were considered distant metastases if imaging
RADIOLOGIC EXTRANODAL SPREAD AND MATTED NODES AS PREDICTORS FOR DISTANT METASTASES
HEAD & NECK—DOI 10.1002/HED APRIL 2016 E1453

showed evident metastases or if suspicious lesions wereprogressive on follow-up scans. Median follow-up for allpatients was 16 months with a range of 0 to 211 monthsas measured from the date of CT or MRI of the head andneck. Eighteen patients had a follow-up without manifestdistant metastases in <12 months.
Statistical analysis
Data were entered in Microsoft office Excel 2011(Microsoft, Redmond, WA). Statistical analyses wereperformed using SPSS 22.0 (SPSS, Chicago, IL). TheMcNemar test was used to examine the associationbetween scoring for ENS and matted nodes on CT andMRI. The chi-square test was used to examine the associ-ation between ENS or matted nodes and the other high-risk factors. Estimates of distant metastases-free survivalwere computed by the Kaplan–Meier method for presenceor absence of each risk factor. The log-rank test was usedto test the statistically significance of differences betweenthese curves. The distant metastases–free survival wasdefined as the date of pretreatment CT or MRI to thedate of the detection of distant metastasis or to the dateof last known follow-up without distant metastasis, inwhich case patients were censored. Multivariable regres-sion models (Cox proportional hazard model for time todetection, and logistic regression for development) werebuilt via a forward selection procedure (p value < .05) inwhich all high-risk factors were included separately.These models enable the quantification of the influenceof the predictive variables with regard to the developmentand time to detection (within 12 months or ever) of dis-tant metastases. A p value of < .05 was considered statis-tically significant, a p value of < .1 was considered toindicate a trend.
RESULTSDistant metastases developed in 78 patients (53.8%),
whereas distant metastases occurred within 12 months in51 patients. Median time to detection of distant metastasisof all 78 patients with distant metastases was 7.0 months.The distant metastasis sites were lungs (n 5 61), bones(n 5 15), liver (n 5 9), skin (n 5 5), adrenal (n 5 1),stomach (n 5 2), and brains (n 5 1).
ENS was detected on 54 of the 96 (56.3%) CT scans,68 of the 111 (61.3%) MRI examinations, and in 87 of145 patients (60.0%) if the CT and MRI scan results werecombined, whereas matted nodes were detected on 34 ofthe 96 CT scans (35.4%), 39 of the 111 MRI examina-tions (35.1%), and in 53 of 145 patients (36.6%) if theCT and MRI were combined. In the 62 patients with CTand MRI, no difference was found between scoring ofENS (p 5 .50) and matted nodes (p 5 1.00). Therefore,in further analyses, scorings on CT and MRI will fre-quently be combined.
Development of distant metastases
In univariate analysis, risk factors significantly associatedwith development of distant metastases (regardless of time)were ENS (p 5 .005) and bilateral lymph node metastases(p 5 .039). For the development of distant metastaseswithin 12 months, these factors were ENS (p < .001) and
lymph node metastasis 6 cm or larger (p 5 .049). Therewas a trend for matted nodes (p 5 .054).
In a Cox proportional hazard model using all risk fac-tors, only ENS was significant (hazard ratio [HR] 5 3.3;95% confidence interval [CI] 5 2.0–5.5; p < .001). In alogistic regression analysis (regardless of time), only ENSand matted nodes were significant risk factors (OR 55.1; 95% CI 5 2.0–13.3; p 5 .001 and OR 0.35, 95% CI0.13–0.90; p 5 0.030, respectively).
Distant metastases-free survival
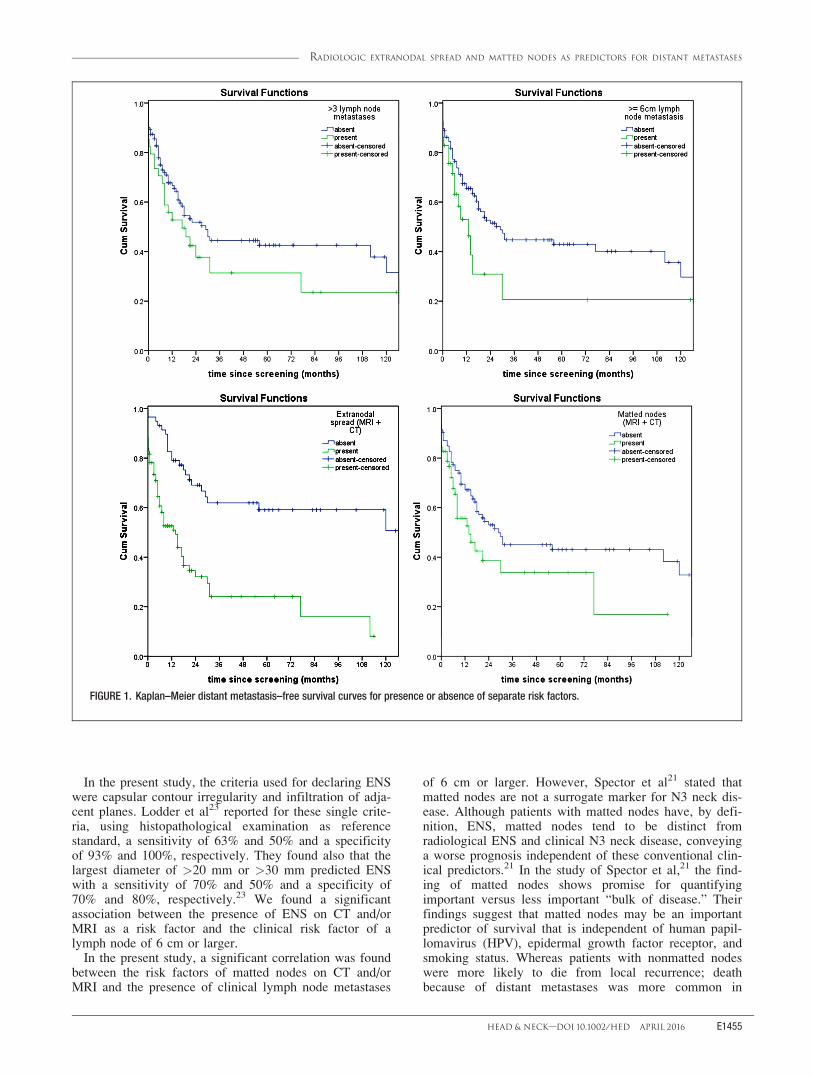
For all risk factors separately (some patients had morethan 1 risk factor), distant metastases-free survival curveswere constructed, which are shown in Figure 1. Only thecurves for bilateral lymph node metastases, second pri-mary tumors, ENS (on CT and/or MRI), and mattednodes (only on CT) differ significantly. There was a trendfor lymph node metastasis of 6 cm or larger (Table 2).
In the group of patients with lymph node metastasis of6 cm or larger (n 5 29), ENS (n 5 27) was not associ-ated with development of distant metastasis (p 5 0.423),whereas, in the group of patients without lymph nodemetastasis of 6 cm or larger (n 5 116), ENS (n 5 60)was a predictive factor (p < .001; Figure 2). In thegroups of patients with and without lymph node metasta-sis of 6 cm or larger, the presence of matted nodes (n 526 and n 5 26, respectively) was not associated withdevelopment of distant metastasis (p 5 .256 and p 5.585, respectively).
After stratifying for the presence (n 5 34) or absence(n 5 111) of more than 3 lymph node metastases, thepresence of ENS (n 5 25 and n 5 62, respectively) wasstill associated with distant metastases (p 5 .010 and p <.001, respectively). The presence of matted nodes (n 514 and n 5 38, respectively) was not associated with dis-tant metastases (p 5 .117 and p 5 .351, respectively)after stratifying for the presence or absence of >3 lymphnode metastases.
Association between risk factors
ENS on CT or MRI was associated with lymph nodemetastases 6 cm or larger (p < .001), second primarytumors (p < .001), locoregional recurrence (p 5 .004),and bilateral lymph node metastases (p 5 .025). Mattednodes on CT or MRI was associated with lymph nodemetastases 6 cm or larger (p < .001) and second primarytumors (p < .001). For other risk factors, no significantassociation with ENS or matted nodes was found.
DISCUSSIONIn the present study, 78 of 145 patients (53.8%) with
high-risk HNSCC were diagnosed with distant metastasesduring screening and follow-up. In these patients with atleast 1 high risk factor, ENS and matted nodes were themost significant risk factors for the development of distantmetastases. Because of this high incidence of distantmetastases, all patients with HNSCC with high risk factorsshould undergo pretreatment screening for distant metasta-ses. Moreover, these high risk factors can be used to selectpatients for intensification of treatment when agents forcurative treatment of distant metastases become available.
DE BREE ET AL.
E1454 HEAD & NECK—DOI 10.1002/HED APRIL 2016
In the present study, the criteria used for declaring ENSwere capsular contour irregularity and infiltration of adja-cent planes. Lodder et al23 reported for these single crite-ria, using histopathological examination as referencestandard, a sensitivity of 63% and 50% and a specificityof 93% and 100%, respectively. They found also that thelargest diameter of >20 mm or >30 mm predicted ENSwith a sensitivity of 70% and 50% and a specificity of70% and 80%, respectively.23 We found a significantassociation between the presence of ENS on CT and/orMRI as a risk factor and the clinical risk factor of alymph node of 6 cm or larger.
In the present study, a significant correlation was foundbetween the risk factors of matted nodes on CT and/orMRI and the presence of clinical lymph node metastases
of 6 cm or larger. However, Spector et al21 stated thatmatted nodes are not a surrogate marker for N3 neck dis-ease. Although patients with matted nodes have, by defi-nition, ENS, matted nodes tend to be distinct fromradiological ENS and clinical N3 neck disease, conveyinga worse prognosis independent of these conventional clin-ical predictors.21 In the study of Spector et al,21 the find-ing of matted nodes shows promise for quantifyingimportant versus less important “bulk of disease.” Theirfindings suggest that matted nodes may be an importantpredictor of survival that is independent of human papil-lomavirus (HPV), epidermal growth factor receptor, andsmoking status. Whereas patients with nonmatted nodeswere more likely to die from local recurrence; deathbecause of distant metastases was more common in
FIGURE 1. Kaplan–Meier distant metastasis–free survival curves for presence or absence of separate risk factors.
RADIOLOGIC EXTRANODAL SPREAD AND MATTED NODES AS PREDICTORS FOR DISTANT METASTASES
HEAD & NECK—DOI 10.1002/HED APRIL 2016 E1455

patients with matted nodes.21 In a more recent study,Spector et al22 found a sensitivity of 93%, a specificity of92%, a positive predictive value of 66%, and a negativepredictive value of 99% for the prediction of distantmetastases by the presence or absence of matted nodes.The authors state that the predictive value of mattednodes needs to be validated in more than 1 institute.22 Asfar as we are aware of, the present study is the first studythat validated matted nodes as a high risk factor fordevelopment of distant metastasis outside the Universityof Michigan Health System.
Since a strong association of radiologically ENS andlymph node metastasis of clinically 6 cm or larger wasfound and most patients (93%) with lymph node metasta-sis of 6 cm or larger had ENS, ENS and matted nodeswere not predictive factors for development of distantmetastasis in patients with N3 disease. However, ENSwas also found in 52% of patients without lymph nodemetastasis of 6 cm or larger and seemed to be a predic-tive factor for distant metastasis in these patients. There-fore, ENS seems to be a risk factor independent of N3.Matted nodes seemed to be a risk factor for distant metas-tases, but not if already stratified for N3 disease or in thepresence of >3 lymph node metastases. This can beexplained by the strong association between matted nodesand lymph node metastasis of 6 cm or larger and the defi-nition of matted nodes: 3 nodes abutting one another withloss of intervening fat that is replaced with evidence ofENS.
There were several potential weaknesses in this study.These retrospectively included patients who underwentCT and/or MRI using different scanners and protocolsover a long period of time. Because ENS and mattednodes are anatomic parameters, bias may have been lim-ited. In this study, ENS was defined radiologically. Sev-eral studies have tried to identify a set of radiologicalcharacteristics predictive for ENS on CT and/or MRI.
These characteristics include: capsular contour irregularityand/or infiltration of adjacent lanes; presence ofnoncontrast-enhancing parts inside a lymph node; irregu-lar contrast enhancement; and central nodal necrosis.Using one or more of these characteristics, sensitivity of60% to 95% and specificity of 72% to 100% have beenreported.23 However, because consensus among patholo-gist on the detection of ENS by histopathological exami-nation (the current gold standard) is not satisfactory,24 thevalue of these accuracy data is debatable. CT and MRIwill only score macroscopic ENS, whereas by using histo-pathology also microscopic ENS will be assessed. How-ever, macroscopic, radiologically determined, ENS isprobably prognostically more important than microscopicENS.25 Therefore, for the pretreatment identification ofradiologically ENS as a high risk factor, only the directassociation with the development of distant metastasis isof importance. In this retrospective study, HPV status ofthe included patients is not known. HPV-positive HNSCChas a different biological behavior than HPV-negativeHNSCC. However, Kann et al20 did not find a differencein presence of radiological ENS between HPV-positiveand HPV-negative patients with advanced oropharyngealcarcinoma. Moreover, HPV was not a predictive factorfor distant control.20 In patients with second primaryHNSCC tumors and distant metastases, these distantmetastases are likely to develop from the newly diag-nosed HNSCC, although it may also be from a previouslytreated HNSCC or synchronous lung or esophageal cancer(the latter was only represented by a few cases in thisstudy).
To prevent patients with distant metastases from exten-sive unnecessary locoregional treatment, patients withHNSCC with clinically 3 or more lymph node metastases,bilateral lymph node metastases, lymph node metastasesof 6 cm or larger, low jugular lymph node metastases,locoregional recurrence and second primary tumors, and
TABLE 2. Differences in Kaplan–Meier distant metastasis–free survivalcurves for each risk factor.
Risk factor
No. of patientswith / without risk
factorDifference,
p value
Lymph node metastases >3 34 / 111 .164Bilateral lymph nodemetastases
74 / 71 .017
Lymph node metastasis �6 cm 29 / 116 .065Low jugular lymph nodemetastasis
23 / 122 .116
Locoregional recurrence 13 / 132 .727Second primary tumor 31 / 114 .034ENS (MRI) 68 / 43 < .001ENS (CT) 54 / 42 < .001ENS (MRI 1 CT) 87 / 58 < .001Matted nodes (MRI) 38 / 73 .610Matted nodes (CT) 33 / 63 .014Matted nodes (MRI 1 CT) 52 / 93 .066
Abbreviation: ENS, extranodal spread.The figures in bold indicate statistical significance.Some of these curves are shown in Figures 1 and 2.
TABLE 1. Patient and tumor characteristics.
Variables No. of patients
SexMale 114Female 31
Age, yMedian (range) 59 (32–84)
Primary tumor siteOral cavity 26Oropharynx 69Hypopharynx 16Larynx 35Unknown primary 7
T classificationT1 9T2 33T3 40T4 47
N classificationN0 20N1 9N2 82N3 30
DE BREE ET AL.
E1456 HEAD & NECK—DOI 10.1002/HED APRIL 2016

particularly those with ENS and matted nodes shouldundergo pretreatment screening for distant metastases.
Because many patients currently undergo nonsurgicaltreatment, radiologically prognostic and predictive factorsare warranted to identify patients who may benefit fromsystemic treatment or closer follow-up to detect and treatoligometastases early when they become manifest. In thepostoperative setting, the presence of ENS is consideredto be an indication to add concurrent chemotherapy toradiotherapy to improve locoregional control and overallsurvival.26,27 Patients with HPV-associated tumors andone of these risk factors for distant metastases are prob-ably not good candidates for deescalation studies.22
Multivariate analysis showed that ENS and mattednodes are the only significant risk factors within thishigh-risk patient group. In clinical practice, the time inter-val between screening and detection of clinically evidentdistant metastases, within which extensive treatment isconsidered futile, is generally 12 months.28 Therefore, themost important high risk factors for screening of distantmetastases from the present study are radiological ENS,clinically lymph node metastases of 6 cm or larger, andradiologically matted nodes.
CONCLUSIONIn this retrospective study of patients with already at
least 1 high risk factor, ENS and matted nodes were bothimportant risk factors for the development of distantmetastases. The predictive value of these high risk factorsfor the development of distant metastases was validated.Patients with HNSCC with clinically (palpably or radio-logically) 3 or more lymph node metastases, bilaterallymph node metastases, lymph node metastases of 6 cmor larger, low jugular lymph node metastases, locore-gional recurrence and second primary tumors, and partic-
ularly those with ENS and matted nodes should undergopretreatment screening for distant metastases.
REFERENCES1. Takes RP, Rinaldo A, Silver CE, et al. Distant metastases from head and
neck squamous cell carcinoma. Part I. Basic aspects. Oral Oncol 2012;48:775–779.
2. Haigentz M Jr, Hartl DM, Silver CE, et al. Distant metastases from headand neck squamous cell carcinoma. Part III. Treatment. Oral Oncol 2012;48:787–793.
3. de Bree R, Haigentz M Jr, Silver CE, et al. Distant metastases from headand neck squamous cell carcinoma. Part II. Diagnosis. Oral Oncol 2012;48:780–786.
4. Kuperman DI, Auethavekiat V, Adkins DR, et al. Squamous cell cancer ofthe head and neck with distant metastasis at presentation. Head Neck 2011;33:714–718.
5. Alvi A, Johnson JT. Development of distant metastasis after treatment ofadvanced-stage head and neck cancer. Head Neck 1997;19:500–505.
6. Leemans CR, Tiwari R, Nauta JJ, van der Waal I, Snow GB. Regionallymph node involvement and its significance in the development of distantmetastases in head and neck carcinoma. Cancer 1993;71:452–456.
7. Leibel SA, Scott CB, Mohiuddin M, et al. The effect of local-regional con-trol on distant metastatic dissemination in carcinoma of the head and neck:results of an analysis from the RTOG head and neck database. Int J RadiatOncol Biol Phys 1991;21:549–556.
8. Braakhuis BJ, Senft A, de Bree R, et al. Expression profiling and predictionof distant metastases in head and neck squamous cell carcinoma. J ClinPathol 2006;59:1254–1260.
9. Suzuki H, Hasegawa Y, Terada A, et al. FDG-PET predicts survival and distantmetastasis in oral squamous cell carcinoma. Oral Oncol 2009;45:569–573.
10. Yao M, Lu M, Savvides PS, et al. Distant metastases in head-and-necksquamous cell carcinoma treated with intensity-modulated radiotherapy. IntJ Radiat Oncol Biol Phys 2012;83:684–689.
11. Haerle SK, Schmid DT, Ahmad N, Hany TF, Stoeckli SJ. The value of (18)F-FDG PET/CT for the detection of distant metastases in high-risk patients withhead and neck squamous cell carcinoma. Oral Oncol 2011;47:653–659.
12. Kubicek GJ, Champ C, Fogh S, et al. FDG-PET staging and importance oflymph node SUV in head and neck cancer. Head Neck Oncol 2010;2:19.
13. J€ackel MC, Rausch H. Distant metastasis of squamous epithelial carcino-mas of the upper aerodigestive tract. The effect of clinical tumor parame-ters and course of illness [in German]. HNO 1999;47:38–44.
14. Loh KS, Brown DH, Baker JT, Gilbert RW, Gullane PJ, Irish JC. A rationalapproach to pulmonary screening in newly diagnosed head and neck can-cer. Head Neck 2005;27:990–994.
15. Leong SC, Javed F, Elliot S, Mortimore S. Effectiveness of X-ray and com-puted tomography screening for assessing pulmonary involvement inpatients with head and neck squamous cell carcinoma. J Laryngol Otol2008;122:961–966.
FIGURE 2. Kaplan–Meier distant metastasis-free survival curves for presence or absence of extranodal spread (ENS) within the group of patientswithout lymph node metastasis of 6 cm or larger.
RADIOLOGIC EXTRANODAL SPREAD AND MATTED NODES AS PREDICTORS FOR DISTANT METASTASES
HEAD & NECK—DOI 10.1002/HED APRIL 2016 E1457

16. de Bree R, Deurloo EE, Snow GB, Leemans CR. Screening for distantmetastases in patients with head and neck cancer. Laryngoscope 2000;110(3 Pt 1):397–401.
17. Brouwer J, de Bree R, Hoekstra OS, et al. Screening for distant metastasesin patients with head and neck cancer: is chest computed tomography suffi-cient? Laryngoscope 2005;115:1813–1817.
18. Senft A, de Bree R, Hoekstra OS, et al. Screening for distant metastases inhead and neck cancer patients by chest CT or whole body FDG-PET: a pro-spective multicenter trial. Radiother Oncol 2008;87:221–229.
19. Ljumanovic R, Langendijk JA, Hoekstra OS, Leemans CR, Castelijns JA.Distant metastases in head and neck carcinoma: identification of prognosticgroups with MR imaging. Eur J Radiol 2006;60:58–66.
20. Kann BH, Buckstein M, Carpenter TJ, et al. Radiographic extracapsularextension and treatment outcomes in locally advanced oropharyngeal carci-noma. Head Neck 2014;36:1689–1694.
21. Spector ME, Gallagher KK, Light E, et al. Matted nodes: poor prognosticmarker in oropharyngeal squamous cell carcinoma independent of HPVand EGFR status. Head Neck 2012;34:1727–1733.
22. Spector ME, Gallagher KK, Bellile E, et al. Patterns of nodal metastasisand prognosis in human papillomavirus-positive oropharyngeal squamouscell carcinoma. Head Neck 2014;36:1233–1240.
23. Lodder WL, Lange CA, van Velthhuysen ML, et al. Can extranodal spreadin head and neck cancer be detected on MR imaging. Oral Oncol 2013;49:626–633.
24. van den Brekel MW, Lodder WL, Stel HV, Bloemena E, Leemans CR, vander Waal I. Observer variation in the histopathological assessment of extra-nodal tumor spread in lymph node metastases in the neck. Head Neck2012;34:840–845.
25. Ferlito A, Rinaldo A, Devaney KO, et al. Prognostic significance of micro-scopic and macroscopic extracapsular spread from metastatic tumor in thecervical lymph nodes. Oral Oncol 2002;38:747–751.
26. Bernier J, Domenge C, Ozsahin M, et al. Postoperative irradiation with orwithout concomitant chemotherapy for locally advanced head and neckcancer. New Engl J Med 2004;350:1945–1952.
27. Cooper JS, Pajak TF, Forastiere AA, et al. Postoperative concurrent radio-therapy and chemotherapy for high-risk squamous-cell carcinoma of thehead and neck. New Engl J Med 2004;350:1937–1944.
28. Brouwer J, Bree R, Hoekstra OS, Langendijk JA, Castelijns JA, LeemansCR. Screening for distant metastases in patients with head and neck can-cer: what is the current clinical practice? Clin Otolaryngol 2005;30:438–443.
DE BREE ET AL.
E1458 HEAD & NECK—DOI 10.1002/HED APRIL 2016