radiologic assessment of total hip arthroplasty:...
TRANSCRIPT

Radiologic Assessment of Total Hip Arthroplasty:
Loosening
Grant Garrigues, Harvard Medical SchoolGillian Lieberman, MD
Grant Garrigues, 2004Gillian Lieberman, MD March 2004

2
Anatomy
www.yoursurgery.com/ProcedureDetails.cfm?BR=5&Proc=27
Liner
Calcar
Stem
Acetabular Component
Femoral Component
www.hipandkneesurgery.net/hip_op.html
Grant Garrigues, 2004Gillian Lieberman, MD

3
Patient JQ
• 67 year-old man• Left THA 10 years
ago• Hip/thigh pain
Lucencies
Density
Position
PACS, MGH
Grant Garrigues, 2004Gillian Lieberman, MD
What do you see?
4
Implant loosening
• >500,000 THA and TKA each year in US• 10% are revisions of failed implants• Overall, very successful
• Aging population, obesity, more THA, younger patients vs.
• Improved surgical technique, implant design, and pharmacotherapy
Grant Garrigues, 2004Gillian Lieberman, MD
Bauer TW et al. Skeletal Rad, 1999.

5
Total Hip Complications• Deep Venous Thrombosis (fatal PE, 0.3%)• Nerve Palsies (1.7%)• Vascular Complications (0.25%)• Fracture/Perforations • Dislocation (2-2.5%)• Leg-length Discrepancy
• Loosening (10%)• Infection (1-5%)• Heterotopic Ossification (significant, 8%)
Short-term
Long-term
Namba RS et al. Current Ortho, 2003.
Grant Garrigues, 2004Gillian Lieberman, MD

6
Radiologic Assessment
• Assessment of long-term complications– Loosening is the most significant
• Plain films: great bone/metal visualization• Radiographic features
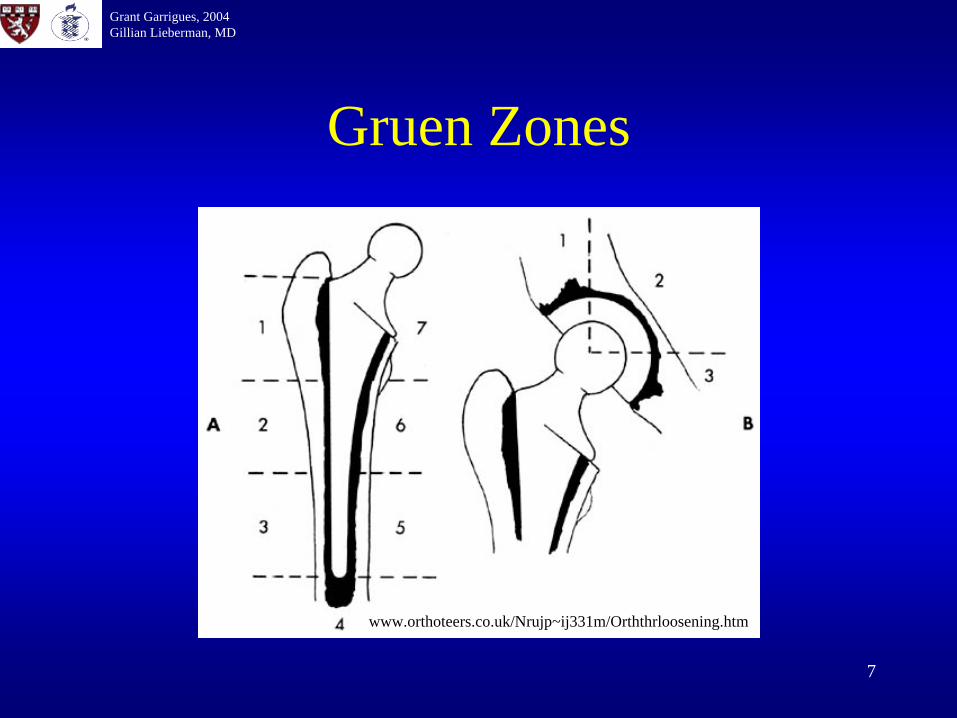
– Peri-implant lucency > 2mm• Describe using Gruen Zones (following slide)
– Stress views / Interval change in position
Keogh CF et al. AJR 2003.
Grant Garrigues, 2004Gillian Lieberman, MD
7
Gruen Zones
Grant Garrigues, 2004Gillian Lieberman, MD
www.orthoteers.co.uk/Nrujp~ij331m/Orththrloosening.htm

8Keogh CF et al. AJR 2003.
White LM et al. Radiology 2000.
Other Modalities
• Arthrography– Effective joint space
visualized– Aspirate and Biopsy
• CT and MRI– Metal artifact
• US and Nuclear medicine– Select applications
Keogh CF et al. AJR 2003.
Grant Garrigues, 2004Gillian Lieberman, MD
Griffiths HJ et al. Rad Clin 1995.

9
Ddx of Radiographic Loosening
• Peri-implant bone loss– Aseptic loosening– Infection– Stress Shielding / Adaptive remodeling– Aging / Osteoporosis
• Mechanical Failure – Catastrophic– Interfacial
Grant Garrigues, 2004Gillian Lieberman, MD
Bauer TW et al. Skeletal Rad, 1999.Tiggles S et al. AJR, 1994.

10
Aseptic Loosening
• Most common cause of TJR failure• Wear debris
– Most generated at the articulating surface– Submicron UHMWPE, HA, TiAlV, CoCr particles– Spread throughout the “effective joint space”– Phagocytosed by macrophages
• Induces bone resorption (osteolysis)• Formation of fibrous, granulomatous tissue
Willert and Semlitsch JBMR 1977.Shanbhag, et al. JOR 1994.
Grant Garrigues, 2004Gillian Lieberman, MD

11
Aseptic Loosening
Osteoclast inHowship’s lacuna
FBGC with wear debris
Interfacial Membrane
Bone Resorption
Courtesy of Arun Shanbhag, MD
Macrophages phagocytosewear debris, leading to twoprocesses.
12
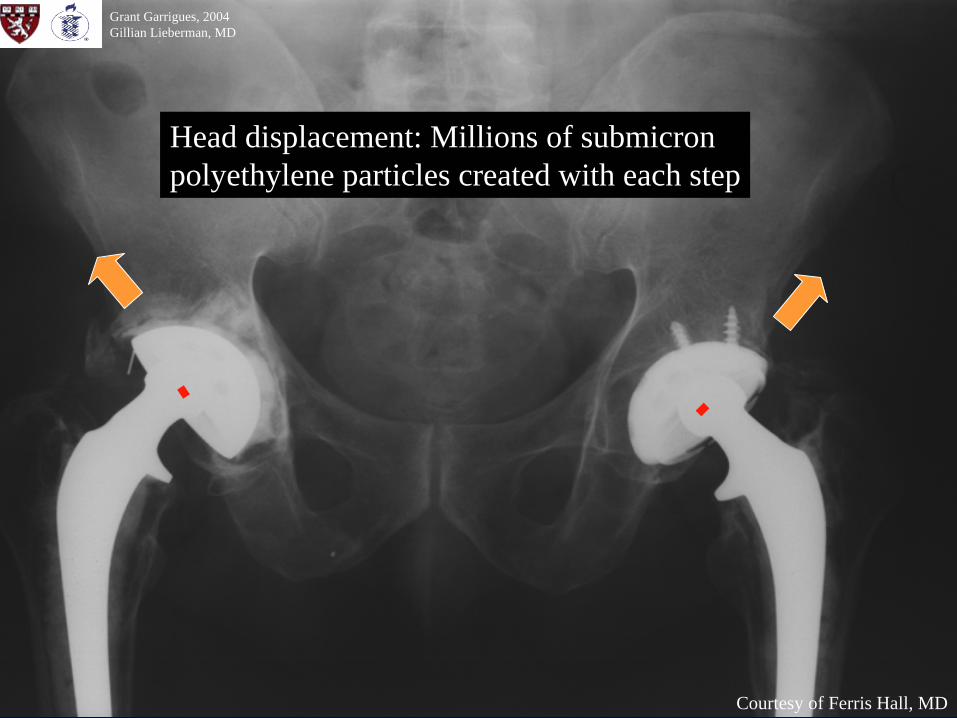
Head displacement: Millions of submicron polyethylene particles created with each step
Grant Garrigues, 2004Gillian Lieberman, MD
Courtesy of Ferris Hall, MD

13
Aseptic Loosening
• Wear debris is the prevailing theory• Hydrodynamic pressure may also
contribute to aseptic loosening– Early loosening from periprosthetic bone loss
• Trauma, chemicals, and thermal damage – Joint pressures >700 mmHg
• “Pumping action” of loosened implants• May cause aseptic loosening without particles• Similar to mechansim of subchondral cysts in OA
Grant Garrigues, 2004Gillian Lieberman, MD
Aspenberg P et al. Acta Ortho 1998.Mjoberg B et al. Ortho 1997.

14
Aseptic Loosening
Sequellae• Painful loosening• Revision arthroplasty• Pathologic fractures
Osteolysis leading to pathologic avulsion fracture
Grant Garrigues, 2004Gillian Lieberman, MD
PACS, MGHBerry DJ J Arthro 2003.

15
Septic Loosening
• Less common today– Laminar flow OR– UV lights– Prophylactic Antibiotics
• Foreign body nidus– Pathogens adhere to biomaterials– S. epidermidis produces glycocalyx
Grant Garrigues, 2004Gillian Lieberman, MD

16
Septic Loosening• Radiographs mimic aseptic
loosening• Dx often with arthrogram and
clinical correlation– Peri-implant bone loss– Sinus tracts– Joint fluid aspiration:
(culture, gram stain, etc.)– Synovial biopsy
• Nuclear Med– Tc-99m nonspecific– In-111 leukocytes preferred
Keogh CF et al. AJR, 2003.Griffiths HJ et al. Rad Clin, 1995.
Arthrogram:sinus tracts and abcesses
Grant Garrigues, 2004Gillian Lieberman, MD
Keogh CF et al. AJR, 2003.

17
Septic Loosening
Sequellae• Painful implant loosening• Revision arthroplasty
– Sterilize site before reimplantation– Antibiotic impregnated cement spacers
• Sepsis, osteomyelitis, sinus tracts
Grant Garrigues, 2004Gillian Lieberman, MD
Bauer TW et al. Skeletal Rad, 1999.

18
Stress Shielding• Loading transferred from bone to stiffer prosthesis
Abaqus, www.hks.com/solutions/sol_hip.html
Finite Element Analysis Interference Stress Interference + Load Stress
Proximal Stress
Distal Stress
Grant Garrigues, 2004Gillian Lieberman, MD
Friedman RJ et al. JBJS, 1993.

19
Stress Shielding
• Stress transferred through stem– Metal is stiffer than bone– Bypasses proximal periprosthetic bone
• Resorption of bone around proximal femoral shaft (Wolff’s Law)
• More common in uncemented• Increased risk of pathologic fracture
Jacobs JJ et al. Ortho Clin 1993.Friedman RJ et al. JBJS, 1993.
Grant Garrigues, 2004Gillian Lieberman, MD
Keogh CF et al. AJR 2003.

20
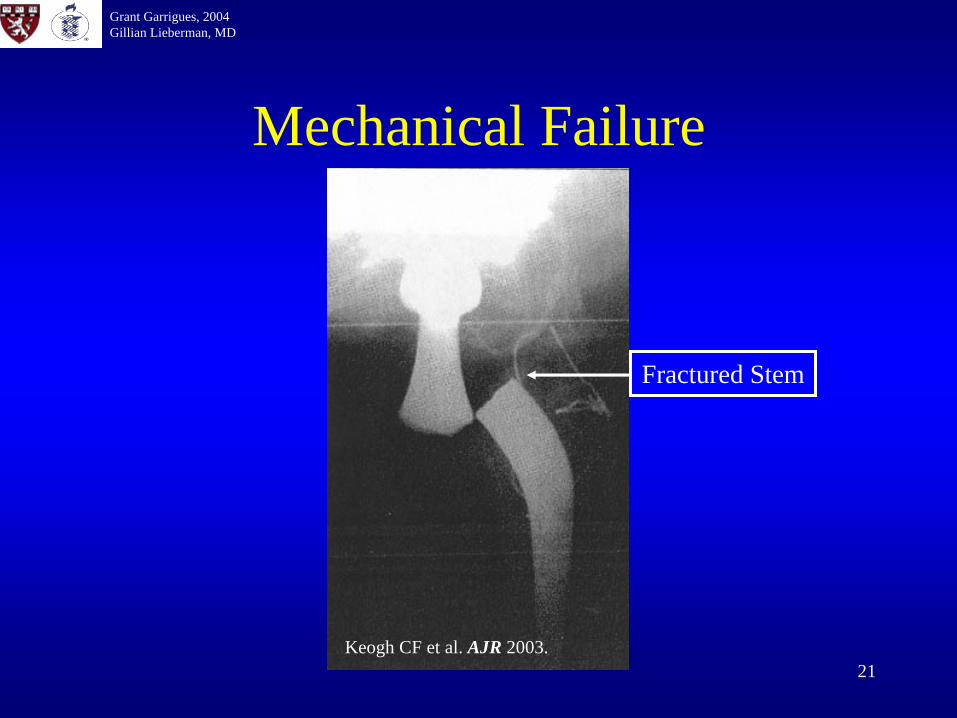
Mechanical Failure
• Catastrophic failure is rare– Fractured stem– Shattered Zirconia ceramic heads
• Interface failure most common– Cement fatigue fracture– Debonding of cement-implant interface– Porous coating fracture
Grant Garrigues, 2004Gillian Lieberman, MD
21
Mechanical Failure
Fractured Stem
Grant Garrigues, 2004Gillian Lieberman, MD
Keogh CF et al. AJR 2003.

22
Cement FractureDebonding: implant-cement interface isdisrupted
Subsidence: implant slides into medullarycanal
Grant Garrigues, 2004Gillian Lieberman, MD
Courtesy of Ferris Hall, MDCourtesy of Ferris Hall, MD
Cortical Reaction

23
Porous Coating FatiguePorous coatings, fiber-metal mesh, and other surfaces allow bone in-growth to cementless implants
Cross-section through fiber-metal mesh shows bone in-growth
Multiple loose beads
Grant Garrigues, 2004Gillian Lieberman, MD
PACS, BIDMCPACS, BIDMC

24
Summary: JQ
• 67 year-old man• Left THA • Hip/thigh pain
•Osteolytic Lesions
•Cortical Reaction•Stress Fracture
•Volumetric wear•Varus shift•Subsidence
PACS, MGH
Grant Garrigues, 2004Gillian Lieberman, MD
Aseptic Loosening of uncementedfemoral component

25
Other THA Complications
• We have discussed loosening, the most common complication of THA, in detail.
• Bonus cases of other radiographically assessable complications follow…

26
Grant Garrigues, 2004Gillian Lieberman, MD
Cement Venogram:cement forced into vein before hardening
Alastair et al. Brief report: fulminating fat embolism syndrome caused by paradoxical embolism through a patent foramen ovale, NEJM, 1993; 329(13):926-963.
Courtesy of Ferris Hall, MD
This is a powerful reminderof the possibility of fat emboli forced through bridging veinsby manipulation in the meduallary canal.
27
Grant Garrigues, 2004Gillian Lieberman, MD
Courtesy of Ferris Hall, MD
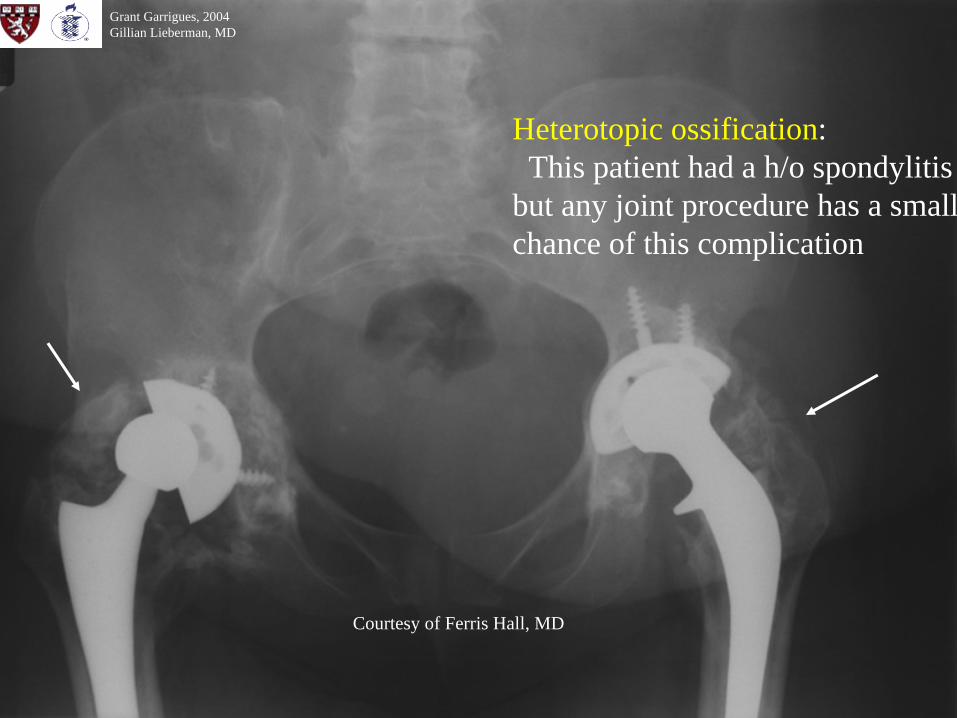
Heterotopic ossification:This patient had a h/o spondylitis
but any joint procedure has a smallchance of this complication

28
References• Aspenberg P, van der Vis H. Fluid pressure may cause periprosthetic osteolysis. Acta
Orthop Scand, 1998; 69(1):1-4.• Bauer TW, Schils J. The pathology of total joint arthroplasty. Skeletal Rad, 1999;
28:483-97.• Berry DJ. Periprosthetic fractures associated with osteolysis. J Arthrop, 2003; 18(3,
supl.):107-11.• Friedman RJ, et al. Current concepts in orthopaedic biomaterials and implant fixation.
JBJS, 1993; 75A(7):1086-109• Griffiths HJ, et al. “Total hip replacement and other orthopedic hip procedures” in Rad
Clinics of N America: Imaging of Orthopedic Hardware, 1995; 33(2):267-87.• Jacobs JJ, Sumner DR, Galante JO. Mechanisms of bone loss associated with total hip
replacement. Ortho Clin of N Amer; 1993; 24(4): 583-90.• Keogh CF, et al. Imaging of the painful hip arthroplasty. AJR, 2003; 180:115-20.• Mjoberg B. The theory of early loosening of hip prostheses. Orthopedics, 1997;
20(12):1169-75.• Namba RS, et al. “Adult reconstructive surgery” in Current Diagnosis and Treatment
in Orthopaedics, 3rd ed, Skinner HB ed.McGraw-Hill, 2003.• Shanbhag A, et al. J Ortho R, 1994• Tigges S, et al. Complications of hip arthroplasty causing periprosthetic radiolucency on
plain radiographs. AJR, 1994; 162:1387-91.• White LM, et al. Complications of total hip arthroplasty: MR imaging. Radiology, 2000;
215(1):254-62.• Willert and Semlitsch. JBMR, 1997
Grant Garrigues, 2004Gillian Lieberman, MD

29
Acknowledgements
Special Thanks to:• Ferris Hall, MD• Arun Shanbhag, PhD• Harry Rubash, MD• Pamela Lepkowski• Larry Barbaras• Gillian Lieberman, MD
Grant Garrigues, 2004Gillian Lieberman, MD