radiographic findings in captive falcons in saudi arabia
TRANSCRIPT
BioOne sees sustainable scholarly publishing as an inherently collaborative enterprise connecting authors, nonprofit publishers, academic institutions, researchlibraries, and research funders in the common goal of maximizing access to critical research.
Radiographic Findings in Captive Falcons in Saudi ArabiaAuthor(s): Jesus L. NaldoDVM and Jaime H. SamourMVZ, PhD, Dipl ECAMSSource: Journal of Avian Medicine and Surgery, 18(4):242-256. 2004.Published By: Association of Avian VeterinariansDOI: http://dx.doi.org/10.1647/2003-027URL: http://www.bioone.org/doi/full/10.1647/2003-027
BioOne (www.bioone.org) is a nonprofit, online aggregation of core research in the biological, ecological, andenvironmental sciences. BioOne provides a sustainable online platform for over 170 journals and books publishedby nonprofit societies, associations, museums, institutions, and presses.
Your use of this PDF, the BioOne Web site, and all posted and associated content indicates your acceptance ofBioOne’s Terms of Use, available at www.bioone.org/page/terms_of_use.
Usage of BioOne content is strictly limited to personal, educational, and non-commercial use. Commercial inquiriesor rights and permissions requests should be directed to the individual publisher as copyright holder.
242
Journal of Avian Medicine and Surgery 18(4):242–256, 2004q 2004 by the Association of Avian Veterinarians
Radiographic Findings in Captive Falcons inSaudi Arabia
Jesus L. Naldo, DVM, and Jaime H. Samour, MVZ, PhD, Dipl ECAMS
Abstract: Radiographic records were reviewed from 1702 falcons of different species that werepresented to the Falcon Specialist Hospital and Research Institute of the Fahad bin Sultan FalconCenter, Riyadh, Kingdom of Saudi Arabia, from September 1, 1998, to March 1, 2002. The mostcommon radiographic findings were homogeneous and nonhomogeneous increased radiopacity andlocalized soft-tissue densities of the lungs and air sacs, hepatomegaly, presence of lead particles orexcessive amounts of sand in the gastrointestinal tract, gastrointestinal tract dilatation, and bonefractures. These findings contribute to the scant information available about health and disease offalcons in the Kingdom of Saudi Arabia in particular and in the Middle East in general.
Key words: radiographs, Kingdom of Saudi Arabia, Middle East, avian, falcons, Falconiformes
Introduction
Radiography is an essential part of falcon medi-cine and is one of the most important diagnostictools available to veterinarians who treat falcons.Radiographic examination is a practical procedureapplicable to the diagnosis of skeletal, abdominal,and thoracic diseases, some of which manifest insimilar nonspecific clinical signs. It is useful as aprimary diagnostic technique and also as an adjunctto other procedures in making a differential diag-nosis, monitoring the progression of clinical con-ditions, and evaluating effectiveness of treatments.Radiographs of falcons are taken during generalhealth examinations for baseline data, during pre-and postpurchase examinations, and for diagnosticworkup of sick birds. In this report we present theradiographic findings of falcons examined during a3.5-year period at the Falcon Specialist Hospital andResearch Institute of the Fahad bin Sultan FalconCenter (FSFC), Riyadh, Kingdom of Saudi Arabia.Our objective was to contribute to the knowledgeof health and disease of falcons in Saudi Arabia inparticular and in the Middle East in general.
Materials and Methods
Clinical records of 5336 falcons of 6 differentspecies, which consisted of 9798 different visitsfrom September 1, 1998, to March 1, 2002, werereviewed. The falcon species included 4268 (80%)
From the Falcon Specialist Hospital and Research Institute,Fahad bin Sultan Falcon Center, PO Box 55, Riyadh 11322,Kingdom of Saudi Arabia.
saker falcons (Falco cherrug), 736 (14%) peregrinefalcons (Falco peregrinus), 106 (1.9%) gyrfalcons(Falco rusticolus), 114 (2%) lanner falcons (Falcobiarmicus), 2 (0.03%) prairie falcons (Falco mexi-canus), and 110 (2%) hybrid falcons. The birdswere of different ages, from juveniles less than 1year old to adults more than 10 years old. About95% of the birds examined were females. Most fal-cons belonged to Saudi falconers, but an undeter-mined number of birds came from Bahrain, Kuwait,Qatar, and the United Arab Emirates.
Physical examinations were performed on all fal-cons that were presented for health screening orvaccination or because of sickness. Selective diag-nostic procedures included parasitologic screening(endo- and ectoparasites, protozoan and haemato-zoan parasites); hematologic testing and biochemi-cal analysis; blood lead analysis; microbiologic cul-ture; and cytologic, endoscopic, and radiographicexaminations.
Of the 5336 falcons presented for examination atthe FSFC, radiographic examinations were per-formed on 1702 (32%). In an undetermined numberof falcons, radiographs were taken more than onceon different occasions.
Before radiographic examination, all falconswere anesthetized with isoflurane administered bymask. Birds under anesthesia for more than 15 min-utes were intubated with an uncuffed endotrachealtube. Anesthesia was induced with 4% isoflurane at0.5–1 L/min and maintained with 2%–3% isofluraneat 0.5 L/min. Radiographs were taken with portablex-ray equipment (ATOMSCOPE HF 80, Mikasa X-
243NALDO AND SAMOUR—RADIOGRAPHIC FINDINGS IN FALCONS IN SAUDI ARABIA
Table 1. Abnormal radiographic findings by system that were identified in captive falcons examined at the Fahad binSultan Falcon Center in the Kingdom of Saudi Arabia from September 1, 1998, to March 1, 2002.
No. ofabnormalfindings
(N 5 1452)
Incidence proportion(% of total
birds examined,N 5 1702)
Respiratory systemIncreased radiopacity of air sac wallsHomogeneous increased radiopacity of the lung fields and air sacsNonhomogeneous increased radiopacity of the lung fields and air sacs
10178185
0.610.510.9
Localized soft-tissue densities (granulomas)Overdistended air sacs (air trapping)Rounding of caudal lung border (lung congestion)
82505
4.82.90.3
Coelomic cavity and GIa systemDistended abdominal cavityForeign body in GI tract
Lead dust, fragments, pelletsExcessive sand
5
78152
0.3
4.68.9
Soft-tissue densities of the crop and esophagus (infection withTrichomonas, Pseudomonas, Candida species) 27 1.6
Soft-tissue densities of the crop (food in crop)Excessive casting material or meal present in the gizzardIncreased radiopacity of the GI tractGas formation in the GI tract (no dilatation)Gas dilatation of the GI tract
6416
2262
0.42.40.41.33.6
Dilatation of the GI tract (no gas formation)Displacement of the proventriculus or ventriculusGI tract obstruction or impactionAscites
26179
20
1.51.00.51.2
LiverHepatomegalyMicrohepaticaHepatic asymmetry
SplenomegalyFecoliths/uroliths
14625383
8.61.50.20.50.2
Musculoskeletal systemLead dust, fragments, or pellets in body tissuesFracture—traumaFracture—gunshot injuryDislocation
138655
0.85.00.30.3
Luxation/subluxationHealed fractureSoft-tissue swelling without bone involvementSoft-tissue swelling with bone involvement
1412499
0.80.72.90.5
ArthritisOsteoarthritisOsteomyelitis/osteoperiostitis
174
0.060.40.2
OsteolysisIncreased bone density
146
0.80.4
Metabolic bone diseaseOsteodystrophy 1 0.06
Urogenital systemIncreased renal density with nephromegalyIncreased renal density without nephromegaly
218
1.20.5
Cardiovascular systemCardiomegalyHomogeneous increased radiodensity of the heart shadowNonhomogeneous increased radiodensity of the heart shadow
36
13
0.20.40.8
Alterations of the heart shape and contour (dilatation of 1 chamber)Abnormal heart shape and contour (small chamber)
63
0.40.2
a GI indicates gastrointestinal.
244 JOURNAL OF AVIAN MEDICINE AND SURGERY
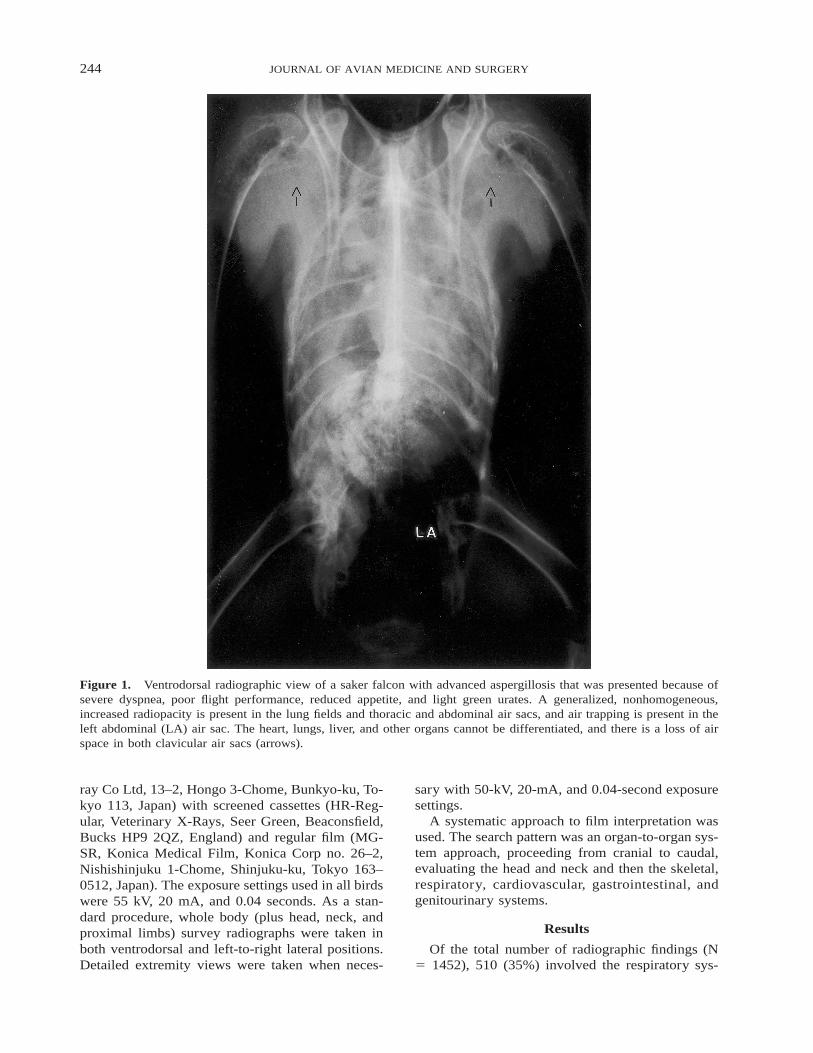
Figure 1. Ventrodorsal radiographic view of a saker falcon with advanced aspergillosis that was presented because ofsevere dyspnea, poor flight performance, reduced appetite, and light green urates. A generalized, nonhomogeneous,increased radiopacity is present in the lung fields and thoracic and abdominal air sacs, and air trapping is present in theleft abdominal (LA) air sac. The heart, lungs, liver, and other organs cannot be differentiated, and there is a loss of airspace in both clavicular air sacs (arrows).
ray Co Ltd, 13–2, Hongo 3-Chome, Bunkyo-ku, To-kyo 113, Japan) with screened cassettes (HR-Reg-ular, Veterinary X-Rays, Seer Green, Beaconsfield,Bucks HP9 2QZ, England) and regular film (MG-SR, Konica Medical Film, Konica Corp no. 26–2,Nishishinjuku 1-Chome, Shinjuku-ku, Tokyo 163–0512, Japan). The exposure settings used in all birdswere 55 kV, 20 mA, and 0.04 seconds. As a stan-dard procedure, whole body (plus head, neck, andproximal limbs) survey radiographs were taken inboth ventrodorsal and left-to-right lateral positions.Detailed extremity views were taken when neces-
sary with 50-kV, 20-mA, and 0.04-second exposuresettings.
A systematic approach to film interpretation wasused. The search pattern was an organ-to-organ sys-tem approach, proceeding from cranial to caudal,evaluating the head and neck and then the skeletal,respiratory, cardiovascular, gastrointestinal, andgenitourinary systems.
Results
Of the total number of radiographic findings (N5 1452), 510 (35%) involved the respiratory sys-
245NALDO AND SAMOUR—RADIOGRAPHIC FINDINGS IN FALCONS IN SAUDI ARABIA
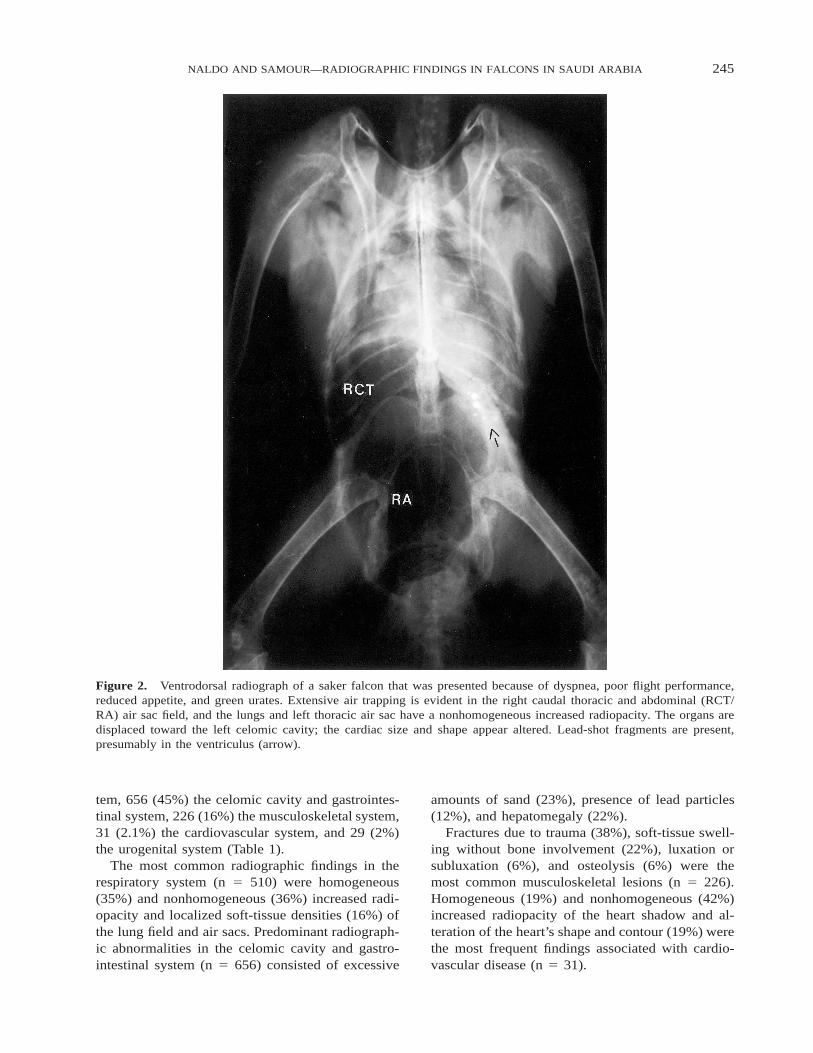
Figure 2. Ventrodorsal radiograph of a saker falcon that was presented because of dyspnea, poor flight performance,reduced appetite, and green urates. Extensive air trapping is evident in the right caudal thoracic and abdominal (RCT/RA) air sac field, and the lungs and left thoracic air sac have a nonhomogeneous increased radiopacity. The organs aredisplaced toward the left celomic cavity; the cardiac size and shape appear altered. Lead-shot fragments are present,presumably in the ventriculus (arrow).
tem, 656 (45%) the celomic cavity and gastrointes-tinal system, 226 (16%) the musculoskeletal system,31 (2.1%) the cardiovascular system, and 29 (2%)the urogenital system (Table 1).
The most common radiographic findings in therespiratory system (n 5 510) were homogeneous(35%) and nonhomogeneous (36%) increased radi-opacity and localized soft-tissue densities (16%) ofthe lung field and air sacs. Predominant radiograph-ic abnormalities in the celomic cavity and gastro-intestinal system (n 5 656) consisted of excessive
amounts of sand (23%), presence of lead particles(12%), and hepatomegaly (22%).
Fractures due to trauma (38%), soft-tissue swell-ing without bone involvement (22%), luxation orsubluxation (6%), and osteolysis (6%) were themost common musculoskeletal lesions (n 5 226).Homogeneous (19%) and nonhomogeneous (42%)increased radiopacity of the heart shadow and al-teration of the heart’s shape and contour (19%) werethe most frequent findings associated with cardio-vascular disease (n 5 31).
246 JOURNAL OF AVIAN MEDICINE AND SURGERY
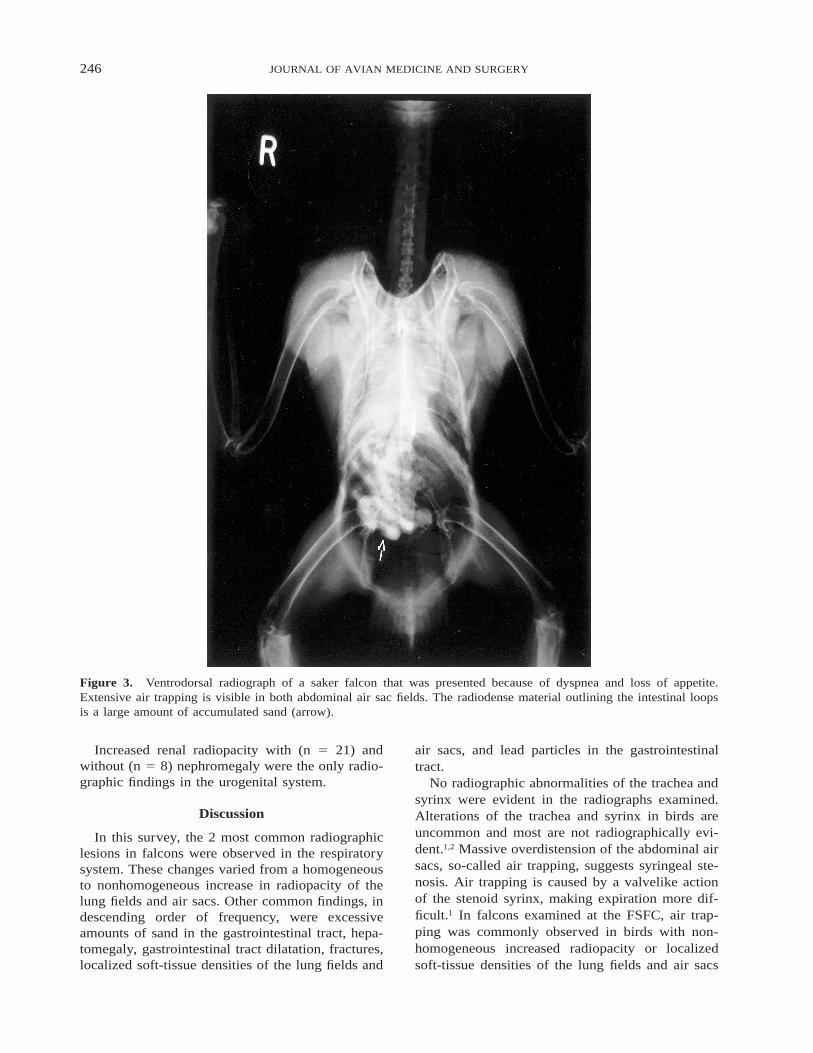
Figure 3. Ventrodorsal radiograph of a saker falcon that was presented because of dyspnea and loss of appetite.Extensive air trapping is visible in both abdominal air sac fields. The radiodense material outlining the intestinal loopsis a large amount of accumulated sand (arrow).
Increased renal radiopacity with (n 5 21) andwithout (n 5 8) nephromegaly were the only radio-graphic findings in the urogenital system.
Discussion
In this survey, the 2 most common radiographiclesions in falcons were observed in the respiratorysystem. These changes varied from a homogeneousto nonhomogeneous increase in radiopacity of thelung fields and air sacs. Other common findings, indescending order of frequency, were excessiveamounts of sand in the gastrointestinal tract, hepa-tomegaly, gastrointestinal tract dilatation, fractures,localized soft-tissue densities of the lung fields and
air sacs, and lead particles in the gastrointestinaltract.
No radiographic abnormalities of the trachea andsyrinx were evident in the radiographs examined.Alterations of the trachea and syrinx in birds areuncommon and most are not radiographically evi-dent.1,2 Massive overdistension of the abdominal airsacs, so-called air trapping, suggests syringeal ste-nosis. Air trapping is caused by a valvelike actionof the stenoid syrinx, making expiration more dif-ficult.1 In falcons examined at the FSFC, air trap-ping was commonly observed in birds with non-homogeneous increased radiopacity or localizedsoft-tissue densities of the lung fields and air sacs
247NALDO AND SAMOUR—RADIOGRAPHIC FINDINGS IN FALCONS IN SAUDI ARABIA
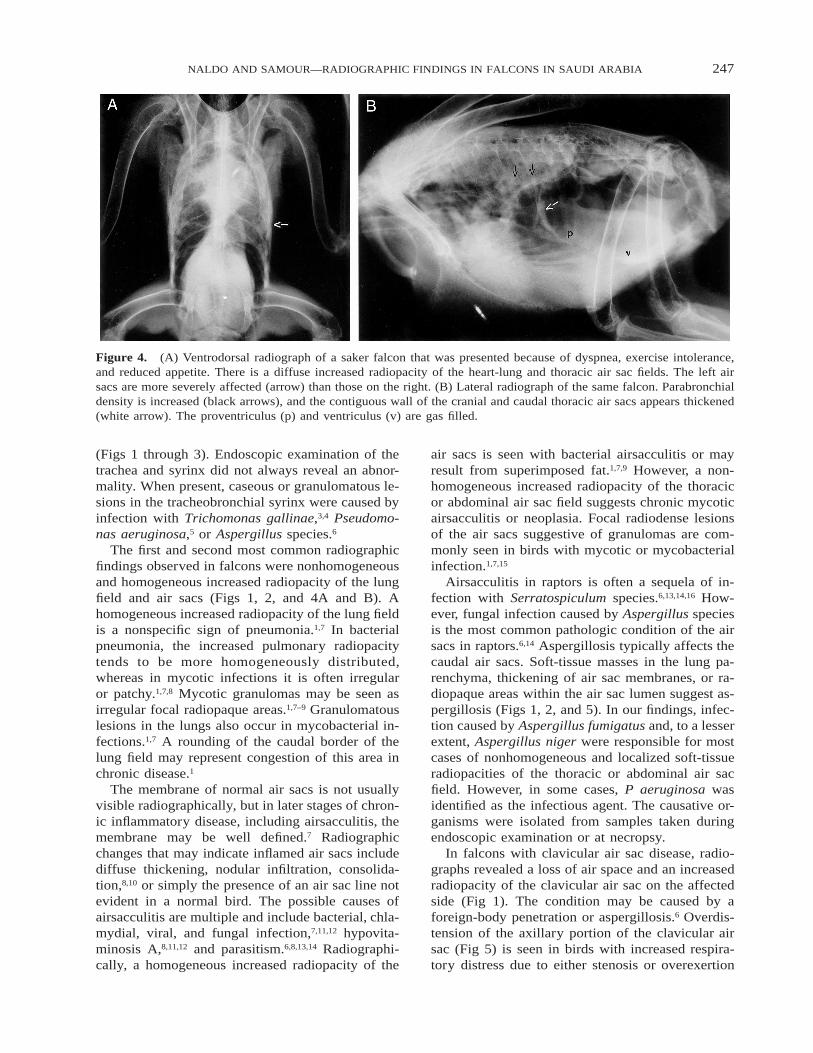
Figure 4. (A) Ventrodorsal radiograph of a saker falcon that was presented because of dyspnea, exercise intolerance,and reduced appetite. There is a diffuse increased radiopacity of the heart-lung and thoracic air sac fields. The left airsacs are more severely affected (arrow) than those on the right. (B) Lateral radiograph of the same falcon. Parabronchialdensity is increased (black arrows), and the contiguous wall of the cranial and caudal thoracic air sacs appears thickened(white arrow). The proventriculus (p) and ventriculus (v) are gas filled.
(Figs 1 through 3). Endoscopic examination of thetrachea and syrinx did not always reveal an abnor-mality. When present, caseous or granulomatous le-sions in the tracheobronchial syrinx were caused byinfection with Trichomonas gallinae,3,4 Pseudomo-nas aeruginosa,5 or Aspergillus species.6
The first and second most common radiographicfindings observed in falcons were nonhomogeneousand homogeneous increased radiopacity of the lungfield and air sacs (Figs 1, 2, and 4A and B). Ahomogeneous increased radiopacity of the lung fieldis a nonspecific sign of pneumonia.1,7 In bacterialpneumonia, the increased pulmonary radiopacitytends to be more homogeneously distributed,whereas in mycotic infections it is often irregularor patchy.1,7,8 Mycotic granulomas may be seen asirregular focal radiopaque areas.1,7–9 Granulomatouslesions in the lungs also occur in mycobacterial in-fections.1,7 A rounding of the caudal border of thelung field may represent congestion of this area inchronic disease.1
The membrane of normal air sacs is not usuallyvisible radiographically, but in later stages of chron-ic inflammatory disease, including airsacculitis, themembrane may be well defined.7 Radiographicchanges that may indicate inflamed air sacs includediffuse thickening, nodular infiltration, consolida-tion,8,10 or simply the presence of an air sac line notevident in a normal bird. The possible causes ofairsacculitis are multiple and include bacterial, chla-mydial, viral, and fungal infection,7,11,12 hypovita-minosis A,8,11,12 and parasitism.6,8,13,14 Radiographi-cally, a homogeneous increased radiopacity of the
air sacs is seen with bacterial airsacculitis or mayresult from superimposed fat.1,7,9 However, a non-homogeneous increased radiopacity of the thoracicor abdominal air sac field suggests chronic mycoticairsacculitis or neoplasia. Focal radiodense lesionsof the air sacs suggestive of granulomas are com-monly seen in birds with mycotic or mycobacterialinfection.1,7,15
Airsacculitis in raptors is often a sequela of in-fection with Serratospiculum species.6,13,14,16 How-ever, fungal infection caused by Aspergillus speciesis the most common pathologic condition of the airsacs in raptors.6,14 Aspergillosis typically affects thecaudal air sacs. Soft-tissue masses in the lung pa-renchyma, thickening of air sac membranes, or ra-diopaque areas within the air sac lumen suggest as-pergillosis (Figs 1, 2, and 5). In our findings, infec-tion caused by Aspergillus fumigatus and, to a lesserextent, Aspergillus niger were responsible for mostcases of nonhomogeneous and localized soft-tissueradiopacities of the thoracic or abdominal air sacfield. However, in some cases, P aeruginosa wasidentified as the infectious agent. The causative or-ganisms were isolated from samples taken duringendoscopic examination or at necropsy.
In falcons with clavicular air sac disease, radio-graphs revealed a loss of air space and an increasedradiopacity of the clavicular air sac on the affectedside (Fig 1). The condition may be caused by aforeign-body penetration or aspergillosis.6 Overdis-tension of the axillary portion of the clavicular airsac (Fig 5) is seen in birds with increased respira-tory distress due to either stenosis or overexertion

248 JOURNAL OF AVIAN MEDICINE AND SURGERY
Figure 5. Ventrodorsal radiograph of a saker falcon with advanced aspergillosis that was presented because of severedyspnea and lost appetite. A generalized, nonhomogeneous increased radiopacity of the left lung field and thoracic andabdominal air sacs is present (L), and the axillary portion of the clavicular air sac appears overdistended (arrows).Excessive sand is present in the ventriculus (v).
of the lower respiratory tract, leading to severe dys-pnea.1,7
Radiographic abnormalities of the coelomic cav-ity and gastrointestinal system were also commonlyobserved. Thickening of the wall of the esophagusor crop may be seen in falcons with vitamin A de-ficiency, endoparasitic infestation,1,9 chronic inflam-mation due to an infection with Candida species1,9,17
or T gallinae,3,4 and bacterial or viral infections.Candidasis was recently described in falcons in Sa-udi Arabia.17 Endoscopic examination of affectedfalcons demonstrated amorphous white-gray togray-green diphtheritic membranes affecting only
the crop.17 Similarly, infection with T gallinae cancause thickening of the esophagus and crop wall.Two types of caseous growths, nodular and mem-branous, were observed in the crop and esopha-gus.3,4 Both types of growths were visible radio-graphically as medium to large granulomas or soft-tissue densities (Fig 6).4
A recent meal or casting material in the crop orgizzard was visible radiographically as either mod-erately or highly radiodense masses, depending onthe type of food items offered. This was a usualfinding in falcons that were presented for exami-nation before the stomach was emptied of casting

249NALDO AND SAMOUR—RADIOGRAPHIC FINDINGS IN FALCONS IN SAUDI ARABIA
Figure 6. Ventrodorsal radiograph of the neck of a saker falcon that was presented because of loss of appetite andswollen neck. A large soft-tissue density, caused by infection with Trichomonas gallinae, is visible in the area of theesophagus and crop. The outline of the trachea (T) is well differentiated.
material or after a recent meal. However, the pres-ence of food in the crop more than 4 hours afterfeeding suggests that crop emptying is delayed,which may lead to an acute toxemia commonlycalled sour crop.18 This condition is common in fal-cons in the Middle East.5,19
Gas formation in the gastrointestinal tract is rarein birds, and any gas present should be consideredabnormal.10 Extensive gas filling of the intestinesmay indicate paralytic ileus, bacterial gastroenteri-tis, or obstruction.7 A uniformly distended gastro-intestinal tract is most commonly associated withfunctional ileus due to viral or bacterial infection,toxicity (eg, heavy metal), septicemia, hypoxemia,
peritonitis, anesthesia,10 parasitism, neoplasia, orforeign-body ingestion. In this study, gas formationin the gastrointestinal tract, with or without an ac-companying dilatation, was observed in falconswith bacterial gastroenteritis, septicemia, lead toxi-cosis, impaction of the gastrointestinal tract withsand, or paralytic ileus of undetermined cause (Fig7). However, gas was often present in the ventric-ulus of clinically normal falcons, most likely causedby aerophagia or altered gastrointestinal motility be-cause of anesthesia. In this study, dilatation of thegastrointestinal tract was the fifth most common ra-diographic finding.
The third most common radiographic finding was
250 JOURNAL OF AVIAN MEDICINE AND SURGERY
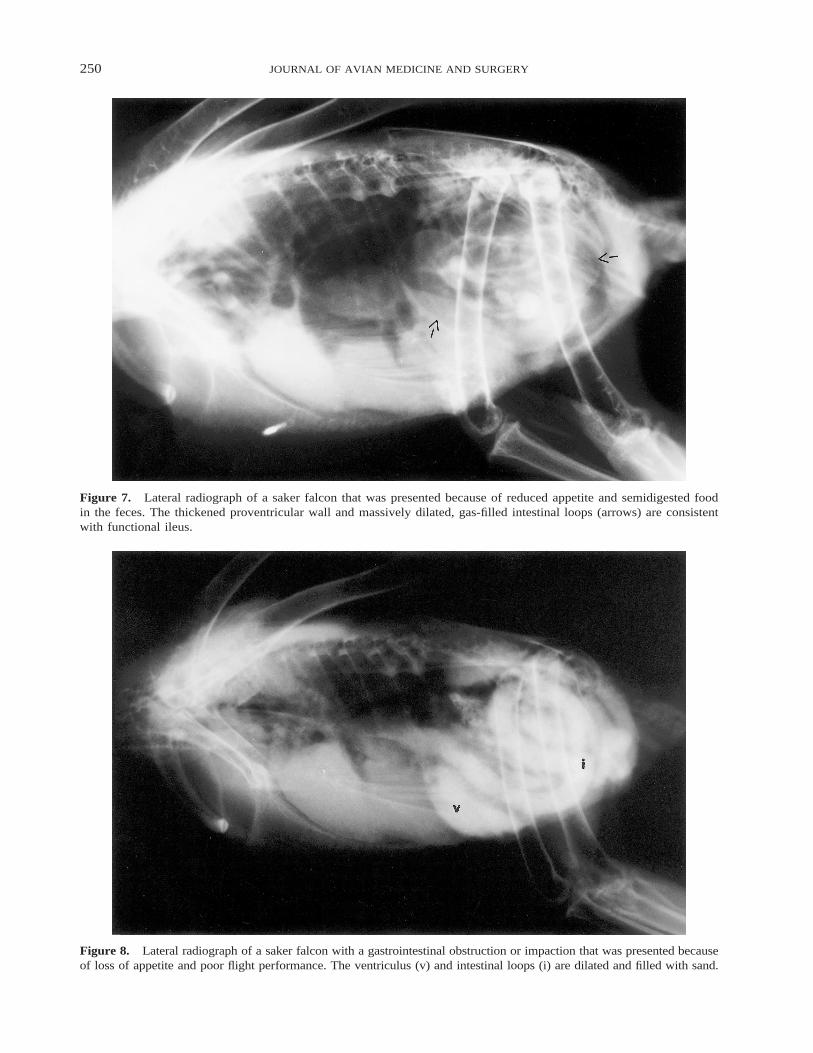
Figure 7. Lateral radiograph of a saker falcon that was presented because of reduced appetite and semidigested foodin the feces. The thickened proventricular wall and massively dilated, gas-filled intestinal loops (arrows) are consistentwith functional ileus.
Figure 8. Lateral radiograph of a saker falcon with a gastrointestinal obstruction or impaction that was presented becauseof loss of appetite and poor flight performance. The ventriculus (v) and intestinal loops (i) are dilated and filled with sand.
251NALDO AND SAMOUR—RADIOGRAPHIC FINDINGS IN FALCONS IN SAUDI ARABIA
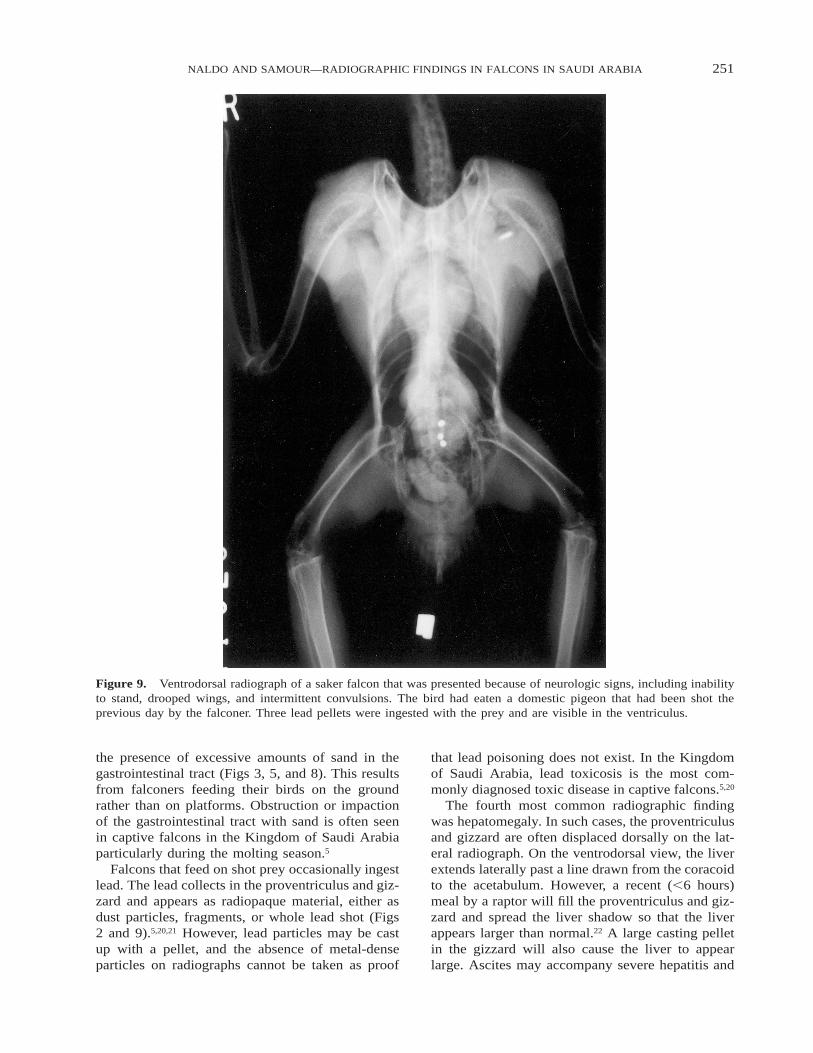
Figure 9. Ventrodorsal radiograph of a saker falcon that was presented because of neurologic signs, including inabilityto stand, drooped wings, and intermittent convulsions. The bird had eaten a domestic pigeon that had been shot theprevious day by the falconer. Three lead pellets were ingested with the prey and are visible in the ventriculus.
the presence of excessive amounts of sand in thegastrointestinal tract (Figs 3, 5, and 8). This resultsfrom falconers feeding their birds on the groundrather than on platforms. Obstruction or impactionof the gastrointestinal tract with sand is often seenin captive falcons in the Kingdom of Saudi Arabiaparticularly during the molting season.5
Falcons that feed on shot prey occasionally ingestlead. The lead collects in the proventriculus and giz-zard and appears as radiopaque material, either asdust particles, fragments, or whole lead shot (Figs2 and 9).5,20,21 However, lead particles may be castup with a pellet, and the absence of metal-denseparticles on radiographs cannot be taken as proof
that lead poisoning does not exist. In the Kingdomof Saudi Arabia, lead toxicosis is the most com-monly diagnosed toxic disease in captive falcons.5,20
The fourth most common radiographic findingwas hepatomegaly. In such cases, the proventriculusand gizzard are often displaced dorsally on the lat-eral radiograph. On the ventrodorsal view, the liverextends laterally past a line drawn from the coracoidto the acetabulum. However, a recent (,6 hours)meal by a raptor will fill the proventriculus and giz-zard and spread the liver shadow so that the liverappears larger than normal.22 A large casting pelletin the gizzard will also cause the liver to appearlarge. Ascites may accompany severe hepatitis and

252 JOURNAL OF AVIAN MEDICINE AND SURGERY
Figure 10. (A) Ventrodorsal and (B) lateral radiograph of a saker falcon that was presented because of severe dyspnea,abdominal swelling, and green urates. A large soft-tissue shadow is present in the abdominal cavity (arrows), thehourglass shape between heart (h) and liver (l) is lost, and the lungs and air sacs are massively compressed. This falconhad ascites, hepatitis, and amyloidosis.
is seen as a diffuse (ground-glass appearance) in-crease in radiopacity of the entire celomic cavity,except for the air-filled lungs, with no differentia-tion of various organs (Fig 10).1,7
Hepatopathy in raptors is characterized radio-graphically by an enlarged liver. Other organs thatmay be enlarged are the spleen and kidneys.18 Her-pesviruses causing hepatosplenitis have been isolat-ed from raptors.23 In a recent study that included 3birds at the FSFC with radiographic evidence ofhepatobiliary disease, 1 bird had histologic evidenceof herpesviral hepatitis whereas 2 birds had evi-dence of amyloidosis.24
The spleen is normally visible only on the lateralview (Fig 11), but it can also be seen on the ven-trodorsal view if greatly enlarged. The size of thenormal spleen measured along its length on the lat-eral view ranges from 9–13.5 mm, 9–12 mm, and12–18 mm in saker falcons, peregrine falcons, andgyrfalcons, respectively (J.L.N. and J.H.S., unpub-lished data, February 2004). A spleen that measuresbeyond this range is considered enlarged. Avian tu-berculosis, lymphoma, chlamydial infections, andsome viral infections will cause splenic enlarge-ment.7,22 At the FSFC, splenomegaly was observedin falcons with bacterial septicemias and herpesviralhepatitis.
Bone fracture was the sixth most common radio-graphic finding in falcons presented for examina-tion. Fractures commonly occur as a result of im-proper handling by novice keepers, car collision ac-cidents during training or hunting, accidents (colli-sion) inside the molting room, and accidentalshooting of the falcon during trapping.5,25 Collision-
type injuries are also manifested as dislocations oravulsions.5 Fractures due to gunshot injuries occurwhen falcon trappers fire a shotgun just beside thebird to scare and force it to land, making it easierto trap. In some instances, the birds are hit by 1 ormore pellets. Several falcons were presented to theFSFC with fracture of the wing bones and lead pel-lets embedded in the body (Fig 12).5 Occasionally,lead pellets were found during radiographic exam-inations of clinically normal falcons that were pre-sented for pre- or postpurchase health checks. In theFSFC, up to 11 lead pellets have been found em-bedded in different parts of the body of an injuredsaker falcon.
Diaphyseal fractures of the extremities were themost common type of fractures detected. In addi-tion, fractures of the ribs, coracoid, clavicle, orscapula were also observed. Several falcons thatwere presented to the hospital had old healed frac-tures, most commonly of the extremities. Vertebralfractures or luxations were located between the no-tarium and synsacrum on the sixth thoracic vertebra,which is the only free thoracic vertebra in a falcon(Fig 11). Falcons with this condition were presentedwith mild clinical signs of poor flight performanceand lameness of 1 or both legs to more severe signsof paresis or leg paralysis. Euthanasia was recom-mended in most cases of vertebral fracture or lux-ation.
With infectious or neoplastic processes, osteoly-sis was the predominant radiographic change. Septicarthritis and osteomyelitis may develop secondaryto open fractures, pododermatitis, penetratingwounds, hematogenous sources, extension from air

253NALDO AND SAMOUR—RADIOGRAPHIC FINDINGS IN FALCONS IN SAUDI ARABIA
Figure 11. Lateral radiograph of a saker falcon that was presented because of poor flight performance and lamenessof both legs. The spleen (s) is enlarged. Anaerobic abscessation (arrow) subsequent to trauma in the caudal thoracicvertebrae and the synsacrum has caused collapse of the sixth and seventh thoracic vertebrae, leading to spinal luxation.
sac disease, or iatrogenic contamination.8,10 In fal-cons with acute septic arthritis, joint effusion dueto synovitis may be the only radiographic change.With advanced infection, destruction of articularcartilage results in loss of joint space, and osteolysisand periosteal changes may occur in the metaphysisand epiphysis. Distal joints are commonly affected,especially when the infection is secondary to septicpododermatitis.1,10 Radiographic changes observedin falcons with pododermatitis ranged from soft-tissue swelling without visible bone lesions to os-teolysis and osteomyelitis of the digits or distal tar-sometatarsus (Fig 13).
Radiographic changes in the urogenital systemwere also seen. On the lateral radiographic view,the kidneys are normally surrounded by air. Loss ofthe air shadow may indicate renal enlargement,presence of abdominal fat or fluid, or dorsal dis-placement of abdominal organs.10 An enlarged kid-ney shadow is frequently seen with enlarged shad-ows of other organs as a sign of generalized infec-tion, secondary to vitamin A deficiency, or with renalneoplasia.7 Bilaterally symmetrical nephromegalyalso occurs with metabolic disease, dehydration, andpostrenal obstruction.10 Renal gout and dehydrationcan produce increased renal radiopacity without en-
largement.8 Nephritis or bolus fluid administrationcan produce a slight increase in size of the kidneyswith variable change in density.8 In the FSFC, about20% of cases with increased renal radiopacity, withor without nephromegaly, were confirmed as vis-ceral gout at necropsy.
The most common radiographic change in thecardiovascular system was an increased radiopacityof the heart shadow. This finding may be caused bypericardial effusion, pericarditis, airsacculitis, orpneumonia. An enlarged heart, calcified major ar-teries, and edema within the air sacs can be seenradiographically. Ascites due to congestive heartfailure is impossible to differentiate radiographical-ly from effusion caused by a visceral tumor, puru-lent airsacculitis, or, occasionally, an enlarged liv-er.22 Likewise, a falcon with egg peritonitis or anormal, pre–egg-laying falcon may have a similarradiographic appearance. Barium contrast radiog-raphy and celiocentesis are useful to differentiatethese cases.
Relative to their body size, the heart of gyrfal-cons, gyrfalcon hybrids, and peregrine falcons ap-pears larger than that of saker or lanner falcons. Thebodyweight of an adult female saker falcon, pere-grine falcon, and gyrfalcon ranges from 900–1150
254 JOURNAL OF AVIAN MEDICINE AND SURGERY
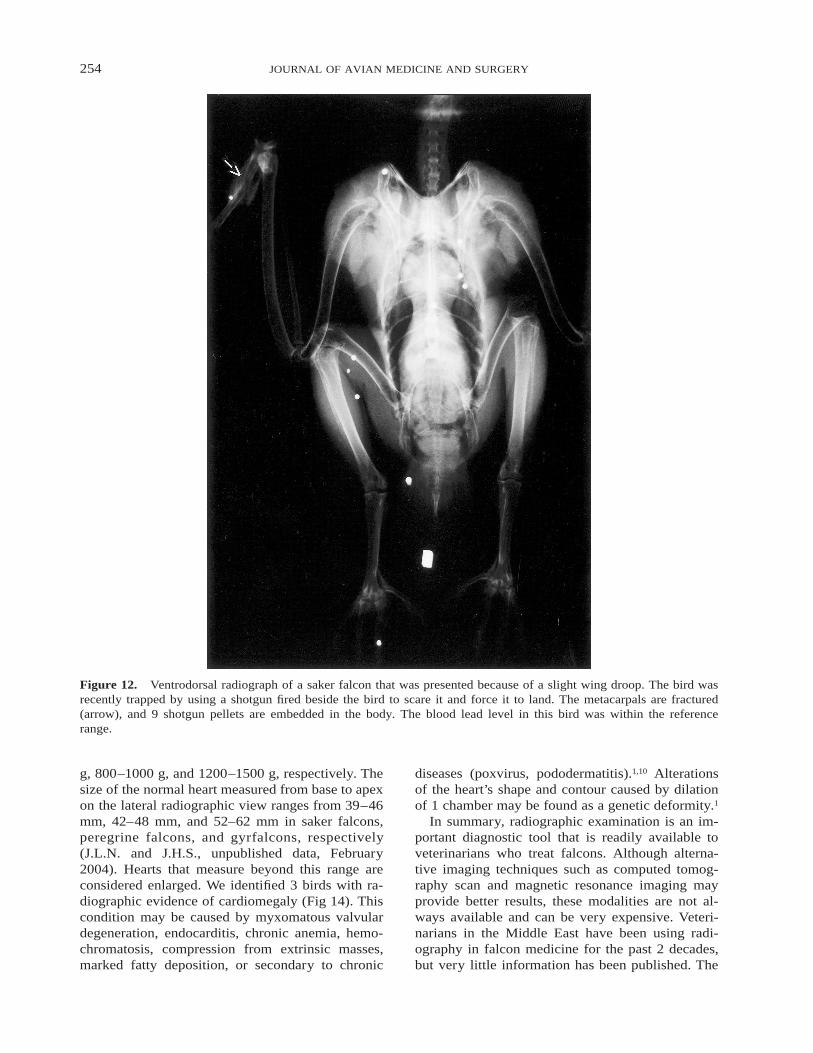
Figure 12. Ventrodorsal radiograph of a saker falcon that was presented because of a slight wing droop. The bird wasrecently trapped by using a shotgun fired beside the bird to scare it and force it to land. The metacarpals are fractured(arrow), and 9 shotgun pellets are embedded in the body. The blood lead level in this bird was within the referencerange.
g, 800–1000 g, and 1200–1500 g, respectively. Thesize of the normal heart measured from base to apexon the lateral radiographic view ranges from 39–46mm, 42–48 mm, and 52–62 mm in saker falcons,peregrine falcons, and gyrfalcons, respectively(J.L.N. and J.H.S., unpublished data, February2004). Hearts that measure beyond this range areconsidered enlarged. We identified 3 birds with ra-diographic evidence of cardiomegaly (Fig 14). Thiscondition may be caused by myxomatous valvulardegeneration, endocarditis, chronic anemia, hemo-chromatosis, compression from extrinsic masses,marked fatty deposition, or secondary to chronic
diseases (poxvirus, pododermatitis).1,10 Alterationsof the heart’s shape and contour caused by dilationof 1 chamber may be found as a genetic deformity.1
In summary, radiographic examination is an im-portant diagnostic tool that is readily available toveterinarians who treat falcons. Although alterna-tive imaging techniques such as computed tomog-raphy scan and magnetic resonance imaging mayprovide better results, these modalities are not al-ways available and can be very expensive. Veteri-narians in the Middle East have been using radi-ography in falcon medicine for the past 2 decades,but very little information has been published. The
255NALDO AND SAMOUR—RADIOGRAPHIC FINDINGS IN FALCONS IN SAUDI ARABIA
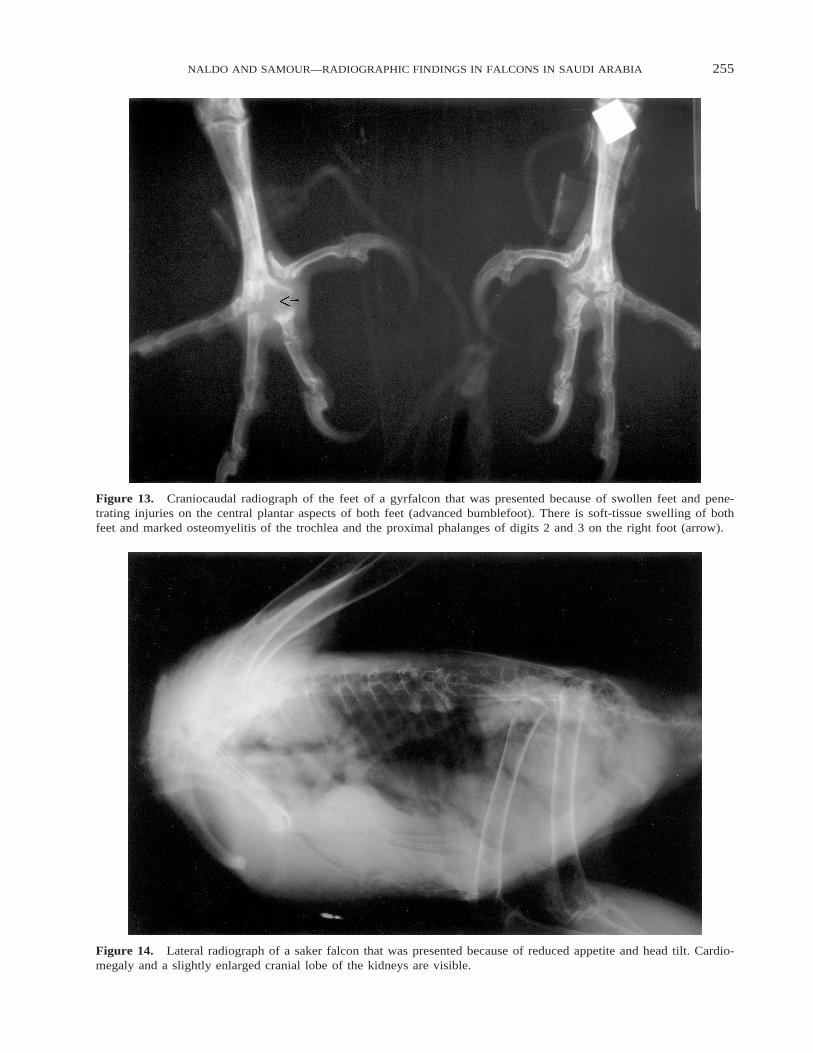
Figure 13. Craniocaudal radiograph of the feet of a gyrfalcon that was presented because of swollen feet and pene-trating injuries on the central plantar aspects of both feet (advanced bumblefoot). There is soft-tissue swelling of bothfeet and marked osteomyelitis of the trochlea and the proximal phalanges of digits 2 and 3 on the right foot (arrow).
Figure 14. Lateral radiograph of a saker falcon that was presented because of reduced appetite and head tilt. Cardio-megaly and a slightly enlarged cranial lobe of the kidneys are visible.

256 JOURNAL OF AVIAN MEDICINE AND SURGERY
results we report will contribute to the knowledgeof health and disease of falcons in Saudi Arabia inparticular and in the Middle East in general.
Acknowledgments: We thank HRH Prince Fahad binSultan bin Abdulaziz Al Saud for his support of the ad-vancement of falcon medicine; Mr Basil Al Abbasi, Di-rector General, for his continuing interest in the clinicaland research program of the Falcon Specialist Hospitaland Research Institute, and the veterinary staff for pro-viding technical assistance.
References
1. Krautwald-Junghanns ME. Avian radiology. In: Ros-skopf W, Woerpel R, eds. Diseases of Cage and Avi-ary Birds. Baltimore, MD: Williams and Wilkins;1996:630–663.
2. Newell SM, Roberts GD, Bennett RA. Imaging tech-niques for avian lower respiratory diseases. SeminAvian Exotic Pet Med. 1997;6:180–186.
3. Samour JH, Bailey TA, Cooper JE. Trichomoniasisin birds of prey (Order Falconiformes) in Bahrain.Vet Rec. 1995;136:345–362.
4. Samour JH, Naldo JL. Diagnosis and therapeuticmanagement of trichomoniasis in falcons in SaudiArabia. J Avian Med Surg. 2003;17:136–143.
5. Naldo JL, Samour JH. Causes of morbidity and mor-tality in falcons in Saudi Arabia. J Avian Med Surg.2004;18:229–240.
6. Forbes NA. Respiratory problems. In: Beynon PH,Forbes NA, Harcourt-Brown NH, eds. Manual ofRaptors, Pigeons and Waterfowl. Gloucestershire,Cheltenham, UK: British Small Animal VeterinaryAssociation; 1996:180–188.
7. Krautwald-Junghanns ME, Trinkaus K. Imagingtechniques. In: Tully TN, Lawton MPC, DorresteinGM, eds. Avian Medicine. Oxford, UK: Butterworth-Heinemann; 2000:52–73.
8. Smith BJ, Smith SA. Radiology. In: Altman RB,Clubb SL, Dorrestein GM, Quesenberry K, eds. Avi-an Medicine and Surgery. Philadelphia, PA: WBSaunders; 1997:170–199.
9. Naldo J. Radiology. In: Samour J, ed. Avian Medi-cine. London, UK: Harcourt Publishers Ltd; 2000:50–60.
10. McMillan MC. Imaging Techniques. In: Ritchie BW,Harrison GJ, Harrison LR, eds. Avian Medicine:Principles and Application. Lake Worth, FL: Wing-ers; 1994:246–326.
11. McMillan MC. Radiology of avian respiratory dis-
eases. Compend Cont Educ Pract Vet. 1986;8:551–558.
12. Tully TN, Harrison GJ. Pneumonology. In: RitchieBW, Harrison GJ, Harrison LR, eds. Avian Medicine:Principles and Application. Lake Worth, FL: Wing-ers; 1994:556–581.
13. Samour JH, Naldo JL. Serratospiculiasis in captivefalcons in the Middle East: a review. J Avian MedSurg. 2001;15:2–9.
14. Cooper JE. Infectious diseases, excluding macropar-asites. In: Cooper JE, ed. Birds of Prey: Health andDisease. 3rd ed. Oxford, UK: Blackwell Science Ltd;2002:84–104.
15. Silverman S. Advanced avian radiographic interpre-tation. Proc Annu Conf Assoc Avian Vet. 1990;339–342.
16. Samour JH. Serratospiculiasis in falcons in the Mid-dle East. Proc Annu Conf Eur Chap Assoc Avian Vet.1999;178–182.
17. Samour JH, Naldo JL. Diagnosis and therapeuticmanagement of candidiasis in falcons in Saudi Ara-bia. J Avian Med Surg. 2002;16:129–132.
18. Forbes NA. Chronic weight loss, vomiting and dys-phagia. In: Beynon PH, Forbes NA, Harcourt-BrownNH, eds. Manual of Raptors, Pigeons and Waterfowl.Gloucestershire, Cheltenham, UK: British Small An-imal Veterinary Association; 1996:189–196.
19. Samour JH. Falcons, Falconry and Veterinary Med-icine in the Middle East. Riyadh, Saudi Arabia. Inpress.
20. Samour JH, Naldo JL. Diagnosis and therapeuticmanagement of lead toxicosis in falcons in SaudiArabia. J Avian Med Surg. 2002;16:16–20.
21. Cooper JE. Fits, incoordination and coma. In: Bey-non PH, Forbes NA, Harcourt-Brown NH, eds. Man-ual of Raptors, Pigeons and Waterfowl. Gloucester-shire, Cheltenham, UK: British Small Animal Vet-erinary Association; 1996:197–207.
22. Harcourt-Brown NH. Radiology. In: Beynon PH,Forbes NA, Harcourt-Brown NH, eds. Manual ofRaptors, Pigeons and Waterfowl. Gloucestershire,Cheltenham, UK: British Small Animal VeterinaryMedical Association; 1996:89–97.
23. Kaleta EF. Herpesviruses of birds: a review. AvianPathol. 1990;19:193–211.
24. Samour JH, Naldo JL. The use of serum bile acidsin the assessment of hepatobiliary function in sakerfalcons (Falco cherrug) in Saudi Arabia. Proc AnnuConf Eur Chap Assoc Avian Vet. 2003;292–296.
25. Naldo JL, Samour JH. Selected orthopedic cases infalcons in Saudi Arabia. Exotic DVM. 2002;4.4:11–13.