rad553 2010 lecture 3 - rad.msu.edu · major fissure • compare ... • usually associated with...
TRANSCRIPT

4/28/2010
1
Lecture 3
Inflammatory Processes
• Process:– Increased vascular permeability
• Water and cellular infiltrations• Results:
– Abscess, ulceration, cavitation• Penetration, perforation and fistula
formation– Scarring, strictures

4/28/2010
2
Inflammatory Processes
• Lungs and pleura• Gastrointestinal tract• Soft tissues of extremities• Brain
Inflammatory Lung, Mediastinal and Pleural Diseases
• Bronchitis– Acute– Chronic
• Pneumonia– Infective– ChemicalChemical
4/28/2010
3
Inflammatory Lung, Mediastinal and Pleural Diseases
• Pulmonary abscess• Pleuritis• Empyema• Lymphadenopathy
Pulmonary Air Space Pattern(Consolidation or Infiltration)
• Alveoli filled with pus, water, blood, ll t icells, protein
• Appearance- fluffy, ill defined margins
• Single (segmental or lobar), multiple or diffuse distributionmultiple, or diffuse distribution
• Rapid development
4/28/2010
4
Pulmonary Air Space Pattern(Consolidation or Infiltration)
• Air bronchograms –fluid filled l li d i fill d b hialveoli surround air filled bronchi
• Butterfly shadow–E.G. Pneumonia, alveolar
pulmonary edema
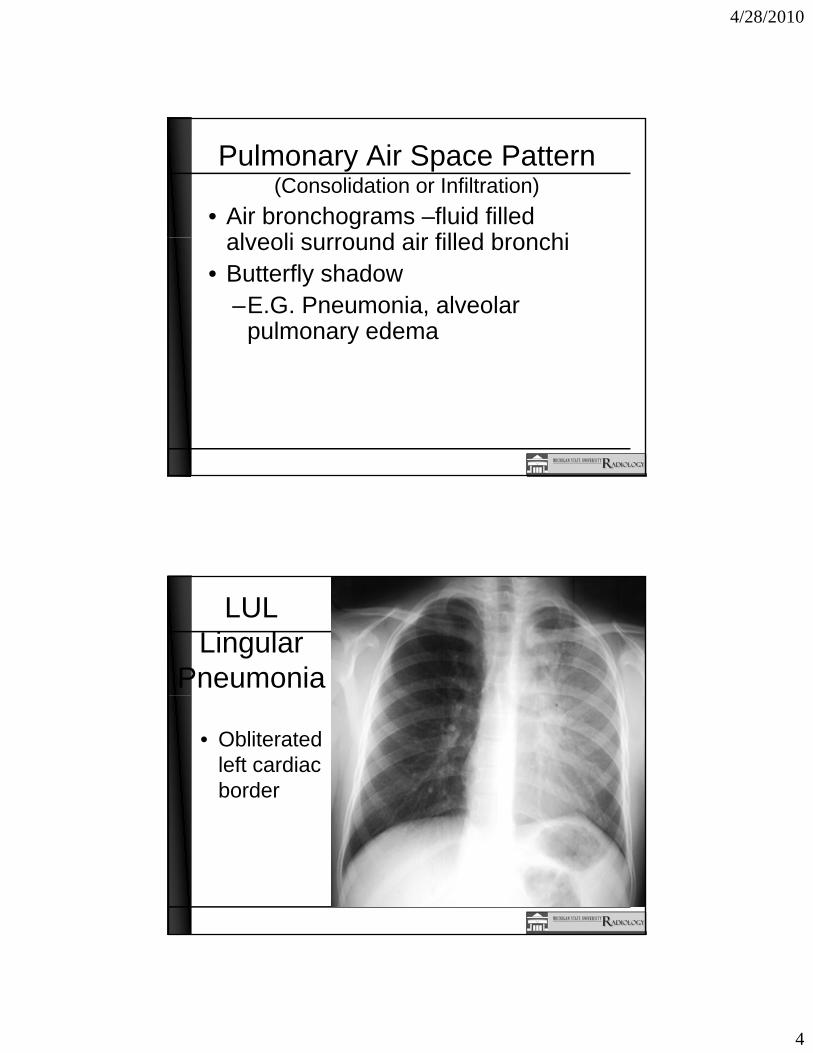
LUL Lingular
Pneumonia
• Obliterated left cardiac border

4/28/2010
5
LULLingular
Pneumonia Lateral
• Consolidation anterior to the major fissure
• Compare to PA exam
LULLingular Pneumonia
4/28/2010
6
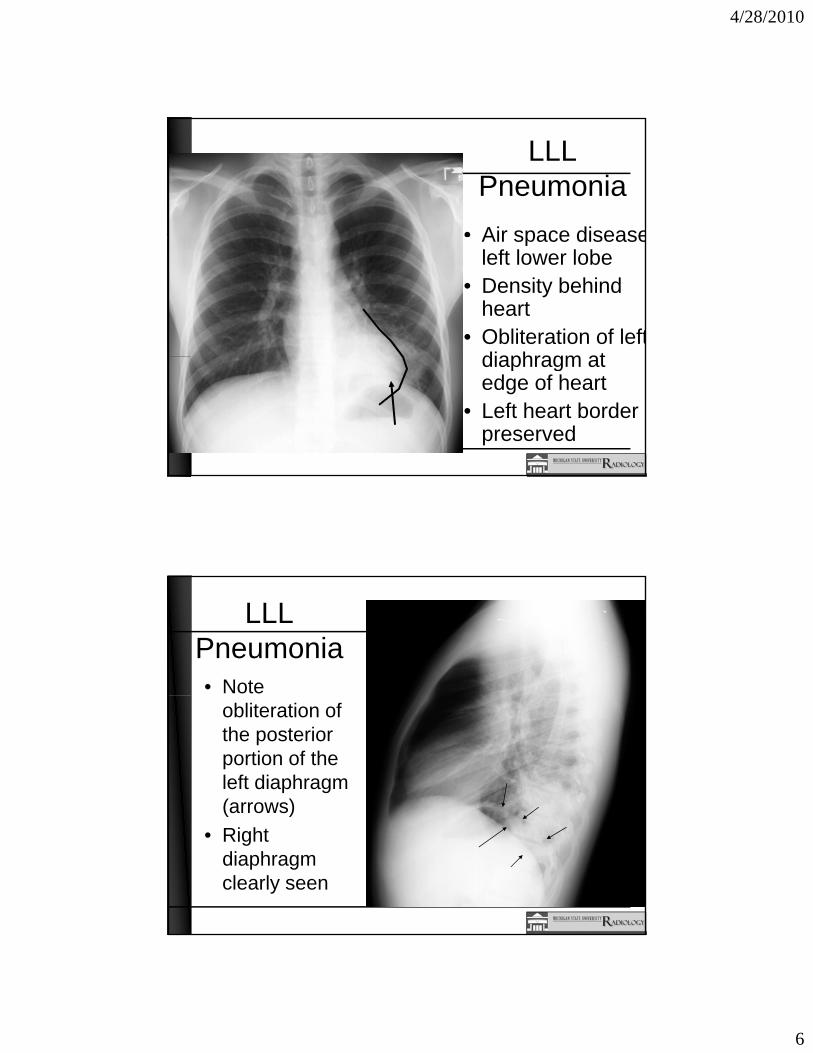
LLL Pneumonia
• Air space diseaseAir space diseaseleft lower lobe
• Density behind heart
• Obliteration of leftdiaphragm atdiaphragm at edge of heart
• Left heart border preserved
LLL Pneumonia• Note
obliteration of the posterior portion of the left diaphragm (arrows)( )
• Right diaphragm clearly seen
4/28/2010
7
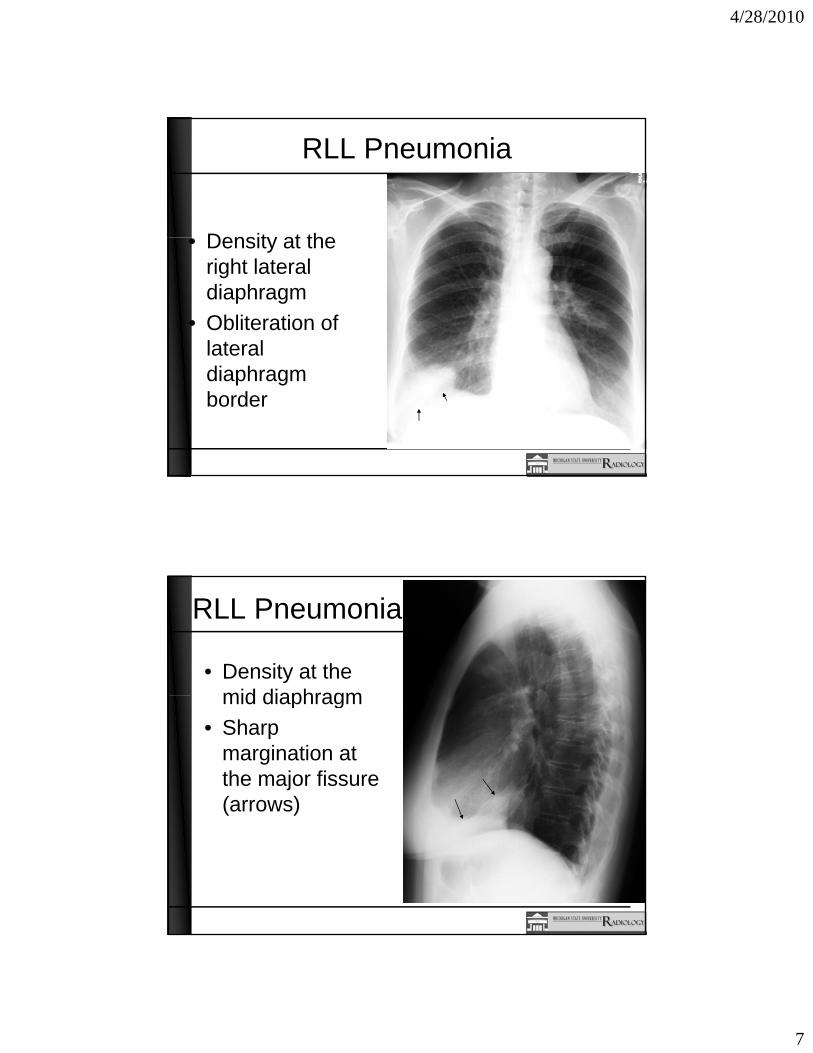
RLL Pneumonia
Densit at the• Density at the right lateral diaphragm
• Obliteration of lateral diaphragm border
RLL Pneumonia
• Density at the mid diaphragmmid diaphragm
• Sharp margination at the major fissure (arrows)( )

4/28/2010
8
Lung Abscess
• Thick walled irregular cavity RUL
• Fluid level representing partial evacuationevacuation of necrotic material via airway
Lung Abscess
• Thick walled i l itirregular cavity RUL
• Fluid level representing partial
ti fevacuation of necrotic material via airway
4/28/2010
9
Pulmonary Interstitial Pattern• Fluid or cells in the pulmonary
interstitial space–e.g. Peribronchial tissue and
bronchial wall, perivascular space and vessels, lymphatic structure
• Alveoli aerated
Pulmonary Interstitial Pattern• Appearance:
–Linear, lattice-like, or multiple small nodules
• Examples:–Cystic fibrosis, bronchiectasis,
asbestosis, silicosis, and other i ipneumoconiosis

4/28/2010
10
Cystic Fibrosis• Bronchial wall
thickening• Ring shadows and
parallel bronchiole walls of bronchiectasis
• Ill-defined linear lesions
• Obstructive airway with low diaphragms
Interstitial Edema CHF
• Bilateral central interstitial linear lattice pattern
• Small nodular lesions
• Ill-defined enlarged hila
• Septal lines (K l ’ )(Kerley’s)
• Multiple horizontal lines near costophrenic angles (Kerley B)

4/28/2010
11
Interstitial Edema CHF• Variation in
another ti tpatient
• Cardiomegaly• Pulmonary
vascular changes aschanges as on prior patient
Classic Pulmonary Edema
• Batwing or• Batwing or butterfly appearance
• Smoke inhalation
4/28/2010
12
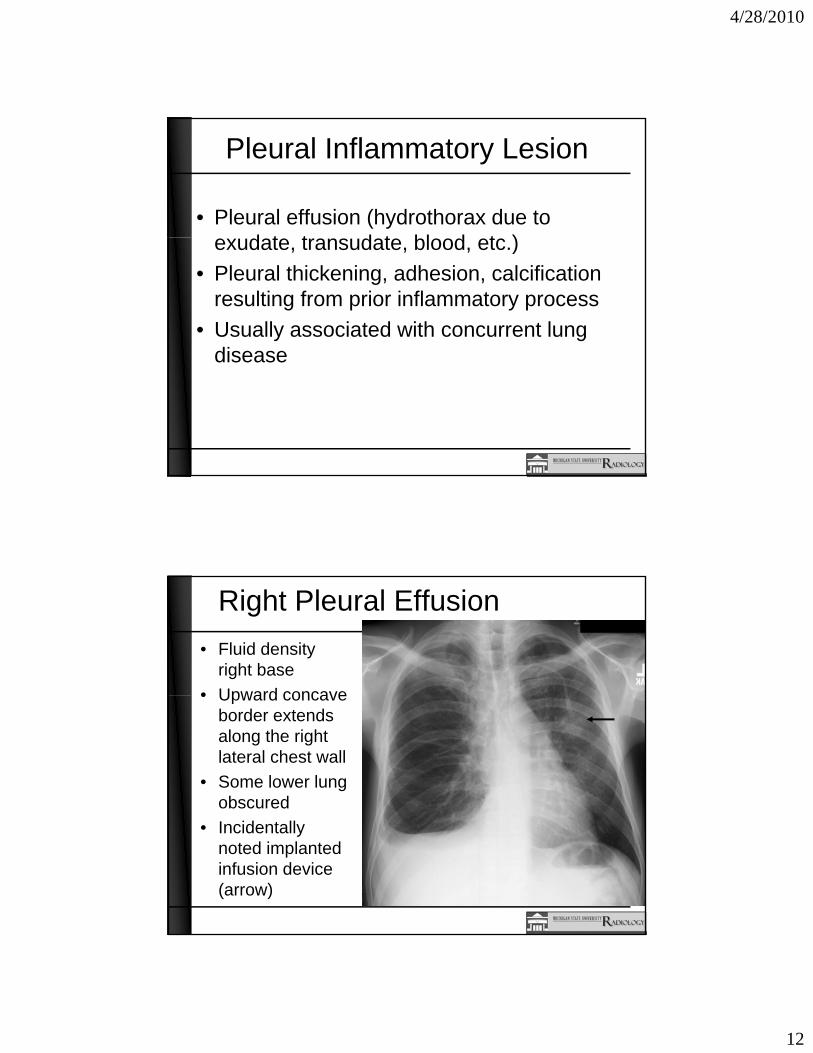
Pleural Inflammatory Lesion
• Pleural effusion (hydrothorax due to d t t d t bl d t )exudate, transudate, blood, etc.)
• Pleural thickening, adhesion, calcification resulting from prior inflammatory process
• Usually associated with concurrent lung diseasedisease
Right Pleural Effusion• Fluid density
right base• Upward concave• Upward concave
border extends along the right lateral chest wall
• Some lower lung obscured
• Incidentally noted implanted infusion device (arrow)

4/28/2010
13
Pleural Effusion
• Blunting of both costophrenic angles (arrows)
• Loss of lower heart marginsheart margins
Pleural Effusion - Plaque• Calcified
plaque along both lateral chest walls (arrows)
• Result of Asbestos e pos reexposure
• Some plaque along diaphragm

4/28/2010
14
Pleural Effusion - Plaque• Calcified
plaque along both posterior chest walls (arrows)
• Result of• Result of asbestos exposure
Esophageal Inflammatory Disease
• Esophagitis commonly due to infection–Bacteria–Virus–Fungus
• Gastroesophageal reflexp g

4/28/2010
15
Esophageal Inflammatory Disease
• Chemical substance corrosion• Radiologic manifestations of
different causes of esophagitis are similar
• No radiologic abnormalities when degree of inflammation is mild
Normal Esophagus• Barium in
esophagus• Smooth indentation
anterior wall upper third from the aortic arch
• Focal ‘ring’ distal• Focal ring distal esophagus at gastric junction

4/28/2010
16
Esophageal Candidiasis
• Multiple oval filling defects along thedefects along the esophageal mucousa
• Plaques of candida along the esophagus (filling defects in(filling defects in barium coating)
Gastrointestinal Inflammatory Disease
• Mucosal changes– Swelling: local or diffuse enlargement of g g
mucosal folds– Defect: ulceration
• Penetration, perforation and abscess formation (ULCER CRATER)
– Scarring: strictureg• Need to use contrast (barium) study to
illustrate the lumen and inner wall of GI tract

4/28/2010
17
Gastric and Duodenal Ulcers• Benign ulcer:
– Ulcer projects beyond lumen– Sharp margin, round barium dot
viewed en face– Edematous halo around ulcer in acute
stage– Mucosal folds radiate out like spokes
of wheel in sub-acute or chronic stage
• Gas in fundus of stomach
Normal Gastrointestinal Study
stomach• Opacification of
stomach, duodenum and jejunum
• Peristalsis in the distal duodenal bulb

4/28/2010
18
Normal Barium Enema• Single
contrast exam• Notice the
normal haustrationsC t t• Competent ileocecal valve
NormalBarium Enema
• Double (air) t tcontrast
• Supine image• Coating of
mucosa and distended with gas
• Appendix is filled with barium
4/28/2010
19
DevelopmentDevelopment And Its
Anomolies
Embryo Milestones Detected by Ultrasound
• Gestation sac 4.5-5 weeksGestation sac• Yolk sac• Embryo• Placenta
4.5 5 weeks5 weeks5-6 weeks8 weeks

4/28/2010
20
Early Gestation• Longitudinal
scan Sac
• Anechoic structure
• Echogenic rim• Gestational sac
Bladder
• Cervix
Embryo
• Endovaginal scan, more detail, resolution
• Gestational sac, embryo (cursors), yolk sacsac
• Gestational age 8 weeks 4 days

4/28/2010
21
Yolk Sac
• Yolk sac indicated by ytwo white arrows
• Amniotic membrane visible as faint
25
visible as faint curvilinear echoes in sac
Embryonic Heart
25
4/28/2010
22
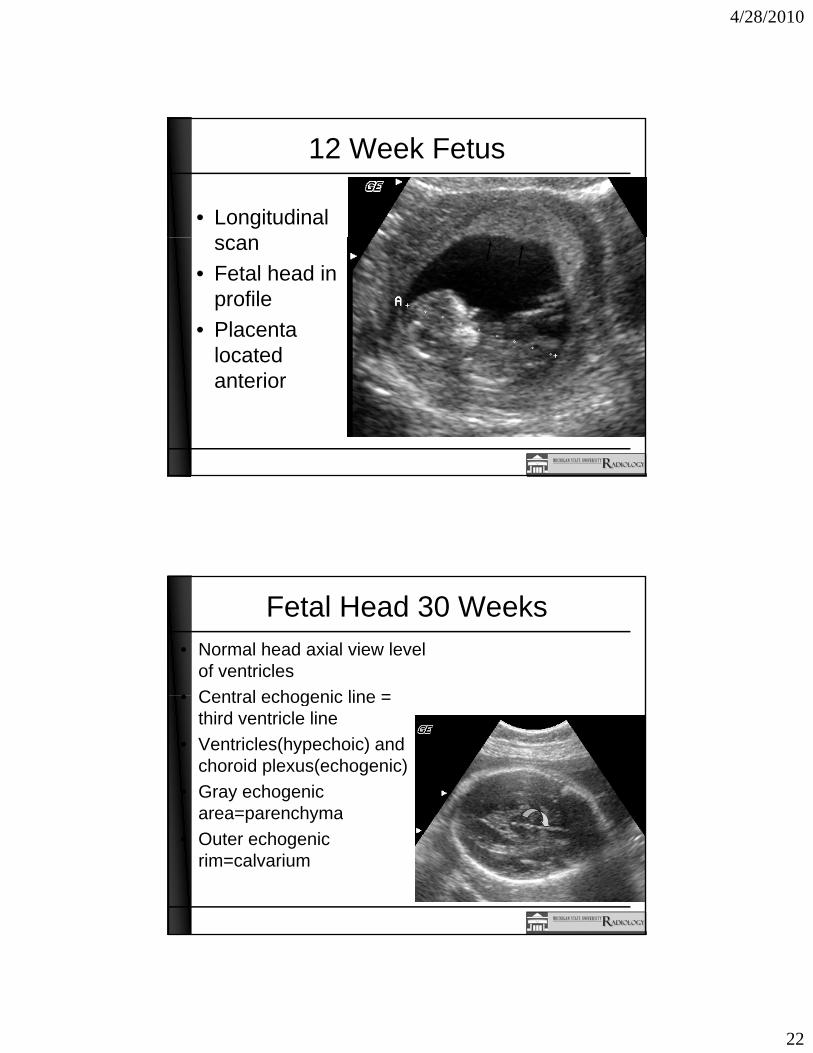
12 Week Fetus
• Longitudinal scan
• Fetal head in profile
• Placenta locatedlocated anterior
Fetal Head 30 Weeks• Normal head axial view level
of ventricles• Central echogenic line =• Central echogenic line =
third ventricle line• Ventricles(hypechoic) and
choroid plexus(echogenic)• Gray echogenic
area=parenchymaarea=parenchyma• Outer echogenic
rim=calvarium

4/28/2010
23
• Four chamber
Normal Fetal Chest
heart view• Heart
chambers labeled RA
RV
LA
LVLV
Fetal Chest and Abdomen
• Sagittal view• Rib shadows • Abdominal
contents
Ribs
Bowel

4/28/2010
24
Normal Fetal Abdomen
• Axial at level of kidneysy
• Echogenic dots above represent spine(arrow)
• KidneysKidneys (arrowhead)
Normal Fetal Pelvis
• Section through level of bladder
• Oval hypoechoic area represents bladder (arrow)
• Femurs parallel linear echogenic Alinear echogenic (A)
• Sacrum under arrow
A

4/28/2010
25
Normal Fetal Spine
• Sagittal view C T L• Sagittal view C,T, L spine
• Parallel row of dots represent ossification centers of pedicles
d b diand bodies• Note: images not
true sagittal
Normal Fetal Spine
• Axial view
*
• Level of cervical, thoracic and lumbar vertebrae
• Ossification centers triangular arrangement
*
• Body in center, pedicles lateral
• * At the center of each spinal canal
*

4/28/2010
26
Fetal Femur
Fetal Cord Insertion
• Transverse abdomenabdomen
• Cord insertion midline
• White represents doppler evaluation
FetalAbdomen
of blood flow in cord
4/28/2010
27
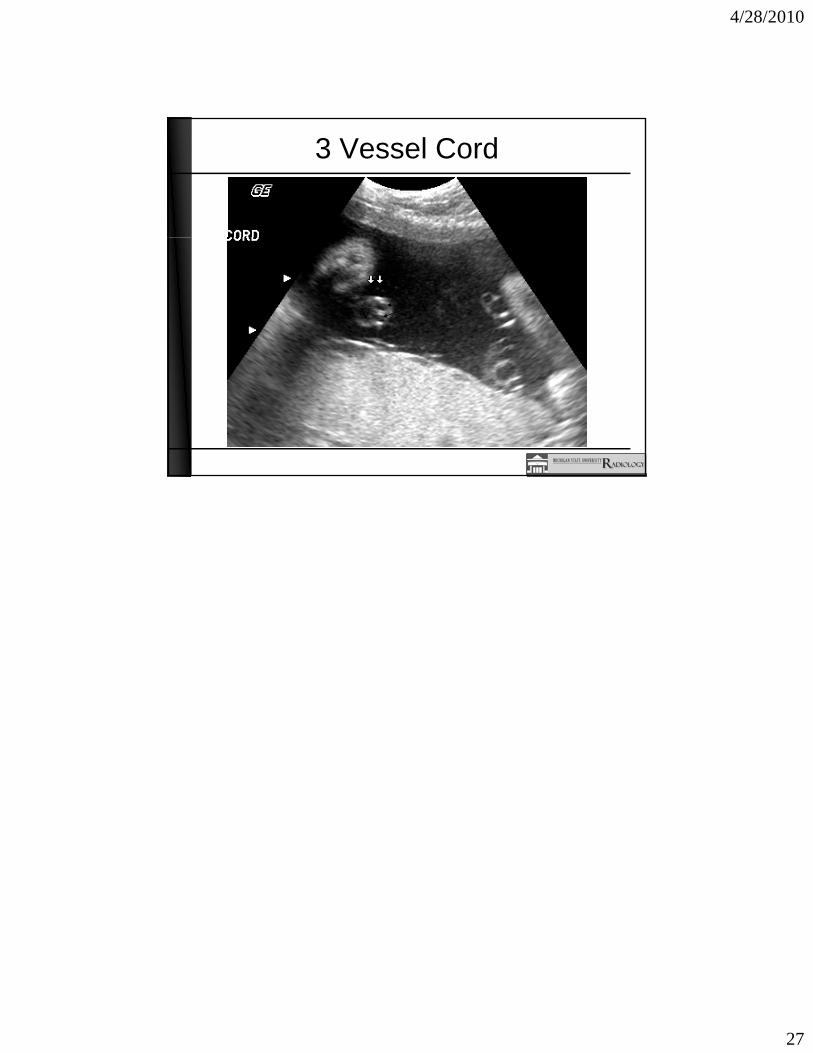
3 Vessel Cord
V A