racial stratification of traditional medicine’s ...hendun.org/journals/mi/pdf/mi-16-1-107.pdf ·...
TRANSCRIPT

Research Article
Medicina Interna: Open Access (MI)
Medcina Intern, 2016 Volume 1(1): 33-41
Racial Stratification of Traditional Medicine’s Consumption in South Africa?Fikile Mabel Vilakazi*
Department of Social Science and Philosophy, Opinkivi, 1st Floor, Keskussairaalantie 2, University of Jyvaskyla, Finland
*Corresponding author: Fikile Mabel Vilakazi, Department of Social Science and Philosophy, Opinkivi, 1st Floor, Keskussairaalantie 2, University of Jyvaskyla, Finland, Tel: +27 31 260 2433; Fax: +27 31 260 2433; Email: [email protected]
Received: October 21 2016; Accepted: December 10, 2016; Published: December 26, 2016
Keywords: Consumption culture, Racial stratification, Traditional medicine trade, Professionalization, Symbolic power and violence.
IntroductionPost-apartheid South Africa remains a highly stratified society
on variable grounds including race, ethnicity, culture, gender, sexual orientation and religion inter alia. Socio-economic inequalities are embedded in different areas including the economy, education, medicine, food and many other consumer related experiences that Lucy [28] best defines as a ‘culture of consumption’ which includes experiences such as the availability of a range of types of goods for sale, the marketization of basic human life experiences like health, housing, education, water, land and food. This paper discusses a ‘culture of consumption’ with specific reference to the marketization and sales of traditional medicines and the embeddedness of stratification and inequalities surrounding such a consumption culture in South Africa. Consumption of traditional medicine is one of the most visible experiences in South Africa. It is practiced by people of all races, genders, cultures and ages. The focus is on social stratification related to a racialized economy and its interplay with a ’consumption culture’ of traditional medicine given South Africa’s past of apartheid. The author’s positionality in this discussion is located in the sociology of consumption, the sociology of professions and feminist theories and specifically surfaces ’symbolic violences’ [7] and ’power over’[4] that are hovering as ghosts over and as remnants in post-apartheid South Africa in the context of traditional medicines consumption culture .
Although the discussion is primarily focused on South Africa, regional and international comparison in some instances is provided, particularly from Brazil, Russia, India and China [BRICS]. This is a deliberate comparison in view of South Africa’s membership to BRICS and the recent development of the BRICS Medical Alliance which aims to promote cooperation between BRICS countries including on traditional medicines. In 2013 BRICS Ministers of Health
Copyright: © 2016 Fikile Mabel Vilakazi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
formed a ‘BRICS Medical Alliance whose objective is to contribute [to] innovative solutions that address the common indigenous and unique medicinal problems and needs of populations in BRICS countries’ [9]. Similar prospects are presented by an action plan for agricultural cooperation which BRICS signed in 2010 in Moscow [8]. In addition, the paper argues for the importance of an honest and open public engagement regarding the need to be cautious and transform a noticeably violent discourse that surrounds the debate about the professionalization of traditional healing not just in South Africa but in many parts of the globe, particularly in Africa, Asia and Latin America.
ObjectivesThe key objective of the review was to understand the
current structuration of race and economics in the context of professionalization of traditional medicine consumption culture in South Africa.
Materials and MethodsThis was largely a retrospective cohort study that derived data
from events that have happened in the past over a period of time [56]. In this context, events of the first 20 years of democracy (1994-2014) in South Africa were studied relying primarily on secondary narratives of traditional healers, public opinion and academic literature. The study takes a standpoint that human behaviour and the ways in which
AbstractIntroduction: Post-apartheid South Africa remains highly stratified on variable grounds including race. The 8.9 percent (whites) of the total population has an average income per capita that is five times higher than that of 79.2 percent (blacks). Socio-economic inequalities are embedded in a ‘culture of consumption’ which includes the availability of goods for sale and the marketization of basic human life experiences including health.
Study Objective: The objective of this review was to ascertain the racial status quo in traditional medicines consumption.
Results: Literature shows that the consumption of traditional medicines is saturated within the Black population at 72 percent whilst data on other race groups is scarce. Evidence points to a racialized economy that existed for more than 100 years (1910 – 2010) with the Black population perpetually positioned at the bottom of the hierarchy.
Conclusion: Further empirical data is recommended to determine whether traditional medicine’s consumption in South Africa is symbolically contaminated by colonial and apartheid legacies.

Citation: Fikile Mabel Vilakazi (2016) Racial Stratification of Traditional Medicine’s Consumption in South Africa? Medcina Intern 2016 1: 107
Medcina Intern, 2016 Volume 1(1): 34-41
people construct and make meaning of their worlds and lives are highly variable and locally specific [25]. The approach therefore relied primarily on the population’s narratives of their own experiences and lived realities as experienced, self-articulated and narrated through secondary means. The key question of the study was how traditional healers experience professionalization in South Africa specifically in relation to medicinal plants consumption culture as an aspect of professionalization? Secondly, how does racial structuration present itself in the economics of traditional medicine’s consumption culture in view of South Africa’s colonial and apartheid legacies? Data was collected as a literature review in order to identify what is known and unknown in the subject area, identify areas of controversy or debate, and help formulate questions that need further research [5].
ResultsA consumption culture of traditional medicine in South Africa
Literature shows that South Africa has a rich plant biodiversity of more than 24000 indigenous plants, representing about 10 percent of all higher plants on earth [53] compared to 10-20 percent in Brazil [10,11] whilst China ranks as third in the world in a number of biodiversity species after Brazil and Colombia [26,27]. The high level of consumption of medicinal plants by citizens in South Africa has resulted in a market demand of certain plant species and in some instances unsustainable harvesting of demanded plant species particularly in kwaZulu Natal province [15]. In addition, there is a myriad of colored traditional healers dispersed throughout the Western and the Northern Cape tracing their roots from indigenous Khoisan heritage mostly visible as Rastafari bush doctors [41], izangoma or herbalists engaged in an almost unnoticed medicinal plants trade estimated at 15.6 million USD per annum [40].
Similarly, Indian [and Black] traditional herbalists and healers have largely incorporated both African and Indian herbs into herbal medicinal trade and operating visibly in Johannesburg, Cape Town and Kwa-Zulu Natal provinces [18]. The struggle for economic capital in medicinal plants trade in South Africa is happening within a context of a highly racialized economy where less than 8.9 percent (whites) of the total population have an average income per capita that is five times higher than that of 79.2 percent (blacks) [14]. Figure 1 shows how income disparities between different races have widened in South Africa since 1910 marking the effects of British colonial and white apartheid domination on South Africa’s racialized economy.
It is noticeable how the Asian population’s average income has rapidly followed that of Whites since the year 2000. Desilver [14] indicates that the actual race amongst the Asian population which enjoys such rapid income growth is that of Indian decent where the infographic (figure1) shows that their average income has increased by 1,982 per person’s Rand value, marking the highest increase between 1917 and 2011. The sharpness of such an increase is noticeable for all race groups in the first and second decades of the democratic dispensation (1990 – 2010), although its influence on the income gap is very little because the gap had widened too much in the preceding 80 years (1910 – 1990) of colonialism and apartheid. This scenario can be easily equated to a ‘symbolic hierarchy’ alluded to by Allen and Anderson [2] which is unpack later in this paper.
Marketization, sales and reliance on traditional medicines and racial stratification
Reliance on and demand for traditional medicines by race: Furthermore, literature reveals that the population of South Africa has increasingly become reliant on traditional medicinal plants for treatment of diseases related to primary health care. This trend is also noticed in other regions of the world where it is estimated that ‘more
than 80 percent of the population in Asia, Africa and Latin America use traditional health care services to meet their primary health care needs’ [52]. The 80 percent estimate in South Africa has become a subject of contestation as seen in a recent household survey which found that only 0.1 percent of the population preferred traditional health practitioners for primary health care compared to 61.2 percent who would go to a public clinic thereby arguing that the WHO 80 percent estimates have no empirical basis [64]. This research was released two years after Nxulamo et al (2011) found that only 1.2 percent of the population utilizes traditional healers. This is a huge discrepancy and warrants further interrogation, especially because there are other studies independent from WHO that have found almost similar results as WHO. One example is a research in South Africa which revealed not so long ago that about 72 percent of black South Africans consumed traditional medicines as a decision based on personal health choice amongst many other possibilities [30]. Again, this estimation shows a large discrepancy from the 0.1 percent findings of Wilkinson [64] and the 1.2 percent of Nxumalo et al [33-36].
Further to this, empirical studies widely exist on the role and importance of traditional medicines in primary health care globally indicating the need for possible integration of traditional medicines and allopathic medicines in primary health care [39]. In Brazil for instance, such integration was started as early as 1986 with the support of the Ministry of Health when a first outpatient hospital was established on Ayurveda medicine in the state of Goiás and still exist today [46,47]. In India a Minister of AYUSH [Ayurveda, Yoga, Unani, Sidhha and Homeopathy] was appointed on the 9th of November 2014 [1] to head a newly formed ministry of AYUSH after being a department for a year under the Ministry of Health in 2013. In addition, traditional healers across India formed a pan-India forum that would press upon government to recognize time-tested medicinal practices that are beyond the purview of Ayurveda, Unani, Siddha and Homeopathy, noting that the meritorious among them deserved administrative patronage’ [43]. In South Africa, a discourse and attempts for integration of traditional and allopathic medicines became intense mostly as part of a holistic response to the management and treatment of HIV/AIDS related illnesses [45,65]. The timing of such a demand for traditional medicines integration and/or recognition remains more relevant now given that there is increased global growth of more than 10 percent on traditional medicinal products for primary health care particularly in BRICS countries as a result of increased regulation, recognition and packaging as demonstrated in Figure 2 [17].
The demand and reliance on traditional medicines is manifested in various forms including the usage of medicinal plants for management and treatment of diseases [57,46,22,33] and the usage of wild medicinal plants both as food and as medicine amongst many other things [60]. One of the most recent empirical data concludes and cautions that ‘ethnopharmacology; biodiversity, agriculture, food and nutrition are inextricably linked but suffer from compartmentalization and a lack of communication which have to be overcome and [that] awareness [is] required on the role played by diversity of crops, especially local species, and consumption of wild species in achieving balanced nutrition’[21]. It is clear that wild plants continue to form a significant proportion of the global food basket [3]. In South Africa, this is factual in as far as it speaks to the question of hunger and starvation where literature shows that affected citizens often resort to consumption of wild plants as an alleviation mechanism [42,12,34]. In some instances there have been casualties and fatalities because some citizens do not always know about the toxicity of wild plants that may cause harm when they resort to them to alleviate hunger [49-51].
Nonetheless, the demand and reliance on traditional plants is proven to be high so much that there is looming extinction of plant

Citation: Fikile Mabel Vilakazi (2016) Racial Stratification of Traditional Medicine’s Consumption in South Africa? Medcina Intern 2016 1: 107
Medcina Intern, 2016 Volume 1(1): 35-41
Figure 1: Average income and population by racial groups in South Africa

Citation: Fikile Mabel Vilakazi (2016) Racial Stratification of Traditional Medicine’s Consumption in South Africa? Medcina Intern 2016 1: 107
Medcina Intern, 2016 Volume 1(1): 36-41
species in most BRICS countries like in South Africa [15] and Brazil [24] due to overharvesting and/or suppression of Savannas and forests. As a result, extinct species are traded at a higher price [30]. In China the need to conserve biodiversity is highly desirable given that it is the third richest country in the world on plant biodiversity after Colombia and Brazil [27]. Regardless of the looming threat of extinction, BRICS countries occupy a sizable portion of arable land and forests that have potential for the production of medicinal plants for the rest of its citizens and the world. Figure 3 shows utilization of forest area in BRICS countries by the year 2011.
Literature reveals that the texture of the demand for utilization of traditional medicines in South Africa is currently concentrated amongst the Black population at 72percent [30]. However, there is an information gap available regarding the demand and reliance on
traditional medicines by other race groups, which leaves a myriad of unanswered questions regarding the remaining 28 percent amongst other racial groups. There is a need for further research in this area. Figure 4 demonstrates the current statistics of reliance and demand of traditional medicines by race in South Africa according to existing academic literature. Comparative racial data on other BRICS countries is also scarce. In Brazil, for instance, literature shows income disparities between racial groups as a factor that contributes to higher mortality rates for the Black population compared to the White population [20], but racial demographic data that is specific to the utilization and demand for traditional medicines is scarce.
Marketization and sales of traditional medicines by race: Currently, there is very limited literature that is available on traditional medicines trade by race. As a result the actual race of the seller on the trade
Figure 2: Expansion of herbal/traditional products in the World.

Citation: Fikile Mabel Vilakazi (2016) Racial Stratification of Traditional Medicine’s Consumption in South Africa? Medcina Intern 2016 1: 107
Medcina Intern, 2016 Volume 1(1): 37-41
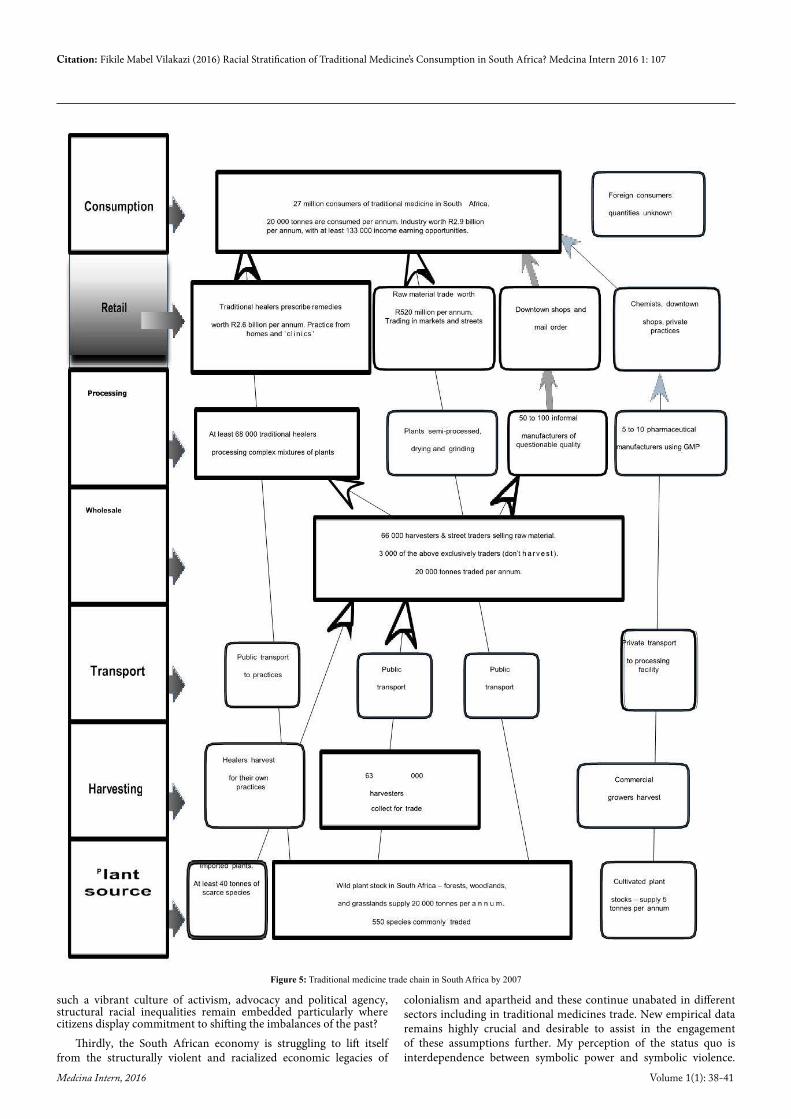
chain of traditional medicines remains unknown. There is a need for additional research in this area. Figure 5 shows the traditional medicine trade chain by 2007, but it does not provide the racial demographic data of traders.
DiscussionRacial stratification in traditional medicine’s ‘marketization and sales’ as a form of consumption culture.
The black population are the majority consumers of traditional medicines in South Africa: In view of existing literature, it is clear that consumption (daily utilization) of traditional medicines is commonly found within the Black population at 72 percent in South Africa [30]. This means that traditional medicine consumption can be considered a part of everyday life for the Black population. The essence of ‘daily life’ is often underestimated in society, but Scott [55] reminds us that the routines, repetitive and rhythmic things that we do every day at the same time in the same places, day after day, like taking care of our health, are the ones that reproduce social life albeit they may seem trivial. If taking care of one’s health on a daily basis in the form of utilization of traditional medicine is seen as part of a consumption culture, then, I agree with Scott [55] and Allen and Anderson [2] that ‘consumption culture’ as defined by Lucy [28] is a socially conditioned phenomenon. It becomes crucial to then analyze
and position the nature of such a social conditioning within a context in which it occurs in order to fully grasp its full measure of expression as I will do now in the context of traditional medicines trade in South Africa. The logic of such an analysis emanates from the fact that macro –level social order is always dependent on micro-level interactions for its accomplishments and reproduction [55].
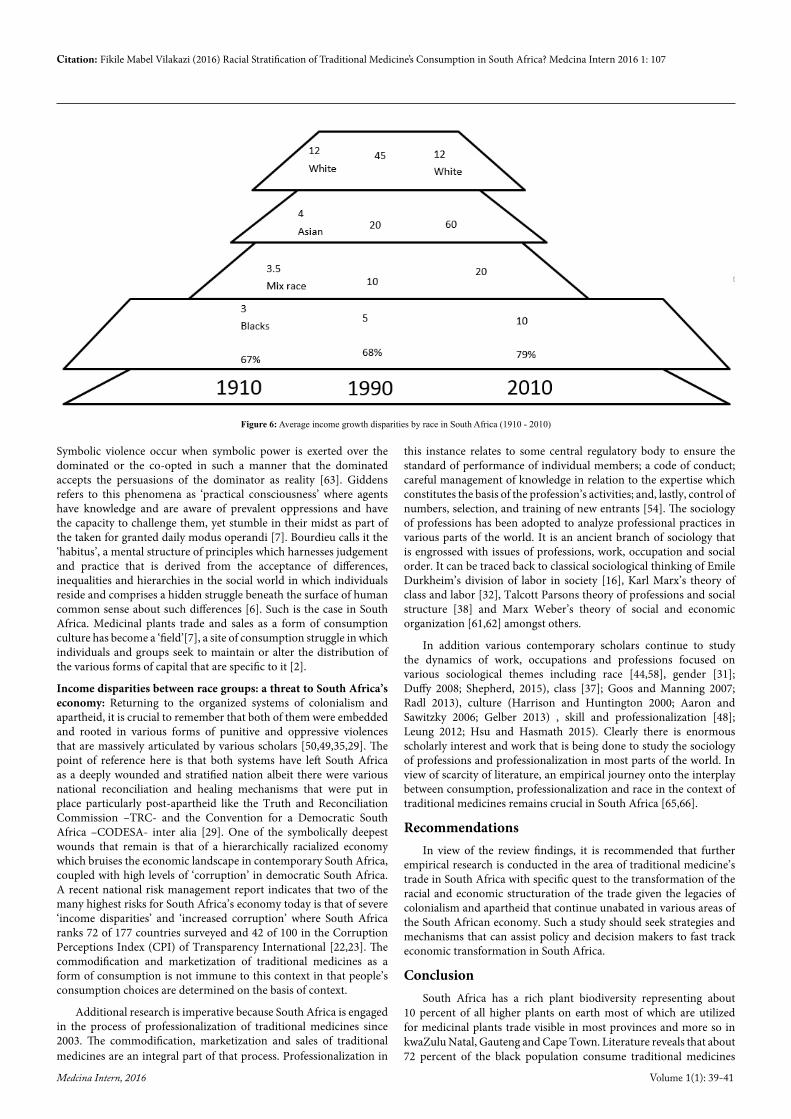
The black population remains at the bottom of the economic hierarchy in South Africa: The first task of analysis in this context is to return to Allen and Anderson’s [2] concept of ‘symbolic hierarchy’ which is said to be determined and maintained by the socially dominant in order to enforce their distinction from other classes in society. The rationale for invoking this concept in the context of South Africa is that literature shows a symbolically hierarchical economy that exists perpetually dating back from colonialism, surpassing apartheid and now in the democratic dispensation. This symbolic hierarchy positions the Black population at the bottom of the economic ladder for a period of 100 years. On the other hand, literature shows the Black population to be the majority (72percent) of the population that utilizes traditional medicines. In view of the historical imbalances, it becomes crucial to then analyze where that 72percent is located in the consumption chain of traditional medicines in order to ascertain transformation or lack of it thereof in the field of traditional medicine consumption. If one has to turn the Mandela infographic (figure 1) into a hierarchy, it will look like figure 6 [58,59].
The second task is to connect this hierarchy to the 72 percent of the Black population that utilizes traditional medicines on a daily basis remaining mindful that the racial identity of traders on traditional medicines is not known due to insufficient empirical data. A myriad of empirical questions and assumptions emerge when such a connection is made. One assumption is that a ‘consumption culture’ of traditional medicines in South Africa is itself a racialized economic culture in that the Black population by virtue of being at the bottom of the economic ladder, cannot be traders but mostly buyers of traditional medicines.
If this assumption is true, it means that the consumption positioning of the Black population in traditional medicines trade is happening from a subjugated conditionality. Theoretically, it appears that the South African racialized economy is stuck in a place which the structuration theory would call an ongoing cycle between structure and agency, where each feeds back into the other [55]. It performs like a cyclic trap where the kind of agency that prevails does not seem to shift the structural barriers to a place of transformation, but work within it and thereby impede possibilities for socio-economic transformation, in this context, racial transformation in the economy. This is the kind of ‘duality of structure’ that Giddens attests, to show that sometimes in social organization the duality between structure and agency is mutually enhancing in such a way that each is trapped by the other almost to a point of no escape [12,13].
Interdependence between symbolic power and symbolic violence in traditional medicine’s trade in South Africa: The second assumption is that the Black population remains at the bottom of the economic ladder by virtue of oppressive systemic arrangements of colonialism and apartheid and they continue to be pervasively violated by the economic system even in the democratic dispensation and the commodification of traditional medicines is not immune to such structurally conditioned socio-economic inequalities. The interest is in the role of symbolic power and violence in maintaining and sustaining the duality of structure in Giddens’s terms, especially in the South African context. One is aware of the antimonies of structure and the intellectual battles that surround it with regards to ontology, methodology and epistemology between Levi Straus, Anthony Giddens, Pierre Bourdieu and Sewell [19,26] but this paper does not elaborate on that debate. Why is it that in a country with
Figure 3: Utilization of forest area by BRICS countries by 2011
Figure 4: Daily consumption of traditional medicines by race in South Africa by 2007.
Citation: Fikile Mabel Vilakazi (2016) Racial Stratification of Traditional Medicine’s Consumption in South Africa? Medcina Intern 2016 1: 107
Medcina Intern, 2016 Volume 1(1): 38-41
such a vibrant culture of activism, advocacy and political agency, structural racial inequalities remain embedded particularly where citizens display commitment to shifting the imbalances of the past?
Thirdly, the South African economy is struggling to lift itself from the structurally violent and racialized economic legacies of
colonialism and apartheid and these continue unabated in different sectors including in traditional medicines trade. New empirical data remains highly crucial and desirable to assist in the engagement of these assumptions further. My perception of the status quo is interdependence between symbolic power and symbolic violence.
Figure 5: Traditional medicine trade chain in South Africa by 2007
Citation: Fikile Mabel Vilakazi (2016) Racial Stratification of Traditional Medicine’s Consumption in South Africa? Medcina Intern 2016 1: 107
Medcina Intern, 2016 Volume 1(1): 39-41
Symbolic violence occur when symbolic power is exerted over the dominated or the co-opted in such a manner that the dominated accepts the persuasions of the dominator as reality [63]. Giddens refers to this phenomena as ‘practical consciousness’ where agents have knowledge and are aware of prevalent oppressions and have the capacity to challenge them, yet stumble in their midst as part of the taken for granted daily modus operandi [7]. Bourdieu calls it the ‘habitus’, a mental structure of principles which harnesses judgement and practice that is derived from the acceptance of differences, inequalities and hierarchies in the social world in which individuals reside and comprises a hidden struggle beneath the surface of human common sense about such differences [6]. Such is the case in South Africa. Medicinal plants trade and sales as a form of consumption culture has become a ‘field’[7], a site of consumption struggle in which individuals and groups seek to maintain or alter the distribution of the various forms of capital that are specific to it [2].
Income disparities between race groups: a threat to South Africa’s economy: Returning to the organized systems of colonialism and apartheid, it is crucial to remember that both of them were embedded and rooted in various forms of punitive and oppressive violences that are massively articulated by various scholars [50,49,35,29]. The point of reference here is that both systems have left South Africa as a deeply wounded and stratified nation albeit there were various national reconciliation and healing mechanisms that were put in place particularly post-apartheid like the Truth and Reconciliation Commission –TRC- and the Convention for a Democratic South Africa –CODESA- inter alia [29]. One of the symbolically deepest wounds that remain is that of a hierarchically racialized economy which bruises the economic landscape in contemporary South Africa, coupled with high levels of ‘corruption’ in democratic South Africa. A recent national risk management report indicates that two of the many highest risks for South Africa’s economy today is that of severe ‘income disparities’ and ‘increased corruption’ where South Africa ranks 72 of 177 countries surveyed and 42 of 100 in the Corruption Perceptions Index (CPI) of Transparency International [22,23]. The commodification and marketization of traditional medicines as a form of consumption is not immune to this context in that people’s consumption choices are determined on the basis of context.
Additional research is imperative because South Africa is engaged in the process of professionalization of traditional medicines since 2003. The commodification, marketization and sales of traditional medicines are an integral part of that process. Professionalization in
this instance relates to some central regulatory body to ensure the standard of performance of individual members; a code of conduct; careful management of knowledge in relation to the expertise which constitutes the basis of the profession’s activities; and, lastly, control of numbers, selection, and training of new entrants [54]. The sociology of professions has been adopted to analyze professional practices in various parts of the world. It is an ancient branch of sociology that is engrossed with issues of professions, work, occupation and social order. It can be traced back to classical sociological thinking of Emile Durkheim’s division of labor in society [16], Karl Marx’s theory of class and labor [32], Talcott Parsons theory of professions and social structure [38] and Marx Weber’s theory of social and economic organization [61,62] amongst others.
In addition various contemporary scholars continue to study the dynamics of work, occupations and professions focused on various sociological themes including race [44,58], gender [31]; Duffy 2008; Shepherd, 2015), class [37]; Goos and Manning 2007; Radl 2013), culture (Harrison and Huntington 2000; Aaron and Sawitzky 2006; Gelber 2013) , skill and professionalization [48]; Leung 2012; Hsu and Hasmath 2015). Clearly there is enormous scholarly interest and work that is being done to study the sociology of professions and professionalization in most parts of the world. In view of scarcity of literature, an empirical journey onto the interplay between consumption, professionalization and race in the context of traditional medicines remains crucial in South Africa [65,66].
RecommendationsIn view of the review findings, it is recommended that further
empirical research is conducted in the area of traditional medicine’s trade in South Africa with specific quest to the transformation of the racial and economic structuration of the trade given the legacies of colonialism and apartheid that continue unabated in various areas of the South African economy. Such a study should seek strategies and mechanisms that can assist policy and decision makers to fast track economic transformation in South Africa.
ConclusionSouth Africa has a rich plant biodiversity representing about
10 percent of all higher plants on earth most of which are utilized for medicinal plants trade visible in most provinces and more so in kwaZulu Natal, Gauteng and Cape Town. Literature reveals that about 72 percent of the black population consume traditional medicines
Figure 6: Average income growth disparities by race in South Africa (1910 - 2010)

Citation: Fikile Mabel Vilakazi (2016) Racial Stratification of Traditional Medicine’s Consumption in South Africa? Medcina Intern 2016 1: 107
Medcina Intern, 2016 Volume 1(1): 40-41
daily whilst data from other racial groups is scarce. The vibrant traditional medicines trade amongst the black, colored and Indian populations in the urban cities of kwaZulu Natal, Gauteng and Cape Town is estimated at 15.6 million USD per annum. This is happening within an economic context where the black population continues to be subjugated since 1910. Literature shows that the black population remained at the bottom of the economic hierarchy for about 100 years between 1910 and 2010 marking the continued presence of colonialism and apartheid legacies in the economic system of South Africa. There were slight economic gains noticeable between 1990 and 2010 but the economic gap was so huge that such gains have not had any impact towards economic transformation even during the democratic dispensation.
There seems to be a symbolic economic hierarchy that is determined and maintained by the socially dominant in order to enforce their distinction from other classes in society. An interdependence between symbolic power and symbolic violence is observed where the dominated seem to have accepted the economic domination as reality and are trapped at the ‘habitus’ in that they may be aware of the ongoing economic struggles but they have accepted them as a matter of mere differences between the dominator and the dominated. Symbolic violence occurs when the dominated accept the dominated state as reality. However, it is not known empirically how much of the status quo affects the traditional medicine trade. Additional research in recommended to focus on racial and economic structuration of the traditional medicine trade to ascertain the effects of the status quo on traditional medicine trade.
References
1. FP (2014) India PM Modi appoints Yoga minister. India: EURONews.
2. Allen D, Anderson P (1994) Consumption and social stratification: Bourdieu’s Distinction. Advances in consumer research 70-74.
3. Bharucha Z, Pretty J (2010) The roles and values of wild foods in agricultural systems. Philosophical Transitions of the Royal Society 365: 2913-2926.
4. Bilgic A (2013) Trust and power of social movements: The case of feminist solidarity in Tahrir. Ankara, Turkey: Bilkent University Press.
5. Bolderston A (2008) Writing an Effective Literature Review. Journal of Medical Imaging and Radiation Sciences 39: 86-92.
6. Bourdieu (1996) Physical space, social space and habitus. Oslo: University of Oslo Institute for Sociology.
7. Bourdieu P (1984) Distinction:A Social Critique of the Judgment of Taste. Cambridge: Havard University Press.
8. http://www.brics5.co.za/about-brics/sectorial declaration/agriculture-ministers meeting/brics- agricultural-action/
9. BRICS (2013a) Constitution: BRICS Medical Alliance. BRICS Ministers of Health.
10. BRICS (2013b) BRICS Joint Statistical Report. South Africa: BRICS.
11. Candim M, Hingst-Zaher E (2010) Brazil´s biodiversity crisis. ICOM News 2.
12. Cloete P, Idsardi E (2012) Bio-fuels and Food Security in South Africa: The Role of Indigenous and Traditional Food Crops.
13. Coad A, Jack L, Kholeif A (2015) Structuration Theory: Reflections on its Further Potential for Management Accounting Research. Qualitative Research in Accounting & Management 12: 153- 171.
14. http://www.pewresearch.org/fact- tank/2013/12/06/chart-of-the-week-how-south-africa-changed-and-didnt-over-mandelas-lifetime/
15. http://www.scienceinafrica.com/old/index.php?q=2002/november/bark.htm
16. Durkheim E (1964) The division of labor in society. New York: Free Press of Glencoe.
17. http://www.euromonitor.com/a-global-overview-of-herbal-traditional-products/report
18. Flint K (2008) Healing traditions:African medicine, cultural exchange and competition in South Africa, 1820 - 1948. Durban: University of KwaZulu Natal Press.
19. Giddens A (1984) The Constitution of society. Cambridge: Polity Press.
20. Giuffrida A (2007) Racial and ethnic disparities in health in Latin America and the Carribean. Inter-American Development Bank.
21. Heywood V (2011) Ethnopharmacology, food production, nutrition and biodiversity conservation: Towards a sustainable future for indigenous peoples. Journal of Ethnopharmacology 137: 1-15.
22. Hughes G, Blouws T, Aboyade O, Davids D, Mbamalu O, et al. (2015) An ethnobotanical survey of medicinal plants used by traditional health practitioners to manage HIV and its related opportunistic infections in Mpoza, Eastern Cape Province, South Africa. Journal of Ethnopharmacology 171: 109-115.
23. IRMSA (2015) IRMSA Risk Report: South Africa Risks 2015. South Africa: The Institute of Risk Management South Africa.
24. Landim M (2010) Brazil’s biodiversity crisis. Heritage in danger Brazil 2: 14-15.
25. LeCompte MD, Schensul JJ (2010) Designing and Conducting Ethnographic Research. United Kingdom: Altamira Press.
26. Lizardo O (2010) Beyond the antinomies of structure: Levi-Strauss, Giddens, Bourdieu, and Sewell. Theory and Society 39: 651-688.
27. http://cdn.intechopen.com/pdfs-wm/21534.pdf
28. Lucy C (2011) Consumer culture. Cambridge. United Kingdom: Polity Press.
29. Mamdani M (2015) Beyond Nuremberg: The Historical Significance of the Post-apartheid Transition in South Africa. Politics & Society 43: 61-88.
30. Mander M, Ntuli L, Diederichs N, Mavundla K (2007) Economics of the traditional medicine trade in South Africa: health care delivery. Sabinet online 189-196.
31. Martin P (2006) Practising Gender at Work: Further Thoughts on Reflexivity. Gender, Work & Organization 13: 299-316.
32. Marx K, Engels F (1988) Economic and philosophic manuscripts of 1844. New York: Amherst: Prometheus Books.
33. Masevhe N, McGawv L, Eloff J (2015) The traditional use of plants to manage candidiasis and related infections in Venda, South Africa. Journal of Ethnopharmacology 168: 367-372.
34. Mavengahama S, McLachlan M, deClercq W (2013) The role of wild vegetable species in household food security in maize based subsistence cropping systems. Springer 1-7.
35. Mhlauli M, Salani E, Mokotedi R. (2015) Understanding apartheid in South Africa through the racial contract. International Journal of Asian Social Science 5: 203-219.
36. Nxumalo N, Alabab O, Harrisa B, Chersicha M, Goudge J (2011) Utilization of traditional healers in South Africa and costs to patients: Findings from a national household survey. Journal of Public Health Policy 32: 124-136.
37. Nzimande B (1991) “The Corporate Guerrillas”– Class Formation and the African Petty Bourgeoisie in Post-1973 South Africa. kwaZulu Natal: University of Natal.
38. Parsons T (1939) The professions and social structure. Social Forces 17: 457-467.
39. Payyappallimana U (2009) Role of Traditional Medicine in Primary Health Care: An Overview of Perspectives and Challenges. Yokohama Journal of Social Sciences 14: 57-77.
40. Petersen L, Charman A, Moll E, Collins R, Hockings M (2014) Bush Doctors and Wild Medicine: The Scale of Trade in Cape Town’s Informal Economy of Wild Harvested Medicine and Traditional Healing. Society and Natural Resources 27: 315-336.
41. Philander L (2012) Hunting Knowledge and Gathering Herbs: Rastafari Bush Doctors In the Western Cape, South Africa. Journal of Ethnobiology 32: 134-156.
42. Pitso FS, Lebese M (2014) Traditional Uses of Wild Edible Plants in Arid Areas of South Africa. Journal of Human Ecology 48: 23-31.

Citation: Fikile Mabel Vilakazi (2016) Racial Stratification of Traditional Medicine’s Consumption in South Africa? Medcina Intern 2016 1: 107
Medcina Intern, 2016 Volume 1(1): 41-41
43. http://www.business-standard.com/article/pti-stories/traditional-healers-form-pressure-group-114110700801_1.html
44. Reskin B (2000) Getting It Right: Sex and Race Inequality in Work Organizations. Annual Review of Sociology 26: 707 - 709.
45. Richter M (2003) Traditional Medicines and Traditional Healers in South Africa: Discussion paper prepared for the Treatment Action Campaign and AIDS Law Project. Cape Town: Treatment Action Campaign and the Aids Law Project.
46. http://www.scidev.net/global/medicine/feature/traditional-medicine-modern-times-facts-figures.html
47. Rosa C (2012) Traditional Medicine and Complementary/Alternative Medicine in Primary Health Care: The Brazilian Experience. In Tech 65-82.
48. Rothman R (1998) Working: Sociological perspectives. New Jersey: Princeton Hall.
49. Ryana E (2015) Violence and the politics of prestige: the fascist turn in colonial Libya. Modern Italy. 20: 123-135.
50. Rydstrom H (2015) Politics of colonial violence: Gendered atrocities in French occupied Vietnam. European Journal of Women’s Studies 22: 1-17.
51. http://www.sabc.co.za/news/a/7fa3c100469667a78303bb8c3c6d57d4/Joburg- family-dies-after-eating-poisonous-mushrooms-20141612
52. Sambo L (2010) The decade of African traditional medicine: Progress so far. African Health Monitor 14: 4-6.
53. SAMRC, CSIR, NDH (2005) National Reference Centre for African Traditional Medicines: A South African Model. Pretoria: National Department of Health; the South African Medical Council and the Center for Scientific Inquiry and Research.
54. Scott J, Marshall G (2009) Professionalisation. New York: Dictionary of Social Science: New York: Dictionary of Social Sciences: Oxford University Press.
55. Scott S (2009) Making sense of everyday life. Cambridge: Polity Press.
56. Sedgwick P (2014) Retrospective cohort studies: advantages and disadvantages. BMJ 1-2.
57. Semenya S, Potgieter M (2014) Bapedi traditional healers in the Limpopo Province, South Africa: Their socio-cultural profile and traditional healing practice. Journal of Ethnobiology and Ethnomedicine 10: 1-12.
58. Sugrue T (2014) The origins of the urban crisis: race and inequality in postwar Dutroit. New Jersey: Princeton University Press.
59. h t t p : / /www.economis t . com/node /21580215? f s r c=scnpe rcen t2 Ftwpercent2Fdcpercent2F&percent3Ffsrcpercent3Dscnpercent2F=twpercent2 Fdc
60. Touwaide A, Appetiti E (2015) Food and medicines in the Mediterranean tradition. A systematic analysis of the earliest extant body of textual evidence. Journal of Ethnopharmacology 167: 11-29.
61. Vilakazi F, Dinbabo M (2015) Regulation of African Traditional Medicines and Public Participation: Empirical Evidence from South Africa. Journal of Studies on Ethnomedicine 9: 109-116.
62. Weber M (1997) The theory of social and economic organization. New York: Simon and Schuter.
63. http://www.ssc.wisc.edu/~wright/Found-c4rev.pdf
64. http://africacheck.org/reports/do-80-of-south-africans-regularly-consult-traditional-healers- the-claim-is-false/#sthash.UcFyCcoe.dpuf
65. Wreford J (2003) Shaming and Blaming: Medical Myths, Traditional Health Practitioners and HIV/AIDS in South Africa. Cape Town: Aids and Society Research Unit, University of Cape Town.
66. Wreford J (2006) Talking with the white: sharing the experiences of white sangomas in South Africa. Cape Town: Aids and Society Research Unit, Center for Social Science.