queensland health nutrition standards for meals and menus · the health outcomes and experience of...
TRANSCRIPT

QUEENSLAND HEALTHNutrition Standards
for Meals and Menus2015

Page 2
Document title: Queensland Health Nutrition Standards for Meals and Menus
Publication date: May 2015
ISBN: TBC
Author: State-wide Foodservices Network
Audience: Foodservice personnel and dietitians within Queensland Health facilities
Review date: 2018
Endorsed by: State-wide Foodservices NetworkContact: [email protected]
URL: http://qheps.health.qld.gov.au/statewidefoodservice/home.htm
Disclaimer: These Standards have been prepared to assist menu planning in Queensland Health Facilities to meet patient and client needs. Menu planning shall be a collaborative process and include input from dietitians, foodservice managers and other key stakeholders.
This document does not replace or remove local assessment processes that should be considered during menu planning. Information within these standards is current at time of publication.
© State of Queensland (Department of Health) 2013
This work is licensed under a Creative Commons Attribution Non-Commercial Share Alike 2.5 Australia licence. In essence, you are free to copy and communicate the work in its current form for non-commercial purposes, as long as you attribute Queensland Health State-wide Foodservices Network, you distribute any derivative work only under this licence and you abide by the licence terms. To view a copy of this licence, visit: http://creativecommons.org/licenses/by-nc-sa/2.5/au/
ForfurtherinformationcontactDietitian-Consultant,State-wideFoodservicesNetwork,DepartmentofNutritionandDietetics,RoyalBrisbaneandWomen’sHospital,ButterfieldStHerston, QLD4029,[email protected],orphone(07)36362288.Forpermissionsbeyondthescopeofthislicencecontact:IntellectualPropertyOfficer, QueenslandHealth,GPOBox48,BrisbaneQld4001,[email protected],phone(07)32341479.
OriginallywrittenbyQueenslandHealthNutritionStandardsWorkingParty,andfirstpublishedinTBC2011. This is version two of Queensland Health’s Nutrition Standards for Meals and Menu, and will remain current until reviewed.
HMMU Apr’13 0425_jk / CMM August '15 0527_ss

Page 3
CONTENTSForeword ......................................................................................... 4 Nutrition Standards Working Party ............................................... 5 Purpose ...................................................................................... 6
Section 1 – Nutrition Standards ...................................................... 7 Overarching principle ................................................................. 8 Adult acute ................................................................................. 9 Adult acute (short stay patients) ................................................. 10 Maternity .................................................................................... 11 Paediatrics ................................................................................. 12 Residential aged care ................................................................. 13 Mental health and acquired brain injury ..................................... 14 Vegetarian and vegan ................................................................. 16 Therapeutic and medical diets .................................................... 17
Section 2 – Meal Component Specifications .................................... 18 Overview .................................................................................... 19 Main (protein) dishes ................................................................. 20 Soups ......................................................................................... 21 Sandwiches ................................................................................ 21 Desserts / Hot Breakfast Protein .................................................. 22 Snacks/mid-meals ..................................................................... 23 Fortificationofmenuitems ......................................................... 23 Portion sizes for meal items ........................................................ 24
Section 3 – Minimum Menu Choice ................................................. 25 How to use the tables ................................................................. 26 Adult acute and Residential aged care ........................................ 27 Texturedmodified ....................................................................... 31 Paediatrics .................................................................................. 34 Mental health and acquired brain injury ..................................... 38
Section 4 – User guide and definitions ............................................ 42 User Guide ................................................................................. 43 DefinitionsandAbbreviations .................................................... 46 References ................................................................................. 48
.Apendix 1 – Length of Stay data ...................................................... 50
Apendix 2 – Reference persons used in Standards Development ...... 54
Apendix 3 – Examples menus .......................................................... 57
Apendix 4 – Minimum serve sizes ................................................... 64

Page 4
FOREWORD The health outcomes and experience of those in our care can be improved with quality meals and good nutrition. The Queensland Health Nutrition Standards for Meals and Menus suports this by providing a framework to enable health facilities to meet the nutritional requirements of the majority of patients, residents and clients.
Originally published in 2012, these standards have been implemented fully or partially around the State and have been used to provide a sound nutritional basis to inform the food contracts for Queensland Health facilities.
As a result, the majority of Queensland Health facilities are able to meet the nutritional requirements of patients, residents and clients without the addition of costly suplements and extensive dietetic input. In conjunction with the Foodservice Best Practice Guidelines, the standards continue to set out overarching principles that ensure a quality, patient-focused, food and nutrition service.
This revised edition of the Queensland Health Nutrition Standards for Meals and Menus incorporates feedback on useability and practicality and aligns to the new NationalHealthandMedicalResearchCouncilAustralianDietaryGuidelines,whicharebasedonthebestavailablescientificevidence.
The full implementation of the Standards across Queensland Health facilities will not only continue to improve patient, resident, and client satisfaction and outcomes but also will be a cost effective way of providing nutrition treatment for malnourished and nutritionally vulnerable people in our care.
Hon Cameron Dick MPMinister for Health and Minister for Ambulance Services

Page 5
Nutrition Standards Review 2015, conducted by the Nutrition Standards Work Group, Statewide Foodservices Network.Michelle Suter Team Leader(Chair) Dietetics & Foodservices Caboolture Hospital
MembersKylie Bruce, Senior Dietitian Nutritionist, Nutrition & Dietetic Services, West Moreton Hospital & Health Service
Trish Cowlishaw, Senior Dietitian, Allied Health, Biloela Hospital
Denise Cruickshank Dietitian Consultant, Food Services Network, Dept of Nutrition & Dietetics, Royal Brisbane & Women’s Hospital
Julianne Donnelly, Team Leader, Nutrition & Dietetics, Princess Alexandra Hospital
Jennifer Ellick, Senior Dietitian – Nutrition & Dietetics Department, Royal Brisbane & Women’s Hospital
Amy Hannigan, Acting Team Leader, Nutrition & Dietetics, Princess Alexandra Hospital
Marion Hogg, Director Nutrition & Dietetics, Ipswich Hospital, West Moreton Hospital & Health Service
Lindsey Johnson, Advanced Dietitian (Food Services), Cairns & Hinterland Hospital & Health Service
Philip Juffs, Dietitian Team Leader Food Service, Nutrition & Dietetics, and Patients Food Services, Royal Brisbane & Women’s Hospital
Troy Litzow, SeniorProjectOfficer–FoodSafetyAuditor(FSA/0282), Food Services Network, Dept of Nutrition & Dietetics, Royal Brisbane & Women’s Hospital
Gai Moritz, Acting Senior Clinical Dietitian (Foodservices / Surgical), Nambour General Hospital
Tara Stevenson, Manager Food Services, Corporate Services, QEII Jubilee Hospital
Acknowledgment of original Work Group, 2012 Julianne Donnelly Redland Hospital (Chair)
Denise Cruickshank State-wide Foodservices Policy and Planning
Dr. Merrilyn Banks Royal Brisbane and Women’s Hospital
Kylie Bruce The Park – Centre for Mental Health
Karly Burton Princess Alexandra Hospital
Laurel Evans Gold Coast Hospital
Dr. Maree Ferguson Princess Alexandra Hospital
Christine Gugole Eventide Aged Care
Mary Hannan-Jones Queensland University of Technology
Fiona Hjortshoj Baillie Henderson Mental Health Facility
Sally McCray Mater Health Services
Anneli Reeves Logan Hospital
Jennifer Shirtcliff Toowoomba Hospital
Aoife Smith Mater Health Services
Michelle Suter Caboolture Hospital
Zoe Walsh Mater Health Services
Dr. Melinda White Royal Children’s Hospital
Liz Wisely Gold Coast Hospital
Katie Vardy Gold Coast Hospital

Page 6
PURPOSEThe Nutrition Standards for Meals and Menus (NSMM) are designed to provide a framework to assist menu planning in hospitals, residential aged care, mental health facilities and acquired brain injury units managed by Queensland Health (QH). This framework aims to meet the nutritional requirements of the majority of patients, residents, consumers and clients taking into account length of stay, age, nutritional status and type of facility. These Standards are designed to be used in conjunction with the State-wide Food Service KPI6 which inform aspects of foodservice provision, menu delivery, type and quality of meal service.
The NSMM are intended to be used by dietitians and foodservice managers in the design and assessment of menus and recipes. These Standards provide baseline requirements for general patient and resident menus. However, they do not replace the need for individual assessment of patients’ nutritional status or needs.
These Standards are based on the premise that patients in QH hospitals and residential aged care facilities are predominantly unwell and have different nutritional requirements to the general public. The Australia Dietary Guidelines 20134 are not aplicable as these recommendations aim to meet the nutritional needs of healthy populations.
However, mental health and acquired brain injury consumers are generally younger, tend to have longer lengths of stay8, 9 and are known to experience increased rates of chronic disease.10, 11 A preventative health aproach is warranted in menu design and choices for these groups, and as such, the National Health and Medical Research Council’s Nutrient Reference Values12 recommendations for chronic disease prevention and The Australia Dietary Guidelines 20134 were considered in the development of this section.
This document is presented in four sections as follows:
Section 1 outlines:
• the overarching principles; • thespecificprinciplesfordifferentpatientgroupsanddiettypes;and• the rationale and evidence for these principles.
Section 2 outlines:
• mealcomponentnutritionspecifications. Section 3 indicates how these principles are put into practice in a menu including:
• minimum menu choices required across the day; and• minimum menu choices required across the cycle.
Section 4 outlines:
• a user guide to assist with menu review process; and• definitionsusedthroughoutthedocument.
The State-wide Food Service Best Practice Guidelines2 and the State-wide Food Service KPIs6 are available on QHEPS intranet.

Nutrition Standards for Meals and Menus
SECTION 1NUTRITION STANDARDS

Page 8
NUTRITION Standards
1.0 OVERARCHING PRINCIPLEAim: Food provision shall meet the nutritional requirements of the majority of patients, residents, consumers and clients, taking into account age, clinical need, nutritional status, psychosocial needs, cultural and religious diversity and length of stay.
BACKGROUND/RATIONALE STANDARDS
Patients in hospital are usually acutely ill or suffering from chronic diseases and thisincreasestheirnutritionalrisk.Thereissignificantevidencethatpoororalintake in addition to clinical treatment or medical disease is responsible for poor nutritional status of patients in hospital.13,14,15,16
The literature suports a link between poor nutrition status, recovery from illness, increased complications, length of hospital stay and increased costs.17,18,19 The literature also suports that cost savings through reduced length of stay and complications can be realised if nutritionally at risk patients orresidentscanbeidentifiedandnutritionalsuportimplemented.20
The State-wide Food Service Key Performance Indicators6 (SFSKPI) have been developed to ensure a client focus and underpins these Standards.
This overarching principal aplies to the patient groups included in Sections 2.0 – 9.0: Adults – Acute, Maternity, Paediatrics, Residential Aged Care, Mental Health and Acquired Brain Injury, Vegetarian and Vegan and those on Therapeutic and Medical Diets.
1.1 Menu planning will be undertaken as a collaborative process and will include dietitians, foodservice managers and other key stakeholders to ensurenutrition,financial,psychosocial,choiceandqualitygoalsaremet.
1.2 A dietitian will be available to assess the food and menu as meeting these NSMM and the requirements (cultural, religious, age, psychosocial, nutritional status) of the population in the facility2.
1.3 The menu is reviewed by a dietitian biennially.2
1.4 Patients/residents/clients are able to access at a minimum, three main meals and three mid-meals each day.2
1.5 Serve size variations* are offered on the menu.
1.6 The facility will endeavour to accommodate cultural and religious food preferences within the restrictions and constraints of food suply issues.
Note: *Refertop47fordefinitionsonservesizes

Page 9
2.0 ADULT: ACUTE (EXCLUDING SHORT STAY PATIENTS)Aim: The food offered provides choice, variety and meets the nutritional needs of the majority of patients, including those with higher protein and energy requirements.
BACKGROUND/RATIONALE STANDARDS
Assessment of length of stay (LOS) at seven QH hospitals indicate that 60% – 75% of occupied bed days (OBD) are patients staying longer than seven days where these patients had an average LOS of 14.7 to 22.4 days (refer to Apendix 1 p 50). Reassessment of LOS at 2 sites in 2014 indicated that aproximately 70% of OBD are patients staying longer than seven days with an average LOS of 17 days.
The literature suports that cost savings, through reduced length of stay and complications, can be realised if nutritionally at risk patients or residents can beidentifiedandnutritionalsuportimplemented.20
Patients assessed with or at risk of malnutrition, or who are admitted for more than seven days in acute facilities, need access to extra food choices and higher energy/protein options at meals and mid-meals. This will increase the likelihood of meeting nutritional and psychosocial needs.
Studieswereidentifiedthatmeasuredtheeffectsofprovidingenergydensemeals and snacks to hospitalised patients21,22,23,24 and reported an increase in bothenergyandproteinintakewhenfortifiedfoodwasprovided.Onestudy23 lookedatfortificationoffoodandacookedbreakfastwhichresultedinthehighest increase in energy and protein intake.
2.1 Adult facilities shall have systems in place to identify patients who are at nutritional risk or are malnourished.
2.2 The standard menu shall provide a minimum choice across cycle length of 35 hot main meals with choices as outlined in Section 3 Minimum Menu (p 26 – 41).
2.3 The standard menu shall provide three main meals and three mid-meals each day. At least two mid meals are substantial i.e. group 1 or 2 (refer to Meal Component Table p 23).
2.4 Thestandardmenushallprovidefortifiedoptionsfor:
• hot cereal;• soup; and • one vegetable per day for all textures.
FortifiedfoodswillmeetthenutritiontargetsoutlinedinSection2 MealComponentSpecifications(p18–23).
2.5 The standard menu shall provide a hot protein breakfast choice for all texturelevels,includingregularunmodified(i.e.full)andTextureAsoft (refertoDefinition–BreakfastProteinp46andMealComponentTable p 22).
Page 10
3.0 ADULT: ACUTE (SHORT STAY PATIENTS)Aim: An additional menu may be provided for patients staying less than seven days. The menu offered shall meet average requirements for protein and energy for the patient group.
BACKGROUND/RATIONALE STANDARDS
Patients who are in hospital less than seven days are considered short stay. These individuals if not assessed as being at nutritional risk do not require extensive choice on the menu or high energy/high protein options at all mid-meals.
Nutrition screening will be carried out to identify those patients at risk and needing the long stay menu. (Refer to EQuIP National Standard 12.6.2)
Assessment of LOS at seven QH hospitals indicate that between 77% and 95% of patients admitted to these hospitals stay less than seven days (refer to Apendix 1 p 50 - 53 for detailed LOS data and analysis). Reassessment of LOS at 2 sites in 2014 indicated that aproximately 70% of OBD are patients staying longer than seven days with an average LOS of 17 days.
Ashortstaymenu(refertop47fordefinition)providesanoportunityto offset increased costs associated with the standard menu against a lower cost menu. In this instance the long stay menu is intended to be targeted to patients/residents that have the highest nutritional needs.
3.1 An alternative menu for short stay patients (LOS less than seven days) shall have minimum choices across the menu cycle as outlined in Table 1.0 Adult Acute Minimum Choice (p 27 − 30) to meet the average requirement for non-nutritionally compromised adults.

Page 11
4.0 MATERNITYAim: The food provided shall meet the majority of nutritional requirements of pregnant and breastfeeding women.
BACKGROUND/RATIONALE STANDARDS
During pregnancy there are increased nutritional requirements.12, 25, 26 Nutrients can generally be met with a normal healthy diet as provided by the standard menu. However elevated iron, iodine and folate requirements need consideration in menu planning. Dietary suplementation of iodine25, 26 and folate12 are required during pregnancy, and for iodine continued during breastfeeding.25, 26
Breastfeeding women have increased energy12andfluid12 requirements thus requireadditionalfoodchoicesandaccesstofluids.Sufficientchoiceshouldbeprovided to allow apropriate options for patients who are overweight, obese or have gestational diabetes.
Where dietary intake is compromised due to hyperemesis gravidarum or other complications, a therapeutic diet and/or nutritional suplement(s) may be required.
Pregnant women and their unborn child are considered at high risk of listeriosis. Current Food Standards Australia and New Zealand (FSANZ) recommendations outline pregnant women should take care with their food choices.27 Facility food safety programs should identify and mitigate listeria risks for maternity patients.
4.1 Pregnant and breastfeeding women shall be provided with the long stay menu (refer to Standard 2.0 Adult: Acute (excluding short stay patients p 9) in acute facilities to assist in meeting the increased energy, protein and micro-nutrient requirements.
4.2 Breastfeeding women shall be provided access to fresh water, additional snacksandotherfluids.
4.3 Breastfeeding women shall be provided with access to nutritional suplements (as assessed by a dietitian) if required.

Page 12
5.0 PAEDIATRICS Aim: The food provided shall offer a range of options that are age and developmentally apropriate.
BACKGROUND/RATIONALE STANDARDS
Nutrition Standards are designed to provide a guideline for menus for children over 12 months. Children under 12 months will have their nutritional needs met by a combination of food and breastmilk or formula28 and will need to be individually assessed or guided by the carer.
LOS data (2011) suports that 60% of bed days (OBDs) are children who stay less than seven days. However the 40% of children who stay longer than seven days have an average LOS of 16.9 days (refer to detailed LOS data in Apendix 1 p 51).
Adolescents in paediatric facilities or units will sometimes require larger servings or the adult acute standard menu.
ADietitianshouldreviewanytexturemodifiedfooditemsfromtheadultStanding Offer Arrangement (SOA) for suitability with respect to sodium content and other additives before use with children under 24 months.
5.1 Paediatric patients in an acute facility shall have access to a menu with 35 hot meal choices across the menu cycle and choices equivalent to those outlined in Table 2 Paediatric Minimum Menu Choice (p 35 – 37).
5.2 Choices shall be available for children requiring therapeutic diets eg.cysticfibrosis,gluten-free.
5.3 All paediatric menus shall be free of whole nuts and nut pastes where possible.
5.4 Choices shall be available for children with food allergies and intolerances.
5.5 Choices for suitable weaning foods with apropriate textures shall be available for infants weaning onto a solid food diet.
Page 13
6.0 RESIDENTIAL AGED CAREAim: The food offered and dining environment provides choice, variety and meets the nutritional and psychosocial needs of the residents, including those withhigherproteinandenergyrequirementsandthoserequiringtexturemodifiedmeals.
BACKGROUND/RATIONALE STANDARDS
Care and services in aged care homes: Information for aproved providers (2014)29, directs facilities to provide meals of adequate variety, quality and quantity in accordance with residents’ individual nutritional needs; 3 meals and 3 mid-meals a day; meals suitable for special dietary requirements having regard to either medical need or religious or cultural observance.
In ageing, energy (kilojoules) requirement is lowered but nutrient requirement is similar or higher than in the younger adult, necessitating the need for more nutrient dense foods.30, 31
Elderly persons are at risk of inadequate dietary intake therefore all residents should be assessed on admission and reviewed as necessary by a dietitian.29
Chewingandswallowingdifficultiesarecommoninthisgroup.Thereforemodificationtofoodtexturemayberequiredwhilestillprovidingnutritionallyadequate choices in apropriate serving sizes.
Residentswithdementiaandothersimilarconditionsbenefitfromfingerfoods.These options can facilitate increased oral intake, independence and self feeding (refertop46forfingerfooddefinition).32,33,34
Constipation and dehydration is a common issue in elderly persons for various reasons,thusencouragingapropriatefoodandfluidintakewillbebeneficial.
A study that measured the effects of providing energy dense meals and snacks to the institutionalised elderly31 reported an increase in both energy and proteinintakewhenfortifiedfoodwasprovided.Anotherstudy23 also looked atfortificationoffoodandacookedbreakfastwhichresultedinthehighestincrease in energy and protein intake.
6.1 Residents in aged care facilities shall receive a menu with a cycle of no less than 14 days and minimum choices across the menu cycle equivalent to those outlined in Table 3 Residential Aged Care Minimum Menu Choice (p 27 – 33).
6.2 Both hot and cold protein breakfast choices shall be offered to residents on full and soft textured diets each day.
6.3 A hot protein breakfast choice shall be offered to all residents on texture B minced and moist and texture C smooth pureed diets each day.
6.4 Finger food options shall be available when required for those residents whoareidentifiedasbenefitingfromthisoption.
6.5 Additionalfoodand/orfluidsuplementsshallbeavailableasrequired.
6.6 Thelongstaymenushallprovidefortifiedoptionsforhotcereal,soup andonevegetableperdayforfullandsofttextures.Fortifiedfoodswill meet the nutrition targets outlined in Section 2 Meal Component Specifications(p19–23).
6.7 Residents shall have the oportunity to have input into menu choices and menu reviews. If residents are unable to have input, family members can be consulted on preferred menu choices or for input into menu reviews.

Page 14
7.0 MENTAL HEALTH AND ACQUIRED BRAIN INJURY Aim: The food provided shall meet the psychosocial and physical health needs of consumers allowing nutritional requirements to be met and suporting healthy choices with a focus on chronic disease prevention and management.
BACKGROUND/RATIONALE STANDARDS
Mental health and acquired brain injury consumers represent a diverse patient population, whose longer length of stay is one important factor in determining their nutritional requirements. Individuals with severe mental illness experience double the rates of obesity compared to the general population and are atsignificantlyhigherriskofchronicdisease,including:cardiovasculardisease, type 2 diabetes and associated risk factors such as dyslipidaemia and hypertension.10, 11 These diet-related disorders are the primary cause of morbidity and mortality in this population who experience a 13 − 25 year shortened life expectancy.10
The menu is an important tool to manage and minimise risk of chronic disease. The Nutrition Standards for this population group are informed by the National Health and Medical Research Council’s Nutrient Reference Values12 which provide advice for reduction of chronic disease risk in the form of Suggested Dietary Targets(SDTs)fordietaryfibre,selectedmicronutrientsandfattyacids,andAcceptable Macronutrient Distribution Ranges (AMDRs) for percentage of energy from protein, fats and carbohydrates in addition to the more recent Australian Dietary Guidelines 2013.4
Toimprovefattyacidprofiletheinclusionofpolyunsaturatedspreadsshould be encouraged.
Individuals with mental illness and acquired brain injuries tend to experience increased apetite and/or decreased satiety as a side-effect of some medications.35Hence,fortifiedmealsaregenerallynotindicatedforthispopulationgroup.However,swallowingdifficultiesareprevalentinindividualswith acquired brain injuries36;therefore,atexturemodifiedmenu(includingtexturesA,BandC),withfortifiedoptions,willberequiredbysomeindividuals.
7.1 In mental health and acquired brain injury settings the menu shall consist of a minimum cycle length of 14 days with choices equivalent to those outlined in Table 4 Mental Health and Acquired Brain Injury Minimum Menu Choice (p 38 – 41).
7.2 Facilities shall have systems in place to identify consumers who are at nutritional risk of or are malnourished.
7.3 Where practicable options shall be available for consumers with food allergies and intolerances.
7.4 Healthy meal options (eg low fat, reduced salt) shall be available at all main meals and mid-meals and these options shall be promoted.
7.5 Themenushallaimtoprovideatleastonefishmealperweek.7
7.6 Unsaturated spreads shall be provided for use to consumers.
7.7 The menu shall aim to provide at least 25 –30gramsoffibreperday.12
7.8 Fresh drinking water shall be available at all times. The suply of chilled water is encouraged where practical.
7.9 Consumers shall be informed of menu choices prior to meal service. Copies of written menus are accessible to consumers.
7.10 Facilitiesaretohaveasevenday‘fingerfood’menuavailable.Thismenu shall align with dietary targets to ensure that nutritional requirements are met.Ifaconsumerrequires‘fingerfoods’forgreaterthansevendays, or on a frequent basis, a dietitian shall review to ensure adequate variety.

Page 15
7.0 Mental Health and Acquired Brain Injury (Continued)
BACKGROUND/RATIONALE STANDARDS
Constipation is prevalent within both patient groups37; therefore, the menu shouldpromoteadequateandconsistentfibreandfluidintake.
Variety and choice to prevent menu fatigue is important to increase satisfaction with the food provided and to prevent excessive food consumption from nutritionally poor sources outside the menu.
The style of meal service allows patients to choose meals and mid-meals, ideally at point of service.
7.11 Consumers shall have the oportunity to have input into menu choices and menu reviews.
7.12 For consumers who are unable to communicate menu preferences, ensure variety in meal choices, record likes/dislikes and/or consult with family and/or friends to ensure individual needs are met.
Note: Patients with an acute ABI to be offered options as per acute adults standard menu (p 9).

Page 16
8.0 VEGETARIAN AND VEGANAim: The food offered shall provide patients choosing to follow a vegetarian or vegan diet ability to meet the majority of their nutritional requirements.
BACKGROUND/RATIONALE STANDARDS
Patients following a vegetarian or vegan diet may do so due to choice, cultural or religious reasons.
Vegetarian diets can be healthy when carefully planned and monitored. Adequate variety of suitable nutritious foods are required to meet individual patient or resident needs.
Protein quality of meals needs to be balanced to include all amino acids over the day which requires careful planning and inclusion of legumes, nuts, seeds and cereals across the three meals.
Studieshaveidentifiedthefollowingnutrientsatrisk:
Protein4,39, Iron 4,12,39,40,41, Zinc12,39,40,41, Iodine39,42, B124,12,39,40,41, Calcium12, 39,40,41, Vitamin D.39,40,41
Suplementation with at risk nutrients may be needed to meet nutritional requirements where patients are longer stay.
8.1 At least two vegetarian/ (including one vegan) options shall be available to choose each day (these can include hot meals, salads and sandwiches) but a minimum of at least one hot vegetarian/vegan choice shall be offered every other day. Depending on frequency of the requirement for vegetarian/vegan options in the facility, these options may or may not apear on the menu the patient receives but do need to be included on the master menu so that apropriate options will be available if required.
8.2 Acute adult and paediatric facilities shall where practical integrate vegetarian choices into the standard menu.
8.3 A variety of protein sources shall be available to vegetarian and vegan patients including cheese, egg, legumes, tofu, nuts, seeds and textured vegetable protein products (with the exception of nuts in paediatric wardsorfacilities).Milkalternatives(eg.soymilk)shallbefortifiedwith calcium and B12 and contain an equivalent level of protein to cows milk.

Page 17
9.0 THERAPEUTIC AND MEDICAL DIETSAim: Patientsidentifiedasrequiringtherapeuticdietsshallhavefoodprovidedthatmeetsthisneed,withtheaimofalsoachievingoverallnutritional requirements and psychosocial needs.
BACKGROUND/RATIONALE STANDARDS
Patients with multiple diet requirements will exist within QH facilities. Every facility should have a process of identifying patients with therapeutic dietary needs.
Integratingtherapeuticdietscreatesefficienciesforfoodservicesthereforeamajority(~90%) of these diets should be integrated into the standard menu with minimum impactontheoverallnutritionalprofileofthemenu.However,notalltherapeuticdiets can be successfully integrated. Special foods may need to be obtained to meet this therapeutic requirement; however, it is expected that no more than 10% of diets require special foods (SFSKPI). Integration of therapeutic diets should not compromise the quality and taste/acceptability of the overall menu for the majority of patients (eg. low salt, reduced fat).
Examples of diets suitable to be integrated into a main menu include:
• TextureAsoft,highfibre,lowfibre,proteinrestricted,fatmodified (eg.suitableforpeopleoncardiovasculardiets),carbohydratemodified (for example, suitable for patients with diabetes) and low lactose.
• Somedietsthatmaybedifficulttointegrateinclude:verylowfat, glutenfree,electrolytemodified(eg.lowsodium,lowpotassium),allergy, milk free or metabolic (eg. ketogenic) diets.
• Texturemodifieddiets(TextureBmincedandmoistandTextureCsmooth puree) should follow the menu choice on the main menu as closely as possible.
Not all therapeutic diets can meet individual nutrition requirements, and a dietitian should determine the adequacy and make recommendations to meet individual patients/residents need.
Some therapeutic diets are short term and are not expected to meet nutritional requirements,examplesincludeclearfluiddiets,investigativediets.
Whilst every effort should be made to maximise choice for the patients requiring therapeutic diets, this may be difficult to achieve.
9.1 Every facility shall have a process of identifying patients with therapeutic dietary need before a meal is served to the patient.
9.2 Common therapeutic diets used in a facility shall be integrated into the standard menu without unnecessary restrictions.
9.3 There is a process to record and modify menus to accommodate patient likes and dislikes (where possible) when long stay patients are placed on a therapeutic and/or medical diet with reduced choice.
9.4 A dietitian shall determine the adequacy of any therapeutic diets for individual patients/residents that are not available on the main menu.
9.5 TexturemodifieddietsshallcomplywiththeAustralian Standardised DefinitionsandTerminologyforTextureModifiedFoodandFluids.43 Additional textures may be provided where dietitians and speech pathologists can provide evidence that textures in the Standards arenotsufficienttomeettheneedsofthepatients/residents/clients.
9.6 Fluid containing foods of the correct texture shall be available at all meals and mid meals to patients/clients/residents requiring thickened fluidstomaximisefluidintakes.
9.7 Allpatientsontexturemodifieddietsshallreceivefortifiedfoodoptions and substantial mid-meal options of suitable texture.

SECTION 2MEAL COMPONENT SPECIFICATIONSNutrition Standards for Meals and Menus

Page 19
NUTRITION STANDARDS MEAL COMPONENT SPECIFICATIONSThesespecificationswereadaptedfromtheVictorianNutritionStandardsforMenu Items.5Somenutrienttargetshavebeenmodified,removedorrelaxedtoensurepatient,resident,consumerandclientneedsaremetwithaspecificfocus on protein and energy requirements.
Each category of meal is divided into groups based on the nutritional value of the meal. These can be used for assessing pre-made products or for recipe analysis when preparing and cooking meals. The User Guide on pages 42–47, and the menu outlines on pages 57-63, explains how these can be used in menu design.

Page 20
MAIN (PROTEIN) DISHES (HOT)• Meat to be trimmed of excess fat, skin and unnecessary bone.
• Products should contain minimal amounts of added sodium but enough to achieve a tasty product. Note that a selection of dishes with less than 10mmol (230mg) sodium/serve will be required.
• Added fat to be poly or mono unsaturated. Note that a selection of dishes with less than 15g of total fat/serve will be required.
• The nutritional analysis for this category should not include potato, rice and pasta unless it is an ingredient in the dish itself eg. lasagne and is analysed asweightoffinalcookedproduct.
GROUP 1 GROUP 2 GROUP 3 GROUP 4^
Description Predominantly cuts of meat such asroasts,grillsandfish(i.e.100%meat content)
The meat component must not weigh less than 100g per serve*
High meat content dishes (i.e. 75% meat content).
The meat content must not weigh less than 100g per serve*
(ovenable crumbing and batter accepted in this category)
Product is even mix of meat/meat alternative and vegetables/ -rice/-pasta (i.e. 50% meat/meat alternative content)
Dishes have a varying protein and fat content
Example Dishes Roast Beef
Grilled Fish
Beef rissoles and gravy
Chicken Chasseur
Spaghetti Bolognaise
Chicken Stir-fry
Singapore noodles
Pumpkin Risotto
Serve Size# Dry, greater or equal to 100g 130g – 160g 150g – 180g Greater or equal to 150g
Energy Greater or equal to 550kJ per serve Greater or equal to 700kJ per serve Greater or equal to 700kJ per serve No target set
Protein Greater or equal to 20g per serve Greater or equal to 15g per serve Greater or equal to 10g per serve Greater or equal to 7g per serve
# The maximum serve size for Texture C Smooth Pureed is 120g (for pasta and potato based dishes 180g).* Texture C – Smooth Pureed dishes are permitted to contain less than 100g of meat per serve.^ = Group 4 is not intended to be a frequent menu item and is only included for variety.

Page 21
SOUPS
GROUP 1 GROUP 2
Description Provides significant protein and energyMay have vitamins and minerals added
Provides moderate protein and energy
Serve Size 120 – 200ml 160 – 200ml
Energy Greater or equal to 600kJ per serve Greater or equal to 400kJ per serve
Protein Greater or equal to 8g protein per serve Greater or equal to 5g protein per serve
Note: Fortification of Soups –addskim/fullcreammilkpowderorreplacewaterwithmilk,cream,cheese,pureedlentils/legumesoryoghurt.Group1andGroup2soupsareconsideredfortifiedsoups.
SANDWICHES
GROUP 1 GROUP 2
Description Provides significant protein and energy Provides moderate protein and energy
Example dishes Ham and cheese sandwich (1 x 30g slice ham and 1 x 20g slice cheese)Salmon and cream cheese sandwich (40g tinned salmon and 1 tbsp cream cheese)
Ham and tomato sandwich (1 x 30g slice ham)Egg and lettuce sandwich (1 x 50g egg)
Serve Size 2 slices bread (4 points) 2 slices bread (4 points)
Energy Greater or equal to 1,250kJ per serve Greater or equal to 1,000kJ per serve
Protein Greater or equal to 15g protein per serve Greater or equal to 8g protein per serve
Page 22
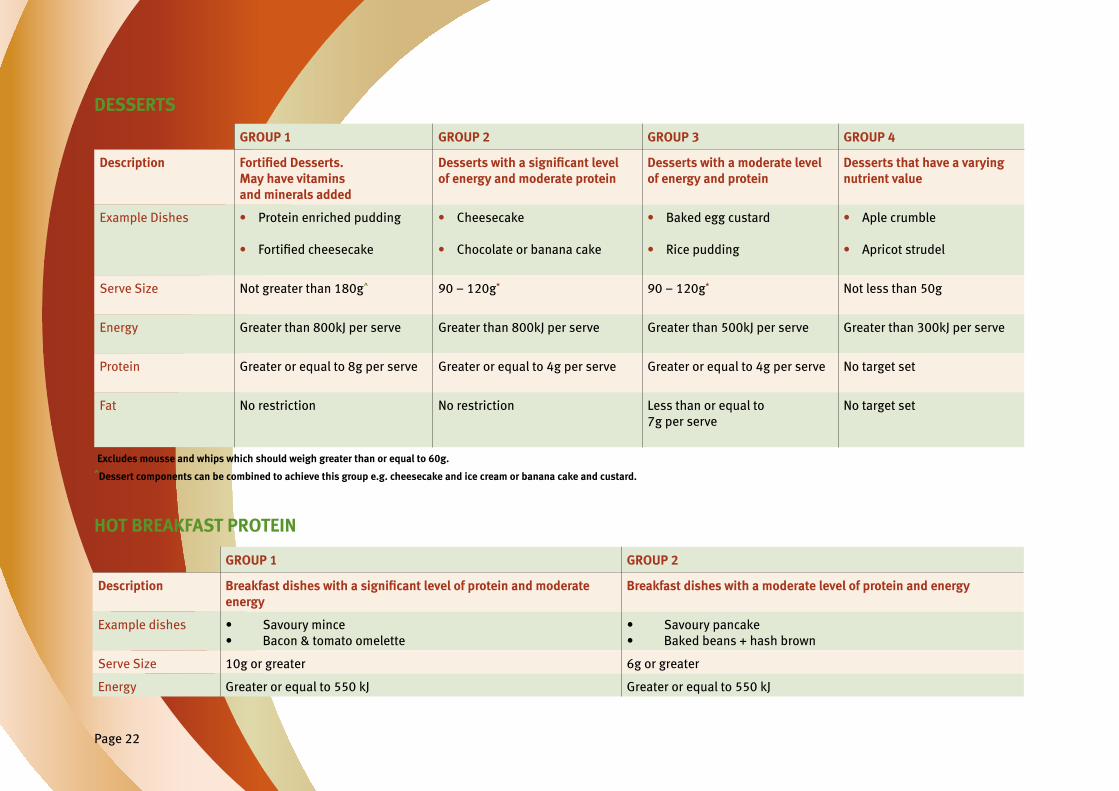
DESSERTS
GROUP 1 GROUP 2 GROUP 3 GROUP 4
Description Fortified Desserts. May have vitamins and minerals added
Desserts with a significant level of energy and moderate protein
Desserts with a moderate level of energy and protein
Desserts that have a varying nutrient value
Example Dishes • Protein enriched pudding
• Fortifiedcheesecake
• Cheesecake
• Chocolate or banana cake
• Baked egg custard
• Rice pudding
• Aple crumble
• Apricot strudel
Serve Size Not greater than 180g^ 90 – 120g* 90 – 120g* Not less than 50g
Energy Greater than 800kJ per serve Greater than 800kJ per serve Greater than 500kJ per serve Greater than 300kJ per serve
Protein Greater or equal to 8g per serve Greater or equal to 4g per serve Greater or equal to 4g per serve No target set
Fat No restriction No restriction Less than or equal to 7g per serve
No target set
*Excludes mousse and whips which should weigh greater than or equal to 60g.^Dessert components can be combined to achieve this group e.g. cheesecake and ice cream or banana cake and custard.
GROUP 1 GROUP 2
Description Breakfast dishes with a significant level of protein and moderate energy
Breakfast dishes with a moderate level of protein and energy
Example dishes • Savoury mince• Bacon & tomato omelette
• Savoury pancake• Baked beans + hash brown
Serve Size 10g or greater 6g or greater
Energy Greater or equal to 550 kJ Greater or equal to 550 kJ
HOT BREAKFAST PROTEIN

Page 23
SNACK/MID-MEALS
GROUP 1 GROUP 2 GROUP 3 GROUP 4
Description High protein, high energy snack Mod protein, high energy snack Low protein, high energy snack
Healthy snack (low fat, no added sugar, high fibre)
Examples • Cheese and crackers• Cheese scone• Sandwich one slice bread (two points) with a proteinfilling• Nuts (not paediatrics)• Yoghurt• Custards
• Cake• Breakfast bar• Muffin• Sandwich one slice bread (two points) with a non-proteinfilling• Dairy dessert (eg. fromage frais, crème brulee)• Mousse
• Chocolate• Potato crisps• Extruded snacks• Dried fruit• Sweet biscuits (2 – 3)• Savoury biscuits (2 – 4)
• Sandwich one slice high fibrebread(twopoints) with a low fat proteinfilling• Nuts (no added salt or fat)• Low fat yoghurt• Low fat cheese and crackers• Fresh fruit or no added sugar tinned fruit
Energy Greater than 500kJ Greater than 500kJ Greater than 500kJ Less than 800kJ
Protein 5g or greater 2g or greater No target set No target set
FORTIFICATION OF MENU ITEMS(Seep46fordefinition)
Toprovideadditionalnutrition,fortificationofcertainmealcomponentsincludinghotcerealsandvegetablesisrequired. Fortificationaimstoincreasetheproteinand/orenergydensityofthemealcomponent.
Description Hot cereal Starchy vegetables Other vegetables
Energy Greater than 550 kJ Greater than 400kJ Greater than 300kJ
Protein 10g or greater 3g or greater 3g or greater
Type of fortification Skim/full cream milk powder, cream, evaporated milk, protein/energy suplement.
Add cheese; a dairy based sauce (eg béchamel, hollandaise); butter, margarine or milk, yoghurtorcreamtosteamedvegetables.Includespotatobake,cauliflowerorbroccoliin cheese sauce, potato wedges with sour cream, potato mashed with butter and added skim milk powder

Page 24
PORTION SIZES FOR MEAL ITEMS
Thefollowingtableidentifiesportionsizesforindividualmealitemsthatarenotincludedinthemealcomponentgroupspecificationsonpages20–23. Variations to serve sizes may occur for therapeutic/medical diets or on a dietitian’s request.
MENU ITEM PORTION SIZE
Fruit juice (100% juice) 100 – 120ml
Hot cereal (porridge, semolina, high protein wheat germ cereal) 150 – 180g
Ready to eat cold cereal Not less than 20g
Milk for cereal Not less than 100ml
Bread/roll 1 slice or equivalent
Yoghurt 100g as snack or dessert component Note: not less than 150g if served as a sole dessert item
Cheese Not less than 15g
Butter or margarine Not less than 7g
Starchy vegetable/rice/pasta 90 – 120g
Non-starchy vegetable 60 – 80g
Fruit, canned and drained Not less than 80g
Fruit, fresh 1 piece or equivalent (100g)
Jelly Not less than 120g
Ice Cream Not less than 50g
Tea, coffee, cordial or milk based drinks 150 – 200ml

SECTION 3MINIMUM MENU CHOICENutrition Standards for Meals and Menus

Page 26
HOW TO USE THE MINIMUM MENU CHOICE TABLESThere are several patient categories covered in this section including
• Adult acute and Residential aged care– short stay and long stay apear in the same table but in separate columns.
• Paediatric
• TextureModified–acute,MentalHealthandAcquiredBrainInjury
• Mental Health and Acquired Brain Injury
For each of the patient categories in this section there are tables for
• Breakfast
• Lunch and Dinner combined
• Mid-meals
Tables within this section outline:
• The minimum number of choices available to be offered including
− Minimum menu choice required per day:
> eg. the standard acute menu requires a minimum of two hot main meals a day (could be served at lunch or dinner or both)
> eg. the short stay acute menu requires a minimum of one hot main meal a day (could be served at lunch or dinner)
− Minimum menu choice required across the menu cycle:
> eg. the standard acute menu requires a minimum of 35 hot meal choices per cycle, with at least 14 being full choices and 21 being soft choices
> eg. the short stay acute menu requires a minimum of 14 hot meal choices per cycle, with at least 7 being full choices and 5 being soft choices
− Minimum menu choices required across the meal groups:
> eg. the standard acute menu recommends that one of the two hot main meals should be a group 1 or 2 meal and a second choice can be a group 1, 2 or 3 meal refer to p 20.
> eg. the short stay acute menu recommends that the main hot protein can be from either group 1, 2 or 3 p 20.

Page 27
Table 1: Adult Acute and Residential Aged Care – Minimum Choice
BREAKFASTSHORT STAY MENU STANDARD MENU LONG STAY MENU EXAMPLES
Per day Per cycle Per day Per cycle Today’s choice Choices across the cycle
Cold cereal –lowfibre 1 2 1 2 Puffed Rice Puffed Rice , Corn flakes
Cold cereal –highfibre 1 2 2 3 MuesliWheat Biscuit
Muesli, Wheat Biscuit, Sultana &
Bran Flakes
Hot cereal 0 0 1 1 Porridge Porridge
Cold protein 1 1 1 2 Yoghurt Yoghurt, Banana Smoothie
Hot protein 0 0 1 At least 3 Grp 1Total 6 choices
Baked beans + hash brown
Baked beans + hash brown, scrambled
egg, cheese & bacon omelette, Chipolatas
+ baked beans, Poached eggs +
tomato, Pancakes + syrup
Bread/toast/rolllowfibre
1 1 1 1 White bread White bread
Bread/toast/rollhighfibre
1 1 2 2 Wholemeal bread Fruit bread
Wholemeal bread, fruit bread
Fresh fruit 1 3 1 3 Banana Banana, mandarin/pears, aple
Tinned fruit and/or juice 1 (juice or fruit) 2 1 juice1 fruit
2 juice4 fruit
Orange juice and/or peaches
Orange juice, aple juice and/or peaches,
prunes
Milk Full and low fat Cereal and drink Full and low fat On cereal and in drink
Full fat, 2% fat Full fat, 2% fat
KEY:Minced = Texture B minced and moist NAS = No Added SugarPureed = Texture C smooth pureed Veg = VegetableMod thick = Level 400 moderately thick Alt = Alternate

Page 28
Table 1: Adult Acute and Residential Aged Care– Minimum Choice (continued)
MAIN MEALlunch and dinner
SHORT STAY MENU STANDARD MENU SUGGESTED MENU EXAMPLES
Per day Per cycle Per day Per cycle Today’s choice Choice across the cycle
Soup (powder base)
1 7 0 0 0 0
Soup Groups 1 and 2
0 0 1 x group 1 or group 2
4 x group 1 7 x group 2
Pea & Ham soup Grp 1 – pea & ham, beef & vege, lentil,
minestroneGrp 2 – Chicken & corn, Creamy
pumpkin, Tomato & bacon, Potato & leek
Main hot protein* Groups 1, 2, 3 and 4
1 x group 1, 2 or 3 14 minimum* (at least 7 soft)
(at least 1 vegetarian choice
every 2nd day)
1 x group 1 or 2
2nd choice* 1 x group 1, 2 or 3
35 minimum 14 x full
21 x soft# 7 x full or soft
(at least 1 vegetarian choice
every 2nd day)
Roast Beef
Chickpea curry
P 57 - 61
Starchy vegetable**** or alternative (eg. rice/pasta/cous cous)
1 2 1 4 starchy veg** 2 alternatives
(as starchy choice)
Roast potato Mashed sweet potato, roast potato, Corn, Mashed potatoRice, noodles, pasta,
cous cous
Fortifiedvegetable**** 0 0 1 3 Caulifloweraugratin Caulifloweraugrain,Potato Bake, Mashed potato (butter & milk)
Orange vegetable**** 1 3 2 3 Mashed pumpkinCarrot
Mashed sweet potato, carrot,
mashed or roast pumpkin
Green/brassica vegetable**** 1 4 2 5 CaulifloweraugratinBeans
Caulifloweraugratin,beans, brussel sprouts, peas,
broccoli
Note: * group4hotproteinmainmealchoicesareonlyforvarietythereforenospecifiedusage.Needatleastonevegetarianhotoptioneverysecondday.SeeStd.8.1p16 # some of the soft choices available on the menu can also be minced choices and included in both choice lists ** including potato prepared different ways i.e. mashed potato, roast potato
**** onefortifiedvegetableoptionneedstobeavailableeachdaywhereavarietyoffortifiedoptionsshouldbeofferedseeStandard2.4(p9)andpage23forfortificationoptions

Page 29
Table 1: Adult Acute and Residential Aged Care– Minimum Choice (continued)
MAIN MEALlunch and dinner
SHORT STAY MENU STANDARD MENU SUGGESTED MENU EXAMPLES
Per day Per cycle Per day Per cycle Today’s choice Choice across the cycle
Side Salad Minimum 4 vegetables
1 1 1 1 Lunch: Lettuce, tomato, carrot sticks, cucumber
0
Main Salad 1 x 100g meat or meat alternative 1 x carbohydrate serve 2 x core vegetables* 2 x rotating vegetable**
1 7 x meat or meat alternative
4 x carbohydrate
4 x rotating vegetable
1 10 x meat or meat alternative
4 x carbohydrate 4 x rotating vegetable
Dinner: Corn beefRice salad
Lettuce & tomatoCucumber & beetroot
See menu P 57 - 61 for meat/alternative choicesRice Salad, Potato salad,
Pineaple, CornLettuce & tomato
Cucumber, beetroot, capsicum, carrot
Sandwich/Wrap/Roll Groups 1 and 2
1 x group 1 0 x group 2
7 x group 1 4 x group 2
1 x group 1 1 x group 2
7 x group 1 7 x group 2
Lunch: Ham & cheeseDinner: Chicken & cranberry
See menu P 57 – 61 for choices
Dessert Groups 1, 2, 3 and 4 Tinned fruit and dairy
1 x group 3 or 4
1 x tinned fruit
and dairy
7 x group 3 or 4
4 x tinned fruit
and dairy
1 x group 1 or 2 2nd choice
1 x group 1, 2, 3 or 4 or tinned fruit
and dairy
6 x group 1 6 x group 2 5 x group 3 5 x group 4
6 x tinned fruit and dairy
Lunch:Apricots & custard
Dinner:Lemon cheesecake
& ice cream
See menu P 57 – 61 for choices
Fruit – fresh 2 (1 soft fruit)
3 2 (1 soft fruit)
3 Lunch: ApleDinner: Fruit in season
Aple, banana, fruit in season
Bread/roll –lowfibre 2 2 2 2 Lunch: White breadDinner: White roll
White Bread, white breadroll
Bread/roll –highfibre 2 2 2 2 Lunch: w/meal breadDinner: w/meal roll
Wholemeal bread, wholemeal breadroll
* core salad vegetables stay the same each day. Eg: lettuce and tomato see p 46
** rotating salad vegetables would change from day to day to add variety Note: There is a requirement for 2 vegetarian/vegan options each day which can be hot meals, salad and sandwiches See Std 8.1 p 16.

Page 30
Table 1: Adult Acute and Residential Aged Care– Minimum Choice (continued)
MID MEALSMorning Tea, Afternoon Tea and Super
SHORT STAY MENU LONG STAY MENU SUGGESTED MENU EXAMPLES
Per day Per cycle Per day Per cycle Today’s Choice Choice across the cycle
Snack
Groups 1, 2, 3 and 4
1 x group 1 or 2
2 x other (notspecified)
4 x group 12 x group 2
1 x group 1 or 22nd choice
1 x group 1, 2 or 3
4 x group 14 x group 22 x group 3
Cheese & biscuits
Fruit cake
Grp 1: Cheese & biscuits, fruit yoghurt, nuts, ½ cheese sandwichGrp 2: Fruit cake, muffin,Breakfastbar,½ vegemite sandwichGrp 3: Potato crisps, 2 x cream biscuits
High protein/energy suplement*
0 0 1 3 Chocolate milk Chocolate milk, Fortifiedfruit
juice suplement, high protein milk
suplement
Drinks Tea, coffee, water, cordial, milk drink Tea, coffee, water, cordial, milk drink tea, coffee, cordial, milk drink, water
Note: *Highprotein/highenergysuplementcanincludecommercialsuplementsorfortifiedmilkdrinks

Page 31
Table 2: Texture Modified Menus Acute, Residential Aged Care, Mental Health & Acquired Brain Injury - Minimum Choice
BREAKFAST Texture Modified menu Suggested Menu Examples
Per day Per cycle Today’s choice Choice across the cycle
Coldcereal–lowfibre 1 minced0 pureed
2 minced0 pureed
Puffed rice Puffedrice,cornflakes
Coldcereal–highfibre 1 minced0 pureed
2 minced0 pureed
Wheatflakebiscuits Wheatflakebiscuits,Puffed brown rice
Hot cereal 1 minced1 pureed
1 minced1 pureed
PorridgePuree Porridge
Cold protein 1 minced1 pureed
2 minced2 pureed
Smooth Yoghurt Smooth Yoghurt
Smooth Yoghurt, banana smoothieSmooth yoghurt, banana smoothie
Hot protein 1 minced1 pureed
3 minced3 pureed
Savoury mincePuree savoury mince
See menu P 62 – 63 for choices across cycle
Bread/toast/roll–lowfibre 0 0
Bread/toast/roll–highfibre 0 0
Fresh fruit 1 minced (offer once/week)0 pureed
1 minced0 pureed
Mashed banana Mashed banana, mashed paw paw
Tinned fruit/juice 1 juice1 fruit x minced*1fruitxpureed
3 juice6 minced*6 pureed
Orange juice Orange juice, aple juice, prune juiceMinced or puree diced peaches + pears, peaches, pears
Milk Full fat On cereal & in drinks Full fat milk Full fat milkNote: *if on minced diet, pureed options can be substituted
Key: minced = Texture B minced and moist NAS = No Added Sugar pureed = Texture C smooth pureed veg = vegetable mod thick = Level 400 moderately thick alt = alternate

Page 32
Table 2: Texture Modified Menus Acute, Residential Aged Care, Mental Health & Acquired Brain Injury – Minimum Choice (continued)
1 pureed *
MAIN MEALlunch and dinner
Long stay menu Suggested Menu Examples
Per day Per cycle Todays Choice Choice across the cycle
Soup# Groups 1 and 2
1 x group 1 #1 x group 2 or powder
based#
5 x group 14 x group 2
Puree Pea & ham Grp 1: pea & ham, beef & vege, lentil, minestrone, chicken & vege
Grp 2: Chicken & corn, Creamy pumpkin, Tomato & bacon, Potato & leek
Main hot protein* Groups 1, 2, 3 and 4##
1 x group 1 or 2-minced1xgroup1or2-pureed
2nd choice* 1 x group 1, 2, 3 or 4
28 minced
28 pureed
Minced roast beef & gravyMinced chick pea curry
Puree roast beef & gravyPuree chick pea curry
See menus on P 62 - 63 to see choice across menus
Starchy vegetable*** or alternative**
1 minced*1 pureed
3 minced*3 pureed
Mashed potatoPuree potato
Mashed/puree sweet potato, mashed/puree potato Mashed/puree pasta
Fortifiedvegetable*** 1 minced*1 pureed
3 minced*3 pureed
Mashed or pureecauliflowerau gratin
Mashed/pureeCaulifloweraugrain,Potato Bake, Mashed potato
(butter & milk)
Orange vegetable*** 2 minced*2 pureed
3 minced*3 pureed
Mashed pumpkin, mashed carrot
Puree pumpkin, puree carrot
Mashed or puree sweet potato, carrots, pumpkin
Green/Brassica vegetable*** 2 minced*2 pureed
5 minced*5 pureed
Mashed or puree Caulifloweraugratin,
Mashed or puree beans
Mashed/pureeCaulifloweraugratin,peas, beans, broccoli, brussel sprouts
*if on minced diet, pureed options can be substituted**starchy vegetable alternative includes pasta, rice, noodles***onefortifiedvegetableoptionneedstobeavailableeachdaywhereavarietyoffortifiedoptionsshouldbeofferedseeStandard6.6andP23 forfortificationoptions# soup texture moderate thick puree##group4hotproteinmainmealchoicesareonlyforvarietythereforenospecifiedusage
NOTE:

Page 33
Per day Per cycle Todays Choice Choice across the cycle
Dessert Groups 1, 2, 3 and 4 Tinned fruit and dairy
1 x group 1 or 2 for both minced***and pureed
2nd choice1 x group 1,2, 3 or 4
minced***and pureedor pureed*** fruit & dairy
3 x group 1- 6 x group 2
6 x group 3&47 pureed tinned
fruit & dairy (2 minced*)
Lunch Mashed Apricots & custard Puree apricots & custard
Dinner Lemon Cheesecake & ice cream*
Lemon cheesecake (without base) & ice cream*
See menus on p 62 – 63to see choice across menus
Fresh fruit 1 minced (once per week)0 pureed
1 minced0 pureed
Mashed banana
*Icecreamnotallowedonthickenedfluiddiets.
Table 2: Texture Modified Menus Acute, Residential Aged Care, Mental Health & Acquired Brain Injury – Minimum Choice (continued)
MID MEALS Morning Tea, Afternoon Tea and Super
Long stay menu Texture Modified menu
Per day Per cycle Per day Per cycle
SnackGroups 1, 2, 3 and 4
2 x group 1 or 2 minced**
2xgroup1or2pureed
**4 x group 1 for both minced and pureed
**4 x group 2 for both minced and pureed
Smooth yoghurt, mashed fruit. Soft cake with custardSmooth yoghurt
& puree fruitChocolate mousse
Grp 1 - Smooth yoghurt + mashed fruit, Fruit smoothie, High protein custard + mashed fruit,
Cheese spread & vege rouladeGrp 2 Soft cake with custard, Chocolate mousse, soft
savourymuffinwithsmoothchutneyGrp 1- Smooth yoghurt & puree fruit, Fruit smoothie,
Cheese spread & vegie roulade, High protein chocolate custard
Grp 2 - Chocolate mousse, Puree cake & custard, pureesavourymuffin&chutney
High protein/energy suplement 1 3 (desirable to have multipleflavoursofthesuplements available)
HP milk suplement
HP Milk suplement, HP fruit suplement, HP pudding suplement
Drinks Tea, coffee, water, cordial, milk drink Tea, coffee, water, cordial, milk drink
Tea, coffee, water, cordial, milk drink
Table 2: Texture Modified Menus Acute, Residential Aged Care, Mental Health & Acquired Brain Injury – Minimum Choice (continued)
Note: ** Please note that some of the snack choices for the minced & moist texture can be the same as those provided for smooth pureed texture.
***Hydrationisimportantinthisgroupensuretooffervarietyofapropriatetexturedfluidsareofferedie.thickenedtea,coffee,cordial,milk, water and includes dairy desserts not just liquids.
Page 34
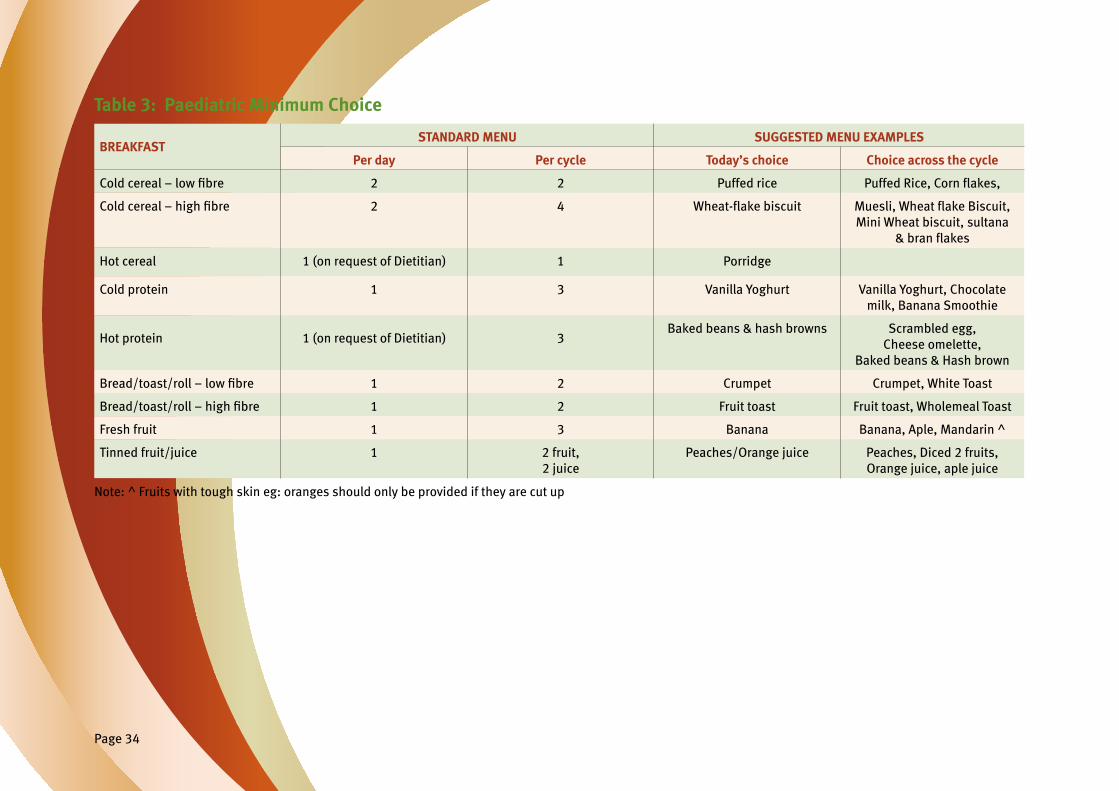
Table 3: Paediatric Minimum Choice
BREAKFASTSTANDARD MENU SUGGESTED MENU EXAMPLES
Per day Per cycle Today’s choice Choice across the cycle
Coldcereal–lowfibre 2 2 Puffed rice PuffedRice,Cornflakes,
Coldcereal–highfibre 2 4 Wheat-flakebiscuit Muesli,WheatflakeBiscuit,Mini Wheat biscuit, sultana
&branflakes
Hot cereal 1 (on request of Dietitian) 1 Porridge
Cold protein 1 3 Vanilla Yoghurt Vanilla Yoghurt, Chocolate milk, Banana Smoothie
Hot protein 1 (on request of Dietitian) 3Baked beans & hash browns Scrambled egg,
Cheese omelette,Baked beans & Hash brown
Bread/toast/roll–lowfibre 1 2 Crumpet Crumpet, White Toast
Bread/toast/roll–highfibre 1 2 Fruit toast Fruit toast, Wholemeal Toast
Fresh fruit 1 3 Banana Banana, Aple, Mandarin ^
Tinned fruit/juice 1 2 fruit, 2 juice
Peaches/Orange juice Peaches, Diced 2 fruits, Orange juice, aple juice
Note: ^ Fruits with tough skin eg: oranges should only be provided if they are cut up

Page 35
Table 3 Paediatric Minimum Choice (continued) MAIN MEALlunch and dinner
STANDARD MENU SUGGESTED MENU EXAMPLES
Per day Per cycle Today’s choice Choice across the cycle
Main hot protein*# Groups 1, 2, 3 and 4
1x group 1 or 2 2nd choice*
1 x group 1, 2, 3 or 4
35 minimum 14 x full
21 x soft#
Roast BeefChickpea curry
See menus on p 57 – 61 to see choice across menus
Starchy vegetable or alternative 1
4 starchy veg**2 alternate (as starchy choice)
Potato Chips
Roast potato Mashed sweet potato, roast potato, Corn, Mashed potato,
Chips, Rice, noodles
Orange vegetable 2 3 Mashed pumpkin Mashed sweet potato, carrot, mashed or roast pumpkin
Green/Brassica vegetable 2 5 Caulifloweraugratin Caulifloweraugratin,beans,peas, broccoli, steamed
cauliflower
Main Salad100g meat/meat alternative1 x CHO serve2 core vegetables 2 rotating vegetable
As requested 7 x meat or meat alternatives4 x CHO
4 x rotating vegetable
Chicken tendersRice salad
Lettuce, tomatoBeetroot, Celery
See menu P 57 – 61 for meat/alternative choices
Rice Salad, Potato salad, Pineaple, Corn, Lettuce & tomato, Celery, beetroot,
capsicum, carrot
Salad – small50g meat/meat alternative & minimum 4 vegetables
As requested 7 meat or meat alternatives ChickenfingersCarrot sticks, celery sticks,
tomato pieces,Capsicum sticks
See menu P 57 – 61 for Carrot sticks, Celery sticks, Capsicum
sticks, tomato pieces
Note: #provided/available in half serves *group4hotproteinmainmealchoicesareonlyforvarietythereforenospecifiedusage. ^ fruits with tough skins eg. Oranges, should only be provided if they are cut up. Need at least one vegetarian/vegan hot option every second day. See Std. 8.2 p 16

Page 36
Table 3: Paediatric Minimum Choice (continued)
MAIN MEALlunch and dinner
STANDARD MENU SUGGESTED MENU EXAMPLES
Per day Per cycle Today’s choice Choice across the cycle
Sandwich/Wrap/Roll Groups 1 and 2
1 x group 1 1 x group 2
5 x group 1 4 x group 2
Ham & cheese wrapEgg & lettuce swich
See menus on p 57- 61 to see choice across menus
Hotfingerfoods 1 (on request of dietitian) 5 Vege Spring Rolls Vege spring rolls, Chicken nuggets, Mini meatpies,FalafelBalls,Fishfingers
Dessert # Groups 1, 2, 3 and 4 Fruit and dairy dessert
1 x group 1 or 21 x group 3, 4 or dairy & fruit dessert
3 x group 1 or 27 x group 3, 4 or dairy &
fruit dessert
LunchApricots & custard
DinnerLemon cheesecake &
ice cream
See menus on p 57 - 61 to see choice across menus
Fruit − fresh 2 3 Banana, fruit in season Banana, aple, fruit in season (not orange unless cut up) ^
Bread/roll −lowfibre 2 2 White bread/roll
Bread/roll −highfibre 2 2 Wmeal bread/roll
Note: #provided/available in half serves *group4hotproteinmainmealchoicesareonlyforvarietythereforenospecifiedusage. ^ fruits with tough skins eg. Oranges, should only be provided if they are cut up. Need at least one vegetarian/vegan hot option every second day. See Std. 8.2 p 16

Page 37
Table 3: Paediatric Minimum Choice (cont)
MID MEALSMorning Tea, Afternoon Tea and Super
SUGGESTED MENU EXAMPLES
Per day Per cycle Today’s choice Choice across the cycle
Snack Groups 1, 2, 3 and 4
3 x group 1 2 x group 2 2 x group 3
(on request of dietitian)
6 x group 14 x group 24 x group 3
Grp 1- Cheese & biscuits, Yoghurt, 2x ¼ s ham swichGrp 2 – Sponge cake, chocolate mousseGrp 3 – Potato crisps, Sweet biscuits
Grp 1 - Cheese & biscuits, Yoghurt, ½ ham swich, Chocolate custard, Cheese scone, ½ chicken swichGrp 2 - Sponge cake, chocolate
mousse, ½ vegemite swich, Cheese spread & crackers
Grp 3 – Potato crisps, Sweet biscuits, Chocolate animal, Savoury biscuit shapes
Drinks Plain milk, milk drink (with malt powder mix).
Water available at all times (after meals and between meals).
Access to low fat and skim milk, soft drinks and cordial on request.
NotspecifiedPlain milk, milk drink (with
malt powder mix).
Water available at all times (after meals and between
meals). Access to low fat and skim
milk, soft drinks and cordial on request.
Plain milk, milk drink (with malt powder mix).
Water available at all times (after meals and between
meals). Access to low fat and skim
milk, soft drinks and cordial on request.
Page 38
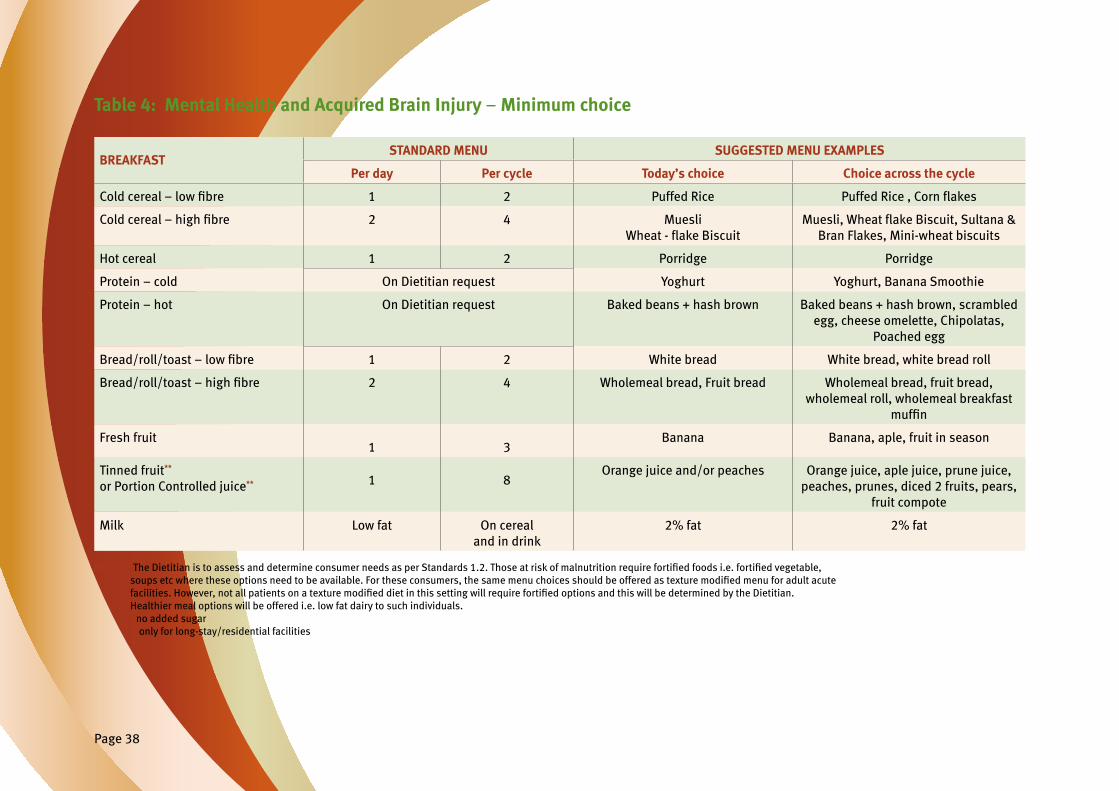
Table 4: Mental Health and Acquired Brain Injury – Minimum choice
BREAKFASTSTANDARD MENU SUGGESTED MENU EXAMPLES
Per day Per cycle Today’s choice Choice across the cycle
Coldcereal–lowfibre 1 2 Puffed Rice PuffedRice,Cornflakes
Coldcereal–highfibre 2 4 MuesliWheat-flakeBiscuit
Muesli,WheatflakeBiscuit,Sultana&Bran Flakes, Mini-wheat biscuits
Hot cereal 1 2 Porridge Porridge
Protein – cold On Dietitian request Yoghurt Yoghurt, Banana Smoothie
Protein – hot On Dietitian request Baked beans + hash brown Baked beans + hash brown, scrambled egg, cheese omelette, Chipolatas,
Poached egg
Bread/roll/toast −lowfibre 1 2 White bread White bread, white bread roll
Bread/roll/toast −highfibre 2 4 Wholemeal bread, Fruit bread Wholemeal bread, fruit bread, wholemeal roll, wholemeal breakfast
muffin
Fresh fruit1 3
Banana Banana, aple, fruit in season
Tinned fruit** or Portion Controlled juice** 1 8
Orange juice and/or peaches Orange juice, aple juice, prune juice, peaches, prunes, diced 2 fruits, pears,
fruit compote
Milk Low fat On cereal and in drink
2% fat 2% fat
Note: *TheDietitianistoassessanddetermineconsumerneedsasperStandards1.2.Thoseatriskofmalnutritionrequirefortifiedfoodsi.e.fortifiedvegetable, soupsetcwheretheseoptionsneedtobeavailable.Fortheseconsumers,thesamemenuchoicesshouldbeofferedastexturemodifiedmenuforadultacute facilities.However,notallpatientsonatexturemodifieddietinthissettingwillrequirefortifiedoptionsandthiswillbedeterminedbytheDietitian. Healthier meal options will be offered i.e. low fat dairy to such individuals. **no added sugar ***only for long-stay/residential facilities

Page 39
Table 4: Mental Health and Acquired Brain Injury – Minimum choice (continued)
MAIN MEALlunch and dinner
STANDARD MENU SUGGESTED MENU EXAMPLES
Per day Per cycle Today’s choice Choice across the cycle
Soup (powder base)* No minimum set and include for seasonal variety 0 0
Soup* Groups 1 and 2 No minimum set
Pea & Ham soup Grp 1 – pea & ham, beef & vege, lentil, minestrone
Grp 2 – Chicken & corn, Creamy pumpkin, Tomato & bacon, Potato & leek
Main hot protein Groups 1, 2, 3 and 4
1 x group 1 or 2
2nd choice 1 x group 1, 2, 3 or 4
35 choices 14 x full 21 x soft
Roast Beef
Chickpea curry
See menu P 57 – 61 for meat/alternative choices
Starchy vegetable or alternative
1 3 Roast potato Mashed sweet potato, mashed/roast potato, Rice/pasta
Orange vegetable 2 3 Mashed pumpkinCarrot
Mashed sweet potato, carrot, mashed or roast pumpkin
Green/brassica vegetable 2 5 CauliflowerBeans
Cauliflower,beans,brusselsprouts,peas,broccoli
Side Salad Minimum 4 vegetables
1 1 Lunch: Lettuce, tomato, carrot sticks, cucumber
Main Salad 100g meat or meat alternative 1 x CHO serve 4 x base vegetables 1 interchangeable vegetable
10 x meat or meat alternative
4 x carbohydrate choices
4 x rotating vegetable
Dinner : Corn beefRice salad
Lettuce & tomatoCucumber & beetroot
See menu P 57 – 61 for meat/alternative choices
Rice Salad, Potato salad, Pineaple, CornLettuce & tomato
Cucumber, beetroot, capsicum, carrot

Page 40
Table 4: Mental Health and Acquired Brain Injury – Minimum choice (continued)
MAIN MEALlunch and dinner
LONG STAY MENU SUGGESTED MENU EXAMPLES*
Per day Per cycle Today’s choice Choice across the cycle
SandwichGroups 1 and 2
1 x group 1 (offer one high fibrebreadchoice)
or 1 x group 2
7 x group 1 7 x group 2
Lunch: Ham & cheeseDinner: Chicken & cranberry
See menu P 57 – 61 for choices
Dessert Groups 1, 2, 3 and 4
No minimum set menu options should consider variety
1
No minimum set menu options should consider variety
7 tinned fruit** and dairy
Lunch: Apricots & custard
Dinner: Lowfattrifle
Fruit – fresh 2 (includes mid-meals) 5 Lunch: ApleDinner: Fruit in season
Aple, banana, fruit in season
Bread/roll/toast −lowfibre 2 Lunch: White breadDinner: White roll
White Bread, white breadroll
Bread/roll/toast −highfibre 2 Lunch: with meal breadDinner: with meal roll
Wholemeal bread, wholemeal breadroll
Note: **no added sugar ***if on minced diet, pureed options can be substituted ****only for long-stay/residential facilities

Page 41
Table 4: Mental Health and Acquired Brain Injury – Minimum choice (continued)
MAIN MEALMorning Tea, Afternoon Tea and Super
LONG STAY MENU
Per day Per cycle Today’s choice Choice across the cycle
SnackGroups 4 only
Three group 4 per day.Offer a variety of healthy, lowfathighfibrechoices
9 Raw nuts, ½ vegemite sandwich (wholegrain/
multigrain), Low fat yoghurt
Grp 4: Low fat yoghurt, Low fat cheese & wholemeal crackers, fresh
fruit, fruit yoghurt, raw nuts, Fruit cake,lowfatmuffin,½vegemitewholegrain sandwich, ½ banana
wholegrain sandwich
High protein/energy suplement and group 3 snacks As requested by Dietitian As requested by Dietitian
Drinks Tea, coffee, water, cordial (no added sugar), milk drink (low fat options)
Tea, coffee, water, cordial (no added sugar), milk
drink (full & low fat options)
Tea, coffee, water, cordial (no added sugar), milk drink (low
fat options)
SECTION 4USER GUIDE
Nutrition Standards for Meals and Menus
SECTION 4USER GUIDENutrition Standards for Meals and Menus
Page 43
USER GUIDE: PUTTING IT ALL TOGETHER
Section 1: Nutrition Standards
Section 1 outlines each Nutrition Standard including the aim, background and rationale.
The Nutrition Standards are measurable and should be used to assess if a sites menu, as well as suporting processes and systems are able to meet these Standards.
• You should be able to answer ‘yes’ or ‘no’ to each Nutrition Standard statements:
> If you answer yes, can you provide the evidence if required?
> If you answer no, then this may be an area for improvement unlessthereisreasonablejustificationastowhyithasnot been met.
Section 2: Meal Component Specifications
Section 2 provides nutritional information on meal components setting minimumlimitsforspecificnutrientstoensurenutritionaladequacy of the menu. The tables outlined in Section 3 Minimum Menu Choice arebasedonthesespecifications.
Section 2 outlines:
• The meal categories i.e. main protein, soup, sandwiches, desserts, hotbreakfastprotein,fortifiedcereals,fortifiedvegetablesand mid-meal snacks.
• The meal component specifications which are displayed as groups undereachcategory.Thespecificationsprovidethedefinition,some examples, recommended serve sizes as well as the energy and protein requirements for each group.
• Portion sizes for non-grouped items are listed separately.
Section 3: Minimum Menu Choice
Section 3 provides the framework for structuring meals across the day as well as across the menu cycle. In order to maximise patient intake, the menu Standards aim to provide a number of choices (as a minimum) that are available to patients per day and per cycle. To ensure maximum choice for main meal hot protein, menus needs to offer a total of 35 choices per cycle. Refer to p 45 to calculate the number of main meal hot protein serves to offer each day based on menu length.
Tables within this section outline:
• The minimum number of choices available to be offered including:
− Minimum menu choice required per day:
> eg. the standard acute menu requires a minimum of 35 hot main meals a day (could be served at lunch or dinner or both)
> eg. the short stay acute menu requires a minimum of one hot main meal a day (could be served at lunch or dinner)
− Minimum menu choice required across the menu cycle:
> eg. the standard acute menu requires a minimum of 35 hot meal choices per cycle, with at least 14 being full choices and 21 being soft choices
> eg. the short stay acute menu requires a minimum of 14 hot meal choices per cycle, with at least 7 being full choices and 5 being soft choices
− Minimum menu choices required across the meal groups:
> eg. the standard acute menu recommends that one of the two hot main meals should be a group 1 or 2 meal and a second choice can be a group 1, 2 or 3 meal (p 20.).
> eg. the short stay acute menu recommends that the main hot protein can be from either group 1, 2 or 3 (p 20).
Page 44
USING THE STANDARDS TO DEVELOP YOUR MENU
1. Determine the length of your menu cycle.
2. List all the items you have available that you plan to use on your menu.
3. Foreachitemthathasamealcomponentspecification(mainhotprotein, soup,sandwiches,dessertandsnacks)placethemintothe‘bestfit’ group. See Apendix 3 for menu examples.
4. Note recommended serve size ranges for other non-grouped meal items.
5. Ensure you have adequate quantity of meal items for your menu. You can check by looking at the recommended minimum number of items per cycle under Section 3.
6. Consider vegetarian and vegan choices in menu planning – see Section 1 for the Standards.
7. Consider what diets can be provided from the main menu and what diets need a separate menu.
8. With the above information you can begin to develop your master menu. (the menu that sits in the kitchen to inform all possible choices for different diet requirements).
a. Menu planning should ensure that the overarching principles in Section 1 of these Standards are met.
b. Menu planning principles such as ensuring variety, colour, texture, taste, apearance and budget should be used to guide your menu development.
Example of the number of daily main hot protein choices across different menu cycle lengths
You will need to know the length of your menu cycle to work out how many choices you should offer per day.
Below is an example of different menu cycle lengths and the number of protein choices you need to provide daily to meet the Standards eg. 35 choices per cycle for standard acute menus.
Repeats are the number of meals that can apear more than once within a cycle once the minimum requirements for variety have been met. Repeats are worked out by multiplying the number of choices per day by number of days in the cycle, then deduct the number of recommended choices (eg. 35 or 28) from the total to see how many repeats would be acceptable.

Page 45
Sample calculations for main hot protein across different menu cycle lengthsYou will need to know the length of your menu cycle to work out how many choices you should offer per day. Below is an example of different menu cycle lengths and the number of choices you need to provide daily to meet the Standards eg. 35 choices per cycle for standard acute menus.
Adult Acute, Residential Aged Care, Mental Health & Acquired Brain Injury : Long stay menu
MAIN MEAL Hot Protein
MENU CYCLE
7 day 14 day 21 day
Lunch 2 choices 1 choice 2 choices 1 choice 1 choice
Dinner 3 choices 2 choices 2 choices 1 choice 2 choices
Possible Repeats# No repeats 7 repeats 21 repeats 7 repeats 28 repeats
Fortexturemodifiedmealswithatotalof28mincedandmoistand28smoothpureedchoices,thedailychoiceswouldbeasfollows:
Adult Acute: Texture Modified Menu
MAIN MEALHot Protein
MENU CYCLE
7 day 14 day 21 day
Lunch 2 Minced and Moist 2 Smooth Puree
1 Minced and Moist 1 Smooth Pureed
2 Minced and Moist 2 Smooth Pureed
1 Minced and Moist 1 Smooth Pureed
Dinner 2 Minced and Moist 2 Smooth Puree
1 Minced and Moist 1 Smooth Puree
1 Minced and Moist 1 Smooth Pureed
1 Minced and Moist 1 Smooth Pureed
Possible Repeats# No repeats No repeat 14 repeats each texture 14 repeats each texture
Note: *can use the same meat with different sauces/gravies to increase variety. #repetitions are only necessary if the 35 meals are the minimum – it is possible to reduce repetition by having additional choices available (see menu meal choices at the end of this document).
Page 46
DEFINITIONS AND ABBREVIATIONSBreakfast Protein
Referstoitemsavailablethatcontributesignificantly to protein intake.
Hot – Examples include eggs, sausages, savoury mince, bacon or baked beans. Note: spaghetti is not high in protein but can be offered in addition to one of the higher protein choices.
Cold – Includes yoghurt, cheese or milk drinks, cold boiled eggs, cold meats.
CHO
Carbohydrate
Choice
The number of available options, either over a day or within the cycle.
Finger Foods
Finger foods may be useful to assist intake and independence. These items do not require utensils thus enable patients to eat these foods on their own without feeding assistance. Examples include sandwiches, meat balls, sausage rolls, mini pies or quiches.
Fortification of Menu Items
Toprovideadditionalnutrition,fortificationofcertain meal components including hot cereals, soups, vegetables anddessertisrequired.Fortificationaimstoincrease the protein and/or energy density of the meal component. See p 21 – 23 for further details.
Fruit
Citrus and tropical fruits are a good source of Vitamin C and should be included each day. The intent is to have a small range of fresh fruit in season that is available for all texture levels so including at least one soft fresh fruit each day that can be mashed or minced. Note: all melons should be adequately sanitised and peeled before serving.
‘Healthy’ meal options
These meal options are lower in saturated fat, fat, energy and/or salt than other items offered at the facility. The Dietitian will assess what options are suitable for patient groups.
High fibre cereals
Theseshouldprovideatleast3gfibreperserve.
Integrated Menu
Refers to a menu structure that enables the most common diets to be ordered from the main menu without compromising taste and nutritional adequacy. Commonly integrateddietsarefibremodified,carbohydratemodified,fatmodified,lowlactoseandsofttexturediets.Somedietsaremoredifficulttointegrateintothemainmenuandmayrequire a separate menu eg gluten free and electrolyte modifieddiets.Howeveritisrecommendedthatsuitableitems from the main menu be used where able.
LOS
Length of stay.
Main menu
All foods available through the standard meal service, not requiring to be made up ‘specially’ as in an individual therapeutic diet.
Meats and Meat Alternatives:
Thefoodsinthisgroup(i.e.redmeats,poultry,fish,egg,nuts and legumes) are very valuable sources of protein as well as being a major source of a number of minerals and vitamins, such as iron, zinc, vitamin B12 and, in the case offish,omega-3fats.4
Red meats are particularly good sources of iron, zinc and B12, and include beef, veal, and lamb. A range of red meats should be offered across the menu cycle so that there is at least one red meat choice each day on the menu.
Arangeofpoultry,pork,eggs,fishandmeatalternatives(i.e. legumes, nuts or seeds) should be considered in menu planning to provide variety and additional nutrients i.e. omega-3fatsinfish.
Menu Assessment
It is a requirement that menus are reviewed biennially against Nutrition Standards for Meals and Menus (refer to Statewide Foodservice Best Practice Guideline2). This assessment would include a major review of menu structure including length of cycle and number of choices. Continual menu reviews should occur on an ongoing basis as required to address changes in contracts and/or SOAs, assess meal quality aspects, products or recipes.
OBD
Overnight bed days.
Salads
The Standards recommend a minimum of four salad vegetables for the side salad as well as the main salad. This includes lettuce (ideally mixed leaf), tomato and two rotating salad vegetables (eg. onion, capsicum, cucumber, grated carrot, celery, mushroom, beetroot or asparagus).
A carbohydrate (CHO) source for salad could include either a starchy vegetable salad item (eg. potato salad, sweet potato salad, corn, or bean mix) or a cereal salad item (eg. pasta salad, rice salad or cous cous salad). A CHO serve should be 90 – 120g. The main salad also requires a source of protein daily.
Page 47
Definitions and Abbreviationscontinued
Serve size variation
The Standards (refer to p 8) recommend that serve size variations be available on the menu including as a minimum small, medium (standard serve) and large options where practical.
For some items (i.e. portion controlled) offering serve size variations may not be practical and visual apearance of such items should be considered.
Main Meal Protein
• A small serve would be considered 75% of a standard serve due to the nutritional value of this meal component.
• A large serve would be up to 150% of a standard serve.
Vegetables
• A small serve would be considered between 50-75% of a standard serve.
• A large serve would be up to 150% of a standard serve.
Desserts
• A small serve would be considered between 50-75% of a standard serve.
• For a large dessert serve, it is suggested that additional components are offered where practical eg. custard, instead of a large portion size, if tray space is an issue.
Short stay menu
An alternative menu may be provided to patients who are not at nutritional risk and are admitted for less than 7 days toanacutefacility.Thismenudoesnotincludefortifiedoptions and has been modelled to provide a reduced choice version of the standard menu.
SOA
Standing offer arrangement. Products that are on the Qld Health State-wide Food Service SOA have gone through the tender process and have been accepted as meeting certain criteria. Current categories for SOA's are: SOA 066 –TextureModifiedfoodsincluding smooth puree and minced and moist textures.
SOA 067 – Full and soft meal components and plated meals. SOA 068 –Thickenedfluidsandthickener
Long stay menu
Long stay patients and those assessed as malnourished or at risk of malnutrition in acute facilities, need to have access to higher energy/protein food choices to increase the likelihood of meeting their elevated nutritional requirements. The standard hospital menu will provide nutrientdensemenuoptionsincludingfortifieditemsincluding a cold and hot protein choice at breakfast, fortifiedcereal,vegetable,soupandmid-mealstomeetnutritional targets and maximize patient/resident/client or consumer choice. This menu is intended to be offered as the standard or general menu in acute adult facilities with the exception of short stay patients i.e. patients staying less than 7 days who would be offered a short stay menu.
Texture modified diets
Terminology used is based on Australian Standardised TerminologyandDefinitionsforTextureModifiedFood and Fluids43.
Vegetables
Starchy vegetables – these vegetables are higher in kilojoules per unit weight than other vegetables but are a major staple in the Australian diet and a useful sourceofsolublefibresoaminimumofoneperday has been recommended. They include potato, corn, and sweet potato.
Green/brassica vegetables – have a good range of nutrients andarelowinkilojoulesandagoodsourceoffibre. Green/brassica vegetables include – green beans, peas, broccoli,cauliflower,brusselsprouts,cabbage,zucchini,spinach and silverbeet.
Orange vegetables – are also a good source of vitamins, mineralsandfibre.Theyincludecarrots,pumpkin and sweet potato. Note: sweet potato is counted as a starchy vegetable as well as orange and are higher in kilojoules.
Page 48
REFERENCES1. Queensland Health. 2008. Queensland Health Foodservices Policy. Queensland Government, Brisbane.
2. Queensland Health. 2009. Queensland Health State-wide Food Service Best Practice Guidelines. Queensland Government, Brisbane.
3. Queensland Health. 1998. Queensland Health Foodservices Policy, Corporate Guidelines and Standards. Queensland Government, Brisbane.
4. National Health and Medical Research Council. 2013. Australian Dietary Guidelines. Canberra: National Health and Medical Research Council.
5. Department of Human Services (DHS) Victoria. 2009. Nutrition Standards for menu items in Victorian hospitals and aged care facilities. Melbourne: Victorian Government. Retrieved 17 January 2008 from http://www.health.vic. gov.au/patientfood/nutrition_Standards.pdf
6. Queensland Health 2010. Queensland Health State-wide KPI's Queensland Government, Brisbane.
7. National Health and Medical Research Council. 2013. Australian Dietary Guidelines-providing the scientificevidenceforhealthierAustraliandiets. Retrieved 2 June 2015 from www.nhmrc.gov.au/guidelines- publications/n55
8. Queensland Mental Health Benchmarking Unit (QMHBU). 2009. Multi-SiteBenchmarkingofExtendedTreatment Acquired Brain Injury Inpatient Mental Health Services Benchmarking Report. Retrieved May 2010 from http:// qheps.health.qld.gov.au/mhbenchmarking/documents/ ABI_Report_09_Web.pdf
9. Queensland Mental Health Benchmarking Unit (QMHBU). 2009. ExtendedTreatmentRehabilitationandDual Diagnosis Mental Health Benchmarking Report. Retrieved May 2010 from http://qheps.health.qld.gov.au/ mhbenchmarking/documents/ABI_Report_09_Web.pdf
10. De Hert M, Schreurs V, Vancampfort D, and Van Winkel R. 2009. Metabolic syndrome in people with schizophrenia: a review. World Psychiatry. 8: 15-22.
11. Dickerson F, Brown C, Daumit G, LiJuan F, Goldberg R, Wohlheiter K, and Dixon L. 2006. Health status of individuals with serious mental illness. Schizophrenia Bulletin. 32: 584–589.
12. National Health and Medical Research Council (NHMRC). 2006. Nutrient Reference Values for Australia and New Zealand including Recommended Dietary Intakes. Australia: Australian Government. Retrieved 23 June 2008 from http://www.nhmrc.gov.au/publications/ synopses/_ files/n35.pdf
13. Almdal, T., L. Viggers, A. Beck, K. Jensen, 2003. Food production and wastage in relation to nutritional intake in a general district hospital – wastage is not reduced by training the staff. Clinical Nutrition, 22 (1): 47-51.
14. Kondrup, J., N. Hohansen, L. Plun, L. Bak, I. Hojlund Laresen, A. Martinsen, J. Andersen, H. Baernthsen, E. Bunch, N. Lauesen, 2002, Incidence of nutrition risk and causes of inadequate nutritional care in hospitals. Clinical Nutrition, 21 (6): 461-468
15. Barton, A., C. Beigg, I. Macdonald, S. Allison, 2000-2. High food wastage and low nutrition intakes in hospital patients. Clinical Nutrition, 19 (6): 445-449.
16. Dupertuis, Y., M. Kossovsky, U. Kyle, C. Raguso, L. Genton, C. Pichard, 2003. Food intake in 1707 hospitalised patients: a prospective comprehensive hospital survey. Clinical Nutrition, 22 (2): 115-123.
17. Gallagher-Allred, C., A. Cobble Voss, K. Koop, 1999. The effect of medical nutrition therapy on malnutrition and clinical outcomes. Nutrition, 15 (6): 512-514.
18. Alison, S. 2003. Hospital food as treatment. Ed. Clinical Nutrition, 22 (2): 113.
19. Isabel, M., M. Correia, D. Waitzberg. 2003. The impact of malnutrition on morbidity, mortality, length of hospital stand and costs evaluated through a multivariate model analysis. Clinical Nutrition, 22 (3): 235-239.
20. Elia, M. 2006. Nutrition and health economics. Nutrition, 22: 576-578.
21. Odlund Olin, A., OP. Osterberg, K. Hadell, I Armyr, S. Jerstrom, O. Ljungqvist. 1996. Energy-enriched hospital food to improve energy intake in elderly patients. American Society for Parenteral and Enteral Nutrition 20 (2): 93-97.
22. Gall, M., G. Grimble, N. Reeve, S. Thomas, 1998, Effectofprovidingfortifiedmealsandbetween-meal snacks on energy and protein intake of hospital patients, Clinical Nutrition, 17(6): 259-264
23. Barton, A., C. Beigg, I. Macdonald, S. Allison, 2000-1. A recipe for improving food intakes in elderly hospitalised patients. Clinical Nutrition, 19 (6): 451-454.
24. Lorefalt, B., U. Wissing, M. Unosson. 2005. Smaller but energy and protein-enriched meals improve energy and nutrient intakes in elderly patients. The Journal of Nutrition, Health and Aging, 9 (4): 243-247.
25. National Health and Medical Research Council. 2010. Public Statement: Iodine suplementation for Pregnant and Breastfeeding Women. Retrieved 16 May 2011 from http://www.nhmrc.gov.au/publications/synopses/ new45_syn.htm
26. National Health and Medical Research Council. 2010. Iodine Suplementation During Pregnant and Lactation - Literature Review. Retrieved 16 May 2011 from http:// www.nhmrc.gov.au/publications/synopses/ new45_syn.htm
27. Food Standards Australia New Zealand. Listeria and food – advice for people at risk. Retrieved 15 May 2011 fromhttp://www.foodStandards.gov.au/_srcfiles/ Listeria.pdf
28. Queensland Health. 2007. A Healthy Start in Life – a nutrition manual for health professionals. Queensland Government, Brisbane.

Page 49
29. Australian Government, 2014. Care and services in aged care homes - Information for aproved providers. Accessed 16 June 2015 from http://www. dss.gov.au/ our-responsibilities/ageing-and-aged-care/for-providers/ guidance-for-providers/care-and-services-in-aged-care- homes-information-for-aproved-providers
30. Alix, E., G. Berrut, M. Bore, F. Bouthier-Quintard, J. Buia,A. Chlala, Y. Cledat, G. d’Orsay, C. Lavigne, R. Levasseur, J. Mouzet, M. Ombredanne, A. Salle, C. Gaillard, P. Ritz. 2007. Energy requirements in hospitalized elderly people. Journal American Geriatrics Society, 55: 1085-1089.
31. Odlund Olin, A., I. Armyr, M. Soop, S. Jerstrom, I. Classon, T. Cederholm, G. Ljunggren, O. Ljungqvist. 2003. Energy-dense meals improve energy intake in elderly residents in a nursing home, Clinical Nutrition, 22 (2): 125-131
32. NSW Health. 2010. Eating Well - A Food and Nutrition Resource for Frail Older People and their Carers. Retrieved 14 April 2011 from http://www.mncrcsd. com.au/uploads/uploads/Eating%20Well-final- NSCCAHS-2010.pdf
33. Jean LA. 1997. Finger food menu restores independence in dining. Health Care Food and Nutrition Focus. 14 (1): 4-6.
34. Ford G. 1996. Putting feeding back into the hands of patients. Journal of Psychosocial Nursing and Mental Health Services. 34 (5): 35-39. 35. Holt, I.G. Peveler, R.C. 2009. Obesity, serious mental illness and antipsychotic drugs. Diabetes, Obesity and Metabolism, 11: 665-679.
36. Ward, E. C. and Morgan, A. T. 2001. Dysphagia following traumatic brain injury in adults and children: assessment and characteristics. In B.E.Murdoch and D. G. Theodoros (Eds.), Traumatic brain injury: ssociated speech, language, and swallowing disorders p. 331-367. San Diego: Singular Publishing Group.
37. De Hert M, Dockx L, Bernagie C, Peuskens B, Sweers K, Leucht S, Tack J, Van de Straete S, Wampers M, Peuskens J.2011. Prevalence and severity of antipsychotic related constipation in patient with schizophrenia: a retrospective descriptive study. BMC Gastroenterology 11:17.
38. National Health and Medical Research Council. 2003. Dietary Guidelines for Australian Adults. Commonwealth of Australia.
39. Craig WJ, Mangels AR. 2009. Position of the American Dietetic Association: vegetarian diets. Journal of the American Dietetic Association. 109 (7): 1266-1282.
40. Craig WJ. 2010. Nutrition concerns and health effects of vegetarian diets. Nutrition in Clinical Practice. 25(6): 613-620.
41. Craig WJ. 2009. Health effects of vegan diets. American Journal of Clinical Nutrition. 89(5): 1627S – 1633S.
42. Lightowler HJ, Davies GJ. 2002. Assessment of iodine intake in vegans: weighed dietary record vs duplicate portion technique. European Journal of Clinical Nutrition. 56(8): 765-770.
43. Dietitians Association of Australia and The Speech Pathology Association of Australia Limited, 2007. AustralianStandardisedTerminologyandDefinitions forTextureModifiedFoodsandFluids.Nutrition and Dietetics, 64: (Supl. 2): S53-S76
44. Cruickshank D. 2009. Development of nutrition Standards for general menus for Queensland Health hospitals and residential aged care facilities. Masters research paper. Unpublished. 45. Gaillard, C., E. Alix, Y. Boirie, G. Berrut, P. Ritz. 2007. Energy requirements in frail elderly people: A review of the literature. Clinical Nutrition 26: 16-24.
46. Gariballa, S. and S. Forster. 2006. Energy expenditure of acutely ill hospitalised patients. Nutrition Journal. 5 (9): 9-15. Retrieved 9 October 2009 from http://web.ebscohost.com.ezp01.library.qut.edu. au/ehost/pdf?vid=1&hid=5&sid=30b27595-a2ff-49fb- bcea-3e20a2de8911% 40sessionmgr10
47. Miles, J. 2006. Energy expenditure in hospitalized patients: implications for nutritional suport. Mayo Clinic Proceedings. 81 (6): 809-816.
48. Johansen, N., J. Kondrup, L. Munk Plum, L. Bak, P. Norregaard, E. Bunch, H. Baernthsen, J. Andersen, I. Larsen, A. Martinsen. 2004. Effect of nutrition suport on clinical outcome in patients at nutrition risk. Clinical Nutrition. 23: 539-550.
49. World Health Organisation. 1981. Energy and protein requirements : report of a Joint FAO/WHO/UNU Expert Consultation [held in Rome from 5 to 17 October 1981], Rome: Italy.
50. Schofield,W.N.1985.Predictingbasalmetabolic rate, new Standards and review of previous work. Human Nutrition. Clinical Nutrition. 39 (Supl 1): 5-41.
51. Sharpe, J-K., Stedman, T., Byrne, N.M., Hills, A.P. 2010. Prediction of resting energy requirements in people taking weight-inducing antipsychotic medications. Nutrition and Dietetics. 67 (3): 166-170.
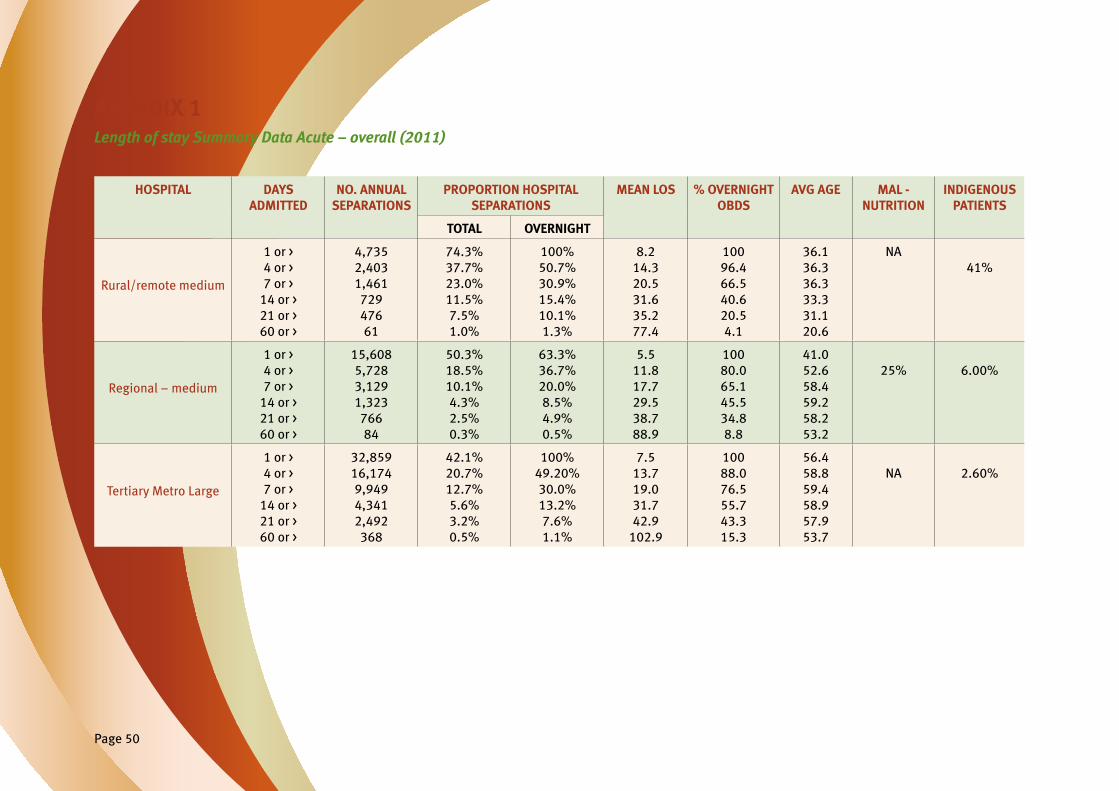
Page 50
APENDIX 1Length of stay Summary Data Acute – overall (2011)
HOSPITAL DAYS ADMITTED
NO. ANNUAL SEPARATIONS
PROPORTION HOSPITAL SEPARATIONS
MEAN LOS % OVERNIGHT OBDS
AVG AGE MAL - NUTRITION
INDIGENOUS PATIENTS
TOTAL OVERNIGHT
Rural/remote medium
1 or > 4 or > 7 or >
14 or > 21 or > 60 or >
4,735 2,403 1,461 729 476 61
74.3% 37.7% 23.0% 11.5% 7.5% 1.0%
100% 50.7% 30.9% 15.4% 10.1% 1.3%
8.2 14.3 20.5 31.6 35.2 77.4
100 96.4 66.5 40.6 20.5 4.1
36.1 36.3 36.3 33.3 31.1 20.6
NA41%
Regional − medium
1 or > 4 or > 7 or >
14 or > 21 or > 60 or >
15,608 5,728 3,129 1,323 766 84
50.3% 18.5% 10.1% 4.3% 2.5% 0.3%
63.3% 36.7% 20.0% 8.5% 4.9% 0.5%
5.5 11.8 17.7 29.5 38.7 88.9
100 80.0 65.1 45.5 34.8 8.8
41.0 52.6 58.4 59.2 58.2 53.2
25% 6.00%
Tertiary Metro Large
1 or > 4 or > 7 or >
14 or > 21 or > 60 or >
32,859 16,174 9,949 4,341 2,492 368
42.1% 20.7% 12.7% 5.6% 3.2% 0.5%
100% 49.20% 30.0% 13.2% 7.6% 1.1%
7.5 13.7 19.0 31.7 42.9
102.9
100 88.0 76.5 55.7 43.3 15.3
56.4 58.8 59.4 58.9 57.9 53.7
NA 2.60%
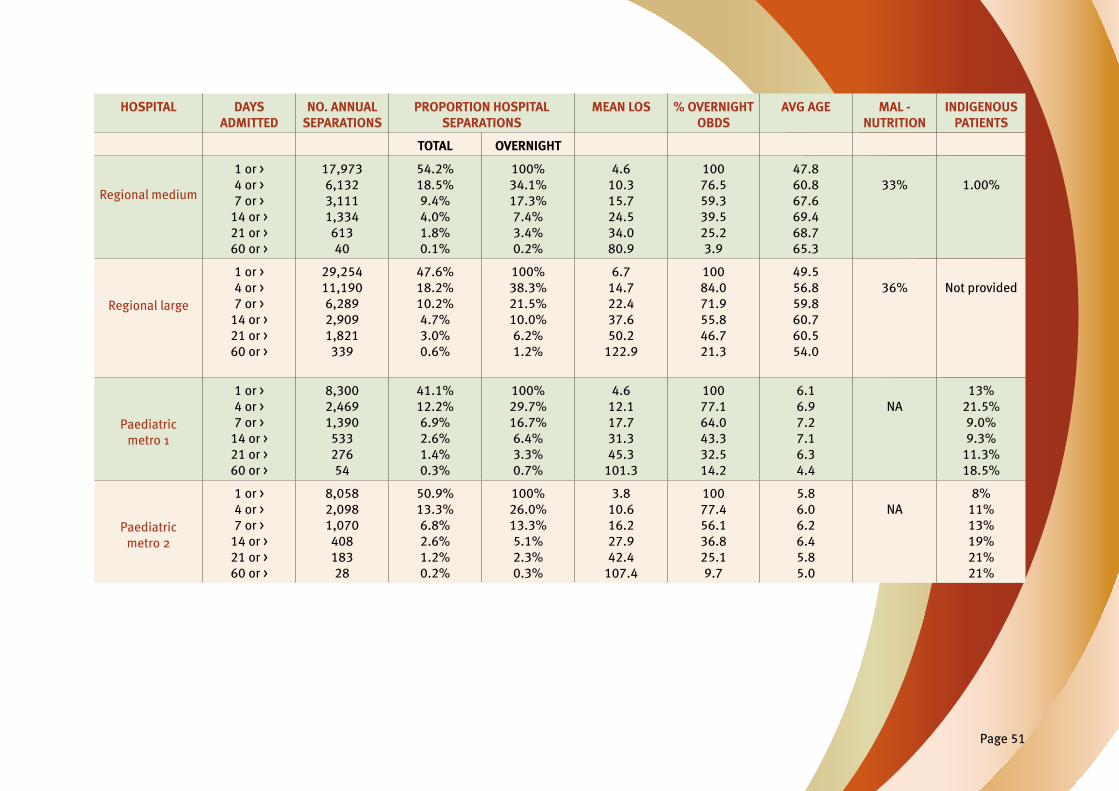
Page 51
HOSPITAL DAYS ADMITTED
NO. ANNUAL SEPARATIONS
PROPORTION HOSPITAL SEPARATIONS
MEAN LOS % OVERNIGHT OBDS
AVG AGE MAL - NUTRITION
INDIGENOUS PATIENTS
TOTAL OVERNIGHT
Regional medium
1 or > 4 or > 7 or >
14 or > 21 or > 60 or >
17,973 6,132 3,111 1,334 613 40
54.2% 18.5% 9.4% 4.0% 1.8% 0.1%
100% 34.1% 17.3% 7.4% 3.4% 0.2%
4.6 10.3 15.7 24.5 34.0 80.9
100 76.5 59.3 39.5 25.2 3.9
47.8 60.8 67.6 69.4 68.7 65.3
33% 1.00%
Regional large
1 or > 4 or > 7 or >
14 or > 21 or > 60 or >
29,254 11,190 6,289 2,909 1,821 339
47.6% 18.2% 10.2% 4.7% 3.0% 0.6%
100% 38.3% 21.5% 10.0% 6.2% 1.2%
6.7 14.7 22.4 37.6 50.2
122.9
100 84.0 71.9 55.8 46.7 21.3
49.5 56.8 59.8 60.7 60.5 54.0
36% Not provided
Paediatric metro 1
1 or > 4 or > 7 or >
14 or > 21 or > 60 or >
8,300 2,469 1,390 533 276 54
41.1% 12.2% 6.9% 2.6% 1.4% 0.3%
100% 29.7% 16.7% 6.4% 3.3% 0.7%
4.6 12.1 17.7 31.3 45.3
101.3
100 77.1 64.0 43.3 32.5 14.2
6.1 6.9 7.2 7.1 6.3 4.4
NA13%
21.5% 9.0% 9.3%
11.3% 18.5%
Paediatric metro 2
1 or > 4 or > 7 or >
14 or > 21 or > 60 or >
8,058 2,098 1,070 408 183 28
50.9% 13.3% 6.8% 2.6% 1.2% 0.2%
100% 26.0% 13.3% 5.1% 2.3% 0.3%
3.8 10.6 16.2 27.9 42.4
107.4
100 77.4 56.1 36.8 25.1 9.7
5.8 6.0 6.2 6.4 5.8 5.0
NA8%
11% 13% 19% 21% 21%
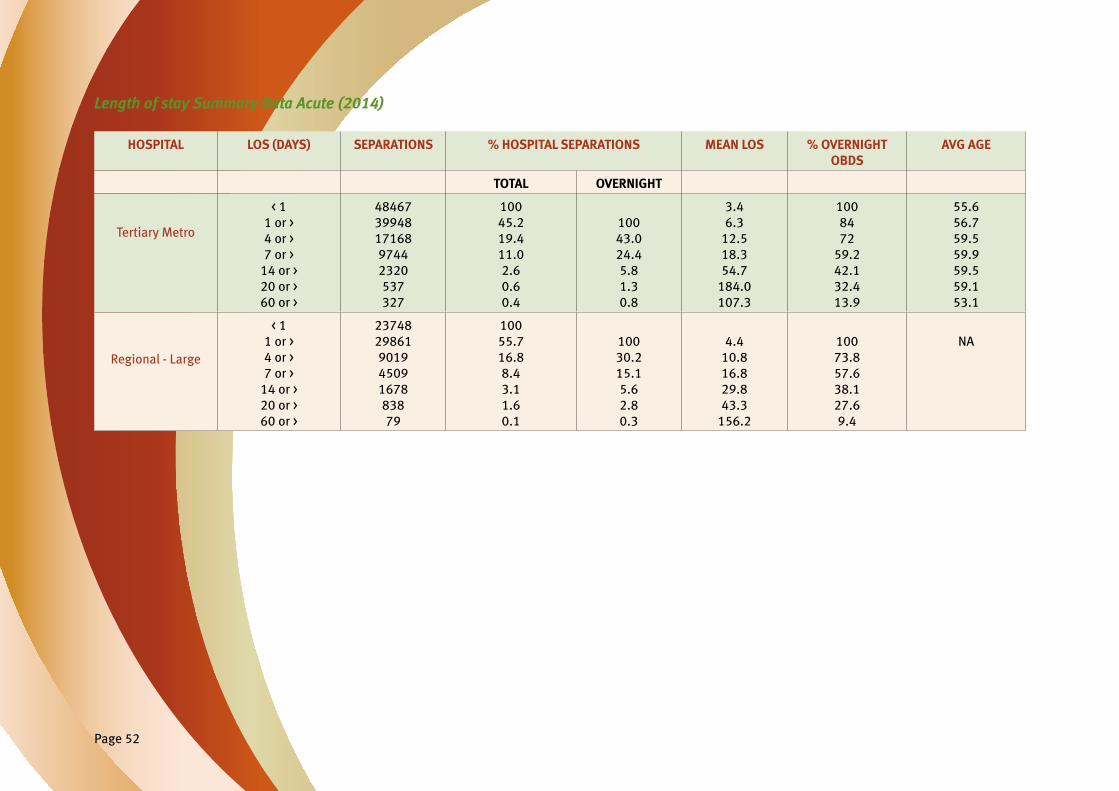
Page 52
HOSPITAL LOS (DAYS) SEPARATIONS % HOSPITAL SEPARATIONS MEAN LOS % OVERNIGHT OBDS
AVG AGE
TOTAL OVERNIGHT
Tertiary Metro
< 11 or > 4 or > 7 or >
14 or >20 or >60 or >
48467399481716897442320537327
10045.219.411.02.60.60.4
10043.024.45.81.30.8
3.46.3
12.518.354.7
184.0107.3
1008472
59.242.132.413.9
55.656.759.559.959.559.153.1
Regional - Large
< 11 or > 4 or > 7 or >
14 or >20 or >60 or >
237482986190194509167883879
10055.716.88.43.11.60.1
10030.215.15.62.80.3
4.410.816.829.843.3
156.2
10073.857.638.127.69.4
NA
Length of stay Summary Data Acute (2014)

Page 53
Length of Stay data for Acquired Brain Injury (ABI) QH facilities (2011)
LOS DAYS (AVERAGE)
GENDER % M/F
AGE(YRS)
WEIGHT(KG)
BMI AVERAGE(KG/M2)
2,991 M 100 50 76 25
1,910 M 60 F 40 50 73 25
700 M 83 F 17 46 85 27
1,778 M 44 F 56 47 71 26
Average 1,845 (5.1 years) M 72 F 28 48 76 25.8
Length of Stay Data for Mental Health Units QH facilities (2011)
MH UNIT DAYS ADMITTED NO. ANNUAL SEPARATIONS
% OVERNIGHT SEPARATIONS
MEAN LOS AVG AGE
Tertiary Metro Large
1 or >
4 or >7 or >
14 or >
21 or >
60 or >
1,356
998820
569
383
73
100%
77.6%
63.8%44.3%
29.8%
5.7%
21.7
27.3
31.941.3
52.7
129.7
40.4
41.7
43.044.2
46.2
54.3
Tertiary Regional Large
1 or >
4 or >
7 or >14 or >
21 or >
60 or >
3,328
3,027
2,238
1,4741,127
417
100%
90.9%67.2%
44.3%
33.9%
12.5%
69.7
75.498.5
145.5
168.3
455
39.4
38.4
39.347.4
39.8
33.8

Page 54
APENDIX 2REFERENCE PERSONS USED IN STANDARDS DEVELOPMENT Adult Reference Persons and Nutrient Targets
Length of stay (LOS)
Analysis of LOS across Queensland Health facilities revealed two distinct patient populations. Those admitted for less than seven days and those that remained longer than fourteen days (refer to Apendix 1 for LOS details). This result informed the recommendation that a basic seven to fourteen day menu be provided for short stay patients. For those patients admitted for more that seven days, or assessed as being malnourished or at risk of malnutrition, a minimum fourteen day menu with additional items is required. Dataanalysisfor2siteswasrepeatedin2014andshowednosignificantchange in the percentage of patients that stay longer than 7 days but did show an increase in the average LOS of those patients.
Age
All adult acute hospitals analysed showed similar age and Occupied Bed Days (OBD)datawiththeexceptionofMountIsawhichhadasignificantlyyoungerpopulation and the highest number of indigenous patients. The average age of patients admitted for less than seven days is 41 – 67 years with exception of Mount Isa where the average age is 33 years. Analysis of patients with LOS greater than seven days revealed 50% OBD are occupied by people with average age 58 – 69 years except at Mount Isa hospital where the average age 36 years and decreases to 21 years for those staying more than 60 days.44
Nutritional Requirements
To determine the energy and protein requirements for the average age of patients admitted to Queensland Health facilities, a reference male of 76kg* was adapted from NHMRC Nutrient Reference Values for Australia and New Zealand including Recommended Dietary Intakes (NRVs).12
*Note: excludes mental health and acquired brain injury refer to section for details on reference weight use.
Standard acute adult patient
Energy and protein requirements* were calculated utilising equations derived from studies30, 45, 46, 47 in acute hospitals and residential aged care to determine the values below;
Energy 105 – 125 kJ/kg/day: 76kg male 8,000 – 9,500kJ
Protein 1.2g/kg/day: 76kg male 95g protein
*Note: Mount Isa Hospital average patient age for LOS greater than seven days was 36 years. Estimated energy and protein requirements for males aged 31 – 50 (Mount Isa) with average weight 76kg.
Energy 125kJ/kg/day 9,500kJ
Protein 1.2g/kg/day 95g
Standard acute menu
For patients with LOS greater than 7 days, Recommended Dietary Intake (RDI) reference values for males aged 51 – 70 years were utilised to assess adequacy of micronutrients. With the priority to meet protein and energy requirements, reference RDIs were not considered achievable and certain nutrients will require consideration in menu planning based on patient population).
A modelled fourteen day cycle with a hot and cold protein choice at breakfast, mid-mealsandfortifiedfooditemsmetestimatedproteinandenergyrequirements (energy 10,200kJ and 107g protein). All RDIs were also met except for folate, magnesium and zinc. For these nutrients only the Estimated Average Requirement (EAR) could be met for zinc. It was noted that EARs for folate and magnesium could not be met (75% and 93% respectively). Dietary fibrelevelsalsofellbelowAdequateIntake(AI)forthisgroup.Theprioritytomeet protein and energy requirements has resulted in certain micronutrient nutrients shortfalls that will require consideration in menu planning. Fibrefortificationmayalsorequireconsideration.Allfacilitieswillneed to consider whether they need to address this shortfall with their own menu based on the patient demographics.

Page 55
This menu was also assessed and met estimated protein and energy requirements for males aged 31 – 50 years. All RDIs for males aged 31 – 50 years were met except for folate and magnesium. EARs for these nutrients couldnotbemet(folate92%andmagnesium88%).Dietaryfibrealsofellbelow AIs for this group.
Short stay adult patient
Energy and protein requirements were derived from NRVs on the basis that RDI for protein for males aged 19 – 70 years is 0.84g/kg and the recommended Energy for sedentary males aged 19 – 70 years is 95 – 110kJ/kg/day.12
Energy 100kJ/kg/day: 76kg male 7,600kJ
Protein 0.84g/kg/day 76kg male 63.8g
Short stay menu
RDI reference values for males aged 51 – 70 years were utilised to assess sample menus for adequacy of micronutrients for short stay menu (i.e. those patients admitted for less than seven days who are not at risk of malnutrition nor require additional energy or protein, for example an admission for management of chest pain). The short stay menu was modelled to provide a minimum seven day cycle or reduced choice fourteen day cycle.
Minimum modelling provided an estimated energy level of 8,300 kJ and 76g protein meeting estimated requirements. All RDIs were met except for folate, magnesium, calcium and zinc however met EAR for calcium. Fibre levels also fell below AI values. Following this exercise, it was acknowledged that some vitamins and minerals will require special consideration in menu planning. Fibrefortificationmayalsorequireconsideration.Allfacilitieswillneedtoconsider whether they need to address this shortfall with their own menu based on the patient demographics.
Aged Care Reference Persons and Nutrient Targets
Standard and pureed 14 day cycle menus were modelled to meet requirements for males aged 70 years or older with an average weight 76kg. Energy and protein requirements were calculated utilising equations derived from literature31, 48,49 in aged care.
Energy 105kJ – 1,26kJ/kg/day 76kg male 7,320 – 9,580kJ
Protein 1.2g/kg: 76kg male 91.2g
Reference RDIs for males aged 70 years or older were used to assess micronutrient adequacy. Suggested Dietary Targets (SDTs) for disease prevention were not aplied to this group as they were felt to be inapropriate for aged care setting. Modelling was based on the use of small serves i.e. 75% of standard serve.
Analysis of the aged care menu revealed similar results to menus modelled for the acute setting with folate, magnesium and zinc not meeting reference RDIs. EAR value for zinc was met (110%) and was marginal for magnesium (99%).AIforfibrewasalsonotachieved.ForpureedmenutheonlyRDInotmetwasfolateandAIoffibrewasalsolow.Similarlytothestandardacutemenu, the priority to meet protein and energy requirements have resulted with certain micronutrient nutrients shortfalls that will require consideration in menu planning. All facilities will need to consider whether they need to address this within their own menu.
Paediatric Reference Person and Nutrient Targets
The reference child on whom recommendations are based is a 7 year old boy (23kg), on the 50th centile on the CDC 2000 growth charts. EnergyrequirementswereestimatedusingSchofieldequation50 and the 4 – 8 year olds RDI for protein was adapted from NHMRC NRVs.12
Energy 6,657kJ
Protein 20g/day

Page 56
Using reference RDIs for 4 – 8 year olds menus modelled met energy needs up to 7,700kJ and protein requirements. All RDIs were also achieved except forfolatehowevertheEARwasmetat119%.TheAIforfibrewasalsonotachieved. Menu choices were modelled on actual consumption and based on the understanding that at mixed adult and paediatric hospital, additional adult food would be offered to older children. Available serves were based on all choices available and those items on the ward at all times (i.e. fresh fruit, yoghurts, juice, milk drink, bread and spreads).
Other assumptions used in modelling included:
• additional juice (100ml) at breakfast;
• half main protein serves;
• half serve* of ice cream and fruit with main meal;
• half serve* of high protein dessert at light meal;
• as mid-meal snacks; and
• one milk drink and two soft drinks or cordials per day. *Note: A half serve was set as half the minimum portion size on p 28 i.e. ice cream = 40g serve.
Mental Health and Acquired Brain Injury Reference Person and Nutrient Targets
Inordertodeterminetherepresentativeprofileofareferencepersonforthisgroup, mean age, heights and weights were sourced from the Queensland Mental Health Benchmarking Unit (QMHBU) data.8, 9 From this data, a reference male with an average adjusted weight of 80kg*, height of 175cm and age of 44 years was determined.
To allow for variation in mobility a range for energy requirements has been developed based on two Physical Activity Levels (PALs); 1.2 (bed rest) to 1.4 (very sedentary). Estimated energy requirements were calculated using the Harris-Benedict equation, with the RMR being reduced by 840kJ/day as the Harris-Benedict equation has been found to overestimate RMR in men taking antipsychotic medications.51 It is acknowledged that some individuals within this group will have higher energy requirements based on age, body weight/body composition and PALs; it is recommended that facilities consider whether they need to address this with their own menu based
on the consumer group. Protein requirements were calculated based on the RDI for males aged 31 – 50 years.12
Energy (PAL 1.2 – 1.4) Males 7,700 – 9,100kJ/day
Protein 0.84g/kg: Males 67g/day
To address the issues of chronic disease prevention, where possible, reference Suggested Dietary Targets (SDTs) and Acceptable Macronutrient Distribution Ranges (AMDRs) in addition to RDIs and EARs for males aged 31 – 50 years were used to assess nutrient adequacy.12 For the standard texture menu, as modelled against the reference male, all RDIs and EARs were met; however, Vitamin C and Potassium did not meet the SDT minimum at 97% and 90% respectively. Sodium exceeded the SDT maximum (137%), however,wasbelowtheUperLevel(UL)of2,300mg.Thetexturemodifiedmenu did not meet the RDIs for folate (90%), magnesium (84%) and zinc (99%), however, when compared against the EARs all were met although magnesiumremainedmarginal(101%).ThetexturemodifiedmenudidnotmeettheSDTminimumsforfibre(70%),vitaminC(82%)andpotassium(99%); Sodium exceeded the SDT maximum (127%), however, was below the Uper Level (UL) of 2,300mg.
Evidently, the micronutrients that were found to fall below the RDI and potentially those that fell below the SDT will require special consideration in each facility undertaking menu planning for these population groups. Fibrefortificationmayalsorequireconsiderationforthetexturemodifiedmenu. It was noted that bread made a large contribution to the sodium content in the standard texture menu. It is acknowledged that bread is a popular staple and it is impracticable to reduce the quantity of bread solely to reduce sodium. Hence, efforts need to be made to provide meals with lower sodium content whist still providing acceptable taste. Soup contributed to a largeportionofthesodiuminthetexturemodifiedmenu,sourcingreducedand low sodium soups is highly recommended. Both the standard texture menuandthetexturemodifiedmenuFellwithintheAcceptableMacronutrientDistribution Ranges (AMDRs) for percentage of energy from protein, fats and carbohydrates.
*Note: Adjusted Ideal Body Weight (IBW) = [(Actual Body Weight – IBW) x 0.25] + IBW IBW = weight at BMI 25

Page 57
APENDIX 3 Example menu for different cycle lengths. Seven day menu cycle Total 35 hot choices – three lunch, two dinner
7 day menu cycle (two lunch items apear on the menu – an alternative item is available if requested) (repeats)
MEAL – WEEK 1 MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY SATURDAY SUNDAY
Lunch – full Roast Beef Pork in Plum Sauce
Chicken Rissoles Roast Lamb Crumbed Fish Lentil Burger Roast Chicken
Lunch – soft Steamedfishinlemon sauce
Lamb rissoles Macaroni Cheese Satay Chicken Fettuccini Carbonara
Chicken Cacciatore
Sweet & sour pork
Lunch – Salad Ham Roast Beef Salmon Meat Loaf Roast Chicken Ham Roast Lamb
Lunch – alt Chilli Beans Vegetarian Quiche Chefs Special Tofu & vege stir fry Pumpkin & chick pea curry
Chefs Special Plain Omelette
Sandwicht Chicken & Hommos
Ham & cheese Roast beef Salmon & cream cheese
Ham & Cheese Roast Lamb Corn Beef & pickle
Lunch dessert Apricots and custard
Pineaple Sponge & custard
Peaches and custard
FruitTrifle Chocolate Cake & Ice-cream
Diced peaches & pears and custard
Aple Pie and custard
Tea - full Lamb (Kofta) Meatballs
Silverside & white sauce
Roast Pork Braised Steak & onions
Chicken in apricot sauce
Lamb Korma Beef Pie
Tea – soft Chickenfingers Salmon Bake Curried beef Steamed pork dumplings
Veal & tomato casserole
Spaghetti Bolognaise
Fish cakes
Tea - salad Egg & Cheese Falafel Chicken Caesar 4 bean salad Roast Pork Corn Beef Mexican Bean
Sandwich Assorted Assorted Egg & lettuce Assorted Falafel & salad swich/wrap
Cheese Assorted
Tea – dessert 1 Lemon Cheesecake (HP)
& ice-cream
Baked Egg Custard & stewed aple
Banana Cake & Custard
Creamed Rice (HP) & peaches
Aple crumble & custard
Crème Caramel & Banana
Bread & Butter pudding (HP) &
peaches
Tea –dessert 2 Chocolate Mousse & Pears
Apricots & Ice-cream
Vanilla slice & ice -cream
Fruit Salad & Ice cream
Diced peaches & pears and custard
Strawberry Mousse & diced
aple
Fruit Salad & ice-cream

Page 58
14 day menu cycle (two lunch, two dinner) (repeats)
MEAL – WEEK 1 MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY SATURDAY SUNDAY
Lunch – full Roast Beef Pork in Plum Sauce
Chicken Rissoles Roast Lamb Crumbed Fish Lentil Burger Roast Chicken
Lunch – Soft Fettuccini Carbonara
Lamb rissoles Macaroni Cheese Satay Chicken Steamedfishinlemon sauce
Chicken Cacciatore
Sweet & sour pork
Lunch – Salad Ham 4 bean salad Roast Lamb Salmon Roast Chicken Meat Loaf Roast Beef
Lunch Sandwich Egg & cheese Chicken & Hommos
Roast beef Ham & cheese Roast Lamb Salmon & cream cheese
Roast Beef
Lunch dessert Apricots and custard
Pineaple Sponge & custard
Peaches and custard
FruitTrifle Chocolate Cake & Ice-cream
Diced peaches & pears and custard
Aple Pie and custard
Tea - full Lamb (Kofta) Meatballs
Peaches and custard
FruitTrifle Braised Steak & onions
Chicken in apricot sauce
Crumbedfish Beef Sausages
Tea – soft Plain Omelette Salmon Bake Curried beef Pumpkin & chick pea curry
Beef in red wine casserole
Spaghetti Bolognaise
Lentil & Potato Cottage Pie
Tea Sandwich Assorted Assorted Egg & lettuce Assorted Falafel & salad swich/wrap
Egg & lettuce Assorted
Tea dessert Lemon Cheesecake (HP)
& ice-cream
Baked Egg Custard & stewed aple
Banana Cake & Custard
Creamed Rice (HP) & peaches
Aple crumble & custard
Crème Caramel & Banana
Bread & Butter pudding (HP)
& peaches

Page 59
14 day menu cycle (repeat)
MEAL – WEEK 2 MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY SATURDAY SUNDAY
Lunch – full Roast Lamb Meat Balls & gravy Lamb Korma Roast Beef Chicken Pie Pork Sausages Vegetarian Lasagne
Lunch – soft Savoury Mince Salmon Bake Cottage Pie Steamed Fish in lemon sauce
Macaroni Cheese Beef Stroganoff
Lunch – salad Turkey Egg & Cheese Chicken Caesar Ham Roast Pork Mexican Bean Corn Beef
Lunch Sandwich Corn Beef & pickle Roast Pork & aple sauce
Falafel & salad swich/wrap
Cheese & Egg Roast beef Chicken & Hommos
Salmon & cream cheese
Lunch dessert Chocolate Mousse & Pears
Apricots & Ice-cream
Vanilla slice & ice -cream
Fruit Salad & Ice cream
Diced peaches & pears and custard
Strawberry Mousse & diced
aple
Fruit Salad &
ice-cream
Tea – full Beef Pie Chicken in apricot sauce
Silverside & White Sauce
Roast Chicken BBQ Pork ribs Crumbed Fish Chicken Rissoles
Tea – soft Vegetable Quiche Beef casserole Pumpkin & chick pea curry
Lamb & tomato casserole
Beef curry Lentil & Potato Cottage Pie
Spaghetti Bolognaise
Tea Sandwich Assorted Assorted Assorted Assorted Egg & Lettuce Assorted Cheese & tomato
Tea dessert FruitTrifle Lemon Cheesecake (HP) & ice-cream
Pineaple Sponge & custard
Bread & Butter pudding (HP) &
peaches
Chocolate Cake & Ice-cream
Creamed Rice (HP) & peaches
Crème Caramel & Banana

Page 60
21 day menu cycle (one lunch, two dinner or two lunch, one dinner – if full option on lunch or dinner then soft sandwiches and soup are an option for the soft diets) (repeats)
MEAL – WEEK 1 MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY SATURDAY SUNDAY
Lunch - full/soft Cottage Pie Salmon Bake Savoury Mince Cheese Omelette Beef Stroganoff Lentil & potato pie Spaghetti Bolognaise
Lunch – Salad Ham Roast Beef 4 bean salad Roast Chicken Salmon Meat Loaf Roast Lamb
Sandwich Chicken & Hommos
Ham & cheese Salmon & cream cheese
Roast beef Ham & Cheese Roast Lamb Corn Beef & pickle
Lunch dessert Chocolate Mousse & Pears
Apricots & Ice-cream
Vanilla slice & ice -cream
Fruit Salad & Ice cream
Diced peaches & pears and custard
Strawberry Mousse & diced
aple
Fruit Salad & ice-cream
Tea - full Silverside & white sauce
Chicken in apricot sauce
Lamb (Kofta) Meatballs
Braised Steak & onions
Roast Pork Crumbed lamb cutlets
BBQ pork ribs
Tea – soft Vegetable Quiche Lamb rissoles Macaroni Cheese Satay Chicken Fish cakes Chicken Cacciatore
Meat Loaf & gravy
Sandwich Assorted Assorted Assorted Assorted Assorted Assorted Assorted
Tea dessert Lemon Cheesecake (HP)
& ice-cream
Baked Egg Custard & stewed
aple
Aple crumble & custard
Creamed Rice (HP) & peaches
Banana Cake & Custard
Crème Caramel & Banana
Bread & Butter pudding (HP)
& peaches

Page 61
21 day menu cycle (repeat)
MEAL – WEEK 2 MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY SATURDAY SUNDAY
Lunch - full/soft Steamed Fish in lemon sauce
Irish Stew Beef Casserole Chicken Rissoles Savoury omelette Sweet & sour pork Cottage Pie
Lunch – Salad Turkey Egg & Cheese Ham 4 bean salad Roast Pork Corn Beef Chicken Caesar
Sandwich Roast Lamb Chicken & Hommos Salmon & cream cheese
Ham & Cheese Roast beef Egg & Cheese Corn Beef & pickle
Lunch dessert Apricots and custard
Pineaple Sponge & custard
Peaches and custard
FruitTrifle Chocolate Cake & Ice-cream
Diced peaches & pears and custard
Aple Pie and custard
Tea - full Roast Beef Pork in plum sauce Quiche Lorraine Roast Lamb Lentil Burger Crumbed Fish Roast Chicken
Tea – soft Plain Omelette Curried beef Pumpkin & chick pea curry
Salmon Bake Veal & tomato casserole
Spaghetti Bolognaise
Macaroni Cheese
Sandwich Assorted Assorted Assorted Assorted Assorted Assorted Assorted
Tea dessert Lemon Cheesecake (HP)
& ice-cream
Aple crumble & custard
Crème Caramel & Banana
Bread & Butter pudding (HP)
& peaches
Baked Egg Custard & stewed aple
Banana Cake & Custard
Creamed Rice (HP) & peaches
MEAL – WEEK 3 MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY SATURDAY SUNDAY
Lunch - full/soft Beef stroganoff Chicken Rissoles Lamb rissoles Seafood Mornay Savoury Mince Irish Stew Roast Chicken
Lunch – Salad Egg & Cheese Turkey Mexican Bean Ham Roast Pork Chicken Corn Beef
Sandwich Chicken & Hommos
Ham & cheese Roast beef Salmon & cream cheese
Roast Chicken Ham & Cheese Egg & cheese
Lunch dessert Diced peaches & pears and custard
Strawberry Mousse & diced aple
Fruit Salad & ice-cream
Peaches and custard
Pineaple Sponge & custard
Chocolate Cake & Ice-cream
FruitTrifle
Tea - full Roast Lamb Pork Sausages Chicken Pie Roast Beef Chicken in Apricot Sauce
Meat Balls & gravy Lamb Korma
Tea – soft Vegetable Quiche Steamed Fish in lemon sauce
Macaroni Cheese Butter Chicken Lentil & potato pie Fettuccini Carbonara
MexicanChilliBeans
Sandwich Assorted Assorted Assorted Assorted Assorted Assorted Assorted
Tea dessert Baked Egg Custard &
stewed aple
Lemon Cheesecake (HP) & ice-cream
Banana Cake & Custard
Creamed Rice (HP) & peaches
Aple crumble & custard
Crème Caramel & Banana
Bread & Butter pudding (HP)
& peaches

Page 62
14 day Smooth puree and Minced and moist (repeats)
MEAL – WEEK 1 MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY SATURDAY SUNDAY
Lunch - Minced & moist
Cottage Pie & Gravy
Salmon Bake & white sauce
Savoury Mince & gravy
Cheese Omelette & tomato sauce
Beef Stroganoff & gravy
Lentil & potato pie & tomato sauce
Minced Spaghetti Bolognaise & tomato sauce
Lunch – Smooth puree
Cottage Pie Salmon Bake Savoury Mince Cheese Quiche (no base)
Beef Stroganoff Lentil & potato pie Spaghetti Bolognaise
Lunch dessert – Minced & moist
Chocolate Mousse & Diced
Pears
Diced Apricots & Ice-cream
Vanilla slice (custard only) & ice –cream/
caramel custard
Diced Fruit Salad & Ice cream/
yoghurt
Diced peaches & pears and custard
Strawberry Mousse & diced
aple
Coconut & Pineaple Pudding
Lunch dessert – smooth puree
Chocolate Mousse & SP
Pears
SP Apricots & Ice-cream/Custard
Vanilla slice (custard only) & ice –cream/
caramel custard
SP Fruit Salad & Ice cream/
yoghurt
SP peaches & pears and custard
Strawberry Mousse & SP aple
Coconut & Pineaple pudding
Tea - Minced & moist
Minced Chicken in apricot sauce
Minced Silverside & white sauce
Lamb (Kofta) Meatballs & mint
yoghurt/ gravy
Minced Braised Steak & onions
Minced Steamed fish&lemon
sauce
Minced Lamb & mint gravy
Minced BBQ pork & BBQ sauce
Tea – Smooth puree
SP chicken in apricot sauce
SP silverside & white sauce
SP lamb & mint yoghurt sauce
SP Braised Steak & onion gravy
SPSteamedfish&lemon sauce
SP Lamb & mint gravy
SP BBQ pork & BBQ sauce
Tea dessert -Minced & moist
Lemon Cheesecake
(HP) no base & ice-cream/lemon
sauce
Baked Egg Custard & diced aple
Aple crumble & custard
Creamed Rice (HP) & diced peaches
Banana Cake & Custard
Crème Caramel custard & mashed Banana & caramel sauce or custard
Bread & Butter pudding (HP) & diced peaches
Tea dessert – smooth puree
Lemon Cheesecake
(HP) no base & ice-cream/ lemon
sauce
Baked Egg Custard & SP aple
SP Aple crumble & custard
SP Creamed Rice (HP) & SP peaches
SP Banana Pudding & Custard
Crème Caramel custard & SP
Banana & caramel sauce or custard
SP Bread & Butter pudding
(HP) & SP peaches

Page 63
MEAL – WEEK 2 MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY SATURDAY SUNDAY
Lunch - Minced & moist
Vegetable Quiche no base & cheese
sauce
Minced Roast Beef & gravy
M& M Macaroni Cheese
Minced Chicken & satay sauce
Fish cakes & white sauce
Minced Chicken Cacciatore
Meat Loaf & gravy
Lunch – Smooth puree
Savoury Baked egg custard & cheese sauce
SP Roast Beef & gravy
SP macaroni cheese
SP chicken & satay sauce
SPfishcakes&white sauce
SP chicken cacciatore
SP Meat Loaf & gravy
Lunch dessert – Minced & moist
Minced Aple Pie & custard
Pineaple Mousse & diced aple
Crème Caramel custard &
caramel sauce or custard
Diced Fruit Salad & ice-cream/
custard
Diced Pineaple Sponge & custard
Chocolate Cake & Ice-cream/ vanilla
custard
FruitTrifle(madewith diced fruit)
& ice-cream/ custard
Lunch dessert – smooth puree
Puree Aple Pie & custard
Pineaple Mousse & diced aple
Crème Caramel custard &
caramel sauce or custard
SP Fruit Salad & ice-cream/ custard
SP Pineaple Sponge & custard
SP Chocolate Pudding & Ice-cream/ vanilla
custard
SPFruitTrifleinlayers & ice-
cream/ custard
Tea - Minced & moist
Minced Lamb Korma
Chicken rissoles & gravy
Minced Beef Casserole
Minced Roast Pork & gravy & aple
sauce
Minced Irish Stew Minced curried beef & gravy
Minced Sweet & sour pork
Tea – Smooth puree
SP Lamb Korma SP Chicken rissoles & gravy
SP Beef Casserole SP Roast Pork & gravy & aple sauce
SP Irish Stew SP Curried Beef & gravy
SP Sweet & sour pork
Tea dessert -Minced & moist
Baked Egg Custard & diced
aple
Cheesecake (HP) Base only & ice-
cream/strawberry sauce
Apricot crumble & custard
Bread & Butter pudding (HP) & diced peaches
Creamed Rice (HP) & diced peaches
Vanilla slice (custard only) & ice –cream/
caramel custard
Berry & aple crumble &
custard
Tea dessert – smooth puree
Baked Egg Custard &
SP aple
Cheesecake (HP) Base only & ice-
cream/strawberry sauce
SP Apricot crumble &
custard
SP Bread & Butter pudding (HP) & SP
peaches
SP Creamed Rice (HP) & SP peaches
Vanilla slice (custard only) & ice –cream/
caramel custard
SP berry & aple crumble
& custard
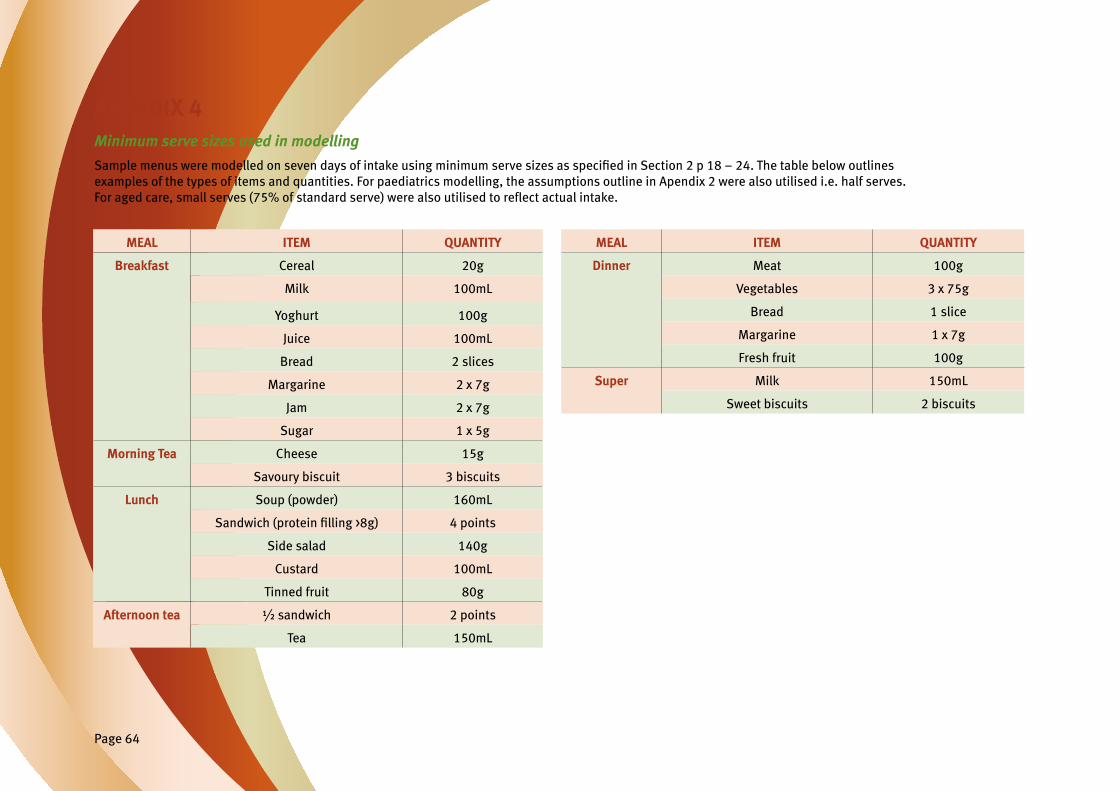
Page 64
APENDIX 4 Minimum serve sizes used in modelling
SamplemenusweremodelledonsevendaysofintakeusingminimumservesizesasspecifiedinSection2p18–24.Thetablebelowoutlines examples of the types of items and quantities. For paediatrics modelling, the assumptions outline in Apendix 2 were also utilised i.e. half serves. Foragedcare,smallserves(75%ofstandardserve)werealsoutilisedtoreflectactualintake.
MEAL ITEM QUANTITY
Breakfast Cereal 20g
Milk 100mL
Yoghurt 100g
Juice 100mL
Bread 2 slices
Margarine 2 x 7g
Jam 2 x 7g
Sugar 1 x 5g
Morning Tea Cheese 15g
Savoury biscuit 3 biscuits
Lunch Soup (powder) 160mL
Sandwich(proteinfilling>8g) 4 points
Side salad 140g
Custard 100mL
Tinned fruit 80g
Afternoon tea ½ sandwich 2 points
Tea 150mL
MEAL ITEM QUANTITY
Dinner Meat 100g
Vegetables 3 x 75g
Bread 1 slice
Margarine 1 x 7g
Fresh fruit 100g
Super Milk 150mL
Sweet biscuits 2 biscuits
