quality programs: hurdles and milestones for health systems and their employed physicians
TRANSCRIPT
Page 0December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Quality Programs:
Hurdles and Milestones for
Health Systems and Their
Employed Physicians
2014 Georgia HFMA Financial Executives Meeting
December 12, 2014

Page 1December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Quality Program Initiatives
Page 2December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Quality Programs in the News
MGMA Physician Practice Assessment Study respondents represented
48,000 physician practices nationwide and disclosed the following regarding
Medicare Quality Reporting Programs:
• 93% reported a negative or significant negative effect on support staff
time.
• 84% reported a negative or significant negative effect on practice
efficiency.
• 85% reported a negative or significant negative effect on clinician
morale.
• Most concerning, 84% of respondents do not believe these programs
enhance their physicians' abilities to provide high quality patient care.
http://www.mgma.com/government-affairs/advocacy/learn/legislative-and-executive-advocacy-response-network-(learn)-research-studies/mgma-
physician-practice-assessment-medicare-quality-reporting-programs-research-results
Page 3December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Quality Programs in the News
Advisory Board headline – November 18, 2014:
Former hospital CFO faces five years in prison over EHR fraud
• The former CFO of the now-shuttered Shelby Regional Medical
Center in Texas has pleaded guilty to falsely attesting to the meaningful
use program.
• Under the 2009 federal economic stimulus package, healthcare
providers who demonstrate meaningful use of certified electronic health
record (EHR) systems can qualify for Medicaid and Medicare incentive
payments.
• 94% of CFOs at struggling hospitals blame botched IT projects .
http://www.advisory.com/daily-briefing/2014/11/18/former-hospital-cfo-faces-five-years-in-prison-over-ehr-
fraud?WT.mc_id=Email|Daily+Briefing+Headline|DBA|DB|Nov-18-2018|||||&elq_cid=1400065
Page 4December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Focus Areas
• Quality Program Staffing
• Acquisition Process
• Systems
• Training
• Monitoring, Reporting, Audits
• Next Levels
Page 5December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Staffing
• Hospital quality
program
implementation
staffing
– Physician (CMO or
CMIO) leadership
– Nurse leadership
– Quality department
• Employed physician
group quality program
implementation
staffing
– Operational leadership
– Physician leadership
– Quality program focus
by specialty
Information systems/technology department staff
Page 6December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Staffing cont.
• Competition for staff resources drives financial
leadership to choices based on:
– Comparative size of the resulting incentive or
penalty dollars at risk.
– Largest potential benefit for staffing resources
invested.
– Specialized expertise requirements may lead to
outsourced staffing choices.
Page 7December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
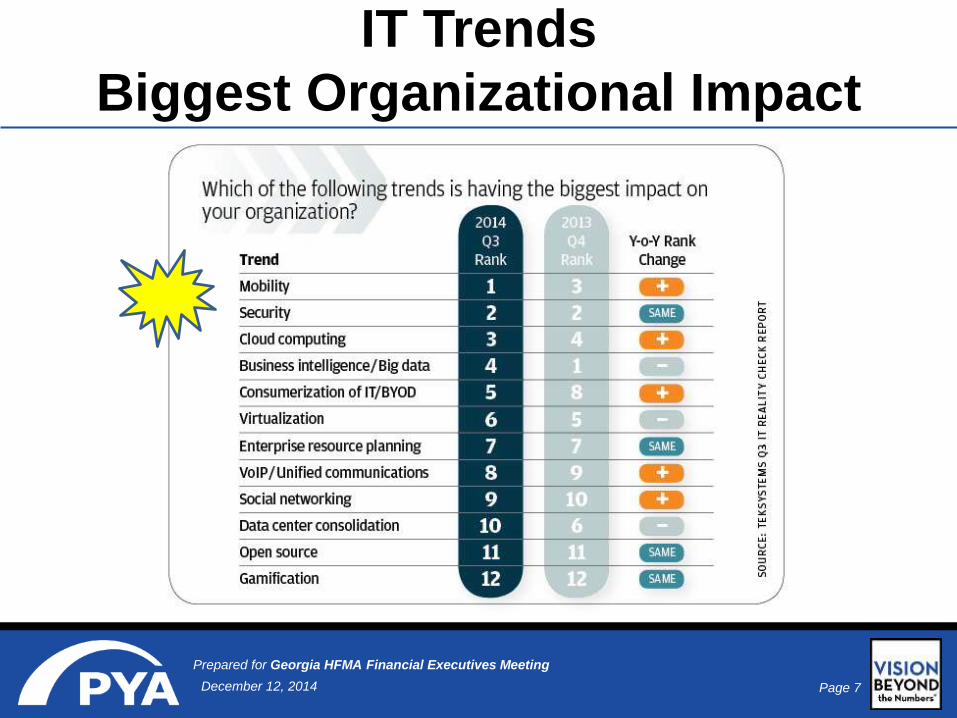
IT Trends
Biggest Organizational Impact
Page 8December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
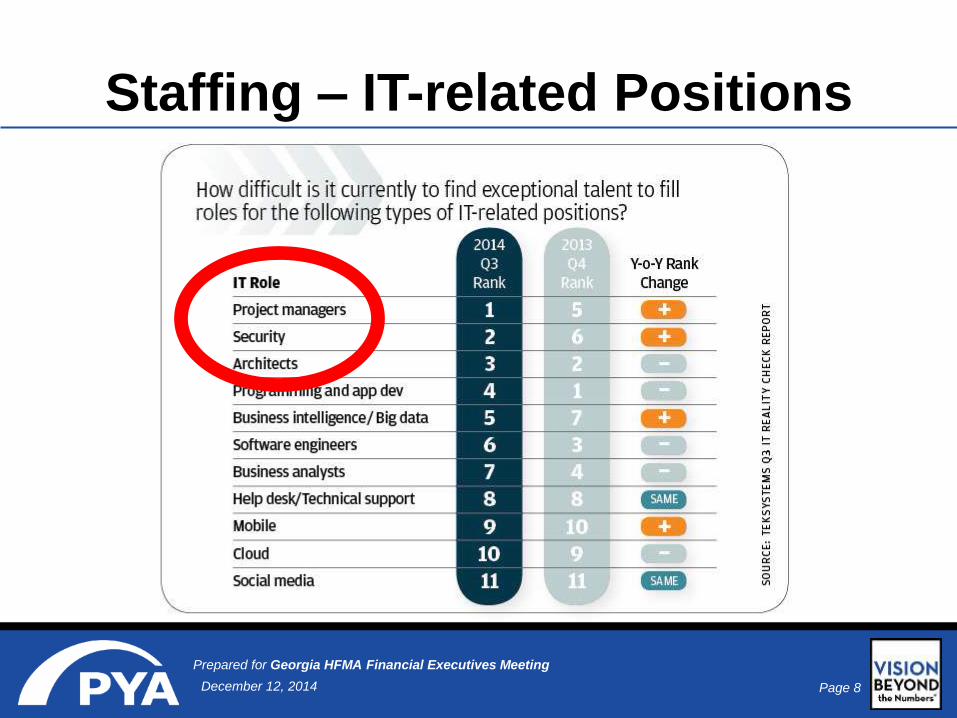
Staffing – IT-related Positions
Page 9December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
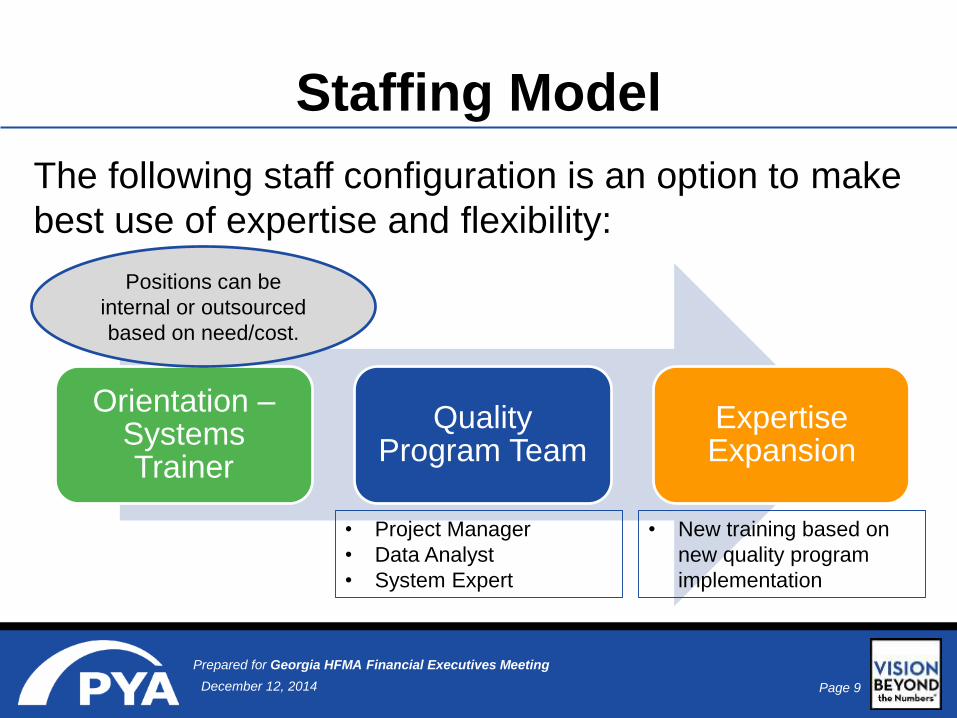
Staffing Model
The following staff configuration is an option to make
best use of expertise and flexibility:
Orientation –Systems Trainer
Quality Program Team
Expertise Expansion
• Project Manager
• Data Analyst
• System Expert
• New training based on
new quality program
implementation
Positions can be
internal or outsourced
based on need/cost.

Page 10December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Acquisitions
Develop EHR strategy for physician practice
acquisitions:
1) List EHR software products you are willing/able to
maintain.
2) Research likely longevity of software product by
vendor.
3) Consider interfaces already in place.
4) Consider software staffing expertise in place.
Page 11December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
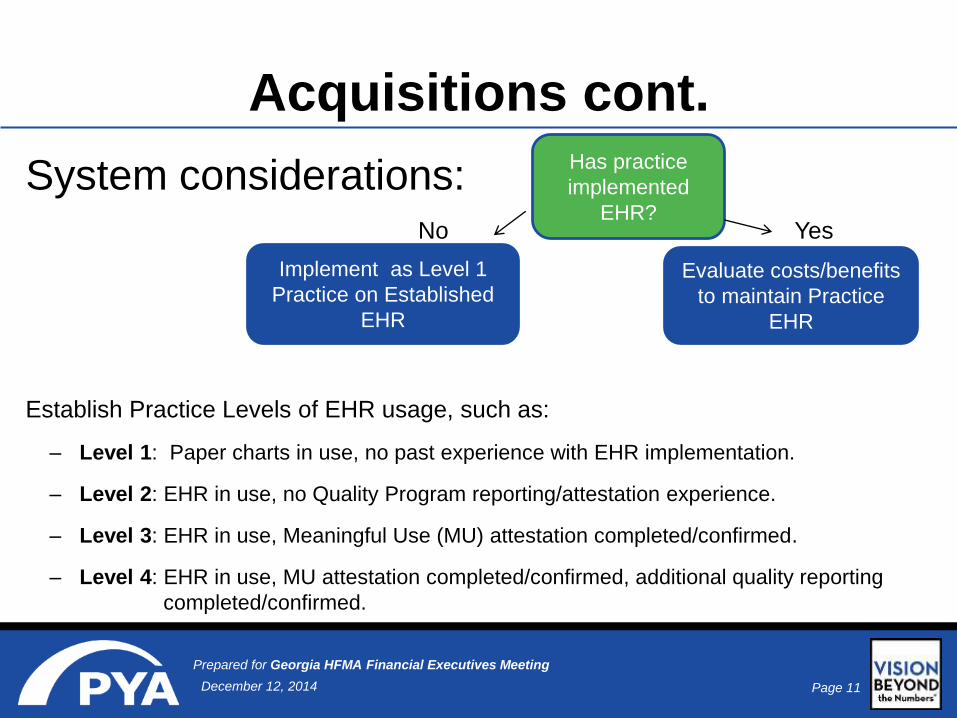
Acquisitions cont.
System considerations:No Yes
Establish Practice Levels of EHR usage, such as:
– Level 1: Paper charts in use, no past experience with EHR implementation.
– Level 2: EHR in use, no Quality Program reporting/attestation experience.
– Level 3: EHR in use, Meaningful Use (MU) attestation completed/confirmed.
– Level 4: EHR in use, MU attestation completed/confirmed, additional quality reporting
completed/confirmed.
Has practice
implemented
EHR?
Implement as Level 1
Practice on Established
EHR
Evaluate costs/benefits
to maintain Practice
EHR

Page 12December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
System(s)
Based on recent client projects and interviews, the following
summarizes the wide range of system(s) experience for health
systems and their employed physician groups:
Single
system
solution –
EHR and
Billing
Hospital
system –
EHR and
Billing
Employed
Physician
Practices
system - EHR
and Billing
Hospital
system –
EHR and
Billing
Employed
Physician
Practices
system V2 -
EHR and
Billing Employed
Physician
Practices
system V1 -
EHR and
Billing
Employed
Physician
Practices
system V1 –
Billing and
paper charts

Page 13December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
System(s)
Necessary to improve collection, storage, and management of
electronic health information
Tracking improvement in processes and patient outcomes
Better communication among providers
Patient accessibility to health information
Patient self-management tools
E-Prescribing

Page 14December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Training
• The EHR system training team needs to be
prepared and have multiple training delivery
methods for:
1) Individual practice new hires at all staffing levels.
2) Acquired physician groups.
3) New workflow processes in response to new
quality program participation.
Page 15December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Monitoring/Reporting
• Use the system-generated Meaningful Use
monitoring report by eligible professional
(EP).
• If Quality Program team is not staffed
sufficiently for monitoring, evaluate an
outsourced staff solution to monitor, report
deficiencies, and develop recommended
workflow changes to achieve MU goals.
Page 16December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Auditing
• Quality Program Staff need to be prepared for
audits relating to incentive program
participation.
• Confirm all documentation is completed and
accessible.

Page 17December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Clinical Quality Measures
2014 for Eligible Professionals
http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/2014eCQMs_EligibleProfessionalsTable_July2014.pdf
Example: one page of complete document:

Page 18December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Aligning Multiple Quality
Program Reporting Options
Page 19December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Next Levels
Page 20December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Next Levels
• Moving from EHR usage as the ‘end’ to the means
to an end.
• EHR usage, staff skills, and tools for proactive
patient care can lead to new reimbursement
opportunities.
EHR
Implementation
EHR usage Staff training Proactive patient care

Page 21December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Next Level:
Iora Health Example
Hospital
Admissions –
40%
Emergency
Visits
– 50%
Net total
healthcare
spending
– 12 to 15%
“A Prescription for Primary Care,” Leadership Fall 2014: www.hfma.org/leadership, November 4, 2014.
• Staffing model
• System use
• Proactive
patient
communication

Page 22December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Next Level:
Patient-Centered Medical Home
• Patient-Centered Medical Home (PCMH)
– A model of primary care that improves clinical
quality, lowers costs, and improves patient
satisfaction through care coordination.
– First program through NCQA started in 2003.
Standards have evolved over the years to be
consistent with Meaningful Use and other
meaningful quality metrics.

Page 23December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
PCMH Facts
• PCMH 2011 and 2014 are closely aligned with Meaningful
Use reporting requirements.
• Practices are not required to have a certified EMR (though a
requirement for chronic care management).
• Each practice location is certified versus each clinician.
Clinicians are certified by way of their practice location.
• Practices must report on 12 months of data. If the practice
EMR has not been in place for 12 months, NCQA will accept
three months of data.
• Calendar year reporting is not required.
Page 24December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Next Level: Transitional
Care Management (TCM)
Overview
• Providers are reimbursed for active follow-up with patients following
discharge from an inpatient facility.
• One face-to-face visit with billing provider must occur within 7 or 14
days (depending on TCM CPT code billed).
• The practice must make contact with the patient within two days of
discharge, educate the patient on their diagnoses, and provide
resources to ensure discharge orders are fulfilled. These services
must be furnished by qualified clinical staff.
• Only one provider may bill for these services.
• Effective transitional care management should help facilitate a
reduction in hospital readmissions as well as improve patient
satisfaction.
Page 25December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Practice Plan for
Implementation – TCM
• Assign staff to review hospital admission log on
a daily basis
• Inform nurse/provider of patient admission
• Specify timeline for follow-up after notification
(by end of day, next day, within two days, etc.)
• Schedule and conduct face-to-face visit
• Evaluate community and referral resources
• Train staff on documentation
• Spot review discharge report and
documentation of follow-up on a monthly basis
for compliance
Page 26December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
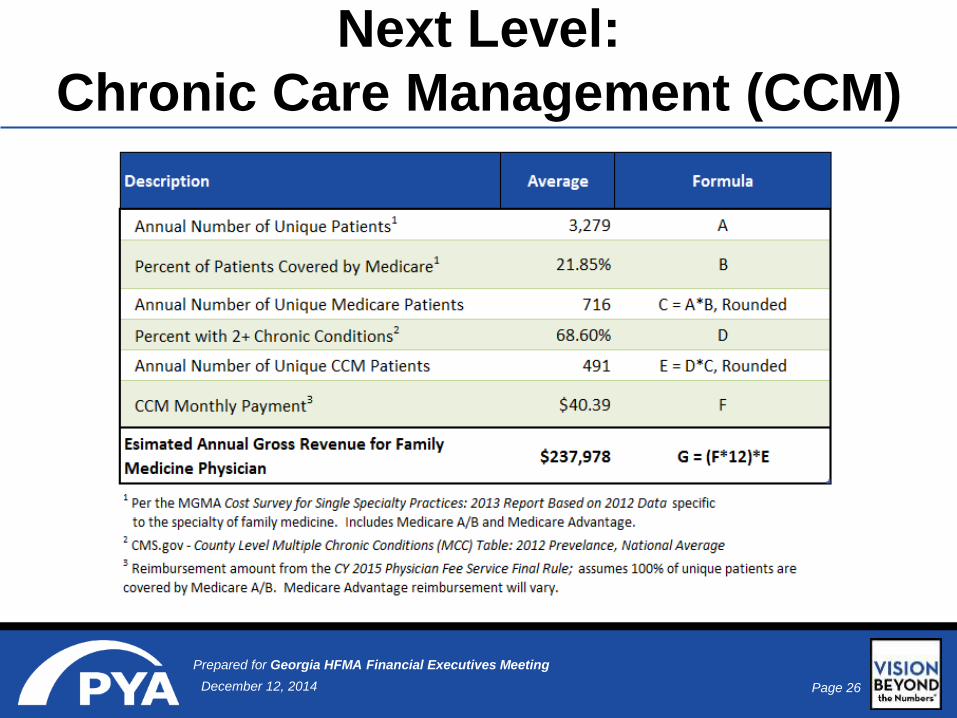
Next Level:
Chronic Care Management (CCM)
Page 27December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
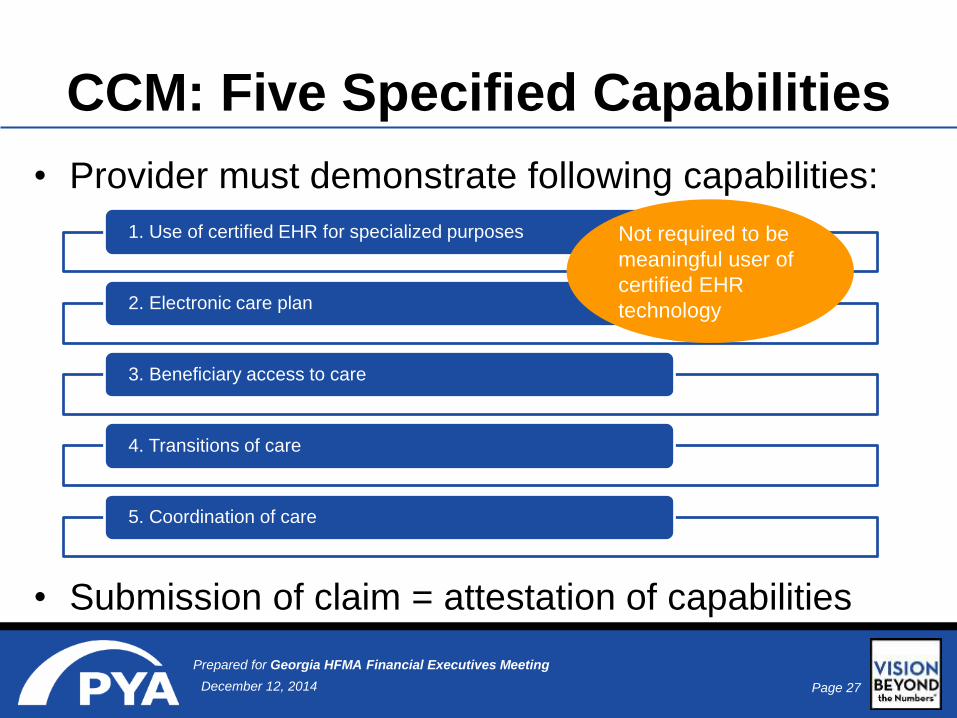
CCM: Five Specified Capabilities
• Provider must demonstrate following capabilities:
• Submission of claim = attestation of capabilities
1. Use of certified EHR for specialized purposes
2. Electronic care plan
3. Beneficiary access to care
4. Transitions of care
5. Coordination of care
Not required to be
meaningful user of
certified EHR
technology
Page 28December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
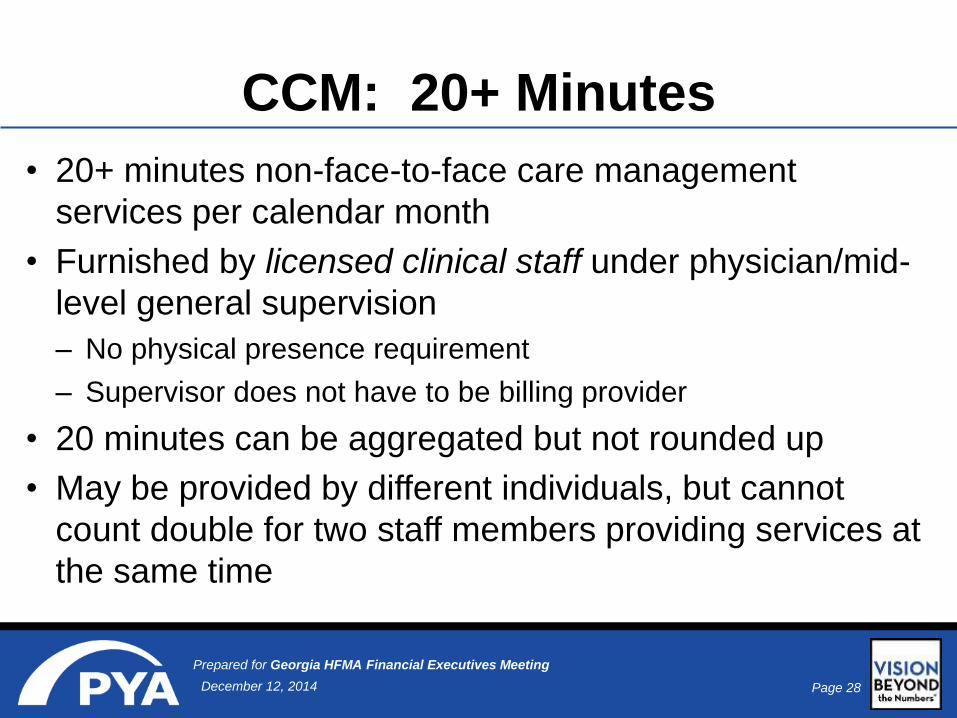
CCM: 20+ Minutes
• 20+ minutes non-face-to-face care management
services per calendar month
• Furnished by licensed clinical staff under physician/mid-
level general supervision
– No physical presence requirement
– Supervisor does not have to be billing provider
• 20 minutes can be aggregated but not rounded up
• May be provided by different individuals, but cannot
count double for two staff members providing services at
the same time
Page 29December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
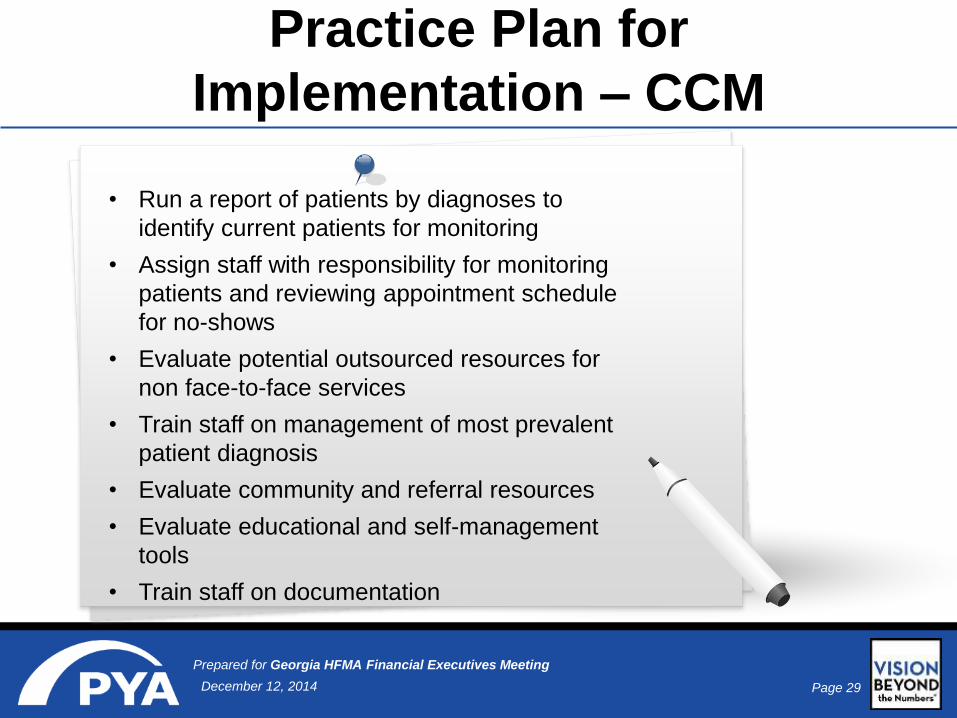
Practice Plan for
Implementation – CCM
• Run a report of patients by diagnoses to
identify current patients for monitoring
• Assign staff with responsibility for monitoring
patients and reviewing appointment schedule
for no-shows
• Evaluate potential outsourced resources for
non face-to-face services
• Train staff on management of most prevalent
patient diagnosis
• Evaluate community and referral resources
• Evaluate educational and self-management
tools
• Train staff on documentation
Page 30December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
TCM/CCM: Staffing Considerations
May require an
increase in
staff to
improve
workflow
Diverse
backgrounds
to
appropriately
address
cultural and
linguistic
needs of
patient
population
May require
staff with more
training
(LPN, RN) -
especially in
the clinical
area to
effectively
assist the
patients
Training in
evidence-
based
approaches to
patient self-
management,
population
management,
and patient
communication
Effective
management
of staff

Page 31December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
TCM/CCM: Policy Implications
Practice should consider policies for:
• Structured communication between the clinician and other care
team members
• Educating patients on illnesses and treatment options
• Identifying patients with certain conditions and monitoring
improvement and/or compliance with recommended treatment
• Follow-up to include newborn hearing tests, lab results, imaging
results, and referrals
• Notifying families of normal and abnormal results
• Monitoring scheduled visits and tracking no shows

Page 32December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Summary
Health systems/hospitals have opportunities to
plan for quality program hurdles in staffing,
policies, systems deployed, and training.
Once the milestones of quality program
requirements are met, additional opportunities
for ‘meaningfully’ using the EHR investment
can lead to improved care and reimbursement.
Page 33December 12, 2014
Prepared for Georgia HFMA Financial Executives Meeting
Thank you!
Linda ClenDening, FACMPE
Consulting Manager
Pershing Yoakley & Associates, P.C.
(865) 684-2735
www.pyapc.com
Co-Presenter:
Sondra McGinnis, RN, FACHE
Erlanger Health System