quality assurance program reporting process for …ioe481/ioe481_past_reports/w9002.pdf · a....
TRANSCRIPT
Reporting Process for Hospitals’Quality Assurance Program
Final Report
By:
Kent Feigner
David Karp
Victoria Vogel
Management Systems Department
3 May 1990
Table of Contents
Executive Summary 1
Introduction 3
H Approach & Findings 4
Recommendations 6
Action Plan 1 3
AppendicesI’
A. Quality Assurance Organization and Information Flow
B. Draft Standard Initial and Follow-Up Report Formats
C Recommended Quality Assurance Reporting Groups
D. Quality Assurance Scheduling Process
E Quality Assurance Database System Specifications
F. Report Codification and Data Entry Process
G Checklists for Tracking/Trending/and Coding Initial andFollow-Up Reports
Ii Oral Presentation Slides

EXECUTIVE SUMMARY
The University of Michigan Medical Center implements a QualityAssurance Program, under the guidance of the Hospital Quality AssuranceCommittee (HQAC), to enhance patient care through the continualassessment of care and discoveries of opportunities for improvement. Aspart of the continual assessment, the program requires HQAC to collectquarterly and/or annual reports from approximately 75departments/services/committees and then summarize the reports in onequarterly hospital-wide report for various governing bodies. Unfortunately,HQAC’s ability to process all the information received is hampered by anumber of factors. The Management Systems project team analyzed thesefactors and made various recommendations to increase the informationprocessing ability of the Quality Assurance Program.
The team discovered that the major factors hindering HQAC were thenumber of reports submitted, length and completeness of the submittedreports, unmanageable scheduling of report due dates, and theineffectiveness of the quality assurance database system.
Under the current system, more reports were submitted to HQAC thanwere necessary. Since all submitted reports were being reviewed,unnecessary reports simply reduced the amount of staff time available forother jobs. The system was also extremely labor intensive due to thevarying lengths of reports. Some of the extremely lengthy quarterly reportswere submitted in three inch binders, requiring hours of staff time toreview and extract the important information. There were also a largenumber of reports that lacked some of the important information. As aconsequence, in 1989; of the 500 submitted reports, only approximately 25were useable for HQAC in preparing- its quarterly report summarizinghospital quality assurance efforts.
The scheduling of report submission dates led to an unmanageableflow of reports to HQAC on the four quarterly due dates, even though only20 percent of the expected reports were submitted. With all the reportsarriving during one day, timely review and feedback was impossible. Thequality assurance database system, into which report data was entered, alsoseemed inadequate for HQAC needs. The primary objection was that thesystem is not user-friendly, thereby preventing necessary tasks likeanalyzing and retrieving stored data. This also made the system ineffectiveat tracking the status, trends, and commonalties of the reports. All of thesefactors offer significant opportunities for improvement of the informationprocessing ability for the Quality Assurance Program.
1

The five recommended improvements are the following:
1. Collect only those reports that are necessaryThis step will cut the number of reports submitted peryear to approximately 360, a 40% decrease over 1989levels, leading to a corresponding reduction in staff timeto review the reports.
2. Finalize and implement a standardized report formatSuch a form would greatly reduce the amount of timerequired to interpret the report, ensure completeness ofthe report by specifying exactly what information isrequired, and make it easier to track report status andcontent.
3. Implement a schedule with a manageable, uniform report flowA recommended schedule is shown in Figure 2 of thereport. It provides a flow of reports that would allowaccurate and timely feedback from HQAC to the reportinggroups and from the governing bodies to HQAC regardingits quarterly hospital-wide summary report.
4. Create a new Quality Assurance Database System using ORACLEThis system would be user friendly and have all possibleoptions required by HQAC including the ability to tracktrends and commonalties in the reports. Completesystem specifications are contained in Appendix E.
5. R,eview Staffmg NeedsWith these recommendations, the anticipated averagetime to review and interpret a quarterly report is 20
- minutes, a 300 percent reduction in staff time from thecurrent system. This time savings, coupled with the 40percent reduction in the number of reports, may offer anopportunity for different staffing allocations.
These improvements should made as soon as possible,definitely completed within one year. For as soon as these changesare made, the staff hours required to monitor the program willdecrease, there will be timely and accurate feedback, and the systemwill allow for efficient tracking of the trends and commonaltieswithin the reports.
2
INTRODUCTION
In September 1989, the University of Michigan Hospitalrevised the Quality Assurance Program. The program was designedto enhance patient care through the continuing assessment of careand the promotion of improvements based on the opportunitiesdiscovered by the assessments. The specifications providing theframework for the program are documented in the “Hospitals’ QualityAssurance Program” (September 1989).
As the documentation specifies, program implementation is theresponsibility of the Hospitals’ Quality Assurance Committee (HQAC)with administrative assistance from the Quality Assurance &Information Services Unit of the Medical Information Department. Asketch of the program organization and information flow is providedin Appendix A. As the Appendix shows, there are approximately 75departments, committees, and services that submit various reports toHQAC. These reports can be categorized into four types:
1. Annual Quality Assurance (QA) Plans2. Quarterly QA Reports3 Annual QA Reports4. Follow-Up Reports.
As the administrative support for HQAC, the Quality Assurance& Information Services Unit is responsible for the collection of thereports, the central documentation of the reported patient careactivities, and the creation of HQAC’s quarterly report for reviewand evaluation by the appropriate hospital administration shown inAppendix A. It was the ability to do these activities, the informationprocessing ability of the Quality Assurance Program, that this projectattempted to improve. The goal being to increase the efficiency inmonitoring report status, create efficient and timely feedback andinformation flows, and track trends and commonalties within thereports.
3

• APPROACH & FINDINGS
The project team began by reviewing the Hospitals’ QualityAssurance Program through:
1 Weekly discussions with the client group, 3 members ofHospital Quality Assurance Steenng Committee
Roseanne Whitehouse, Staff Associate Ambulatory CareServices
Ingrid Hemming, Assistant Director, MedicalInformation Services
Linda Creps, Director, Medical Information Services
2. Research of pertinent documents including the Hospitals’Quality Assurance Program, and Medical Staff By-laws.
With this background information, the team visit ed the currentsystem to view the process, flowcharted the system, and collectedrelevant data regarding the reports and staff time. These activitiesled to an understanding of program requirements and the trackingand analysis of QA operations.
J The program requirements are displayed an Appendix A, whichshows the groups that must report and the types and frequency ofreports they submit. Upon discussions with the client group, it wasclear that under the current system more reports were submitted toHQAC then were required or necessary. In 1989, for example, therewere approximately 500 quality assurance reports submitted, fromthe only 20 percent of participants who actually reported. AsAppendixc A shows, however, only approximately 360 reports peryear, from all participants, are actually required and necessary.
Tracking QA operations, through discussions with the clientgroup, also pointed to other opportunities for improvement of the QAProgram’s information processing ability. With the current system,submitted reports often lacked information or contained excessiveamounts of unnecessary information. Once again, 1989 data showsthat roughly 25 of the 500 reports collected were useable by HQAC.Report due dates also frequently were not met, with approximately80 percent of the groups failing to report in 1989. When the dateswere met, the number and size of submitted reports wereunmanageable, making timely review and feedback impossible.
4
Quarterly report sizes averaged from 4 to 22 pages in length, thusrequiring approximately 45 minutes to 2.5 hours to review.
Once reports were received, the Quality Assurance &Information Services unit entered the report into their dBase IIIdatabase. The database was used to store important report dataj butrarely, if ever, was the stored data retrieved or analyzed due to thecomplications involved. This made the database ineffective attracking the status, trends, and commonalties of the reports.
5

RECOMMENDATIONS
To improve the information processing ability, we present fiverecommendations which will result in an implementation of theQuality Assurance Program that is both manageable and efficient forall groups involved. A summary of the recommendations follows:
1. Collect only necessary reports2. Finalize standardized report formats3. Implement a Quality Assurance Scheduling Process4. Utilize a user-friendly database system for data manipulation5. Review staffing requirements given the potential for improvement
COLLECT ONLY NECESSARY REPORTS
The first recommendation is that HQAC collect only thosereports, shown in Appendix A, that are necessary. This change willallow the number of reports received by HQAC to drop byapproximately 40% this year and will account for complete reportingfrom all groups. The difference that will be result can be seen inFigure 1, below.
Estimated Numbs of AllQuality Assce Raposu
fct an Avage Yw
(Based oø 1989-1990 Figures)
Effect of Changes
Figure 1. Changes in the Estimated Number of Reports fromRecommendation 1.
BeforeChanges
600
500
400
300
Changes
100
01 2
6

FINAUZE STANDARDIZED REPORT FORMATS
The second recommendation is that a standardized reportformat be finalized and then implemented. Appendix B shows thecurrent draft version of the recommended standardized form. Thefinalized version should contain blank space to simplify the task offitting responses on the form and to increase the readability of theform once it is filled out. This will probably require a two sidedform. The content of the form, however, should remain as shown inAppendix B, since the information that is asked is precisely thenecessary and sufficient information for HQAC’s purposes.
The time required to interpret and codify the standard reportshould be under 20 minutes, well below the 45 minute to 2.5 hoursthat it currently requires. The benefits that HQAC and the QualityAssurance and Information Services Unit will see as a result of thereport standardization are:
1. Adherence to the Quality Assurance Program2. Complete reporting3. Assignment of responsibility for reports4. Easier tracking of report status and report content5. 300% Time savings in the interpretation of the report.
IMPLEMENT A QUALITY ASSURANCE SCHEDULING PROCESS
The third recommendation is to implement a Quality AssuranceScheduling Process to provide a manageable, uniform flow ofinformatioi to HQAC. Our proposed process, shown in Figure 2 (nextpage), involves seven weeks of report collection, two weeks ofHQAC’s report preparation, and ten weeks for the review of the HQACreport.
Allocating seven weeks to collect reports is based on IngridHemming’s suggestion to have weekly report collection with amaximum of ten reports due per week, which allows timely andaccurate feedback. Additionally, Quality Assurance requirementsmandated keeping all services within a department together andassigning each group a specific week to report. The recommendedbreakdown into groups is shown in Appendix C. By observing theabove constraints, seven groups and therefore seven weeks arerequired.
7

Groupi(9 services)
Group 2(14 services)
Group 3(13 services)
collect reportsGroup 4
(10 servIces) prep. and review UQACreport
Group(S services)
Group 6(10 services)
Group 7(7 services)
Report Prep.
Report Review
1 2 3 4 5 6 7 19
Figure 2. Quality Assurance Activities
The next two weeks of the process are allocated for thepreparation of the HQAC report. This task will involve summarizingthe collected data and then, based on the summary, writing thereport. Once completed, the report is subsequently submitted forreview and feedback, involving revision if necessary. This last partof the process is designed with flexibility for adapting to theschedules of the groups that receive the report and to also allownecessary time for feedback from these groups. The resultingprocess is a nineteen week cycle. To help clarify these results,Appendix D contains a flowchart that diagrams the schedulingprocess from a HQAC and Quality Assurance & Information Servicesperspective.
In order to satisfy the requirements of the Quality AssuranceProgram the reporting process must occur four times a year. Ourrecommended scheduling to fulfill this requirement is shown inFigure 3 (following page). As this figure shows, we recommendbeginning the process at the beginning of February, May, Septemberand November. The May collection process would also include theAnnual Plan and Annual Report collection. Thus, scheduling preventsAugust and late December reporting, periods when it would bedifficult for the groups to satisfy the deadline because of newresidents and/or vacation time. Note that this schedule also places aheavy workload on Quality Assurance & Information Services duringthe months of April, July, October/November, and lateDecember/Januar with the heaviest workload during July.
8

We recommend setting each groups quarterly report due datesusing a spread sheet package like Excel. This will require the user toenter the process starting dates and will then generate the group duedates. Once the initial yearly quality assurance schedule isdetermined, as in Figure 3 for example, report due dates can begenerated.
collect repots
• prep. and review BQACrepoct
V//Z.4
Feb Mar Apr May jun. july Au S.p Oct Nov D.c Jan Feb Mar
MONTH
Figure 3 Recommended Yearly Quality Assurance Schedule
A yearly schedule, such as that in Figure 3, would provide
1. A smooth flow of information to HQAC and Quality AssuranceS Information Services
2. An accountability mechanism for departments, services, andcommittees
3. Continuity of reporting by departments, services, andcommittees
4. Increased awareness of everyone’s role and responsibility
UT[LIZE A USER-FRIENDLY DATABASE SYSTEM FOR DATAMANWULATION
The fourth recommendation regards the database used byQuality Assurance & Information Services to store the data from the
9

submitted reports. In order to develop the ability to track reporttrends and commonalties in a user friendly database system, werecommend using the application “ORACLE” to create a new QualityAssurance Database Management System. The specifications for therecommended system, which were written with suggestions fromIngrid Hemming and Roseanne Whitehouse, are presented inAppendix E. The specifications may be given directly to aprogrammer who could, with minimal time commitments fromoutside sources, create the database system that we recommend.
This database system would have a total of seven options.Depending on the type of access granted a user: Professional, DataEntry Clerk, or Departmental; only some or all of the options wouldbe shown. The list of options, their description, and the type of userthat could use each option is given in Table 1 (following page).
Table 1. Database Options
El NCT IflN
Add, Modify, Delete, orPrint Reports
Set, or View Due DatesView Status of ReportsPrint Upcoming Report
Reminders or Late Notices
Sort, or View Records basedon any field
Add, Modify, or Delete users,user identifications,passwords, or access levels
Add, Modify, or Delete theTracklng/Trending/ andCoding elements
Copy data to storage mechanismsuch as floppy or hard diskdrive
ACCESS LEVELREQUIRED
ProfessionalData Clerk
Any - butdepartmentalcan only view itsown dates andstatus
ProfessionalData Clerk
Professional
Professional
ProfessionalData Clerk
7. Exit Leave System
10
Any
(DTIflM
1. Maintain Reports
CJ 2. Maintain Scheduler
3. Maintain Data Summary
4. MainEain Passwords
5. Maintain Tracker System
6. Back-Up

C
With the database, the recommended process of codifying andentering a report is shown in Appendix F. When the report is givento Quality Assurance & Information Services, it will be date stamped,assigned a report number, interpreted by a professional and thencoded onto a tracking)trending/coding checklist similar to the one inAppendix G. The checklist and the report, the latter is needed forbasic information, will then be given to a data entry clerk who willenter the data onto the database system exactly as it appears on thechecklist and report.
As mentioned earlier, we recommend ORACLE be used to buildthis database system. Several IBM PC compatible databaseapplications were reviewed, including Lotus, dBase III, dBase IV,Paradox, RBase, and ORACLE. The criteria for acceptance was that theapplication be user-friendly, menu-driven, table relational and allowcustom designed help screens. dBase III, which is currently in use,failed to meet all of these criterion and therefore the possibility ofmodifying the current system was rejected. The two databaseapplications that met these criteria were RBase and ORACLE.ORACLE’s ability to roll up on to the mainframe without anyadditional programming far outweighed the additional disk space,approximately 2 Mb, required, since the long term plan is to put theQuality Assurance Database System onto the mainframe. Ifnecessary, because of the disk space required by ORACLE, a 40 Mbhard drive could be purchased for approximately $400 (wholesalecost). With the archiving of the current dBase III database systemand data onto floppy disks, it’s very likely, however, that enoughspace for a new ORACLE system would be freed on the existing harddrive.
The’ database system as specified in Appendix C would allowrecord sorting on a variety of keys to track the trends andcommonalties in the reports, a primary goal of the implementedQuality Assurance Program. Its basic design characteristics wouldalso make the database system both powerful and user-friendly.
REVIEW STAFFING GWEN THE POTENTIAL FOR IMPROVEMENT
The fifth recommendation is to review the staffingrequirements after the database management system is completed.Originally, Medical Information Services required between 45minutes and 2.5 hours to review and interpret a QA quarterly report.
11
With the recommendations in place, the average time needed toreview, interpret and enter a QA quarterly report should be no morethan 20 minutes, an average time reduction of 300 percent perreport. Given the magnitude of reports received by HQAC, this wouldresult in a substantial time savings and consequently, it may beadvisable to allocate staffing differently.
n.
)
12
ACTION PLAN
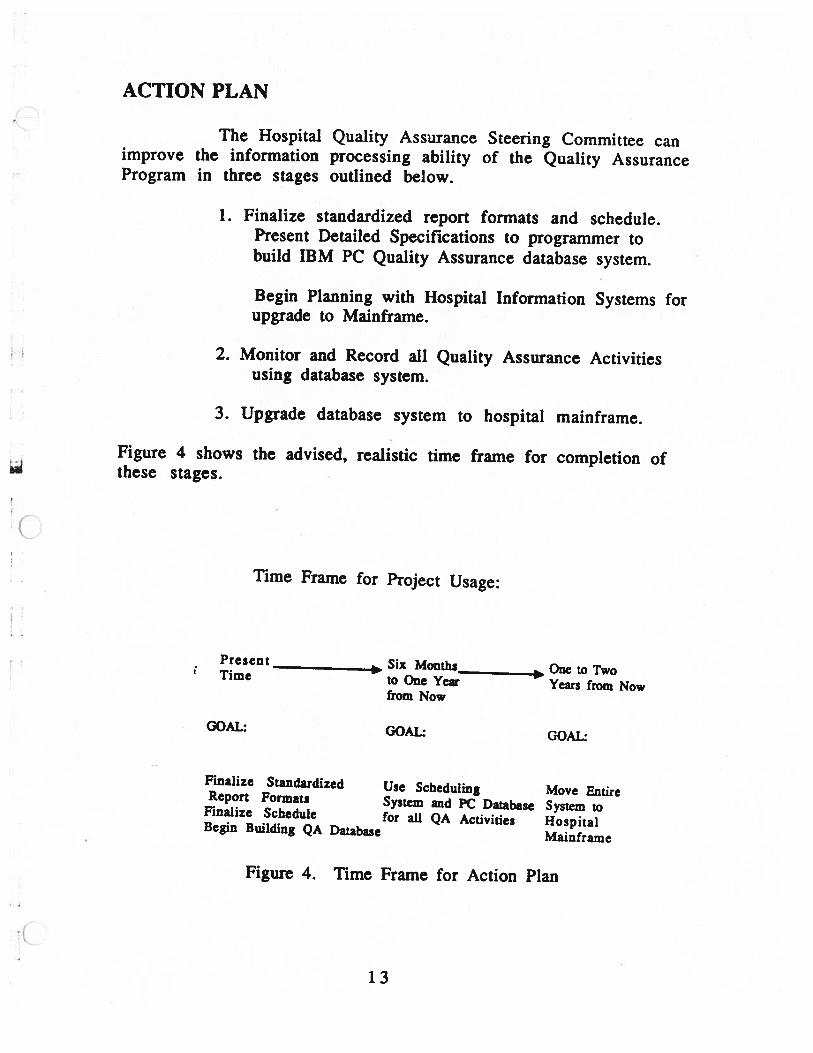
The Hospital Quality Assurance Steering Committee canimprove the information processing ability of the Quality AssuranceProgram in three stages outlined below
1 Finalize standardized report formats and schedulePresent Detailed Specifications to programmer tobuild IBM PC Quality Assurance database system.
Begin Planning with Hospital Information Systems forupgrade to Mainframe.
2. Monitor and Record all Quality Assurance Activitiesusing database system.
3. Upgrade database system to hospital mainframe.
Figure 4 shows the advised, realistic time frame for completion ofthese stages.
Time Frame for Project Usage:
Present
_______________
Six Months____________ One to TwoTime to One Year Years from Nowfrom Now
GOAL GOAL GOAL
Finalize Standardized Use Scheduling Move EntireReport Formats System and PC Database System toFinalize Schedule for all QA Activities HospitalBegin Building QA Database Mainframe
Figure 4. Time Frame for Action Plan
13

As the figure shows, within six months Hospital QualityAssurance Steering Committee should oversee the finalizing of thereport format and schedule. The main focus should be on thescheduler, since it appears that the standardized format will bepassed on to UARCO (professional form developers). Therefore, asmentioned in Recommendations, a final decision needs to be made onthe yearly schedule, and then the schedule dates need to be chosenand groups notified of their yearly due dates.
During this time, the creation of the database system also oughtto be started, so that within one year the system will be operational.Once operational, Quality Assurance & Information Services shouldswitch from their present database system to the new one. This willgreatly improve their efficiency in monitoring reports’ status andtracking the trends and commonalties in reports. The planning forthe move to the mainframe should also begin as soon as possible.
Overall, implementation of these recommendations willsignificantly improve both the quality and efficiency of QA reporting.The better quality of QA reporting will allow HQAC to produce moreaccurate summary reports. The increased reporting efficiency willimprove HQAC’s ability to monitor reports and reduce costs throughtime savings. The end result being an increase in the quality ofimplementing the Quality Assurance Program.
14

Appendix A
Quality Assuance Organization and Information Flow

ClAn
ical
Dep
artm
ent,
(54)
Off
ice
ofal
njc
ajA
ffai
r,
Dep
artm
ent,
(10)
Med
ical
Sta
ff
Com
mit
tee,
(7)
Adj
unct
Par
tici
pan
t,
Mult
idis
cip
ljy
Gro
up,
(Q
uart
eR
epor
tF
oll
ow
-R
epor
t
n
Quar
terj
yR
epor
t
Ann
ual
Pla
nP
oll
ow
.up
Rep
oç
Quar
terl
yR
epo
Ann
ualR
epo
Ann
ual
Pla
nP
ollo
w..i
jpR
epor
t
Quar
terj
yR
epor
t
C (Quart
erl
y
Ann
uai
Pla
n
FoIl
o’w
-uR
epor
t
QU
A!.
In’
ASS
UR
AN
CE
CO
MM
ITT
Ee
Appendix C
Recommended Quality Assurance Reporting Groups
I
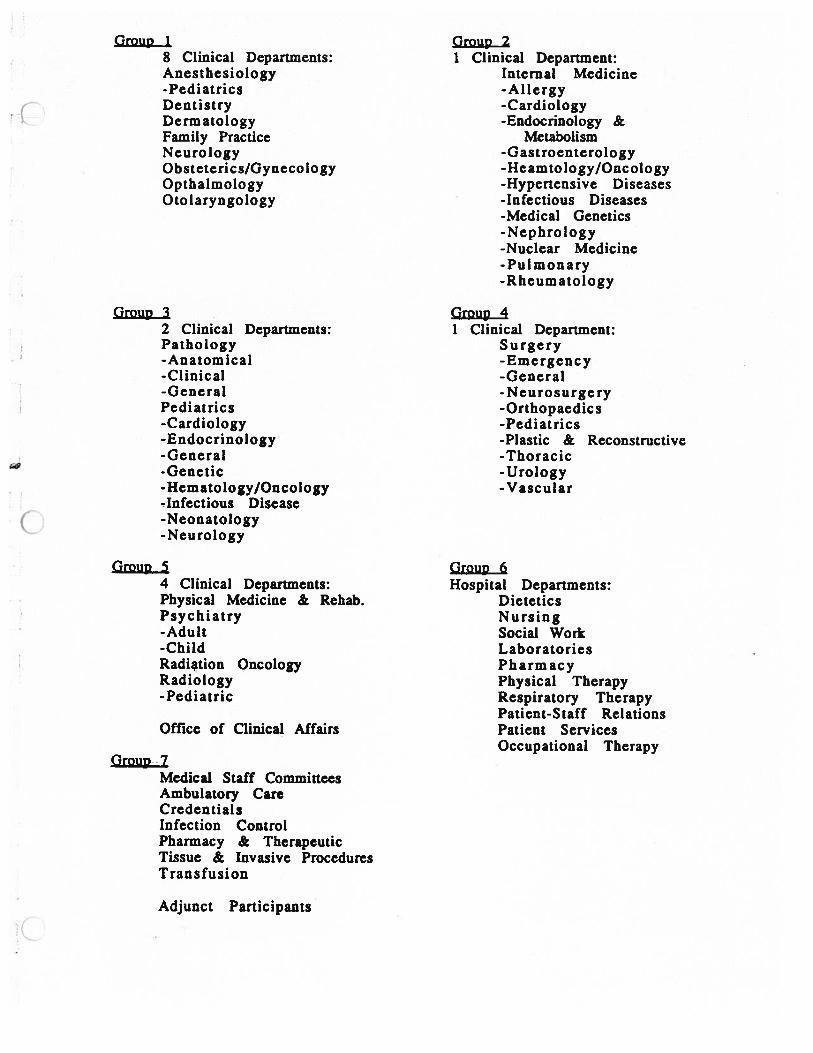
Group 1 Group 28 Clinical Departments: 1 Clinical Department:Anesthesiology Internal Medicine-Pediatrics -AllergyDentistry -CardiologyDermatology -Endocrinology &Family Practice MetabolismNeurology -GastroenterologyObsteterics/Gynecology -Heamtology/OncologyOpthalmology -Hypertensive DiseasesOtolaryngology -Infectious Diseases
-Medical Genetics-Nephrology-Nuclear Medicine- Pulmonary-Rheumatology
Group 3 Group 42 Clinical Departments: I Clinical Department:Pathology Surgery-Anatomical -Emergency-Clinical -General-General -NeurosurgeryPediatrics -Orthopaedics-Cardiology -Pediatrics-Endocrinology -Plastic & Reconstructive-General -Thoracic-Genetic -Urology-Hematology/Oncology -Vascular-Infectious Disease-Neonatology-Neurology
Group 5 Group 64 Clinical Departments: Hospital Departments:Physical Medicine & Rehab. DieteticsPsychiatry Nursing-Adult Social Work-Child LaboratoriesRadiation Oncology PharmacyRadiology Physical Therapy-Pediatric Respiratory Therapy
Patient-Staff RelationsOffice of Clinical Affairs Patient Services
Occupational TherapyGroup 7
Medical Staff CommitteesAmbulatory CareCredentialsInfection ControlPharmacy & TherapeuticTissue & Invasive ProceduresTransfusion
Adjunct Participants
Appendix D
Quality Assurance Scheduling Process

t.b
—R
ep
ort
Co
llecti
on—
IS
end
Rem
inde
rN
otic
esI
Set
Gro
upD
ueD
ates
Not
ify
each
Dep
t.?t
mon
thpr
ior
toD
uefo
ryea
rS
ervi
ceof
Dat
es‘
Dat
e
$$
No
ID
ept/
Ser
vic
esu
bmit
sY
esC
odif
yR
epor
t&
ire
po
rtby
Due
Dat
eE
nter
inD
atab
ase
All
Gro
ups
(See
App
endi
xF)
Rep
orte
dI
IA
IN
ol
TI
I*
Yes
II
T1W
EE
K7*1
Sen
dL
ate
Not
ice
Col
lect
Lat
eR
epor
tw
ithin
1w
eek
IS
umm
ariz
eD
atab
ase
Dat
a1
1W
EE
K81
*I
I
Rep
ort
Rev
iew
——
—
—i
II
II
Rev
ise
Sub
mit
toQ
AS
ubm
itto
QA
II
Wri
teS
umm
ary
IC
omm
itte
eS
teer
ing
Com
mit
tee
Rep
ort
I1
1W
EE
LC
j4**
‘WEE
K1
Q‘1W
EE
K8
/9Y
esN
oi
II
IS
ubm
itto
:I
LR
epor
tP
repa
rati
on—
’E
ndof
thir
dsc
hedu
ling
ECCA
11
WE
EK
15*1
Ipr
oces
sfo
ryea
rM
edic
alS
taff1W
EE
K1
5I
IC
A&
F1W
EE
K16
1*E
xecu
tive
Boa
rdan
dR
egen
tsth
rou
gh
ECCA
and
CA
&F1
1W
eek
16
/17
*1
I

Appendix E
Quality Assurance Database System Specifications

The purpose of this appendix is to list and explain thespecifications of the University of Michigan Hospitals’ QualityAssurance Program’s computer database management system and toserve as a basis for the construction of the computer databasemanagement system.
The database system stresses a menu-driven, table-relationaldesign; that is, the system is composed of several tables, eachcontaining necessary atthbutes for quality monitoring. There areseven tables in this system (Log, Report, Report Data, Follow-upReport, Follow-up Report Data, Contact and Department) and each isinterconnected through a common key (usually the record #). Thespecific variables in each table are listed in Figure 1 (following page).
In order for the system to operate efficiently, it is necessary tominimize the worker-hours required to enter the report informationinto the computer system. Through the examination of the qualitymonitoring process, our project team has determined that the QualityAssurance Program reports and follow-up reports must first bereviewed by professionals who will interpret the report and fill outthe tracking/trending/coding checklist (see Appendices G and H).The checklist is divided into four sections: important aspect of care,indicator, problems identified and actions to be taken. This checklistwill then be given to data entry clerks who will in turn enter thedata as it appears on the checklist into the database system. Anexplanation of how the data will be entered will follow later in thisdocument.
To sign onto the system, an executable batch file must be runthrough a . simple statement (i.e. run quality system). Immediately,the user will be prompted to enter his/her user identification andpassword (both of which are assigned to every user or departmentby a professional). If the user identification and password match arow in the log table, access will be given to the user based upon apre-determined security level. If the two entries do not match, theuser will be given the opportunity to reenter the appropriate useridentification and password or exit the system. Depending upon thelevel of access given the user a menu with various actions willappear.
Due to the nature of this system, there are three distinct typesof access within the system: professional access, data clerk access anddepartmental access. Professional access gives the user seven
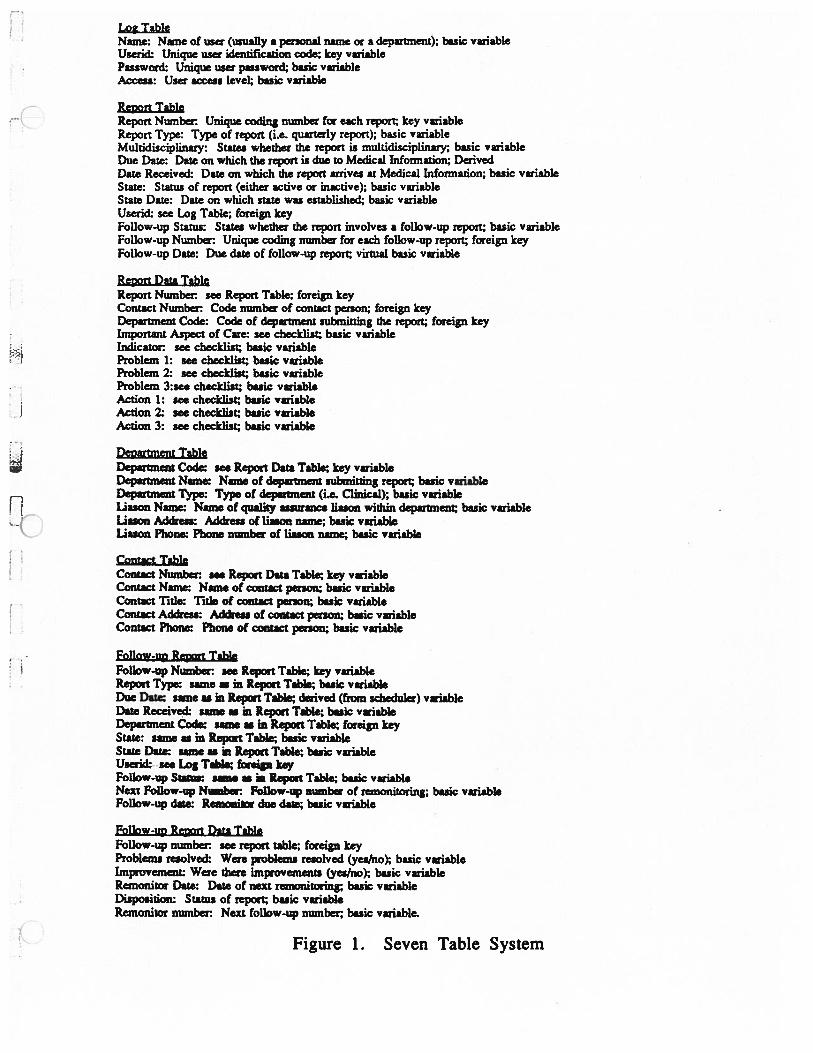
Lo2 TableName: Name of user (usually a personal name or a department); basic variableUserid: Unique user identification code; key variablePassword: Unique user password; basic variableAccess: User access level; basic variable
Ret,ort TableReport Number: Unique coding number for each report, key variableReport Type: Type of report (i.e. quarterly report); basic variableMultidisciplinary: Stares whether the report is multidisciplinary; basic variableDue Dare: Date on which the report is due to Medical Information; DerivedDate Received: Date on which the report arrives at Medical Infonnation; basic variableState: Status of report (either active or inactive); basic variableState Date: Date on which stare was established; basic variableUserid: see Log Table; foreign keyFollow up Status States whether the report involves a follow up report, basic variableFollow up Numbw Unique coding number for each follow up report, foreign keyFollow-up Date Due date of follow-up report, virtual basic variable
Renort Data TableReport Number see Report Table foreign keyContact Number: Code number of contact person; foreign keyDepartment Code: Code of department submitting the report foreign keyImportant Aspect of Care: see checklist, basic variableIndicator: see checklist, basic variableProblem 1: see checklist; basic variableProblem 2: see checklist, basic variableProblem 3:see checklist, basic variableAction 1: see checklist, basic variableAction 2: see checklist, basic variableAction 3: see checklist, basic variable
Department TableDepartment Code: see Report Data Table; key variableDepartment Name: Name of department subanitting report, basic variableDepartment Type: Type of department (La. Clinical); basic variableUason Name: Name of quality asswence liason within department, basic variableLiason Address: Address of lion name; basic variableLiason Phone: Phone number of liason name; basic variable
Contact TableContact Number: see Report Data Table; key variableContact Name Name of contact parson, basic variableContact ThIe Title of contact person, basic variableContact Address Address of contact person, basic variableContact Phone: Phone of contact person; basic variable
Follow-up Report TableFollow-up Number: see Report Table key variableReport Type: same in Report Table; basic variableDue Date: same as in Report Table; derived (from scheduler) variableDate Received: same as in Report Table; basic variableDepartment Code: issue as in Report Table; foreign keyState: same as in Report Table; basic variableState Date: same as in Report Table; basic variableUserid: see Log Table; foreign keyFollow-up Status: same as in Report Table; basic variableNext Follow-up Niunher: Follow-ic number of remonitoring; basic variableFollow-up date: Remoniior due date; basic variable
Follow up Report Data TableFollow.up number: see report table; foreign keyProblems resolved: Were iroblems resolved (yes/no); basic variableImprovement. Were there usiprovements (yes/no) basic variableRemonitor Date: Date of next resnonitoring; basic variableDisposition: Status of report, basic variableRemonitor number: Next follow-up number basic variabla.
C-Figure 1. Seven Table System

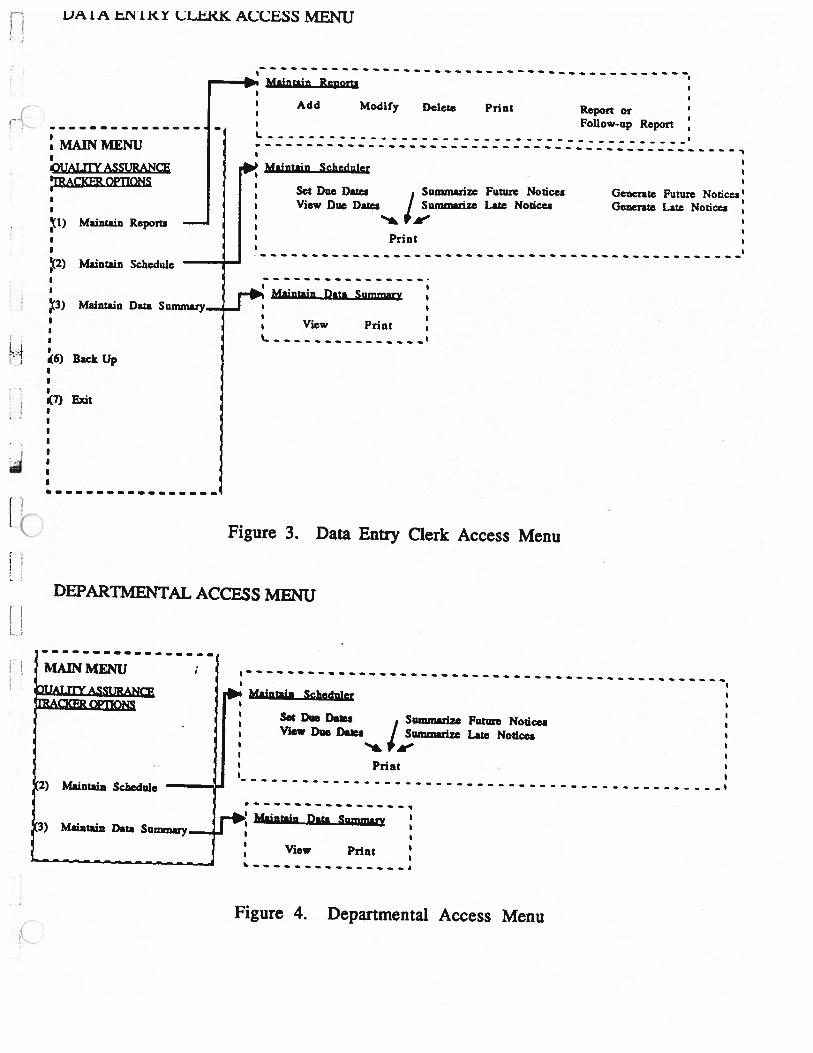
options: maintain reports, maintain scheduler, maintain datasummary, maintain passwords, maintain tracker system, back-upsystem and exit. The professional menu is listed inFigure 2 (below). Data clerk access gives the user five options:maintain reports, maintain scheduler, maintain data summary, backup system and exit. The data entry clerk menu is listed in Figure 3(following page). Departmental access gives the user limited optionsof maintain scheduler and maintain data summary and the exitoption. The departmental menu is listed in Figure 4 (following page).
PROFESSIONALACCESS MENU Maintain Renorts
Add Modify Delete Print Report orFollow-up ReportI I
I
kUALrrY ASSURANCE rb Maintain Scheduleri
Set Due Dates , Summarize Future Notices Generate FutureView Due Dates I Summarize Late Notices Generate Late Notices ‘I II .L,(l) Maintain Reports II I PrintI III
__
-
12) Maintain Schedule
I
Maintain Data Summary i13) Maintain Data Summary......
View Print II I(4) Maintain Password..
(5) Maintain Tracker System — ,I 101% Maintain Password.I
I
(6) Back Up Add Modify Delete l
7) Eait
-:Maintain Tracker System
Add Elements Delete Elements Modify Elements
Figure 2. Professional Access Menu
I)P1A ENIKY 1.LtKK ACCbSS MENU
OUALffY ASSURANAcKER OPTIONS
(1)
(2) Maintain Schedule
(3) Maintain
6) Back Up
7)Exit
Report orFollow-up Report
DEPARTMENTAL ACCESS MENU
Data Entry Clerk Access Menu
Maintain Reports
MENU
Modify Delete Print
Maintain Scheduler
Maintain Reports
SctDueDatesView Due Dazes
L
Summarize Future Notices Generate Future Notices’Summarize Late Notices Generate Late Notices
Data SMaintain Data Summary
View PrintL
Figure 3.
ia Msintai. Scheduler
Set Due Da*sView Due Dates
Summarize Future NoticesSummarize Late Notices
Maintait Data Summary
View PrintI.
Figure 4. Departmental Access Menu

The following is a list and explanation of the various menu optionsmentioned above:
1. Maintain Reports
This options allows the user to add, modify, delete and print reports(initial and follow-up). If selected, the maintain reports optionsprompts the user to another menu with eight options: add report,add follow-up report, modify report, modify follow-up report, deletereport, delete follow-up report, print report and print follow-upreport. Each option does the following:
a. add report or follow-up report: This allows the user to add areport or follow-up report by producing a complete report or follow-up checklist identical to the list used by data clerks, thus allowingthe user to enter the information by selecting the appropriate choiceson the computer tracking/trending/coding checklist via arrow keysor a short number/key code.
b. modify report or follow-up report: This allows the user to changethe checklist answers on the computer within a report or follow-upreport. A particular report or follow-up report is selected by the
( user via report number or the combination of department and duedate. The checklist mentioned above then appears on the computerscreen with the original selections highlighted. The user thenchanges the selections through use of the arrow keys or a shortnumber/key code.
c. delete report or follow-up report: This allows the user to delete areport from the database system. The report is selected either byreport number or by department and due date. Before deleting thereport, the user is given an opportunity to prevent the deletion.When the user fails to prevent the deletion, the report is deletedfrom the database.
d. print report or follow-up: This allows the user to print out areport or follow-up report by record number or department and duedate. The print out appearance is shown in Figure 5 (following page).Note: These options are given to those users withprofessional or data clerk access only.

Record Number [100001] Contact Number [101]Report Type [Clinical ] Contact Name [John Doe]Due Date [04-23-1990] Contact Title [Multidisciplinary [no] Contact Address [Status [Active ] [Status Date [ ] Contact Phone [936-4040]Userid [ ] Follow-up Status [yes]Follow-up Number [1001] Follow-up date [04-23-1991]
Important Aspect of Care: Type of care [DiagnosticPriority [High-risk by, omission
Indicator: Elements of Quality [Continuity of Care, Transfer of Information]Type of Indicator [Structure ]
Problem 1: Type of Problem [Diagnosis ICategory of Problem [Systems ]Severity of Problem [Risk to patients ]Impact of Problem [Hospital ]
Action 1: Type of Action [Knowledge, Orientation, In-service training]ByWhom[ ]ByWhatDate[ I
Problem 2: Type of Problem [ ICategory of Problem [ ISeverity of Problem [Impact of Problem [ ]
I , Action 2 Type of Action [ ]ByWhom[ IBy What Date [ ]
Problem 3: Type of Problem [ ]Category of Problem [ ]Severity of Problem [ ]Impact of Problem [ ]
Action 3: Type of Action [ ]ByWhom[ ]ByWhatDate[ ]
Figure 5. Sample Record Entry
2. Maintain Scheduler
This option allows the user to set due dates for future reports,view current due dates, summarize future notices (report or followup report), summarize late notices (report or follow-up report),generate future notices, generate late notices and print due dates orsummaries. Each of the options are defined below:
a. set due dates for future reports: This option allows the user to setthe due dates for future reports. As mentioned earlier in the projectscheduling section of this document, the reports are spread out overa wide time period to even out the workload for MedicalInformation. This option sets the due dates for reports due duringthe next year by calling a project scheduling program which whenrun will produce the list of due dates up to a user specified futuretime.
b. view current due dates: This option allows the user to view butnot change the due dates of both reports and follow-up reports. Ifthe user access is departmental, the user may only view the duedates of that department (this is ensured by the initial user sign-onand is one of only three options in this section open to departmentalaccess).
c. summarize future notices: This option gives the user a summary,on the computer screen, of upcoming reports or follow-up reportsbased on due date or department.
d. summarize late notices: This options gives the user a summary, onthe computer screen, of late initial or follow-up reports ordered bydue date or department.
e. generate future and late notices: These two options producestandardized forms addressed to particular department liasonswhose departments have either a report or follow-up report due in atime frame specified by the user or have failed to submit a report orfollow-up report.

f. print due dates and summaries: This option allows the user toprint either the list of report or follow-up due dates in a userspecified time window or the summaries generated above.Departmental access allows the user to print both due dates andsummaries for that particular department only.Note: Departmental access gives authorization to view orprint the same departmental due dates or summaries only.
3. Maintain Data Summary
This option allows the user to sort and then view records basedon indicator, aspects of care, departments or actions to be taken. Thisis the trending aspect of the database system which will aid QualityAssurance & Information Services in the production of Hospitals’Quality Assurance Committee’s quarterly report.Note: This option is given to Professionals and Data EntryClerk users only.
4. Maintain Passwords
This option allows the user to add, modify or delete users, user• •..
identifications, passwords and access levels. The specific options are• listed below:
a. add user: This option allows for the addition of a new user. Theuser identification and passwords are entered twice to ensureaccuracy. Assuming the two entries of user identification andpassword match, the computer systems asks for the access levelrequired by the new user.
b. modify user: This option allows for the changing of a useridentification, password or access level. The user will be promptedto enter the old user identification and password and assuming amatch, will be given the option of changing a user identification, apassword, an access level or any combination of the three. Shouldeither the user identification or password need to be changed, theuser will be asked to enter the new user identification or passwordtwice to ensure accuracy. A new access level must be entered onlyonce. The new user identification and/or password does not becomeactive until typed twice identically.
c. delete user: This option allow for the deletion of a user. In orderto prevent accidental deletion, confirmation by the current user isnecessary before deletion is possible.Note: Only users with Professional access are given thisoption
5. Maintain Tracker System
This option allows the user to add, modify or delete tracking,trending and coding elements from the computer database systemchecklist. This option increases the future flexibility of the computerdatabase management system The specific selections are listedbelow:
a. add elements: This option allows the user to add additionalelements to the computer checklist. The user is asked through amenu driven process to show the location of the new element (i.e.important aspect of care, indicator, problems identified or actions tobe taken).
b. modify elements: This option allows the user to change anelement on the computer checklist. Through a simple menu drivenprocess, the user selects the element to be altered. The user thentypes the replacement element.
c. delete 1ements: This option allows the user to remove an elementfrom the computer checklist. The process of deletion is similar tomodification, accept for the fact that the element is deleted instead ofaltered.All previous reports and follow-up reports may be affected by any ofthese three structure changes.Note: Only users with Professional access are given thisoption
6. Back-up
This option allows the user to create a back-up version of thecomputer database management system onto either a hard drive,floppy disk or other storage mechanism.Note: Access levels of professional and data entry clerkmay perform this function.
7. Exit
This allows the user to exit the system and is usable by all access levels.
C
Appendix F
Report Codification and Data Entry Process

Rep
ort
Dat
e/T
ime
___
Rep
ort
Num
ber
Rep
ort
Che
ckli
stan
dJ
Dat
aE
nter
edS
ubm
itte
dS
tam
ped
byA
ssig
ned
and
Com
plet
e?O
rigi
nal
Rep
ort
9_in
toD
atab
ase
Qua
lity
Che
ckli
st(s
eeG
iven
toD
ata
Ass
ura
nce
App
endi
xG
&H
)E
ntry
Cle
rkon
Arr
ival
Fil
led
Out
bya
Pro
fess
ion
al
Rep
ort
Sent
Bac
kto
Con
tact
Per
son
orD
epar
tmen
tL
iaso
nW
ith
Doc
umen
tati
onD
etai
ling
Mis
sing
Info
rmat
ion
(wit
hin
one
wee
k)

Appendix G
Checklists for Trackj,Pjrefld./ Coding Initial and Fo11ow
Reports

UNIVERSITY OF MICHIGAN HOSPITALSQUALITY ASSURANCE PROGRAM
TRACKING/TRENDING/CODING ELEMENTS FOR HQA INITIAL REPORTS
STUDY NUMBER:_____________________
Multi-disciplinary and/or integrated study: Yes_____ No______Participants:
Elements of Quality1.) Effectiveness
Practitioner Performance/CompetenceSupport Staff PertormancelComp.• Medical Record System• Risk Minimization• Identification of Patient Needs• Achievement of Desired Outcome
2.) AcceptabilIty to Patient• Responsiveness to perceived needs• Level of communication, concern, courtesy• Timeliness of Care• Achievement of Desired Outcome
3.) Accessibility/Availability• AccesstoCare• Availability of Care• Emergency and After-hours Care
4.) Efficiency/Appropriateness• Timeliness of care• Identification of patient needs• Appropriate use of resources
5.) Continuity of Care• Coordinated/continuous care• Transfer of Information• Treatment follow-up
b. Type of Indicator1.) Structure2.) Process3.) Outcome
a.
1. Submitting area. a. Important Aspect of Careb. Clinical Indicator
2. Important Aspect of Care a. Type of Care1.) Diagnostic2.) Therapeutic3.) Preventive4.) Rehabilitative5.) Supportive6.) Paliative
b. Priority1.) High-volume2.) High-risk by:
• omission• commission
3.) Problem-prone for• patients• providers
3. Indicator
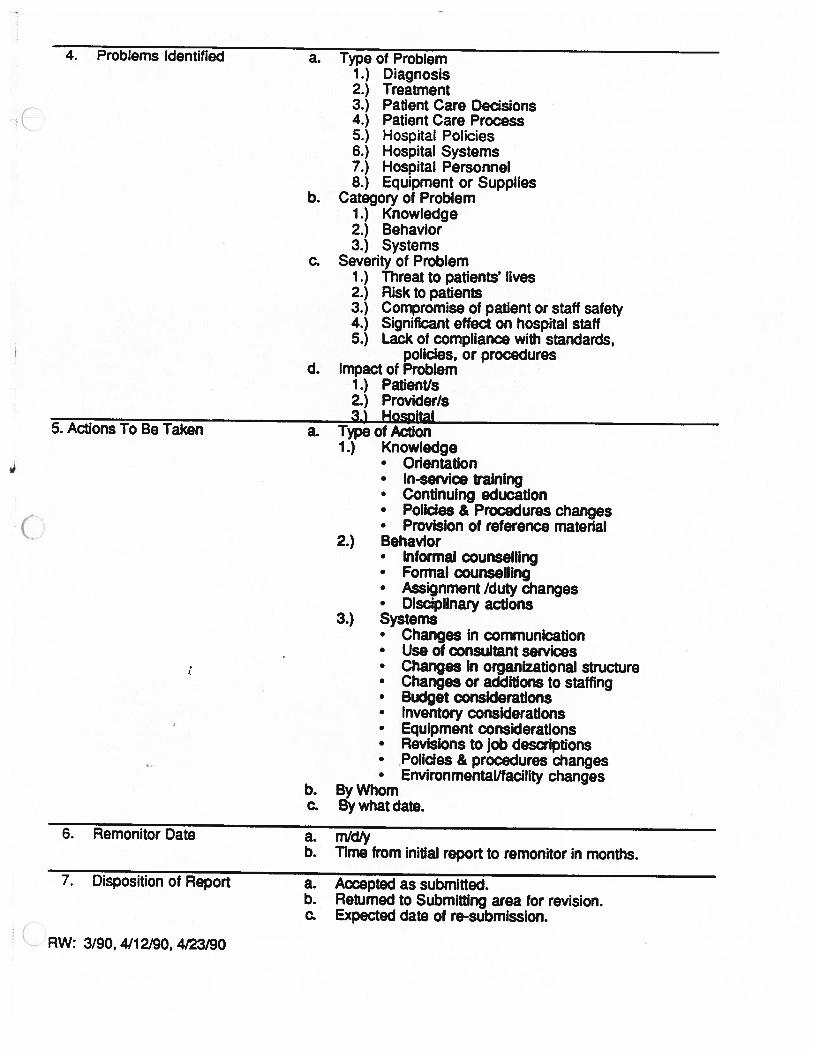
a. Type of Problem1.) Diagnosis2.) Treatment3.) Patient Care Decisions4.) Patient Care Process5.) Hospital Policies6.) Hospital Systems7.) Hospital Personnel8.) Equipment or Supplies
b. Category of Problem1.) Knowledge2.) Behavior3.) Systems
c. Severity of Problem1.) Threat to patients’ lives2.) Risk to patients3.) Compromise of patient or staff safety4.) Significant effect on hospital staff5.) Lack of compliance with standards,
policies, or proceduresd. Impact of Problem
1.) Patient/s2.) Provider/s3.) Hospital
a. Type of Action1.) Knowledge
• Otientation• In-service training• Continuing education• Polloes & Procedures changes• Provision of reference matenal
2.) BehavIor• Informal counselling• Formal counselling• Assignment /duty changes• Disciplinary actions
3.) Systems• Changes in communication• Use of consultant services• Changes in organizational structure• Changes or additions to staffing• Budget considerations• Inventory considerations• Equipment considerations• Revisions to job descriptions• Policies & procedures changes• Environmental/facility changes
b. By Whomc. By what date.
4. Problems Identified
5. Actions To Be Taken
CRW:
6. Remonitor Date a. rnld/yb. Time from initial report to remonitor in months.
7. Disposition of Report a. Accepted as submitted.b. Returned to Submitting area for revision.c. Expected date of re-submission.
3/90,4/12/90,4/23/90
UNIVERSITY OF MICHIGAN HOSPITALSQUALITY ASSURANCE PROGRAM
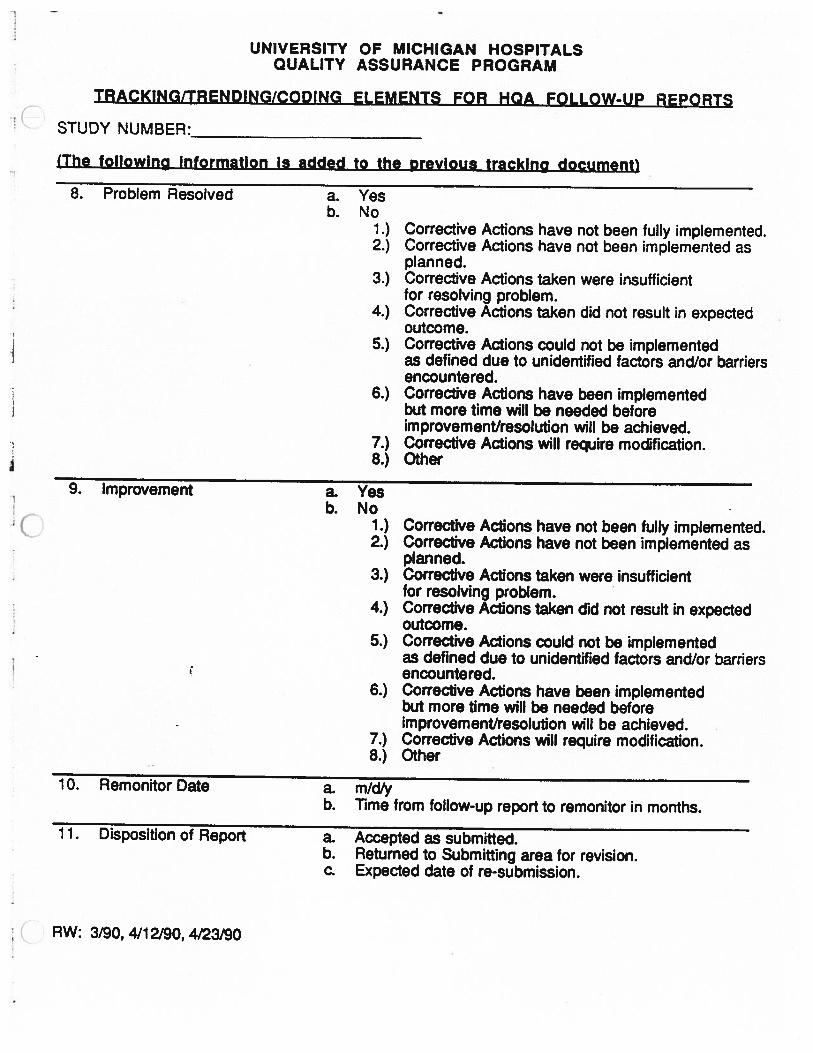
TRACKING/TRENDING/CODING ELEMENTS FOR HOA FOLLOW-UP REPORTS
C STUDY NUMBER:______________________
(The followino information is added to the Drevlous tracking document)
8. Problem Resolved a. Yesb. No
1.) Corrective Actions have not been fully implemented.2.) Corrective Actions have not been implemented as
planned.3.) Corrective Actions taken were insufficient
for resolving problem.4.) Corrective Actions taken did not result in expected
outcome.5.) Corrective Actions could not be implemented
as defined due to unidentified factors and/or barriersencountered.
6.) Corrective Actions have been implementedbut more time will be needed beforeimprovement/resolution will be achieved.
7.) Corrective Actions will require modification.8.) Other
9. Improvement a. Yesb. No
1.) Corrective Actions have not been fully implemented.2.) Corrective Actions have not been implemented as
planned.3.) Corrective Actions taken were insufficient
for resolving problem.4.) Corrective Actions taken did not result in expected
outcome.5.) Corrective Actions could not be implemented
as defined due to unidentified factors and/or barriersencountered.
6.) Corrective Actions have been implementedbut more time will be needed beforeimprovement/resolution will be achieved.
7.) Corrective Actions will require modification.8.) Other
10. Remonitor Date a. m/db. Time from follow-up report to remonitor in months.
1 1. Disposition of Report a. Accepted as submitted.b. Returned to Submitting area for revision.c. Expected date of re-submission.
RW: 3/90, 4/12/90, 4/23/90

Rep
ortin
gP
rocess
for
Hosp
itals’Q
uality
Assu
rance
Pro
gram
for:
The
Un
iversity
ofM
ichig
anH
osp
itals’Q
uality
Assu
rance
Corn
mittee
by:
Kent
Feig
ner
David
Karp
Victo
riaV
ogel
I

Major Points for Presentation:
1) Information & Report Formats
- by Victoria Vogel
2) Scheduling System
- by Kent Feigner
3) Database Specifications
- by David Karp
Information & Report Formats
Three Major Points:
1) Why was the Project Needed?
2) Goals of the Project
3) Benefits from Standard Reports

‘C
Appendix H
Oral Presentation Slides

IUNIVERSITY OF MICHIGAN HOSPITALS’ QUALITY ASSURANCE PROGRAM I• :..‘:
Initial Study Report
Multidisciplinary and/or integrated Study:
__________
Participants:
• QUARTERLY REPORT FOR: _Jan-March 1990
___________
(Please complete one form per indicator)
SUBMITTED BY
________________
• CIiiic DepartmertDiision/Secton/Secvice________________
_______________
• HosØtai-Based Departrner
________
• Medical Staff By-Laws Committee_____________
_____________
•Oth_______• Services/Providers involved______________
IMPORTANT ASPECT OF CARE:
INDICATOR:
PROBLEM/S IDENTIFIED AND/OR OPPORTUNITIES FOR IMPROVEMENT:1.
impact of the problem:
Action/s to be taken:Who or what is expected to change?
Who is responsible for implementing action?
What action is appropriate?
Whn ic “ nm ir’? (flj
Yes:_____ No:_____
CONTACT PERSON:Name:Title:Address:_________________Phone:__________________
RemonRor Date:2.
Impact of the problem:
Action/s to be taken:Who or what is expected to change?
Who is responsible for implementing action?
What action is appropdate?
When chafloe exoeded to occur? CDate Renuor Date:3.
Impact of -the problem:
Actionls to be taken:Who or what is expected to change?
Who is responsible for implementing action?
What action is appropriate?
When is change expected to occur? (Date)
rev: 4/10/90 CODE NUMBER:.hqal rep 1.0 DATE RECV’D:_
Remonitor Date:
(OUALrr( ASSURANCE DOCUMENTI CONFIDENTIALjLA 333.21515. ?0175

600B
eforeC
hanges
After
Changes
500-
400-E
stimated
Num
berof
All
Quality
Assurance
Reports
foran
Average
Year
300-
(Based
on1989-1990
Figures)
200-
100-
0-
1E
ffectof
Changes
2
Co
mp
arison
ofC
hangesin
the
Estim
atedN
um
ber
ofR
eports
for
Univ
ersityof
Michigan
Ho
spitals’
Qu
alityA
ssuran
ce
1,U
Benefits of Standard Report Forms:
1) Create Adherence to Process
2) Ensure Complete Reporting
3) Assign Responsibility
4) Enable Tracking Capability
5) Save Time

Collection Ideas
- Weekly Reporting
- 10 Reports/Week Maximum

Group
1(9
services)
Group
2(14
services)
Group
3(13
services)
Group
4(10
services)
Group
5(8
services)
Group
6(10
services)
Group
7(7
services)
Rep
ort
Prep
.
Rep
ort
Review
1234
56
QA
Activ
ites
78
co11et
reports
prep
.and
review
HQ
AC
repo
rt
10
WEEK

Recommended Guidelines
- No August Collection
- No late December Collection

Pro
po
sedS
ched
ule
-g
iven
recom
mendatio
ns
collect
reports
•prep
.and
review
HQ
AC
_4
FebM
arA
prM
ayJu
ne
july
Aug
Sep
Oct
Nov
Dec
JanF
ebM
ar
MO
NT
H
report
I
r_

—R
eportC
olle
ctio
n—
1
SetG
roupD
ueD
atesN
otifyeach
Dept./
foryear
Service
ofD
ates
Send
Rem
inderN
oticesI
month
priorto
Due
Date
End
ofthird
schedulingprocess
fory
ear
No
I
I
Subm
itto
QA
Corn
rnittee1
1W
EK
14*1
Subm
itto
QA
Steering
Corn
mittee
1WE
EK
-10
AliG
roupsR
eported
Write
Su
mm
aryR
eport1
1W
EE
K8/9
*1
IL
Rep
ort
Pre
para
tion
+
Dept./S
ervicesubm
itsrep
ort
byD
ueD
ate
No
Yes
Codify
Report
&E
nterin
Database
(SeeA
ppendixF)
Send
Late
Notice
Collect
Late
Report
with
inI
week
Rep
ort
Rev
iew—
——
—
Revise
Yes
**WE
EK
7**
I•
Sum
marize
Database
Data
11
WE
EK
8*1I
I
II
No
II
I*
II
II
I
IS
ubmit
to:
__
__
__
____
ECCA1W
EE
K15*1
Medical
Staff
‘WEEK
15
II
CA
&F
11
WE
EK
161*
IE
xecutiveB
oardand
Regents
IthroughE
CC
Aand
CA
&F
’1W
eek
16/17*1I

PR
OF
ES
SIO
NA
L-,
AC
CE
SSM
EN
U—
Maintain
Reports
Add
Modify
Delete
Prin
tR
eportor
_________
_______
Follow
-upR
eport—
——
—a—
—-—
-—
_—
_-—
_—
_-.—
_—
_a_,
MA
INM
EN
U
‘OU
AL
YA
SSUR
AN
CE
ir
Maintain
Scheduler
RA
CK
ER
OPTIO
NS
SetD
ueD
atesS
umm
arizeF
utureN
oticesG
enerateF
utureN
oticesV
iewD
ueD
atesI
Sum
marize
Late
Notices
Generate
Late
Notices
(1)M
aintainR
eports—
::
:P
rint
2)
Maintain
Schedule—
Maintain
Data
Sum
mary
(3)M
aintainD
ataSum
mary......
....IV
iewP
rint
II
I
:(4)M
aintainPassw
ords_______
(5)M
aintainT
rackerSystem
—
Maintain
Passw
ordsI
II
II
I
(6)B
ackU
p:
Add
Modify
Delete
::
7)
Exit
a—
a—
a—
aa
aa
aa
—a
I
—:
Maintain
Tracker
System
Add
Elem
entsD
eleteE
lements
Modify
Elem
ents
)0
U
SAMPLE CHECKLIST
Important Aspect of Care
a. Type of Care
1.) Diagnostic
2.) Theraputic
3.) Preventative
4.) Rehabilitative
5.) Supportive
6.) Paliatjve
b. Priority
1.) High-volume
2.) High-risk by:
• omission
• commission
• Problem-prone for
• patients
• providers

C Record Number [100001] Contact Number [101]Report Type [Clinical I Contact Name [John Doe]Due Date [04-23-1990] Contact Title [ jMultidisciplinary [no I Contact Address [Status [Active I [ jStatus Date [ I Contact Phone [936-4040]Userid [ I Follow-up Status [yes]Follow-up Number [1001] Follow-up date [04-23-1991]
Important Aspect of Care: Type of care [DiagnosticPriority [High-risk by, omission
Indicator: Elements of Quality [Continuity of Care, Transfer of InformationType of Indicator [Structure I
Problem 1: Type of Problem [Diagnosis ]Category of Problem [Systems ]Severity of Problem [Risk to patients ]Impact of Problem [Hospital ]
Action 1 Type of Action [Knowledge, Orientation, In-service trainingByWhom[ IBy What Date [ ]
Problem 2: Type of Problem [ ICategory of Problem [ ISeverity of Problem [ ]Impact of Problem [ I
Action 2: Type of Action [ IByWhom[ IByWhatDate[ I
Problem 3: Type of Problem [ ICategory of Problem [ ISeverity of Problem [ IImpact of Problem [ ]
Action 3 Type of Action [ IByWhom[ IBy What Date [ ]
Plan of Action for Implementation:
Now:
1) Revise Forms Per Feedback
2) Set Schedule
3) Present Specifications to ProgrammerPossibilities:? RBase, Oracle, Paradox ?
4) Finalize Checklist Format for Follow-upfor Tracking Report
Future:
1) Implement Database
2) Train Personnel for Mainframe Upgrade

Tim
eF
rame
forP
rojectU
sage:
Pre
sent
Tim
eS
ixM
onthsto
One
Year
fromN
ow
*O
neto
Tw
oY
earsfrom
Now
GO
AL
:G
OA
L:
GO
AL
:
Begin
Implem
entatio
nof
New
QA
Plan
Use
Scheduling
System
andD
atabasefor
allQ
AA
ctivities
Move
Entire
System
toH
osp
italM
ainfram
e
In Summary:
Why Accept?
Increase the Ability of Quality Assurance toMonitor Reports
• Standardize Methods for Reporting Studies
0
• Reduce Number of Reports by about 40%
• Provide Manageable Flow of Reports
• Ability for Trending/Tracking Important Data