quality account - djerriwarrh health services
TRANSCRIPT

Djerriwarrh Health Services
Quality Account 2015–16

2 Djerriwarrh Health Services Quality Account Report 2016
Contents
1. Consumer, carer and community participation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
1.1 Doing it with us not for us: strategic direction 2010–13 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
1.2 Interpreter services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
1.3 Victorian Health Experience Survey – patient experience score . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
1.4 Improving Care for Aboriginal Patients program . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
1.5 Community health priority population group response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9–10
2. Quality and safety. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
2.1 Feedback and complaints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
2.2 People Matter survey score . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
2.3 Positive workplace culture and prevention of bullying and harassment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14–15
2.4 Staff survey results and programs improvement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16–17
2.5 Accreditation status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
2.6 Adverse events . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
2.7 Quality indicators including Staphylococcus aureus bacteraemia rate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20–21
2.8 Hand hygiene compliance and influenza immunisation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22–25
2.9 Victorian perinatal services performance indicators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
2.10 Victorian Audit of Surgical Mortality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
2.11 Residential aged care indicators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
2.14 Quality improvement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
3. Continuity of care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
3.1 Victorian Healthcare Experience Survey – ‘Leaving hospital’ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
3.2 Continuum of care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32–33
3.3 Continuum of care case study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
3.4 Advance care planning and case study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
3.5 Organisational policy for end-of-life care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36

3Djerriwarrh Health Services Quality Account Report 2016
Welcome
DR JOHN BALLARD, Administrator, Djerriwarrh Health Services
This 2016 Quality Account Report marks another new beginning for Djerriwarrh Health Services. The Quality Account Report was previously produced as the Quality of Care Report.
This year it has been transformed to provide a more robust, transparent and accountable report with performance benchmarked against all Victorian public health services and hospitals.
Those three words – robust, transparent, accountable – are useful to keep in mind as you review the Quality
Account Report, because they characterise so much of what has been achieved across Djerriwarrh in the 2015-16 financial year.
In my role as Djerriwarrh Health Services’ Administrator it has been my pleasure to support the determination of staff under the leadership of chief executive, Andrew Freeman, to be a health service that all can be proud of, most of all the communities who rely on Djerriwarrh to be safe, professional and contemporary.
ANDREW FREEMAN, Chief Executive, Djerriwarrh Health Services
Putting together this 2016 Djerriwarrh Health Services Quality Account Report has provided all staff involved an opportunity to reflect on where we have come from, where we have got to, and where and how we must continue to strive to ensure Djerriwarrh is a safe, confident, capable service with a positive and powerful future.
The Quality Account Report provides a new way to benchmark our performance and provide transparency and accountability to our patients, residents, clients, community, staff and other stakeholders.
It provides comparisons with peer organisations across metropolitan and regional Victoria in a format that
encourages further questioning and sets clear direction as to where our Health Service should be placing its emphasis.
I’m pleased to note that Djerriwarrh recorded above State averages on many of the indicators. We can pause and take some quiet pride in that, but our goal is to see sustained improvement.
I urge you to read through this first Djerriwarrh Health Services Quality Account Report and understand that while Djerriwarrh has come a great way in 12 months, continuous improvement across the Service is now standard practice.

Consumer, carer and community participation
1.

5Djerriwarrh Health Services Quality Account Report 2016
1.1 Doing it with us not for us: strategic direction 2010–13
Djerriwarrh Health Services established the Strengthening Multicultural Communities (SMC) project in 2012 in response to a rapid growth in refugees and migrants making their home in the Melton region.
Work on health issues and social inclusion began with the Chin community, an ethnic group from Myanmar, but in 2015 the need to work with the multicultural community more broadly was recognised.
Three community consultation workshops were conducted in 2015 to inform the direction and method of engagement for future SMC community activities. Workshop participants included members of Melton City Council, a cultural diversity nurse and representatives of indigenous Australian, Bangladeshi, Egyptian, German, Greek, Italian, Polish, Solomon Islands and British communities. The consultation workshops were open to all community members and attended by 28 people.
The workshops were designed to offer a safe informal environment to share thoughts and ideas, using health literacy principles for communication method and tool selection. Core questions asked at the beginning and end of each workshop were “Do you feel a part of the Melton community?” and “How can we celebrate multiculturalism in Melton?”
A common workshop response was how sport and food helps to unite communities, with events or activities highly recommended by participants as a way to engage with Culturally and Linguistically Diverse (CALD) groups.
The majority of participants also stressed the significant barriers to engagement. They reported experiencing feelings of isolation, being stigmatised because of personal beliefs and being unaware of cultural or community expectations, and highlighted experiences of racism and discrimination.
Based on workshop recommendations, consultation with service providers via the New and Emerging Communities Network and internal health promotion staff, four projects were planned and implemented with the Chin community during 2015–2016: Burmese Language School (36 weekly participants); Child Safety Car Restraint Day (four families); Chin National Day 2016 (160 attendees); and Bike Safety (four attendees).
BURMESE LANGUAGE SCHOOL
The Victorian Multicultural Commission funded this start-up in 2015 with a $2600 grant for a community-run series of Burmese language classes. As there are 31 Chin dialects, it was agreed that the Language School would teach Burmese to build a sense of community and not segregate the different dialects.
Six classes were run by three local Chin women with more than 30 participants each week. The project was designed to be self-sustaining and the community has since entered into a partnership with the Melton South Community Centre to continue running the classes by themselves.
CHIN NATIONAL DAY 2016
Djerriwarrh Health Services (DjHS) supported New Hope to run Chin National Day in February at the Melton Community Hall with a celebration of the Burmese Chin Community that included live performances, guest speakers and a traditional lunch.

6 Djerriwarrh Health Services Quality Account Report 2016
1.2 Interpreter services
The City of Melton and Moorabool Shire combine to make a culturally rich and vibrant community that’s home to an expanding mix of people of diverse cultures and nationalities.
Nearly one quarter of City of Melton resident are from a non-English speaking background, with the largest population groups coming from India, the Philippines and Malta (ABS, 2013). In contrast, five per cent of Moorabool Shire residents are from non-English speaking backgrounds with the largest population groups having migrated from Germany, the Netherlands and Malta (ABS, 2013).
To optimise delivery of client care and provide for better health outcomes all round, Djerriwarrh Health Services (DjHS) must be responsive to the needs of residents from all cultures represented in its community.
Reflecting this commitment, DjHS aims to ensure that services are accessible to clients from all language groups.
In 2015–16, DjHS engaged the Victorian Interpreting and Translating Services (VITS) to provide 1183 on-site and 498 telephone interpreting services to support client assessment and treatment. Specific language requests reflect the changing nature of the local community, with the most frequently requested languages being Arabic (33 per cent); Burmese (15 per cent); Dinka (a community language in southern Sudan, 12 per cent); Auslan (six per cent); and Vietnamese (four per cent).

7Djerriwarrh Health Services Quality Account Report 2016
1.3 Victorian Health Care Experience Survey – patient experience score
The Victorian Healthcare Experience Survey (VHES) collects data from users of Victorian public health services, using an independent contractor reporting to the Department of Health and Human Services.
As the tables below show, in 2015–16 Djerriwarrh Health Services (DjHS) consistently exceeded state VHES averages.
VHES questionnaires are distributed in the month following a hospital admission or an emergency department attendance, and responses can be completed online or in hard copy. Contact information is confidential and questionnaires are available in English and other community languages.
The results of these surveys are shared with staff, Quality and Safety
Committee, Diversity and Consumer Advisory
Committee and the Board.
Victorian Healthcare Experience Survey (VHES) – Results
Bacchus Marsh Hospital Melton Health STATE AVERAGE
Jul–Sept15 overall 95.86% 91.60%
Oct–Dec15 96.73% 98.33% 92.20%
Jan–Mar16 97.31% N/A 91.50%
Apr–Jun16 92.26% N/A 91.30%
From July to September 2015 all DjHS reports were combined, but from 30 September 2015 separate reports were provided for Bacchus Marsh and Melton Regional Hospital and Melton Health. There is no data for January–March 2016 and April–June 2016 at Melton Health due to a low survey response rate.
Statewide averageMelton HealthBacchus Marsh Hospital
Jul – Sep 15 Oct – Dec 15 Jan – Mar 16 Apr – Jun 160
20
40
60
80
100
VHES – Results 2015–2016

8 Djerriwarrh Health Services Quality Account Report 2016
1.4 Improving Care for Aboriginal Patients program
Djerriwarrh Health Services’ (DjHS) Aboriginal Health team works to increase capacity to achieve better health and wellbeing for individuals and community.
In 2015–16 the team implemented HealthWorks, a project to promote healthy transition to adulthood and facilitate pathways to employment, tied into Priority 3 of the Victorian Koolin Balit Strategy to facilitate a “healthy transition to adulthood”.
HealthWorks takes a holistic approach that recognises the role of education and employment in health and wellbeing while responding to community concerns about employment and future opportunities for young Aboriginal people. It supports participants to gain and retain employment with skills and experience that enhance job prospects, and connects with local services to cover health and social issues that can impact job retention. This includes recognising the role of adults and parents as role models.
Activities included parenting support programs, cultural events, health promotion activities, career development programs, a homework support program and cultural competency training for community service organisations.
Project tracking includes:
• 83 per cent of participants report increased confidence to engage in physical activity
• 71 per cent report increased confidence to make healthier food choices
• 71 per cent report improved teamwork, initiative, organization, self-management and computer skills
• More than 513 people participated in health promotion activities including cooking groups, physical activity programs and health information sessions
• DjHS recruited six Aboriginal community volunteers who provided 129 days of community volunteer work
• 40 staff completed Aboriginal cultural competency training delivered by the Victorian Aboriginal Community Controlled Health Organisation
The HealthWorks project was informed by annual consultation with the Aboriginal community to identify community priorities, with the DjHS Aboriginal Men’s Group, Women’s Group and Parents group leading the planning and delivery of agreed activities.
The strength of partnerships with community organisations has been pivotal to HealthWorks’ success, bringing expertise and resources to support a common goal. Community organisations involved to date include: • Brimbank Melton Local Learning and Employment
Network• Care Connect• Carers Victoria• Centrelink • CoHealth• Djerriwarrh Community Education Service• Friends of Melton Botanic Gardens• Health West• Kirrip Aboriginal Corporation• MacKillop Family Services• Matchworks• Melton Men’s Shed• Melton Secondary College• Melton Waves Pool• Moorabool Shire Council• Melton City Council• Victorian Aboriginal Child Care Agency• Victorian College of Optometry • Victorian Legal Aid Service

9Djerriwarrh Health Services Quality Account Report 2016
1.5 Community health priority population group response
Community Engagement and Participation
Djerriwarrh Health Services’ (DjHS) Health Promotion Team partners with community and external agencies to address social and environmental drivers of health at a local level, and provides opportunities for community members to participate in decisions that influence health and wellbeing.
Linking Melton South is an innovative place-based community development facilitated by DjHS over three years. The project aims to promote a vibrant and connected community capable of responding to local aspirations and needs, and uses a model called ‘assets-based community development’.
That means, instead of focusing on what is lacking, the focus is on the strengths and resources present in the community.
During 2015–16, more than 1300 people and 32 local organisations were involved in Linking Melton South events and activities. Four Linking Melton South projects have been informed by the local community: Dream Big Festival, Linking Melton South Pop-up Services Hub, Mosaic Garden at Melton South Community Centre, and At the Platform – a music event at Melton train station.
At the Platform
Music Event
Mosaic
Garden
Pop-Up Hub
Dream Big
Festival
200
300
200
595

10 Djerriwarrh Health Services Quality Account Report 2016
1.5 Community health priority population group response
WALK WITH HER
In late 2015 Djerriwarrh Health Services (DjHS), with Melton Women Making It Happen, City of Melton and Caroline Springs Square, began planning a walk to encourage people to walk together for a safer, more respectful, more equal community. About the same time, Melton Women Making It Happen helped to identify 14 new women to profile and celebrate for the 2016 Melton Women Making It Happen International Women’s Day program.
In March 2016 Safer City Day presented Walk With Her led by the 2015 and 2016 Melton Women Making It Happen women, with more than 120 people walking together to help end violence against women. Participants came from organisations including City of Melton, Victoria Police and the State Emergency Service. Clothesline displays set up around Lake Caroline displayed more than 200 supporting t-shirts.
FUTURE ACTION
The 2015–2016 Melton Women Making It Happen group has already begun planning activities for the next 12 months to align with the findings of the Royal Commission into Family Violence (Victoria) and the new ‘Change the Story’ Framework.
A dedicated and innovative group of women in our community have made significant gains in raising awareness of this important issue and addressing some of the key drivers for violence against women.
Caption to go here??

Quality and safety
2.

12 Djerriwarrh Health Services Quality Account Report 2016
CASE STUDY – CONSUMER FEEDBACK
Consumer feedback is an important way of identifying how Djerriwarrh Health Services (DjHS) can improve. In early 2016, a member of the public informed DjHS that its disabled public toilet at Bacchus Marsh & Melton Regional Hospital was not easily accessible. As a result, DjHS immediately made a number of improvements to the on-site disabled public toilet, making it more accessible for all. Initiatives to communicate change and offer opportunity for consultation and feedback to employees have included executive forums on all campuses; a Djerriwarrh Health Services newsletter; introduction of a committee governance structure; and all employees involved in decision about new values and behaviours.
2.1 Feedback and complaints
Consumer feedback is an increasingly important way for Djerriwarrh Health Services (DjHS) to monitor its services.
All feedback is reviewed by the relevant department in DjHS and reported to the executive Quality and Safety Committee and Board.
Listening to what consumers tell us is vital to a continuous quality improvement cycle, as without feedback we only have half the story.
DjHS gains feedback from consumers in several ways, including “Have your say” forms at collection points; and through the DjHS website which has contact details and a feedback tab.
All feedback is recorded in the DjHS feedback system, whether it’s provided formally, as notes or enquiries.
Introducing DjHS Diversity and Consumer Advisory Committee
Feedback Jul 15
Aug 15
Sep 15
Oct 15
Nov 15
Dec 15
Jan 16
Feb 16
Mar 16
Apr 16
May 16
Jun 16
2015–16 YTD
Complaints 3 2 3 8 7 2 5 4 3 7 11 9 64
Compliments 13 10 16 25 15 12 13 5 19 18 42 22 210
“ Have your say” enquiries/ suggestions
5 11 41 4 6 0 0 9 4 4 11 4 99
TOTAL 21 23 60 37 28 14 18 18 26 29 64 35 373
Feedback 2015 – 2016

13Djerriwarrh Health Services Quality Account Report 2016
2.2 People Matter survey score
The annual People Matter Survey provides a means for Djerriwarrh Health Services (DjHS) staff to share beliefs, attitudes and insights about their workplace. It provides an opportunity to gauge what is valued in the workplace, an organisation’s culture, and staff commitment and satisfaction.
In 2015 only 22 per cent of Djerriwarrh Health Service staff responded to the 2015 People Matter Survey, but in 2016 that number almost doubled.
Number of responses
Response Rate
2016 245 40%
2015 149 22%
POST SURVEY
In response to the People Matter Survey results, DjHS Senior Management Team will develop an action plan to address the lowest scoring areas in the survey. Survey results, the action plan and progress updates are shared with all staff.
DjHS places high emphasis on the responsibility to ensure all staff are treated fairly and not exposed to bullying or harassment behaviours.
Staff who report having personally experienced bullying at work in the previous 12 months was below group average, However, there is a need to continue to improve in this area.
Since the 2015 survey, DjHS steps to address bullying behaviours in the workplace have included a review of procedures, which have been updated and made accessible to all staff; introduced new Values and Behaviours across DjHS with ongoing support for the leadership team; and – as well as a mandatory competency requirement – DjHS has introduced face-to-face education sessions on bullying and harassment.
DjHS has experienced major change in 12 months and this was reflected by 77 per cent of survey respondents indicating they had been directly affected by significant change in that period.
Initiatives to communicate change and offer opportunity for consultation and feedback to employees have included executive forums on all campuses; a Djerriwarrh Health Services newsletter; introduction of a committee governance structure; and all employees involved in decision about new values and behaviours.

14 Djerriwarrh Health Services Quality Account Report 2016
2.3 Positive workplace culture and prevention of bullying and harassment
In August 2016 Djerriwarrh Health Services (DjHS) celebrated the launch of its new values program, with staff functions at every service site.
After the program launch, the important work of holding values-based conversations in everyday work began.
In other words, time to start putting words into actions and ensure values are embedded into all the work undertaken at DjHS.
By developing a values-driven culture and enacting the program fully, DjHS will ensure expected behaviours occur naturally and unconsciously – and become a normal part of workplace language and behaviours.
DjHS understands the potential impact of workplace culture on individuals’ health and wellbeing and has chosen CLEAR values of:• Compassion• Leadership• Excellence• Accountability • Responsibility
Training in Bullying and Harassment and Social Media are mandatory competencies for all DjHS staff, with more than three quarters completing both requirements as part of a commitment to eliminate bullying.

15Djerriwarrh Health Services Quality Account Report 2016
2.3 Positive workplace culture and prevention of bullying and harassment
Bullying and harassment
75%
80%
85%
90%
Bullying and Harassment
Social Media
50
60
70
80
40
30
20
10
0
Personally experienced bullying
at work in the last 12 months
Personally experienced bullying
and submitted a formal complaint
Were you satisfied with the way your formal complaint was handled?
Even though Djerriwarrh Health Services (DjHS) is below the state average of staff who report having experienced bullying at work in the previous 12 months as indicated in the People Matters Survey, we recognise there is still work to be done. We are committed to providing our staff and managers with education, training and reviewing our procedures to ensure they are effective.
MENTAL HEALTHThe annual staff health and wellbeing survey canvasses all Djerriwarrh Health Services staff members regarding their health behaviours and their opinions of the workplace environment. The data below is sourced from the 2015 Djerriwarrh Health Services staff health and wellbeing survey.
By management
DjHS is committed to supporting health within the organisation. As a health promoting workplace we create social, economic, cultural and physical environments that support health. We do this by strengthening the understanding and the skills of individuals to create and maintain health for themselves, for their families and their communities.
1 in 3 respondents reported feeling stressed often or very often, with an increase of 8% since 2014.
70.24% reported they found their workplace generally supportive, though the perception of support decreased with each level of management.
2014 74.78%
201567.85%
Undecided 2.41%
Very often 10.84%
Often 25.30%
Slightly often 39.76%
Not often 21.69%
YES
NO
2014 57.39%
201552.38%
Mandatory Competency People Matters Survey
Staff stress rateFeelings of support
16 Djerriwarrh Health Services Quality Account Report 2016
2.4 2015 Staff survey results and programs improvement2015 staff wellbeing at DjHS
WHO WE ARE
HEALTH STATUS
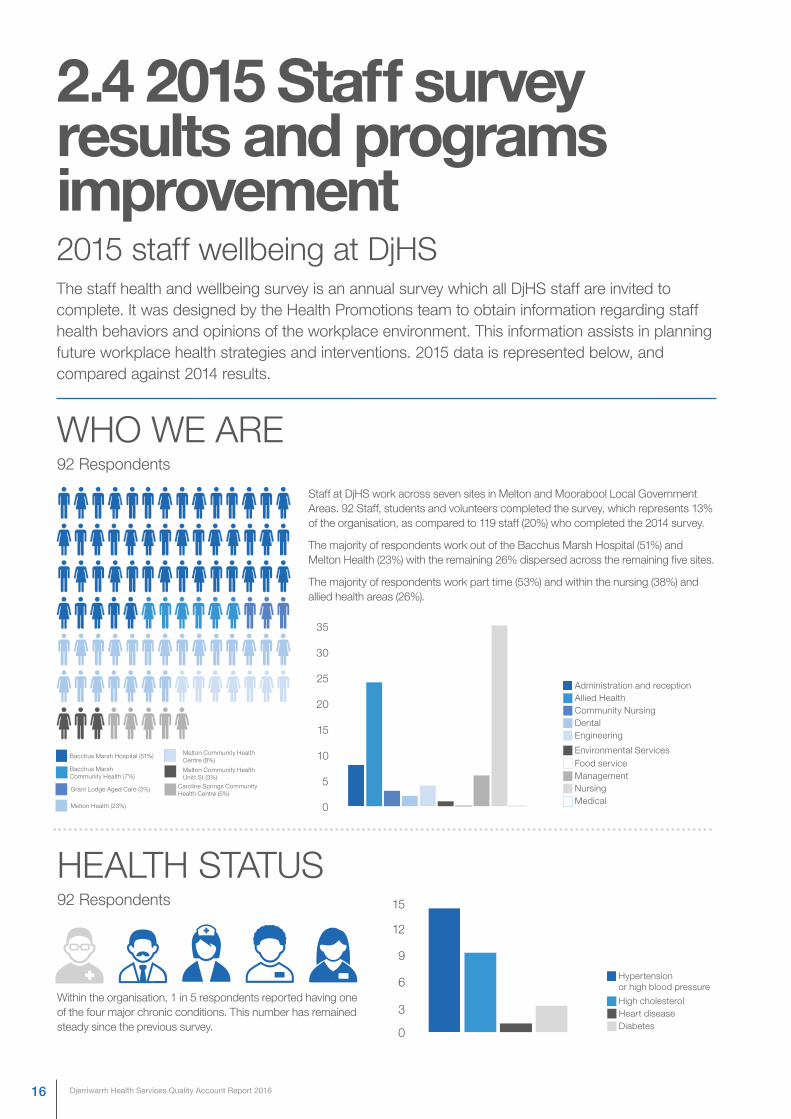
The staff health and wellbeing survey is an annual survey which all DjHS staff are invited to complete. It was designed by the Health Promotions team to obtain information regarding staff health behaviors and opinions of the workplace environment. This information assists in planning future workplace health strategies and interventions. 2015 data is represented below, and compared against 2014 results.
Staff at DjHS work across seven sites in Melton and Moorabool Local Government Areas. 92 Staff, students and volunteers completed the survey, which represents 13% of the organisation, as compared to 119 staff (20%) who completed the 2014 survey.
The majority of respondents work out of the Bacchus Marsh Hospital (51%) and Melton Health (23%) with the remaining 26% dispersed across the remaining five sites.
The majority of respondents work part time (53%) and within the nursing (38%) and allied health areas (26%).
Within the organisation, 1 in 5 respondents reported having one of the four major chronic conditions. This number has remained steady since the previous survey.
92 Respondents
92 Respondents
Bacchus Marsh Hospital (51%)
Grant Lodge Aged Care (3%)
Melton Community Health Centre (8%)
Melton Community Health Unitt St (3%)
Caroline Springs Community Health Centre (5%)
Bacchus Marsh Community Health (7%)
Melton Health (23%) 0
0
3
6
9
12
15
Administration and reception
Hypertension or high blood pressure
Allied Health
High cholesterol
Community NursingDentalEngineering
Environmental ServicesFood serviceManagement
Heart disease
Nursing
Diabetes
Medical
5
10
15
20
25
30
35

17Djerriwarrh Health Services Quality Account Report 2016
FOOD AND DRINKPHYSICAL ACTIVITY
The Australian Dietary Guidelines recommend a minimum 6–8 glasses of water per day.
The Australian Dietary Guidelines recommend a minimum of 5 serves of vegetables and 2 serves of fruit per day for adults over 18.
26% of respondents in 2015 and 35% or respondents in 2014 told us they were drinking 7 or more glasses of water per day.
11% of respondents in 2015 and 12% or respondents in 2014 told us they were eating the recommended 5 serves of vegetables or more, while 74% of respondents in 2015 and 80% in 2014 reported eating the recommended serves of fruit.
The number of people who are aware of the recommended 5 serves of vegetables and 2 serves of fruit has increased from 48% to 53% across the same period.
Desk job26.09%
Active enough28.26%
Not encouraged20.65
No time34.78% | 26.09%
Too tired47.83%
Not motivated22.83%
Shift work17.39%
Decreased sick leave absenteeism by 25.3%
Decreased worker compensation costs by 40.7%
Decrease disability management costs by 24.2%
Save $5.81 for every $1 invested in employee health
and wellbeing.
92 Respondents
The main ways staff reported being active during work hours were:
• Take a walk
• Get up and move around
• Break to stretch
• Chat with colleagues
1 in 5 respondents reported that they met the World Health Organisation guidelines of 30 minutes or more physical activity during the day.
92 Respondents
What prevents you from being physically active?
+
HEALTH PROMOTIONSuccessful health and wellbeing programs provide an excellent return on investment. One meta-evaluation looking at economic return of worksite health promotion programs found that such programs:
Healthy working environments can improve productivity, staff morale and enhance the ability of an organisation to attract and retain staff. It can also decrease staff turnover, absenteeism, accidents and injuries, and worker compensation claims.
This is a 4% decrease from 2014. 1 in 4 reported that they spend 6 or more hours sitting during the day.
Inside work Outside work

18 Djerriwarrh Health Services Quality Account Report 2016
2.5 Accreditation status
ACCREDITATION BY THE AUSTRALIAN COUNCIL OF HEALTHCARE STANDARDS
In July 2015 the Australian Council on Healthcare Standards (ACHS) undertook a full assessment of Djerriwarrh Health Services (DjHS). Following its assessment, the ACHS issued 43 quality improvement recommendations to implement within 90 days in order for DjHS to secure accreditation.
Of the 43 recommendations, 39 related to the Governance for Safety and Quality in Health Service Organisations. The remaining four related to Standard 9: Recognising and responding to clinical deterioration in acute healthcare.
In response, DjHS developed a detailed plan to implement the required improvements with an improvement action plan and working groups to address all ACHS recommendations.
A new governance committee structure was established to improve reporting, identification, analysis and monitoring of adverse incidents.
These new committees allowed a cross-section of medical professionals to come together and share information, develop trust in the clinical review process, and share best practice information and evidence. The committees also developed key clinical indicators, benchmarks and trends that monitored outcomes for patients, staff and the Board and identified areas for improvement.
This all ensures better communication across the organisation and a greater capacity to independently identify and review adverse incidents and events.
Other actions and improvements put in place by DjHS in response to the ACHS assessment included:
• Establishment of a new, robust clinical governance structure by DjHS Administrator, Dr John Ballard
• Appointment of experienced Chief Executive Andrew Freeman to lead a new management team
• Recruitment of new senior clinical practitioners• Greater investment in equipment and training to
improve standards of care• Engaged additional support to DjHS from the
Department of Health and Human Services, Western Health and the Royal Women’s Hospital
• Development and implementation of new organisational values of Compassion, Leadership, Excellence, Accountability and Respect
• Commitment to continuous improvement of clinical effectiveness and outcomes through robust monitoring, review, analysis and improvement
• Development of ongoing education and skills training for clinicians
• Greater engagement with local communities in planning, designing, measuring and evaluating the health service and patient experience
• Inclusion of community representation in the clinical governance structure
The rapid implementation of this program to secure accreditation brought significant and substantial change for the service and its staff. It has fundamentally improved DjHS and ensured the health service is fit to serve the communities of Bacchus Marsh, Melton and Caroline Springs.
In late January 2016 the ACHS re-assessed DjHS and confirmed it had met all requirements for accreditation.

19Djerriwarrh Health Services Quality Account Report 2016
2.6 Adverse events
THE WALLACE REPORT
In March 2015 the Department of Health and Human Services (DHHS) was notified by the Consultative Council of Obstetric and Paediatric Mortality and Morbidity (CCOPMM) that a cluster of perinatal deaths had occurred in 2013 and 2014 at Djerriwarrh Health Services.
The Department commissioned an independent review by Professor Euan Wallace, a senior obstetrician who concluded that seven of the 11 cases demonstrated deficiencies in clinical care.
Professor Wallace’s independent review made 10 recommendations for improvements for implementation in 2015–16. Nine of these required change specific to DjHS.
As well as the independent review, the Minister for Health appointed Dr John Ballard as Administrator on 27 October 2015 under section 61(2) of the Health Services Act 1988.
With support from Western Health and The Royal Women’s Hospital, all nine of Professor Wallace’s recommendations have been implemented. These include:
• Establishment of 24/7 on-call paediatric cover for newborns
• Monthly multidisciplinary Perinatal Mortality and Morbidity Review meetings with input from Western Health
• Weekly maternity and neonatal clinical meetings with staff to facilitate team communication, review clinical activity and identify issues and planning opportunities
• Development of a set of clinical indicators that allows DjHS to accurately monitor clinical outcomes and report these to the board
• Provision of Maternity Services Education Program (MSEP) training for all maternity and obstetrics staff in conjunction with the Royal Women’s Hospital
• Purchase of eight cardiotocography (CTG) machines and a centralised electronic fetal surveillance and alert system to allow for early detection of potential problems
• Provision of formal Fetal Surveillance Education Program (FSEP) training for all medical and midwifery staff. FSEP training is also now mandatory for all staff on an annual basis. At least two FSEP Level III (highest level possible) trained staff are now rostered on to service every birth suite shift at DjHS
• Appointment of a Clinical Resource Midwife as well as implementation of a new rostering process which ensures shift overlap between staff members

20 Djerriwarrh Health Services Quality Account Report 2016
2.7 Quality indicators including Staphylococcus aureus bacteraemia rate
BACKGROUND
• Bloodstream Infections (BSIs) are common and can cause significant illness and death
• More than half of these infections are associated with procedures performed in healthcare facilities
• Patients who develop BSIs whilst in hospital are more likely to suffer complications during their hospital stay, often resulting in increased length of stay and increased healthcare costs
• Staphylococcus aureus bacteraemia is the most common cause of healthcare associated bloodstream infections
• Patients who are immunocompromised, on haemodialysis, or in Intensive Care Units (ICUs) are more likely to develop a healthcare-associated BSI
• Quality improvement activities include surveillance
involving monitoring and reporting of Staphylococcus aureus bacteraemia to relevant State jurisdictions that are then reported into a national database for benchmarking and research
• The use of intravascular catheters is the most common medical procedure associated with bloodstream infections
ACTIONS TO ADDRESS STAPHYLOCOCCUS AUREUS BACTERAEMIA RATES
• In 2008, Australian Health Ministers endorsed that all hospitals monitor and report Staphylococcus aureus bacteraemias. Staphylococcus aureus rates are included as a Key Performance Indicator in National Health Services Agreement performance
• As a result of this Agreement, all public hospitals including psychiatric hospitals – but excluding residential aged care beds – must perform Staphylococcus aureus surveillance
• Djerriwarrh Health Services (DjHS) conducts continuous surveillance for Staphylococcus aureus rates using the Victorian Healthcare Associated Infection Surveillance System (VICNISS) Staphylococcus aureus surveillance module in line with Victorian Government legislation
• This provides a method to count Staphylococcus aureus bacteraemia and seek guidance about how to investigate the causes and the prevention of healthcare-associated Staphylococcus bacteraemias
• VICNISS has developed competency units for Infection
Control Practitioners. This helps validate data to ensure Infection Control Practitioners have the knowledge required to rigorously adhere to VICNISS protocols to generate correct denominator data and correctly identify infection events such as Staphylococcus aureus bacteraemias
• Infection Control Practitioners at DjHS have completed the VICNISS competency units to support their practice

21Djerriwarrh Health Services Quality Account Report 2016
2.7 Quality indicators including Staphylococcus aureus bacteraemia rate
EVIDENCE OF QUALITY & SAFETY
• Staphylococcus aureus bacteraemia surveillance includes all patients admitted to DjHS with a bloodstream infection, a bacteraemia caused by Staphylococcus aureus
• When a positive blood culture occurs at DjHS it is reviewed by a healthcare worker trained in infection control to determine if the clinical criteria meet the Staphylococcus aureus bacteraemia definition. This will be an Infection Control Consultant employed by the health service supported by an Infectious Diseases Physician when required
• Every healthcare-associated bacteraemia is investigated to identify the cause, and corrective action is initiated to prevent escalation and future infections
• DjHS collects and submits data to VICNISS monthly with a report generated from VICNISS quarterly
• VICNISS Staphylococcus aureus bacteraemia reports show there have been no reportable Staphylococcus bacteraemias at DjHS in 2015–16.

22 Djerriwarrh Health Services Quality Account Report 2016
2.8 Hand hygiene compliance and influenza immunisation
BACKGROUND
Hand Hygiene is essential in the prevention and control of healthcare-associated infections, and protects staff and consumers.
The “5 Moments for Hand Hygiene” was developed by the World Health Organisation in 2009 and adopted by Hand Hygiene Australia in 2008.
The aim of Hand Hygiene is to:
• protect patients from acquiring infectious agents from the hands of healthcare workers
• help protect patients from infectious agents (including their own) entering their bodies during procedures
• protect healthcare workers and the healthcare surroundings from acquiring patients’ infectious agents
Hand Hygiene is performed:• using soap and water to wash and dry hands thoroughly;
or• using waterless hand rubs, such as alcohol-based
hand rubs
The “5 Moments for Hand Hygiene” must be practised by all staff for all patient care:
1. Before touching a patient
2. Before any procedures on a patient
3. After body fluid exposure or risk
4. After touching a patient
5. After touching a patient’s surroundings
Healthcare workers must perform Hand Hygiene before and after every patient contact, to prevent patients becoming colonised with healthcare-associated organisms from other patients and the healthcare environment.
Emphasis is placed on preventing the transfer of organisms from a contaminated body site to a clean body site during patient care. Hand hygiene must also be performed after contact with objects such as medical charts and equipment.
ACTIONS
Djerriwarrh Health Services’ (DjHS) staff Hand Hygiene compliance is measured by Gold Standard auditors who complete an annual auditor’s competency module with Hand Hygiene Australia.
There are three audit periods annually with results reported to the Victorian Government and to all levels of governance within the health service, in line with legislative requirements. The Victorian Government has set a compulsory compliance rate of 80 per cent.
Clinical units also post unit results on the “Knowing How We Are Doing” board. One DjHS Gold Standard auditor was selected by Hand Hygiene Australia to assess and validate the expertise of auditors throughout the Grampians Region.
Two staff members were selected from clinical areas to undertake the general Hand Hygiene auditor’s education module to encourage ownership of the Hand Hygiene program in individual clinical areas and promote compliance.
EVIDENCE OF QUALITY & SAFETY:
There has been a huge effort throughout DjHS to increase the visibility and importance of Hand Hygiene. Large Hand Hygiene stations, designed by a staff member, have been set up at all entrances to DjHS sites to encourage patients, visitors and staff to practise Hand Hygiene on entry.
Smaller Hand Hygiene stations have been placed outside all patient wards and clinical consulting rooms in DjHS community health centres.

23Djerriwarrh Health Services Quality Account Report 2016
2.8 Hand hygiene compliance and influenza immunisation
Audit Period Bacchus Marsh Campus Melton Health Campus Target
Audit 1 – 2015 82.2% 85.3% 77%
Audit 2 – 2015 84.6% 88.5% 80%
Audit 3 – 2015 86.9% 89.6% 80%
Audit 1 – 2016 87.4% 88% 80%
Audit 2 – 2016 87.7% 89.3% 80%
There has been significant improvement in Hand Hygiene compliance at DjHS, reflecting a strong cultural shift. We are striving to improve these results in 2016–17.

24 Djerriwarrh Health Services Quality Account Report 2016
2.8 Hand hygiene compliance and influenza immunisation
BACKGROUND
Influenza is caused by Influenza A and B viruses, which can result in minor or major epidemics of seasonal influenza most years – and usually during winter.
Those most affected are usually the frail and the elderly or people with pre-existing serious chronic illness, but anyone can get sick from the ‘flu.
The disease may be short-lived with mild symptoms and a few muscle aches; or a severe illness with muscle aches, feeling dreadful, high temperature, chills and uncontrollable shakes right through to life-threatening pneumonia and even organ failure.
The influenza virus is spread through droplets and contact with virus-contaminated equipment, so infection control
precautions such as Hand Hygiene, patient isolation and use of personal protective equipment (PPE) are essential.
Influenza vaccination is not compulsory, but all direct clinical staff at Djerriwarrh Health Services (DjHS) are encouraged to be vaccinated, based on the risk they may be exposed to and transmit the disease to co-workers, vulnerable patients and their families.
Maintaining a high level of immunity among healthcare workers helps to minimise the risk of transmission.
In 2016 healthcare workers were immunised with a quadrivalent vaccine that covered all four the circulating viruses. Vaccine immunity lasts about one year, and so it’s important to receive an influenza vaccination annually.
EVIDENCE OF QUALITY AND SAFETY
• DjHS achieved a vaccination compliance rate of 78.1 per cent for 2016
• Data was submitted for all DjHS campuses: Bacchus Marsh, Melton Health, Melton Community Health and Caroline Springs

25Djerriwarrh Health Services Quality Account Report 2016
2.8 Hand hygiene compliance and influenza immunisation
INITIATIVES TO BOOST AND ENCOURAGE VACCINATION
• Mobile/roaming vaccination trolleys visiting all clinical areas
• Frequent vaccination sessions at all campuses
• Face-to-face influenza education and discussion
• Influenza presentation posted to the intranet for staff unable to attend face-to-face sessions
• Posters and promotional material on display, with progressive tally of compliance charted in clinical areas
• Lollipops to reward all staff being vaccinated
• High visibility vests showing an animated “flu bug” worn by vaccinators
• Vaccinated “flu bug” stickers for staff name badges following vaccination
• Community vaccinations for primary school teachers, Disability Industrial Workshop and Country Fire Authority to increase “herd immunity” in the community
• DjHS senior leadership support for staff participation in the program
EVIDENCE OF QUALITY AND SAFETY
• Use a tissue when coughing or sneezing
• Stay at home if you have flu-like symptoms
• Dispose of tissues into the bin and wash your hands
• The best way to protect yourself and others from the flu is to get vaccinated
INFLUENZA VACCINATION 2016
Total Vaccines Given:
Category Total Staff Employed Total Staff Vaccinated % Vaccinated % Target
Victorian Public Health Services
114,957 91,831 79.9% 75%
Djerriwarrh Health Services
611 477 78.1% 75%

26 Djerriwarrh Health Services Quality Account Report 2016
2.9 Victorian perinatal services performance indicators
Data from 2013–2014 covered a period where birth numbers at Djerriwarrh Health Services increased dramatically, and at the same time a number of significant adverse events occurred – which have been subject to wide scrutiny.
It is important to note how much has changed in the provision of maternity care at Djerriwarrh. Victorian perinatal services performance indicators are 10 statewide indicators whose collation improves outcomes for Victorian women and their babies.
Indicator 2: Term infants without congenital abnormalities who require additional care
This indicator focuses on the quality of care immediately before and after birth. Djerriwarrh Health Services’ rate of 2.8 per cent was well below the state average of eight per cent.
Indicator 4: Rate of women who plan for a vaginal birth after a caesarean birth in Victorian public hospitals
Caesarean section can be a lifesaving procedure. It is, however, associated with greater health risks for the mother and her baby. Having a caesarean for the first birth greatly increases the need for a Caesarean birth with subsequent births. Careful consideration of a vaginal birth after a Caesarean birth provides the mother and her care team an opportunity to consider giving birth naturally. Djerriwarrh’s natural choice rate of 34.1 per cent compares with the state average of 27.9 per cent. Results in 2013 reflect a stronger commitment to collaborative working with expectant mothers.

27Djerriwarrh Health Services Quality Account Report 2016
2.10 Victorian Audit of Surgical Mortality
Djerriwarrh Health Services (DjHS) annual data from the Victorian Audit of surgical Mortality (VAMS) was received in July 2016 and notes no surgery-related deaths at Djerriwarrh for a very long time.
Learnings from the VAMS program are used and shared by surgeons and all operating theatre, post-operative nursing and allied health staff.
SURGICAL SERVICES REVIEW
In November 2015 Professor David Watters and Professor Ian Gough were asked by the Department of Health and Human Services (DHHS) to review DjHS’s surgical service and concluded the service to be, overall, very safe.
Professor Watters and Professor Gough noted an important reality of DjHS was that all 16 visiting surgeons
also worked at other hospitals. Their review identified this is a risk in clinical handover and information. As a result DjHS has significantly improved communication with the visiting surgeons, by completion of surveys to canvass views and providing regular updates about DjHS by group emails.
SURGICAL AUDIT AT DJHS
In 2016 DjHS launched a virtual surgical audit program after DHHS started providing quarterly data on the outcomes for DjHS surgical patients with post-operative complications who do not return to DjHS for care. This data is now shared with surgeons on an individual basis. Surgeons are provided with a series of questions to ensure cases are being reviewed at another hospital, that lessons can be learned, and continuous improvements can be made at DjHS.
The data and completed review questions are the subject of a twice-yearly review with surgeons, completed by telephone.

28 Djerriwarrh Health Services Quality Account Report 2016
2.11 Residential aged care indicators
Djerriwarrh Health Services (DjHS) is part of the National Aged Care Quality Indicator program. This program measures five key areas of care for people in residential aged care. Monitoring these key areas and regularly canvassing active feedback from residents and families means services can be continually fine-tuned and improved.
CASE STUDY – PAULA’S STORY
Paula (not her real name) is an 88-year-old woman who lives at DjHS’s Grant Lodge facility. She has dementia and
is often sleepy during the day and agitated in the evening. The National Aged Care Quality Indicator program identified that Paula was using more than nine different medications, some of which she had been taking for many years. This prompted staff at Grant Lodge to request a full review of Paula’s medication intake.
Following the review, her pharmacist and general practitioner agreed she could reduce her medication; one medicine was changed and administered at a different time of day meaning Paula was less sleepy during the day, experienced fewer periods of agitation, and had an improved quality of life at Grant Lodge.
Grant is slightly higher than the state average in the areas of nine or more medications, falls, unplanned weight loss and pressure injuries. These indicators are reported on a monthly basis to the DjHS Residential Aged Care Services Committee. Research is continuing to establish the reasons for this and how Djerriwarrh Health Services can address and improve the situation.
Rate per 1000 Bed Days
9 or more Medications
Falls Use of Restraints Unplanned Weight Loss
Pressure Injuries0
2
4
6
8
12
10 State
Grant Lodge

29Djerriwarrh Health Services Quality Account Report 2016
2.14 Quality improvement
Djerriwarrh concentrates on improving community health and wellbeing from the beginning of a patient’s journey.
Improving care and services can make a big difference in the antenatal period, and as part of the improvement at Djerriwarrh, all staff working in Maternity Services are
required to complete the Fetal Surveillance Education Program (FSEP). This program increases staff knowledge, skills and ability to assess the baby before birth to identify, prevent and manage any potential problems. All the evidence supports good antenatal care, and regular assessment of fetal development assists in planning for the best possible birth.

Continuity of care
3.
31Djerriwarrh Health Services Quality Account Report 2016
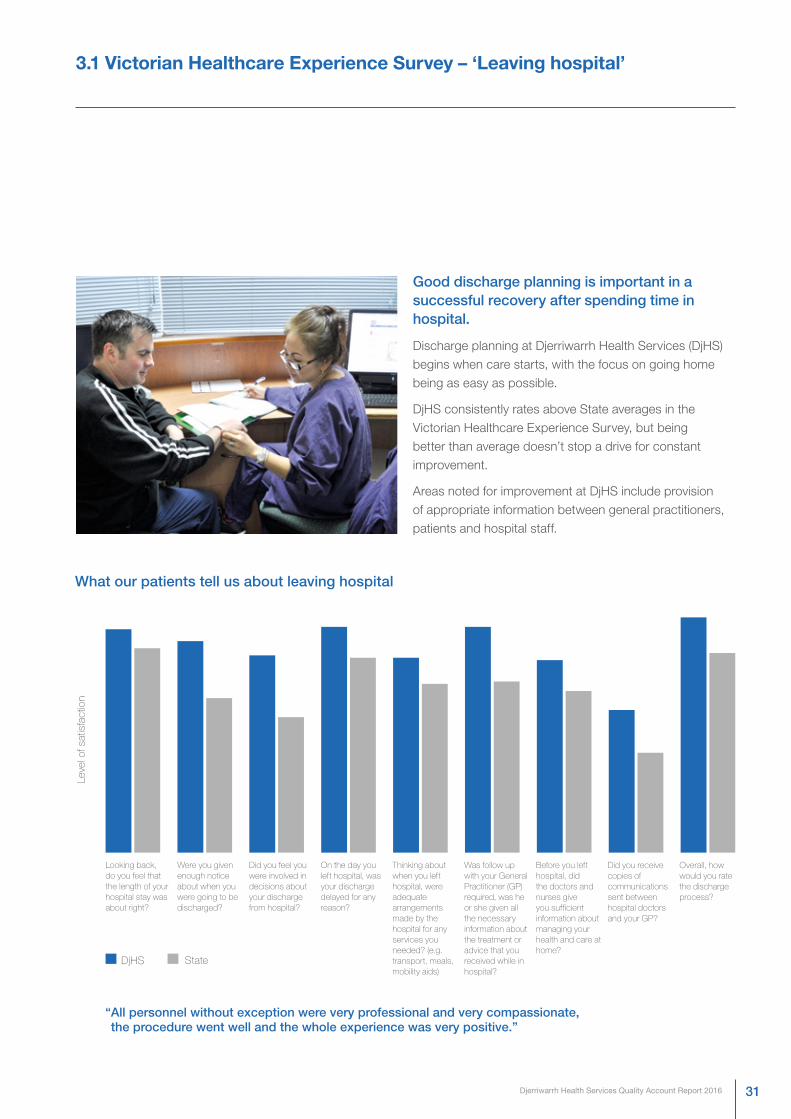
3.1 Victorian Healthcare Experience Survey – ‘Leaving hospital’
Good discharge planning is important in a successful recovery after spending time in hospital.
Discharge planning at Djerriwarrh Health Services (DjHS) begins when care starts, with the focus on going home being as easy as possible.
DjHS consistently rates above State averages in the Victorian Healthcare Experience Survey, but being better than average doesn’t stop a drive for constant improvement.
Areas noted for improvement at DjHS include provision of appropriate information between general practitioners, patients and hospital staff.
Looking back, do you feel that the length of your hospital stay was about right?
Were you given enough notice about when you were going to be discharged?
Did you feel you were involved in decisions about your discharge from hospital?
On the day you left hospital, was your discharge delayed for any reason?
Thinking about when you left hospital, were adequate arrangements made by the hospital for anyservices you needed? (e.g. transport, meals, mobility aids)
Was follow up with your General Practitioner (GP) required, was he or she given all the necessaryinformation about the treatment or advice that you received while in hospital?
Before you left hospital, did the doctors and nurses give you sufficient information about managing yourhealth and care at home?
Did you receive copies of communications sent between hospital doctors and your GP?
Overall, how would you rate the discharge process?
Leve
l of s
atis
fact
ion
StateDjHS
“ All personnel without exception were very professional and very compassionate, the procedure went well and the whole experience was very positive.”
What our patients tell us about leaving hospital

32 Djerriwarrh Health Services Quality Account Report 2016
3.2 Continuum of care
BACKGROUND
Managing the rising cost of healthcare is a major challenge for people in Djerriwarrh Health Services’ (DjHS) area that crosses the Shire of Moorobool and City of Melton.
As part of its planning for future healthcare, DjHS participated in Australia’s first large-scale telehealth clinical trial, funded by the Australian Government Broadband Enabled Telehealth Pilots Program.
Following the trial, DjHS proceeded with the continuum of care, using telehealth home monitoring to deliver health related services and information. The capabilities offered by fast broadband infrastructure and rapid advances in health technologies have revolutionised delivery of health services for chronic disease management particularly in remote or regional communities.
AIM
Individuals with poorly controlled diabetes are a high cost to the health system as they typically have a combination of complex medical conditions, and in many cases frequently visit the hospital.
Telehealth services can help people with chronic diseases such as diabetes to better self-manage their conditions
at home and reduce hospital admissions. This system uses a home monitor with a large screen to guide patients through different procedures such as taking blood pressure, recording blood oxygen, blood glucose, electrocardiogram, body temperature, body weight, spirometry and provide answers to clinical questionnaires if a trend is picked up by the telehealth nurse.
RESULT
Results show that clients involved in telehealth home monitoring are uniformly positive about the benefits of the telemonitoring and report increasing awareness of their conditions and a much greater capacity for self-management. Many examples where an exacerbation
in the patient’s condition has been detected and early intervention either avoided hospitalisation or resulted in a better outcome of haemoglobin A1C (HbA1C) have been observed.
CONCLUSION
Intervention can prevent hospitalisations, reduce length of stay, reduce social dislocation and improve quality of life. Home telemonitoring enables clients to monitor their own health variables in their own homes. This has been shown to deliver cost-effective, timely and improved access to quality care. Improvements in technology are reducing the need for travel, providing timely access to services,
improving the ability to identify developing conditions, and providing new ways to educate and support management of chronic conditions. Consequently it has the potential to reduce the burden on the healthcare system by providing more affordable strategies to support individuals to effectively self-manage their conditions such as diabetes.

33Djerriwarrh Health Services Quality Account Report 2016
3.2 Continuum of care
The CSIRO Telehealth Trial Final Report makes a significant contribution to quantifying the effects of introducing at home telemonitoring of vital signs to manage a heterogeneous group of chronically ill patients.
In addition this project reports on the effect of workplace culture, capacity for innovation and organisational change management in successfully integrating a new model of care with long-established service models. The report clearly documents that success metrics for deploying telehealth services relate more to on-site clinical leadership, capacity to accommodate change and flexibility of existing processes and systems – than any technical issues associated with the telehealth monitoring equipment or patient adherence to measurement schedules.
The availability of such a rich set of patient data has allowed development of a sophisticated risk stratification system. Daily records of vital signs and questionnaire responses were used to identify statistically significant changes in these variables which are likely to indicate an exacerbation of the patient’s chronic condition.
Results from Home Monitoring Results from CSIRO Research
Reduces need for travel Assess changes in clients conditions remotely
Provides timely access to services and early intervention Provide appropriate care interventions earlier
Improves ability to identify developing conditions Help clients stay out hospital
New ways to self-educate and self-manage chronic conditions Improve clients’ quality of life
Achieved HbA1c outcome to target Deliver cost-effective services
Improved glycaemic control Deliver timely and improved access to quality care
Identified sleep apnoea Enhance self-management
Delay need for starting dialysis and early intervention for cardiac events Help reduce social dislocation and enhance quality of life

34 Djerriwarrh Health Services Quality Account Report 2016
3.3 Continuum of care case study
Better outcomes for patients by working together
CASE STUDY 1
Mr W is 69-years old and lives in Greendale, a small town in the Moorabool Shire. He cares for his 97-year-old mother at home, and was referred by his GP for managing his insulin adjustment.
Mr W’s diabetes had progressed following finding cancer in fifth vertebrae in the spine that required a surgical intervention with two rods, one bracket and 10 screws inserted.
He was required to attend eight months of weekly chemotherapy with travel to Ballarat and his carer’s responsibilities. When Mr W was referred, his HbA1C was 10 per cent.
Priority for Mr W was having his chemotherapy and balancing his role as a carer. Telehealth home monitoring was recommended, and Mr W’s diabetes has been managed remotely and virtually.
This has reduced the burden of travel, provided time for Mr W to concentrate on his health condition, freed time for him to spend caring for his Mother, early intervention for managing his glycaemic control to prevent complications, achieving HbA1C target and a significant financial benefit.
CASE STUDY 2
Mr G and Mr R were both diagnosed with type 2 diabetes.
When they were seen by the endocrinologist, further testing led to findings of type 1 diabetes.
While managing diabetes takes a toll at any time, it is even more challenging learning of a differential diagnosis and having to have basal/bolus insulin injections daily for the rest of their lives.
Telehealth home monitoring discussions was proposed to Mr G and Mr R and both accepted the new concept as a way to reduce anxiety about managing insulin dosing, and reducing frequency of appointments. It also means data is monitored daily and early intervention is established.
Mr R attended Dose Adjustment For Normal Eating (DAFNE) training for his self-management. Following the training, Mr R still requires some support to build his confidence in self-management.
Telehealth home monitoring supports glycaemic control, but neither Mr G nor Mr R were aware of other health complexities. When they commenced remote monitoring, a trend of hypertensive events and ECG abnormalities was picked up.
Both were contacted and with further follow-up investigations by their GPs. Both have oral hypertensive agents reviewed. Mr R had a first degree heart block identified from his investigative procedures. Both have HbA1C in target range.
CASE STUDY 3
Ms A attended diabetes exercise group for her diabetes management plan.
On completion of a seven-week exercise program, Ms A felt her motivation would reduce. Remote monitoring was discussed and Ms A has been using telehealth home monitoring as a lifestyle self-management tool.
Ms A had to stop her monitoring as she is a carer for her sister with mental health and was hospitalised.
Ms A’s diabetes management was sub-optimal during this period and she was told by the endocrinologist she had to commence insulin. Ms A contacted the telehealth nurse coordinator to restart the monitoring. Her glycaemic control is now in target range and self-management has progressed.

35Djerriwarrh Health Services Quality Account Report 2016
3.4 Advance care planning and case study
Djerriwarrh Health Services (DjHS) saw nearly 2000 clients aged more than 75 in the 2015–16 financial year. Of those 1997 people, only 13 had an Advance Care Plan or an identified substitute decision-maker.
While this is a low base to start from, the percentage of people coming to DjHS with an Advance Care Plan or developing an plan during an episode of care is trending upwards. The aim is to increase year-on-year, with a 2016–17 target of four per cent of patients 75 years and older having an Advance Care Plan.
CASE STUDY
DjHS District Nursing had been providing daily medication for an 83-year-old client living at home alone. The client also received personal care three times weekly and shopping weekly.
Family members said their elderly relative’s cognition had declined, but there had been no GP visit to investigate, although it was recognised the person’s health was getting worse and a son had been granted legal medical Power of Attorney and a daughter as financial Power of Attorney.
The client had been admitted to hospital a number of times over six months due to falls and deconditioning, and the service had concerns over safety at home alone.
Residential care was not an option, and the preference was to stay at home.
After a further accident resulting in serious injuries, DjHS District Nursing organised an aged care assessment and a family meeting, where the son and daughter agreed it was time to trial a period of respite and possibly permanent placement in residential care.
Cognitive decline meant the client’s decision-making capabilities were compromised but with responsibility delegated to family, respite care was organised and the client later agreed to stay in residential care.
This experience demonstrates how an individual’s autonomy can be preserved through discussion and involvement of family or carers in decision-making and the pivotal role of a substitute decision-maker.
INCREASED UPTAKE OF ADVANCE CARE PLANS AT DJERRIWARRH HEALTH SERVICE
Incorporating the questions regarding an Advance Care Plan into the routine assessment of every client who comes into DjHS is already underway.
This will normalise the assessment and questions for clinical staff and people who visit DjHS, aligning with the Department of Health and Human Services’ Statement of Priorities, “Having the Conversation”.
Key staff who will become Advance Care Plan champions are being trained and will be a resource for all clinical staff and clients, providing positive role models and a sounding board for other clinicians to support participation in the Advance Care Plan process.
All DjHS staff are the target of an education program to raise awareness of Advance Care Planning as a client-centric process to increase autonomy in future healthcare decisions.
This includes reviewing current documentation to ensure it as user-friendly as possible for clinicians, clients, families and carers, and linking with community stakeholders including Primary Health Networks to share knowledge and resources.

36 Djerriwarrh Health Services Quality Account Report 2016
3.5 Organisational policy for end-of-life care
Djerriwarrh Health Services (DjHS) implemented its compulsory end-of-life policy in 2015.
The service also has in place an End-of-Life Care Pathway to guide multidisciplinary care based on comfort and dignity. It is respectful of patients’ choices, and aims to provide holistic end-of-life care in consultation with patients, family and carers.
In 2015–2016, 75 per cent of palliative care patients died at DjHS with an End-of-Life Care Pathway in place.
In the year ahead the focus will be on improving utilisation of the pathway to provide for all palliative care patients. This includes all palliative care patients whether at Djerriwarrh Health Services or at home.

37Djerriwarrh Health Services Quality Account Report 2016
Additional information for our community
WE APPRECIATE YOUR FEEDBACK
Please provide us with feedback on the form attached regarding our Quality Account Report or via ww.djhs.com.au
DISTRIBUTION OF THIS REPORT
The 2015–2016 Quality Account Report is distributed to healthcare partners, GP clinics and community leaders. Copies are available in Djerriwarrh Health Services foyers and for download from www.djhs.com.au
WHAT DO YOU THINK OF THIS REPORT?
Please complete this survey and return to:
Chief Executive, PO Box 330, Bacchus Marsh, Victoria, 3340
Was this report easy to understand? (please circle)
What did you like most about this report?
What information would you like to see in this report?
Do you have any suggestions or feedback on other services Djerriwarrh Health Services could offer the community?
Thank you for your comments.
YES NO

38 Djerriwarrh Health Services Quality Account Report 2016
ABOUT DJERRIWARRH HEALTH SERVICES
Djerriwarrh Health Services (DjHS) serves the rapidly expanding population areas of Melton and Moorabool Shires
BACCHUS MARSH AND MELTON REGIONAL HOSPITAL
A 42-bed acute hospital which includes 11 maternity beds, a wide range of theatre procedures, outpatient care and community health. Grant Lodge is a 30-bed residential aged care facility adjacent to the hospital
Tel: 03 5367 2000
MELTON HEALTH
Ambulatory care for Day Medical, Adult Health, Women and Children’s Health and Dental Services
Tel: 03 9747 7600
BACCHUS MARSH COMMUNITY HEALTH CENTRE
Allied health, counselling, community nursing and palliative care
Tel: 03 5367 4599
MELTON COMMUNITY HEALTH CENTRE
Allied health and counselling services
Tel: 03 8746 1100
CAROLINE SPRINGS COMMUNITY HEALTH CENTRE
General community health programs
Tel: 03 9361 9300

39Djerriwarrh Health Services Quality Account Report 2016

www.djhs.org.au | Djerriwarrh Health Services | ABN 83 271 740 698