q1 - heart failure in primary care · k. melissa hayes, dnp, anp-bc, chfn q1 1 'lvforvxuhv...
TRANSCRIPT

Outpatient Management of Heart Failure in Primary Care
National Nurse Practitioner Symposium July 2020
Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
1

Disclosures
Dr. Dellise has no disclosures.
Dr. Hayes had no disclosures.
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
2

Objectives
DISCUSS implications of heart failure management strategies highlighting key considerations for primary care.
IDENTIFY challenges of optimization of guideline-directed medical therapy in heart failure patients.
REVIEW the appropriate adjustment of heart failure medications according to the volume status of the patient.
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
3
Presentation Outline
~Background and significance
~Definitions; HFpEF vs HFrEF
~Cases_HFpEF ~Hospital to Home
~Cases_HFrEF ~Resources
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
4
AHA 2017 Heart Disease & Stroke Statistics Update, Heart Disease and Stroke Statistics—2010 Update: A Report From the American Heart Association Circulation, Feb 2010; 121: e46 - e215.
The number of adults living with heart failure has increased from about 5.7 million (2009-2012) to about 6.5 million (2011-2014).
One in 5 Americans will be >65 years of age by 2050.
HF incidence increases with age, rising from approximately 20 per 1000 individuals 65 to 69 years of age; to >80 per 1000 individuals among those ≥85 years of age.
960,000 new cases annually.
Hospital admissions rates have increased approximately 150% over the past 2 decades.
Half of the hospital admissions are patients with HFpEF.
Half of the hospital admissions are patients with HFrEF.
Heart Failure Facts
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
5

The number of Americans with HF is expected to significantly worsen in the future.
(Yancy, et al., 2013)
Getty Images / tiero
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
6

Definitions
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
7
Heart Failure
A complex clinical syndrome resulting from any structural or functional cardiac disorder that impairs
the ability of the ventricle to FILL with blood or EJECT blood. (Yancy, et al., 2013)
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
8
HFpEF vs HFrEF
Diastolic Failure - Heart Failure with Preserved Ejection Fraction (HFpEF) result of the inability of the heart to relax and FILL with blood (EF ≥ 45%)
Systolic Failure - Heart Failure with Reduced Ejection Fraction (HFrEF) result of the inability of the heart to EJECT blood (EF ≤ 40%)
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
9
Heart Failure Mid-Range EF (HFmEF)
Grey area with LVEF > 40 but no quite 50-55% HFmEF
Group treated based on symptomatology, etiology and usually end up being treated as LVEF HFrEF.
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
10
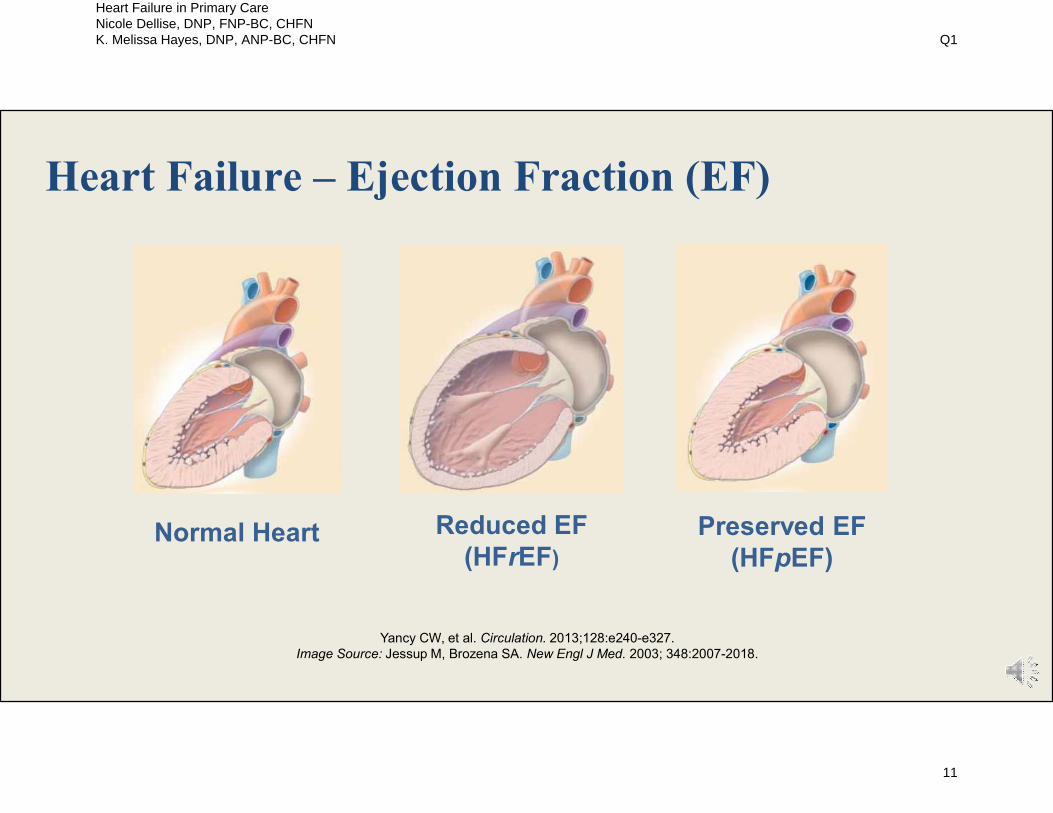
Yancy CW, et al. Circulation. 2013;128:e240-e327.Image Source: Jessup M, Brozena SA. New Engl J Med. 2003; 348:2007-2018.
Reduced EF (HFrEF)
Normal Heart Preserved EF (HFpEF)
Heart Failure – Ejection Fraction (EF)
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
11

Classifications of Heart Failure
Circulation 2013;128:e240-327.
Classification Ejection Fraction (EF)
Heart failure with reduced ejection fraction (HFrEF)• Formerly referred to as systolic heart failure
< 40%
Heart failure with preserved ejection fraction (HFpEF)• Formerly referred to as diastolic heart failure
> 50%
HFmEF borderline 41-49%
HFrEF improved - patients with a history of HFrEF > 40%
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
12

Brief Pathophysiology Review
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
13
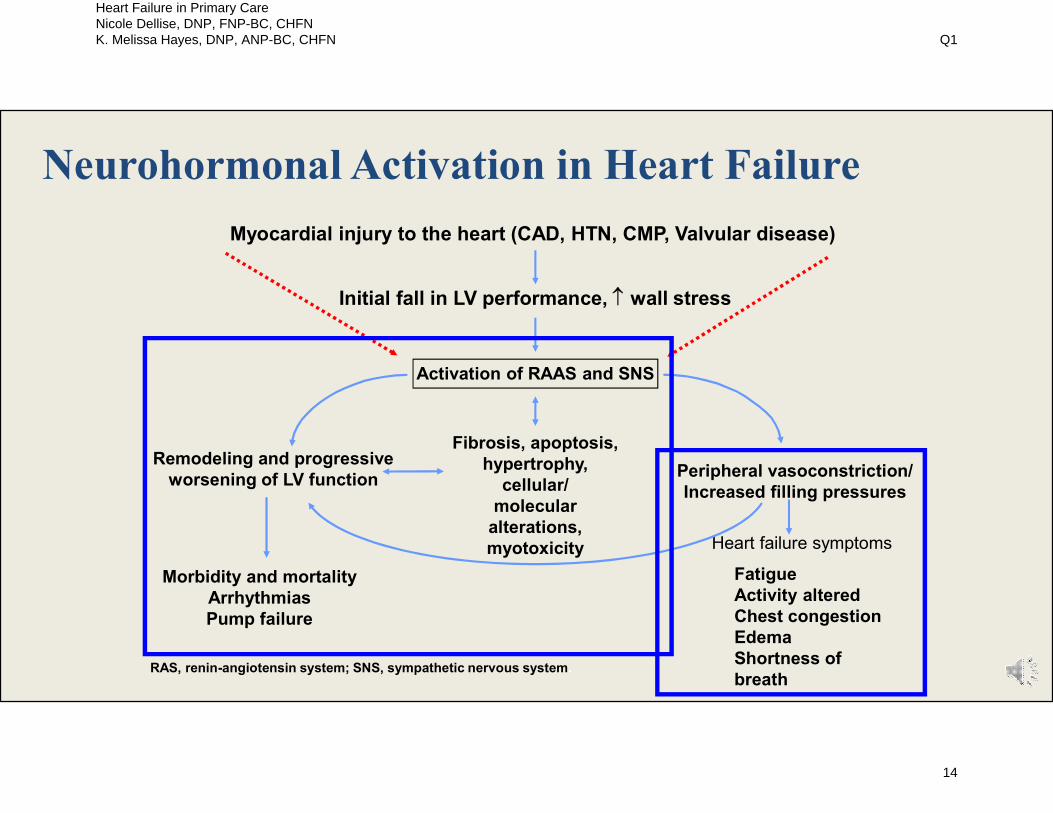
RAS, renin-angiotensin system; SNS, sympathetic nervous system.
Myocardial injury to the heart (CAD, HTN, CMP, Valvular disease)
Morbidity and mortalityArrhythmiasPump failure
Peripheral vasoconstriction/Increased filling pressures
Heart failure symptoms
Remodeling and progressiveworsening of LV function
Initial fall in LV performance, wall stress
Activation of RAAS and SNS
Fibrosis, apoptosis,hypertrophy,
cellular/molecular
alterations,myotoxicity
FatigueActivity altered Chest congestionEdemaShortness of breath
Neurohormonal Activation in Heart Failure
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
14

Altered gene expression Apoptosis
Remodeling
Pathogenesis of Heart Failure
Myocardial Insult
Myocardial Dysfunction
Renin-Angiotensin-Aldosterone Activation
Sympathetic Activation
Reduced Organ Perfusion
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
15
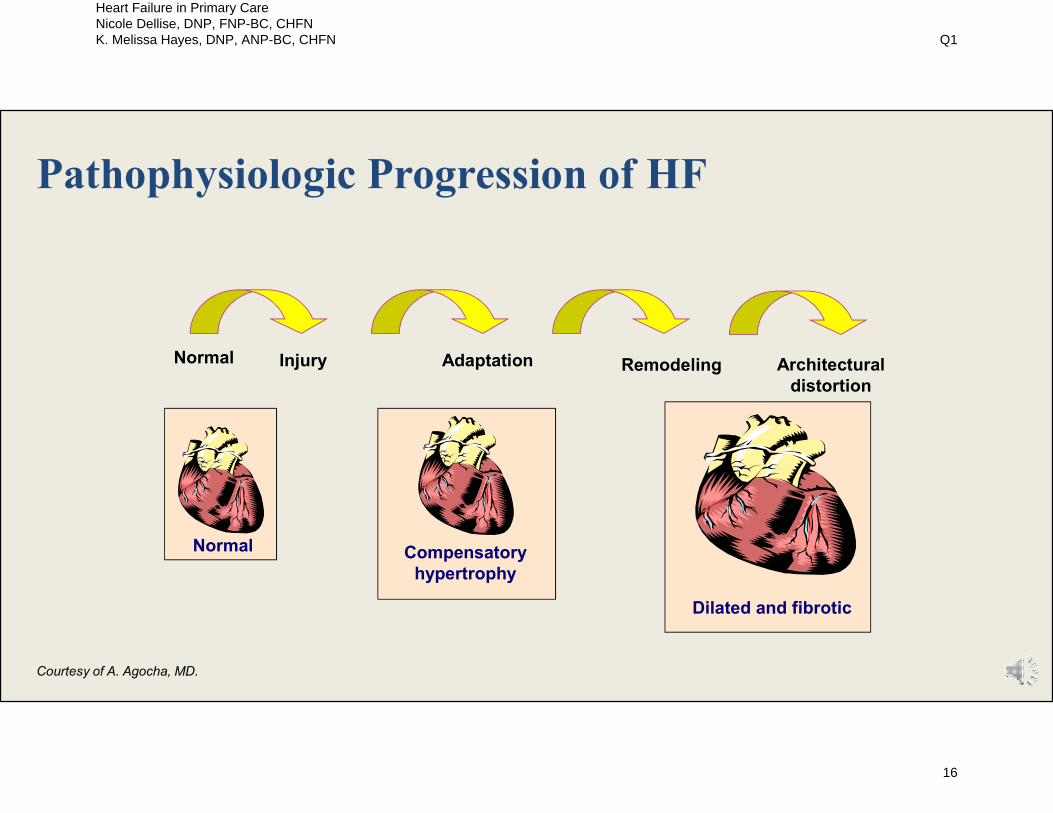
Pathophysiologic Progression of HF
Injury Adaptation Remodeling
Normal
Dilated and fibrotic
Compensatory hypertrophy
Architecturaldistortion
Normal
Courtesy of A. Agocha, MD.
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
16
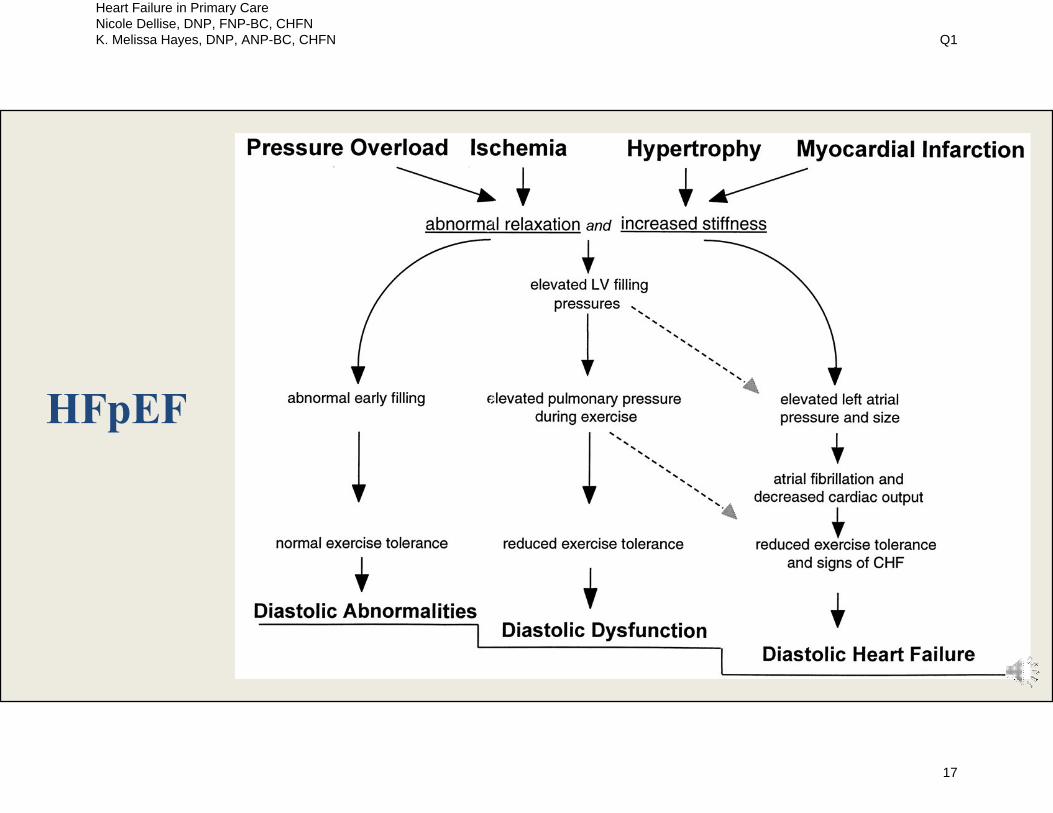
HFpEF
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
17

ACC/AHA HF Stage vs NYHA Class
ACC/AHA HF Stage
High risk for developing heart failure (HF) No structural disease
Structural heart diseaseNo HF symptoms
Structural heart diseasePrior or current HF symptoms
Refractory end-stage HFrequiring special interventions
Jessup M et al. N Engl J Med. 2003;348:2007-2018. New York Heart Association/Little Brown and Company, 1964. Adapted from Farrell et al. JAMA. 2002;287:890-897.
A
B
C
D
NYHAFunctional Class
Asymptomatic
Symptomatic with moderate exertion
Symptomatic with minimal exertion
Symptomatic at rest
Class I
Class II
Class IV
Class III
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
18

HFpEF HFrEF
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
19
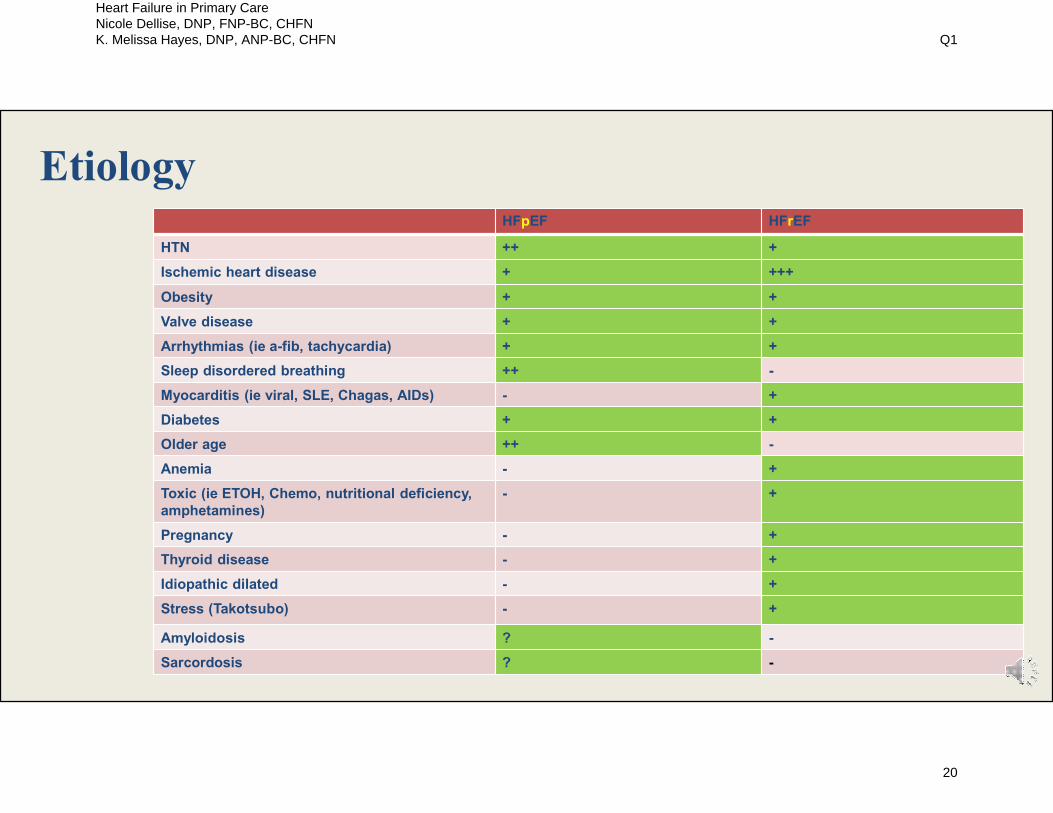
Etiology HFpEF HFrEF
HTN ++ +
Ischemic heart disease + +++
Obesity + +
Valve disease + +
Arrhythmias (ie a-fib, tachycardia) + +
Sleep disordered breathing ++ -
Myocarditis (ie viral, SLE, Chagas, AIDs) - +
Diabetes + +
Older age ++ -
Anemia - +
Toxic (ie ETOH, Chemo, nutritional deficiency, amphetamines)
- +
Pregnancy - +
Thyroid disease - +
Idiopathic dilated - +
Stress (Takotsubo) - +
Amyloidosis ? -
Sarcordosis ? -
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
20

Diagnostics HFpEF HFrEF
Signs and Symptoms of HF
+ +
Diagnosis of Exclusion + -
B-Type Nauturtic Peptide - or + ↓ ↑ + ↑↑
Chest X-Ray + +
ECG + +
Transthoracic Echocardiogram
+ +
Right heart Catherization + +
Stress testing + +
Left heart catherization + +
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
21

SymptomsHFpEF HFrEF
Dyspnea + +
Orthopnea + +
Paroxysmal nocturnal dyspnea
+ +
Fatigue + +
Reduced exercise capacity + +
Cough or Wheezing + +
Confusion/Delirium + +
GI Symptoms: early satiety, nausea, vomiting, abdominal discomfort
+ +
Sudden weight gain more than 2 pounds in one day or 5 pounds in 1 week
+ +
Chest pain + +
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
22

Physical ExamHFpEF HFrEF
Rales ++ ++
Peripheral edema + ++
Jugular venous distension + ++
S3 + ++
S4 ++ +
Displaced point of maximal impulse - ++
Mitral regurgitation murmur + ++
Hepatomegaly and/or ascites + ++
Cool extremities + ++
Narrow pulse pressure + ++
Hypotension + ++
Tachycardia + ++
Hypertension ++ +
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
23

Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
24

Measuring JVP
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
25

Goals
HFpEF HFrEF
Reduce Symptoms + +
Improve Quality of Life + +
Decrease hospitalizations + +
Reduce Mortality + +
Identification and treatment of co-morbidities
+ +
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
26

Guideline Directed Medical Therapy
HFpEF HFrEFDiuretics ++ ↓ symptoms ++ ↓symptoms
ACE Inhibitor, ARB, or ARNI - ++ ↓ morbidity & mortality
Beta Blocker - ++ ↓ morbidity & mortality
Aldosterone Antagonist + (?) ++ ↓ morbidity & mortality
Hydralazine/isosorbide dinitrate - ++ ↓ morbidity & mortality for AA
Corlanor - ++ ↓ hospitalization
Digoxin - ++ ↓ hospitalization
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
27

Interventions
HFpEF HFrEF
ICD Therapy - Recommended for primary prevention of SCD
CRT - Indicated for HFrEF with LBBB
Heart Transplant - Indicated for HFrEF who meet criteria
Permanent Mechanical Circulatory Support
- Indicated for HFrEF who meet criteria
Chronic Inotropes - Indicated for HFrEF who meet criteria
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
28
Case Study
Heart Failure with Preserved Ejection
Fraction
Image Source: Jessup M, Brozena SA. New Engl J Med. 2003; 348:2007-2018.
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
29

Case Study HFpEF: Mr. Jones
55 year old Caucasian male
Past Medical History
HFpEF
Obstructive Sleep Apnea
Hypertension
Chronic Kidney Disease, Stage 3
Uncontrolled Diabetes Type 2
TIA
Hyperlipidemia
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
30

Case Study HFpEF: Mr. Jones
Aspirin 81mg Lipitor (Atorvastatin) 40mg QHS Bumex (Bumetanide) 4mg BID Aldactone (Spironolactone)
25mg daily Cymbalta (Duloxetine) 30mg
daily Lyrica (Pregablin) 200mg TID Cozaar (Losartan) 25mg QHS
MEDICATIONS
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
31
Case Study HFpEF: Mr. Jones
EKG 3/2020
Sinus Rhythm
Boarder line left axis deviation
Cardiac Stress Test 9/2018
Indication: Shortness of breath and Chest pain
No evidence of ischemia or infarct
LVEF greater than 70%
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
32
Case Study HFpEF: Mr. Jones Echocardiogram 10/2019
Normal left ventricular size with mild to moderate hypertrophy.
Normal systolic function.
Stage II diastolic dysfunction.
Normal right ventricular size and function.
No significant valvular disease.
PA systolic pressure estimated at 37mmHg plus RA pressure.
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
33

Case Study HFpEF: Mr. Jones
Heart Failure Hospitalization # 1
• Presented with progressive dyspnea on exertion. Walking 10 feet causes severe dyspnea. ADLs cause dyspnea.
• Noted gradual weight gain over 2 months (252 pounds to 288 pounds). • Not responding to Lasix 80 mg BID. • Admission vital signs: BP 187/90, HR 77, RR 22, oxygen 98 % RA • Admission Labs: Sodium 136, Potassium 4.9, BUN 76, Creatinine 2.6, BNP 78 • Reports he does not monitor fluid or sodium intake. •Established with heart failure clinic• Lasix (Furosemide) 80 mg BID•Aldactone (Spironolactone) 25 mg Qday•Cozaar (Losartan) increased 50 mg QHS•Advised patient to keep blood pressure log
October
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
34

Case Study HFpEF: Mr. Jones
Heart Failure Hospitalization # 2
• Admitted following right heart catheterization demonstrating significant volume overload.• RA = 27 mean • PA = 40/31 mean = 34• PCW = a wave = 31 v wave = 33 mean = 28• SVR 23 Wood Units• PVR 1.3 Wood Units
• Admission vital signs: BP 125/82, HR 82, RR 18, oxygen 97 % RA• Admission weight 278 pounds• Admission labs: Sodium 138, potassium 4.5, BUN 66, Creatinine 2.4, BNP 67
• Lasix (Furosemide) 80 mg BID• Aldactone (Spironolactone) 25 mg daily• Cozaar (Losartan) 50 mg QHS• HF teaching and reinforcement
November
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
35
Case Study HFpEF: Mr. Jones
Heart Failure Hospitalization # 3
• Admitted from clinic with volume overload• Symptoms: Abdominal dissension, LE edema, JVD elevated 16 cm, orthopnea.• Admission vital signs: BP 133/72, HR 72, RR 20, oxygen 97 % RA• Admission weight 282 pounds• Admission labs: Sodium 140, potassium 4.6, BUN 68, Creatinine 2.6, BNP 88
• Diuretic switched to Bumex (Bumetanide) 6 mg BID• Aldactone (Spironolactone) 25 mg Qday• Cozzar (Losartan) 50 mg QHS• HF teaching and reinforcement• Comorbidities Contributing?
• Diabetes Seen by endocrinology for uncontrolled diabetes type 2• OSA compliant w/ CPAP• HTN controlled• CKD, stage 3 kidney function stable • Medication review: ? Lyrica• Socioeconomic factors?
February
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
36

Case Study HFpEF: Mr. Jones
FOLLOW UP:
Seen in clinic for post hospital follow
up 7 days after discharge.
SUBJECTIVE:
Able to walk from home to mailbox
without limitations. Denies orthopnea.
Limiting sodium and fluid intake. Wearing CPAP nightly. Blood
glucose average 200s
EXAM:
JVD 7 cm. Trace LE edema
VITALS:
BP 126/89, HR 78, RR 16, oxygen saturation 98%
WEIGHT:
270 pounds
LABS:
Sodium 139, potassium 4.8,
BUN 58, creatinine 2.2, bnp 66
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
37

HFpEF Clinical Pearls
Management of hypertension
Management of fluid
Management of Co-Morbidities
Assess Socioeconomic
Factors
Labs:
BNP NOT always elevated w/ HFpEF
and or Obesity
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
38
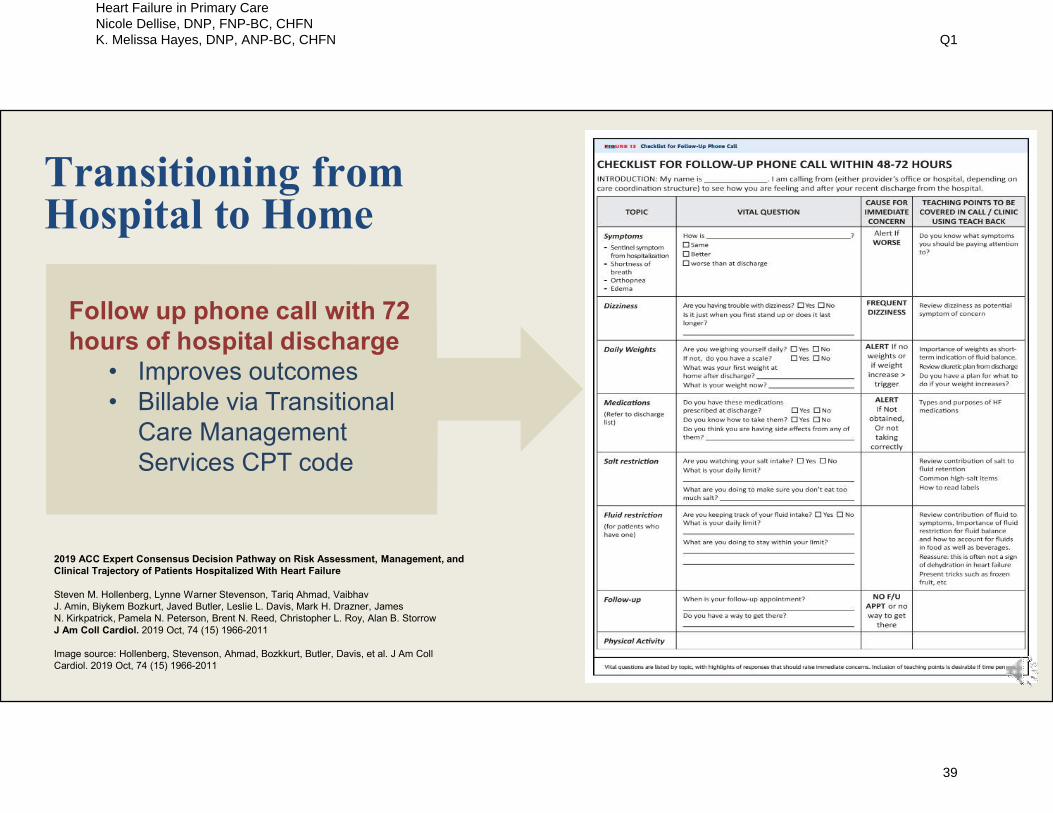
Transitioning from Hospital to Home
Follow up phone call with 72 hours of hospital discharge
• Improves outcomes• Billable via Transitional
Care Management Services CPT code
2019 ACC Expert Consensus Decision Pathway on Risk Assessment, Management, and Clinical Trajectory of Patients Hospitalized With Heart Failure
Steven M. Hollenberg, Lynne Warner Stevenson, Tariq Ahmad, Vaibhav J. Amin, Biykem Bozkurt, Javed Butler, Leslie L. Davis, Mark H. Drazner, James N. Kirkpatrick, Pamela N. Peterson, Brent N. Reed, Christopher L. Roy, Alan B. StorrowJ Am Coll Cardiol. 2019 Oct, 74 (15) 1966-2011
Image source: Hollenberg, Stevenson, Ahmad, Bozkkurt, Butler, Davis, et al. J Am Coll Cardiol. 2019 Oct, 74 (15) 1966-2011
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
39

First post-discharge visit checklist
• History• Exam• Testing• Medication• Therapy Considerations• Patient Education• Consultations
Transitioning from Hospital to Home
Image source: Hollenberg, Stevenson, Ahmad, Bozkkurt, Butler, Davis, et al. J Am Coll Cardiol. 2019 Oct, 74 (15) 1966-2011
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
40

Transitioning from Hospital to Home
Transitional Care Management Services
CPT Code 99495: Moderate Complexity
Communication within 2 business days of discharge
Moderate complexity medical decision making
Face to face visit within 14 days of discharge
CPT Code 99496: High Complexity
Communication within 2 business days of discharge
High complexity medical decision making
Face to face visit within 7 days of discharge
Getty Images / fcscafeine
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
41
Co-Managing Heart Failure in Primary Care
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
42

Co-Managing Heart Failure in Primary Care
Partner with local heart specialist or cardiologist.
Get to know the hospitalists team that takes care of the HF pts in local hospital.
Connect with community resources such as home health, medication delivery services.
Communicate any medications changes to the cardiologist or concerns for disease progression.
Knowing when to refer for advanced care.
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
43
Case Study
Heart Failure with Reduced Ejection Fraction
Image Source: Jessup M, Brozena SA. New Engl J Med. 2003; 348:2007-2018.
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
44

Case Study HFrEF: Mrs. Smith
HPI: Mrs. Smith is a 51 yo AA female with history of HFrEF 2/2 to hypertensive heart disease with LVEF of 20-25%. Presents today for follow up after recent hospitalization.
Current symptoms include: DOE with walking around in home and ADLs, No DOE at rest, + PND about 2 nights a week, + 2 pillow orthopnea, LE edema, and early satiety.
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
45

Case Study HFrEF: Mrs. Smith
PMH:
Hospitalization for new onset HF symptoms
Hypertension x 20 years (non-adherent)
Type 2 DM x 10 years
Obesity
Family History:
Father with Cardiomyopathy
Social:
Stopped all ETOH 2 years ago
No illicit drugs, non-smoker
Divorced, lives with mom and son
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
46

Case Study HFrEF: Mrs Smith
Glucophage (Metformin) 500mg BID Lasix (Furosemide) 80mg once a day Coreg (Carvedilol) 12.5mg once a day Lopressor (Metoprolol) 25mg once a day Prinivil (Lisinopril)10mg once a day KDUR (Potassium chloride) 10meq QD
MEDICATIONS
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
47
VS: Weight 245# , b/p 155/80, HR 78, o2 sat 98%, rr 16, Temp 98.6
Gen: AA female well developed, well nourished in NAD
HEENT: EOMs intact bilaterally, PERRLA bilaterally, oropharynx benign, neck supple, no carotid bruits
CV: regular rate and rhythm, S1S1, +S4 no S3, soft II/VI systolic apical murmur, PMI slightly laterally displaced. JVD 8-10 cmh20 noted pt sitting 90 degrees, no HJR
Pul: Bilat CTA
Ab: normoactive BS, non-tender, non-distended, no HJR, no heptosplenomegaly
Extremities: Bilateral LE 2+ edema to knees, 2+ bilateral LE pulses
Case Study HFrEF: Mrs. Smith
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
48
Most RecentTesting:
ECHO: Severe depressed LV systolic function with severe global hypokinesis with LVEF est at 20-25%.
Impaired relaxation (Stage I diastolic dysfunction).
Normal right ventricular size and function.
No significant valvular disease.
RA pressure estimated at 8
Cardiac Cath: No significant coronary artery disease
LABS: Glucose 204, KCL 4.3, CL 102, Co2 28, BUN 16, Creat1.2, CA 9.6 ; BNP= 1194
Case Study HFrEF: Mrs. Smith
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
49

Diagnosis:
HFrEF Class C, NYHA class IIIb, etiology likely hypertensive heart disease.
WET VS DRY?
Case Study HFrEF: Mrs Smith
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
50

Plan:
WET - Needs increased diuresis (what ss = ? WET)
Has increased B/P - Good time to increase after load reduction by changing over to ARNI (STOP Prinivil (Lisinopril) x 36 hrs)
Beta blocker optimization?? (on 2 different ones) point to only be on one…which one? Coreg (Carvedilol)12.5mg increase to BID after increased diuretics for a few days.
STOP Lopressor (Metoprolol )
Add Aldactone (Spironolactone) 25mg QD
Consider adding Digitex (Digoxin) 0.125mcg
Increase diuretic to 80mg BID to lose 1-2 pounds a day….
Increase KCL to 10meq BID (KCL is on the low side)
Case Study HFrEF: Mrs. Smith
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
51

Once optimized:
Consider Adding isosorbide/hydralazine (bidil ) slow increase to 1 tab BID-TID
Repeat ECHO and if LVEF remains < 30 % will need referral to EP for ICD for primary prevention
Case Study HFrEF: Mrs. Smith
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
52

Follow up visit:
HOW SOON?
WHAT NEXT?
Case Study HFrEF: Mrs. Smith
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
53

What would plan be if patient was DRY on exam?
Case Study HFrEF: Mrs. Smith
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
54

HFrEF Clinical Pearls
When Dry increase Beta
blocker (if HR & B/P allow)
When Wet increase ACE/ARB/ARNI
( if B/P & Lab allow)
36 hour wash out changing from ACE
to ARNI
Higher Creatine Higher Diuretic
Dose
Lasix (Furosemide) 80mg = Demadex (Torsemide) 20mg = Bumex
(Bumetanide) 2mg
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
55

Patient Teaching
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
56
Patient Teaching: Key Points
Medication Review
Activity Level
Dietary and Sodium restrictions (no added salt)
Fluid restrictions (1500-2000ml/day)
Daily weight monitoring
Assessment of peripheral edema
Substance use counseling if appropriate
List of warning signs of decompensation
Bring list of medications and daily weights to each outpatient visit
Who to call for worsening symptoms or ICD discharge
Smoking Cessation
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
57

Same time
Same scale
Notify provider for weight gain > 2 lbs. above baseline
Daily Weights
Getty Images / TerryJ
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
58
MEDS TO AVOID
NO NSAIDS for pain
Watch for the TZDs: Actos( Pioglitzxone), Avandia (Rosiglitazone) etc)
Worsening renal function (all diabetic meds)
Calcium Channel Blockers in LVEF <40%
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
59

When to refer?
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
60
Slow The Slide
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
61
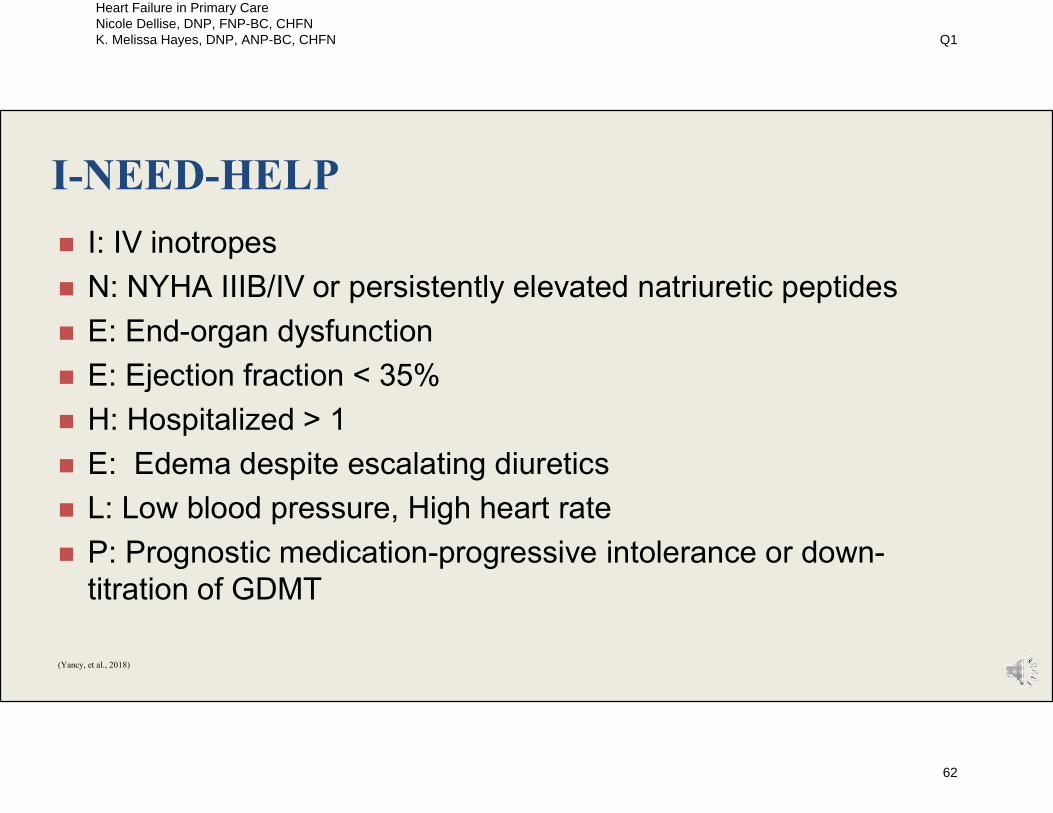
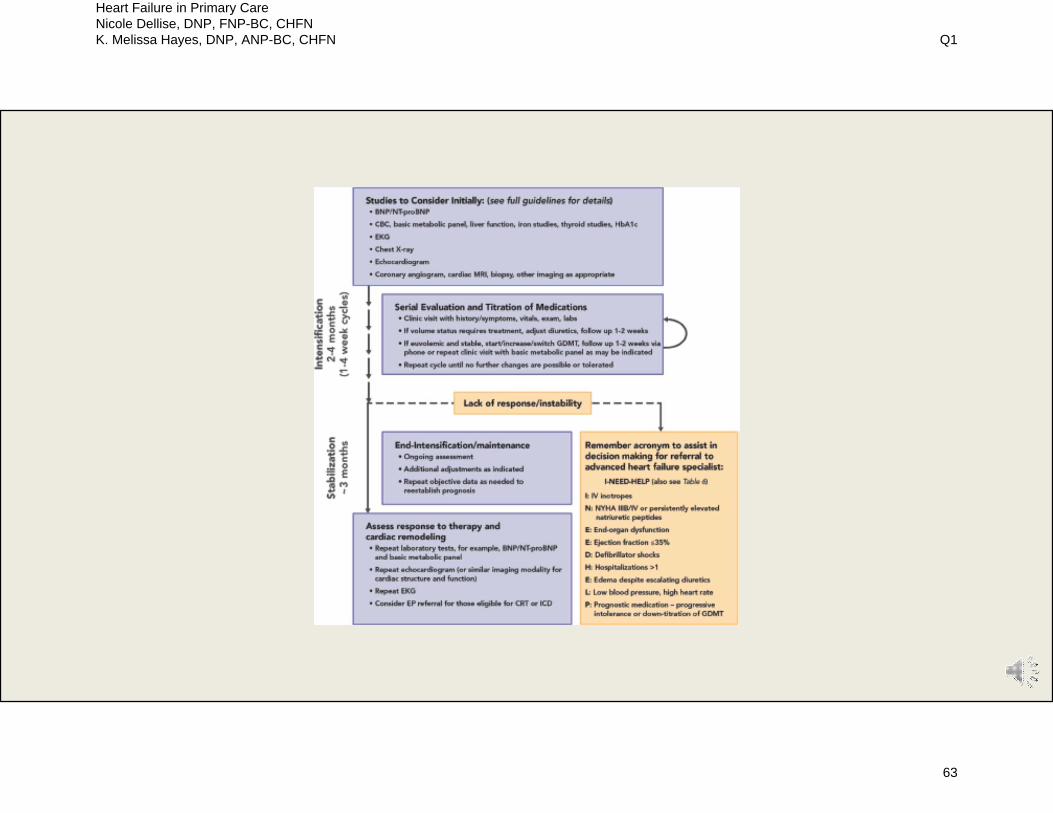
I-NEED-HELP
I: IV inotropes
N: NYHA IIIB/IV or persistently elevated natriuretic peptides
E: End-organ dysfunction
E: Ejection fraction < 35%
H: Hospitalized > 1
E: Edema despite escalating diuretics
L: Low blood pressure, High heart rate
P: Prognostic medication-progressive intolerance or down-titration of GDMT
(Yancy, et al., 2018)
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
62
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
63

Stages, Phenotypes and Treatment of HF
or ARNI
(Yancy, et al, 2013)
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
64

Clinician and Patient Resources American Association of Heart Failure Nurses
https://www.aahfn.org/
Heart Failure Society of America
https://hfsa.org/
American Heart Association
https://www.heart.org/en/health-topics/heart-failure
2019 ACC Expert Consensus Decision Pathway on Risk Assessment, Management, and Clinical Trajectory of Patients Hospitalized with Heart Failure http://www.onlinejacc.org/content/74/15/1966?rss=1
2013 ACCF/AHA Guideline for Management of Heart Failure https://www.ahajournals.org/doi/full/10.1161/cir.0b013e31829e8776
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for Management of Heart Failure https://www.ahajournals.org/doi/full/10.1161/CIR.0000000000000509
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
65

On the Horizon
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
66
On the Horizon for HF
SGLT2 inhibitors significantly improve HF related outcomes, decreasing the frequency of HF
related hospitalizations as well as CV related Death
The FDA has approved Farxiga (dapagliflozin) due to the reduction of risk for CV death and HF hospitalization in people with chronic HFrEF Class II-IV (McMurray et al., 2019; Petrie, 2020)
COVID-19 Impact (unknown)
CardioMems_Remote Hemodynamic monitoring
(Guide-HF)
Wojcik & Warden (2019) Curr Cardiol Rep. Sep 14;21(10):130. doi: 10.1007/s11886-019-1219-4.Mechanisms and Evidence for Heart Failure Benefits from SGLT2 Inhibitors.
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
67

SUMMARY
HFpEF vs HFrEF: Goals are the same but treatment is vastly different.
Management of Co-Morbid conditions is essential for reducing Heart Failure exacerbations.
Primary Care providers are essential in co-management of the Heart Failure patient.
Collaboration and resources are readily available.
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
68
Questions? Email Us! [email protected]
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
69

References Axon, R. N., & Williams, M. V. (2011). Hospital readmission as an accountability measure. JAMA, 305(5), 504-505. doi:
10.1001/jama.2011.72
Buggey, J., Mentz, R. J., DeVore, A. D., & Velazquez, E. J. (2015). Angiotensin Receptor Neprilysin Inhibition in Heart Failure: Mechanistic Action and Clinical Impact. J Card Fail, 21(9), 741-750. doi: http://dx.doi.org/10.1016/j.cardfail.2015.07.008
Collins, S., Storrow, A. B., Albert, N. M., Butler, J., Ezekowitz, J., Felker, G. M., . . . Lenihan, D. J. Early Management of Patients With Acute Heart Failure: State of the Art and Future Directions. A Consensus Document From the Society for Academic Emergency Medicine/Heart Failure Society of America Acute Heart Failure Working Group. J Card Fail, 21(1), 27-43. doi: 10.1016/j.cardfail.2014.07.003
DeWalt, D. A., Malone, R. M., Bryant, M. E., Kosnar, M. C., Corr, K. E., Rothman, R. L., . . . Pignone, M. P. (2006). A heart failure self-management program for patients of all literacy levels: a randomized, controlled trial [ISRCTN11535170]. BMC Health Services Research, 6, 30. doi: 10.1186/1472-6963-6-30
Hollenberg, 2019 ACC Expert Consensus Decision Pathway on Risk Assessment, Management, and Clinical Trajectory of Patients Hospitalized With Heart Failure
Steven M. Hollenberg, Lynne Warner Stevenson, Tariq Ahmad, Vaibhav J. Amin, Biykem Bozkurt, Javed Butler, Leslie L. Davis, Mark H. Drazner, James N. Kirkpatrick, Pamela N. Peterson, Brent N. Reed, Christopher L. Roy, Alan B. Storrow
J Am Coll Cardiol. 2019 Oct, 74 (15) 1966-2011
Jencks, S. F., Williams, M. V., & Coleman, E. A. (2009). Rehospitalizations among patients in the Medicare fee-for-service program. [Research Support, Non-U.S. Gov't]. N Engl J Med, 360(14), 1418-1428. doi: 10.1056/NEJMsa0803563
Jessup, M. et al. (2016) 2016 ESC and ACC/AHA/HFSA heart failure guideline update — what is new and why is it important? Nat. Rev. Cardiol. doi:10.1038/nrcardio.2016.134
Krumholz, H. M., Merrill, A.R., Schone, E.M., Schreiner, G.C., Jersey, C., Bradley, E.H., …Drye, E.E. (2009). Patterns of hospital performance in acute myocardial infarction and heart failure 30-day mortality and readmission. Circulation: Cardiovascular Quality and Outcomes, Journal of the American Heart Association, 2, 407-413.doi: 10.1161/CIRCOUTCOMES.109.883256
Lindenfeld, J., Albert, N. M., Boehmer, J. P., Collins, S. P., Ezekowitz, J. A., Givertz, M. M., . . . Walsh, M. N. (2010). HFSA 2010 Comprehensive Heart Failure Practice Guideline. J Card Fail, 16(6), e1-194. doi: 10.1016/j.cardfail.2010.04.004
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
70

References Loop, M. S., Van Dyke, M. K., Chen, L., Brown, T. M., Durant, R. W., Safford, M. M., & Levitan, E. B. (2016). Comparison of Length of Stay,
30-Day Mortality, and 30-Day Readmission Rates in Medicare Patients With Heart Failure and With Reduced Versus Preserved Ejection Fraction. Am J Cardiol. doi: 10.1016/j.amjcard.2016.04.015
Murray, M. D., Tu, W., Wu, J., Morrow, D., Smith, F., & Brater, D. C. (2009). Factors associated with exacerbation of heart failure include treatment adherence and health literacy skills. Clin Pharmacol Ther, 85(6), 651-658. doi: 10.1038/clpt.2009.7
McMurray, J. et al DAPA-HF Trial Committees and Investigators (2019).Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. The New England journal of medicine, 381(21), 1995–2008. https://doi-org.proxy.library.vanderbilt.edu/10.1056/NEJMoa1911303
Mozaffarian, D., Benjamin, E. J., Go, A. S., Arnett, D. K., Blaha, M. J., Cushman, M., . . . Turner, M. B. 2015). Heart Disease and Stroke Statistics—2015 Update: A Report From the American Heart Association. Circulation, 131(4), e29-e322. doi: 10.1161/cir.0000000000000152
Philbin, E. F., Dec, G. W., Jenkins, P. L., & DiSalvo, T. G. (2001). Socioeconomic status as an.independent risk factor for hospital readmission for heart failure. Am J Cardiol, 87(12), 1367-1371. doi: http://dx.doi.org/10.1016/S0002-9149(01)01554-5
Petrie, M. C.… McMurray, J. (2020). Effect of Dapagliflozin on Worsening Heart Failure and Cardiovascular Death in Patients With Heart Failure With and Without Diabetes. JAMA, 323(14), 1353–1368. Advance online publication. https://doi-org.proxy.library.vanderbilt.edu/10.1001/jama.2020.1906
Roger, V.L., Go, A.S., Lloyd-Jones, D.M., Adams, R.J., Berry, J.D., Brown, T.M., …Wylie-Rosett, J. (2011 ). Heart disease and stroke statistics-2011 update: A report from the American Heart Association. Circulation: Journal of the American Heart Association, 123, e18-e209. doi: 10.1161/CIR.0b013e3182009701
US Department of Health and Human Services, Centers for Disease Control and Prevention. (2010). Heart Failure Fact Sheet . Retrieved from http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_heart_failure.htm.
Wojcik & Warden (2019) Curr Cardiol Rep. Sep 14;21(10):130. doi: 10.1007/s11886-019-1219-4.Mechanisms and Evidence for Heart Failure Benefits from SGLT2 Inhibitors.
Yancy, C. W., Januzzi, J. L., Jr., Allen, L. A., Butler, J., Davis, L. L., Fonarow, G. C., . . . Wasserman, A. (2018). 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol, 71(2), 201-230. doi: 10.1016/j.jacc.2017.11.025
Yancy, C. W., Jessup, M., Bozkurt, B., Butler, J., Casey, D. E., Drazner, M. H., . . . Wilkoff, B. L. (2013). 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation, 128(16), e240-e327. doi: 10.1161/CIR.0b013e31829e8776
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
71
References
Yancy, C. W., Jessup, M., Bozkurt, B., Butler, J., Casey, D. E., Jr., Colvin, M. M., . . . Westlake, C. (2016). 2016 ACC/AHA/HFSA Focused Update on New Pharmacological Therapy for Heart Failure: An Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. doi: 10.1161/cir.0000000000000435
Yancy, C. W., Jessup, M., Bozkurt, B., Butler, J., Casey, D. E., Jr., Colvin, M. M., . . . Westlake, C. (2017). 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Card Fail, 23(8), 628-651. doi: 10.1016/j.cardfail.2017.04.014
Yehle, K. S., & Plake, K. S. (2010). Self-efficacy and educational interventions in heart failure: a review of the literature. Journal of Cardiovascular Nursing, 25(3), 175-188. doi: 10.1097/JCN.0b013e3181c71e8e
Ziaeian, B., & Fonarow, G. C. (2016). The Prevention of Hospital Readmissions in Heart Failure. Progress in Cardiovascular Diseases, 58(4), 379-385. doi: http://dx.doi.org/10.1016/j.pcad.2015.09.004
Heart Failure in Primary Care Nicole Dellise, DNP, FNP-BC, CHFN K. Melissa Hayes, DNP, ANP-BC, CHFN Q1
72