pyrexia of unknown origin · pyrexia of unknown origin by: abd. salman . what is fever?? elevated...
TRANSCRIPT
Pyrexia of UNKNOWN origin By: Abd. Salman

What is FEVER??
elevated core body temperature of more than 38.0°C, it is a response to cytokines and acute phase proteins.
Cytokines such as??
Acute phase proteins from??such as??
*Cytokine such as interleukins (IL-1), interferons, TNF
*Acute phase proteins from liver in response to inflammation such as:
-CRP & serum amyloid A host defense, repair & regeneration
-anti oxidants: SOD (scavenge for ROS)
-ferritin & lactoferrin: iron-binding proteins to prevent iron uptake by bacteria
-Immunoglobulins??
Fever can be infectious or non-infectious

PUO??
a temperature above 38.0°C on multiple occasions for more than 3 weeks, without diagnosis, despite initial investigation in hospital for 1 week.
These initial investigations include:
-investigations over 3 days of inpatient care, 3 outpatients visits or 1 week of intensive ambulatory investigations
Subsets of PUO:
1- HIV-related
2- Immunodeficient
3- Nosocomial
But this doesn’t mean that all patients will be in one of these 3 groups
So we have a patient with fever >3 weeks and we don’t know the cause of this fever despite initial investigations
How can we know the cause?
that’s what we have to know by the end of this lecture…
CAUSES OF PUO:
1- infectious 30%
2- malignancy 20%
3- connective tissue disorders 15%
4- miscellaneous 20%
5-idiopatheic 15%
INFECTIOUS:
a) Specific locations:
-abscesses: hepatobiliary, urinary tract, prostate, pulmonary
-infective endocarditis
-infection of the oral cavity
-infection of head & neck
-bone and joints
b) Specific organisms:
-TB (particularly extra-pulmonary) -HIV1 -CMV -EBV
-fungal (candida)

c) Special patients groups:
-travel or residency: TB “Asia, Africa” & Malaria
-nosocomial: pneumonia & UTI
-HIV-positive patients: acute retroviral syndrome & mycobacteria
MALIGNANCY:
-lymphoma & leukemia
-renal, liver, colon, stomach, pancreas tumors
CONNECTIVE TISSUE DISORDERS:
-old patients: arteritis, polymyalgia rheumatic
-young patients: SLE, vasculitis, polymyositis, Behcet’s disease, rheumatic fever “specially in Asia”
MISCELLANEOUS:
-CVS ( Atrial myxoma, aortitis, aortic dissection )
- RS ( Sarcoidosis, PE, allergic alveolitis )
- GI ( IBD, Pancreatitis, Alcoholic liver disease )
- Metabolic (Thyrotoxicosis, thyroiditis, pheochromocytoma, hypertriglyceridemia, any hypothalamic lesions )
- Hematological (Hemolytic anemia, Paroxysmal nocturnal hemoglobinuria)
- Inherited ( FMF, Periodic fever symptoms )
- Drug reactions ( Antibiotic fever)
In some groups we have to consider specific causes:
1- periodic fever syndrome should be considered in those with family history
2- children & young adults think about infections “specially viral”
3- older adults think about infectious causes such as TB, intra-abdominal abscess, UTI, infective endocarditis OR non-infectious causes such as tumors
4- in men don’t forget prostate
TOO MANY CAUSES

TOO MANY INVESTIGATIONS SHOULD BE DONE

IT’S CHALLANGING DIAGNOSIS
Signs & Symptoms:
In addition to fever
1-sweating
2-chills & rigors
3-headache
4-anorxia
5-dehydration
6-weakness
7-skin rashes
8-vomiting
Don’t forget to ask the patient about drug history, some drugs are pyrogenic.
Diagnosis:
Highly detailed history & physical examination should be repeated at regular intervals
Then we move to investigations.
Investigations:
-as we said, the initial investigations will be negative when we say that this patient has PUO so, we have to do further microbiological & non-microbiological investigations.
- Remember that you have to put your priorities in the selection of appropriate investigations according to “special groups”, for example, I will not focus on MALIGNANCY in young adults before searching for INFECTIOUS causes
Investigations include:
1-sputum for mycobacteria stains & culture
2-serologyHIV test & ferritin estimation
3-imaging of the abdomen (US & CT)
4-ECHO
5-CBC
6-urinalysis
7-ESR & CRP
8-culture: blood, sputum, CSF, urine, stool according to presentation
9-analysis & culture of abnormal fluid collection (joints, pleura)
10-LFT, ANA, RF, TSH
11-antibodies to HIV1

If we find a lesion on imaging what should we do??
Take biopsy to do culture, histopathology & nucleic acid detection.
-if the patient is on antimicrobial drug do 16s rRNA gene highly specific for detection of organisms in pure culture
Positron Emission Tomography (PET)??

Use PET for vasculitis & to select biopsy site.
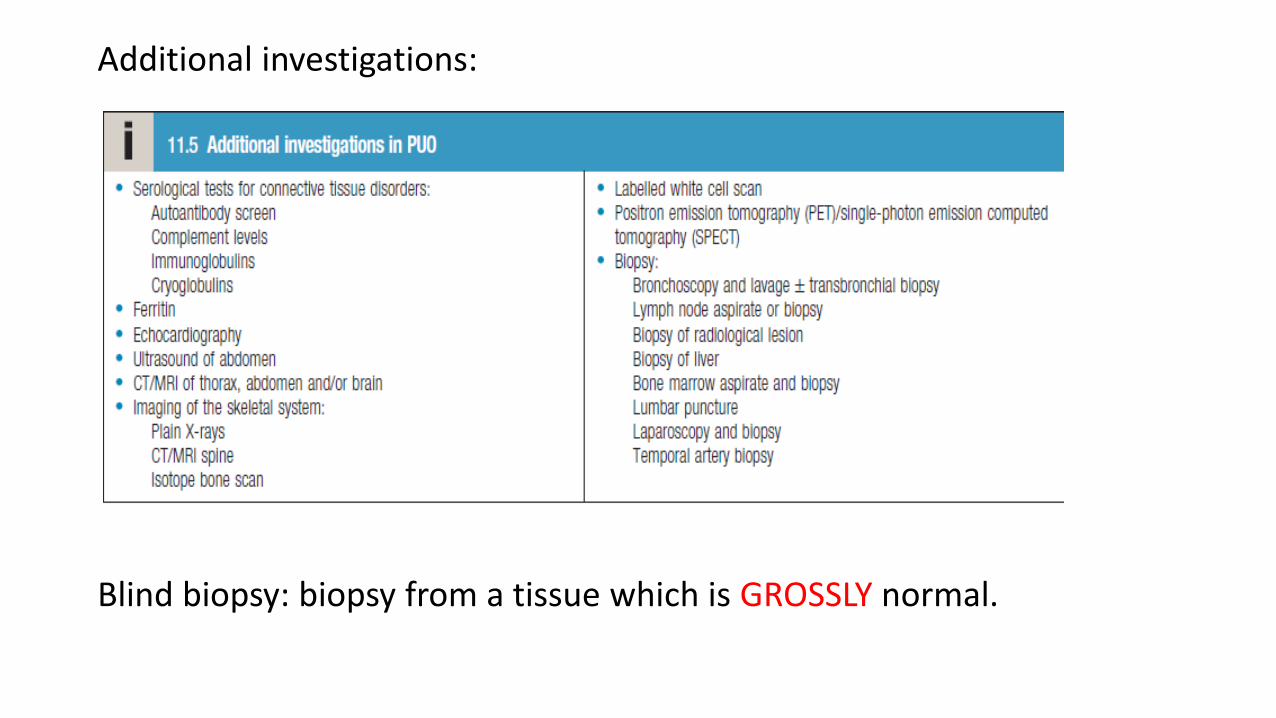
Additional investigations:
Blind biopsy: biopsy from a tissue which is GROSSLY normal.

Treatment:
-in some cases, fever may resolve spontaneously
- Non-drug therapy: rest, fluids intake, stop any unnecessary drug intake (some drugs are pyrogenic), good nutrition & supplements, cooling the skin
- Drug therapy:
- Acetaminophen “Paracetamol”
- Aspirin and other nonsteroidal anti-inflammatory drugs
- Antipyretics
- In cases of infection, antibiotic, antifungal, or antiviral drug, depending on the cause of the infection.
→ Further management is focused on the underlying cause
Prognosis :
No cause is found in approximately 10%. Without significant symptoms like weight loss the mortality is low
THANK YOU