pulmonary embolism - eleanor r. hethcox, dnp,...
TRANSCRIPT
Pulmonary Embolism:
A Case Study of Delayed and Misdiagnosis
by Eleanor Hethcox, ACNP-BC

Subjective
• Patient Profile– 31 year old Caucasian female
– Resident of Galveston County
– Single mother
– full time RN
– Athletic – weight lifting/cardio 6 days/week; kickboxer
– Non-smoker; BMI 20; occasional etoh intake, no recent prolonged travel, active lifestyle

Background Information
• Chief complaint – right sided flank pain
• HPI – 31 y/o CF presents to urgent care clinic w/right sided flank pain X 6 months; described as sharp, stabbing pain; intermittent occurring 4-5 times in the past 6 months lasting only a few minutes. Pt noticed she has been much more fatigued than usual and is unable to tolerate the intensity of training considered normal for her.
Background Continued
• Latest episode occurred 48 hours ago, pain 10/10 with SOB; supine position worsens the pain; pt tried prescribed ibuprofen 800 mg and MOM - nothing alleviated pain. 2 months ago, pt experienced palpitations and syncopal episode without injury.
• Six months ago, pt originally presented to PCP w/stabbing right flank pain, fever, and recent UTI; was dx with complicated cystitis and finished a course of Abxwith resolution of fever only. Pt reports having US of kidneys – unremarkable.
Background
• Subsequent visits to PCP and urgent care were unremarkable. Residents dx her with MSK strain and pt was given 800 mg ibuprofen TID PRN for pain.
• Patient encountered faculty physician at Urgent Care and requested a chest radiograph. Patient was then released to go back to work the following day.
• Faculty physician immediately called patient back to clinic for blood work; CBC w/diff, CMP, d-dimer, cardiac enzymes were drawn
Past Medical/Surgical/Family
History
• Past medical Hx – frequent UTI, gestational diabetes; G3P1
• Surgical Hx – breast augmentation (2005); tympanoplasty right (1980s)
• Family Hx – mother and MGM with HTN; others unremarkable-no family history of blood clotting disorders
• ROS – denied chest pain, fever, cough, hemoptysis, wheezing, lower leg pain, SOB, no recent extended travel
• Medications – Yaz (Drospirenone/Ethinyl Estradiol) daily, MV daily, ibuprofen 800 mg TID PRN for pain
Objective
• Physical examination
• Diagnostics tests
• Rationale for exam and diagnostic test components

Physical Examination Findingsupon admission
• Blood pressure – WNL; HR – WNL; Temp – 36.9C; RR –18; O2 sats – 99% on room air
• Pain level - 0/10 sitting and standing; 10/10 lying supine
• CV: S1S2, RRR, no murmurs auscultated; Pulmonary –CTA bilaterally, bilateral upper and lower extremities findings unremarkable. Tenderness and pain elicited on right flank/chest in supine position. All other systems WNL.
Diagnostics
• Blood work – CBC with diff, cardiac enzymes, D-dimer, ABGs*,ESR-WESTGN, PT/INR, BNP, factor V Leiden, protein C, Protein S, anti-cardiolipinantibodies*
• V/Q Scan –not performed (replaced by CT angiogram)
• Pulmonary angiogram – gold standard in PE dx
• Echocardiogram – assess RV function; blood flow
• EKG – rule out cardiac events; MI
• Doppler of the BLE – look for possible DVT
Rationale of Diagnostics
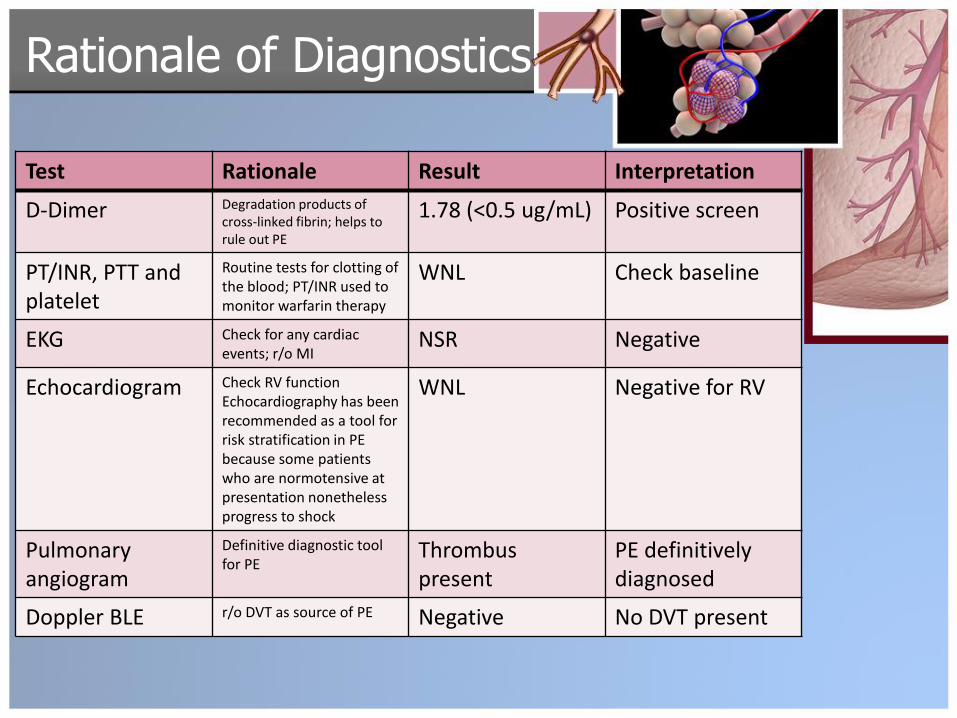
Test Rationale Result Interpretation
D-Dimer Degradation products of cross-linked fibrin; helps to rule out PE
1.78 (<0.5 ug/mL) Positive screen
PT/INR, PTT and platelet
Routine tests for clotting of the blood; PT/INR used to monitor warfarin therapy
WNL Check baseline
EKG Check for any cardiac events; r/o MI
NSR Negative
Echocardiogram Check RV functionEchocardiography has been recommended as a tool for risk stratification in PE because some patients who are normotensive at presentation nonetheless progress to shock
WNL Negative for RV
Pulmonaryangiogram
Definitive diagnostic tool for PE
Thrombuspresent
PE definitivelydiagnosed
Doppler BLE r/o DVT as source of PE Negative No DVT present
Assessment
• Differential Diagnoses:
– Pneumonia vs. pulmonary embolism vs. renal calculi vs. upper UTI vs. intercostal muscle strain
• Formulation of Diagnosis:
– Episode of fever, SOB, syncopal episode, palpitations, right sided flank/chest pain, use of oral contraceptives in the last 12 months.
– D-dimer positive, Chest Xray, Pulmonary Angiogram
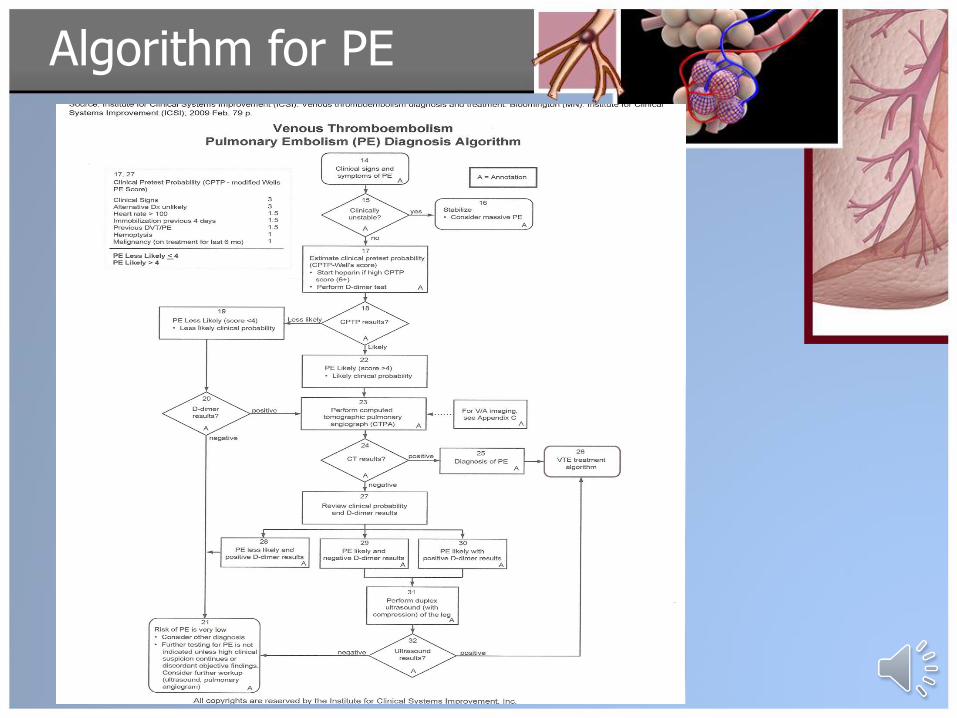
Algorithm for PE
Plan with Rationale
• Heparin – Low molecular weight heparin (LMWH) is preferred for initial treatment due to better safety and outcomes. Enoxaprin was used;
• Vitamin K antagonist – warfarin. Patient should begin warfarin on first day concurrent with heparin; INR should be greater than 2.0. before d/c heparin.
• Echocardiogram – to assess right ventricular dysfunction; decide on thrombolytics.
• Daily EKGs and continue cardiac monitoring
• Supplemental Oxygen 2L/min per NC
• Guiac was performed prior to initiation of heparin therapy to rule out GI bleed.
Education
• Patient
– Ms. B is a Cardiology RN and is very familiar with PE. She is given altered teaching by one of her fellow RNs and internists.
– Ms. B is ordered to stop taking OCP immediately and to use alternative methods of birth control – diaphragm, condoms, abstinence.
– Warfarin, side effects, uses and importance of scheduled blood testing of PT/INR levels are discussed briefly.
– Patient is ordered to rest. No strenuous activities until follow up in 2 weeks. Patient advised to discontinue weight lifting, cardio and kickboxing until approved by her PCP.
• Family - no teaching. Family not available.

Follow-up
• Follow up with PCP was done in 2 weeks.
• PT/INR checks in the first 2-3 weeks then scheduled to adjust warfarin levels.
• Repeat CT scan was performed 5 months after discharge due to presentation of similar signs and symptoms, but now with hx of PE. CT findings were negative.
• Six months post discharge, warfarin was discontinued and asa 81 mg daily was prescribed.
• Ms. B was given the approval by her PCP to resume normal activities.
• Since last check up, pt has developed HTN and is currently on asa81 mg daily, MV daily, enalapril 5 mg daily. Potential to develop pulmonary HTN, RV dysfunction.
• Patient won a settlement in the amount of $200,000 from the manufacturers of Yaz.
Learning Points
• LISTEN to your patients!
• Screening tests should not guide decision making.
• Patient repeated visits to urgent care should send up a RED FLAG!
• Low-risk female patients for PE in the context of use of OCP should be evaluated more closely.
• Clinicians need to recognize motion as a risk factor for thromboembolic disease in young athletes (Rand, 2014).
• Delay and misdiagnosis is common in acute pulmonary embolism (Martinez, 2010).
• Higher age, misdiagnosis and hx of cancer associated with mortality from PE; Days of delay not associated w/mortality (Martinez, 2010).
References
• Alonzo-Martinez, J. A. (2010). Delay and misdiagnosis in sub-massive and non-massive acute pulmonary embolism. European Journal of Internal Medicine, pp. 278-282.
• Barkley, T.W. & myers, C.M. (2008). Practice Guidelines for Acute
Care Nurse Practitioners. St. Louis: Saunders Elsevier.
• Institute for Clinical Systems Improvement (2009) Venous thromboembolism diagnosis and treatment. Bloomington (MN): Institute for Clinical Systems Improvement (ICSI); p. 79.
• Kahanov, L., & Daly, T. (2009). Bilateral Pulmonary Emboli in a
Collegiate Gymnast: A Case Report. Journal of Athletic Training (National Athletic Trainers’ Association), 44(6), 666-671.
References• Khan, S., Smulders, Y. M., de Vries, J. P., & Spoelstra-de Man, A. E.
(2013). Life-Threatening Complications of Hormonal Contraceptives: A Case History. Case Reports In Obstetrics & Gynecology, 1-3. doi:10.1155/2013/186230.
• Papadakis, M., McPhee, S.J. & Rabow, M.W. (2014). Current medical
diagnosis and treatment 2014, (54th ed.). New York: McGraw-Hill.
• Rand, K. M., & Sherman, C. B. (2014). An Unusual Case of Pulmonary Embolism in a Young Healthy Female Competitive Rower. Rhode Island Medical Journal, 97(6), 57-59.
• Smolowitz, J., Honig, J. & Reinisch, C. (2010). Writing DNP clinical
case narratives: Demonstrating and evaluating competency incomprehensive care. New York: Springer Publishing.

References
• Thompson, B.T. & Hales, C.A. (2014). Overview of Pulmonary
Embolism. Retrieved from http://www.uptodate.com on October 20, 2014.
• U.S. Department of Health and Human Services, ARQH, National Guideline Clearinghouse. (2014). Venous thromboembolism
(VTE). Retried from http://www.guideline.gov/content.aspx?id=48195 on
October 10, 2014.
• Wu, C. Q., Grandi, S. M., Filion, K. B., Abenhaim, H. A., Joseph, L., &Eisenberg, M. J. (2013). Drospirenone-containing oral contraceptive pills and the risk of venous and arterial thrombosis: a systematic review. BJOG: An InternationalJournal Of Obstetrics And Gynaecology, 120(7), 801-810. doi:10.1111/1471-0528.12210

Discussion Questions
• Given the presentation of this patient, what screening tool would you use to assess the likelihood of pulmonary embolism and why?
• What are the common risk factors of PE?
• Are there any ethical or legal issues in this particular case? Do you believe that any of the several physicians that encountered the patient prior to admission were negligent?
• How common is misdiagnosis of pulmonary embolism?
• Does morbidity and mortality due to PE depend on delay or misdiagnosis?
• Why would the hospitalist not perform an ABG on this patient?
• What are the long term complications of pulmonary embolism and infarction?