pulmonary arterial hypertension: review and updates veronica franco, md, msph section of pulmonary...
TRANSCRIPT

Pulmonary Arterial Hypertension: Pulmonary Arterial Hypertension: Review and UpdatesReview and Updates
Veronica Franco, MD, MSPH
Section of Pulmonary HypertensionSection of Heart Failure and Transplantation
Ohio State University
Today…
• Nomenclature review - classification
• Diagnosis
• Prognosis
• Treatment

Today…
• Nomenclature review - classification
• Diagnosis
• Prognosis
• Treatment

Is it Primary vs Secondary Pulmonary Hypertension?Is it Pulmonary Arterial
Hypertension (PAH) or Non-PAH?No!!! Dated Nomenclature

Pulmonary Hypertension Is a Disease of Triggers

• Pulmonary hypertension (PH) with left heart disease – WHO Class 2
– Trigger: High LA Pressure
• PH with lung disease/hypoxemia - WHO Class 3
– Trigger: Hypoxemia and Parenchyma Distortion
• PH due to chronic thrombotic and/or embolic disease – WHO Class 4
– Trigger: Obstruction
The 2003 Venice Classification of Non-PAH Pulmonary Hypertension

The 2003 Venice Classification of PAH - WHO Class 1
• Pulmonary Arterial Hypertension
– Familial PAH (FPAH)
– Idiopathic PAH (IPAH)
– Associated PAH (APAH)
• Connective tissue disease (CTD)
• Human immunodeficiency virus (HIV)
• Portal hypertension
• Anorexigens
• Congenital heart disease (CHD)
– Persistent pulmonary hypertension of the newborn (PPHN)
– PAH with venule/capillary involvement
Trigger: Mutation/Polymorphism
Trigger: Permissive Phenotype

Importance of Classification: Why do it?
• Efficacy: What’s the trigger? Can you change it?
• Safety: Can it hurt the patient?
• Cost: How much are we spending for limited efficacy and small changes in QOL?
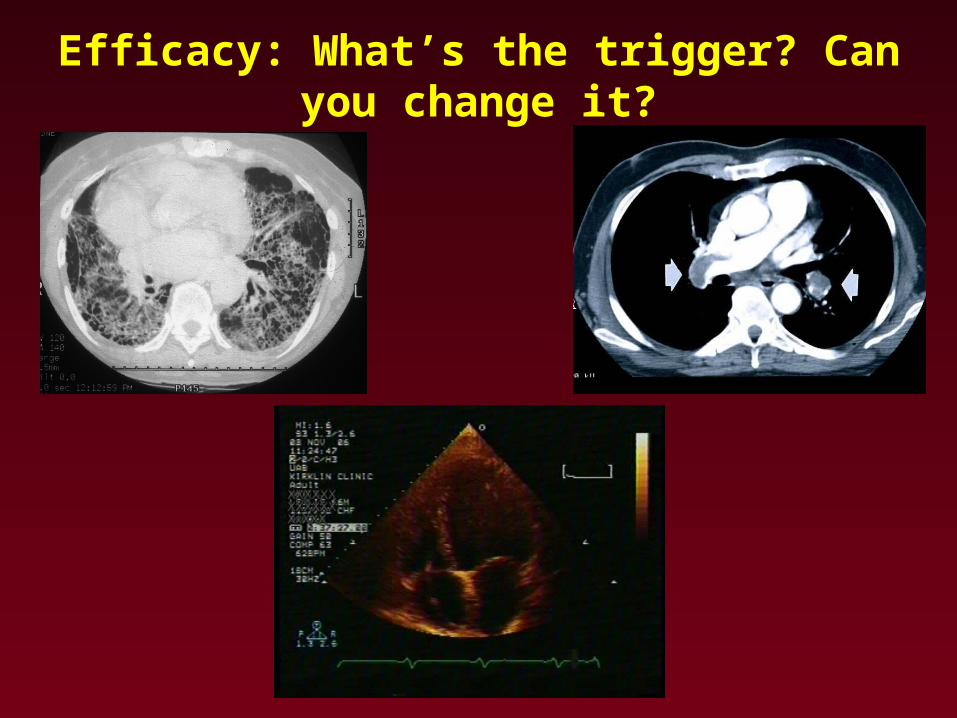
Efficacy: What’s the trigger? Can you change it?

Safety: Can it hurt the patient?
• LV dysfunction: Pulmonary edema
• ILD/COPD: Worsen V/Q mismatch
• CTEPH: Delay referral for
thromboendarterectomy

Cost: How much are we spending for limited efficacy and
small changes in QOL?
• Bosentan: ~35-40k per year
• Sildenafil: ~12-15k per year
• Inhaled Iloprost: ~60k per year
• IV Prostacyclins: ~60-120k per year

Pulmonary Arterial Hypertension
• Classification
• Diagnosis
• Prognosis
• Treatment

Schema for Patient Evaluation
Echocardiogram
Chest x-Ray
PFTs +/- Chest CT
? RVSP, RVE, RAE
Left heart disease (valvular, HF, CAD) Bubble echo - Congenital heart disease
Emphysema
FibrosisThoracic abnormality
Sleep study Obstructive Sleep apnea
VQ scan, angiogram Chronic thromboembolic disease
SerologiesHIVCTD: scleroderma, SLE, RA, MCTD
LFTs
Eval cirrhosis and Portal HTN
Portopulmonary Hypertension
RHCRequired for diagnosis of PAHVasodilator study

RHCDiagnosis PAH =
Cardiac Catheterization to Assess Severity and Prognosis of PAH
• To measure wedge pressure or LVEDP
• Scrutinize wedge tracings!!!!
• Wedge sat; End expiration
• To exclude or evaluate CHD
• To establish severity and prognosis
• To test vasodilator therapy
Catheterization is required for every patient with suspected pulmonary HTN.
LVEDP = left ventricular end diastolic pressure.

Pulmonary Arterial Hypertension
lumen
media
intima
adventitia
Normal pulmonary arteriole
Plexiform lesion
Pulmonary arteriole in PAH
Barst et al. J Am Coll Cardiol. 2004;43:40S-47S.
• Mean Pulmonary artery ≥ 25 mmHg (rest) ≥ 30 mmHg
(exercise).
• Wedge pressure ≤ 15 mmHg
• PVR > 3 Woods units
Pulmonary Venous Hypertension:
• Valvular heart disease (HD)
• Hypertensive HD
• Cardiomyopathies
• Transmitted pressure results in reactive vasoconstriction
Treat primary problem

Pulmonary Arterial Hypertension
• Classification
• Diagnosis
• Prognosis
• Treatment

Natural History of PAH: NIH Registry1,2
NIH = National Institutes of Health.Predicted survival according to the NIH equation. Predicted survival rates were 69%, 56%, 46%, and 38% at 1, 2, 3, and 4 years, respectively. The numbers of patients at risk were 231, 149, 82, and 10 at 1, 2, 3, and 4 years, respectively. *Patients with primary pulmonary hypertension, now referred to as idiopathic pulmonary hypertension.
1. Rich et al. Ann Intern Med. 1987;107:216-223. 2. D’Alonzo et al. Ann Intern Med. 1991;115:343-349.
Predicted survival*
69%
56%
46%
38%
Per
cent
sur
viva
l
Years

Survival by PAH Etiology
CHD = congenital heart disease; CVD = collagen vascular disease; HIV = human immunodeficiency virus; PAH = pulmonary arterial hypertension; PPH = primary pulmonary hypertension; PoPH = portopulmonary hypertension.McLaughlin et al. Chest. 2004;126:78S-92S.
0
20
40
60
80
100
0 1 2 3 4 5 6
CHD
CVD
HIV
PPH
PoPH
Years
Per
cent
sur
viva
l
Prognosis in Mixed Treated/Untreated Cohorts
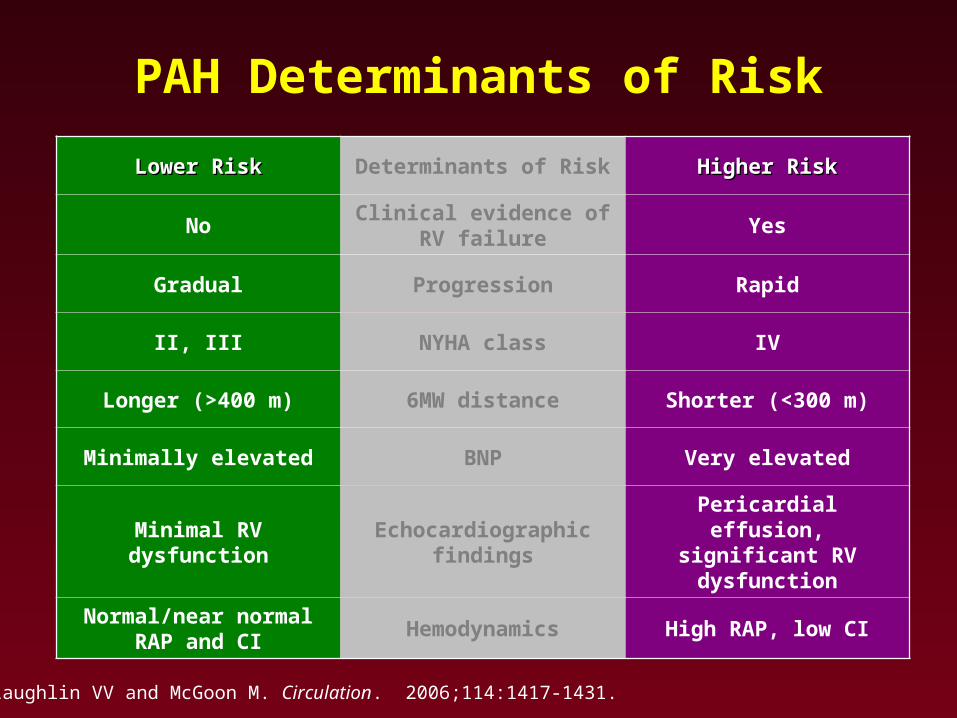
PAH Determinants of Risk
Lower RiskLower Risk Determinants of Risk Higher RiskHigher Risk
NoClinical evidence of
RV failureYes
Gradual Progression Rapid
II, III NYHA class IV
Longer (>400 m) 6MW distance Shorter (<300 m)
Minimally elevated BNP Very elevated
Minimal RV dysfunctionEchocardiographic
findings
Pericardial effusion,significant RV dysfunction
Normal/near normalRAP and CI
Hemodynamics High RAP, low CI
McLaughlin VV and McGoon M. Circulation. 2006;114:1417-1431.

McLaughlin VV, et al. Circulation. 2002;106:1477-1482.
0
20
40
60
80
100
Su
rviv
al (
%)
0 12 24 36 48 60 72 84
No. at risk 162 33 95 70 48 30 20 10
Months
FC=3
FC=4p=0.0001 by log-rank test
847260483624120
100
80
60
40
20
0
FC=1
No. at risk:
FC=2
FC=3
FC=4S
urv
ival
(%
)
Months
Impact of Functional Class on Survival
Functional Class at Baseline
Functional Class at 17±15 mos
102030466386112115

Correlation of Six-minute-walk Test and WHO Functional Class
*p<0.05 vs control subjects
†p<0.05 vs WHO functional class II
‡p<0.05 vs WHO functional class III
Miyamoto S et al. Am J Respir Crit Care Med. 2000;161:487-492.
0
100
200
300
400
500
600
700
800
Control WHO II WHO III WHO IV
Dis
tan
ce w
alke
d i
n 6
min
ute
s (m
)
*
*†
*†‡

Correlation of Six-minute-walk Test With Survival in PPH
0
20
40
60
80
100
0 10 20 30 40 50 60
Su
rviv
al r
ate
(%) Long distance group
(≥332 m)
Short distance group(<332 m)
Time (mo)
6-minute-walk distance strongly predictive of survival
– <332 m: 20% 3-year survival
– >332 m: 92% 3-year survival
Miyamoto S et al. Am J Respir Crit Care Med. 2000;161:487-492.

Nagaya N et al. Circulation. 2000;102:865-870.
p<0.05
p<0.0001
By multivariate analysis, higher BNP at baseline (RR=11.971, p=0.0348) and at follow-up (RR=25.880, p=0.0243) were independent predictors of mortality
0
20
40
60
80
100
0 12 24 36 48
BNP <150 pg/mL
BNP ≥150 pg/mL
Su
rviv
al r
ate
(%)
Time (mo)
0
20
40
60
80
100
0 12 24 36 48S
urv
ival
rat
e (%
)
Time (mo)
BNP ≥180 pg/mL
BNP <180 pg/mL
Baseline BNP Follow-up BNP
Plasma BNP as a Prognostic Indicator of Mortality in Patients With PPH

Predicting Survival andFollowing Therapy
• Clinical parameters
– functional class
– exercise capacity
– neurohormones
• Hemodynamics
• Imaging
– right ventricle: function and size
– pulmonary artery remodeling (future)

Schematic Progression of PAH
Time
PAP
PVR
CO
Pre-symptomatic/ Compensated
Symptomatic/ Decompensating
Symptom Threshold
CO=TPG
PVR
PAP=pulmonary artery pressure; PVR=pulmonary vascular resistance; TPG=transpulmonary gradient.Courtesy of: Vallerie V. McLaughlin, MD.

Schematic Progression of PAH
Time
PAP
PVR
CO
Pre-symptomatic/ Compensated
Symptomatic/ Decompensating
Symptom Threshold
Right Heart Dysfunction
Declining/ Decompensated
CO=TPG
PVR
PAP=pulmonary artery pressure; PVR=pulmonary vascular resistance; TPG=transpulmonary gradient.Courtesy of: Vallerie V. McLaughlin, MD.

Goals of Therapy
• Improve symptoms
– 6-minute walk (>380 m)
– functional class (I or II)
– CPET (VO2 max >10.4)
– quality of life
• Improve hemodynamics
• Improve survival

What Drug and When

PAH Treatments―a Historical Overview
CCB, anticoagulation, digitalis, diuretics
EpoprostenolBosentan Iloprost
Ambrisentan
Sildenafil
SC treprostinil
IV treprostinil
CCB = calcium channel blocker.
<1995 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007

When to use a Calcium Antagonist ?

(Years)
Long-term CCB responders
Long-term CCB failure
38 33 30 22 13 8 3 3 2 1
19 12 7 4 0Subjectsat risk, n
Cum
ulat
ive
Sur
viva
l
Long-term CCBrespondersLong-term CCBfailure
0
.2
.4
.6
.8
1
0 2 4 6 8 10 12 14 16 18
O. Sitbon et al. Circulation 2005;111:3105-3111
Survival in IPAHLong-term CCB responders
p=0.0007

PAH
Basic therapy
Oral anticoagulants, Diuretics, O2, Digoxin ...
Oral CCB
Continue CCB
Sustained Response
Yes
Positive Negative
Vasodilator study
No CCB +++
Fall in mPAP > 10 mmHg+ mPAP < 40 mmHg+ Normal CO
Sitbon O, et al. Circulation. 2005;111:3105-3111.
3rd World PAH Symposium. J Am Coll Cardiol 2004;43:1S-90S.
ACCP Guidelines. Chest 2004;126:1S-92S.
Galiè N, et al. ESC Guidelines. Eur Heart J 2004;25:2243-78.
Close monitoring of long-term clinical and hemodynamic effects

Vasodilator StudyAnticoagulate ± Diuretics ±
Oxygen ± Digoxin
Sustained Response
Positive
Oral CCB
Continue CCB
Yes
Negative
Lower Risk Determinants of Risk Higher Risk
NoClinical Evidence of
RV FailureYes
Gradual Progression Rapid
II, III NYHA Class IV
Longer (>400 m) 6 Minute Walk Distance Shorter (<300 m)
Minimally elevated BNP Very elevated
Minimal RV DysfunctionEchocardiographic
FindingsPericardial Effusion
Significant RV Dysfunction
Normal/Near normal RAP and CI
Hemodynamics High RAP, Low CI
What is the Optimal Treatment Strategy?
McLaughlin VV and McGoon M. Circulation. 2006;114:1417-1431.
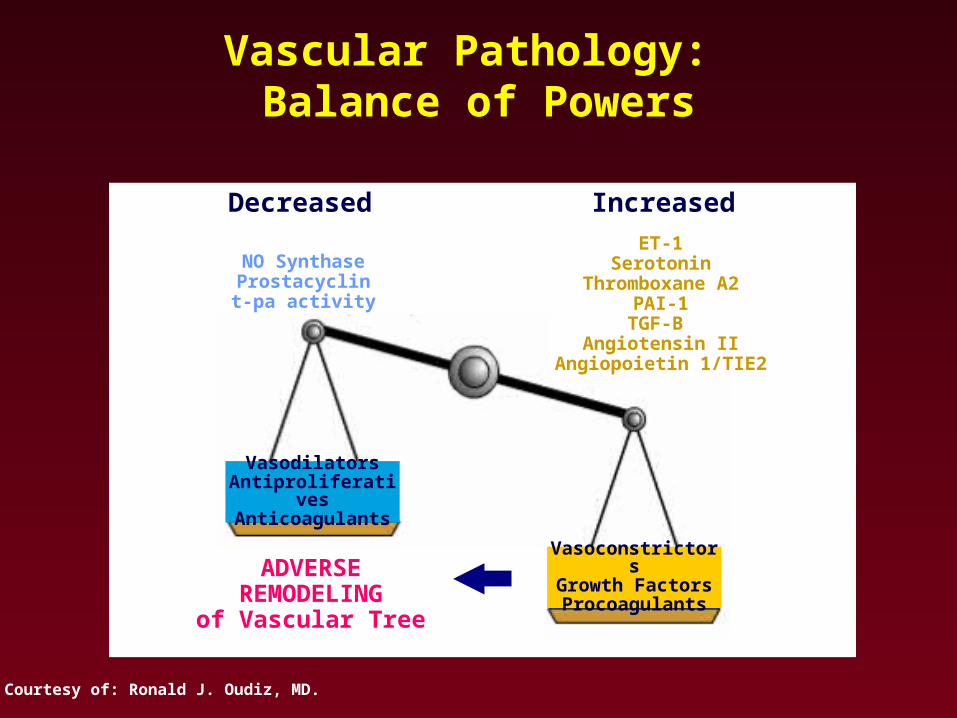
Vascular Pathology: Balance of Powers
Courtesy of: Ronald J. Oudiz, MD.
VasodilatorsAntiproliferativesAnticoagulants
VasoconstrictorsGrowth FactorsProcoagulants
ET-1Serotonin
Thromboxane A2PAI-1
TGF-B Angiotensin II
Angiopoietin 1/TIE2
NO SynthaseProstacyclint-pa activity
ADVERSE REMODELING
of Vascular Tree
IncreasedDecreased

↓ vasoconstriction
↓ proliferation
Prostacyclins
• Intravenous (epoprostenol, treprostinil)*
• Subcutaneous (treprostinil*)
• Inhaled (iloprost*, treprostinil†)
• Oral (beraprost‡)
*FDA approved†Investigational/in development
‡Non-FDA approved

Epoprostenol: Indications
• NYHA Class III or IV PAH
• Contraindicated in severe LV systolic dysfunction (LVEF <30%)
• Cost ~ $60,000 to $120,000/year depending on dose

Important Points: Epoprostenol
• Functional capacity, hemodynamics, and survival are improved
• Baseline NYHA functional class is predictor of survival
• Response after 12 to 18 months can predict subsequent outcomes
• Most benefit apparent in first 12 to 18 months
• Dosing: Outcomes with moderate dosing are the same as with aggressive dosing
McLaughlin VV et al. Circulation. 2002;106:1477-1482.

IV Treprostinil
• Approved by FDA in January 2005
• Has safety (longer half-life) and convenience advantages (no mixing or cold packs, smaller pump) over IV epoprostenol
• Can be used for de novo patients and transitions from epoprostenol
• Improvements in hemodynamics and functional status similar to epoprostenol
• Requires at least double the epoprostenol dose (may be more expensive)

SC Treprostinil• Requires capable patient
• Site pain is major impediment
– Affects 85%
– Local measures: ice, heat, lidocaine, capsaicin, collagenase ± effective
– NSAIDs, narcotics, gabapentin ± effective
– PLOgel new topical; promising, but unconfirmed reports of benefit; not useful at active site
• Expensive (~$60,000 to $120,000/year)
• pain
• erythema
• induration
• pain
• erythema
• induration

Inhaled Iloprost
• Approved for class III - IV PAH
• Duration of hemodynamic effect only 90 minutes
• Requires frequent administration; at least 6x/day at 10 to 15 minutes
• Has favorable effects on gas exchange in pulmonary fibrosis
• Cost of ~ $60,000-$70,000/year
Olschewski H, et al. N Engl J Med. 2002;347:322-329.

Endothelin Antagonists (ERAs)
• Oral
– “Nonselective” ERA/ERB
• Bosentan*
– “Selective” ERA
• Ambrisentan*
• Sitaxsentan†
*FDA approved†Investigational/in development

Bosentan (Tracleer) Indication
• PAH with WHO Class III (or II - IV) symptoms “to improve exercise capacity and decrease the rate of clinical worsening”
• Dose 62.5 mg BID oral for 4 weeks
• 125 mg BID oral thereafter if liver functions OK
• Costs ~$36,000/year
• Contraindicated with glyburide and cyclosporine
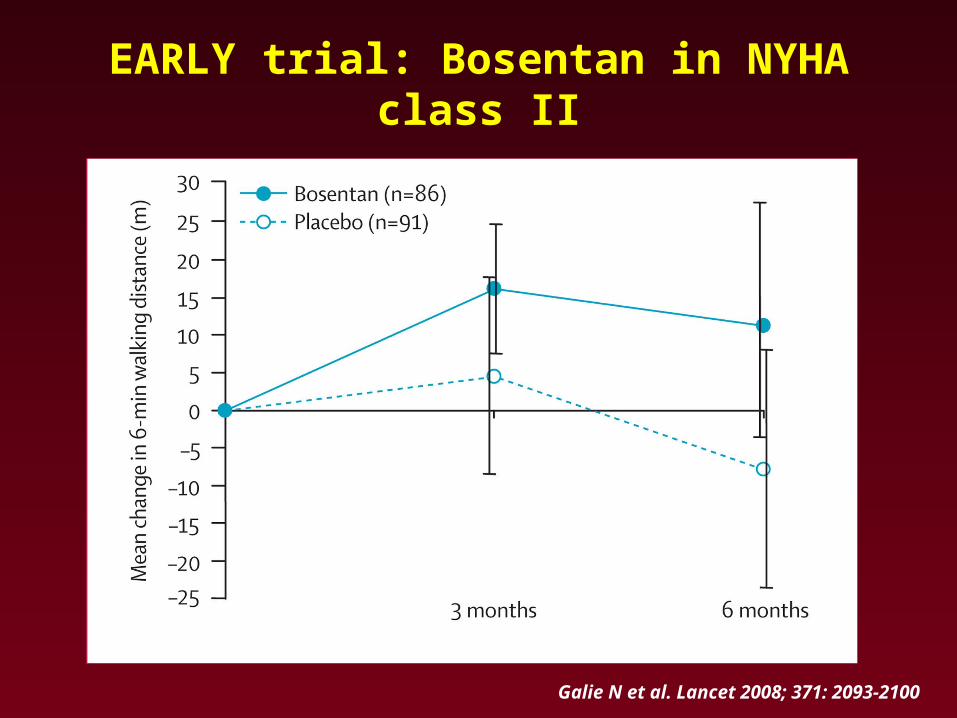
EARLY trial: Bosentan in NYHA class II
Galie N et al. Lancet 2008; 371: 2093-2100

Bosentan Monitoring
• Liver enzymes: initial and monthly (stop if >5x elevation) reversible with cessation; can try rechallenge with lower dose
• Watch for leg edema/pulmonary edema/nasal congestion
• Hemoglobin: initial, 1 and 3 months
• May interfere with hormonal birth control; barrier method advised
• Caveat: Response takes time (up to 2 to 3 months), should be used with caution in Class IV patients and not without right heart catheterization to document presence of PAH

Ambrisentan (Letairis) Indication
• PAH with WHO Class II - III symptoms “to improve exercise capacity and decrease the rate of clinical worsening”
• Dose 5 mg qD
• Consider increasing to 10 mg qD if tolerated
• Costs ~$36,000/year
• Contraindicated with cyclosporine

Which ERA?
• FDA approved: both
• Cost: similar
• Dosing: BID (bosentan) vs QD (ambrisentan)
• Sildenafil interaction (bosentan)
• LFT issue: 11% bosentan vs 2-3% ambrisentan
1. Galie N, et al. Presented at: the Annual Meeting of the American Thoracic Society; May 20, 2005; San Diego, CA

PDE 5 Inhibitors
• Oral
– Sildenafil*
– Tadalafil†
*FDA approved†Investigational/in development

Sildenafil
• FDA approved in June 2005 for PAH (WHO Group 1) “to improve exercise ability” regardless of functional class
• Must not be used with nitrates, but compatible with other drugs
• Metabolized by liver (CYP3A4 isoenzyme), slowed in cirrhotics, no effect of renal failure
• Oral and relatively inexpensive (~ $12,000/year)
• Side effects: headache, Blue haze periphery of vision in up to 11%

-30
-20
-10
0
10
20
30
40
50
60
70
Week 4 Week 8 Week 12
placebo sildenafil 20mg sildenafil 40mg sildenafil 80mg
*p<0.0001
****
**
Sildenafil in PAH: SUPER-1, 6-Minute Walk Test Change from Baseline to Week 12
45 m
46 m
50 m
n=278
Ch
ang
e fr
om
Bas
elin
e (m
)
Ghofrani HA, et al. Presented at: the 20th Annual Meeting of the American College of Chest Physicians; October 23, 2004; Seattle, Washington.

0
10
20
30
40
50
60
70
Week 12 (n=149) Month 12 (n=149)
6-M
WD
Me
an
Ch
an
ge
fro
m
Ba
se
lin
e (
m)
(95
% C
I)
Exercise Capacity at Week 12 and 1 Year
Mean = 50 mMean = 54 m
Rubin L, et al. Presented at: the Annual Meeting of the American Thoracic Society; May 20, 2005; San Diego, CA.

Investigational Protocols
Vasodilator StudyAnticoagulate ± Diuretics ±
Oxygen ± Digoxin
Oral CCB
Continue CCB
Higher Risk
Sustained Response
Positive
Lower Risk
Yes
Negative
What is the Optimal Treatment Strategy?
Atrial septostomyLung Transplant
Reassess – considercombo-therapy
ERAs or PDE-5 Is (oral)Epoprostenol or Treprostinil (IV)
Iloprost (inhaled)Treprostinil (SC)
No Epoprostenol or Treprostinil (IV)
Iloprost (inhaled)ERAs or PDE-5 Is (oral)
Treprostinil (SC)
McLaughlin VV and McGoon M. Circulation. 2006;114:1417-1431.

Rx of Heart FailureRx of Heart Failure
Jessup M, Brozena S. N Engl J Med. 2003;348:2007-2018.
Stage AHigh risk with no
symptoms
Stage BStructural
heart disease, no symptoms
Stage CStructural disease,
previous or current
symptoms
Stage DRefractory symptoms requiring special
intervention
Risk factor reduction, patient and family education
Treat hypertension, diabetes, dyslipidemia; ACE inhibitors or ARBs in some patients
ACE inhibitors or ARBs in all patients; beta-blockers in selected patients
ACE inhibitors and beta-blockers in all patients
Dietary sodium restriction, diuretics, and digoxin
Cardiac resynchronization if bundle-branch block present
Revascularization, mitral-valve surgery
Consider multidisciplinary team
Aldosterone antagonist, nesinitide
Inotropes
VAD, transplantation
Hospice

Early, Risk-based and
Combination Therapy:
Changing Paradigms for PAH?

Rx of Pulmonary HypertensionRx of Pulmonary Hypertension
Stage A
High risk with no
symptoms
Stage B
PAH with+ VDC
Stage C
PAH with - VDC
Low Risk
Stage D
Refractory symptoms requiring special
intervention
Risk factor reduction, patient and family education
Calcium Channel Blockers
Bosentan +/- Sildenafil +/- Ventavis
Dietary sodium restriction, diuretics
Aldactone and digoxin
IV meds (Flolan or Trepostonil)
Consider multidisciplinary team
Inotropes, atrial septostomy
Transplantation
Hospice
Stage C
PAH with - VDC
High Risk
Combination therapy
Sleep apnea, Obesity, Uncontrolled hypertension and/or depress LVEF, drug abuse

Hoeper et al. Eur Respir J. 2005;26:858-863.
Goal-Oriented TherapyDiagnosis of PAH
Vasoreactivity test negativeNYHA II or IV
Baseline examination and 3-to-6-month reevaluation to assess treatment goals(6MWD >380 m, peak VO2 >10.4 mL/min/kg,
peak systolic BP >120 mm Hg during exercise)
Treatment goals not met
First-line treatment bosentan
Treatment continued
Addition ofsildenafil
Treatment continued
Addition ofinhaled iloprost
Treatment continued
Transition from inhaled to intravenous iloprost
Treatment continued
Highly urgent lung transplantation

• Traditional therapies; diuretics, oxygen, phlebotomy still used as indicated; anticoagulants recommended
• Calcium Channel Blockers should be used in Class II or III acute responders but followed closely for safety & efficacy
• Newer agents are tailored to WHO class – ACCP Guidelines
– Class IV – Infused prostacyclins
– Class III – Oral endothelin receptor antagonists (ERAs), phosphodiesterase (PDE) 5 inhibitors, infused or inhaled prostacyclins
– Class II – PDE 5 inhibitors, or ERAs
• Consider therapy if evidence of Right Ventricular Dysfunction
• Combination therapies and an array of investigational therapies hold hope for the future
• Role of transplantation/septostomy now diminished because of new effective pharmacologic therapies
Summary:
Treatment

Rubin, L. J. et. al. Ann Intern Med 2005;143:282- 292
Indications for Referral to a Specialized Center for Rx of PAH
Unexplained dyspnea on exertion with evidence of PH on Echo
Evidence of moderate to severe PH•Estimated PAS pressure > 45 mm Hg on Echo•Symptoms consistent with NYHA functional class II or worse•Near-syncope or syncope
Absence of substantial left- sided cardiac disease or parenchymal lung disease
Clinical or echocardiographic evidence of RV dysfunction•Lower-extremity edema•Ascites•Right ventricular enlargement or systolic dysfunction on echocardiography



Rubin, L. J. et. al. Ann Intern Med 2005;143:282-292
The Role of PCP in Dx and Coordinated Care of PAH
RECOGNIZEpossible PAH in the pt w unexplained DOE
INITIATEappropriate SCREENING•CXR, PFT, Echo, VQ, Oximetry
FACILITATEappropriate referral to specialty center•Contact the specialist in PAH•Obtain referrals and approvals from pt’s insurer• Provide pt’s records to the specialty center
PROVIDEregular FOLLOW UPin the pt’s local community•Assess volume status, vital signs and oxygenation•Monitor lab tests : E-lytes, LFTs, BUN/Cr•Manage anticoagulation for INR 2-3
PROVIDE EMERGENCY CAREin the pt’s local community

Adapted from Gaine S. J Am Med Assoc 2000;284:3160-68
Normal ArteryNormal Artery Reversible DiseaseReversible Disease Irreversible DiseaseIrreversible Disease
PAH: A Progressive Vasculopathy
Stop progression and Reverse Disease

IPAH: Contrast enhanced CT shows dilated pulmonary artery with mosaic attenuation in the lung parenchyma.
Non-PAH: Severe ILD: Coarse reticular changes with honeycombing suggesting pulmonary fibrosis in the lower lobes in this patient with IPF
Using Appropriate Diagnostic Strategies for Appropriate Patient Types: HRCT

Other Investigational Therapies
• Statins (HMG coreductase inhibitors)
• K+ channel openers
• NO donors
• Rho kinase inhibitors
• Tyrosine kinase inhibitors
• Angiogenesis factors
• Gene therapy
– NOS, K+ channel openers
• Serotonin receptor antagonists
• Inhaled vasoactive intestinal peptide

Subcutaneous
Patient
No
No
Low
No
No
HoursHoursMinutesHalf-life
Yes (no ice)YesBulky pump
HighHighRisk of serious infections, including sepsis
LowHighRisk of cardiovascular collapse
NoYesSterile conditions for frequent drug constitution required
YesYesThrombus
SurgicalSurgicalImplant of catheter
IntravenousIntravenousDelivery of drug
TrepostinilEpoprostenolCharacteristic
Subcutaneous Treprostinil: Potential Advantages Over IV

Indications for SC Treprostinil
• PAH with WHO Class II to IV symptoms
• Cost ~$60,000 to $120,000/year (exclusive of costs for administration/monitoring; IV more expensive)

Treprostinil Sodium Injection
• Administered via continuous infusion using an ambulatory pump designed for subcutaneous infusions
• Administered via a self-inserted subcutaneous catheter
• Patients must have immediate access to backup infusion pump to prevent the risk of worsening of PAH symptoms due to interruption of therapy

Smooth muscle cell vasoconstriction Smooth muscle cell proliferation? Apoptosis
The Endothelin System
SMC ETB
EC ETB
ReceptorETA
TrpIleIleAspLeuHisCysTyrVal PheCys
CysCys Ser
Glu
SerSerLeu
Met
Asp
Lys
N
C
ET convertingenzyme
ET-1
Big ET-1
sitaxsentanambrisentan
bosentan
Circulating ET-1 levels in PAH PA endothelial cell expression in PPH

Summary:
Use of Clinical Parameters, Hemodynamics, and Imaging Techniques to Predict Survival and Therapeutic Options
• High index of suspicion
• Thorough diagnostic evaluation, need RHC
• Exclude thromboembolic disease
• Vasodilator testing to eliminate inappropriate CCB use

PlaceboPlacebo44 meters44 meters