publisher - arcus sportklinik und klinik · main focuses are on sports traumatology, knee-, hip-,...
TRANSCRIPT


September 2009
Imprint:
Publisher:ARCUS Kliniken PforzheimRastatter Str. 17-1975179 PforzheimPhone: +49 7231 60556 0 web www.sportklinik.deemail [email protected] Editorial Management:Prof. univ. cath. Cuenca EC Bernhard [email protected] Editor and Marketing:Heiko [email protected] Graphics & Layout:Buero 01Pforzheim Print:Kraft Druck GmbHEttlingen
Disclaimer:Please note that statements made in this brochure are of general nature and do not necessarily apply for every patient. Therefore, individual advice of your treating physician is absolutely necessary.

3
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Welcome
Dear patients,
With this information brochure we would like to present you the most important part of our operative work. We refer to 20 years of own experience in in- and out-patient services and the current scientific status.
Since 1989, more than 65.000 patients have been operated and about 150.000 patients treated in the ARCUS Clinics. With more than 7.600 surgeries and about 38.000 treated patients in 2009, we have become one of the biggest orthopaedic sports-traumatologic accidental surgery centers in Germany and Europe.
Where does this success come from?
It is based on tireless dedication and hard work, consequent implementation of latest operation- and treatment methods and full use of the best technical possibilities. We always used a substantial part of our revenues for new investments. And finally, in 2006, we were able to open up a new clinic equipped with the highest technical standards and a very pleasant, patient- and staff-friendly atmosphere. It has more than 6 operating theatres, 70 beds and 22 beds in the ward station on a total of 17.000 m² that means together with already available capacities of the former cli-nic 9 operating theatres, 90 inpatient beds and 30 ward station beds. The clinic is divided into a private clinic and a clinic for other patients with 30 beds which are listed on the bed requirement planning of the state of Baden-Württemberg. Here, also patients with statutory health insurance can be offered in-patient treatment.
We want to provide you an understandable overview of our range of services and answer open questions in the case of a planned operation. Should you have any further questions about our services, special surgery techniques or our clinics in general, please do not hesitate and contact us.
More information please find on www.sportklinik.de
Your ARCUS Clinics Team
Gen
eral Info
rmatio
n
4 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Table of Contents
General Information
Welcome 3
Table of Contents 4
Clinic Portrait / Competence Center / Science 6
Basic Values of the ARCUS Clinics Pforzheim 7
Spectrum of Surgery / Facts & Figures 8
Medical Management 9
Specialist Areas 11
Diagnostics 12
Quality Management 15
Interesting Facts & Organization 16
Anesthesia 18
Operative Spectrum - Knee
Meniscus 22
Anterior Cruciate Ligament (ACL) 26
Knee-Cap (Patella) 33
Arthrosis 36
Orthobiology 44
Knee Malalignment 46
Knee Endoprosthetics 49
Operative Spectrum - Shoulder
Shoulder Impingement Syndrome 55
Calcified Tendinitis of the Shoulder (tendinosis calcarea) 57
Shoulder Luxation 59
Rotator Cuff Damages 61
Injuries and Arthrosis of the Acromioclavicular Joint (AC-joint) 63
Collarbone Fracture (clavicle fracture) 65
Humeral head fracture 67
Shoulder Endoprosthetics 69
Operative Spectrum - Hip
Hip Joint Arthrosis (coxarthrosis) 73
Hip Arthroscopy 76
Step-by-step Plan for Treatment of Coxarthrosis 78
Total Endoprosthesis: Material and Fixation 79
5
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Gen
eral Info
rmatio
n
Operative Spectrum - Elbow
Tennis Elbow 82
Golfer’s Elbow 84
Sulcus-ulnaris Syndrome or Cubital Tunnel Syndrome 84
Loose Joint Bodies 85
Osteochondrosis Dissecans 85
Stiff Elbow and Elbow Arthrosis 86
Elbow Prostheses 87
Luxations and Instability 88
Operative Spectrum - Foot
Foot / Ankle / Achilles Tendon 89
Big Toe 89
Small Toe 91
Metatarsus/ Tarsus 92
Heel 93
Achillodynia 94
Achilles Tendon Rupture 95
Ankle Disorders 96
Neurosurgery / Spinal Column
General Information 102
Cervical Spine (CS) 103
Lumbar Spine (LS) 109
How to find us 115

6 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
The ARCUS Clinics – a Portrait
6
The ARCUS Clinics comprise a private clinic with 60 beds which was opened in 1995, and a clinic also approved by the statutory health insurance system with 30 beds. The new clinic complex was opened up in 2006. Here, 6 operating theatres equipped with state-of-the-art technology, and 22 beds in the ward station and the intensive care unit are available.The privately insured patient which can chose individual surgical treatment within the private clinic is offered a specialized unit with first class hotel comfort – an excellent overall service.The statutorily insured patient is, although statutory health insurance companies do only pay for “basic primary health care”, still provided a high-level clinic standard i.e. a standard on far above-average level compared to most other clinics.
Competence Center
In the ARCUS Clinics up to 7.500 patients are operated each year – with increasing tendency. Main focuses are on sports traumatology, knee-, hip-, shoulder-, elbow-, orthopedic-, and accident surgery, endoprosthetics and in the private clinic also on spinal surgery. External cooperating surgeons additionally cover vascular- and neu-rosurgery and an experienced team of anesthetists offers besides intra-operative control also post-operative pain therapy for in-patients. In cases of cardiologic problems during and after surgery we can refer to our cardiology section and state-of-the-art technical equipment.In the adjoining orthopedic joint practice patients can get out-patient treatment. This enables us to constantly control and optimize our own operation- and aftercare results what already proved successful e.g. rehabilitation periods of our patients could demonstrably be shortened.Special importance since many years has treatment of top athletes in the conservative and surgical area. As medical partner of the “Deutsche Sporthilfe” we offer a 24-hour acute service for sponsored top athletes. This comprises best diagnostics, operative treatment if necessary and a comprehensive rehabilitation program to accelerate recovery and support the athlete to regain physical fitness as soon as possible.Our medical range of services is completed by cooperating partners in therapy, rehabilitation, prevention and orthopedic technology.Perfect interdisciplinary collaboration of surgeons of different areas, physiotherapists and orthopedic technicians form the basis for an optimal and focused patient care both in the in- and the out-patient sector.
Science
The leading physicians of the ARCUS Clinics are members of all important national and international professional associations and regularly work for them as referees. Moreover, the ARCUS Sports Clinic cooperates with the association for science and further education in orthopedics. Together they regularly organize training pro-grams for physicians and physiotherapists which are acknowledged as such by the Ärztekammer Nordbaden.
7
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 7
Gen
eral Info
rmatio
n
Basic Values of the ARCUS Clinics Pforzheim
Our Mission
Our Medical Demand
In the ARCUS Clinics Pforzheim, long-term experience and specialization in different medical areas as well as use and development of medical state-of-the-art technology is the key to success. Scientific exchange of experiences and know-how is part of our daily work life. Our international appreciation is our continuous commitment.
Patient Focus
Orientation towards the patient – our customer – is the basis of our activities. We make highest demands on the quality of patient care and offer dedicated medical attendance from prevention and therapy until rehabilitation. Competent care and service improve healing results.
The architecture of the ARCUS Clinics creates an environment where efficiency and the patients’ individual needs are optimally harmonized.
Employee Focus
The dedication of our qualified employees ensures the success of our clinic. Therefore we expect above-average performances and support professional development by providing further education measures. Professional and socially competent com-munication between the employees is the most important condition for a good working team.
Managers are role models and support the employees’ dedication through a coope-rative management style.
Economy
Since many years now, the ARCUS Clinics Pforzheim have been successful private facilities on the health sector.
Optimal treatment concepts and results as well as economic success are inseparably linked with each other and one area strengthens the other.

8 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Spectrum of Surgery / Facts & Figures
Figures
2009 1.Quarter 2010
Anterior Cruciate Ligament Surgery 1222 335
Meniscus Surgery 1632 394
Cartilage Surgery 175 41
Hip Arthroscopy 172 60
Shoulder Surgery 1101 348(except prostheses)
Elbow Surgery 179 68
Total 7671 2210(except prostheses)
Endoprosthetics (artificial joints)
2009 1.Quarter 2010
Knee 662 210
Hip 327 109
Shoulder 101 36
Total 1105 361

9
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 9
Gen
eral Info
rmatio
n
Medical Management
Prof. univ. cath. Cuenca ECBernhard RieserMedical DirectorPartner of the ARCUS Sports ClinicMedical Specialist for Orthopedic Surgery
Dr. med. Wolfgang MiehlkeLeading PhysicianMedical Specialist for Ortho-pedic Surgery, Trauma Surgery and Sports Medicine
Prof. Dr. med. Christian HeiselLeading PhysicianMedical Specialist for Orthopedic Surgery, Special Orthopedic Surgery and Trauma Surgery
Dr. med. Ludwig BösLeading PhysicianPartner of the ARCUS Sports ClinicMedical Specialist for Orthopedic Surgery and Sports Medicine
Dr. med. Thomas AmbacherLeading PhysicianMedical Specialist for Orthopedic Surgery, Trauma Surgery and Sports Medicine
Prof. Dr. med. Uwe SpetzgerLeading PhysicianMedical Specialist for Neurosurgery
Dr. med. Andree EllermannLeading PhysicianPartner of the ARCUS Sports ClinicMedical Specialist for Orthopedic Surgery, Trauma Surgery, Sports Medicine and Chirotherapy
Prof. Dr. med. Rüdiger Schmidt-WiethoffRüdiger Schmidt-WiethoffLeading PhysicianMedical Specialist for Orthopedic Surgery, Special Orthopedic Surgery, Trauma Surgery and Sports Medicine

1010
Kreuzbandriss Arthrose Varus Valgus Kinderversorgung
DIE KN IEORTHESE AUS CARBONFASER
INDIVIDUELLE ANFERTIGUNG, EXTREM LEICHTMIT OPTIMALER ANATOMISCHER PASSFORM
ORTEMA PFORZHEIM ORTEMA PFORZHEIM DAS K-COM KNIEORTHESENKONZEPTDAS K-COM KNIEORTHESENKONZEPT
Herz l i c h
Wi l lkommenHer z l i c h
Wi l lkommen
UNSERE LEISTUNGEN IM ÜBERBLICK:
Rumpforthesen-Technik:Fixierend und wachstumslenkend
Orthesen und Knieorthesen:Stabilisierung und Entlastung
Arm- und Beinprothesen:Nutzung modernster Technologien
Sport-Orthopädie:Protektion & Prävention
Schuh- und Einlagen-Technik:Korrektur des Gangbildes
Bandagen-Technik:Von Kopf bis Fuß nach Maß
ORTEMA GmbH Filiale Pforzheim · Rastatter Straße 17-19 · 75179 Pforzheim · Tel. +49(0)72 31-139 66 67 · Fax +49(0)72 31-1 39 66 84 · [email protected] GmbH Filiale Waiblingen · Alter Postplatz 13 · 71332 Waiblingen · Tel. +49(0)7151-985994-0 · Fax +49(0)7151-985994-94 · [email protected]
Hauptsitz ORTEMA GmbH · Kurt-Lindemann-Weg 10 · 71706 Markgröningen · Tel. +49(0)7145-912081 · Fax +49(0)7145-912980 · [email protected]
www.ortema.de

11
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Specialist Areas
11
We cover the whole spectrum of orthopedic surgery. Therefore, in order to ensure our high quality standard, eight leading physicians manage the area of their spe-cialization.
Our Focus Areas:
• Sports Traumatology
• Knee Surgery
• Shoulder- and Elbow Surgery
• Hip Surgery
• Foot- and Ankle Joint Surgery
• Endoprosthetics
• Trauma Surgery
• Neuro- and Spinal Surgery (for privately insured patients and self-payers)
• Blood Vessel Surgery
• Cardiology
Specialist Practices within the ARCUS Clinics
Besides the orthopedic clinics, there are also different specialist practices integra-ted into the ARCUS Clinics complex to extend the spectrum.
• Orthopedic joint practice Rieser / Bös / Ellermann / Miehlke / Ambacher / Schmidt-Wiethoff / Heisel / Sobau
• Private practice for neuro- and spinal surgery Prof. Dr. med. Uwe Spetzger
• Practice for radiology and nuclear medicine Dr. med. Berthold Winter
• Private practice for cardiology Dr. med. W.O. Schüler & Colleagues
• Specialist practice for anesthesia and pain therapy Dr. med. Carla Weber
Gen
eral Info
rmatio
n

12 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Diagnostics
12
Thanks to state-of-the-art technical equipment of the latest generation, the ARCUS Clinics can always refer to the best method to provide optimal diagnostics and therapy planning.
Cross-Sectional Diagnostic Imaging and Digital X-Ray
In the adjoining practices there exist two 1.5 Tesla MRI scanners (nuclear spin) with the latest equipment, technology for digital X-ray, a Dual Source CT, a nuclear medi-cine section as well as a cardiac catheter laboratory for comprehensive diagnostics.
All digital images taken with CT, MRI and digital X-ray as well as the arthroscopic images generated during surgery are stored in a central PACS-system and can be retrieved at any time in the treatment rooms of the orthopedic joint practice, the wards and in the operating theatres. There are certified monitors available for reporting in all sections.
CT (computed tomography)
The Siemens Dual Source SOMATOM Definition CT (2 x 64 rows) is by using a second x-ray tube and a second detector much more efficient than devices of the “simple” construction. Its excellent image quality and high resolution at the lowest possible radiation exposure for the patient enables fast and precise diagnosis and increases its reliability. It also enables us to examine coronary heart vessels without cardiac catheter. Temporal resolution of the SOMATOM Definition is with 83 ms not depen-dant on the patients’ heart rate. This makes it possible to examine every heart at every heart rate e.g. diagnosis of acute chest pain, visualization of coronary arteries and function analysis of the heart. Combined with the currently highest possible resolution of less than 0.4 mm, the SOMATOM Definition can display smallest anato-mic structures, whether complex osseous structures or finest details of the coronary tree. Thanks to the large gantry aperture, the scan length of 200 cm and the highest possible x-ray generator performance almost all acute in-patients regardless of their physical constitution and size can be examined and valuable time gained between scan and diagnosis.
MRI (magnetic resonance imaging = nuclear spin tomography)
The ARCUS Clinics have two 1.5 Tesla MRIs of the latest generation at their disposal. Equipped with AudioComfort, a combination of several innovative technical mea-sures for noise reduction, the former usual noise level reached during MRI can be reduced by up to 97%. The ability to scan the patient in the feet first position as well as total-body examinations in the time of only 12 minutes make the Magnetom Avanto the most efficient and patient-friendliest system of its class and is decisive for pre-operative diagnostics of poly-traumatized patients.
The Magnetom Avanto is furthermore equipped with the new and innovative Tim-technology. Heart is the revolutionary matrix coil concept where 76 coil elements can be combined with up to 32 high-frequency channels [76x32]. This visibly improves recording speed and picture quality. The Magnetom Avanto also stands out through

13
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 13
Gen
eral Info
rmatio
n
especially powerful gradient systems (comparable with “motors” for MR), what facilitates fast examinations of the heart or detailed analyses of brain functions.
Cardio MRI is thanks to modern software a simple and fast examination of heart function, myocardial morphology, extension of infarction and 3D-coronary anatomy. In most cases the examination is completed in less than 30 minutes. This method is of particular importance for sports medicine. The decided diagnostic of heart muscle inflammation is not comparable with any other method.
Digigal X-Ray
The orthopedic joint practice has a dose-reduced direct-digital x-ray apparatus at its disposal. With only 40% of usual radiation exposure it enables images with higher resolution and therefore better basis for diagnostics.
Mobile CT and Navigation Device
With the CT, complex surgery procedures can also be carried out with navigation. This enables better results when being confronted with complicated anatomic con-ditions or complex fractures.
Operating Theatres
All nine operating theatres are connected to the digital clinic network. This ensures internal as well as external data transfer. All images taken during surgery are recor-ded and stored in the patient’s file. By means of an external surrounding camera system also transfer of external footage is possible (besides arthroscopic images). When conducting live-surgery, this enables transfer of e.g. positioning of the pati-ent or preparation of transplants/implants to national and international congresses and other events.
On two screen walls, surgery can be followed from the outside. The operation ma-nager is responsible for occupancy and optimal allocation of the operating theatre.
Sterilization Zone
Our operating theatres are provided with sterile material via nonintersecting corri-dors. Sterilization is equipped with top quality devices only. Each instrument used can be referred to the respective patient via a bar code. With this, absolute traceability, the so-called sterile-chain can be documented.
A modern system documents all working steps and provides insight into availability of the OP sets. Moreover it automatically controls withholding periods.
Diagnostik

14 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Anzeige
ARCADIS Orbic 3D - Mehr Präzision bei der operativen Versorgung von Knochen- und Gelenkbrüchen
Die präzise Identifizierung und Repositionierung dislozierter Knochenfragmente, das Setzen von Pedikelschrauben in die Wirbelsäule und die Lagekontrolle von Osteosyn-thesematerial zählen zu den größten Herausforderungen in der Unfallchirurgie und Neurochirurgie. In vielen Fällen liefert die konventionelle 2D-Projektionsbildgebung nicht genügend Informationen, um solche Eingriffe präzise zu kontrollieren. Für die exakte Versorgung von Knochen- und Gelenkfrakturen steht mit dem mobilen C-Bogen ARCADIS® Orbic 3D von Siemens ein hervorragendes System zur Verfügung, das mittels der interaoperativen 3D-Bildgebung deutliche Informationsvorteile über die jeweilige Fraktur der Knochen und Gelenke im Vergleich zu herkömmlicher 2D-Bilddarstellung bietet. Hauptanwendungen sind Versorgungen der oberen und unteren Extremität, der gesamte Wirbelsäule, Hüfte/Becken sowie des Gesichtsschä-dels. Die intraoperative 3D-Bildgebung ermöglicht dem Chirurgien die sofortige Beurteilung der Ergebnisse, wie z.B. der Lagekontrolle von Schrauben. Notwendige Korrekturen können direkt während der OP erfolgen, das postoperative CT wird in den meisten Fällen nicht mehr benötigt und eine nochmalige Operation kann vermieden werden. Dies bedeutet eine entscheidende Verbesserung sowohl für die körperliche Belastung des Patienten, als auch für den klinischen Arbeitsablauf und die notwendigen Kosten.
Digitales RöntgenDigitaler OP
Das digitale Röntgen.
STARC medical GmbH · Jathostraße 9 · 30916 Isernhagen · Tel. 0511 260962-00 · Fax 0511 260962-90 · [email protected] · www.starc-medical.de
Dr. med. Michael Müller-Autz – STARC PACS-Anwender
„Mehr Zeit für Medizin.“
Digitales Röntgen & Digitaler OP
15
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Quality Management
15
In 2005, already before moving into our new buildings, the ARCUS Clinics imple-mented a comprehensive quality management system in which all employees were gradually included.
Thanks to the great acceptance and the dedication of our staff we were able to form working groups which from then on continuously have been analyzing, adapting and optimizing our internal working procedures and structures.
On this basis we decided to choose CTQ (Cooperation for Transparency and Quality in the Healthcare Sector) as quality management system.
The aim of this system is to motivate directors and employees of the respective faci-lity to implement an internal quality management system with patient orientation and continuously improve it on a self-managing basis (source: http://www.ktq.de/..).
The first certification was successfully completed in November 2006 by the company NIS Zert. Recertification was passed in 2009.
Responsible for quality management are:
Quality Manager: Quality Representative:Sigrun Goos Dr. med. Wolfgang MiehlkeHead of Nursing Services Leading Physician ARCUS [email protected] [email protected]
Qualitätsphilosophie & QualitätspolitikThe ARCUS Clinics management has committed to integrate quality management in any operating structure. Orientation towards the patient is the focus of our activities and patient satisfaction is our continuous aim.
Our employees are the main driving force for the success of our clinic.
Therefore employee oriented management, a broad offer of further education programs and professional cooperation are being paid special attention.
In all areas and professional groups quality is a major aim and all our employees are bound to active contribution. Volunteer working groups help improving the quality. This continuous process of improvement includes all structures, processes and results of our clinic.
Gen
eral Info
rmatio
n

16 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Interesting Facts & Organization
16
Day of Surgery
You are planning to undergo surgery at our clinic. We would like to provide you with some information.
On the day of surgery
• do not eat for 6 hours before the operation
• do not drink for 2 hours before the operation (exception: some mineral water or normal water in combination with medication, see chapter „Anaesthesia“ from page 18).
• do not chew gums or suck on sweets
• do not smoke
• do not use make-up or cream on your face
Furter information regarding anaesthesia please find in chapter “Anaesthesia” from page 18.
Appointment and length of stay:
Please note that the time of your appointment and the actual start of the opera-tion may vary; amongst other things because of the time needed for preparation procedures.
This does also apply for the time needed in the recovery room before you are moved to your room or can leave the hospital (if treated out-patiently). Length of your stay depends on many different factors and therefore cannot be definitely planned. It is only an estimated time slot.
Leaving the Recovery Room:
• the most important criteria is the physical condition of the patient. Whether being in the condition to leave the hospital is exclusively subject to the decision of the anesthesiologist and surgeon
• also important is the completeness of the medical documents needed for further treatment

17
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Interesting Facts & Organization
17
Average Recovery Time after Surgery:
• 2 hours for minor surgeries
• at least 4 hours for larger surgeries, for major surgeries also over night if need be
We hope you understand that there might be longer waiting times. Please apologize for any inconvenience.
Accompanying Person:
• your accompanying person can leave the house in the meantime. Please leave a contact phone number with the recovery room staff and you will be informed as soon as the patient is able to leave the hospital
• out of hygienic reasons, access to the recovery room is not allowed (special ex-ceptions: e.g. operations of children)
• to facilitate transport of the patient to the car, a wheel chair is at your disposable. Please leave it in front of the recovery room afterwards.
Pharmacy:
Please note that the pharmacy is only open until 7.00 pm. You should hand in the prescription for the thrombosis prophylaxis in time.
For out-patient operations:
You will get the first anti-thrombosis injection before leaving the recovery room out of our stock. Thus it is important that you take one anti-thrombosis injection out of the package you received and leave it with the operation theatre staff at the reception desk.
Please do not underestimate the importance of a consequently carried out thrombosis prophylaxis. Even young patients are in the potential risk of thrombosis.
Gen
eral Info
rmatio
n

18 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Anesthesia
18
General Information
There are different anesthetic procedures possible to stop the feeling of pain du-ring surgery. Under general anesthesia you are asleep during the procedure; under regional anesthesia, only a particular part of the body becomes anesthetized.
Sometimes the best solution is a combination of both methods, e.g. for hip-, and knee replacement surgery, or cruciate ligament replacement and shoulder operations.
By using “pain catheters” excellent pain therapy can even be ensured in the days following the operation.
All operating theatres of the ARCUS Clinics are equipped with state-of-the-art an-esthesia apparatuses and monitoring units.
Our anesthesiological team will care for your safety and well-being during the whole surgery. We ensure a pain free procedure, seamless monitoring of your vital functions such as circulation and respiration, and thus are anytime able to react to any changes and take the appropriate measures.
What should be considered before anesthesia?
You will receive individual advice regarding the appropriate and necessary anest-hetic procedure. Please consider that you can contribute largely to the success of anesthesia. Therefore, the following introductions should be strictly observed:
• do not eat for 6 hours before the operation
• do not drink for 2 hours before the operation (exception: some mineral water or normal water in combination with medication)
• do not chew gums or suck on sweets
• do not smoke
• do not use make-up or cream on your face
• please inform the anesthesiologist about all medication you take regularly at home. He will decide which medication can be taken on the day of surgery. It also may be necessary to stop taking particular medicines some days before sur-gery (2-10 days). This does apply in particular for medicines with anticoagulant activity (e.g. Marcumar), acetylsalicylic-acid-containing drugs (e.g. Aspirin, ASS), clopidogrel (e.g. Plavix, Iscover) as well as metformin-containing substances for treatment of Diabetes mellitus.

19
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Anesthesia
19
An
esthesia
Preanesthetic PreparationBefore going under anesthesia, an infusion cannula is placed into your arm vein to give you a mild sedative. Small electrodes are affixed to your chest for later cardiac monitoring. Then you are moved to the preparation room. Here, we start as pre-paration of the anesthesia with seamless monitoring of your cardiac activity (ECG) and continuous measurement of the oxygen level in your blood (via finger sensor). Your blood pressure is checked automatically.
General Anesthesia
To induce general anesthesia, well-tolerated narcotics and analgesics are injected into your vein through the previously placed permanent venous cannula, and du-ring anesthesia permanently given into the blood with a syringe pump. As soon as you are asleep a breathing aid in form of a laryngeal mask is inserted into your mouth. Ventilation via laryngeal mask is a simple and gentle procedure without any negative effect on the vocal cord functions. If the operation requires the patient to be positioned in prone- or lateral position, easing ventilation is generally reached with endotracheal intubation with medicinal muscle-relaxation i.e. by means of a laryngoscope and under visual control, a tube is inserted past the vocal cords directly into the trachea. Of course we are monitoring you the whole time with the utmost care. While you are under anesthesia, your heart- and circulation- as well as your breathing parameters are recorded with a modern automatic monitoring system. This enables us to immediately react on anything abnormal. The ideal depth of an-esthesia is investigated by recording your brain activities. The length of anesthesia is adjusted precisely to the duration of the operation. This means you will wake up immediately after the end of the operation.
Aftercare will then be carried out in the ward station, where you can drink something shortly after the operation and see your family.
20 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Anesthesia
20
Regional Anesthesia
Plexus Anesthesia
For operations of shoulder, elbow and hand, a possible anesthetic procedure is plexus anesthesia.
Here, sensivity to pain in your arm or shoulder is stopped temporarily for several hours by anesthetizing the nerve plexus supplying your shoulder and arm with a local anesthetic. In this time it is “normal” that you are not able to move your arm.
Additionally you are given a “mild” general anesthesia to ensure your well-being and comfort during surgery.
Spinal Anesthesia
Pain free operations of the lower stomach area below the belly button are also enabled by spinal anesthesia.
For this local anesthesia of the spinal marrow a very thin cannula is used to inject the anesthetic between the 3rd and the 4th spinous process of the lumbar vertebrae (far away from the spinal cord) into the so-called “liquor area”.
You can make it much easier for us to find the spinal channel by arching your back during the puncture i.e. bend forwards and press your chin to your chest.
After only a short time you will feel a sensation of warmth and an increasing heavi-ness of your legs. Before starting the operation, sufficient spread of the anesthesia is checked. Depending on the type of local anesthetic used, it may last for up to 6 hours. Sometimes, anesthetizing the bladder nerves may cause temporary urinary retention. In rare cases, especially younger patients may develop headaches after spinal anesthesia.
Peridural Anesthesia
Peridural anesthesia (PDA) is also regarded as one of the procedures which are close to the spinal cord. Compared with spinal anesthesia however, the hard outer membrane surrounding the spinal cord and the nerves branching from it are not punctured. This means that more local anesthetic has to be injected than with spi-nal anesthesia, and that the effect comes slightly delayed. Basically, a PDA could be used as sole anesthetic agent for surgical procedures of the lower part of the body; however, because of the delayed effect it is rather used as additional method for postoperative pain therapy with major surgeries. The thin catheter placed into the peridural space for this procedure can be used for continuous pain therapy during the first days after surgery.
Whether one of these techniques is appropriate in your case should be discussed with your anesthesiologist.
Fig. 1:Plexus Anesthesia
Fig. 2:Spinal Anesthesia
Fig. 3:Spinal Anesthesia

21
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Anesthesia
21
An
esthesia
Combination of General- and Regional Anesthesia
As already mentioned before, it may be useful for many operations to combine both types of anesthesia.
General anesthesia saves you having to consciously witness the operation and en-sures safe artificial ventilation.
Regional anesthesia stops the pain during and after surgery. By continuously giving local anesthetics you will need considerably less strong analgesics, so that there are fewer side effects such as nausea, vomiting or tiredness.
In case that a catheter has been inserted, it is also possible to use it several days for in-patient pain therapy.
Leg nerve Block (so-called 3-in-1 blockade / femoral and sciatic catheter)These forms of so-called peripheral regional anesthesia are used especially for cruciate ligament surgery, knee joint replacement as well as complex foot surgery.
Here, normally after indication of the general anesthesia, the femoral nerve in the groin supplying the front parts of the knee joint, knee extensor and hip flexor muscles is identified by means of an electrical nerve stimulation device. A single injection of local anesthetics brings long-lasting pain reduction. Insertion of a thin catheter near the nerve enables further injections in the days following the operation, so that first physiotherapeutic treatment can be carried out largely without pain. If knee joint replacement shall be done by means of a (partial-) prosthesis, a second catheter is being placed near the sciatic nerve which mainly supplies the posterior thigh area and the lower leg.
Therefore it is quite understandable that even after major surgery you will feel no or only slight pain when waking up from the general anesthetic.
For arm- and shoulder operations there are analogue procedures.
Peripheral Nerve Blocks
For operations on hands or feet, additional very effective pain therapy can also be achieved by nerve blocks which are carried out peripherally, that means further away from the main nerve trunk. This includes the hand- and the foot block.
The advantage is only small impairment on muscle activity of the affected limbs, a reduced demand for anesthetics and long postoperative pain reduction.
22 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Meniscus
22
General Information
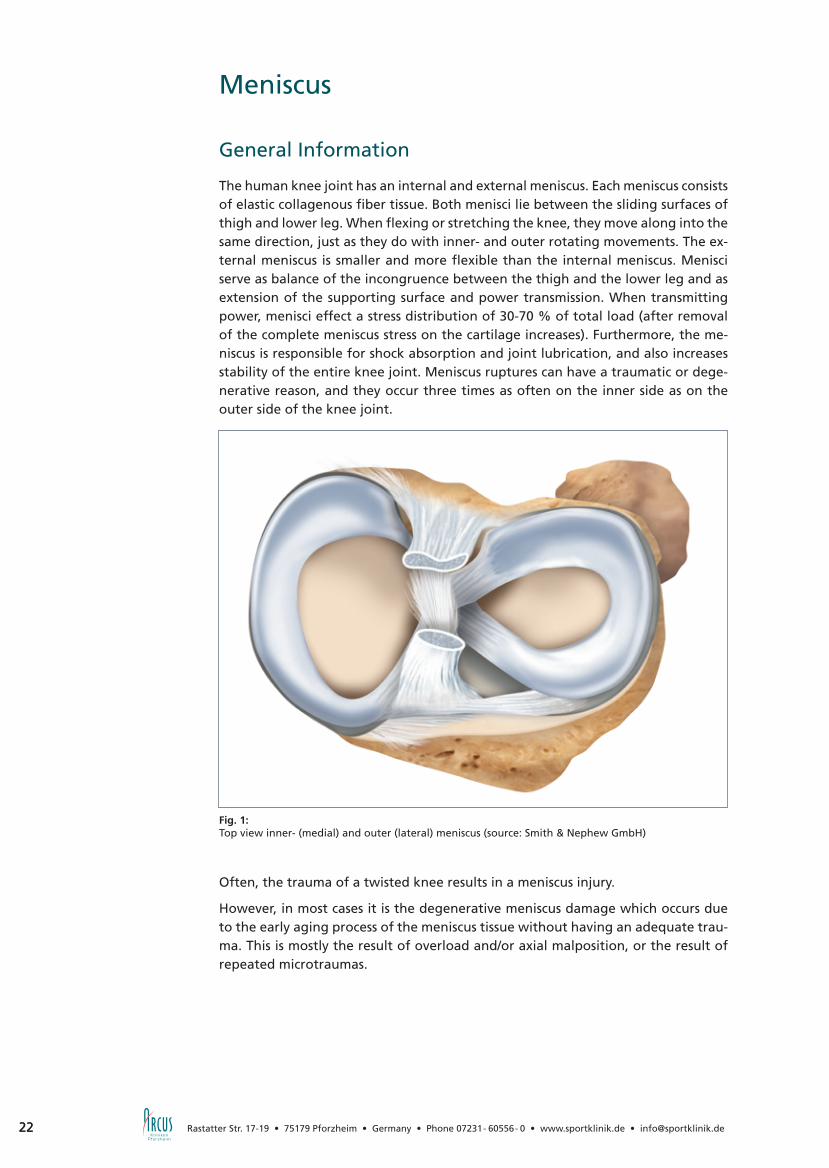
The human knee joint has an internal and external meniscus. Each meniscus consists of elastic collagenous fiber tissue. Both menisci lie between the sliding surfaces of thigh and lower leg. When flexing or stretching the knee, they move along into the same direction, just as they do with inner- and outer rotating movements. The ex-ternal meniscus is smaller and more flexible than the internal meniscus. Menisci serve as balance of the incongruence between the thigh and the lower leg and as extension of the supporting surface and power transmission. When transmitting power, menisci effect a stress distribution of 30-70 % of total load (after removal of the complete meniscus stress on the cartilage increases). Furthermore, the me-niscus is responsible for shock absorption and joint lubrication, and also increases stability of the entire knee joint. Meniscus ruptures can have a traumatic or dege-nerative reason, and they occur three times as often on the inner side as on the outer side of the knee joint.
Often, the trauma of a twisted knee results in a meniscus injury.
However, in most cases it is the degenerative meniscus damage which occurs due to the early aging process of the meniscus tissue without having an adequate trau-ma. This is mostly the result of overload and/or axial malposition, or the result of repeated microtraumas.
Fig. 1:Top view inner- (medial) and outer (lateral) meniscus (source: Smith & Nephew GmbH)

23
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 23
Kn
ee
Meniscus
Medical Conditions
The most common symptoms of meniscus damages are pain in the outer- or inner side of the knee joint, especially under stress and specific rotational movements. A “block” in the joint i.e. temporary inability to flex or stretch the knee is a specific indication for a basket handle- or lap tear. Another indication can be swelling or hyperthermia of the knee joint due to the acute irritation.
TherapyTherapy of meniscus damages can, depending on the degree of severity, be carried out conservatively or surgically. When having a stable meniscus rupture which is relatively free of symptoms and stands physical stresses of everyday life, treatment can be made with combined medical-physical therapy.
Operative therapy is made with a minimally invasive and arthroscopic technique. Because of known long-term consequences, therapists always try to retain as much meniscus tissue as possible with young patients. When having a basket handle or lap treat of the meniscus, in some cases even stitching up the rupture is enough. When these ruptures lie within the central area of the meniscus which is well supplied with blood, there are good chances of recovery. The chance of this kind of therapy being successful has to be decided by the experienced surgeon during surgery.
Fig. 2:Complex rupture after partial meniscectomy
Fig. 3:Complex rupture without any suture option
Fig. 4:Bucket handle tear
Fig. 5:Meniscus suture

24 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Meniscus
24
Meniscus Suture
In our ARCUS Clinics different suturing techniques are used, depending on the need. All of them are well-proven, and show few complications and good chances of re-covery. In order to accelerate wound healing of the torn part of the meniscus and induce ingrowth of blood vessels, fissures are previously prepared by “needling” and “rasping” them with microsurgical instruments. When having a small fissure only or a cruciate ligament rupture at the same time, this often is completely sufficient and is seen as indirect suture technique. When having an isolated meniscus injury or a bigger fissure, however, a direct meniscus suture is necessary and carried out by stitching up the fissure.
Partical Meniscectomy If it turns out that stitching up the meniscus is not possible, partial meniscectomy is being carried out. Here, as much as necessary but as little meniscal tissue as possible is being removed to keep the remaining meniscus stable and functional. Due to this partial removal of the meniscus the supporting surface becomes smaller, but (of course depending on the amount of tissue removed) this normally has no negative effect on joint functions.
Aftercare
After surgery, you are not allowed to drive yourself. In most cases we prescribe an anti-inflammatory medication which has to be taken regularly. Furthermore, prophylaxis of thrombosis and embolism by an abdominal injection is essential as long as walking on crutches. A drainage positioned into the knee joint normally is removed after one or two days, suture material after 10-12 days. This process is being carried out by the referring specialist or family doctor.
Having had a meniscus suture, the knee should not be bent under stress for more than 90 degrees within the first 12 weeks (do not squat!). During the first 2 weeks, the only pressure the knee shall be load with is sole contact. The 3rd and 4th week, load can amount to 20 kg and afterwards the patient can start with moderate muscle training. In most cases, start of intensive sporting activities is possible after 3-4 months.
After partial meniscectomy it is not allowed to put full weight on the leg for about 5-7 days. Moreover, as long as walking on crutches, adequate prophylaxis of throm-bosis and embolism is necessary.
25
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 25
Kn
ee
Meniscus
Meniscus Replacement
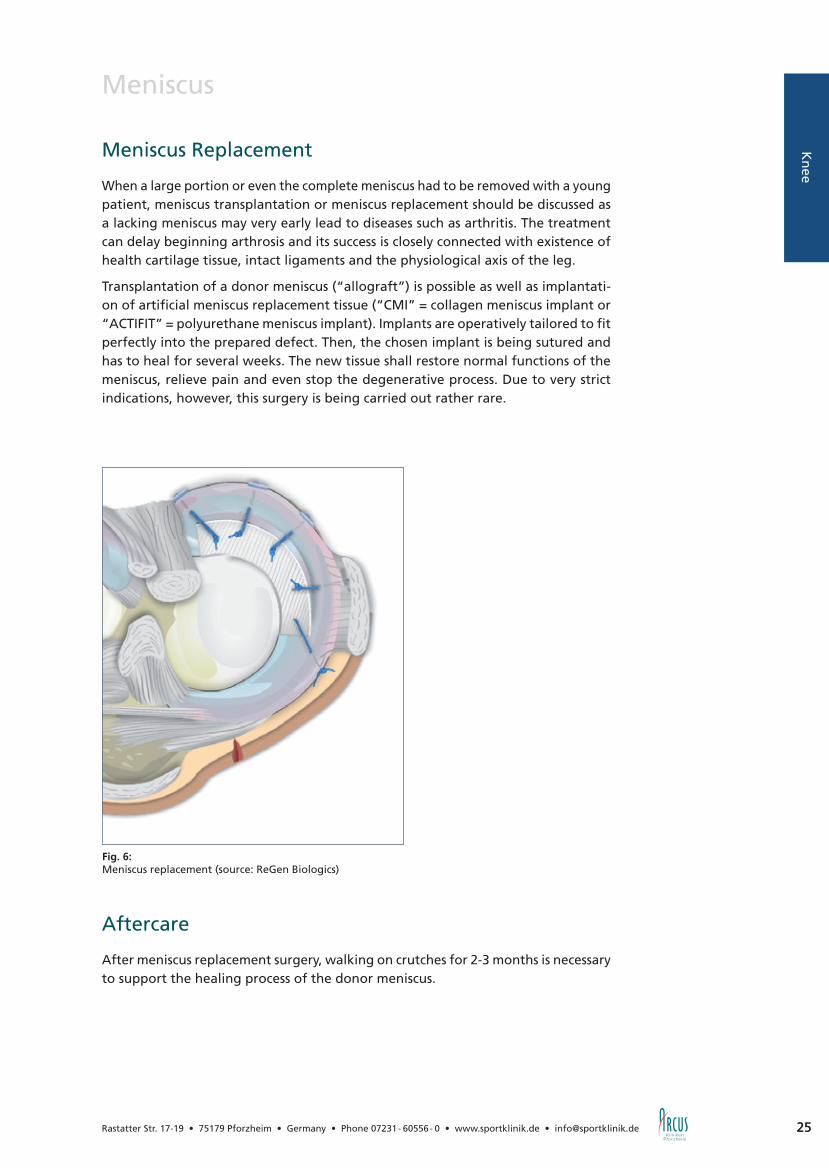
When a large portion or even the complete meniscus had to be removed with a young patient, meniscus transplantation or meniscus replacement should be discussed as a lacking meniscus may very early lead to diseases such as arthritis. The treatment can delay beginning arthrosis and its success is closely connected with existence of health cartilage tissue, intact ligaments and the physiological axis of the leg.
Transplantation of a donor meniscus (“allograft”) is possible as well as implantati-on of artificial meniscus replacement tissue (“CMI” = collagen meniscus implant or “ACTIFIT” = polyurethane meniscus implant). Implants are operatively tailored to fit perfectly into the prepared defect. Then, the chosen implant is being sutured and has to heal for several weeks. The new tissue shall restore normal functions of the meniscus, relieve pain and even stop the degenerative process. Due to very strict indications, however, this surgery is being carried out rather rare.
Aftercare
After meniscus replacement surgery, walking on crutches for 2-3 months is necessary to support the healing process of the donor meniscus.
Fig. 6:Meniscus replacement (source: ReGen Biologics)

26 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Anterior Cruciate Ligament (ACL)
26
General Information
Cruciate ligament injuries are often the result of acute accident- or sports injuries. When having injured the cruciate ligament, the knee joint swells up due to the he-matoma. More symptoms are painful limitation of knee movability and, depending on the severity of injury, the feeling of instability on the affected leg. In this acute condition, diagnosis may be very difficult as pain, swelling and tense muscles hinder medical examination. A positive result of the pivot-shift test is seen as reliable sign for an anterior cruciate ligament rupture; a positive Lachman provides the best likelihood ratio.
Besides the orthopedic examination, magnetic resonance imaging (MRI) is recom-mendable with new cruciate ligament injuries as a high percentage of patients also have concomitant injuries such as meniscus-, medial collateral ligament-, and cartilage damages. With the magnetic resonance imaging the entire extent of the injury can be detected. Therefore, MRI has special relevance with regard to surgery planning as well as for allocation of concomitant injuries to be operated (e.g. menisci, lateral ligaments and/or the dorsolateral capsule edge with rupture of the Popliteus tendon).
Difficulties with Cruciate Ligament Ruptures
Our cruciate ligaments form the central stabilizing column of the knee joint
(fig. 1). Their principle purpose is to prevent the knee joint against abrupt stopping- and accelerating movements as well as rotational movements. Injuries of cruciate ligaments occur in more than 90 % of all cases to the anterior cruciate ligament (ACL). The cruciate ligament rupture causes serious impact on natural movements of the joints. Although with muscular and trained athletes a cruciate ligament rupture
Fig. 1:Knee joint with cruciate ligaments and menisci (source: Smith & Nephew GmbH)
Femoral condyle
posterior cruciate ligament
anterior cruciate ligament
inner (medial) meniscus
Fibula
outer (lateral) meniscus
Tibia (shinbone)

27
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 27
Kn
ee
Anterior Cruciate Ligament (ACL)
can be compensated in the beginning with conservative therapy, damage of further structures and with this a considerably higher risk of arthrosis has to be expected.
After having had a cruciate ligament rupture, most patients focus on regaining their condition first. Need for surgery depends on activity, symptoms of instability and age, and especially the athletic patient benefits here from prompt operative treatment. Conservative treatment, however, is also completely justified with low instability symptoms and low physical activity. With cruciate ligament injuries in childhood and adolescence, operative reconstruction by the use of appropriate techniques should be considered to prevent serious consequential injuries such as damages of secondary joint cartilages or menisci. We have just published comprehensive experiences and numerous studies regarding this issue.
Current Surgical Techniques
Thanks to the enormous development of arthroscopic surgical techniques, treatment options for cruciate ligament replacements have improved considerably over recent years. Shorter operation times and a reduced surgical trauma, less pain and better cosmetic results speak for today’s minimally invasive operation methods. Correct surgical treatment, however, needs maximum experience (fig. 2+3) and therefore should be carried out in specialized centers. In the ARCUS Clinics in Pforzheim more than 1200 arthroscopic cruciate ligament surgeries are carried out every year. Ar-throscopic cruciate ligament replacement using autologous tendon transplants has reached standard level by now. Used are hamstring tendon transplants (semiten-dinosus- and gracilis tendon) in triple- and quadruple binding technique as well as patellar tendon strips, quadriceps tendons and after multiple ruptures also donor grafts. Common characteristics of all these transplants are their tear resistance and flexibility which are similar to the anterior cruciate ligament. But they differ regar-ding the removal technique and their anchoring possibilities.
Fig. 2:Arthroscopic image of a fresh ACL-rupture
Fig. 3:Cruciate ligament reconstruction of semitendinosus tendon graft
28 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Anterior Cruciate Ligament (ACL)
28
Hamstring Grafts (hamstring tendons: semitendinosus- and gracilis tendon)
Through a small incision at the inner shinbone head, the semitendinosus- and gra-cilis tendon are being removed and then doubled to create a quadruple-transplant (fig.4). Alternatively, when having a sufficiently long semitendinosus tendon, there is also the possibility to remove the semitendinosus tendon only and tie it together to a triple- respectively quadruple bundle.
Advantages of the usage of hamstring tendons are fewer problems with removal, less pain, and cosmetically more favorable scars. Another essential advantage of this method is the hamstring graft gaining almost the natural elasticity of a cruciate ligament during the healing process. Relevant dysfunctions due to the removal of the hamstring do not occur.
Partellar Tendon (tendon below knee cap)
As cruciate ligament replacement, the middle third of the tendon is being removed as “bone-tendon-bone” graft (fig. 5). Advantage of this method is stable fixation and fast bone ingrowth of the transplant.
Disadvantageous however is pain which may occur at the donor site and a possible reduction of muscle power of the thigh extensor muscle. Statistics show that the so-called “anterior knee pain” occurs more often after having had an anterior cruciate ligament reconstruction with patellar tendon than with hamstring graft.
„Double-Bundle“ Reconstruction
Some teams favor currently a new procedure using hamstring tendons in double-bundle constructions. With this technique, replacement of the ACL is made accor-ding to its anatomic structure with a doubled transplant string of anteromedial and posterolateral fiber bundles (fig. 6). The higher biomechanical efficiency gained by this double-bundle reconstruction technique however has so far only been proven by experimental simulations. Furthermore, it needs more complex surgery- and anchoring techniques which long-term efficiency regarding optimized knee stabili-zation has not been shown yet. Within the scope of controlled studies, this method is also being used by us.
Quadriceps Tendon (tendon of thigh extensor)
The quadriceps tendon graft with small patellar bone block is mainly used in revision surgery (re-rupture of cruciate ligament). Although it shows biomechanical charac-teristics comparable to the natural cruciate ligament, removal of the transplant is very complex and time-consuming, and therefore did not gain general acceptance as first line therapy. Advantage of this method is the possibility of implant-free press-fit anchoring of the quadriceps tendon graft into the thigh bone, whereby biologically optimal healing and simplified surgery in case of revision treatment is ensured. Disadvantages are the demanding surgical procedure for removal of the tendon and weakening of the thigh extension functions.
Fig. 4:Quadrupled harmstring tendon graft reinforced by Endobuttons® or Retrobuttons®.(source: Arthrex GmbH)
Fig. 5:Patellar tendon graft as ACL/PCL reconstruction (source: Arthrex GmbH)
Fig. 6:Double-bundle ACL reconstruction (schematic image)

29
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 29
Kn
ee
Anterior Cruciate Ligament (ACL)
Donor Tendons
Donor tendons (allografts) are mainly used in America. Advantage of this method is the fact that removal of suitable reconstruction material is no longer required. Disadvantageous however are possible immune responses and the higher failure rate. Usage of donor tendons is being considered as alternative treatment especially with secondary- or third operations when there is lack of the patient’s own trans-plant possibilities. Since 1993, the ARCUS Clinics are regarded the most experienced specialized surgery unit in Germany using donor tendons for cruciate ligament reconstruction.
Fixation of Cruciate Ligament Grafts
Common aim of all reconstruction techniques is primary stable graft anchorage. For this purpose, there are many different fixation materials such as metallic or bioabsorbable interference screws, staples, pins or fixation buttons available (fig. 7, 8a, 8b). For all systems used at present, an initial retention force which meets post-operative stabilization demands has been certified. In the end, however, anchorage of the implant until complete healing remains the real weak point of cruciate ligament plastics.
Time of Cruciate Ligament Reconstruction
When having a new rupture, treatment in the sense of first line therapy can be done within the first 24 to 48 hours. This option is possible for example when treating an osseous rupture of the cruciate ligament or other concomitant injuries that need immediate medical care (e.g. meniscus ruptures that can be stitched up or complex knee instabilities with rupture of medial- or lateral collateral ligament). In normal cases, surgery is planned after 4-6 weeks when the inflammation has subsided. During this inflamed phase, operative treatment is not recommended due to the proven increased complication rate in the sense of post-operative movement disor-
Fig. 7: Fixation of ACL replacement: Transfix® and bioabsorbable screw (source: Arthrex GmbH)
Fig. 8a: Fixation of ACL replacement: Endobutton® or Retrobutton® (source: Arthrex GmbH)
Fig. 8b: Fixation material: bioabsorbable screw and Endobutton® (source: Smith & Nephew GmbH)

30 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Anterior Cruciate Ligament (ACL)
30
ders. Reduction of this “6-week-period” is possible and supportable when the joint becomes irritation-free before.
Until the date selected for surgery, the joint is being treated with functional con-servative methods, where the focus lies on how to reduce the swelling and regain functional mobility. Furthermore, preoperative usage of stabilizing knee orthoses is indicated for strong instability symptoms and concomitant lesions of the medial collateral ligament.
Aftercare
Rehabilitation after cruciate ligament reconstruction surgery is an important compo-nent of our therapy concept. On the one hand, treatment concentrates on regaining the full range of physiological mobility, full muscular control and coordination, and returning to full activity. On the other hand, current methods of Aftercare are adapted to scientifically proven phases of healing. At present, the accelerated rehabilitation program propagated in the 90ies has given way to adapted and more restrictive postoperative therapy planning which considers individual tissue reactions and the healing process. Today, postoperative care with knee orthoses stabilizing the knee joint is considered standard. With optimal rehabilitation, stable reconstruction of knee joint function and –stability can be expected after 6-9 months.
ARCUS rehabilitation program for cruciate ligament reconstruction:
Stationary phase (2-3 days):Ice-pack and lymph drainage. Start with physiotherapy in the pain free area as well as “walking school” on elbow crutches. Further measures are muscle stimulation, lymph drainage and thrombosis prophylaxis. Removal of redon-drainage the 2nd day after surgery.
Fig. 9: Donjoy® knee brace (source: Ormed.DJO)
31
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 31
Kn
ee
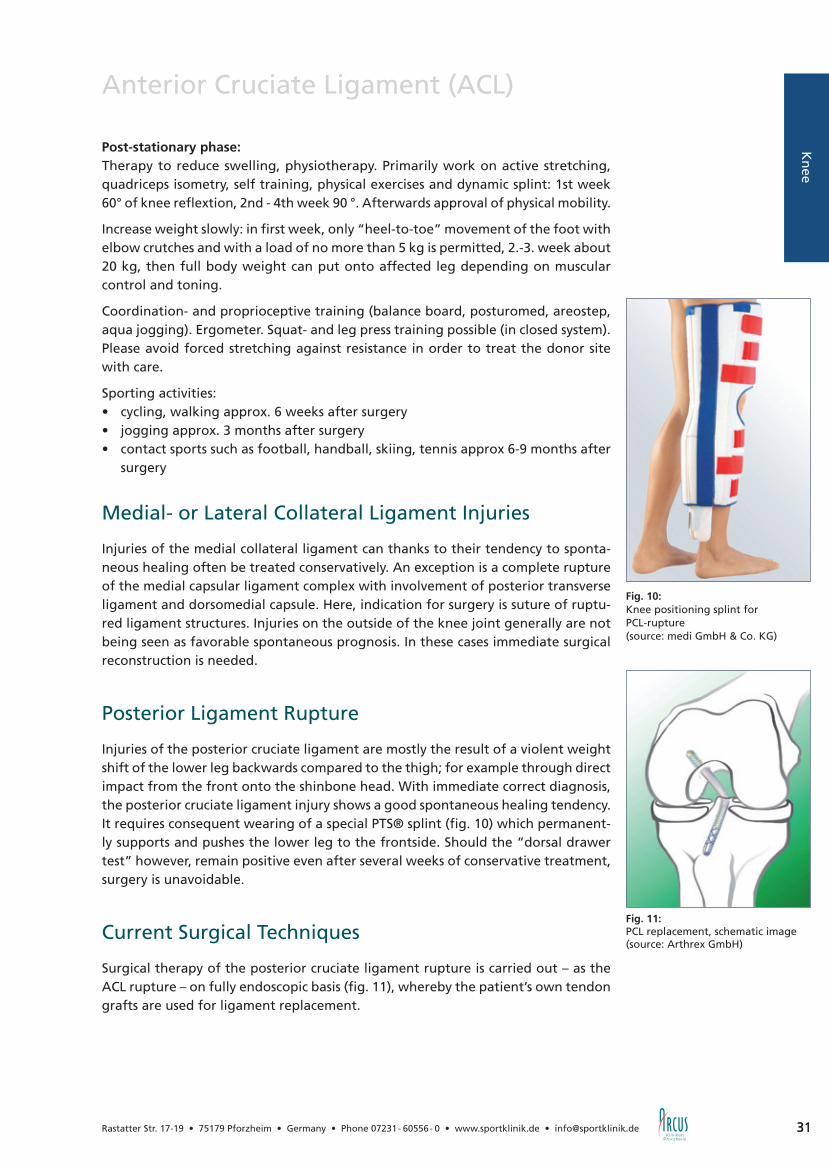
Fig. 10: Knee positioning splint for PCL-rupture (source: medi GmbH & Co. KG)
Anterior Cruciate Ligament (ACL)
Post-stationary phase: Therapy to reduce swelling, physiotherapy. Primarily work on active stretching, quadriceps isometry, self training, physical exercises and dynamic splint: 1st week 60° of knee reflextion, 2nd - 4th week 90 °. Afterwards approval of physical mobility.
Increase weight slowly: in first week, only “heel-to-toe” movement of the foot with elbow crutches and with a load of no more than 5 kg is permitted, 2.-3. week about 20 kg, then full body weight can put onto affected leg depending on muscular control and toning.
Coordination- and proprioceptive training (balance board, posturomed, areostep, aqua jogging). Ergometer. Squat- and leg press training possible (in closed system). Please avoid forced stretching against resistance in order to treat the donor site with care.
Sporting activities:• cycling, walking approx. 6 weeks after surgery• jogging approx. 3 months after surgery• contact sports such as football, handball, skiing, tennis approx 6-9 months after
surgery
Medial- or Lateral Collateral Ligament Injuries
Injuries of the medial collateral ligament can thanks to their tendency to sponta-neous healing often be treated conservatively. An exception is a complete rupture of the medial capsular ligament complex with involvement of posterior transverse ligament and dorsomedial capsule. Here, indication for surgery is suture of ruptu-red ligament structures. Injuries on the outside of the knee joint generally are not being seen as favorable spontaneous prognosis. In these cases immediate surgical reconstruction is needed.
Posterior Ligament Rupture
Injuries of the posterior cruciate ligament are mostly the result of a violent weight shift of the lower leg backwards compared to the thigh; for example through direct impact from the front onto the shinbone head. With immediate correct diagnosis, the posterior cruciate ligament injury shows a good spontaneous healing tendency. It requires consequent wearing of a special PTS® splint (fig. 10) which permanent-ly supports and pushes the lower leg to the frontside. Should the “dorsal drawer test” however, remain positive even after several weeks of conservative treatment, surgery is unavoidable.
Current Surgical Techniques
Surgical therapy of the posterior cruciate ligament rupture is carried out – as the ACL rupture – on fully endoscopic basis (fig. 11), whereby the patient’s own tendon grafts are used for ligament replacement.
Fig. 11:PCL replacement, schematic image (source: Arthrex GmbH)

3232
Ärzte-Serviceline 0180 2 95 95 95 (6 Cent pro Gespräch aus dem deutschen Festnetz. Aus Mobilfunknetzen sind abweichende Preise möglich.)
Die effizienteste Form der Quadrizeps-Stimulation*
* Dr. H. H. Pässler, Sven Feil (M. A.): Die Effektivität des kneehab™.
ATOS-Klinikzentrum Heidelberg 2006
Mit der patentierten multipath™ Technologie
Die Rehabilitation nach Knie- und Hüftoperationen ist oft
mühsam und langwierig. Mit Kneehab XP™ kommen Ihre
Patienten schneller wieder auf die Beine. Kneehab XP™
verfügt über die einzigartige, patentierte multipath™
Technologie, die deutlich mehr Muskelfasern stimuliert
und stärkere Muskelkontraktionen auslöst. Das ist gut für
den Quadrizeps und gut für Ihre Patien ten – denn es be-
schleunigt die Heilung um bis zu sieben Tage*.
www.neurotechgroup.com
AZ_KneehabXP_185x280.indd 1 07.01.2009 12:48:50 Uhr
33
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Knee-Cap (Patella)
33
Kn
ee
General Information
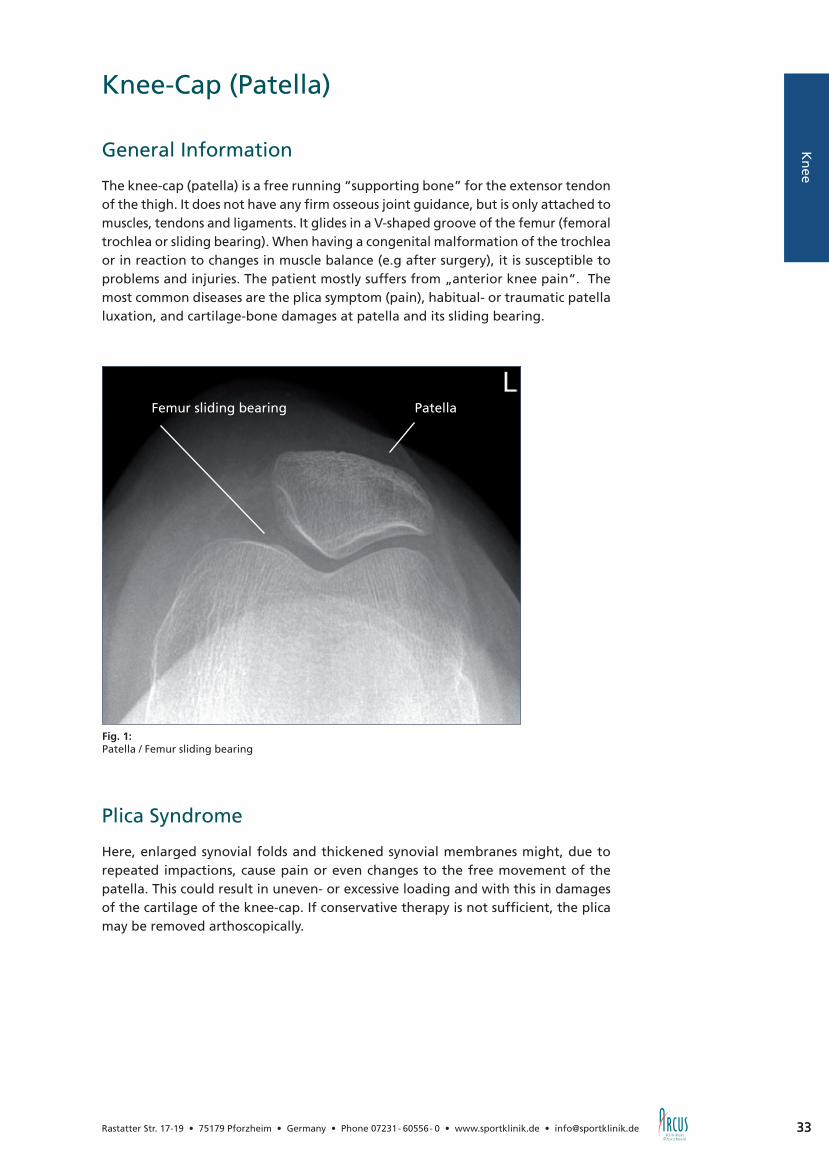
The knee-cap (patella) is a free running “supporting bone” for the extensor tendon of the thigh. It does not have any firm osseous joint guidance, but is only attached to muscles, tendons and ligaments. It glides in a V-shaped groove of the femur (femoral trochlea or sliding bearing). When having a congenital malformation of the trochlea or in reaction to changes in muscle balance (e.g after surgery), it is susceptible to problems and injuries. The patient mostly suffers from „anterior knee pain“. The most common diseases are the plica symptom (pain), habitual- or traumatic patella luxation, and cartilage-bone damages at patella and its sliding bearing.
Plica Syndrome
Here, enlarged synovial folds and thickened synovial membranes might, due to repeated impactions, cause pain or even changes to the free movement of the patella. This could result in uneven- or excessive loading and with this in damages of the cartilage of the knee-cap. If conservative therapy is not sufficient, the plica may be removed arthoscopically.
Fig. 1:Patella / Femur sliding bearing
PatellaFemur sliding bearing

34 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Knee-Cap (Patella)
Habitual- or Traumatic Patella Luxation
A distinction is made between congenital disorder and acute injuries when having had an accident. The habitual patella (sub) luxation occurs congenitally and insta-bility of knee-cap is due to shallow tracks or weak ligaments and muscles to hold the kee-cap and knee joint capsule. With the traumatic patella luxation instability is usually the result of an accident (luxation towards the outside).
Conservative Therapy
Depending on severity of the knee deviation, a conservative treatment approach can be carried out first. Exercises shall train the vastus medialis muscle regarding leg extension. Important is cooperation of the patient as treatment can only be successful when exercises are consequently being carried out for at least 3-6 months. Longer periods of immobilization and leg rest, however, should be avoided in any case.
Surgical Treatment of Habitual Patella Luxation
In case that conservative treatment alone is not enough, operative measures have to be considered. Depending on cause and detected damages correcting surgery may be necessary. Lateral release (fig. 2+3) and/or medial tightening (fig. 4) are treatment options. Another option for treatment of cartilage damages of the knee-cap or osseous knee-cap luxation may be to transfer piece of the lower leg bone inwards. Here, the attachment of the patellar ligament at the tibia is detached from the bone, and reattached with screws about 1-2 cm further inside. Should the damage be caused by thigh problems, surgical correction of the hip joint may be necessary. Depending on the case, it makes sense to carry out supplemental cartilage therapies and/or a combination of the treatment methods described above.
Fig. 3:Outer capsule after lateral release
Fig. 4:Inner capsule: medial tightening
Fig. 2:Outer capsule: patella lateralization
Patella
Patella
Femur
capsule cut
knee arthroscopy(right)

35
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Knee-Cap (Patella)
35
Kn
ee
Surgical Treatment of Traumatic Patella Luxation
In some cases, when only the joint capsule has been torn by the traumatic patella luxation and caused a haematoma within the knee, an arthroscopic knee washout can be sufficient to prepare the knee for conservative treatment. Operative methods are needed for cracked cartilages or torn medial patellofemoral ligaments (MPFL). Most often, the cracked-off cartilage-bone fragment can be reattached through a small insicion, using bioabsorbable anchors. A suture of the cartilage capsule can also be treated with this arthroscopic method. Replacement of a torn MPFL is biomechanically necessary for restoring the patella function and carried out with the patient’s own tendon material from the inner side of the thigh. Similar to ACL reconstruction, the method of choice is minimally-invasive surgery.
AftercareDuring aftercare the patient can put full weight onto the straight leg after 2-3 weeks, squatting or climbing stairs is possible after 5-6 weeks. At this time, an intensive muscle training shall be started to strengthen the especially quick weakening vastus medialis muscle.
Spontaneous Cartilage-Bone Lesions (osteochondrosis dissecans)
There are cases where the area around the patella and its sliding bearing is not suf-ficiently supplied with blood and begins to die. At an advanced stage, the cartilage lying above is also destroyed.
Therapy
Initial treatment depends on the stage and is conservative in most cases. Rest, no sporting activities and anti-inflammatory medication may be necessary for pain relief.
If X-ray or MRI examinations show progress of the disease, small holes should be drilled surgically into the center of inflammation to stimulate vascularization and healing. This is called antegrade- or retrograde drilling. In some cases, dead tissue has to be removed before it comes loose and becomes a “joint mouse”. This would cause further cartilage damage to still healthy sections of the joint. Afterwards, the bone lying below is also surgically drilled in order to stimulate vascularization and regeneration of cartilage tissue. In recent years, we have increasingly become able to successfully treat such disorders with bone-cartilage transplants (mosaic plastics, see chapter arthrosis).

36 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Arthrosis
How does a normal joint actually work?
Generally spoken, a joint movably connects the ends of two bones. To avoid these rough bones rubbing against each other directly, these contact surfaces are co-vered with an approx. 3-4 cm thick layer of cartilage (fig. 1). This layer is extremely smooth, reduces friction within the joint (lower than two smoth ice surfaces against each other) and elastically absorbs shocks when walking. These special mechanical characteristics are maintained by complicated biochemical, molecular and electro-physiological connections and require an intact closed surface and a stable collagen fiber network. This complex “composite material” is produced and controlled by cartilage cells (chondrocytes). Disorders can be of mechanical kind (sudden physical force such as the impact experienced in a car accident, high grade sprains, chronic overweight, varus/valgus malalignment, cruciate ligament instabilities, lacking me-nisci) or of biomechanical kind (metabolic diseases, rheumatism, gout, calcification, circulatory disorder). Several facts are here ensured: so does reasonable endurance sport, marathon runners included, not increase danger of arthrosis, whereas the varus/valgus alignment especially in combination with meniscus damage, radical meniscus surgery and/or overweight poses a significant risk of arthritis.
Cartilage damage is divided into four different levels of severity:1. stage: slight superficial fibrillation2. stage: deeper tear and large surface fibrillations3. stage: deeper defect (to the bone) with strong fibrillation, mechanically not
acceptable4. stage: exposed bone
Traumatogenic Cartilage Damages
When twisting one’s knee or incurring a contusion as a result of an accident (skiing, playing football etc.) a piece of cartilage (diameter approx. 1-2 cm) may crack off the complete cartilage layer. Surrounding edges are intact and of normal height, the bone below is unaffected and shows good regenerative ability. This kind of damages responds well to all treatment methods mentioned in the following.
Degenerative Wear
Less positive are prospects for cartilage damages developed during one’s lifetime by monotonous stress alone or in conjunction with varus- or valgus deformity, gout, rheumatism, or damages to menisci or cruciate ligaments. These damages soften the cartilage (1. stage) and later result in fibrillation of the complete layer (2. stage). In stage 2-3, the cartilage layer is only half as thick as normal and extremely frayed and there may occur detached or loose fragments of cartilage.
This stage can no longer be repaired by the body itself without outside help. Specia-lists already talk of severe cartilage damage even though pain may still be bearable for the patient and thus is not perceived as warning signal. Especially this early stage of progressive cartilage degeneration though offers good prospects of successful cartilage surgery. Unfortunately, many patients wait too long.
Fig. 1:Knee joint damaged by arthrosis (source: medi GmbH & Co. KG)
Fig. 2:Schemed image of arthrosis grades of severity(source: medi GmbH & Co. KG)
grade I
grade II
grade III
grade IV

37
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Arthrosis
37
Kn
ee
In the final stage (4. stage) the cartilage tissue is completely destroyed, the „tyre tread“ completely gone. Bone grinds on bone, grooves develop and osseous over-hangs make stretching the leg increasingly difficult. Varus- and valgus deformities increase. Even modern surgical measures for cartilage reconstruction are only limitedly successful in this stage. Real hyaline cartilage cannot regenerate. The only thing an orthopaedic surgeon can do is facilitating growth of replacement- and fiber carti-lage and help improving its quality and strenght, or carry out time-consuming cell culture and transplantations which, however, are still quite limited in their range of application.
Basically it can be said that once cartilage damage has begun, the wearing process will continue with increasing speed, and without early therapeutic intervention, freedom from pain can only be achieved by implanting artificial joint prostheses.
Treatment of Arthrosis
Method of treatment depends on cause and severity of the disease. With instruments for arthroscopic surgery we are not only able to see the cartilage damage and record it for later documentation; we can also very gently treat the damage by means of these micro-instruments at the same time.
Debridement
Frayed edges are removed with a mini cutter and the surface is smoothed. Instable cartilage parts are removed to prevent further fraying.
At the same time meniscus damages are being repaired whereby, in an early stage, suturing the meniscus should be the preferred treatment method. In some cases, it makes sense to remove part of the synovial membrane to reduce risk of contusions within the joint.
Methods of Cartilage Regeneration (stem cell techniques)
They base on “migration” of bone marrow stem cells into damaged cartilage areas where they develop into replacement cartilages.
Thus, having a case of half-thickness cartilage defect with furthermore severe fraying, there is still a possibility to stimulate the body’s own cartilage repair. For the first 3-4 years, this replacement cartilage is relatively rich in cells and does not consist of as many cartilage cells (chondrocytes) which produce synovial fluid. Furthermore, it can not stand as much mechanical load as original hyaline-cartilage and therefore often causes knee irritations and knee pain. However, this replacement cartilage (fibrocartilage) is still better than a completely exposed bone. Just compare this damage for example with a burn injury: the skin is wrinkled, less elastic, sensitive to injury, does not get a tan and is hairless - but it is far better than having a per-manently open wound.
There are clear indications that in most cases (unfortunately not always) replacement cartilage develops into better load-resistant hyaline-cartilage after several years.

38 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Arthrosis
38
“Microfracture Technique” (according to Steadman)
Operative beginnings of surgical refreshing of cartilage date back to the 50’s (Pridie drillings). Here, several holes of about 2 mm are sieve-like drilled into the exposed surface of the bone. With this, small “islands of regeneration” are created, but only in few cases a continuing cartilaginous scar tissue. Nowadays, we prefer the less traumatizing “microfracture technique” according to Steadman which has been developed in the early 90s (fig. 3+4).
The bone surface is pierced with a fine awl to create hairline cracks and tiny holes, resulting in a stronger cartilaginous scar tissue to cover the entire affected area.
Just imagine grass seeds on trodden down and dry soil: without previously breaking up the ground, the seed would have no chance to take root. After sowing the seeds, it is not allowed to walk on the lawn for some time to protect it. The same applies to a joint: piercing the bone loosens the bony surface and enables bone marrow stem cells to seep out and potential blood stem cells to settle. And to protect this sensitive area, it is necessary to walk on crutches at the beginning.
Abrasion Arthroplasty (according to L. L. Johnson)
If parts of the bone are already exposed (4. stage), one treatment possibility is to debride and smooth the remaining bone and wait for improvement. But there is also a chance of helping the body filling bald areas with new cartilage-like scar tissue again – and results can be as good as after treatment with microfracture technique. We just refresh the exposed, extremely hardened surface of the bone with small cutters, as developed by L. Jonson in the early 80’s.
Fig. 3:Grade IV cartilage damage at the knee,treatment with micro fracture
Fig. 4:Cartilage repair 1 year after micro fracture

39
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Arthrosis
39
Kn
ee
Different Methods of Cartilage Transplantation
Cartilage-Bone Transplantation (OATS and mosaic plastics)
Small cartilage-bone cylinder-shaped pieces are removed from knee areas with lo-wer physical load and fit into prepared holes in the defective area. Advantage: this method creates immediately functioning hyaline cartilage for the defective area and healing is very fast thanks to the “press-fitted” bony cylinders. Furthermore, expenses are rather limited. However, this method is technically demanding and requires a high degree of surgical expertise and experience, especially when being carried out arthroscopically.
Thus, although seen as routine surgery on knee joint and ankle, it is still not recom-mendable for shoulder and hip.
Specific demands of ankle surgery: the typical cartilage-bone defect is situated behind the inner ankle, inaccessible from the front. Thus, the inner ankle has to be detached first to be able to press the donor-cylinder extracted from the knee (the ankle joint does not have enough cartilage tissue to create a transplant) into the defect of the talus, and then screwed back in afterwards.
Problems finding donor sites arise in about 10% of all cases when 1-2 donor cylin-ders shall be extracted. Therefore, the amount of donor cylinders is limited. There exist artificial, absorbable plugs with cartilage-like characteristics (Trufit®, fig. 7), which have proven to be very successful in filling up these donor-holes. In some cases, smaller defects (also at ankle joint) can be treated with such absorbable plugs immediately. After 1-2 years these plugs are replaced by the body’s own bone-, cartilage- and connective tissue cells.
Cartilage Cell Cultivation = Autologous Chondrocyte Transplantation ACT
This method caused quite a stir in the media in the mid 1990’s. In a first operation, several cartilage particles are removed from the knee joint, propagated in a complex cell culture and finally implanted in the defective area in a second surgical procedure. The new cells have to grow and propagate further cells for a new cartilaginous struc-ture – a very complex process that requires strict adherence to Aftercare guidelines given; that may include walking on crutches for 8-10 weeks. During this time, enough exercise with a continuous passive motion device (4-6 weeks, 4-6 hours each day)
Fig. 5:Mosaic plastics at femoral condyle of knee joint
Fig. 6:Mosaic plastics at knee joint
Fig. 7:Scheme of resorbable Trufit® dowel
40 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Arthrosis
40
as after microfracture treatment is necessary, respectively strongly recommended by us. With this exercise, formation of a good and stable new cartilage surface is essentially supported (see below).
In some cases, after verification of the diagnosis and indication, approval of cost transfer has to be obtained from the health insurance company first before cell removal and transplantation afterwards can be carried out. Thus, bureaucracy so-metimes makes 3 surgical steps necessary.
And costs are high; the cultivation of new cells in a laboratory alone costs 4.500.00 – 8.000.00 Euros – and is covered from public health insurance companies only for part of the patients. Furthermore, operation technique is very demanding and may require a second surgical procedure, let alone the arthroscopically controlled check after 1-2 years.
All these methods can help rebuilding the attacked or worn cartilage layer of the joint. However, this can only be successful if any possible causal disturbance factor has been eliminated:
• Meniscal lesions have to be smoothed or even better sutured. Meniscus trans-plantations are so far not available for wider clinical usage.
• Ligament instabilities have to be eliminated, especially the anterior cruciate ligament (ACL) has to be sufficiently stable.
• Leg axes need to be straight (see chapter varus/valgus malalignment).
• Overweight shall consequently be reduced until a bodymass index of less than 25 is reached. This is done by reducing food intake and starting sporting activities (at the beginning in the water).
Aftercare for joint-preserving Arthrosis Treatment
See chapter varus/valgus malalignment page 46.

41
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Arthrosis
41
Kn
ee
ResultsUntil today, there unfortunately has not been found any general patent remedy for the advanced stage of the degenerative joint disease – except for artificial joint reconstruction which should be delayed as long as possible. With treatment by con-tinuous passive exercise the Canadian R. Salter achieved excellent results already in 1984 (in an animal experiment with a 6 weeks continuous training even in cases of severe joint damage). Of course, on the one hand, a human patient cannot be tied to a motion device for 6 weeks, and on the other hand many diseases heal much faster and better with animals than with humans. However, we think that this af-tercare concept is a revolutionary method for the future.
Our experiences with abrasion arthroplasty for arthrosis treatment – whether with or without continuous passive motion - date back to its beginnings in Germany in 1984. In own tests carried out during aftercare we can, similar to the American studies, achieve good and satisfying results in about 60-70%. Please consider that without any treatment constant worsening of joint functions has to be expected.
Supportive Medication Therapy
Injections with hyaluronic acid have shown to be successful in improving joint lub-rication, and we at the ARCUS Clinisc are very proud to have actively contributet to the launch of hyaluronic acid in Germany in the early 90’s. A step that has proven to be successful in the long term. In extensive studies, hyaluronic acid has mainly been proven positive. Generally, a series of 3 to 5 injections is recommended (at the price of approx. 230 euros each/status 2009). Unfortunately, neither public health insurance companies nor the employers’ liability insurance association are willing to pay for this treatment so far; the patient is yet again self-payer.
In order to support cartilage repair, we recommend an additional long-term therapy with cartilage builders glucosamine and chondroitin (e.g. 3x1 capsule ARTROSTAR ®). This combination of approx. 1500 mg glucosamine and approx. 1200 mg chondroitin sulfate per day is commonly regarded as supportive cartilage therapy. International studies and in the meantime working groups in Germany as well are proving the anti-inflammatory- and cartilage supporting characteristics of these substances which furthermore are free of unpleasant gastrointestinal side effects such as the for cartilage unfavorable NSAR. A capsule of ARTROSTAR ® contains 500 mg gluco-samine HCL and 400 mg chondroitin sulfate. Unfortunately, public health insurance companies do not pay for this treatment. Positive effects of homeopathic medicines such as Zeel® or Ney Arthros® are much less proven and only a few treatments are normally not suitable as therapy approach.

42 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Exercise Therapy
The best thing you can do for your joint is to have plenty of exercise while avoiding overexertion, e.g. by loosing weight, wearing well-padded shoes in the initial phase, avoiding long walks/runs on hard surfaces such as asphalt etc. Train your muscles with slowly increasing endurance sports. Suitable are “soft straightforward sports” such as cycling, walking, Nordic walking and swimming.
New Physiotherapy Options:
• Aqua jogging which enables intensive circulatory- and muscular training without overloading the affected knee.
• Reflective muscle training with the whole body vibrator type Galileo. The patient stands on a plate vibrating with about 40 Hz what is automatically balanced by the muscles. This has already been proven to be an effective training method for muscles and bones. We are currently investigating positive effects on cartilage regeneration after the surgical procedures mentioned above.
Tips for Further Improvement of Treatment Success:
• Stick to the period of no or restricted weight-bearing given by us.
• Move your joint as intensively as possible without overloading it.
• Make use of the advantages of hyaluronic acid injections for the affected joint: start first series 3 weeks after surgery; repeat after 6-12 months.
• Work consequently on weight reduction. Even a few kilograms less add up with 2-3 million steps per year as a knee-, ankle- or hip joint is loaded with the 2 to 5 fold of body weight; depending on height of step.
• Drink enough water (instead of coffee or soft drinks) so that body and cartilage do not become dehydrated and with this brittle and prone to injuries.
• Train your joints according to a varied program:
- In the initial build-up phase, about 2-6 months after surgery soft, we recom-mend guided movements without transmitting the load of body weight such as cycling or water training. Then slowly start with walking / Nordic walking e.g. also combined with special training shoes (MBT-shoes).
- Later you can add a mixture of cross-training, running (at the beginning on hard ground, then cross-country), as well as total body exercise in the gym.
• Accept that not every joint affected by arthrosis can regain its former sporting ability.
• Keep to the follow-up appointments stipulated.
• Make use of our offer for an arthroscopic check about 1 year after surgery.
• Please consider that without any treatment constant worsening of joint func-tions has to be expected.
Arthrosis

43
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 43
Kn
ee
Arthrosis

44 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Ortho-Biologie
44
Modern Therapy Methods in Orthopaedics / Trauma SurgeryTissue Regeneration PrinciplesDifferent types of human tissue need different time periods for regeneration. An injury of the oral mucosa for example heals completely within a few days, muscle injuries need 3-4 weeks, bones usually 6-12 weeks.
It has been known for some time now, that any information needed for the forma-tion of new tissue cells lies in these cells and in-between areas as well as to a large extent within the platelets.
Bone Growth Factors:Research to this topic dates back until far into the 80’s, and since the mid-90’s, con-centrates of such collagenous bone growth factors, gained of animal bone extract, are allowed as preparation and for clinical use. In 1997, the ARCUS Clinics have been one of the first orthopaedic specialist units to officially use these bone growth factors, and since then has been treating hundreds of bone defects that do not normally heal very successfully. Particularly suitable is this material for very problematic bone healing processes with infections (infected pseudo-arthrosis).
Besides such concentrates which provide a huge number of bone growth factors in the perfect mixture ratio quasi as seed capital for bone healing, there are also treatment possibilities with isolated special factors (e.g. BMP7). However, they have to be given in a local overdose what may increase possible unwanted side effects.
Growth Factors of Platelets PRP (Platelet Rich Plasma)In recent years, treatment with the body’s own growth factors - 10 to 60 ml of the patient’s own blood which is specially prepared and centrifuged – has become more and more popular. Here, growth factors within the platelets are enriched and the liquid gained (several milliliters) is given into the areas with low healing tendency (e.g. Achilles tendon- or meniscus suture). And there are also many cases in which artificial bone material is saturated with those factors to fill bone defects. The advantage is improvement of healing free of side effects, especially in cases with unfavorable conditions. Another new treatment method is injecting the patient’s own factors directly into the affected area. When using this method at the Achilles tendon, the patient is with suitable orthotic shoe inlays capable of walking already after 4-5 weeks thanks to good healing acceleration.
Fig. 2:Minimally invasive Achilles tendon suture
Fig. 1: Development of stem cell into bone cell. Besides correct surrounding conditions (type of surrounding tissue, pressure, exercise, rest, chemical composition of surrounding etc.) availability of several different growth factors at the perfect time and in the optimal concentration are necessary.
Fig. 3:Injection of body-own growth fac-tors (PRP)

45
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Ortho-Biologie
45
Kn
ee
Support of Cartilage RepairReal regrowth of original cartilage substance is still a dream. But nevertheless we have learned a lot about cartilage reconstruction (fibrous cartilage) and how it can be improved to become a more stable long-term scar. Besides operative requirements, injection therapy with hyaluronic acid has become an important factor. It does not only reduce friction (with “synovial fluid”) but affected cartilage cells are also pro-vided an immediately functioning basic frame for formation of cartilage as “com-posite material”. Furthermore, hyaluronic acid icreases, and that is very important, the water-binding capacity of the attacked and frayed cartilage. It becomes more elastic and nutrition of cartilage cells is improved by the water flowing in and out with every step. More water molecules in turn increase the piezoelectric effect to which the biological meaning of stimulation of cartilage metabolism is attributed.
There is enough literature available about the positive effects of hyaluronic acid therapy. It is no coincidence that more and more orthopaedists and surgeons re-commend this therapy. They daily experience patients which achieve an improve-ment of their symptoms - in some cases already after the third injection - and that this condition lasts for 6-12 months (after a therapy of only 3-5 injections). That is incredibly much longer than the pure biochemical half-life of molecules within a joint which in most cases is 1-3 days.
Unfortunately, decision-making committees of public insurance companies refer to the few neutral or negative studies (which can be found on every scientifically discussed problem) and the current situation is: self-payer status.
CostsOur surgeons at the ARCUS Clinics are highly qualified specialists which always offer the latest state-of-the-art surgical techniques, as far as they have proven to be successful. To what extent health insurance companies are willing to pay for the respective treatments however, has to be checked in each individual case. Unfor-tunately we cannot give any generally binding statement as to how one or another medical progress will be reflected in cost transfer of public- or private health insu-rance companies in the future.
We care about your health. Therefore we will always offer you the most promising treatment options; regardless of the cost situation. In a personal interview we will see which treatment option suits you and your needs. We will always be at your disposal to inform you about minimally necessary measures, the recommended therapy and an optimal, comprehensive and holistic treatment.
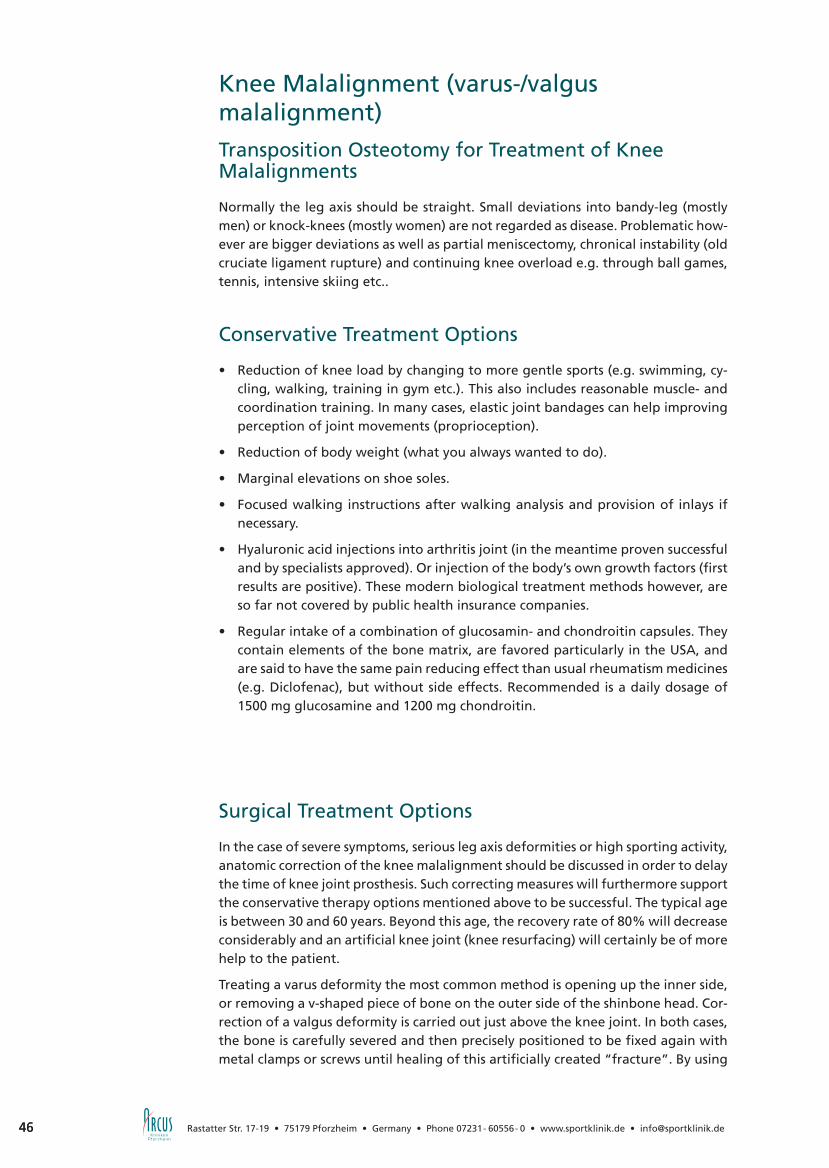
46 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Knee Malalignment (varus-/valgus malalignment)
46
Transposition Osteotomy for Treatment of Knee Malalignments
Normally the leg axis should be straight. Small deviations into bandy-leg (mostly men) or knock-knees (mostly women) are not regarded as disease. Problematic how-ever are bigger deviations as well as partial meniscectomy, chronical instability (old cruciate ligament rupture) and continuing knee overload e.g. through ball games, tennis, intensive skiing etc..
Conservative Treatment Options
• Reduction of knee load by changing to more gentle sports (e.g. swimming, cy-cling, walking, training in gym etc.). This also includes reasonable muscle- and coordination training. In many cases, elastic joint bandages can help improving perception of joint movements (proprioception).
• Reduction of body weight (what you always wanted to do).
• Marginal elevations on shoe soles.
• Focused walking instructions after walking analysis and provision of inlays if necessary.
• Hyaluronic acid injections into arthritis joint (in the meantime proven successful and by specialists approved). Or injection of the body’s own growth factors (first results are positive). These modern biological treatment methods however, are so far not covered by public health insurance companies.
• Regular intake of a combination of glucosamin- and chondroitin capsules. They contain elements of the bone matrix, are favored particularly in the USA, and are said to have the same pain reducing effect than usual rheumatism medicines (e.g. Diclofenac), but without side effects. Recommended is a daily dosage of 1500 mg glucosamine and 1200 mg chondroitin.
Surgical Treatment Options
In the case of severe symptoms, serious leg axis deformities or high sporting activity, anatomic correction of the knee malalignment should be discussed in order to delay the time of knee joint prosthesis. Such correcting measures will furthermore support the conservative therapy options mentioned above to be successful. The typical age is between 30 and 60 years. Beyond this age, the recovery rate of 80% will decrease considerably and an artificial knee joint (knee resurfacing) will certainly be of more help to the patient.
Treating a varus deformity the most common method is opening up the inner side, or removing a v-shaped piece of bone on the outer side of the shinbone head. Cor-rection of a valgus deformity is carried out just above the knee joint. In both cases, the bone is carefully severed and then precisely positioned to be fixed again with metal clamps or screws until healing of this artificially created “fracture”. By using

47
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Knee Malalignment (varus-/valgus malalignment)
47
Kn
ee
so-called stably-angled plates and screws the healing process has considerably been improved in recent years:
• reduced pain
• improved mobility
• possibility of a reliable healing rate.
Such treatments can normally be combined with cartilage regeneration- or cartilage transplantation procedures. All metal parts used are removed after 1 year when carrying out an arthroscopically controlled check. Insufficiently healed cartilage can immediately be treated again.
Even if it seems to be a serious surgical treatment: these correction measures heal faster than cartilage within the knee joint as it needs time for creation of a new cartilage layer, the so-called “bioprosthesis”. By combining all these surgical therapy methods (operative refreshment of arthrosis and cartilage transplantation if necessary, correcting measures for knee deformities, cartilage supportive hyaluronic injections) it is today in fact possible to stimulate regrowth of new stable cartilage tissue.
Aftercare for joint-preserving Arthrosis Treatment:
Depending on severity and extent of the arthrosis, walking on forearm crutches to keep pressure off the affected area might be necessary for up to 10 weeks. During the first 4-6 weeks, only a “heel-to-toe” movement of the foot with a load of not more than 5 kg is permitted; during the following 2-6 weeks about 20 kg (walking on crutches is still necessary). In this period in some cases even driving is possible. Cars with automatic transmission can be driven much earlier with operated left knee joint. For the whole time though, you should move your joint as much as possible. Therefore we prescribe use of a continuous passive motion device. The more often you use this device (at least 4 hours per day and additionally 2-3 hours at night) the better the result (proven by numerous studies).
Fig. 1:Bow-leg deformity with single-sided wear of inner joint space
Fig. 2:X-ray image of whole leg with planning scheme for determi-nation of correction angle
Fig. 3:Stably-angled spread-up correc-tion of bow-legged lower leg
Fig. 4:Stably-angled spread-up correc-tion at thigh

48 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Knee Malalignment (varus-/valgus malalignment)
48
Should your joint react with swelling and pain after these 8-10 weeks of careful rehabilitation training, it is still not ready to carry your whole body weight. Another phase without too much pressure, further medication and external treatment mea-sures such as radiotherapy and ointment bandages is inevitable. Please don’t give up in this hard time, as after 3-6 months (in rare cases up to 9 months) noticeable and lasting improvement, even in cases with severe arthrosis, will show up.
Until today, there unfortunately has not been found any general patent remedy for the advanced stage of the degenerative joint disease – except for artificial joint reconstruction which should be delayed as long as possible. Please consider that without any treatment constant worsening of joint functions has to be expected.
Smith&Nephew GmbHMendelssohnstraße 15d22761 Hamburg · DeutschlandTel. +49 (0)40 70 700 - 0Fax +49 (0)40 70 700 - [email protected]
Hochleistungsdisziplin Kniegelenk
Wir haben unsere Implantate für die arthroskopische Sportmedizinentwickelt. Die hohen Ansprüche von Patienten aus dem Leistungs-sport mit Kreuzband- und Meniskusverletzungen sind unser Maßstab für anatomische Präzision, komplikationsfreie Einheilungsprozesse und Haltbarkeit auch bei extremer Beanspruchung des Gelenks.Unser Beitrag zu uneingeschränkter Bewegungsfreiheit – auch für Nichtleistungssportler.

49
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 49
Kn
ee
Knee Endoprosthetics
General Information
Arthrosis stands for the degenerative wear of joint partners rubbing against each other (cartilage wear). Healthy joints are covered with a cartilage layer in order to improve sliding properties. However, there are cases when these joint surfaces are such worn, that the underlying bone surfaces are in direct contact and there is no more chance for improvement by arthroscopic cartilage shaving (joint arthroscopy) or osseous joint transposition. Here, artificial replacement of the joint is in most cases a reasonable alternative to joint reconstruction. Major aim is long-lastingly reduce pain and rebuild the patient’s physical activity.
Already more than hundred years ago there have been made attempts to artificially replace painful joints. First successes were achieved in the 60’s and many prostheses of this time had a long life-time. Since then, the number of artificial joints implan-ted has continuously increased. Today, more than 300 000 hip- and knee joints are successfully used every year in Germany. Thanks to the good results of the last de-cades, artificial shoulder joint replacement is experiencing a growing number too.
This artificial joint is a so-called endoprosthesis (Greek: endo-inside) and is often also called total endoprosthesis as both joint segments are replaced by an artificial surface respectively an artificial joint partner. In case that only one joint segment is replaced, it is called hemi-endoprosthesis. This form is sometimes used for treatment of shoulder fractures. At hip- and knee joint however, always both parts of the joint are replaced as they carry the whole body weight and a hemi-prosthesis does not ensure sufficient pain reduction.
Of course there are also risks with endoprosthetics as it is a complex and challenging surgical procedure. Nowadays, implanting an artificial joint replacement is a routine operation but possible complications such as inflammation, thrombosis (blood clots) or damage of surrounding structures (nerves and vessels) cannot be excluded. There-fore, such surgical treatment should only be carried out in specialized units which have sufficient experiences with of artificial joint replacement. As parts of the joint are replaced by metal implants, loosening of the prosthesis can happen in the long term. However, a lifespan of more than 25 years is possible with hip prostheses. This depends on the one hand on the implants and the anchoring technique used, but on the other hand also on the surgeon and its experience.
Used materials correspond to highest demands. They shall ensure highest sliding properties with minimal friction and at the same time have the lowest wearing ef-fect as possible. Therefore, they are adjusted to each other perfectly and selected accordingly. Today, the most common materials used are: metal alloys (titanium- and cobalt-chromium-alloys), plastics (polyethylene) and ceramics (aluminium- or zirconium oxide).

50 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Knee Endoprosthetics
50
Anatomy and Functions
The biggest human joint is the movable connection between femur and tibia and consists of three parts: an inside and an outside section of the joint between the femur and the tibia (femorotibial joint), in between in the joint gap the menisci, and the third part which lies between patella (kneecap) and thigh bone (patellofe-moral joint).
All parts of the joint are covered with a cartilaginous layer and are enclosed in a common joint capsule. The synovial membrane produces a liquid that nurtures the cartilage wich has together with the menisci a shock absorbing effect. Ligament structures between the bones stabilize the joint (e.g. cruciate- and collateral liga-ments); muscles and tendons ensure movability of the joint (primarily straightening and bending). With bent knees, small rotational movements are also possible.
Knee Joint Arthrosis (gonarthrosis)
Most common reason for a knee joint disease is cartilage wear (arthrosis), which is mainly caused by leg axis deformities (varus- or valgus malalignment). Moreover, gonarthrosis may occur as the consequence of injuries, rheumatic- and metabolic disorders as well as deformities.
Loss of cartilage results in increasing stiffening and deformation of the joint, whe-reby stretching is in most cases the first movement to be lost. Osseous overhangs (osteophytes) form which in some cases even can be felt through the skin. At the same time, the pain occurs; at the beginning only in association with initial move-ments or periods of stress, later also at night and at rest. This results in increasing reduction of walking distances and finally in limitation of the quality of life.
Arthrosis can be seen in a normal X-ray image, whereby the narrowing of the joint cavity between femur and tibia is regarded as indirect sign of cartilage loss. Joint
Fig. 2:Bicompartmental partial replacement(source: Smith & Nephew GmbH)
Fig. 3:Total knee endoprosthesis(source: Smith & Nephew GmbH)
Fig. 1:Unicompartmental patellofemoral repla-cement (source: Smith & Nephew GmbH)

51
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Knee Endoprosthetics
51
Kn
ee
surfaces are often destroyed and do not optimally fit together, and the leg axis be-comes more and more deformed (bow-leg or knock-knee malposition). Moreover, the joint may swell due to the permanent irritation.
Knee Joint Prosthesis: Material – Fixation - Durability
If a joint maintaining therapy is not possible due to severity of the damage or because of the age of the patient, and all other conservative and surgical options (physiotherapy, painkillers, joint irrigation etc.) have been tried, a total knee repla-cement is necessary (TKR).
Major aim of this surcigal procedure is a pain-free, stable and movable knee joint whereby the natural leg axis is restored.
Operation techniques and implants which have been more and more improved over the last decades make this therapy method to one of the most common and most successful routine operations in orthopaedic surgery (with about 150 surgeries per year in Germany).
The knee endoprostheses used these days are known as resurfacing implants as they only replace worn cartilage surfaces, while preserving the patient’s own knee ligament structures. Depending on the severity of the arthrosis, there are different types of prostheses which do only replace frayed parts of the joint and support healthy areas.
Generally a distinction is made between the following types of prostheses:
• Unicompartmental prostheses (fig. 1, 4, 5) (unicondylar sledge or patellofemoral replacement): the isolated replacement of only one joint segment requires the other segments to be affected only very slightly and the ligament structures to be intact.
• Bicompartmental prostheses (fig. 2, 6) (mono- or bicondylar).
1) Monocondylar prostheses only replace inner (medial) joint segments and the joint between patella and thigh.
2) Bicondylar prostheses (TKR) replace joint surfaces of inner (medial) and outer (lateral) joint segments, while maintaining the patient’s own ligament structures as far as possible. The segments of thigh and lower leg are not mechanically linked with each other. In case that the ligament structures are damaged, a zylinder-shaped connection of both segments enables stabilization of the joint even without ligaments. Knee endoprostheses lying parallel to the bone which were formerly used very often, dispense preserving the patient’s own ligament structures under resection of large bone areas. Today, these prostheses are used only in exceptional cases.
All prosthesis types are available in different sizes; by means of the pre-operative planning sketch, model size and fixation of the prosthesis are specified. Here, in-dividual requirements such as age, gender, shape of bone, body weight etc., are taken into consideration. According to this planning, leg axes are measured and the prosthesis planned in its alignment.

52 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Knee Endoprosthetics
52
There exist different fixation techniques for implantations: The cemented TKR is regarded as the “gold standard” worldwide. Here, the implants are fixed to the bone with antibiotic cement. In rare cases, also the cement-free “press-fit” anchoring technique can be used. Depending on the fixation technique used, the components are either made of titanium or a chrome-cobalt alloy. As gliding support a polyethy-lene inlay is inserted between the replaced surfaces, which is either fixed to the basis plate or rotates and glides between the surfaces (mobile inlay).
Regardless of the fixation type, a life-span of normally 12-15 years is expected. When being in a good physical condition, second surgery to change the prosthesis can be carried out at any time. Here, special prostheses are available for any stage of bone defects.
Treatment prior to Surgery and Surgical Procedure
Surgery is preceded by an in-depth patient interview, clinical and radiological exami-nations and detailed planning. Additionally, an internistic/anaesthesiological check including ECG, pulmonary function- and blood test is carried out. In most cases the operation is carried out using a tourniquet, and need for allogenic- or autologous blood can normally be excluded. The blood collected in the drainage during sur-gery can at the end be led back to the patient via a feedback system. Stationary (in-patient) admission usually takes place the day of surgery.
Depending on the individual arrangement made, the operation is carried out under general anaesthesia or spinal anaesthesia. Access to the affected joint is conducted through an approx. 10 cm long incision at the front side of the knee. When having removed the destroyed joint surfaces with precision instruments, the prosthesis components are fixed to the femur and the tibia. Due to the general public opinion and own experiences, replacement of the posterior patella surface is only carried out in cases of severe damage. When having checked the artificial joint for mobility, the wound is closed layer by layer with insertion of drainage tubes. Finally, a control X-ray is taken after surgery.
Fig. 5:Slide prosthesis, side view
Fig. 6:Total knee endoprosthesis
Fig. 4:Slide prosthesis, front view

53
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Knee Endoprosthetics
53
Kn
ee
Aftercare
Joint replacement operations are exclusively carried out unter in-patient conditions. In order to ensure optimal success, early postoperative mobilization by means of physiotherapy is strongly recommended. Depending on the already mentioned techniques for implantation, in most cases immediate load on the operated leg is permitted. However, crutches have to be used for 4-6 weeks to protect the soft part tissue. For most patients, the stay in the clinic of about 7-10 days is followed by a 3-week rehabilitation program. Within the scope of regular, outpatient check-ups at close intervals, the progress of the patient is documented and if necessary the mobilization therapy prolonged.
Joint Replacement and Sports
Having a severe knee joint arthrosis, noticeable limitation of physical activities has to be expected. When the symptoms are gone after joint replacement surgery, the desire for more sportive exercise certainly comes up again. Internationally there is a broad consensus that at least so-called “low-impact” sports such as cycling, swimming, sailing, diving, playing golf and bowling can be supported. Sports such as tennis, basket ball and skiing however, are only possible to a limited extent. Completely avoided shall be contact sports such as foot ball or hand ball. Recommendations for those different sports are also dependent on the patient’s performance level. As a rule of thumb it can be said that sports practiced prior to surgery are allowed afterwards as well.

5454
Leben in BewegungMenschen erwarten von einem künst-lichen Gelenk, dass sie sich damit wieder gut bewegen und aktiv am Leben teilnehmen können – und dass es möglichst lange hält.
Zimmer entwickelt seit 75 Jahren Im-plantate, Werkstoffe und Operations-methoden und kann Langzeitergebnisse von bis zu 25 Jahren vorweisen. Und wir forschen weiter: An weichteil schonenden minimalinvasiven Operationstechniken, immer individuelleren Lösungen und knochensparenden Implantaten für die Ansprüche jüngerer und aktiver Patienten.
Zimmer Germany GmbHMerzhauser Straße 112DE-79100 Freiburgwww.zimmergermany.de
Die Zimmer Holdings Inc. ist das weltweit führende reine Orthopädie-Unternehmen in der Forschung, Entwicklung, Produktion und im Vertrieb von Implantaten der Wiederherstellungs- und Unfallchirurgie. Das Unternehmen entwickelt, produziert und vertreibt u.a. künstlichen Gelenk ersatz, Trauma- und Wirbelsäulenprodukte, Produkte zur biologischen Regeneration defekter Gelenke und Dentalimplantate. Zimmer besitzt Niederlassungen in 25 Ländern, beschäf-tigt über 7.700 Mitarbeiter und vertreibt Produkte und Technologien in mehr als 100 Ländern.
ZIM_Anz_Patient_d_185x135_neuer Text.indd 1 12.01.2009 14:58:23 Uhr
Smith & Nephew GmbHOrthopädie & Traumatologie
Mainstraße 2D 45768 Marl
T +49 (0)2365 91 81 0F +49 (0)2365 91 81 10info.marl@smith-nephew.comwww.smith-nephew.dewww.arthrose-info.com
Am Anfang steht immer die Idee.
™Warenzeichen von Smith & Nephew.
Gemeinsam mit renommierten Ärzten und Wissenschaftlernschaffen wir in unseren Forschungseinrichtungen in der Schweiz,
Großbritannien und Belgien neue Produktlösungen für die Orthopädieund Traumatologie. Die Schenkelhalsprothese NANOS oder dasGENESIS™ II Kniesystem in Kombination mit dem innovativen Werkstoff
OXINIUM™ sind beste Beispiele dafür. Wir von der neuenSmith & Nephew lassen kreative Visionen Realitätwerden – für die optimale Versorgung des Patienten.

55
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 55
Sho
uld
er
Shoulder Impingement Syndrome
Causes
The shoulder joint is stabilized and moved mainly by the four tendons of the so-called rotator cuff. These tendons are situated in a narrow bony canal between the ball and the socket (acromion) which directly surrounds the shoulder joint. During the course of life, possible signs of wear can cause increasing narrowing of this canal what in turn may lead to painful inflammations of tendons and bursae. In advanced stages permanent damages of the rotator cuff may occur which lead to lasting painful movement restrictions of the shoulder joint.
Signs and Symptoms
Patients mostly complain of pain at night when lying on the shoulder or pain which occurs with spreading movements from a certain angle. This pain is due to compres-sion of the rotator cuff and the bursae lying above between ball and socket. Mobility of the arm is in most cases painfully limited; sometimes occurs also loss of power.
Diagnostics
Examination and questioning of the patient give in most cases decisive indications to impingement. Besides this, bony changes which result in narrowing of the sliding canal of the supraspinatus tendon can be visualized by special x-ray images. In order to confirm this diagnose of tendon damage, sonography of the shoulder or a MRI are needed.
Treatment
In early stages freedom or at least reduction of pain can be achieved by simple measures such as: temporary rest (avoiding working overhead within the painful area, no carrying of weights with outstretched arms), medication with analgesic and decongestant effect, local ice- or heat treatment as well as special physiotherapy. However, if the painful condition continues even after several months of conse-quent treatment, or the diagnosed tendon damage is confirmed, surgical repair of the tendon and removal of the bony narrowing is recommended. In case that the tendon has only minor damages, enlargement of the bony narrowing is sufficient.

56 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Shoulder Impingement Syndrome
Surgical Treatment
The first operation step is thorough assessment of the damage by arthroscopy. Further steps depend on the injuries detected during arthroscopy. Injured tendons can be treated through a small incision. In case that there is no obvious damage at the tendons, the only thing to do is grinding the bone edges at the acromion (socket) to reduce narrowing of the tendon gliding canal. Grinding the acromion is called acromioplasty and can be performed arthroscopically through two small incisions. After surgery, an in-patient stay of 1-2 days is necessary. If no operation of the tendon has been necessary, special rest of the operated shoulder is not needed. However, the shoulder joint should be treated with care for about 4-6 weeks. Informations about a special aftercare program you will receive from your ward physician. Pain limits always have to be respected, but supportive therapies such as decongestant medication and local ice-treatment are possible.
Results and Risks
With about 90% of the patients, complaints resolve within 3-6 months. In rare cases painful movement restriction of the arm remains. Operation-related risks such as infects, injuries to nerves and vessels occur rather infrequent.

57
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 57
Sho
uld
er
Calcified Tendinitis of the Shoulder (tendinosis calcarea)Causes
The shoulder joint is stabilized and moved mainly by the four tendons of the so-called rotator cuff. These tendons are situated in a narrow bony canal between the ball and the socket which directly surrounds the shoulder joint. During the course of life and often unnoticed at first may occur signs of wear, particularly with the supraspinatus tendon. This in turn can result in calcifications which also occur mostly with the supraspinatus tendon. These calcifications may lead to the so-called shoulder impingement syndrome (p. 55).
Signs and Symptoms
Patients mostly complain of pain at night when lying on the shoulder or pain which occurs with spreading movements from a certain angle. In most cases mobility of the arm is painfully limited. Acute pain may also be an indirect indication for break-up of a calcium deposit.
Diagnosis
Examination and questioning of the patient offers in most cases the essential hint that leads to a disorder in the area of the rotator cuff. Diagnosed calcium deposits can then be confirmed by x-ray images and sonography. These measures also help to differentiate between a chronic stage or an acute stage with break-up of the calcium deposit.
Treatment
Generally speaking, calcium deposits can resolve spontaneously. Unfortunately, this involves in most cases considerable discomfort. Being in this stage the motto is “first wait and see”. By temporary rest, analgesic- and decongestant medication, and local treatment with ice or heat, pain can be eased and calcium resorption supported. However, if the pain continues unchanged over a longer period of time, and the calcium deposit remains on the x-ray images without any changes operative remo-val of the deposit is recommended. Alternatively, the calcium deposit can also be destroyed by shockwave therapy, but effectiveness of this method is not definitely proven so far.

58 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Calcified Tendinitis of the Shoulder (tendinosis calcarea)Operation of Calcium Deposits within the Rotator Cuff
First step of this operation is localizing the calcium deposit by means of arthoscopy. After longitudinal incision of the affected tendon, the calcium is removed with a spoon as completely as possible. Possible occurring bone edges which lead to com-pression of the affected tendon are grinded arthroscopically. In rare cases, when the deposit cannot be found during arthroscopy, a small incision is needed for cal-cium removal. Very often, complete removal is not possible, but a large part of the remaining calcium residues resolves little by little by itself.
Aftercare
After surgery, an in-patient stay of 1-2 days is necessary. Discomfort will not disappear immediately after surgery but slowly during the following weeks. Therefore, rest for 4-6 weeks is recommended. Mobilization of the shoulder should be started carefully with the painfree area, and pain limits should strictly be respected. Aftercare can be supported by decongestant medication and local ice treatment. Convalescence of about 3-6 months should be expected until recovery of painfree functioning of the shoulder joint. In order to achieve good operation results, aftercare should be performed according to a previously defined schedule which is given to you by your ward physician.
Results and Risks
With about 90% of the patients, the surgery brings back a painfree situation. With incomplete removal of the calcium deposit, some discomfort may remain. Operation-related risks such as infects or injuries to nerves and vessels occur rather infrequent.
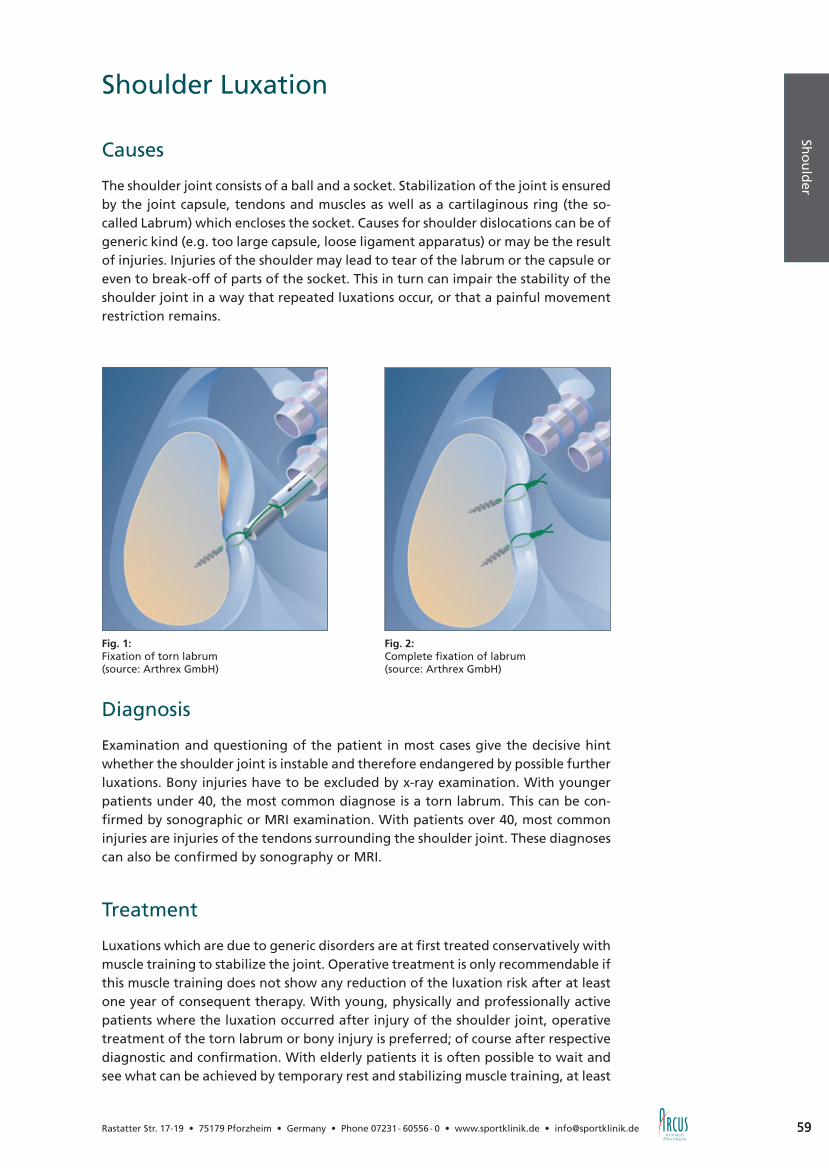
59
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 59
Sho
uld
er
Shoulder Luxation
Causes
The shoulder joint consists of a ball and a socket. Stabilization of the joint is ensured by the joint capsule, tendons and muscles as well as a cartilaginous ring (the so-called Labrum) which encloses the socket. Causes for shoulder dislocations can be of generic kind (e.g. too large capsule, loose ligament apparatus) or may be the result of injuries. Injuries of the shoulder may lead to tear of the labrum or the capsule or even to break-off of parts of the socket. This in turn can impair the stability of the shoulder joint in a way that repeated luxations occur, or that a painful movement restriction remains.
Diagnosis
Examination and questioning of the patient in most cases give the decisive hint whether the shoulder joint is instable and therefore endangered by possible further luxations. Bony injuries have to be excluded by x-ray examination. With younger patients under 40, the most common diagnose is a torn labrum. This can be con-firmed by sonographic or MRI examination. With patients over 40, most common injuries are injuries of the tendons surrounding the shoulder joint. These diagnoses can also be confirmed by sonography or MRI.
Treatment
Luxations which are due to generic disorders are at first treated conservatively with muscle training to stabilize the joint. Operative treatment is only recommendable if this muscle training does not show any reduction of the luxation risk after at least one year of consequent therapy. With young, physically and professionally active patients where the luxation occurred after injury of the shoulder joint, operative treatment of the torn labrum or bony injury is preferred; of course after respective diagnostic and confirmation. With elderly patients it is often possible to wait and see what can be achieved by temporary rest and stabilizing muscle training, at least
Fig. 1:Fixation of torn labrum(source: Arthrex GmbH)
Fig. 2:Complete fixation of labrum(source: Arthrex GmbH)

60 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Shoulder Luxation
if an injury of the tendons could be excluded. Generally it can be said that therapy has to be planned individually for every patient.
Surgical Stabilization of the Shoulder
The first operation step is thorough assessment of the damage by arthroscopy. Further steps depend on the injuries detected during arthroscopy. In case that no severe capsule injuries are diagnosed, stabilization can be performed arthroscopically. However, should severe damages to the labrum and the capsule ligament apparatus be confirmed, open stabilization through an approx. 6 cm long incision at the front side of the shoulder joint is inevitable. Primary aim of the operation is to re-attach the torn labrum to the rim of the socket. Here, small metal dowels are used. If there are furthermore bony injuries at the rim of the socket, an additional piece of bone retracted from the iliac crest has to be screwed to the socket.
Aftercare
After surgery, an in-patient stay of about 2 days is necessary. In order to avoid re-peated luxations of the shoulder joint, special aftercare is recommended. It includes conservative measures such as limitation of movement and consequent wearing of a shoulder sling for 6 weeks. Detailed information material is given to you by your ward physician. Furthermore, special muscle training as well as avoidance of over-head- and contact sports is necessary for about 4-6 months.
Results and Risks
With 90-95% of the patients stabilization can be regained. In rare cases, limitations to outward movements of the arm due to shortening of the joint capsule remain. Operation-related complications such as infects and injuries of nerves and vessels occur rather infrequent.

61
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 61
Sho
uld
er
Rotator Cuff Damages
Causes
The shoulder joint is stabilized and moved mainly by the four tendons of the so-called rotator cuff. These tendons are situated in a narrow bony canal between the ball and the socket which directly surrounds the shoulder joint. During the course of life and often unnoticed at first may occur signs of wear, particularly with the supraspinatus tendon. In extreme cases a complete hole can develop in a tendon; and here, the supraspinatus tendon is the very often affected too. In many cases there already has been a damage to the tendon which first is detected after a fall or physical overload. Acute tendon ruptures occur rather infrequent.
Signs and Symptoms
Patients mostly complain of pain at night when lying on the shoulder or pain which occurs with spreading movements from a certain angle. This pain can radiate up to the hand and in most cases mobility of the arm is painfully limited. Sometimes there also is loss of power.
Diagnosis
Examination and questioning of the patient in most cases give the decisive hint to a damage of the rotator cuff. Bony changes which lead to narrowing of the sliding canal of the rotator cuff can be detected by special x-ray images. Normally, a so-nographic examination is enough to securely confirm the tendon damage; only in rare cases MRI is needed.
Fig. 3:Supraspinatus tendon defect(source: Zimmer Germany GmbH)
Fig. 4:Supraspinatus tendon suture(source: Zimmer Germany GmbH)
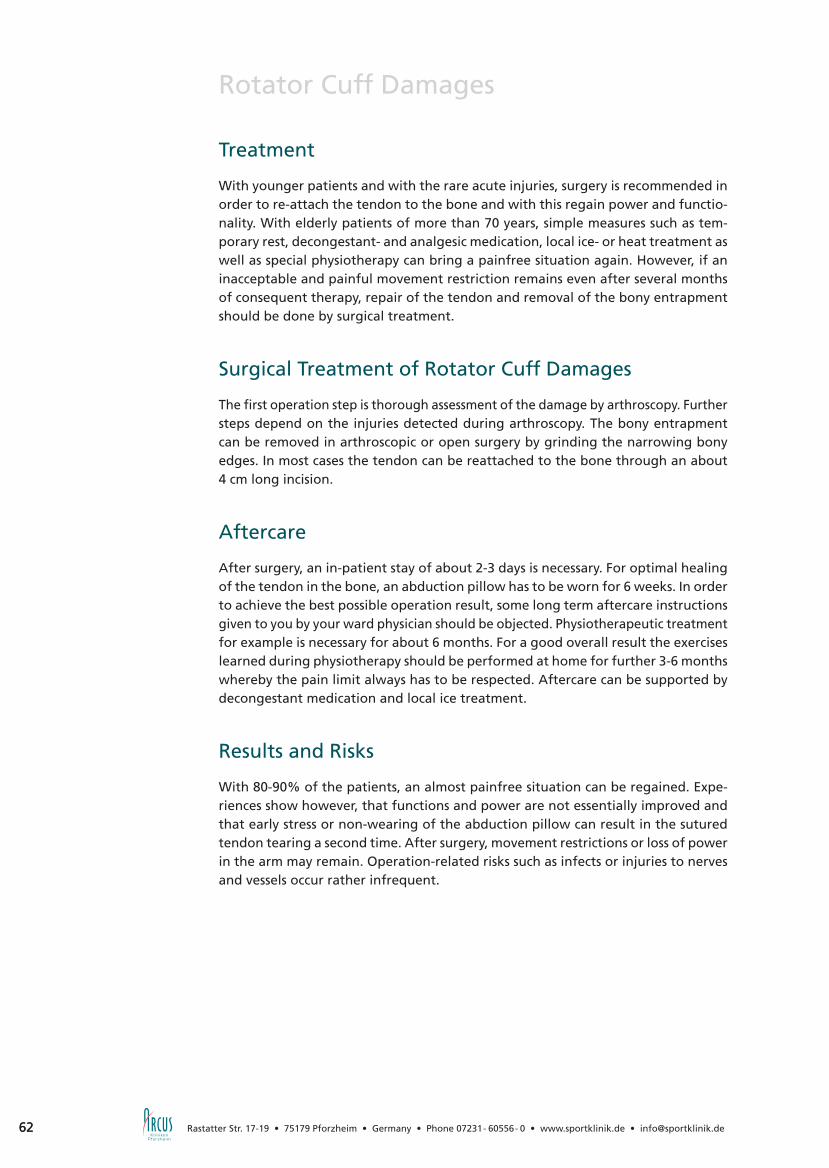
62 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Rotator Cuff Damages
Treatment
With younger patients and with the rare acute injuries, surgery is recommended in order to re-attach the tendon to the bone and with this regain power and functio-nality. With elderly patients of more than 70 years, simple measures such as tem-porary rest, decongestant- and analgesic medication, local ice- or heat treatment as well as special physiotherapy can bring a painfree situation again. However, if an inacceptable and painful movement restriction remains even after several months of consequent therapy, repair of the tendon and removal of the bony entrapment should be done by surgical treatment.
Surgical Treatment of Rotator Cuff Damages
The first operation step is thorough assessment of the damage by arthroscopy. Further steps depend on the injuries detected during arthroscopy. The bony entrapment can be removed in arthroscopic or open surgery by grinding the narrowing bony edges. In most cases the tendon can be reattached to the bone through an about 4 cm long incision.
Aftercare
After surgery, an in-patient stay of about 2-3 days is necessary. For optimal healing of the tendon in the bone, an abduction pillow has to be worn for 6 weeks. In order to achieve the best possible operation result, some long term aftercare instructions given to you by your ward physician should be objected. Physiotherapeutic treatment for example is necessary for about 6 months. For a good overall result the exercises learned during physiotherapy should be performed at home for further 3-6 months whereby the pain limit always has to be respected. Aftercare can be supported by decongestant medication and local ice treatment.
Results and Risks
With 80-90% of the patients, an almost painfree situation can be regained. Expe-riences show however, that functions and power are not essentially improved and that early stress or non-wearing of the abduction pillow can result in the sutured tendon tearing a second time. After surgery, movement restrictions or loss of power in the arm may remain. Operation-related risks such as infects or injuries to nerves and vessels occur rather infrequent.

63
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 63
Sho
uld
er
Injuries and Arthrosis of theAcromioclavicular Joint (AC-joint)Causes
The joint lying between the socket and the collarbone is called AC-joint. Falling onto the shoulder is often accompanied by ruptures of the joint ligaments. This can result in an upward dislocation of the collarbone. But the AC-joint can also be damaged in association with degenerative signs (arthrosis) which may occur when physically working hard.
Signs and Symptoms
After ligament ruptures arises painful movement restriction of the shoulder joint, which fortunately recedes with 80% of the patients. Very often, patients also comp-lain of pain at night when lying on the shoulder or pain which occurs with spreading movements from a certain angle. When palpating the joint, pain arises on pressure. In some cases after ligament ruptures, one can even see that the outer end of the collarbone points upwards.
Diagnosis
Examination and questioning of the patient in most cases give the decisive indication of an AC-joint damage. With ligament ruptures, the outer end of the collarbone may visible and palpable point upwards and cause heavy pain. Bony changes can be visualized by focused x-ray images. With arthrosis, cause of discomfort respec-tively localization of the AC-joint as definite cause can be achieved by injecting an analgesic into the joint space.
Treatment
Treatment of ligament ruptures of the AC-joint can be performed either conser-vatively or surgically. If surgical treatment is necessary depends on severity of the ligament rupture. Up to a grade III rupture we in most cases recommend conserva-tive therapy first. That means resting the shoulder and avoiding weight stress and
Fig. 5:Stabilization of AC-joint (source: Arthrex GmbH)
Fig. 6:Stabilization of AC-joint (source: Arthrex GmbH)

64 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Injuries and Arthrosis of theAcromioclavicular Joint (AC-joint)spreading movements over the horizontal level for about 6-8 weeks. Only in few cases there is absolute need for immediate operation. When having treated the ligament rupture conservatively and a painful movement restriction develops there are several operation methods to regain painfree mobility and correct position of the collarbone even after years.
Pain which results from degenerative wear of the AC-joint can be eliminated by chiseling off the outer end of the collarbone.
Operative Treatment
In case of an isolated arthrosis of the AC-joint, the outer end of the collarbone is removed (approx. 7-10 mm). This can be done by arthroscopic surgery or open sur-gery through two small incisions. If the arthrosis results from a former injury with rupture of the joint ligaments, the outer end of the collarbone is removed (like with AC-arthroscopy) and the collarbone reattached in correct position with a body-own ligament which passes to the socket (there additionally may also be need for wires, screws or an artificial ligament). When operating ligament ruptures directly after the accident we mostly make use of temporary fixation of the collarbone by wires. They are removed in a second small operation 6-8 weeks later after healing of the ligament suture.
Aftercare
After surgery, an in-patient stay of about 2-3 days is necessary. Aftercare of AC-joint operations depends on the surgical method used. Removal of the outer end of the collarbone alone does not require special rest. When having stabilized the joint with ligaments, wire slings or screws, limitation to movement has to be objected for about 6-8 weeks to avoid avulsion of the ligaments or breakage of the metal implant. You will receive a special aftercare program from your ward physician. The pain limit always has to be respected. Aftercare can be supported by decongestant medication and local ice treatment.
Results and Risks
About 80% of the patients regain painfree mobility of the shoulder joint within 3-6 months. After joint stabilization with metal implants, there is the danger of 20% of breakage or loosening of the metal as well as repeated upward dislocation of the outer end of the collarbone. Further operation-related risks which occur more often are wound healing disorders and infects. Injuries to nerves and vessels occur rather infrequent.
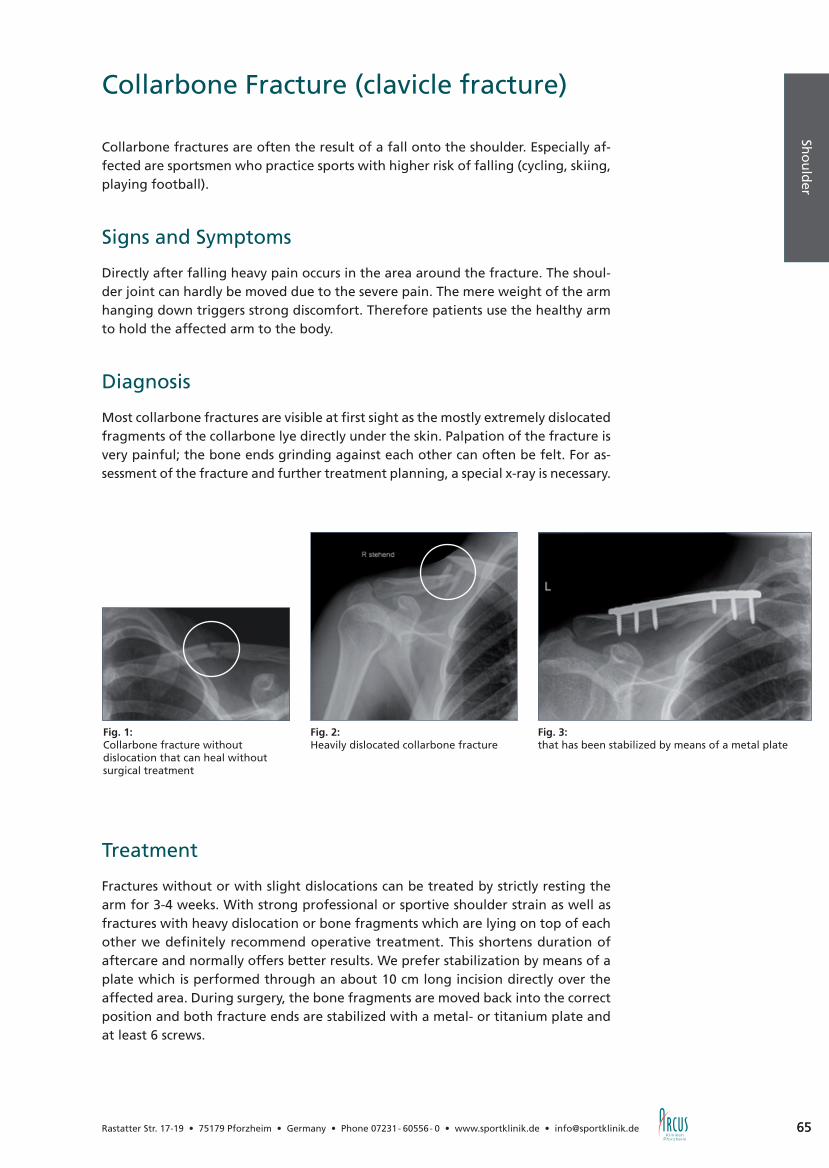
65
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 65
Sho
uld
er
Collarbone Fracture (clavicle fracture)
Collarbone fractures are often the result of a fall onto the shoulder. Especially af-fected are sportsmen who practice sports with higher risk of falling (cycling, skiing, playing football).
Signs and Symptoms
Directly after falling heavy pain occurs in the area around the fracture. The shoul-der joint can hardly be moved due to the severe pain. The mere weight of the arm hanging down triggers strong discomfort. Therefore patients use the healthy arm to hold the affected arm to the body.
Diagnosis
Most collarbone fractures are visible at first sight as the mostly extremely dislocated fragments of the collarbone lye directly under the skin. Palpation of the fracture is very painful; the bone ends grinding against each other can often be felt. For as-sessment of the fracture and further treatment planning, a special x-ray is necessary.
Treatment
Fractures without or with slight dislocations can be treated by strictly resting the arm for 3-4 weeks. With strong professional or sportive shoulder strain as well as fractures with heavy dislocation or bone fragments which are lying on top of each other we definitely recommend operative treatment. This shortens duration of aftercare and normally offers better results. We prefer stabilization by means of a plate which is performed through an about 10 cm long incision directly over the affected area. During surgery, the bone fragments are moved back into the correct position and both fracture ends are stabilized with a metal- or titanium plate and at least 6 screws.
Fig. 2:Heavily dislocated collarbone fracture
Fig. 3:that has been stabilized by means of a metal plate
Fig. 1:Collarbone fracture without dislocation that can heal without surgical treatment

66 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Collarbone Fracture (clavicle fracture)
Aftercare
After surgery the arm should be relieved by wearing a shoulder sling until removal of the stitches after 2 weeks. This eases the pain and supports healing of the wound. From the first day on you can move your arm in the shoulder sling. You will learn respective exercises from your physiotherapist. After about 2 days you can leave the hospital. From the third week after surgery you can take off the sling and move the arm without additional weights. Most fractures are stably healed after 12 weeks but the plate should not be removed before one year after surgery what is done in a short out-patient surgery. Complications such as infects, healing disorders of the fracture or a repeated fracture after plate removal occur rather rare.
Fig. 4:Fracture at the external end of the collarbone
Fig. 5:A special clavicle hook plate is needed for stabilization

67
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 67
Sho
uld
er
Humeral head fracture
A humeral head fracture is often a result of a fall onto the shoulder. Especially affected are elderly women with osteoporosis as well as sportsmen who practice sports with higher risk of falling (cycling, skiing, motorcycling).
Signs and Symptoms
Directly after falling heavy pain occurs in the area around the fracture. The shoulder joint can hardly be moved due to the severe pain. In many cases the patient can feel the bone ends grinding against each other. The healthy arm should hold the affected arm to the body.
Diagnosis
In order to assess whether it is “only” a heavy contusion or a real humeral head fracture, x-ray images are needed. With them also type and severity of the fracture can be defined. A distinction is made between fractures with 2, 3 and 4 bigger bone fragments as well as difficult comminuted fractures. By means of the x-ray images taken further treatment can be planned.
Fig. 1:Slightly dislocated fracture, healing by immobilization and physiotherapy
Fig. 2:Completely dislocated fracture
Fig. 3:Stabilization with plate

68 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Humeral head fracture
TreatmentBy means of the x-ray images is decided whether an operation is necessary. Heavily dislocated fractures are operated. Fractures without or with slight dislocation can normally be treated conservatively by temporarily resting the affected arm and practicing physiotherapeutic exercises afterwards. However, with heavy professional or sportive strain we nevertheless recommend surgery also for slightly dislocated fractures as it shortens the period of aftercare and supports better results. The surgery method used depends on the type of fracture. Fractures with only one fragment can often be stabilized with screws. Complicated fractures with 3 or 4 bone fragments require stabilization by nails or plates. And with comminuted fractures is sometimes even makes sense to use a prosthesis. We prefer stabilization with a plate – even with complicated fractures. During surgery all bone fragments are moved back into the correct position by opening the skin directly over the fracture for approx. 15 cm. Then all those fragments are affixed to one plate (of metal or titanium).
Aftercare
After surgery the arm should be relieved by wearing a shoulder sling until remo-val of the stitches after 2 weeks. This eases the pain and supports healing of the wound. From the first day after surgery on you can move your arm in the shoulder sling. You will learn respective exercises from your physiotherapist. After about 4-5 days you can leave the hospital. From the third week after surgery you can take off the sling and move the arm without additional weights. Most fractures are stably healed after 12 weeks but the plate should not be removed before one year after surgery. Complications such as infects, healing disorders of the fracture or a repeated fracture after plate removal occur rather rare. Typical for humeral head fractures is that with about a third of all patients, discomfort when lying on the shoulder, as well as discomfort or movement restrictions when spreading the arm or moving it outwards can remain despite correct stabilization.

69
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 69
Sho
uld
er
Shoulder Endoprosthetics
Shoulder prosthesis with arthrosis and after bone fractures
Causes
Within the frame of age-related wearing processes, or after circulatory disorders or fractures of the ball, there might occur loss of joint cartilage and damage of the shoulder joint with painful limitation to its functions. In later stages then the mus-culature recedes what results in increasing stiffening of the joint.
Signs and Symptoms
At the beginning, increasing pain occurs with rotational movements and spreading of the arm to the side. Later, every movement is accompanied by pain and the shoulder joint shows progressing movement restrictions; the patient suffers from pain at night and rest pain.
Diagnosis
Examination and questioning of the patient in most cases offers the decisive indi-cation of shoulder joint arthrosis. This assumption can then be confirmed by x-ray. For operation planning and assessment of the tendons surrounding the shoulder joint, further examination by sonography is necessary. In some cases even CT or MRI are needed.
Fig. 1:Shoulder ball replacement without socket(source: Zimmer Germany GmbH)
Fig. 2:Total shoulder joint endoprosthesis(source: Zimmer Germany GmbH)
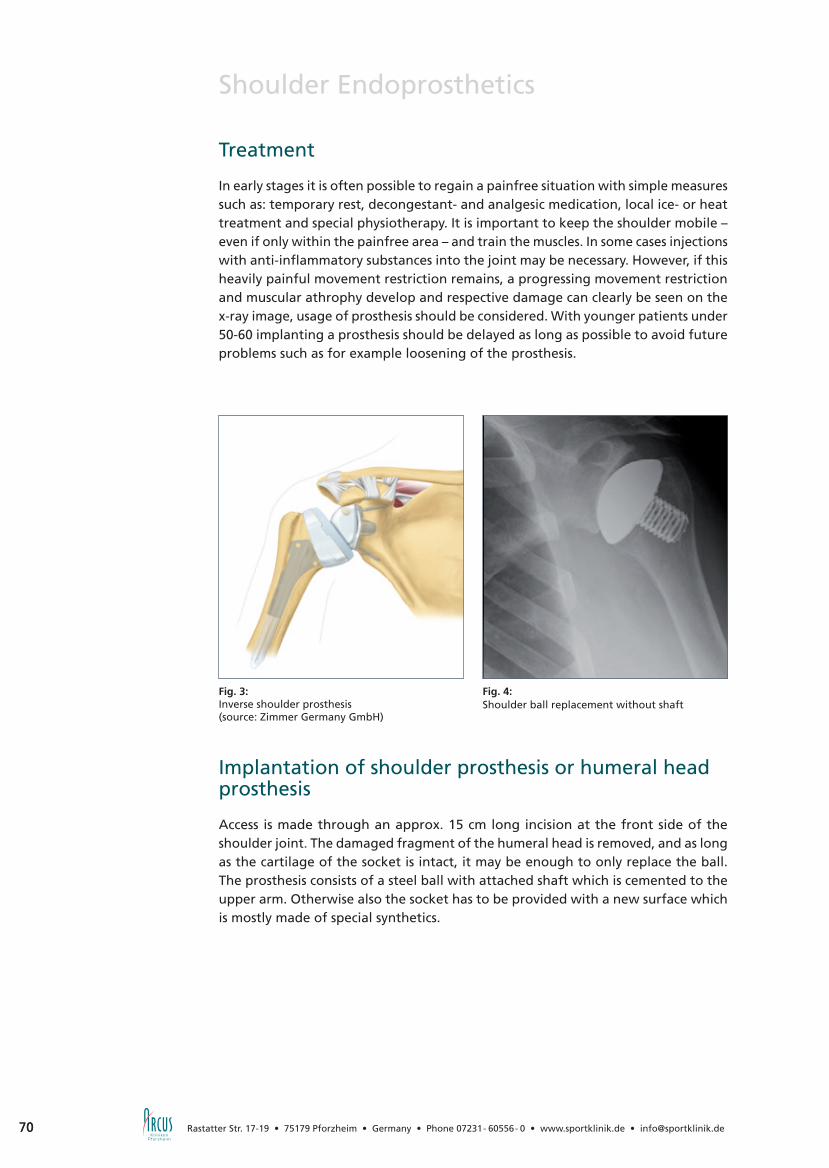
70 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Shoulder Endoprosthetics
Treatment
In early stages it is often possible to regain a painfree situation with simple measures such as: temporary rest, decongestant- and analgesic medication, local ice- or heat treatment and special physiotherapy. It is important to keep the shoulder mobile – even if only within the painfree area – and train the muscles. In some cases injections with anti-inflammatory substances into the joint may be necessary. However, if this heavily painful movement restriction remains, a progressing movement restriction and muscular athrophy develop and respective damage can clearly be seen on the x-ray image, usage of prosthesis should be considered. With younger patients under 50-60 implanting a prosthesis should be delayed as long as possible to avoid future problems such as for example loosening of the prosthesis.
Implantation of shoulder prosthesis or humeral head prosthesis
Access is made through an approx. 15 cm long incision at the front side of the shoulder joint. The damaged fragment of the humeral head is removed, and as long as the cartilage of the socket is intact, it may be enough to only replace the ball. The prosthesis consists of a steel ball with attached shaft which is cemented to the upper arm. Otherwise also the socket has to be provided with a new surface which is mostly made of special synthetics.
Fig. 3:Inverse shoulder prosthesis(source: Zimmer Germany GmbH)
Fig. 4: Shoulder ball replacement without shaft

71
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 71
Sho
uld
er
Shoulder Endoprosthetics
Aftercare
After surgery, an in-patient stay of about one week is necessary. In order to achieve the optimal operation result, aftercare should be carried out according to a previously defined scheme which is given to you by your ward physician. It depends on the type of prosthesis used and on the tendons sutured during operation. During the first weeks, limitation to outward rotations has to be objected in order to prevent sutured tendons from tearing again. Physiotherapy is necessary for about 3-6 months but to achieve the best possible result, exercises should be practiced independently at home for further 3-6 months.
Results and Risks
With 80-90% of the patients, shoulder prosthesis helps regaining painfree functioning of the shoulder joint. The achievable level of movability depends on condition of the joint prior to operation and your contribution. Operation-related risks such as: A humerus fracture during attachment of the prosthesis, sprains of the artificial joint, infects or injuries to nerves and vessels occur rather rare. As with any artificial joint, the shoulder prosthesis may loosen some day and need to be replaced. According to the experiences made so far, an average lifespan of 10 years is expected, whereby loosening mostly occurs with the artificial socket.

72 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
BORT OmoFX
Variable Arm-Abduktionsorthese zur therapeutischkorrekten Lagerung in 30° oder 50°
Impingementsyndrom, Schultergelenksverletzungen, Zustand nachRotatorenmanschetten-Ruptur – es gibt viele Indikationen bei denendie Lagerung des Schulter- und Ellenbogengelenkes notwendig wird.Aber nur eine optimale Lösung für den Patienten:Die BORT OmoFX mit freipositionierbaren Stabilisierungsbändern vereint sichere Fixierung und therapeutisch sinnvolle Lagerung desArmes.BORT OmoFX – hoher Tragekomfort für und gute Compliance bei dem Patienten.
Art. Nr. 121 100BORT OmoFXPos.Nr. 20.09.01.0011
www.bort.com
O R T H O P Ä D I E | C H I R U R G I E | S P O R T M E D I Z I N | R E H A B I L I T A T I O N
Schulterarthroskopie für Fortgeschrittene
Die Vielfalt unserer Produkte für sämtliche Schulterprozeduren wie z.B. die Rotatorenmanschettenrekonstruktion ist so groß wie der anatomische Anspruch dieser komplexen Indikationen. Das intelligente Design und die Zuverlässigkeit unserer Instrumente und Implantate ermöglichen optimale Operationsergebnisse für die nachhaltige Wiederherstellung der Bewegungsfreiheit der Patienten.
Smith&Nephew GmbHMendelssohnstraße 15d22761 Hamburg · DeutschlandTel. +49 (0)40 70 700 - 0Fax +49 (0)40 70 700 - [email protected]
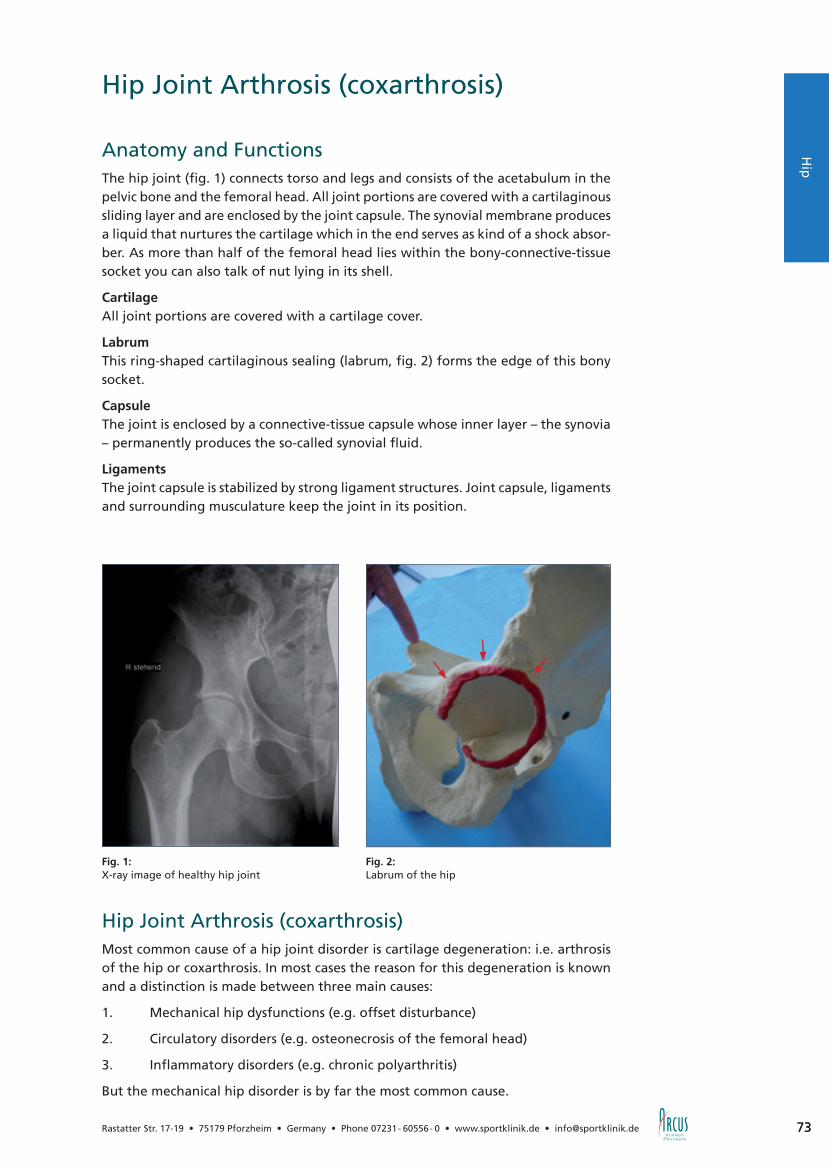
73
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 73
Hip Joint Arthrosis (coxarthrosis)
Anatomy and FunctionsThe hip joint (fig. 1) connects torso and legs and consists of the acetabulum in the pelvic bone and the femoral head. All joint portions are covered with a cartilaginous sliding layer and are enclosed by the joint capsule. The synovial membrane produces a liquid that nurtures the cartilage which in the end serves as kind of a shock absor-ber. As more than half of the femoral head lies within the bony-connective-tissue socket you can also talk of nut lying in its shell.
CartilageAll joint portions are covered with a cartilage cover.
LabrumThis ring-shaped cartilaginous sealing (labrum, fig. 2) forms the edge of this bony socket.
CapsuleThe joint is enclosed by a connective-tissue capsule whose inner layer – the synovia – permanently produces the so-called synovial fluid.
Ligaments The joint capsule is stabilized by strong ligament structures. Joint capsule, ligaments and surrounding musculature keep the joint in its position.
Hip Joint Arthrosis (coxarthrosis)Most common cause of a hip joint disorder is cartilage degeneration: i.e. arthrosis of the hip or coxarthrosis. In most cases the reason for this degeneration is known and a distinction is made between three main causes:
1. Mechanical hip dysfunctions (e.g. offset disturbance)
2. Circulatory disorders (e.g. osteonecrosis of the femoral head)
3. Inflammatory disorders (e.g. chronic polyarthritis)
But the mechanical hip disorder is by far the most common cause.
Fig. 1: X-ray image of healthy hip joint
Fig. 2: Labrum of the hip
Hü
fteH
ip

74 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Hip Joint Arthrosis (coxarthrosis)
The Femoral Neck Offset
Figure 3 shows the normal form of femoral neck and femoral head in cross-section. The femoral head protrudes the femoral neck both at the front and the back side. This midsection of the femoral neck is called offset. There are often disease patterns where this passage is much flatter (offset disturbance, fig. 4); this is mostly the result of a growth disorder of sportily active patients in the adolescence.
This offset disturbance leads to the femoral neck hitting the socket edge when ben-ding forwards (fig. 5). The first thing which becomes injured is the “sealing ring” of the hip, the so-called labrum. An early symptom of this offset disturbance is groin pain. During the following course of disease the cartilage of the socket becomes destroyed. Without treatment this loss of protecting cartilage leads to an increa-sing arthrosis with stiffening of the joint. At the advanced stage, ball and socket become partly damaged and do not optimally fit into each other any longer. At the same time run-in- and stress pain starts, later pain occurs also at night and while at rest. All this finally results in reduction of the walking distance and in an enormous reduction of the quality of life.
Diagnosis
Diagnosis can be set by typical anamnesis, examination and by means of a normal x-ray image, whereby narrowing of the joint space between hip- and femoral bone is an indirect sign of cartilage loss. The MRI enables more precise examination of labrum and cartilage.
Fig. 3:Offset
Fig. 4:Offset disturbance
Fig. 5:Impingement

75
Ellenb
og
en
75
Hü
fte
Hip Joint Arthrosis (coxarthrosis)
Therapy of Offset Disturbance and Prevention for Hip ArthrosisTherapy of this offset disturbance is always carried out surgically as there is no reli-able conservative therapy known. This means restoration of the femoral neck offset and removal or suture of the torn labrum. With this the cartilage is protected and hip arthrosis prevented.
If a patient suffers from groin pain, differentiated assessment shows the dimensions of this growth disorder and already existing damages. Besides clinical examination and conventional x-ray images, the most important method here is MRI; and it is decisive that NMR is made with intra-articular contrast medium and on special se-quences. This is the only possibility to achieve a differentiated result about labrum and condition of the cartilage.
In order to avoid early degeneration of the hip joint correcting surgery should be carried out. We offer you a new operation technique at the ARCUS Clinics to repair this defect by means of hip arthroscopy (p 76). The torn part of the labrum is re-moved under arthroscopic control and the lacking femoral neck midsection formed artificially. This takes away the femoral neck entrapment and degeneration of the hip can be stopped or avoided.
www.sporlastic.de · [email protected]
Hüftbandage zur konservativenoder postoperativen Behandlungvon Hüftgelenkerkrankungen.
Hip

76 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Hip Arthroscopy
In recent years, hip arthroscopy has become a standard surgery method when treating hip disorders. With this technique formerly common large incisions and resulting soft tissue damages as well as a long rehabilitation period can be prevented.
Indications for hip arthroscopy are:
• Loose joint bodies• Labrum ruptures• Degenerative changes• Beginning hip arthrosis (p. 73)• Movement restrictions of the hip• Cartilage injuries• Inflammations of the synovial membrane• Tear of the central hip ligament (Lig. teres)• Joint infections• Impingement of the hip (see step-by-step plan for treatment of hip arthrosis p. 78)• Problems after hip replacement surgery
The surgery technique is very challenging and requires long term experience. There-fore we are very proud that more than 100 hip arthroscopies are carried out at the ARCUS Clinics every year.
Fig. 1: Hip arthroscopy
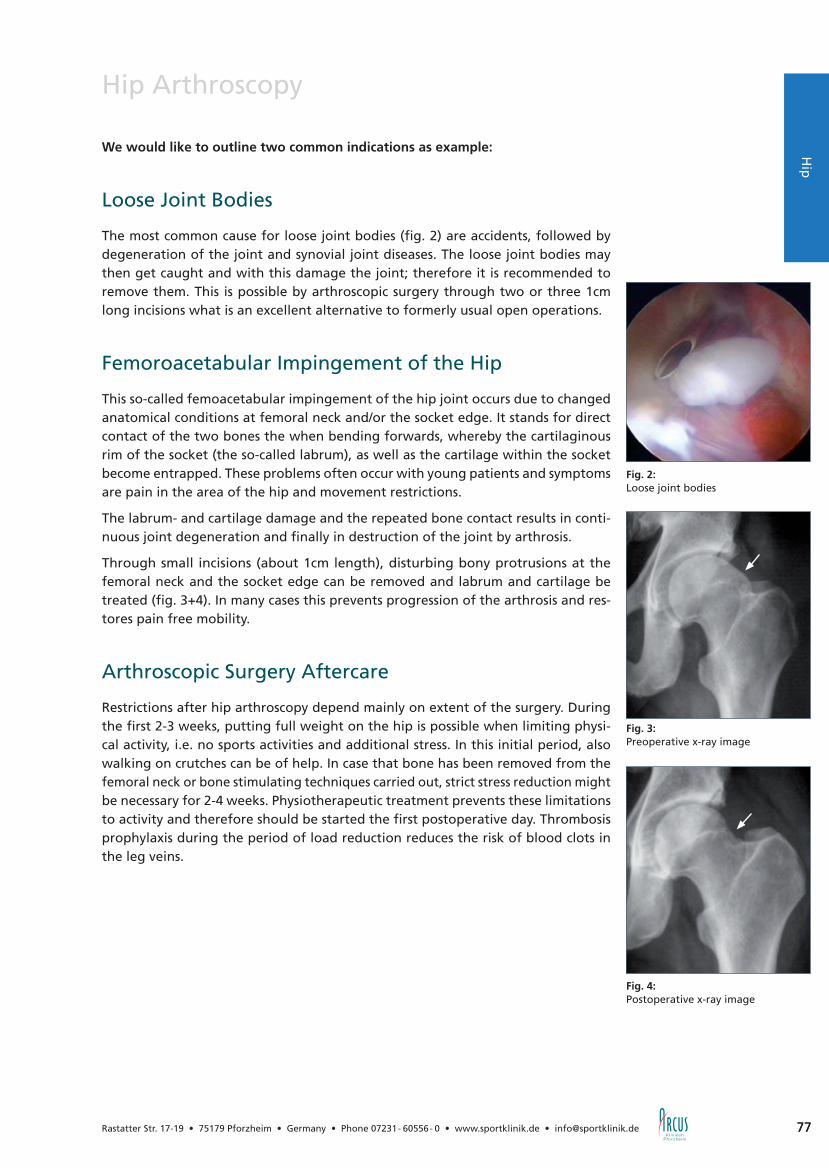
77
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 77
Hip
Hip Arthroscopy
We would like to outline two common indications as example:
Loose Joint Bodies
The most common cause for loose joint bodies (fig. 2) are accidents, followed by degeneration of the joint and synovial joint diseases. The loose joint bodies may then get caught and with this damage the joint; therefore it is recommended to remove them. This is possible by arthroscopic surgery through two or three 1cm long incisions what is an excellent alternative to formerly usual open operations.
Femoroacetabular Impingement of the Hip
This so-called femoacetabular impingement of the hip joint occurs due to changed anatomical conditions at femoral neck and/or the socket edge. It stands for direct contact of the two bones the when bending forwards, whereby the cartilaginous rim of the socket (the so-called labrum), as well as the cartilage within the socket become entrapped. These problems often occur with young patients and symptoms are pain in the area of the hip and movement restrictions.
The labrum- and cartilage damage and the repeated bone contact results in conti-nuous joint degeneration and finally in destruction of the joint by arthrosis.
Through small incisions (about 1cm length), disturbing bony protrusions at the femoral neck and the socket edge can be removed and labrum and cartilage be treated (fig. 3+4). In many cases this prevents progression of the arthrosis and res-tores pain free mobility.
Arthroscopic Surgery Aftercare
Restrictions after hip arthroscopy depend mainly on extent of the surgery. During the first 2-3 weeks, putting full weight on the hip is possible when limiting physi-cal activity, i.e. no sports activities and additional stress. In this initial period, also walking on crutches can be of help. In case that bone has been removed from the femoral neck or bone stimulating techniques carried out, strict stress reduction might be necessary for 2-4 weeks. Physiotherapeutic treatment prevents these limitations to activity and therefore should be started the first postoperative day. Thrombosis prophylaxis during the period of load reduction reduces the risk of blood clots in the leg veins.
Fig. 2: Loose joint bodies
Fig. 3: Preoperative x-ray image
Fig. 4: Postoperative x-ray image

78 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Step-by-step Plan for Treatment of CoxarthrosisIn case that joint arthrosis had been diagnosed, there was so far only the option of artificial hip joint replacement (THR) if conservative treatment methods such as physiotherapy, thalassotherapy, massages, pain medication etc. had already proven unsuccessful.
Furthermore, treatment did consider neither severity of the disease nor age of the patient. Therefore we developed a step-by-step plan which ensures stage-related therapy.
1. Moderate coxarthrosis with protrusions:
Considerable improvement of discomfort can be achieved by recovering the stage of compensated arthrosis with arthroscopic hip surgery (p. 76). Disturbing osteophytes at femoral neck and socket are removed and the contract capsule partly recessed what brings back movability. Additionally, removal of torn parts of the labrum and inflamed portions of the synovial membrane allow considerable pain reduction. And with this method even loose joint bodies can be removed what enables the patient to be physically active again and delay an artificial hip implant.
2. Advanced arthrosis with young patients(Female patients under 60, male patients under 65):
When the joint is completely destroyed, joint-preserving surgery no longer makes sense. However, in order to preserve as many bones as possible, younger patients are implanted a femoral head cap (fig. 2) - a resection of the femoral neck is not neces-sary. Advantage is here preservation of normal anatomy (offset, force transmission and size of femoral head) what is needed for the normal range of movement. The resulting stability enables sportive activity without limitations. Another important advantage is the protection of bone substance which might become decisive with regard to a future revision.
Not every hip arthrosis can optimally be treated with a femoral head cap. In such cases we alternatively use short-stem hip prostheses.
3. Advanced arthrosis with elderly patients(Female patients over 60, male patients over 65):
As the femoral neck is here not strong enough to carry surface replacement due to the reduced level of calcium carbonate in the bones, complete hip arthroplasty is the only option. This is another treatment where we achieve enormous progress, and besides better materials there have also been essential improvements with the operation technique. By developing the concept of minimally-invasive surgery (MIS) we only need very small incisions (6-8 cm). But the decisive advantage is the fact that almost no muscles have to be detached. This brings minimization of tissue trauma, an overall gentle operation method and less pain. Immediate full strain is possible and blood loss is reduced what in turn accelerates rehabilitation.
Fig. 1: 46 year old man with arthritis
Fig. 2: Hip with surface replacement(source: Smith & Nephew GmbH)
Fig. 3: Total endoprosthesis
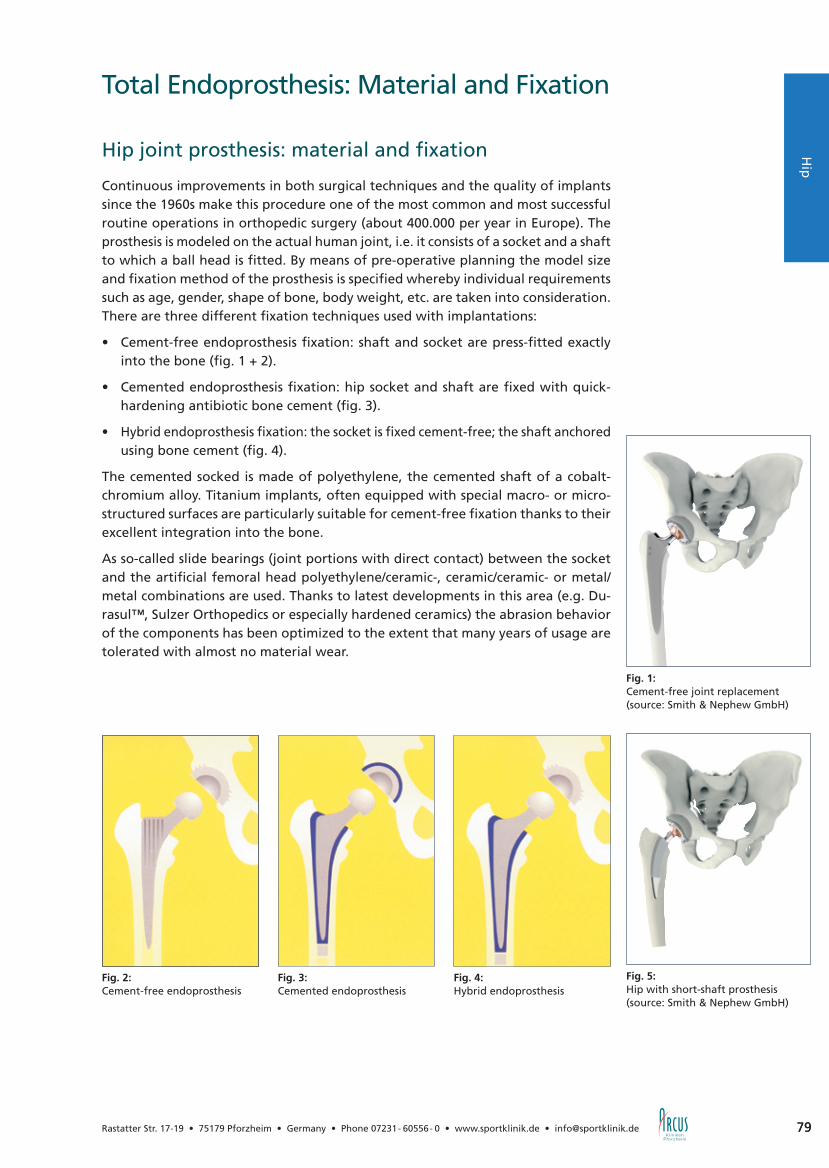
79
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 79
Hip
Total Endoprosthesis: Material and Fixation
Hip joint prosthesis: material and fixation
Continuous improvements in both surgical techniques and the quality of implants since the 1960s make this procedure one of the most common and most successful routine operations in orthopedic surgery (about 400.000 per year in Europe). The prosthesis is modeled on the actual human joint, i.e. it consists of a socket and a shaft to which a ball head is fitted. By means of pre-operative planning the model size and fixation method of the prosthesis is specified whereby individual requirements such as age, gender, shape of bone, body weight, etc. are taken into consideration. There are three different fixation techniques used with implantations:
• Cement-free endoprosthesis fixation: shaft and socket are press-fitted exactly into the bone (fig. 1 + 2).
• Cemented endoprosthesis fixation: hip socket and shaft are fixed with quick-hardening antibiotic bone cement (fig. 3).
• Hybrid endoprosthesis fixation: the socket is fixed cement-free; the shaft anchored using bone cement (fig. 4).
The cemented socked is made of polyethylene, the cemented shaft of a cobalt-chromium alloy. Titanium implants, often equipped with special macro- or micro-structured surfaces are particularly suitable for cement-free fixation thanks to their excellent integration into the bone.
As so-called slide bearings (joint portions with direct contact) between the socket and the artificial femoral head polyethylene/ceramic-, ceramic/ceramic- or metal/metal combinations are used. Thanks to latest developments in this area (e.g. Du-rasul™, Sulzer Orthopedics or especially hardened ceramics) the abrasion behavior of the components has been optimized to the extent that many years of usage are tolerated with almost no material wear.
Fig. 2:Cement-free endoprosthesis
Fig. 3:Cemented endoprosthesis
Fig. 4:Hybrid endoprosthesis
Fig. 5: Hip with short-shaft prosthesis(source: Smith & Nephew GmbH)
Fig. 1: Cement-free joint replacement(source: Smith & Nephew GmbH)
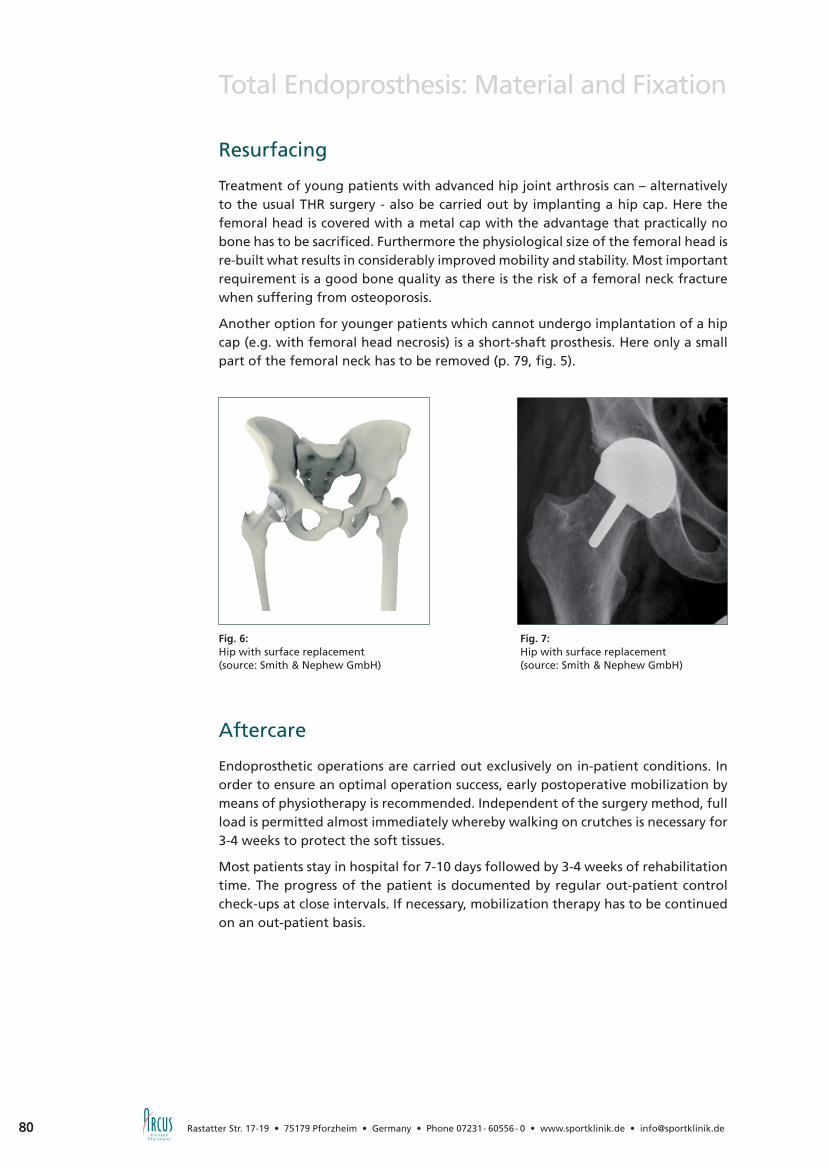
80 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Total Endoprosthesis: Material and Fixation
Resurfacing
Treatment of young patients with advanced hip joint arthrosis can – alternatively to the usual THR surgery - also be carried out by implanting a hip cap. Here the femoral head is covered with a metal cap with the advantage that practically no bone has to be sacrificed. Furthermore the physiological size of the femoral head is re-built what results in considerably improved mobility and stability. Most important requirement is a good bone quality as there is the risk of a femoral neck fracture when suffering from osteoporosis.
Another option for younger patients which cannot undergo implantation of a hip cap (e.g. with femoral head necrosis) is a short-shaft prosthesis. Here only a small part of the femoral neck has to be removed (p. 79, fig. 5).
Aftercare
Endoprosthetic operations are carried out exclusively on in-patient conditions. In order to ensure an optimal operation success, early postoperative mobilization by means of physiotherapy is recommended. Independent of the surgery method, full load is permitted almost immediately whereby walking on crutches is necessary for 3-4 weeks to protect the soft tissues.
Most patients stay in hospital for 7-10 days followed by 3-4 weeks of rehabilitation time. The progress of the patient is documented by regular out-patient control check-ups at close intervals. If necessary, mobilization therapy has to be continued on an out-patient basis.
Fig. 6: Hip with surface replacement(source: Smith & Nephew GmbH)
Fig. 7: Hip with surface replacement(source: Smith & Nephew GmbH)

81
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 81
Hip
Joint Replacement and Sports
Having a severe hip joint arthrosis, noticeable limitation of physical activities has to be expected. When the symptoms are gone after joint replacement surgery, the desire for more sportive exercise certainly comes up again. Internationally there is a broad consensus that at least so-called “low-impact” sports such as cycling, swimming, sailing, diving, playing golf and bowling can be supported. Sports such as tennis, basket ball and skiing however, are only possible to a limited extent. Completely avoided shall be contact sports such as foot ball or hand ball. Recommendations for those different sports are also dependent on the patient’s performance level. As a rule of thumb it can be said that sports practiced prior to surgery are allowed afterwards as well.
Total Endoprosthesis: Material and Fixation

82 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Elbow
Fig. 1: Radial epicondyle
General Information
The elbow is a very stable and highly congruent joint which comprises three diffe-rent portions. It serves as hinge between upper arm and ulna and enables turning movements of ulna, radius and upper arm.
Stabilization is given through the bony guide, the tight capsular ligament apparatus and the muscles surrounding the joint. Nevertheless, the elbow is the second most frequently-dislocating joint.
Injuries and disorders of the elbow are mostly of complex nature, and understanding different possible diseases is an essential condition for successful therapy. Especially the anatomic vicinity to nerves and vessels requires an experienced surgeon specia-lized in this area.
Besides clinical examination, there are also conventional x-ray, sonography, MRI and CT available for diagnostics.
Tennis Elbow (Epicondylitis humeri radialis)
This diagnosis rather stands for a symptom. It refers to pain occurring on the lateral epicondylus of the upper arm with pain radiating to the forearm extensor muscle (fig.1).
In many cases this disease is caused by unusual heavy physical activity or monoto-nous work (e.g. desk jobs). This triggers an inflammation of the forearm extensor muscle base at the lateral humeral condyle. Normally, when being treated early with symptomatic therapy including physiotherapy, anti-inflammatory procedures and wearing of a bandage, acute symptoms can be eased or healed.
Thus it is recommended to even treat chronic progressions (symptoms for more than 6 months) conservatively first for a sufficiently long time before considering surgical therapy.
However, if these conservative treatment methods remain unsuccessful, operation indication is set after a differentiated diagnosis of the elbow with conventional x-ray and MRI (fig. 2). In case that surgical treatment is needed, the elbow should be operated not only open (via incision) but also arthroscopically (with camera tech-nology). This is indispensable for identification and treatment of the reason for this chronic progression which is lying inside the joint. One of the most common causes for chronic pain development is instability of the outer capsule-ligament apparatus.
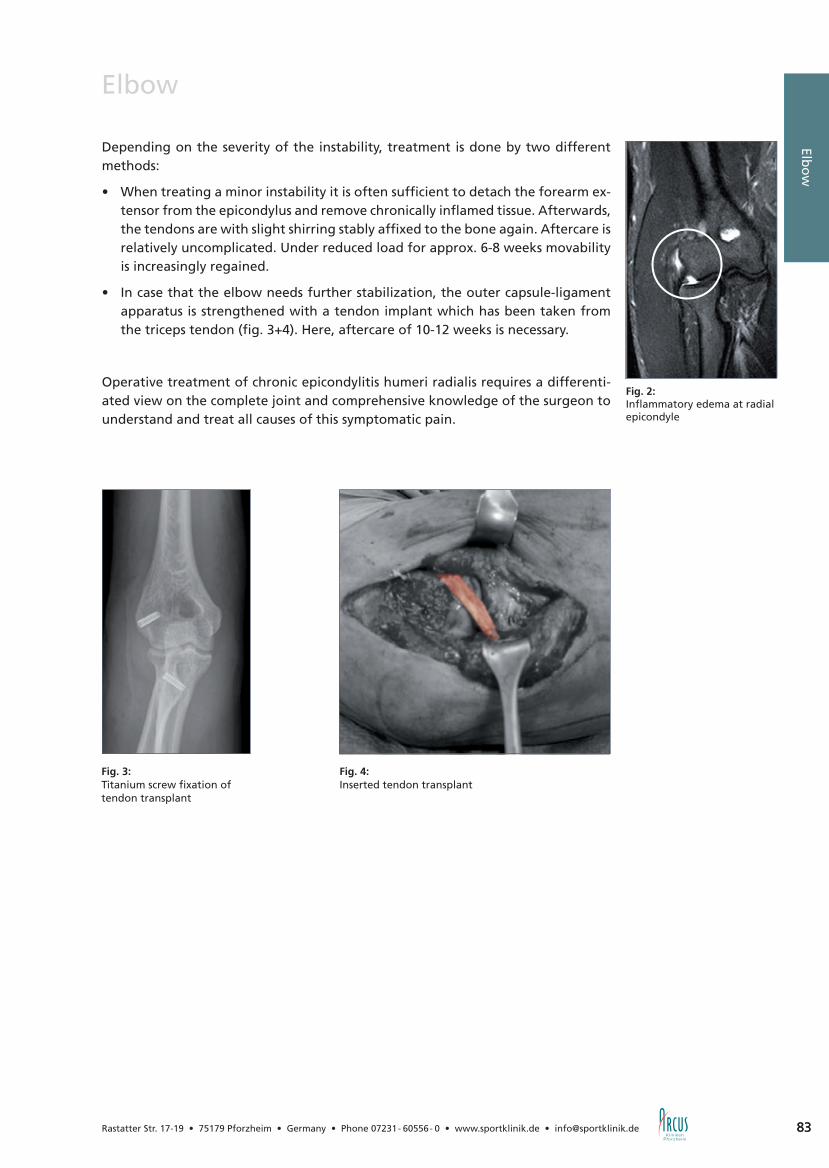
83
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Fig. 2: Inflammatory edema at radial epicondyle
83
Elbow
Depending on the severity of the instability, treatment is done by two different methods:
• When treating a minor instability it is often sufficient to detach the forearm ex-tensor from the epicondylus and remove chronically inflamed tissue. Afterwards, the tendons are with slight shirring stably affixed to the bone again. Aftercare is relatively uncomplicated. Under reduced load for approx. 6-8 weeks movability is increasingly regained.
• In case that the elbow needs further stabilization, the outer capsule-ligament apparatus is strengthened with a tendon implant which has been taken from the triceps tendon (fig. 3+4). Here, aftercare of 10-12 weeks is necessary.
Operative treatment of chronic epicondylitis humeri radialis requires a differenti-ated view on the complete joint and comprehensive knowledge of the surgeon to understand and treat all causes of this symptomatic pain.
Fig. 3: Titanium screw fixation of tendon transplant
Fig. 4: Inserted tendon transplant
Elbo
w
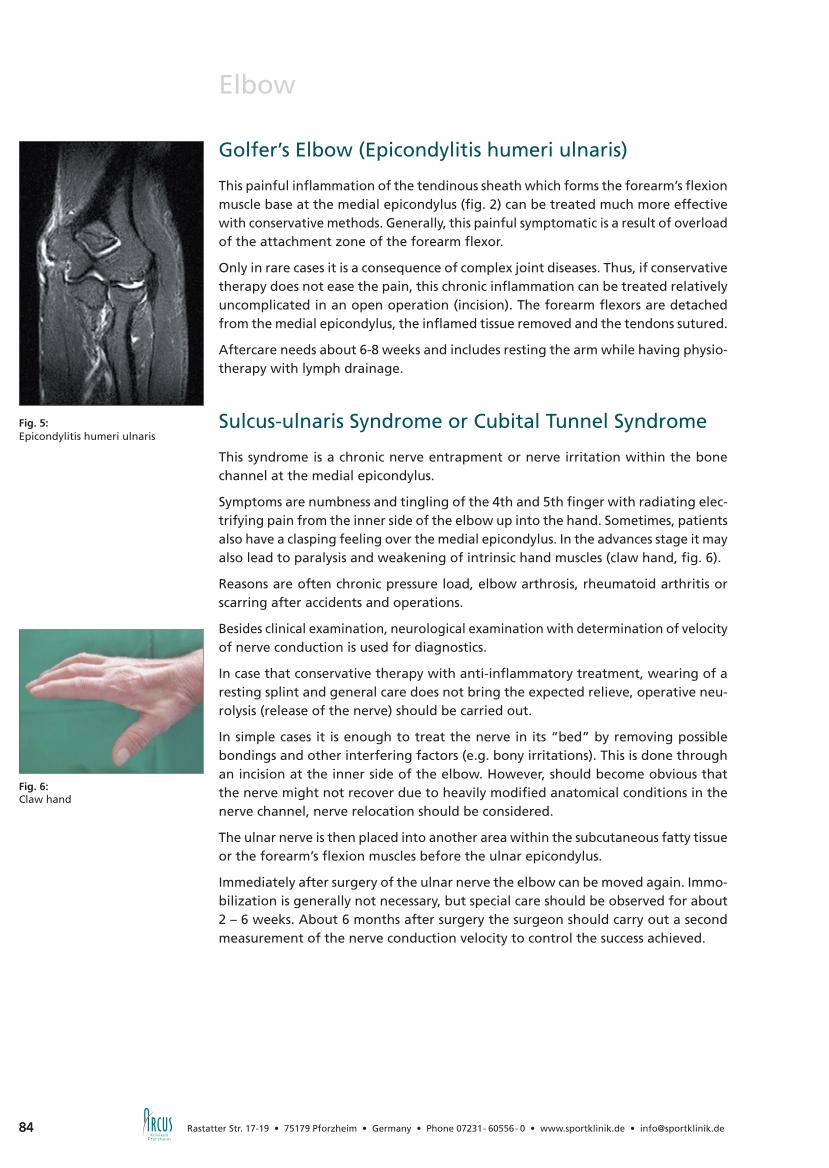
84 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Elbow
Fig. 6: Claw hand
Golfer’s Elbow (Epicondylitis humeri ulnaris)
This painful inflammation of the tendinous sheath which forms the forearm’s flexion muscle base at the medial epicondylus (fig. 2) can be treated much more effective with conservative methods. Generally, this painful symptomatic is a result of overload of the attachment zone of the forearm flexor.
Only in rare cases it is a consequence of complex joint diseases. Thus, if conservative therapy does not ease the pain, this chronic inflammation can be treated relatively uncomplicated in an open operation (incision). The forearm flexors are detached from the medial epicondylus, the inflamed tissue removed and the tendons sutured.
Aftercare needs about 6-8 weeks and includes resting the arm while having physio-therapy with lymph drainage.
Sulcus-ulnaris Syndrome or Cubital Tunnel Syndrome
This syndrome is a chronic nerve entrapment or nerve irritation within the bone channel at the medial epicondylus.
Symptoms are numbness and tingling of the 4th and 5th finger with radiating elec-trifying pain from the inner side of the elbow up into the hand. Sometimes, patients also have a clasping feeling over the medial epicondylus. In the advances stage it may also lead to paralysis and weakening of intrinsic hand muscles (claw hand, fig. 6).
Reasons are often chronic pressure load, elbow arthrosis, rheumatoid arthritis or scarring after accidents and operations.
Besides clinical examination, neurological examination with determination of velocity of nerve conduction is used for diagnostics.
In case that conservative therapy with anti-inflammatory treatment, wearing of a resting splint and general care does not bring the expected relieve, operative neu-rolysis (release of the nerve) should be carried out.
In simple cases it is enough to treat the nerve in its “bed” by removing possible bondings and other interfering factors (e.g. bony irritations). This is done through an incision at the inner side of the elbow. However, should become obvious that the nerve might not recover due to heavily modified anatomical conditions in the nerve channel, nerve relocation should be considered.
The ulnar nerve is then placed into another area within the subcutaneous fatty tissue or the forearm’s flexion muscles before the ulnar epicondylus.
Immediately after surgery of the ulnar nerve the elbow can be moved again. Immo-bilization is generally not necessary, but special care should be observed for about 2 – 6 weeks. About 6 months after surgery the surgeon should carry out a second measurement of the nerve conduction velocity to control the success achieved.
Fig. 5: Epicondylitis humeri ulnaris

85
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 85
Elbo
w
Fig. 7: Removal of loose joint body
loose joint body
Loose Joint Bodies
Symptoms are clear. It generally is a sensation of entrapment with limitation of movability, a painful joint, grinding and cracking.
Loose joint bodies (fig. 7) are usually the result of an already existing disease such as arthrosis (loss of cartilage with damage of the joint), Osteochondrosis dissecans (circulatory disorder of a bone area with loss of cartilage), instabilities, synovial chondromatosis (formation of cartilaginous bodies within the synovial membrane) or the consequence of an accident.
In most cases conservative therapy would not bring the result expected as loose joint bodies form a higher risk of irreparable consequential damages to the joint cartilage.
In order to not only ease pain but also retain the joint it is recommendable to remove those loose joint bodies with arthroscopic surgery (minimally-invasive camera tech-nique). If necessary, the real cause for the disorder can be treated at the same time.
Osteochondrosis Dissecans or Aseptic Bone Necrosis (Morbus Panner)
This disease mostly occurs with active and sportive children/teens and rather with boys than with girls. It is a circulatory disorder of the humerus near the joint surface of the radial head. Most obvious symptom is load-dependent pain, and depending on the stage of the disease also the sensation of entrapment and limitation of mo-vability. This circulatory disorder of the bone leads to displacement of its cartilage layer what in turn results in further consequences (as with loose joint bodies). The best prognosis is given when the disease is recognized at an early stage. By redu-cing pressure load and resting the elbow, a pain-free condition can be achieved and rejection of the cartilage prevented. However, should the disease already be in an advanced stage with (partial-) displacement of cartilaginous tissue, good results can better be achieved with arthroscopic surgery by drilling the affected area and
carrying out an appropriate cartilage therapy (fig. 8+9).
Elbow
Fig. 8: Drilling of damaged cartilage bone area
Fig. 9: Cartilage therapy by microfracture surgery after removal of loose joint body

86 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Stiff Elbow and Elbow Arthrosis
Mobility limitations of the elbow are either the result of changed soft tissue condi-tions or bony, mechanical barriers. In most cases it is a combination of both. Reasons for these movement restrictions may be accidents and their consequences (e.g. step joints with resulting joint degeneration, loose joint bodies, adhesions within the joint, scarring after operations) or a “normal” arthrosis (wear and tear of joint cartilage and bony sections of the joint). But limitation can also occur without vi-sible radiological changes. In these cases limitation is mostly caused by adhesions within the joint (arthrofibrosis) with an additional shortening/shrinkage of the joint capsule. Depending on the form of elbow stiffness, conservative therapy may be enough to increase mobility again. Useful may be manual therapy with physical
exercise, anesthesiologic methods such as local pain catheters, or usage of special mobilizing splints. In most cases however (depending on discomfort and level of limitation) the joint needs operative treatment (open or arthroscopic) in order to regain a satisfactory level of mobility.
The aims of arthrolysis (operative loosening of adhesions - possible in arthrosco-pic or open surgery) are restoration of mobility and furthermore improvement of joint mechanics. Thus depending on the diagnosis, disturbing bone spurs and loose joint bodies are removed, the cartilage surface smoothed, adhesions mobilized and shortened joint capsules cut. With this, pain is considerably reduced, often even eliminated. And the long-term prognosis is noticeably improved.
With completely destroyed joints or after exhausted joint-preserving therapy, the elbow can also be replaced by an artificial joint/prosthesis.
86
Elbow
Fig. 10-12: Before and after joint cleansing of an arthritic joint
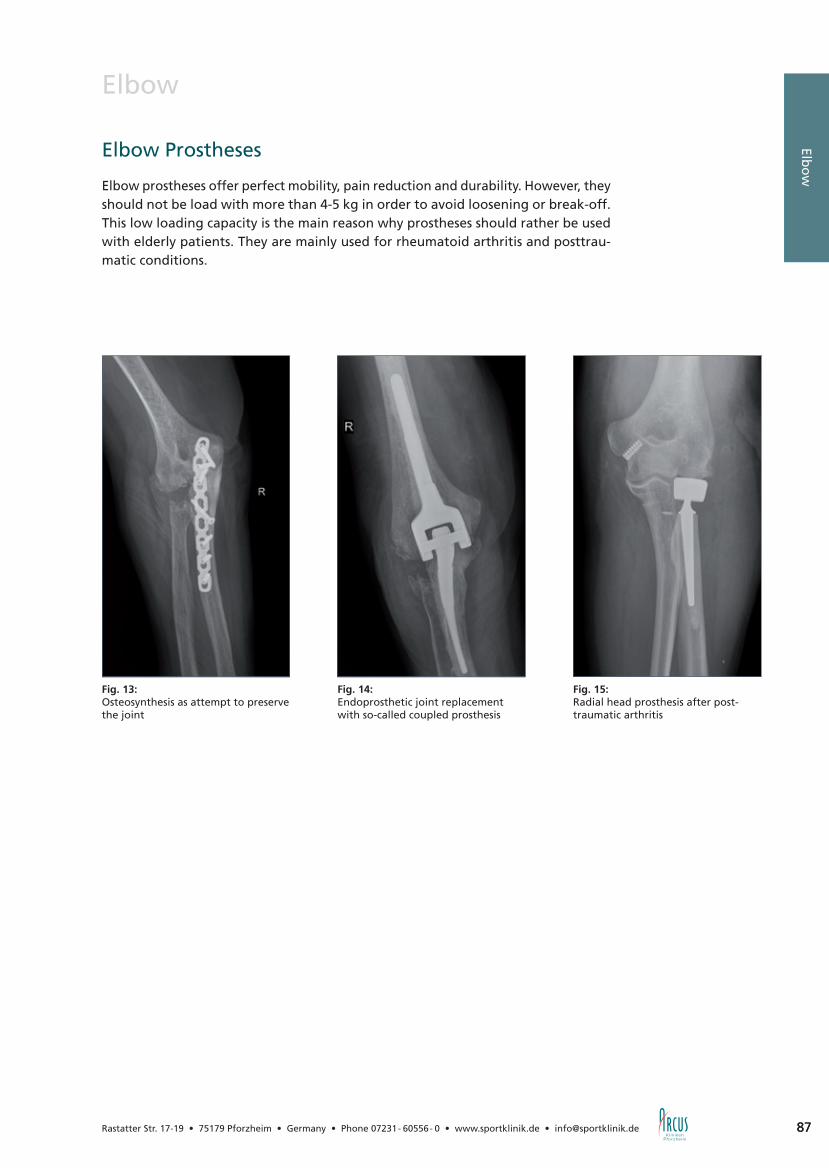
87
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 87
Elbo
w
Elbow
Elbow Prostheses
Elbow prostheses offer perfect mobility, pain reduction and durability. However, they should not be load with more than 4-5 kg in order to avoid loosening or break-off. This low loading capacity is the main reason why prostheses should rather be used with elderly patients. They are mainly used for rheumatoid arthritis and posttrau-matic conditions.
Fig. 13:Osteosynthesis as attempt to preserve the joint
Fig. 14:Endoprosthetic joint replacement with so-called coupled prosthesis
Fig. 15:Radial head prosthesis after post-traumatic arthritis
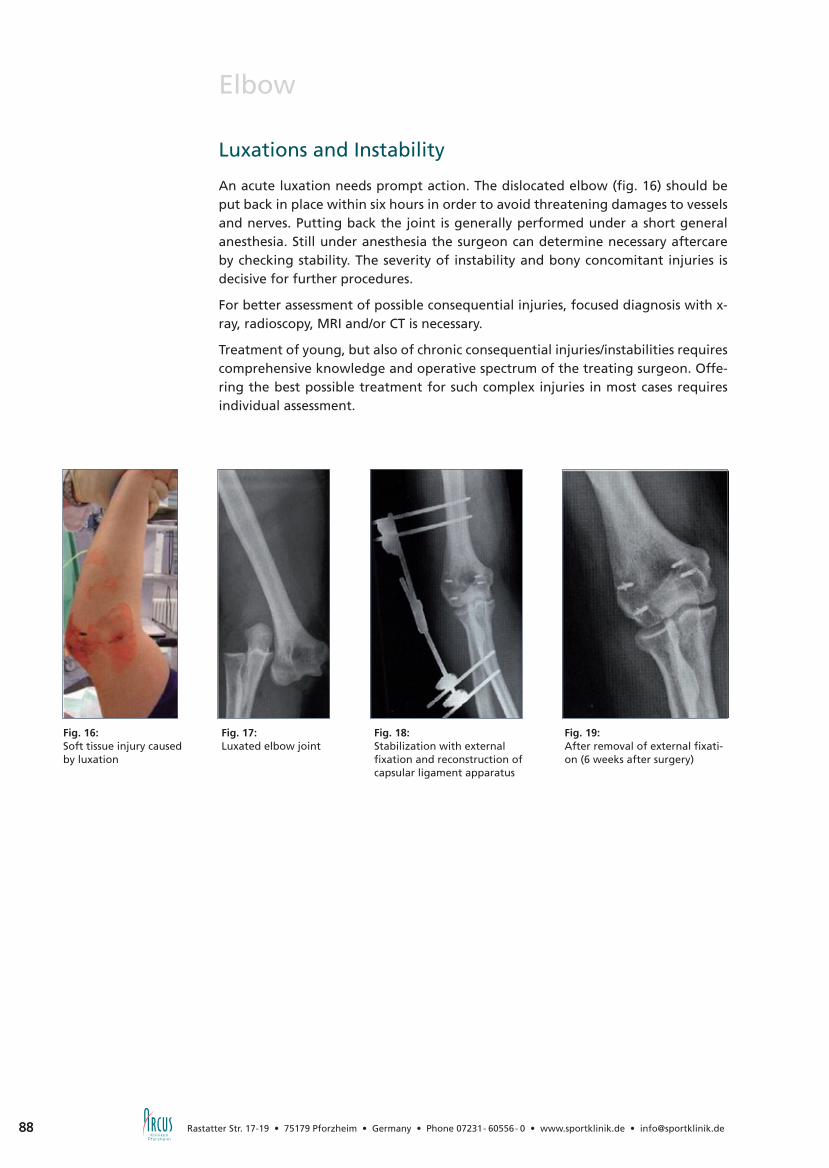
88 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Elbow
Fig. 16: Soft tissue injury caused by luxation
Fig. 17: Luxated elbow joint
Fig. 18: Stabilization with external fixation and reconstruction of capsular ligament apparatus
Fig. 19: After removal of external fixati-on (6 weeks after surgery)
Luxations and Instability
An acute luxation needs prompt action. The dislocated elbow (fig. 16) should be put back in place within six hours in order to avoid threatening damages to vessels and nerves. Putting back the joint is generally performed under a short general anesthesia. Still under anesthesia the surgeon can determine necessary aftercare by checking stability. The severity of instability and bony concomitant injuries is decisive for further procedures.
For better assessment of possible consequential injuries, focused diagnosis with x-ray, radioscopy, MRI and/or CT is necessary.
Treatment of young, but also of chronic consequential injuries/instabilities requires comprehensive knowledge and operative spectrum of the treating surgeon. Offe-ring the best possible treatment for such complex injuries in most cases requires individual assessment.
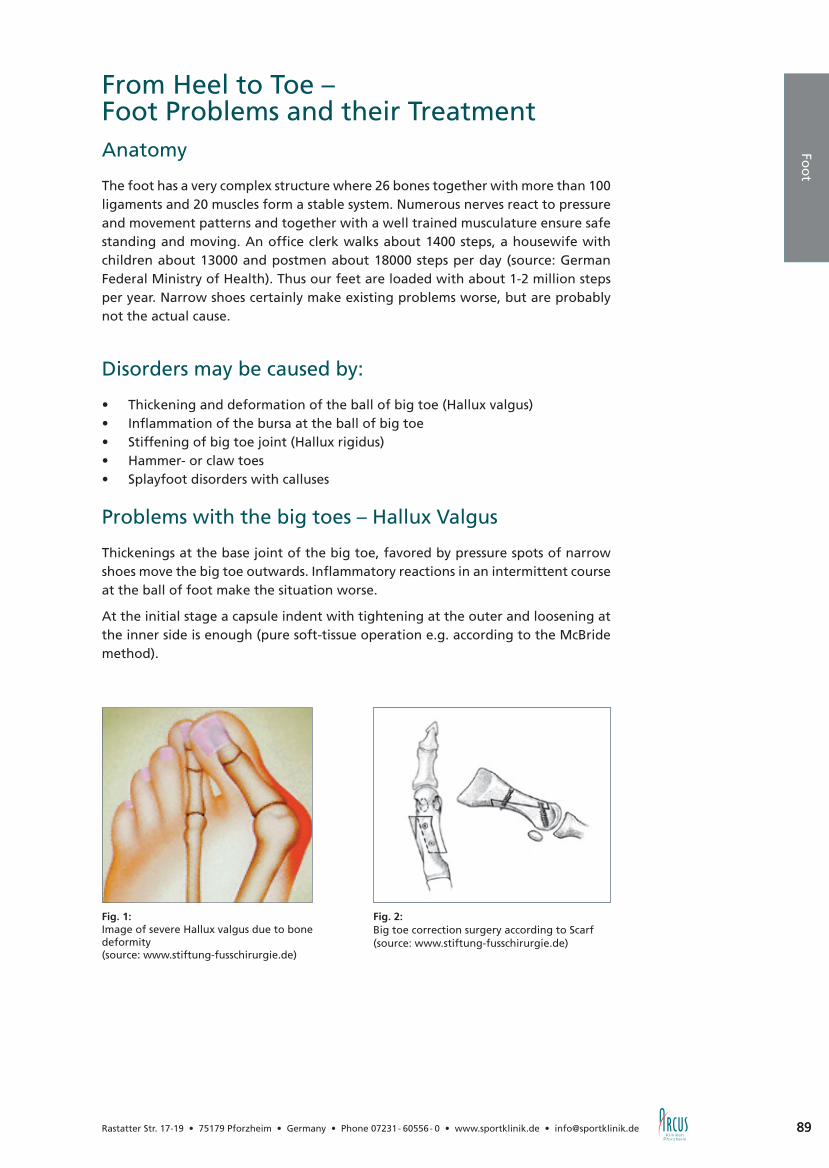
89
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 89
Foo
t
From Heel to Toe – Foot Problems and their TreatmentAnatomy
The foot has a very complex structure where 26 bones together with more than 100 ligaments and 20 muscles form a stable system. Numerous nerves react to pressure and movement patterns and together with a well trained musculature ensure safe standing and moving. An office clerk walks about 1400 steps, a housewife with children about 13000 and postmen about 18000 steps per day (source: German Federal Ministry of Health). Thus our feet are loaded with about 1-2 million steps per year. Narrow shoes certainly make existing problems worse, but are probably not the actual cause.
Disorders may be caused by:
• Thickening and deformation of the ball of big toe (Hallux valgus) • Inflammation of the bursa at the ball of big toe• Stiffening of big toe joint (Hallux rigidus) • Hammer- or claw toes • Splayfoot disorders with calluses
Problems with the big toes – Hallux Valgus
Thickenings at the base joint of the big toe, favored by pressure spots of narrow shoes move the big toe outwards. Inflammatory reactions in an intermittent course at the ball of foot make the situation worse.
At the initial stage a capsule indent with tightening at the outer and loosening at the inner side is enough (pure soft-tissue operation e.g. according to the McBride method).
Fig. 2: Big toe correction surgery according to Scarf(source: www.stiftung-fusschirurgie.de)
Fig. 1:Image of severe Hallux valgus due to bone deformity(source: www.stiftung-fusschirurgie.de)

90 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
From Heel to Toe – Foot Problems and their TreatmentTo treat severe malpositioning of the big toe, the bone needs correcting surgery too; and there are numerous methods to do so. The formerly common method which even today is still practiced in some cases, to simply resect the base joint of the big toe (method according to Keller-Brandes) should only be used in exceptional cases. There are more modern proven possibilities to preserve the toe’s base joint such as surgery according to Chevron or Kramer when treating moderate cases or Scarf and Hackenbroich when treating severe cases.
Aftercare is normally carried out without wearing a plaster. With a so-called fore-foot relief shoe or a vacuum shoe (e.g. Vacopedes) even careful walking is possible.
Fig. 3-4:X-ray images before and after correction surgery of severe deformity of big- and little toe(source: DePuy)

91
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 91
From Heel to Toe – Foot Problems and their TreatmentBig Toe Arthritis
Hallux rigidus
After accidents or chronic overload (e.g. by several sprains from playing football) joint wear within the base joint of the big toe can result in painful limitation to mobility. First remedy brings a stiff inlay with dispensing aid at the soles. Recommen-dation as regards the operation method is still stiffening the big toe’s base joint, as pain-free and normal loading capacity can be achieved without bigger long-term consequences. In case that bony prominences are disturbing and arthritis is not in a so far advanced stage, operative joint cleansing and if necessary slight shortening may help for some time. Small artificial toe joints are another option, but they do not bring back satisfactory full loading capacity in every case.
Problems with the small toesHammer Toes
Unequal muscle drawing results in distortion of one or several of the small toes. Pressure points develop at the raised middle joint as well as at the tiptoe and under the metatarsal head. In the initial stage when the distortion can still be corrected, wearing inlays is often sufficient.
When treating a contracted malposition, the head of the base joint is removed (surgery method according to Hohmann) to form a replacement joint. Aftercare is normally carried out without wearing a plaster. Walking with a so-called forefoot relief shoe is possible. Modern operation techniques preserve the metatarsopha-langeal joint (surgery method according to Weil) and ensure better pain reduction when rolling the forefoot (metatarsalgia).
Fig. 6:Pressure problems with hammer toe(source: www.stiftung-fusschirurgie.de)
Fig. 7:Repositioning of metatarsal headOperation method according to Weil (source: DePuy)
Fig. 5: Hallux rigidus after stiffening of big toe
Foo
t

92 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
From Heel to Toe – Foot Problems and their TreatmentMetatarsusFatigue Fracture
Too much load over a longer period such as jogging or long hiking trips may lead to hairline cracks in the bone which initially are not visible on normal x-ray images. The MRI helps making a diagnosis. Generally, treatment is done conservatively i.e. by pressure relief or a plaster-replacing shoe (e.g. Vacopedes).
Tarsus
Arthrosis
The small tarsal bones can develop the same signs of wear than bigger joints of our body. Artificial joint replacement however is not necessary, as with simple stiffening of the affected small bones satisfactory and pain-free loading capacity can be res-tored without triggering functional limitations. After such a stiffening operation, walking on crutches is necessary for some weeks. But in many cases, full loading and thus walking with removable plaster-replacing shoe (e.g. Vacopedes) is possible after about 4 weeks.
Bone Circulation Disorders (aseptic bone necrosis)
The bone oedema syndrome has only been known for some years now. First disco-vered by MRI analyses, the main causes have still not been investigated in detail. Theories about what causes this disorder are overload, micro fractures, circulation disorders etc. (source: http://en.wikipedia.org/wiki/Aseptic_necrosis).
The patient feels load-dependent pain in the foot without finding a certain possible reason; in most cases there are no external signs. Causal therapy is - except for de-tected fatigue fractures - not known so far. Besides relieving measures such as rest, inlays, relief or immobilization, the therapeutic approach focuses on stimulation of blood circulation. There have been good healing results when treating cases in the initial stage with hyperbaric oxygen therapy, but public health insurance companies unfortunately are not offering any reimbursement options. Alternatively, there is a therapy method based on circulation-stimulating infusions (Iloprost) which also shows noticeable shortening of this painful and disabling course of disease. Ope-rative treatment is useful at a later stage (drilling of the affected bone area, near to joints also cartilage bone transplantations e.g. knee or Achilles joint up to joint replacement in severe cases).
Fig. 9: Cast replacement by removable vacuum support shoe(source: Oped GmbH, Vacopedes)
Fig. 8: Bone formation after fatigue fracture of metatarsal bone
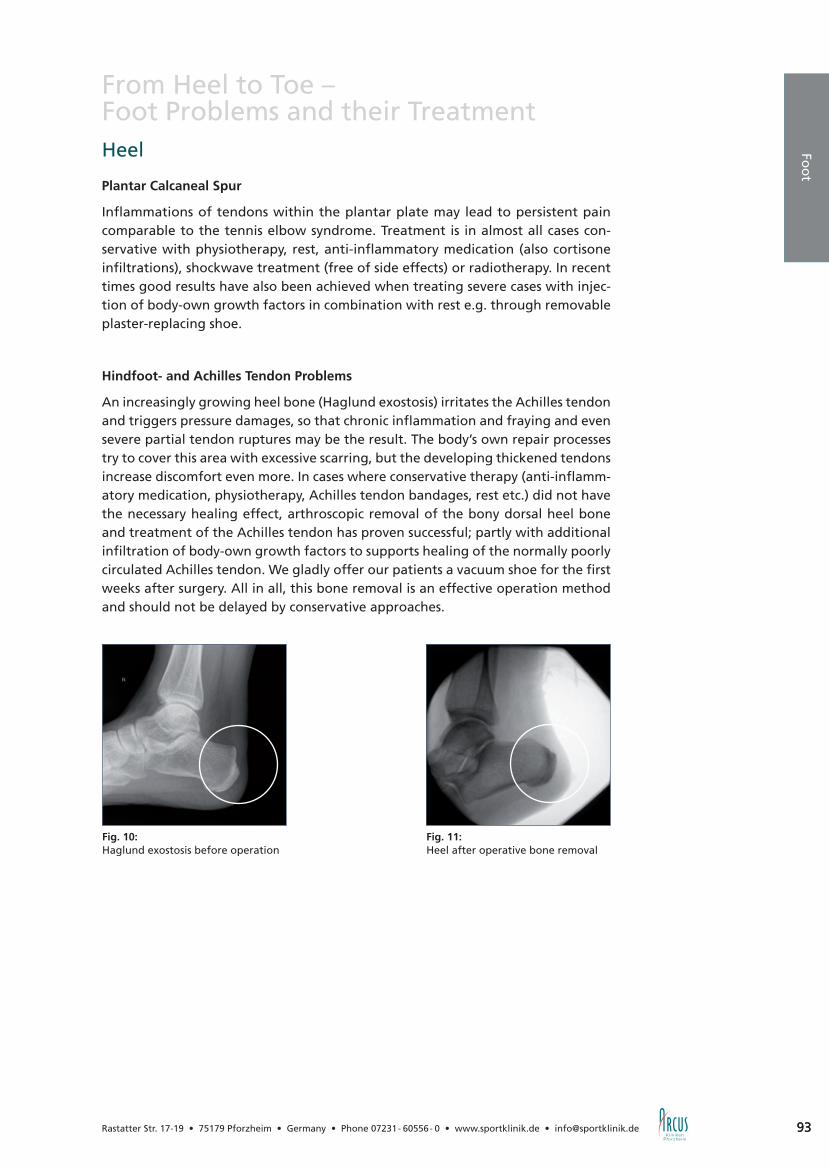
93
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 93
From Heel to Toe – Foot Problems and their TreatmentHeel
Plantar Calcaneal Spur
Inflammations of tendons within the plantar plate may lead to persistent pain comparable to the tennis elbow syndrome. Treatment is in almost all cases con-servative with physiotherapy, rest, anti-inflammatory medication (also cortisone infiltrations), shockwave treatment (free of side effects) or radiotherapy. In recent times good results have also been achieved when treating severe cases with injec-tion of body-own growth factors in combination with rest e.g. through removable plaster-replacing shoe.
Hindfoot- and Achilles Tendon Problems
An increasingly growing heel bone (Haglund exostosis) irritates the Achilles tendon and triggers pressure damages, so that chronic inflammation and fraying and even severe partial tendon ruptures may be the result. The body’s own repair processes try to cover this area with excessive scarring, but the developing thickened tendons increase discomfort even more. In cases where conservative therapy (anti-inflamm-atory medication, physiotherapy, Achilles tendon bandages, rest etc.) did not have the necessary healing effect, arthroscopic removal of the bony dorsal heel bone and treatment of the Achilles tendon has proven successful; partly with additional infiltration of body-own growth factors to supports healing of the normally poorly circulated Achilles tendon. We gladly offer our patients a vacuum shoe for the first weeks after surgery. All in all, this bone removal is an effective operation method and should not be delayed by conservative approaches.
Fig. 10: Haglund exostosis before operation
Fig. 11: Heel after operative bone removal
Foo
t

94 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Achilles Tendon Problems
Achillodynia
Achillodynia is the degeneration process of soft tissue in the centre of the poorly circulated Achilles tendon. The body’s own incomplete attempts to repair the da-mage lead to painful thickening of the tendons.
Main causes are: monotonous overload (painful running training especially with shortened Achilles tendon), overpronation (pes valgus) or other foot deformities, wearing too stiff soles or too much cushioned heels what results in the Achilles ten-don experiencing strong prestraining with every step, arthrosis-dependent uneven loading (knee, hip etc.).
Harmless in the initial stage, but very painful. Therapy is at first conservative with reduction of exercise load, check of running shoes and their cushioning, physiotherapy with instructions for stretching exercises, in some cases also kinetic tape. Individual inlays, especially after professional video-recorded walking-running analysis. Shock-wave therapy (public health insurance companies do not cover the costs so far) and also inflammation- and pain reducing therapy via x-ray or proton radiation. We also made good experiences with the injection therapy of body own growth factors (see chapter ortho-biology, page 44), while other infiltrations e.g. with cortisone should be used very carefully because of the danger of rupture of the tendon. In cases of therapy resistance, the degenerative thickening of the tendon is removed surgically.
New American approaches consider the mentioned hindfoot-, heel- and Achilles tendon problems and also their extensions to the metatarsus including forefoot deformities to be one single syndrome: the CT-band syndrome (calf-to-toe band, J. Oster 2009). Therefore, lower legs with calf musculature, Achilles tendon, plantar fascia, foot- and toe joints are regarded and treated together as one single unit.
Fig. 1: Achillodynia (left side with thickened tendon)
Fig. 2: Achillodynia with partial rupture of Achilles tendon

95
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Achilles Tendon Problems
Achilles Tendon Rupture
The complete rupture of the Achilles tendon is one of the most common sports in-juries, mostly occurring with males between 30 and 50. Treatment is here medically necessary as this injury otherwise results in a scarred extension of the tendon with sometimes considerable loss of power and gait disorders. Conservative treatment is possible as long as the tendon ends have not spread. Within the first 24 hours, a lower leg cast is applied (or a lower leg orthosis which has to be worn very conse-quently). Afterwards an individually adjusted lower leg walker has to be worn for 4 weeks; removable only at night and for body care. Complementary physiotherapeutic treatment is needed even longer. Among experts, advantages and disadvantages of such a conservative therapy are still controversial. We see better and above all faster positive results in immediate operative treatment with minimally invasive technique (small incisions, suture for initial hold of tendon fibers and accelerated healing process through injection of growth factors). Here, the patient is with appropriate orthoses capable of walking within 4-5 weeks in most cases.
Fig. 3:Minimally invasive Achilles tendon suture
Fig. 4:Injection of body-own growth factors (PRP)
Fig. 5:Closed wound
Foo
t

96 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Ankle Disorders and their Treatment
Anatomy
The ankle joint comprises the the true ankle joint (upper ankle joint) and the sub-talar joint (lower ankle joint). The latter is rarely affected by injuries and therefore discusses in association with ankle osteoarthritis. The upper ankle joint (UAJ) is the connection between the ground-contacting foot with the talus as lower portion of the joint and the tibia carrying the body weight which forms the upper joint surface together with the inner malleolus. Laterally lying we can see the fibula. This construction enables a sliding movement = flexion and extension and thus the power when walking or jumping. Stable ligaments prevent lateral tilting. At the inner malleoulus the broad and stable delta ligament, at the outer malleolus three considerably thinner ligaments from which the anterior- and medial collateral ligament are often partly or even completely ruptured when twisting one‘s ankle (supination trauma, distorsion).
Ligament Injuries
• Strain of ligaments and joint capsule, sprain (grade I) Treatment: ice, compressions, elevated resting, full loading possible after few
days.
• Partial rupture (grade II) Treatment: as grade I, additionally walking on crutches necessary for some days
and wearing of a stabilizing ankle brace (e.g. Aircast or Malleo-Tri-Step) for 2-4 weeks. Physiotherapy is recommended for improvement of coordination and muscular stabilization as prevention against new injuries.
• Ligament rupture (grade III). Treatment: as grade II, but with the joint being splinted for up to 6 weeks. With
severe instability even operative ligament suture.
• Chronic instability of lateral collateral ligament after repeated distortion. If phy-siotherapy, broadened heels and elastic bandages do not bring improvement, operative ligament surgery should be considered. When having a sufficiently stable and worn-out scar, it can be doubled and sutured again to tighten it (surgery according to Broström). Advantage: anatomic reconstruction. In case of a rupture of two ligaments or severe instability, strengthening of the ligaments has to be carried out by using additional material e.g. periosteum (periosteal flap surgery), tendons from the foot or recently also tendons from the knee. Advantage: very good stabilizing effect. Disadvantage: complex surgery, difficult anatomic positioning.
Complications of such operations: - Infections (less than 1%) - Slight movement restrictions (1-2%) - Sensory disturbances at the outer side of the foot - Insufficient stabilization
• Syndesmosis rupture: Rupture of the tight ligament connection between lateral malleolus and shinbone.
With proven rupture (by MRI), fixation with screw and walking on crutches for 6 weeks is necessary.
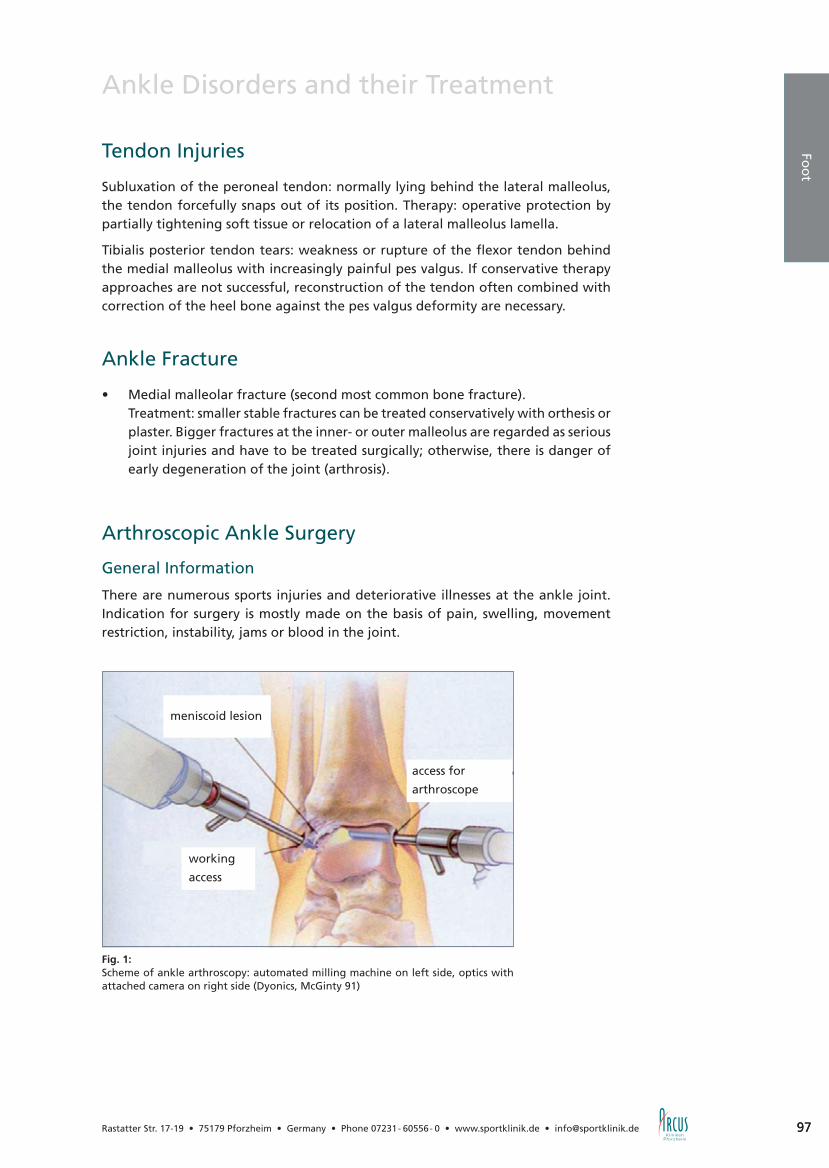
97
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 97
Ankle Disorders and their Treatment
Tendon Injuries
Subluxation of the peroneal tendon: normally lying behind the lateral malleolus, the tendon forcefully snaps out of its position. Therapy: operative protection by partially tightening soft tissue or relocation of a lateral malleolus lamella.
Tibialis posterior tendon tears: weakness or rupture of the flexor tendon behind the medial malleolus with increasingly painful pes valgus. If conservative therapy approaches are not successful, reconstruction of the tendon often combined with correction of the heel bone against the pes valgus deformity are necessary.
Ankle Fracture
• Medial malleolar fracture (second most common bone fracture). Treatment: smaller stable fractures can be treated conservatively with orthesis or
plaster. Bigger fractures at the inner- or outer malleolus are regarded as serious joint injuries and have to be treated surgically; otherwise, there is danger of early degeneration of the joint (arthrosis).
Arthroscopic Ankle Surgery
General Information
There are numerous sports injuries and deteriorative illnesses at the ankle joint. Indication for surgery is mostly made on the basis of pain, swelling, movement restriction, instability, jams or blood in the joint.
Fig. 1: Scheme of ankle arthroscopy: automated milling machine on left side, optics with attached camera on right side (Dyonics, McGinty 91)
Foo
t
meniscoid lesion
access for
arthroscope
working
access
98 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Ankle Disorders and their Treatment
Arthroscopic Ankle Surgeries
• Consequential damages after dislocations with stress pain, instability or blockages through loose joint bodies are the most common causes. Furthermore inflam-mations of the synovial membrane, adhesions and scarrings with movement restrictions (arthrofibrosis) and limitations to mobility as a result of entrapped scar tissue (meniscoid syndrome) can be treated successfully.
• Protruding osteophytes at the front side of tibia and talus are especially with ball players and dancers a common cause for pain, swelling and movement restriction. Arthroscopic removal of these osteophytes is a promising and well-proven treatment option.
• When suffering from joint cartilage damage, a cartilage treatment similar to the one at the knee joint can be carried out. In most cases, the damaged car-tilage is carefully removed, smoothed and the underlying bone brushed up in order to stimulate fibrocartilage regeneration. In rare cases treatment includes transplantation of donor cartilage.
Major Ankle Surgeries
Deep cartilage defects with underlying bone defects are called Osteochondritis diss-ecans (OD). They occur mostly at the inner side of the talus which is very difficult to reach, and causes are severe distortions, chronic instabilities or circulatory disorders of the bone. They are divided into four grades:
• Grade I: Bone oedema, circulatory disorder without changes in the bone struc-ture, intact cartilage layer.
Treatment: rest, use of crutches, circulation stimulating measures (hyperbaric oxygen therapy HBOT or iloprost injections, see chapter foot, p. 89). In case of persisting progression, the affected area can be drilled from the rear side under arthroscopic control.
• Grade II: beginning demarcation, displacement of a mostly oval-shaped cartilage bone fragment, in most cases still intact cartilage layer, but sometimes partly frayed. This lesion is potentially instable and reaches grade III soon without treatment. Thus, either early and consequent conservative treatment with rest for a longer period or surgical treatment is necessary.
• Grade III: the cartilage bone fragment has detached completely from the talus bone but still lies in its „mouse bed“. This condition does not heal by itself. For therapy please refer to stage IV.
• Grade IV: The cartilage bone fragment has broken off the bone and as loose joint body causes additional damages by interfering with the joint.
There is only one option: surgical treatment. In favorable cases refixation of the fragment, otherwise simple removal of the fragment and stimulation of self-healing (mostly possible without removal of inner malleolus, but then with reduced chances of fast healing). Another promising method is cartilage bone transplantation: a healthy cylinder-shaped piece of cartilage bone is taken from the knee and transplanted into the defect area of the talus. Here, the inner

99
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 99
Ankle Disorders and their Treatment
malleolus has to be removed in order to reach the affected area; it is affixed with screws afterwards.
Advantage: load stable condition within 5-6 weeks. Complete surgery possible in one session. Public health insurance companies cover the costs of this operation method.
Disadvantage: Transplant has to be extracted from the knee.
Alternative possibility: autologous chondrocyte transplantation (ACT) = cultivation and transplantation of the body’s own cartilage cells (see chapter arthrosis, p. 36).
Advantage: high-tech procedure with best chances for development of new load-stable hyaline cartilage. No additional injury at the donor site. By using recent tech-nologies of spheroid ACT even detachment of the inner malleolus can be avoided.
Disadvantage: expensive (public insurance companies cover the costs only to a li-mited extent; mostly clinics are allowed only a limited number of ACT-operations. Surgically challenging. This method is only appropriate for flat defects; otherwise the bone defect has to be filled up when removing the cells. Normally, two surgical steps are needed (first cell extraction for cultivation and later transplantation). In some cases however, after verification of the diagnosis and indication, approval of cost transfer has to be obtained from the health insurance company first before cell removal and transplantation afterwards can be carried out. Here, bureaucracy makes 3 surgical steps inevitable.
Foo
t

100 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Ankle Disorders and their Treatment
Besides the information given, please also note the following:
Prior to operation
Do not put your joint under unnecessary strain; this might extend your recovery period after the operation. If necessary train walking on crutches.
Arrange treatment dates with your physiotherapist or masseur, beginning about 1-2 days after the operation. For further information about a planned operation please refer to chapter anesthesia from page 18.
Aftercare
With most ankle joint surgery patients an extended program for postoperative care is arranged. Special details of aftercare are mentioned in the operation record. Generally applies:
Do not put full weight on the foot the first days after surgery and rest your foot in an elevated position. Until completed wound healing (5-10 days) support your foot by walking on crutches. Cool the joint with dry ice-pack several times a day for approx. 15 min.
Movement and Drainage
After rest of 2-3 hours get up and walk a few steps. By activating the lower leg mu-sculature you can help preventing thrombosis best. In case that the small drainage bottle becomes filled, please do not worry and leave it alone. Under no circumstances empty the bottle, nothing will happen.
Dressing Change and Aftercare
The day after surgery please visit us for change of dressing. The next change after 2-3 days can be carried out from your referring specialist or family doctor.
Taking a shower is possible after 1 week; removal of stitches is done approx. 14 days after surgery. Full loading is permitted after 5-10 days in most cases. Please carefully read the chapter „Aftercare“ of your operation record which serves as information for you and for other physicians as well as physiotherapists dealing with the case.
We kindly ask you to arrange a follow-up examination after 3 weeks and in some cases again after 3 months.

101
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 101
I D E E N B E W E G E N .
© O
RMED
.DJO
08/
09
www.ormed-djo.de
AIRCAST® AIRGO™■ ATF-Zugband zur einstellbaren Limitierung in Pro- und Supination■ hohe Stabilität und einfachste Handhabung
IMMER EINEN SPRUNG VORAUS
Hotline: 0180 1 676 333
3438_08_aircast_185x135 1 07.08.09 19:29
Foo
t

102 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Neurosurgery / Spinal Column
General Information
With increasing age occur signs of wear and tear at intervertebral discs and spinal joints. Damages of the disc tissue are due to most different reasons as herniated discs are usually the result of accidents or other unforeseeable events. The interver-tebral disc consists of a hard fibrous ring and a softer inner part. The disc tissue is not supplied by blood vessels; supply is ensured only through diffusion, a complex system of suction- and pressure effect of the vessels surrounding the spinal column and the spinal canal.
If the water content of the intervertebral disc declines, it loses its shock absorbing effect and shrinks what can clearly be seen in MRT. Its height is visibly reduced and the MRT signal shows lower water content. By increasing wear and tear the disc finally loses its elasticity and protrudes; and the fibrous ring is forcefully stretched – what causes heavy back pain. Of course, this situation may recede, but in most cases the increasing wearing down of the intervertebral disc and the pressure from within onto the fibrous ring result in small tears through which the gelatinous portion of the disc tissue is being squeezed out (sequestration). By squeezing onto nerves or the spinal cord within the spinal canal, this leaked disc tissue can cause heavy pain and even neurological deficits such as paralysis, changes in sensation or bladder-gastrointestinal disorders.
A previously damaged disc cannot offer the same shock absorbing effect than a healthy one. All these degenerative changes result in the vertebral bodies being moved together and stressed excessively. Osteochondrosis as the result of this con-dition is also perfectly visible in MRT. Due to the chronic overload of the vertebral bodies with low spondylolisthesis further signs of degeneration occur (facet joint arthrosis). Bony and cartilaginous protrusions lead to narrowing of the nerve chan-nels (foraminal stenosis) and the spinal channel (spinal stenosis). Both degenerative narrowing conditions with chronic pressure lead to stress-dependent pain and after longer duration also to neurological deficits.

103
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 103
Neu
rosu
rgery / Sp
inal C
olu
mn
Neurosurgery / Spinal Column
Cervical Spine (CS)
Die Halswirbelsäule (HWS) mit insgesamt 7 Wirbelkörpern ist der beweglichste Wirbelsäulenabschnitt und stellt die mobile Verbindung zwischen dem Kopf und der restlichen Wirbelsäule her. Aus dieser Bewegungsfunktion resultieren die unterschiedlichen Probleme bei degenerativen (verschleißbedingten) und trauma-tischen (verletzungsbedingten) Erkrankungen. In der Halswirbelsäule liegt direkt hinter den Bandscheiben das Rückenmark, sodass aus dieser engen Lagebeziehung viele Probleme entstehen. Degenerative Halswirbelsäulenerkrankungen kommen gehäuft auch bei jüngeren Menschen vor. Klinisch-neurologisch muss man zwischen radikulären (Kompression der Nervenwurzeln) und medullären (Kompression des Rückenmarks) Symptomen und Defiziten unterscheiden. Ein Druck auf das Rücken-mark muss nicht immer Schmerzen verursachen, ist jedoch ein langfristiges Problem, da die Schädigung der Rückenmarksbahnen langsam fortschreitende Störungen mit Gleichgewichtsstörungen, Gangunsicherheit und schleichender Querschnittsympto-matik verursachen (cervikale Myelopathie).
Degenerative Osteochondrosis
Cause
Is wear and tear or a gradual restructuring process with degeneration of the inter-vertebral disc and protrusions or extensions of the vertebral bodies. This bone- and connective tissue growth results in nerve- or spinal cord compression. Generally it can be said that pain cannot be treated satisfactorily with conservative therapy.
Symptoms
Are often chronic pain in neck and back of the head or pain radiating to shoulder, arm and fingers. Depending on the nerve affected and the dimension of this nerve entrapment symptoms may also be lack of force, paralysis and changes in sensation.
Diagnosis
Is made by neurologic examinations as well as special examinations of the spinal column; in individual cases also by electrophysiological measurements. X-ray ima-ges of the cervical spine and sometimes so-called functional images are necessary. Moreover, a CT and/or a MRT should be carried out. In rare cases even a cervical myelography for further invasive diagnostics is necessary.
Therapy
In case that no neurologic deficits occur, primary aim should be conservative therapy with intensive physiotherapy and pain medication. If no adequate improvement can be achieved, indication for operative measures should be checked and discussed new. Here, individual advice and definition of the optimally suitable surgery method are of decisive importance.

104 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Neurosurgery / Spinal Column
Operation Method
Minimally-invasive technique (under local anesthesia):periradicular infiltration (PRI) – radiologically controlled facet infiltration
When treating with periradicular infiltration (PRI) and the radiologically controlled facet infiltration a mixture of local anesthetic and a crystalloid corticoid preparation is used. After local anesthesia of the skin a thin cannula is inserted under radiological control directly to the point where the nerve exits the foramen and 1 – 2 ml of the medication injected. Under x-ray control, this medicine can also be applied into the small vertebral bodies near the cervical spine. Its local effectiveness requires only low dosages; the medication does only work directly at the site of action and degrades very slowly. However, in most cases there are several sessions necessary to achieve long-term freedom from pain.
Microsurgical Operations: Ventral discectomy with placeholder
Here, access is made via the front of the neck with complete removal of the da-maged disc. Decompression of nerve structures (nerve roots and spinal marrow) is made with the operating microscope. At the end a placeholder is inserted instead of the damage disc which has a re-erecting effect to the intervertebral disc space and relieves the neuroforamen; the development of osteophytes is prevented. Different materials such as polymer cement (PMMA) or synthetic cages (PEEK) are used. Only in rare and difficult cases with accompanying loosening of the mobile segment screwing together of the cervical spine and a titanium plate is necessary.
Ventral Foraminotomy
Here, access is also made via the front side of the neck to open up the nerve chan-nel. Compared to ventral discectomy however, preservation of the disc is possible.
Dorsal microsurgical techniques:Foraminotomy, Laminectomy, Laminoplastics
With dorsal foraminotomy, a bony entrapped nerve root can be decompressed by removing the osteophytes. A sole laminectomy with complete removal of the ver-tebral arch offers a good possibility to relieve the spinal cord. However there is the risk of instability afterwards and so it is used only rarely or in combination with a stabilizing procedure. Laminoplastics with dorsal extension and reconstruction of the spinal canal is another possibility to treat cervical myelopathy when suffering from cervical spinal canal stenosis. This method is especially promising when treating an ossification of the posterior longitudinal ligament.
105
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 105
Neurosurgery / Spinal Column
Aftercare
Directly after surgery the patient starts with mobilizing exercises. After microsur-gical operations at the cervical spine there are no noticeable limitations to sitting, lying or walking, and even wearing of a neck collar is not necessary. The in-patient stay at the hospital normally lasts 2-3 days. The following week start physiotherapy and further conservative measures. As regards other activities after a cervical spine surgery we would be pleased to give you individual advice.
Disc Herniation
Cause
Due to degeneration of the intervertebral disc there sometimes occur tears in the fibrous ring through which the inner gelatinous portion of the disc is squeezed out. The possible resulting pressure onto nerves or the spinal cord causes pain and neurologic deficits.
Symptoms
Acute neck pain and heavily radiating pain to arms and fingers with the feeling of weakness and numbness or other abnormal sensations. With severe neurological deficits such as paralysis, changes in sensation or bladder-gastrointestinal disorders, immediate operation may be necessary in individual cases.
Diagnosis
Diagnosis is made with neurologic examinations and special examinations of the spinal column; if necessary also electrophysiological measurements. Moreover, X-ray images of the cervical spine with functional images as well as a current MRT are needed.
Therapy
Without obvious neurological deficits, conservative therapy should be the first choice. Treatment comprises pain medication and if necessary immobilization with neck brace. After the acute phase starts intensive physiotherapy. In case that conser-vative therapy does not bring the required result, indication for operative measures should be checked and discussed new. Here, individual advice and definition of the optimal time of operation as well as the optimally suitable operation method is of decisive importance.
Operation Method
Ventral microsurgical discectomy with placeholder
Here, access is made via the front of the neck with complete removal of the damaged disc. Decompression of nerve structures (nerve roots and spinal marrow) is made with the operating microscope. At the end a placeholder is inserted instead of the damage disc which has a re-erecting effect to the intervertebral disc space and re-lieves the neuroforamen; the development of osteophytes is prevented. Different materials such as polymer cement (PMMA) or synthetic cages (PEEK) are used.
Neu
rosu
rgery / Sp
inal C
olu
mn

106 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Neurosurgery / Spinal Column
Ventral microsurgical discectomy with artificial intervertebral disc
With younger patients with a mobile and only slightly damaged disc, preservation of the mobile segment can be achieved by implanting a disc prosthesis after micro-surgical removal of the real disc.
Dorsal microsurgical foraminotomy
With dorsal foraminotomy small and outwards situated soft herniated discs can be removed and the entrapped nerve root decompressed.
Aftercare
Directly after microsurgical operation mobilization is recommended. Drainages are only inserted in exceptional cases and the patient normally does not have to wear a neck brace. The in-patient stay lasts normally 2-3 days. In the week following the surgery physiotherapy and further conservative measures are started.
Cervical Myelopathy
Cause
Cervical myelopathy is a gradual wearing process with degeneration of the disc. Developing bony protrusions (osteophytes) narrow the spinal canal at the cervical spine and thus lead to compression of the spinal cord.
Symptoms
In many cases occurs chronic pain in neck and back of the head, but often this does only pose little discomfort. However, even if not very strong - the permanent pres-sure onto the spinal cord results in the medium term in irreversible damages to the spinal cord and therefore poses respective risks.
Diagnosis
Is made by neurologic examinations as well as special examinations of the spinal column; in individual cases also by electrophysiological measurements. X-ray images of the cervical spine and sometimes so-called functional images are necessary. Mo-reover, a CT and/or a MRT should be carried out whereby assessment of the MRT as regards possible signs in the spinal cord for myelopathy is of particular importance.
Therapy
With a manifest cervical myelopathy, conservative treatment is relatively promising.
Operation Method
Microsurgical ventral discectomy with placeholder
Here, access is made via the front of the neck with complete removal of the da-maged disc. Decompression of nerve structures (nerve roots and spinal marrow) is made with the operating microscope. At the end a placeholder is inserted instead of the damage disc which has a re-erecting effect to the intervertebral disc space and with this prevents the development of new osteophytes. Different materials such as polymer cement (PMMA) or synthetic cages (PEEK) are used.

107
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 107
Neurosurgery / Spinal Column
Microsurgical ventral decompression with removal of vertebral bodies and plate osteosynthesis
Access is made via the front of the neck. By means of an operation microscope the vertebral body (or bodies) and the adjacent discs are removed what creates a long relieving effect to the spinal cord. In order to re-stabilize the spinal column after-wards, implantation of a tricortical iliac crest bone grafting or a metal vertebral body replacement is necessary. Additionally a ventral plate osteosynthesis has to be carried out in order to ensure sufficient stability. However, this relatively complex operation method is rather rare.
Dorsal microsurgical decompression and laminoplastics
A microsurgical decompression is carried out in several stages. Here, the ligamenta flava and possible osteophytes are removed. Reconstruction of the spinal canal by laminoplastics is a preferred surgery method when treating very long cervical ste-noses especially with elderly patients.
Aftercare
Directly after surgery the patient starts with mobilizing exercises. After microsurgical operations at the cervical spine there are no noticeable limitations to sitting, lying or walking, and even wearing of a neck collar is not necessary. The in-patient stay at the hospital normally lasts 3-4 days. Only in rare cases and with previous neuro-logic deficits rehabilitation treatment is necessary. As regards other activities after a cervical spine surgery we would be pleased to give you individual advice.
Fractures
Cause
Acute or recent physical violence to the cervical spine with rupture of the ligament structures and fractures of the vertebral bodies, vertebral arches and vertebral joints. But fractures may also be the result of tumors, inflammations of the spinal column or osteoporosis.
Symptoms
Neck pain, headache and other discomfort near the whole spinal column. Further-more movement restrictions of the spinal column and various degrees of neurolo-gical deficits.
Diagnosis
Is made with a neurological examination and a special examination of the spinal column. Furthermore, X-ray images of the cervical spine as well as so-called func-tional images are necessary, and a CT and a MRT should be carried out. In rare cases nuclear medicine examinations are needed for further diagnostics.
Therapy
FIn case that no obvious instability or neurological deficits can be detected, treatment can be done conservatively. This includes stabilization by means of a neck brace and pain medication. After the acute phase controlled physiotherapy can be started. When treating fractures of the cervical spine offering individual advice regarding
Neu
rosu
rgery / Sp
inal C
olu
mn

108 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Neurosurgery / Spinal Column
indication to operation as well as choosing the most appropriate operation method is of decisive importance.
Operation Method
Microsurgical ventral discectomy with removal of vertebral bodies and plate osteosynthesis
Access is made via the front of the neck. By means of an operation microscope the damaged parts of the disc and the broken vertebral body are removed what enables decompression of the nerves and the spinal cord. Afterwards the cervical spine is re-stabilized by implanting a tricortical iliac crest bone or a metal vertebral body replacement. Additionally a ventral plate osteosynthesis is needed to ensure sufficient stability.
Dorsal microsurgical decompression with stabilization
A microsurgical decompression is carried out in several stages by removing ligaments and compressed parts of the bone. Stabilization of the cervical spine is carried out by dorsal fixation with a screw-rod system. In rare cases and only with severe rup-tures with massive instability, ventral and dorsal stabilization techniques need to be applied both at the same time.
Aftercare
Mobilization should follow surgery as soon as possible. After complex stabilization operations, the patient should furthermore wear a neck crest during the initial phase. Especially with previous neurologic deficits, rehabilitation treatment is necessary.

109
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 109
Neurosurgery / Spinal Column
Lumbar Spine (LS)
The lumbar spine (LS) is the lower part of the spinal column with a total of 5 verteb-ral bodies. It connects legs and pelvis with the rest of the spinal column. By walking upright, this part of the spinal column is exposed to heavy stress, what often causes painful irritations summarized under the generic term “back pain”. Important is here differentiation in this wide range of disease patterns which range from simple pain symptoms to complex disc herniations with neurological deficits. Degenerative lumbar spine disorders are very common symptoms and may also affect younger patients.
Disc Herniation
Cause
The degeneration process of a disc results in loss of liquid, reduction of height and finally in laceration of the fibrous ring. The leaked disc tissue exerts pressure on the nerves what causes pain and also may lead to neurological deficits.
Symptoms
Acute and chronic, stress-dependent back pain which radiates to the leg. Movement restrictions of the spinal column, weakness and loss of power of legs and feet. The sensation of tingling, warmth and cold in the legs. Gait disorder with the feeling of insecurity when walking. Impairment of the rolling movements of the foot when walking. Bladder- and bowel voiding dysfunctions.
Diagnosis
Is made with a neurological examination and a special examination of the spinal column. Furthermore, X-ray images and functional images of the lumbar spine are needed and a MRT should be carried out as it offers optimal view on the herniated disc.
Therapy
Cases without obvious neurological deficits should be treated conservatively first. This comprises intensive physiotherapy and pain medication; in some cases also local infiltrations. However, if these measures do not bring adequate improvement, in-dication for operative treatment should be assessed and discussed. Here, individual advice and definition of the best strategy and the optimal operation method are of decisive importance. Herniated discs which cause acute high levels of paralysis or bladder-colon disturbances need to be treated in an emergency operation.
Operation Method
Minimally-invasive percutaneous nucleotomy
DThis procedure is carried out under local anesthesia. Under radiologic control a cannula is inserted sideways into the disc space to inject contrast medium. Then the respective disc tissue is removed by means of a pneumatically operated suction- and cutter mechanism. This technique is especially suitable for patients with subligamen-tal disc herniation. Patients with relevant bony narrowing of the nerve exit canals (foraminal stenosis), in an advanced stage of degeneration with resulting reduction of disc height (osteochondrosis), or a definitely sequestered disc do not benefit from this operation method in the long term.
Neu
rosu
rgery / Sp
inal C
olu
mn

110 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Neurosurgery / Spinal Column
Transforaminal endoscopic discectomy
This operation method can be carried out under local- or general anesthesia. Access is made via an 8-10 cm long incision from the side next to the spinal column. Through this incision the endoscope is inserted to the nerve exit canal (foramen) to remove the sequestered disc under endoscopic control. This minimally-invasive technique is especially suitable for patients with extremely outside-lying disc herniation (lateral sequester).
Microsurgical sequestrectomy
This microsurgical operation is carried out under local anesthesia. Access is made through a 2 – 3 cm long incision, whereby a special speculum is used to retract the back muscles to the side. The spinal canal and the nerves lying inside are reached via the natural bone window. After preparation by means of the operation microscope the leaked disc material can be removed with a special miniature forceps. The disc itself is preserved and only degeneratively changed material is removed; this helps to maintain the function of the disc. Entrapped nerves are immediately relieved and the radicular radiating pain eases. Disturbances in sensation and paralysis however need some time for complete regression.
Aftercare
With microsurgical operations, mobilization is started immediately after surgery. Getting up and walking is already possible the day of surgery. Also wearing a girdle is not necessary as statics and biomechanics of the lumbar spine are not impaired by this gentle microscopic treatment. The in-patient stay normally lasts 2 – 3 days, physiotherapy and other conservative therapies are started the week after surgery. Although patients feel recovered after a very short time, carrying heavy load or un-dertaking strenuous sporting activities should be avoided during the first 3 – 4 weeks. Duration of disability varies individually and depends on many different factors.
Facet Syndrome
Cause
Excessive strain on the spinal column not only causes damages to the discs but also leads to mechanical wear and tear on the vertebral joints, or more precisely on the inner surfaces – the so-called facets. Thus the term facet syndrome stands for wear and tear (arthrosis) of the small vertebral joints. Due to signs of wear or degenera-tive spondylolisthesis occurs excessive strain on the joints and with this continuous wear and damage of the joint cartilage. Exuberant bone formation and extension of joint facets are the result.
Symptoms
Back pain after periods of long standing, sitting or lying and when getting up. Most common complaints are back pain radiating to the buttock and the groin to the thigh. Rotating movements of the spinal column are painful, especially getting up in the morning can be very difficult.

111
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 111
Neurosurgery / Spinal Column
Diagnosis
Is made with a neurologic examination and a special examination of the spinal co-lumn. Moreover, X-ray images of the lumbar spine with functional images as well as images of CT and MRI help proving the diagnosis. Also helpful may be testinfil-trations of the vertebral joints.
Therapy
Conservative measures and pain medication can be successful when treating the fa-cet syndrome. With many patients, sling table therapy is very successful in the short term. All in all however, success of conservative therapies when treating advanced stages of facet degeneration.
Operation Method
Radiologically controlled facet infiltration (diagnostic and therapeutic)
Radiologically controlled facet infiltrations are carried out under local anesthesia. After local anesthesia of the skin a thin cannula is inserted directly into the facet joint at the lumbar spine and a small amount of local anesthetic (approx. 2 ml) injected under radiologic control. For diagnosis it initially is helpful to perform injections from both sides of the mobile segment. When therapeutically treating a facet block which can also be combined with a periradicular infiltration (PRI), a mixture of a local anesthetic and a crystalloid corticoid compound is injected. Here, too, a thin cannula is inserted into the skin after local anesthesia and a small amount of the mixture (2 – 3 ml) injected directly into the small vertebral joints. This medicine can also be injected directly into the tissue surrounding the nerve exit at the foramen. The local effectiveness needs only small dosages and the mixture has a long-lasting effect. Nevertheless several sessions are necessary to achieve long term freeness of pain.
Interspinous Retractor
This low invasive operation can be carried out optionally under local anesthesia or short-acting anesthesia. Under x-ray control the retractor is inserted through an ap-prox. 4 cm long incision at the back and then positioned between the bony spinous processes to relieve the vertebral joints. The operation is normally carried out on in-patient basis but patients can already walk the day after surgery. This in-patient stay lasts about 1 – 2 days.
Aftercare
There is no special aftercase necessary after radiologically controlled facet infiltration or the PRI. The therapy can lead to comprehensive reduction or even complete eli-mination of discomfort. After implantation of an interspinous retractor, progression is controlled via x-ray and clinical check-ups. Complementary conservative therapy measures are in most cases very helpful.
Neu
rosu
rgery / Sp
inal C
olu
mn

112 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Neurosurgery / Spinal Column
Spinal Canal Stenosis
Cause
Narrowing of the verterbral canal occurs mostly with elderly patients due to chronic wear as well as exuberant bone formation, vertebral joint arthrosis, disc protrusions, ligament thickenings and vertebral body dislocations. The spinal canal with the nerves inside becomes increasingly narrow and the continuous pressure results in pain and neurological deficits.
Symptoms
In most cases stress-dependent back pain which radiates to the legs. Other symptoms are weakness or loss of muscle power in legs and feet or the sensation of tingling, warmth and cold in the legs. Furthermore gait disorder with the feeling of insecurity when walking. Characteristic are also the symptoms of spinal intermittent claudication (claudicatio spinalis). Here, walking distances have to be more and more reduced.
Diagnosis
Is made by neurologic examinations as well as special examinations of the spinal column. X-ray images of the lumbar spine and so-called functional images are neces-sary. Moreover, a CT and/or a MRT should be carried out. In rare cases even a lumbar function myelography for further invasive diagnostics is necessary.
Therapy
With a severe spinal canal stenosis, conservative treatment has little prospect of suc-cess as it is nearly impossible to have influence on the bony narrowing of the lumbar spinal canal i.e. the mechanical compression of the nerves. In the case of massive instability of the lumbar spine, even microsurgical decompression is not sufficient. In these individual cases, stabilization has to be considered. Here, individual advice and choice of the optimal surgery method are of essential importance.
Operation Method
Microsurgical Decompression
This microsurgical operation is performed under general anesthesia. Access is made through a 2 – 3 cm long incision, whereby a special speculum is used to retract the back muscles to the side. The spinal canal and the nerves lying inside are reached via the natural bone window. Under microscopic control the enlarged facet joint segments are undermined by means of diamond micro milling cutters and small punches what extends the nerve exit canal and the spinal canal. Thanks to an ope-ration method newly developed some years ago (Spetzger, et al) the spinal canal can be decompressed from both sides through only one access. This method has by now already become one of the standard procedures for microsurgical treatment of spinal canal stenoses (Spetzger, et al). The disc itself is preserved if no obvious disc herniation can be detected. In many cases, the facet joint is heated up with special forceps and treated with bipolar coagulation. This has a positive effect on local pain. Trapped nerves are relieved and the radiating pain eases quickly. With following conservative therapy extending the walking distance is achieved very soon.

113
Ellenb
og
en
Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected] 113
Neurosurgery / Spinal Column
Aftercare
With microsurgical operations, mobilization is started immediately after surgery. Getting up and walking is already possible the day of surgery. Also wearing a girdle is not necessary as statics and biomechanics of the lumbar spine are not impaired by this gentle microscopic treatment. The in-patient stay normally lasts 3 - 4 days, physiotherapy and other conservative therapies are started the week after surgery.
Fractures
Cause
Fractures are often caused by acute violence on the thoracic- or lumbar spine or are the result of an accident in the past with rupture of ligament structures and fractures of vertebral bodies, vertebral arches and vertebral joints. But fractures can also occur in connection with tumors, inflammations of the spinal column or as sign of osteoporosis.
Symptoms
Severe diffuse back pain and discomfort throughout the whole spinal column with movement restrictions up to neurologic deficits. Especially with elderly patients or as a result of certain diseases, fractures may occur as a result of minor falls.
Diagnosis
Is made with a neurologic examination as well as a special examination of the spinal column. Furthermore, X-ray images with functional images as well as a CT and a MRI are necessary; in some cases even nuclear medicine examinations are needed for more precise diagnostics. Important is here differentiation and consideration of the actual cause.
Therapy
If there is neither obvious instability nor any neurological deficit detectable, treat-ment can be done conservatively. Adjustment of an individual girdle as well as stabilization by means of special physiotherapeutic measures together with pain medication bring often complete healing. When treating fractures of the thora-cic- and lumbar spine, individual advice as well as discussion of the indication and most appropriate operation technique is of decisive importance. With osteoporotic fractures or vertebral body metastases, minimally-invasive techniques with injection of PMMA-cement show very good results.
Operation Method
Vertebroplasty and Kyphoplasty
Minimally-invasive surgery can be performed optionally under local- or general anesthesia. In prone position and under permanent x-ray control, one or two can-nulae are inserted through the pedicle of the affected vertebrae. Then the verteb-ral body is re-erected by inflating a balloon (kyphoplasty). In case that this special positioning has already caused this re-erection, polymer cement (PMMA) is directly injected into the vertebral body (vertebroplasty). This pasty cement fills the broken vertebrae from the inside and hardens within several minutes so that immediate stabilization is achieved.
Neu
rosu
rgery / Sp
inal C
olu
mn

114 Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
Aftercare
Mobilization is possible directly after surgery what enables the patient to get up and walk already the day of operation. Girdles are only necessary in individual cases. The in-patient stay normally lasts 1 – 2 days and in the week following the surgery physiotherapy and other conservative treatments can be started.
Neurosurgery / Spinal Column

115
Ellenb
og
en
115
Directions
Directions via the A8 motorway Karlsruhe-Stuttgart
• Leave the A8 motorway at exit 43 junction Pforzheim West with direction to Pforzheim-Zentrum (city center).
• Stay in the left hand lane and turn into the Karlsruher Straße (B10). Follow the road for about 400 m.
• Leave the Karlsruher Straße (B10) and turn right into the Stuttgarter Straße.
• Follow the road for about 600 m. Then turn right into the Rastatter Straße.
Rastatter Str. 17-19 • 75179 Pforzheim • Germany Phone +49 7231- 60556- 0 • Fax +49 7231- 60556- 3044
www.sportklinik.de • [email protected]
A8
AS PFORZHEIM WEST
B10 / Karlsruher Str.
B10
INDUSTRIEGEBIETWILFERDINGERHÖHE
Raststatter Str.
Wilhelm-Becker Str.
Stuttgarter
Str.
STUTTGARTMÜNCHEN
FRANKFURTKARLSRUHE
ZENTRUM

Rastatter Str. 17-19 • 75179 Pforzheim • Germany • Phone 07231- 60556- 0 • www.sportklinik.de • [email protected]
ARCUS Kliniken
Rastatter Str. 17-1975179 Pforzheim Germany
Phone +49 7231 605560Fax +49 7231 60556 3044