public health module venue date unit: public health aspects of diabetes wb1 © 2010
TRANSCRIPT

Public Health Module
VenueDate
Unit: Public Health Aspects of Diabetes
WB1
© 2010

2
Course Aims
This unit will:
– Explore how common diabetes is;
– Familiarise students with the risk factors of diabetes
– Explore the efficacy interventions for the prevention and management of diabetes
WB3
LTPHN/JS © 2010
3
Outline
Part I: DIABETES AS A PUBLIC HEALTH PRIORITY 1. What is diabetes?2. Classifying diabetes 3. Epidemiology - how common is diabetes? 4. Risk factors and consequences
Part 2: PREVENTING AND MANAGING DIABETES 1. Primary prevention of diabetes2. Secondary prevention3. Screening in diabetes4. Self care 5. Monitoring diabetes care
WB3
LTPHN/JS © 2010

What is health?WB5
WHO Definition ‘a state of complete
physical, mental and social
well-being and not merely
the absence of disease or
infirmity’
Antonovosky: Salutogenic model
‘sense of coherence’
Seedhouse and Duncan: Achievement of potential
Empirical Lack of health
4 LTPHN/JS © 2010

What is public health?
‘the science and art of preventing disease, prolonging life and promoting health through the organized efforts of society’
C.E.A. Winslow, 1920
5
WB6
LTPHN/JS © 2010
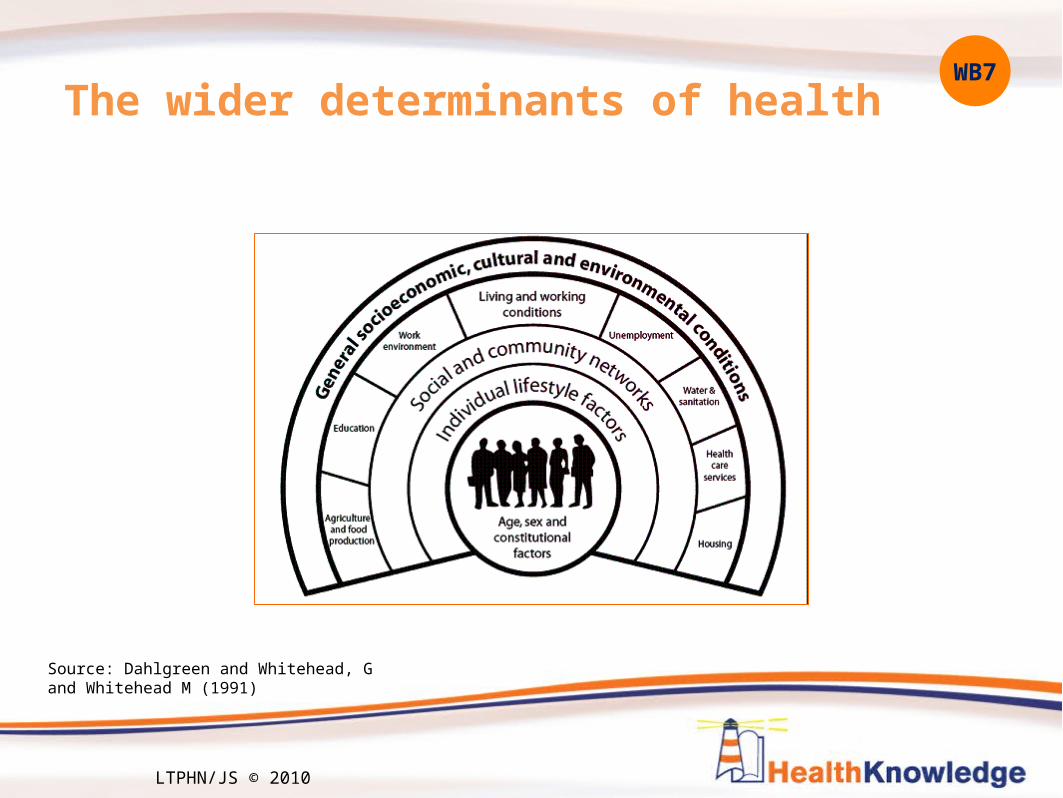
The wider determinants of health
Source: Dahlgreen and Whitehead, G and Whitehead M (1991)
WB7
6 LTPHN/JS © 2010

The challenge for public healthWB7
7 LTPHN/JS © 2010

Statistical description of nation’s healthWB8
Census data
Health Inequalities data
Infant Mortality Rates
8 LTPHN/JS © 2010

9
1. What is diabetes?
Diabetes results from reduced production of the hormone
insulin, resistance of body tissues to the effect of insulin,
or both.
The result is abnormally high levels of glucose in the blood and
widespread disturbances to metabolism.
WB9
LTPHN/JS © 2010

10
History
• 30-90AD: Diabetes named by Greek Physician Aretaeus: means ‘a flowing through’ to describe its constant thirst, excessive urination and weight loss
• Japanese name: 'Shoukachi', the thirst disease
• 1600s: Professor Thomas Willis of Oxford University describes urine in diabetes mellitus as ‘wonderfully sweet’, distinguishing it from diabetes insipidus
• 1889: Oskar Minkowski and Joseph von Mering of University of Strasbourg remove a dog’s pancreas - it produces diabetes
• 1921: Banting & Best isolate insulin, successfully treats a patient, transforming diabetes to a treatable, chronic condition
WB9
LTPHN/JS © 2010

The Healthy Body
3. Insulin triggers liver to take up glucose and turn into glycogen
1. Glucose, produced from carbohydrates, released into bloodstream
2. The pancreas produces insulin, also released into the bloodstream
4. Insulin enables cells to take up glucose
Source: Diabetes UK, Diabetes and the Body animation (www.diabetes.org.uk/Guide-to-diabetes/Introduction-to-diabetes/What_is_diabetes/Diabetes-and-the-body/)
WB14
11 LTPHN/JS © 2010

12
2. Classification
• The WHO recognises several types of diabetes• Type 1• Type 2• Gestational diabetes• Other types
WB16
12 LTPHN/JS © 2010

I. Type 1 Diabetes
The pancreas unable to produce insulin
Accounts for ~15% of diabetes in the UK
Mainly diagnosed in children/young adults
Characterised by insulin deficiency
Symptoms develop quickly
WB16
13 LTPHN/JS © 2010

14
In type 1 diabetes, no insulin is available so cells are unable to take in glucose
WB17
LTPHN/JS © 2010

15
Symptoms of type 1 diabetes
• Frequent and excessive urination• Thirst• Dehydration• Tiredness• Urinary or genital tract [eg thrush] infections• Blurred vision• Symptoms develop quickly
• Can progress to ketoacidotic coma
WB15
LTPHN/JS © 2010
16
Type 2 diabetes
• Characterised by insulin resistance, though may also have deficiency [Used to be classified as Non-insulin dependent diabetes (NIDDM) but can require insulin]
• Similar acute symptoms to type 1• Compared with type 1, often develops gradually• Some have no symptoms at diagnosis • Milder forms: can be controlled by diet, and exercise• Accounts for ~85% of diabetes in the UK• Mainly diagnosed in older adults though increasingly seen in
younger age groups too
WB17
LTPHN/JS © 2010

17
II. Type 2 diabetes
Fat deposits affect cells’ insulin (i) sensitivity. They are less able to take in glucose (g)
WB19
LTPHN/JS © 2010

18
III. Gestational diabetes
• Excess blood glucose during pregnancy (both diabetes mellitus and impaired glucose regulation)
• Increased risk of diabetes related complications in pregnancy
• Health consequences for the baby include increased risk of• birth complications: caesarean sections; still births and
perinatal deaths • very high birth weight babies • birth defects• obesity and diabetes in the child.
• For the mother:• increased long term risk of type 2 diabetes (30% as opposed to
10% in the general population)• higher risk of diabetes-related complications in
subsequent pregnancies
WB20
LTPHN/JS © 2010

19
IV. Other types
• Monogenic diabetes• 1-2% of all diabetes, affecting 20,000-40,000 in UK• Usually develops in under 25s• Due to a single gene mutation• Runs in families – affected person has 50% chance of
passing on
• Currently 6 types of monogenic diabetes recognised• Some types managed by diet and exercise alone • Often initially misdiagnosed as type 1 or type 2 diabetes • Diagnosing correctly can help
• inform which treatments are most appropriate • give some idea of how the diabetes is likely to progress • affected families understand their risk of diabetes and/or risk to
their children
WB22
LTPHN/JS © 2010

20
Diabetes insipidus
• Moderately rare condition - affects 1 in 25,000
• Symptoms of excessive urination
• Distinct from diabetes mellitus: • not related to production or sensitivity to insulin• Urine not sweet• related to function of vasopressin hormone in the pituitary gland
WB23
LTPHN/JS © 2010

Classifying glucose regulation
Normoglycaemia (low risk of
diabetes/CVD)
FPG: ≤ 6.0mmol/l
Impaired glucose regulation
(higher risk of diabetes/ CVD)FPG: >6 to <7mmol/l
Diabetic
(high risk of CVD)FPG: 7.0 + mmol/l
“Healthy” “Diabetic”
DiabetesLow risk
Risk
Glucose levels
WB23
21 LTPHN/JS © 2010

22
3. Long term impact of diabetes
• Diabetes is an important cause of death and disability
• Diabetes is a leading cause of blindness, renal failure and neuropathy in the UK
• Life expectancy is reduced on average by 20 years in those
with Type 1 diabetes and up to 10 years in Type2 diabetes
WB12
LTPHN/JS © 2010

23
RetinopathyRetinopathyCommon cause of Common cause of blindness in peopleblindness in people
of working age in Westof working age in West
NephropathyNephropathy20% of all ESRD20% of all ESRD
Erectile DysfunctionErectile DysfunctionMay affect up to 50%May affect up to 50%
Macrovascular Macrovascular 2–4 x increased risk 2–4 x increased risk
of CVD, 75% have of CVD, 75% have hypertensionhypertension
Foot ProblemsFoot Problems15% develop 15% develop
foot ulcers; 5–15% need foot ulcers; 5–15% need amputationamputation
Source: The Audit Commission. Testing Times. A Review of Diabetes Services in
England and Wales, 2000.
WB12
LTPHN/JS © 2010

24
‘Macrovascular’ complications cardiovasular diseases
• Biggest cause of death in diabetes:• 75% of deaths in people with diabetes caused by
cardiovascular disease
• People with diabetes have:• 2x risk of death from heart disease• 1.5-4x risk of stroke
WB12
LTPHN/JS © 2010

25
‘Microvascular’ complications
Nerves (neuropathy): – affects up to 60-70% of people with diabetes– symptoms include tingling or burning, pain, numbness– increases the chance of foot ulcers and limb amputation– other conditions e.g. erectile dysfunction
Eyes (retinopathy):– biggest cause of blindness in working aged adults in UK – long-term damage to the small blood vessels in the retina– after 15 years of diabetes, ~ 2% of people become blind, and about
10% develop severe visual impairment
Kidneys: – Disease detected by protein in the urine– affects 30% of people with diabetes
WB13
LTPHN/JS © 2010

Source: Yorkshire & Humber Public Health Observatory 2008
Deaths from diabetes~ 2700 death certificates with diabetes as cause of death pa~26,000 deaths from the diseases caused by diabetes paSo death certificates underestimate diabetes attributable deaths. Variations by area too:
WB25
26 LTPHN/JS © 2010
27
Cost of diabetes
• Diabetes is a clinical area of high expenditure• eg in one year, October 2007 to September 2008, there were
31.9 million NHS items prescribed = £581.2 million
• ~ 5% of total NHS spend is used for the care of people with diabetes
• The growth in expenditure on prescribing for diabetes is greater than any other major clinical area
WB26
LTPHN/JS © 2010

28
4. Prevalence of diabetes
• Current prevalence• Trends• Models
WB27
LTPHN/JS © 2010

Global impact
• Diabetes accounts for estimated 5.2% all world mortality• 80% deaths occur in low & middle income countries• Prevalence increasing fastest in these countries
Source: WHO
WB25
29 LTPHN/JS © 2010

Diabetes prevalence in England
• 2.1 million on diabetes registers
• BUT 25% in coronary care have undiagnosed Type 2 DM
• Y&H PHO modelling estimates:• another 400,000+
not diagnosed• The estimated prevalence of
diabetes (diagnosed and undiagnosed) is 4.82% of population of England
• prevalence varies by area
WB27
30 LTPHN/JS © 2010

Trends
• Diabetes expected to rise in England to 6.5% by 2025
WB28
31 LTPHN/JS © 2010

Diabetes UK Silent Assassin Campaign
What do these images say to you about diabetes?
WB29
32 LTPHN/JS © 2010

33
5. Risk factors
• Why consider risk factors?
• Type 1 v 2
WB30
LTPHN/JS © 2010

Type 1
• Highest prevalence in northern European populations
• Strong familial link – genetic factors
30
6
4
2
0.3
0 5 10 15 20 25 30 35
identical twin
sibling
father
mother
no familymembers
Fam
ily
mem
ber
aff
ecte
d
% risk of type 1 diabetes
WB30
34 LTPHN/JS © 2010

Relative risks of type 2 diabetes
• Population factors:WB• Family history; • Age; • Socioeconomic
circumstances; • Ethnicity
• Modifiable risk factors• Obesity; • Exercise; • Smoking
0 5 10 15 20 25
OBESITY
age
ethnicity
socioeconomicfactors
SMOKING
Ris
k fa
cto
r
RR
WB31
35 LTPHN/JS © 2010
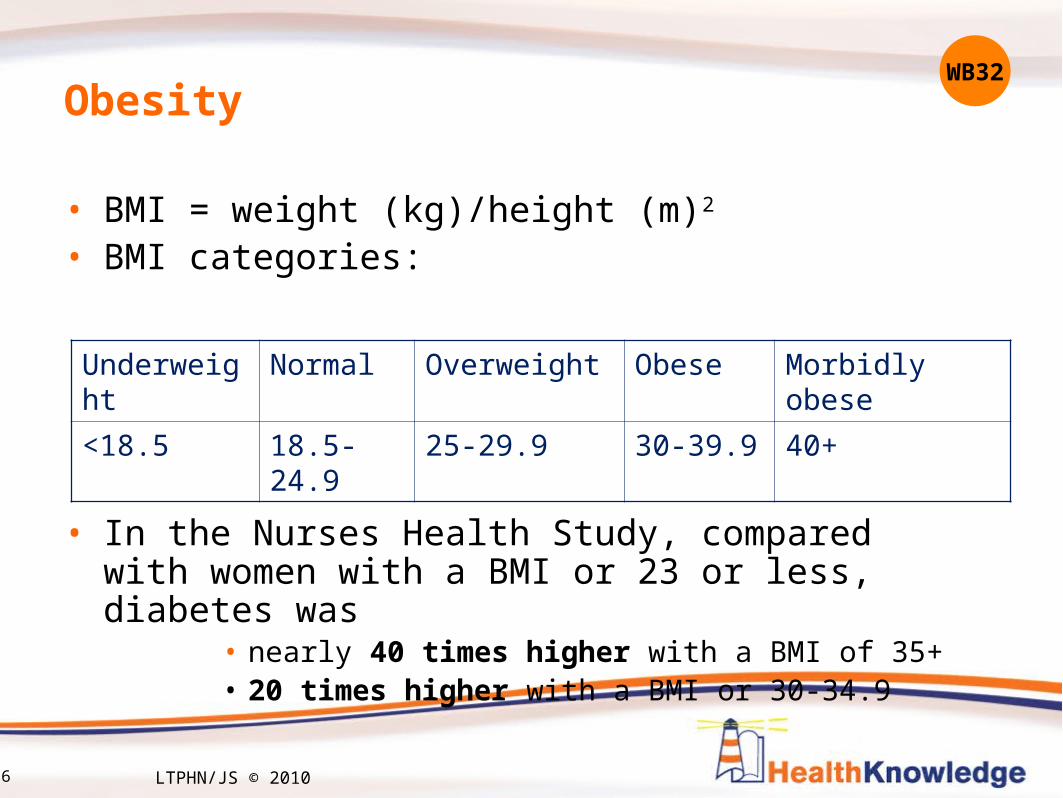
Obesity
• BMI = weight (kg)/height (m)2
• BMI categories:
• In the Nurses Health Study, compared with women with a BMI or 23 or less, diabetes was
• nearly 40 times higher with a BMI of 35+ • 20 times higher with a BMI or 30-34.9
Underweight Normal Overweight Obese Morbidly obese
<18.5 18.5-24.9 25-29.9 30-39.9 40+
WB32
36 LTPHN/JS © 2010

37
Ashwell shape chartWB34
Take Care OK Take Care Action
LTPHN/JS © 2010

38
Physical activity, obesity and the risk of diabetes
WB33
LTPHN/JS © 2010

Age
Prevalence of doctor-diagnosed diabetes, by age
WB34
39 LTPHN/JS © 2010

40
Ethnicity
• In England, compared with the general population, rates of diabetes are:
• 3-4 x higher Bangladeshi, Pakistani and Indian men• 5 x higher in Pakistani women• 3 x higher in Bangladeshi and Black Caribbean women • 2.5 in Indian women
• When assessing risk of diabetes, need to consider ethnicity, & also need to consider gender
WB35
LTPHN/JS © 2010

Deprivation Age adjusted prevalence of known diabetes by fifths of deprivation score
• Mortality and morbidity are increased by socio-economic deprivation
• The complications of diabetes have been shown to be more prevalent in areas of high socioeconomic deprivation
J Epidemiol Community Health 2000;54:173-177
WB36
41 LTPHN/JS © 2010

42
Other risk factors
• Smoking: • small relative risk compared to obesity, but of public health
importance given prevalence of smoking, particularly in poorer socioeconomic groups
• Physical health problems
• Mental health
WB37
LTPHN/JS © 2010

43
Diabetes and gender
• Risk factors affect men and women differently
• Risk of death from heart disease linked to diabetes is greater in women than men:
• Is diabetes more harmful to women? and/or• Is treatment better for men? and/or??
• Gestational diabetes: numbers of diabetes cases in women of childbearing age increasing
• Risk factors: family history; pre-pregnancy obesity; advanced maternal age; gestational diabetes in previous pregnancy; ethnic background; large baby (≥ 4.5 kg) in a previous pregnancy; smoking
WB38
LTPHN/JS © 2010

44
Part 1 summary• Diabetes is a chronic condition
– It can lead to CVD, kidney failure, limb amputation and blindness
• Type 1 and type 2 diabetes share similar symptoms but different public health implications
• Type 2:– 85% of diabetes in UK– Obesity most important modifiable risk factor. – more common in people over 40 years, Pakistani, Bangladeshi, Indian
and African Caribbean populations • Women and poorer socioeconomic groups more at risk of diabetes
complications and death from diabetes
• Problems assessing the health burden of diabetes because: – ~20% with type 2 diabetes remain undiagnosed– diabetes seldom recorded as cause of death but its complications –
heart disease, stroke, renal failure – are leading causes of death.
WB40
LTPHN/JS © 2010

45
Exercise: ‘Westport’ PCT’s local diabetes Needs Assessment
• ‘Westport’ PCT needs to understand the current impact of diabetes on its population – prevalence, health consequences and effects on services - and to forecast the impact of diabetes in the future
• From what you’ve learnt in the module so far, how would you find out about the impact of diabetes on your local population?• What sources of data could you access?• What information would you collect specifically? Who would you ask?
WB41
LTPHN/JS © 2010

46
Part 2: Preventing and managing diabetes
1. Primary prevention of diabetes
2. Secondary prevention
3. Screening in diabetes
4. Self care
5. Monitoring diabetes care
WB42
LTPHN/JS © 2010

47
1. Primary prevention
• Three strategies for primary prevention- • Upstream- whole population
• Midstream- special high risk groups e.g. children, elderly
• Downstream- high risk ‘individuals’
• Type 2 prevention Government priority in England:
“The NHS will develop, implement and monitor strategies to reduce the risk of developing type 2 diabetes in the population as a whole and to reduce the inequalities in the risk of developing type 2 diabetes.”
Standard 1 of the Diabetes National Service Framework, 2003
WB43
LTPHN/JS © 2010
48
Population measures
• Reducing obesity• Increasing physical activity
• Choosing health: choosing a healthy diet and choosing activity– 5-a-day– 5-a-week
WB43
LTPHN/JS © 2010

49
Identifying high risk individuals
• Why?– Can target interventions to those most at risk
• How?– Risk assessment considering
» Weight (BMI, waist circumference)» Blood pressure» Cholesterol» Blood glucose
WB45
LTPHN/JS © 2010

50
NHS Health Check WB46
LTPHN/JS © 2010

Interventions for high risk individuals• Lifestyle interventions significantly reduce progression rates
to diabetes in prediabetic individuals• Trials have shown that sustained lifestyle changes in diet
and physical activity can reduce the risk of developing type 2 diabetes
Study Country % risk reduction
Diabetes Prevention Programme (Tuomilehto et al, 2001)
Finland 58
DAQing (Pan et al, 1997) China 46
Diabetes prevention programme (Knowler et al, 2002)
America 58
WB47
51 LTPHN/JS © 2010
52
Programmes for high risk
• Medications & non-drug interventions to:– reduce blood pressure– lower cholesterol (eg statins)– manage blood glucose
• Community referrals for programmes on:– exercise– weight management – smoking cessation
• Specialist referrals for bariatric surgery?
WB48
LTPHN/JS © 2010

Exercise: theory…
• Chief Medical officer Report 2004: ‘5 a week’ call for action
• At least 30 minutes exercise 5 times a week can improve health, prevent diabetes and reduce overweight
WB48
53 LTPHN/JS © 2010

54
…reality?
And…people with diabetes less likely to meet exercise recommendations
WB49
LTPHN/JS © 2010

55
target high risk or provide for the whole population?
In public health, there is often debate about whether to target high-risk individuals or offer population wide strategies to promote health and prevent disease
Think of some of the pros and cons of these contrasting approaches for lifestyle interventions to adopt healthier diets and take more exercise to prevent diabetes
WB50Exercise 2: Encouraging healthy eating and regular exercise
LTPHN/JS © 2010
56
3. Screening
• Primary prevention– To identify people at increased risk of disease
• Secondary prevention– To identify early stages of disease
NSC found no evidence to implement national screening for diabetes in UK.
Better strategy to:– optimise management of blood pressure and hyperglycaemia in people with
known diabetes; and– ensure universal screening for eye disease
WB53
LTPHN/JS © 2010

57
4. Self care and self managementDESMOND for type 2 diabetes
• Diabetes Education and Self Management for Ongoing and Newly Diagnosed patients
• Group sessions to help new patients to– identify their own health risks – develop behaviour and health goals tailored to their
own circumstances
• Evaluation found:– greater weight loss & smoking cessation – improvements in beliefs about illness– No change in HBA1c
WB56
LTPHN/JS © 2010

58
5. Monitoring diabetes care
• Why?– To find out if services delivered as intended– To find out whether services reaching groups that need them
• How?– Local monitoring, checks, visits, feedback– National data
• Monitoring against targets: access• Patient survey: patient experience• Hospital admissions & procedures: outcomes
WB59
LTPHN/JS © 2010

59
NCHOD admissions and procedures
Age standardised rates of emergency hospital admissions for diabetic coma and ketoacidosis, by region
0
5
10
15
20
25
30
35
NORTH E
AST
NORTH W
EST
YORKS & H
UMBER
EAST MID
LANDS
WEST M
IDLA
NDS
EAST OF E
NGLA
ND
LONDON
SOUTH EAST
SOUTH WEST
Regions in England
dia
be
tic
co
ma
an
d k
eto
ac
ido
sis
e
me
rge
nc
y h
os
pit
al
ad
mis
sio
ns
/re
sid
en
t p
op
ula
tio
n
WB61
LTPHN/JS © 2010

60
Part 2 summary
• Type 2 diabetes is preventable• Complications of diabetes can be avoidable• Interventions aim to:
– encourage healthy eating and regular exercise– reduce blood pressure, cholesterol and improve glucose regulation– reduce complications
• Programmes in England to improve diabetes care focus on identifying high risk individuals, rewarding quality services, screening for retinopathy
• Monitoring indicates room for improvement in access and effectiveness
WB63
LTPHN/JS © 2010

61
Exercise 3: Shaping your local services
‘Westport’ PCT’s public health department has been asked to recommend how Nowhere should develop its diabetes services.
• How would you assess the impact of diabetes services
provision locally?• From what you’ve learnt in the module, how would
you decide on your top priorities for diabetes in your local area?
• Think about:– Prevention vs treatment– Evidence based programmes vs learning through doing– National policy priorities and targets
WB64
LTPHN/JS © 2010