public health leadership and management for the 21st century
DESCRIPTION
A Global Health Leadership Report, University of Southern California, USCTRANSCRIPT

Institute for Health Promotion and Disease Prevention Research
GRADUATE COURSE GUIDELINES
Institute for Health Promotion and Disease Prevention Research
GLOBAL HEALTH LEADERSHIP REPORTS BEST PRACTICE SOLUTIONS TO ENHANCE THE PERFORMANCE OF HEALTH SYSTEMS M. RICARDO CALDERÓN, SERIES EDITOR
PUBLIC HEALTH LEADERSHIP AND MANAGEMENT FOR THE
21ST CENTURY
May 2010

PublicHealthLeadershipandManagementforthe21stCentury May2010
22
INSTITUTE FOR HEALTH PROMOTION & DISEASE PREVENTION RESEARCHKeck School of MedicineUniversity of Southern California (USC)1000 South Freemont Avenue, Unit 8 Alhambra, California 91803
The Global Health Leadership Reports is a publication of the USC Institute for Health Promotion and Disease Prevention Research (IPR). The opinions expressed herein are those of the editor and author(s) and do not necessarily reflect the views of the University of Southern California. Excerpts from these publications may be freely reproduced acknowledging Global Health Leadership Reports as the source.
Internet: http://mph.usc.edu/ipr/Internet: http://mrcalderon.com
GLOBAL HEALTH LEADERSHIP TEAM
SERIES EDITOR:
M. Ricardo Calderón, M.D., M.P.H.Senior Administrative Director, International Training Programs; Associate Professor, Preventive Medicine; Founding Director, MPH Global Health Leadership Track and Regional Director, Latin America and the Caribbean, USC-IPR & Area Director & Health Officer, County of Los Angeles Department of Public Health
INFORMATION DISSEMINATION INITIATIVE
Carina Lopez, M.P.H.Program Manager
The GLOBAL HEALTH LEADERSHIP REPORTS series was created by Professor M. Ricardo Calderón during his tenure at the Institute for Health Promotion and Disease Prevention Research (IPR) of the University of Southern California’s Keck School of Medicine (USC). It was designed to provide a forum to faculty and students of the USC Master of Public Health (MPH) Program to share lessons learned and best practice solutions to enhance the performance of health systems around the world. The research, training and service of university faculty and students is published in a variety of peer reviewed and professional journals traditionally and due to scholarly purposes. While this is the acceptable professional and academic manner to contribute with original unpublished research, social science analyses, scholarly essays, critical commentaries and letters to the editors, there is an extensive body of practical information and valuable knowledge that is either not submitted for publication or that takes too long to be published. This lack of information exchange may reflect a missed opportunity to strengthen, expand and diversify knowledge learning and capacity development to trouble-shoot, problem-solve, make informed choices, prioritize investments, implement evidence-based practices and/or lead innovation and change in the healthcare industry and public health systems.
The Global Health Leadership Reports series was created to fill some of the gaps in information dissemination and exchange and, more importantly, the timely integration of research findings and best practice solutions into program development, implementation and evaluation for enhanced institutional performance and population health outcomes. This is accomplished by developing electronic publications that can be easily distributed by e-mail, posted in websites or transmitted by internet around the world. This is also done by capitalizing upon the research efforts and practical solutions developed by faculty and graduate students throughout their teaching and learning experience, graduate education, classroom debates, and group discussions including a variety of projects that are implemented by talented, creative and innovative faculty and students.
We trust that the reader will be open to our publication rationale and approach, and will contribute to further disseminate reliable information for the effective development of community and global health programs, plans and policies. We hope that the Global Health Leadership Reports will stimulate discussion and reflection, propel continued dialogue, and encourage the pioneering of new combinations of innovative approaches and practical solutions to enhance the performance of health systems and improve the health status and wellbeing of individuals, families and communities worldwide. We also hope to contribute to fulfill the vision to create healthy people living in healthy environments locally and globally, and living longer, quality lives in a world with less pain and suffering, less injuries and disease, less health inequities and disparities, and a world where our minds and bodies perform at optimum levels.
At a Glance

PublicHealthLeadershipandManagementforthe21stCentury May2010
3
EXECUTIVE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
COURSE INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
1.LearningOutcomes 2.CourseFormatandGradingCriteria 3.TeachingPhilosophy
I. FUTURE-FOCUSED LEADERSHIP . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
1.Lecture:GlobalHealthLeadershipTrack&InterdisciplinaryGlobalHealthTraining
2.Lecture:PublicHealthLeadershipFrameworkforthe21stCentury
3.TeamExercise:CreatingIndividualandSharedVisions
4.Discussion:ConceptPaper#1:DevelopingaVisionaryLeadershipApproach
5.Bibliography
II. LEADING PUBLIC HEALTH INSTITUTIONS . . . . . . . . . . . . . . . . . . . . 26
1.Lecture:TransformationalLeadership
2.IndividualExercise:LeadershipversusManagement
3.Lecture:PublicHealthLeadershipPrinciples
4.Discussion:ConceptPaper#2:DevelopingEmpoweredLeaders
5.Lecture:SWOTAnalysis
6.Self-DirectedStudyProjectandPaper#1:SWOTAnalysis
7.Bibliography
III. FORMULATING STRATEGY. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
1.Lecture:LeadershipApplicationsinPublicHealth 2.ClassExercise:SystemsThinking
3.Discussion:ConceptPaper#3:BuildingInternalandExternalPartnerships
4.Lecture:LeadershipandthePlanningProcess
2.Lecture&ClassExercise:Asset-BasedCommunityStrategies
6.Lecture:ParticipatoryStrategicPlanning
7.Discussion:ConceptPaper#4:BuildingSupportforaStrategicPlan
8.Self-DirectedStudyProject&Paper#2:CreatingaStrategicandanImplementation Plan
9.Bibliography
Table of Contents

PublicHealthLeadershipandManagementforthe21stCentury May2010
4
Table of ContentsIV. LEADING AND MANAGING CHANGE. . . . . . . . . . . . . . . . . . . . . . . . . .68 1.Lecture:LeadershipandOrganizationalCulture
2.IndividualExercise:TimeManagementMatrix
3.Lecture:PeacetimeManagement&WartimeLeadership
4.ConceptPaper#5Discussion:ImplementingAdaptiveLeadership
5.Lecture:ManagingPersonalandOrganizationalChange
6.CaseStudy:TheCenterforDiseasePreventionandControl(CDC)FuturesInitiative
7.Lecture:ServantLeadership
8.Discussion:ConceptPaper#6:CommunicatingChange
9.Bibliography
V. DEVELOPING PUBLIC HEALTH ORGANIZATIONS . . . . . . . . . . . . . . . . 95
1.Lecture:BuildingaLearningOrganization
2.Lecture:CreatingOrganizationswithManyLeaders
3.Discussion:ConceptPaper#7:CreatinganEnvironmentforInnovation
4.Lecture:DevelopingaPerformanceOrientedCulture
5.ClassExercise:WinasMuchasYouCan
6.Discussion:ConceptPaper#8:CreatingSelf-DirectedWorkTeams
7.Self-DirectedStudyProjectandPaper#3:IQ(IntelligenceQuotient),Emotional
Intelligence(EQ)andSpiritualQuotient(SQ)
8.Bibliography
VI. IMPLEMENTING STRATEGY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 112
1.Lecture:TheFiveFundamentalPrinciplesandTenCommitmentsofExemplaryLeadership
2.ClassExercise:CollaborativeLeadership
3.Lecture:CapstoneInitiativesandActionLearning:CollaborativeLeadershipChange
Project
4.Discussion:ConceptPaper#9:TurningVisionintoAction
5.Lecture:CrisisandEmergencyRiskCommunication
6.Lecture:RiskandHighStressCommunication
7.TeamExercise:WestNileVirusMessageDevelopment
8.Discussion:ConceptPaper#10:BecomingCustomerCentric
9.Bibliography

PublicHealthLeadershipandManagementforthe21stCentury May2010
53
EXECUTIVE SUMMARY:
TheInstituteofMedicine(IOM)publishedin1988aproposaltoensuretheefficiencyandeffectivenessofpublichealthservicesintheUnitedStates.Thisbook,TheFutureofPublicHealth,thatconcluded“TheNationhadlostsightofitspublichealthgoalsandhadallowedthesystemofpublichealthtofallintodisarray”.In2002,theIOMreleasedarelatedpublication,TheFutureofthePublic’sHealthinthe21stCentury,callingforanoverhaulofgovernmentpublichealthinfrastructureandnewpartnerstoaddressthenation’shealthchallenges.InherentinthiscalltoactionwastheIOMrecommendationthat“wemustbeledbythosewhohavethemasteryoftheskillstomobilize,coordinateanddirectbroadcollaborativeactionswithinthecomplexpublichealthsystem…..theseskillsneedconstantrefinementandhoning”.Consequently,avarietyofleadershipdevelopmentinstitutesweredesignedandimplementedbydifferentacademicandpublichealthinstitutionstoenhancetheperformanceofhealthsystemsandimprovepopulationhealthoutcomesacrosstheUnitedStates.Atthesametime,theneedfor,andthecriticalimportanceof,publichealthleadershipdevelopmenthadalreadybeenfeltinmanyhealthsystemsaroundtheworldandarangeoftrainingprogramswereunderdevelopmentand/orimplementation.
Asamedicalandpublichealthexpertwithinternationaltechnicalcooperationexperienceinovertwentycountries,IacceptedthechallengetorestructureandrevitalizethepublichealthsysteminLosAngelesCountyin1999.Bythistime,myworkexperiencehadtransitionedfromprivateclinicalpracticeandhealthcaredeliverytoa5,000-MayanIndiantowninGuatemala,toarangeoftechnicalandmanagerialpositionsincluding,butnotlimitedto,malariapreventionandcontrol,nation-widesurveillanceofendo-epidemicdiseases,maternalandchildhealth,reproductivehealthandfamilyplanning,nutritionandfoodprogramming,pharmaceuticalassistance,HIV/AIDS/STDs,healthpromotionandwellness,andinfectiousandchronicdiseasepreventionandcontrol.Mymedicalandpublichealthexperience,particularlyinthedevelopingworld,hadtaughtmethat(1)healthpromotion,wellnessanddiseasepreventionandcontrolareaffectedbyindividual,social,economicandenvironmentalfactorswithinandbeyondcommunitiesthatmustbeaddressedcomprehensively,and(2)protectingandimprovingthehealthandwellbeingofapopulationisasharedresponsibilityamongresidents,publicinstitutions,privatefor-profitandnon-profitorganizations,keystakeholders,opinionleadersandpolicymakers.
Therefore,Icreatedtwostrategicapproachestoaddressthechallengestoimprovehealthsystemperformanceandpopulationhealthoutcomes.First,aCommunityLiaisingProgramattheCountyofLosAngelesDepartmentofPublicHealth.Thisprogramwasdesignedtolead,organizeandsupportaconcertedpublic,privateandnon-profitsectorefforttostrengthen,expandanddiversifypreventionprogramsandpublichealthservices(M.RicardoCalderón,SeriesEditor,TheBestPracticeCollection:DevelopingaCommunityLiaisingPrograminLosAngeles,CountyofLosAngelesDepartmentofPubicHealth,July2009).Second,acourseonPublicHealthLeadershipandManagementforthe21stCenturyfortheMasterofPublicHealth(MPH)ProgramattheUniversityofSouthernCalifornia(USC).Ironically,thiscoursewasnotapprovedbytheMPHprogramadministrationduringthreeconsecutiveyears.However,whenUSCwasinvitedtoimprovethepublichealthinfrastructureinChinadueto(1)thehealthandsocioeconomicimpactoftheSARS(SevereAcuteRespiratorySyndrome)epidemicin2003,and(2)theassessmentoftheChineseCentersforDiseaseControlandPrevention(CCDC)revealinganeedforpublichealthleadershipdevelopmentatalllevels,thecoursebecamethepivotalpublichealthleadershipdevelopmenttoolofferedbyUSCinChina(M.RicardoCalderón,SeriesEditor,GlobalHealthLeadershipReports,StrengtheningthePublicHealthInfrastructureinChinatobetterrespondto21stCenturyThreats,InstituteforHealthPromotionandDiseasePreventionResearch,UniversityofSouthernCalifornia,June2005).
Atotaloftencertificateprogramsweredeliveredtothetop1,070publichealthdirectors,physicians,hospitaladministratorsanduniversityprofessorsinChinaduring2004and2005.TwocertificateprogramsweredeliveredinPublicHealthIntelligenceandLeadershipto144Chineseprofessionals.AthirdcertificateprograminPublicHealthLeadershipandEmergencyResponsewasgivento110professionals.ThiswasfollowedbysevencertificateprogramsinPublicHealthLeadershipandCrisisandEmergencyRiskCommunicationforanadditional816publichealthleadersatnational,provincialandcitylevels.ThePublicHealthIntelligenceandLeadershipCertificateProgramsintegratedintelligenceknow-how(scientificknowledge)andleadershipskills(executiveleadershipandmanagementtools)requiredtosuccessfullydirectpublichealthorganizationsandcoordinatepublichealthpreparednessandemergencyresponse.

PublicHealthLeadershipandManagementforthe21stCentury May2010
6
ThispublicationdescribesthePublicHealthLeadershipandManagementforthe21stCenturycourseindetail.ItprovidestheguidelinesofthecourseastaughttoprofessionalsatCCDC/ChinaandMPHstudentsatUSC/LosAngeles.Itisintendedtoguidecoursedevelopmentandinstructioninindustrializedanddevelopingcountriesinacademicandinformalsettings,andtostrengthen,expandanddiversifytheknowledgeandskillsofpopulation,healthanddevelopmentworkforces.ItisbasedonaPublicHealthLeadershipFrameworkcomprisingsixintegratedleadershippractices.Theseleadershippracticesareinterdependent.Alteringonewillaffectalltherestandmasteringallwillenableleaderstoachieveoutstandinghealthsystemperformanceandsuccessfulimplementationofinstitutionalvisionandoverallstrategy.ThecourseandtheframeworkpavedthewayforthecreationoftheUSCMPHGlobalHealthLeadershipTrackin2006andthelaunchingoftheMPHLeadership,ManagementandGovernanceTrackatthenewlycreatedSchoolofCommunityandGlobalHealthatClaremontGraduateUniversity(CGU)in2008.
Thispublicationreflectsajourneyoflessonslearnedandbestpracticesolutionsinatotaloftwentysevencountries.Icannotpossiblyacknowledgeeveryonewhohasplayedaroleinmyprofessionalgrowthanddevelopment.However,Iwishtoexpressmygratitudeandappreciationtothoseprofessors,mentors,friendsandinstitutionsmostcloselyconnectedtomyleadershipdevelopment---Drs.PaulTorrens,LesterBreslow,JonathanE.FieldingandRalphFrericks(UniversityofCalifornia,LosAngeles),MichaelF.Kipp(Kipp&Associates),JamesR.Morgan(StrategyandManagementDynamics),Dr.A.PaulBradley,Jr.(TheBradleyGroup,Inc),Dr.RobertBrien(TheHavefordGroup),PaulD.Storfer(HRTechnologies),Drs.AlexNorman,GerardRossey,AlanGlassmanandRichardMoore(CaliforniaStateUniversity,Northridge),Dr.VincentCovello(CenterforRiskCommunication),Dr.HughH.Tilson(UniversityofNorthCarolinaatChapelHill),Rev.Dr.GaryGunderson(EmoryUniversity),CarolWoltring(PublicHealthInstitute),MarkFriedman(FiscalPolicyStudiesInstitute),Dr.C.AndersonJohnson(UniversityofSouthernCaliforniaandClaremontGraduateUniversity),Dr.FernandoZacarías(PanAmericanHealthOrganization/WorldHealthOrganization),andDr.M.RobertoCalderón(PanAmericanHealthOrganization/WorldHealthOrganizationandWorldVisionInternational).Alsodeeplyimportantinmydevelopmentarethelearningenvironmentsofthefollowing“AlmaeMatres”andinstitutions:UniversidaddeSanCarlosdeGuatemala(USAC),UniversityofCalifornia,LosAngeles(UCLA),UniversityofSouthernCalifornia(USC),CaliforniaStateUniversity,Northridge(CSUN),UniversityofNorthCarolinaatChapelHill(UNC),AmericanManagementAssociation(AMA),andtheLosAngelesCountyTrainingAcademy.
Finally,IwishtoextendmygratitudeandappreciationtoCarinaLopez,M.P.H.,forheron-the-jobandoff-workdedication,contributionsandassistanceastheProjectManagerfortheInformationDisseminationInitiativeoftwoofmypublicationseries---“TheLosAngelesCountyBestPracticeCollection:ReliableInformationforEffectiveCommunityHealthPlans,ProgramsandPolicies”,andthe“USCGlobalHealthLeadershipReports:BestPracticeSolutionstoEnhancethePerformanceofHealthSystems”.
M.RICARDOCALDERÓN,M.D.,M.P.H.LosAngeles,California,USA
May2010
Management is doing things right. Leadership is doing the right things -Peter Drucker
“Rather than saying it cannot be done, let’s find a way to get it done”. - M. Ricardo Calderón

PublicHealthLeadershipandManagementforthe21stCentury May2010
7
COURSE INTRODUCTION:
Public Health challenges in the 21st Century include disparities in population health status, new pub-
lic health stakeholders, evolving epidemiology of global disease and injury, increased performance
accountability, and heightened expectations for public health system preparedness (National Public
Health Leadership Institute, University of North Carolina at Chapel Hill, 2003). Public Health systems
must be led by those who have mastery of the skills to mobilize, coordinate, and direct broad col-
laborative actions within complex public health systems (Institute of Medicine, 2002), including the
ability to lead multi-faceted, multi-sectoral and multi-national initiatives. The Public Health Leader-
ship and Management for the 21st Century Course focuses, therefore, on the knowledge, skills
and practical tools needed to direct organizations and small and large-scale initiatives to successful
implementation of institutional vision and overall strategy. It is intended for students who will pursue
leadership positions in public health and health care settings, including the task to build learning
organizations, develop leaders at every level, and create partnerships and networks to maximize indi-
vidual and organizational performance as well as public health system response. As students prepare
for and enter leadership careers, they face a workplace that is very different from the one manag-
ers faced a decade ago and one that will change significantly during their tenures. This course will
provide them with the know-how and skills to transfer self-understanding, critical reasoning, scien-
tific knowledge, and analytical problem finding and solving skills to rapidly changing environments
and public health challenges in the 21st century, including visionary and decision-making skills and
emotional intelligence.
1. LEARNING OUTCOMES
At the completion of this course, students will be equipped with knowledge, skills and abilities to:
• Discuss current challenges to public health and public health leadership
• Demonstrate their understanding of leadership skills needed in the 21st Century
• Assess their individual change style and its impact on leading change
• Explore the role of health departments in working collaboratively in communities
• Apply the principles of leading change and collaborative leadership to their work
• Partner effectively with communities and stakeholders
• Develop institutional vision and strategic plans and assess the extent of their implementation
• Make the distinction between manager/management and leader/leadership
• Describe various leadership styles and articulate their own
• Identify their particular leadership strengths to leverage and areas to target for development

PublicHealthLeadershipandManagementforthe21stCentury May2010
8
• Utilize action learning and reflective practice for ongoing growth as a leader
• Frame and focus attention to adaptive challenges
• Assure development and sharing of organizational learning
• Use systems thinking to lead innovation and change
• Envision the public health future and develop and lead teams to create it
2. COURSE FORMAT & GRADING CRITERIA
This Course is organized into six major Modules –future-focused leadership, leading public health
systems, formulating strategy, leading and managing change, developing public health organizations,
and implementing strategy. Each Module offers an applied training opportunity to gain advanced
knowledge to build executive and managerial skills. Students will engage in lectures, discussions,
explorations, self-study and assessments, case analyses, practice and application.
A range of learning approaches will be used to teach specific elements of the course including, but
not limited to, Lectures (to convey basic body of information), Self-Directed Learning (intensive study,
reading, writing and/or research on particular issues), Audiovisual Materials (to showcase specific
themes or topics), Peer Education (sharing of information, knowledge, skills or experience among stu-
dents), and Class Discussions (in-depth questions and answers). Case Analyses, based on select read-
ings assignments, will be discussed in each of the sessions and will reinforce the learning objectives
of the course. These analyses will integrate leadership and management principles with public health
practice, policies and programs. In addition, they will reflect on lessons learned and best practices of
public health systems in international settings. Students will be expected to attend lectures, participate
and in class discussions, complete reading assignments, prepare two-page concept papers, write proj-
ect papers, make class presentations, and contribute to information sharing and exchange.
Grades will be based on class participation (10%), development of ten two-page concept papers on
related class themes and topics (20% [10 @ 2 points each]), presentation of three ten-page, self-
directed study project papers (30% @ 10 points each]), and a final examination (40%). Classes will
consist of one 3-4 hour session per week for a total of 16 weeks. Each class will consist of approxi-
mately 50-minute lectures followed by corresponding class and team discussions or debates including
individual, team and class exercises and presentations.

PublicHealthLeadershipandManagementforthe21stCentury May2010
9
3. TEACHING PHILOSOPY
My teaching philosophy evolved from many years of teaching and training experience in many coun-
tries both in academic and non-academic settings. As I reflect on my values and beliefs regarding
teaching and learning, I find that my teaching philosophy focuses on three primary goals supported
each by three objectives as follows:
1. Teaching state-of-the-art, practical knowledge, skills and competencies: I am a proponent of (1.1)
Action Learning to address issues, challenges and opportunities. In Action Learning, students try to
deeply understand a real problem, take wise decisions, and reflect on what they have learned. Stu-
dents must develop a commitment to questioning, reflection, action, and learning from such actions
rather than stopping with recommendations for others, and a commitment to “learning” as well as
“results”. Learning is, therefore, as important as the action. I complement this objective with (1.2)
Problem-Based Learning. In order to get students to think, I challenge students to “learn to learn”
by working cooperatively in groups to seek solutions for real world problems. I utilize problems to
engage the students’ curiosity, initiate learning of the subject matter, think critically and analytically,
and find and use appropriate learning resources. I also use (1.3) Diverse Teaching and Learning Tech-
nologies to encourage discussion and interaction on the themes and topics of the course and, more
importantly, to translate theory and ideas into action plans, apply practical knowledge, and deliver
results. My learning approaches include, but are not limited to, Lectures (to convey basic body of in-
formation), Self-Directed Learning (intensive study, reading or research on particular issues), Audiovi-
sual Materials (to showcase specific themes or topics), Peer Education (to share information, knowl-
edge and experience among students), Class Discussions (in-depth questions, answers and debates),
and Case Studies (to reflect on lessons learned and best practices from real life). I expect students
to attend lectures, complete reading assignments, lead and facilitate discussions and debates, make
class presentations, and contribute to information sharing and exchange.
2. Developing the students’ leadership skills: I believe that globalization and the rapid pace of
changes in technology and socioeconomic and political environments require a new teaching and
learning orientation. A student who is trained to become a “leader” will do the “right thing”. A stu-
dent with no leadership training will do “things right”. Doing things right does not necessarily mean
implementing the best or more appropriate or cost-effective strategy. One of my teaching goals is
to develop “student-leaders” with practical knowledge and tools to do the right thing. I integrate
(2.1) Visionary and Systems Thinking Skills to accomplish this. I teach students visionary and future-
focused skills so that they will spend most of their decision-making time looking forward. I combine
this with skills to assess what the problem really is and what its wider and systemic causes are. This
enables students to examine the root causes and forces that shape the issues and the challenges
PublicHealthLeadershipandManagementforthe21stCentury May2010
10
they will face in the workplace. I also try to develop (2.2) an Entrepreneurial Spirit and Life-Long
Learning Skills among students. Students must appreciate that the institutions in which they will
work operate in a fast changing marketplace that seeks products and services to meet emerging
customer, patient or population needs, including 21st public health challenges, emergencies and
threats. In view of rapid scientific and technological progress, I encourage students to take charge
of their own learning and develop a life-long learning attitude. Also, I encourage them to look for
creative ways to connect their institutions to the world around them, exploring and imagining new
forms of (2.3) Collaboration and Teamwork that will support their missions and advance strategic
plans. This includes strategic partnerships and alliances and a deep appreciation of the strength of
diversity to assure a higher level of responsiveness, creativity, innovation and organizational learning.
3. Developing the students’ communication skills: I want all my students to understand that com-
municating with others is an essential skill in business dealings, governmental settings, academic
environments, family affairs, and even in romantic relationships. I engage students in written and
spoken discourse to develop their communications skills to (3.1) Educate and Train Others, (3.2) Pro-
mote Innovation and Change, and (3.3) Articulate and Defend Technical Positions and Approaches.
My goal is to provide students with intrapersonal and interpersonal processing, listening, observa-
tion, questioning, analysis, evaluation and speaking skills. I believe that use of these processes is
developmental and transfers to all areas of life ---home, school, community, work, and beyond.
It is through communication that action learning, problem-based learning, teaching and learning
methodologies, visionary and systems thinking, entrepreneurial spirit and life-long learning, and
collaboration and teamwork occur. Also, I strongly believe that students and adults learn by doing
and, in addition to leading and facilitating class discussions and debates and contributing to infor-
mation sharing and exchange, I expect students to prepare multiple One-Page Concept Papers (brief
but cogent well-written essays to develop research, conceptualization, and information consolida-
tion and proposal skills), make PowerPoint Presentations (to develop presentation, public speaking,
spokesperson and representation skills), and 10-Page Individual/Team Project Papers (to help stu-
dents apply the knowledge and skills acquired through the course curriculum to the work they will
perform in the future as public health practitioners, leaders and educators). I utilize Project Papers
as an opportunity for students to practice being a collaborative leader of change in their future
work environments, either internally within their organizations or externally with other institutions
or the community. It is also a virtual reality experience in which they (a) assume positions of leader-
ship, i.e., Ministers or Directors of Public Health, (b) assess the strengths, weaknesses, threats and
opportunities of a health system, program, policy or service, and (c) develop health system change
recommendations based on the knowledge and skills gained in class. Individual Project Papers also
provide an opportunity to promote and evaluate the knowledge, creativity, resourcefulness, progress
and learning experience of students.

PublicHealthLeadershipandManagementforthe21stCentury May2010
11
Finally, I am committed to providing a learning environment that is exciting, fun, inspiring and
respectful while comprehensive and thorough. More importantly, I strive to create an environment
where students feel valued, appreciated and safe to candidly discuss topics and propose new ideas,
and one that empowers the students and teacher to pursue learning and personal and professional
growth and development.
I. MODULE 1: FUTURE-FOCUSED LEADERSHIP
1. Lecture: Master of Public Health (MPH) Global Health Leadership Track & Interdisciplinary Global Health Training
1.1. Why Global Health Leadership?
a. Track Name & Rationale:
• Uniqueness
• Responsiveness
• Relevance
• Integration
b. Statement of Need: A response to new public health challenges and opportunities
created by:
• Rising inequities in healthcare and health status around the globe
• Changing demographic patterns of disease and epidemiological transitions, and
• Increasing globalization and 21st Century threats
c. Track Purpose: Train students and develop leaders with world-class knowledge and
skills in:
• Public Health Leadership and Management principles and
• Population-based disease prevention and control, in order to
• Improve the health of people around the world, and
• Strengthen global public health systems

PublicHealthLeadershipandManagementforthe21stCentury May2010
12
d. Track Goals: Prepare students to:
• Respond effectively to the full range of 21st Century threats
• Use scientific knowledge and leadership tools to guide public health action, and
• Create multidisciplinary approaches to enhance global public health research, practice and
policy-making
e. Learning Outcomes:
• EXPLAIN the global context in which public health problems occur and the need to respond
to the health consequences of international emergencies
• DESCRIBE how globalization, rising infectious and chronic diseases, and natural and man
made disasters make the health and wellbeing of people of the world increasingly interde-
pendent
• APPRECIATE the increasing influence of determinants arising in foreign countries to any
country’s health and safety
• APPLY leadership and management skills needed in the 21st century to effectively lead lo-
cal, national and global public health systems
• APPLY scientific knowledge and leadership tools and resources to promote health, prevent
illness and fight disease around the world
• UTILIZE lessons learned and best practices to play leadership roles in promoting global
health through improved research, practice and policy-making
• ADVOCATE for multidisciplinary, multisectoral and multinational disease prevention and
control initiatives to improve the health of the people around the world
• PROMOTE the mutual benefits of improving the health status and wellbeing of other
countries
• DESCRIBE the advantages of information sharing and expertise exchange among countries
and international partners
• PROMOTE health system development and reform worldwide through the engagement of
world-wide networks, partnerships and public and private health institutions

PublicHealthLeadershipandManagementforthe21stCentury May2010
13
f. Program Description:

PublicHealthLeadershipandManagementforthe21stCentury May2010
14
1.2. Why Interdisciplinary Global Health Training?
a. Perspective for Discussion:
• Global health problems cross geopolitical boundaries
• Solutions require coordinated interdisciplinary actions by all nations
• Research and training is crucial to address 21st century threats
• Critical to share experiences and lessons learned across nations
b. Emerging Infections:
c. Historical Emerging Infections:
d. Severe Acute Respiratory Syndrome (SARS)
• 32 countries, 8464 cases, 799 deaths (11/102 – 06/17/03 WHO)
• Estimated Economic Costs (reduction in annual GDP): China $7.2B, Hong Kong $3.0 - $6.6 B,
Korea $1.3 - $3.0 B, Taiwan $2.5 – $5.3B
• Regional Cost: $16 – $30 B (NY Times & ADB: SARS Economic Impacts and Implications (Fan,
E.X. May 2001)
• Standard Economic Model: Economic Growth = Health
• New Economic Model: Economic Growth < > Health
1973 ROTAVIRUS 1991 MDR-TB1977 EBOLA VIRUS 1992 CHOLERA EPIDEMIC1977 LEGIONNAIRES’ DISEASE 1994 CRYPTOSPORIDIUM1981 TOXIC SHOCK SYNDROME 1998 HONG KONG BIRD FLUE1982 LYME DISEASE 1999 WEST NILE VIRUS1983 HIV/AIDS 2001 ANTHRAX1983 HELICOBACTER PYLORI 2003 SARS
Year 610 INFLUENZA IN CHINA (SARS?)Year 644 LEPROSYYear 900 SMALLPOX (RHAZES)Year 1348 BLACK DEAQTH (PLAGUE)Year 1495 THE GREAT POX (SYPHILIS)Year 1510 THE RED SICKNESS (SCARLET FEVER)Year 1546 JAIL FEVER (TYPHUS)Year 1557 MALARIAYear 1567 SMALLPOX

PublicHealthLeadershipandManagementforthe21stCentury May2010
15
e. Protecting Health in a Transforming World:
• Preparedness planning
• Collaborative response
• Training and education
• New research agenda
• Proactive communication
• Linkages between disciplines
• Political will
• Expect the unexpected
f. China’s Public Health Training Program: Outcomes Approach Logic Model:

PublicHealthLeadershipandManagementforthe21stCentury May2010
16
g. USC/CCDC Public Health Intelligence and Leadership Develop Program: The inte-
gration of Scientific Knowledge (public health intelligence) and Leadership Skills
• Two Certificate Programs in Public Health Intelligence and Leadership (Summer 2004)
• A Certificate Program in Public Health Leadership & Emergency Response (Fall 2004)
• Seven Certificate Programs in Public Health Leadership & Crisis and Emergency Risk
Communication (Fall 2004 and Winter 2005)
• 1070 top medical, public health, hospital administration directors (Chinese Center for
Disease Control and Prevention and the Ministry of Health) and university professors of China

PublicHealthLeadershipandManagementforthe21stCentury May2010
17

PublicHealthLeadershipandManagementforthe21stCentury May2010
18
h. Public Health Opportunities:
i. Desired Future:
• Increased public health system efficiency
• Enhanced public health emergency response
• Improved global health
2. LECTURE: PUBLIC HEALTH LEADERSHIP FOR THE 21ST CENTURY
2.1. FUTURE-FOCUSED LEADERSHIP
a. Leadership & Managerial Skill Evolution:
Developperformance-basedandaccountabilitystructures
Focusonqualityassuranceinservicedelivery
Ensurepublictrustinpublichealthorganizations
Leadinnovation
Enlargecadreofpublichealthleaders
Leadershiproles
Prioritizeinvestmentstoimprovehealth
Prioritizepoliciesthancanimprovethepublic’shealth
Assureevidence-basedpractices

PublicHealthLeadershipandManagementforthe21stCentury May2010
19
b. The Role of the Leader-Manager:
c. Developing New Perspectives:
• Changing perspectives to facilitate organization and program change
• Creating new perspectives
• Changing mental models
d. Imagination:
• If you do not know where you are going, any road will take you there
e. Leadership Abilities and Practices:
Passionatevision
Externalfocus
Clearvaluesandstrategy
Organizationalalignment
Effectivemanagementofhumancapital
Seamlessexecution
Createavision
Synthesizeknowledge
Becreative,resourceful
Fosterandfacilitatecollaboration
Cultivatesystemsthinkers
Possessentrepreneurialability
Setpriorities
Formcoalitions&buildteams
Mastermanagementtechniques
Actasacolleague,friendandhumanitarian
PublicHealthLeadershipandManagementforthe21stCentury May2010
20
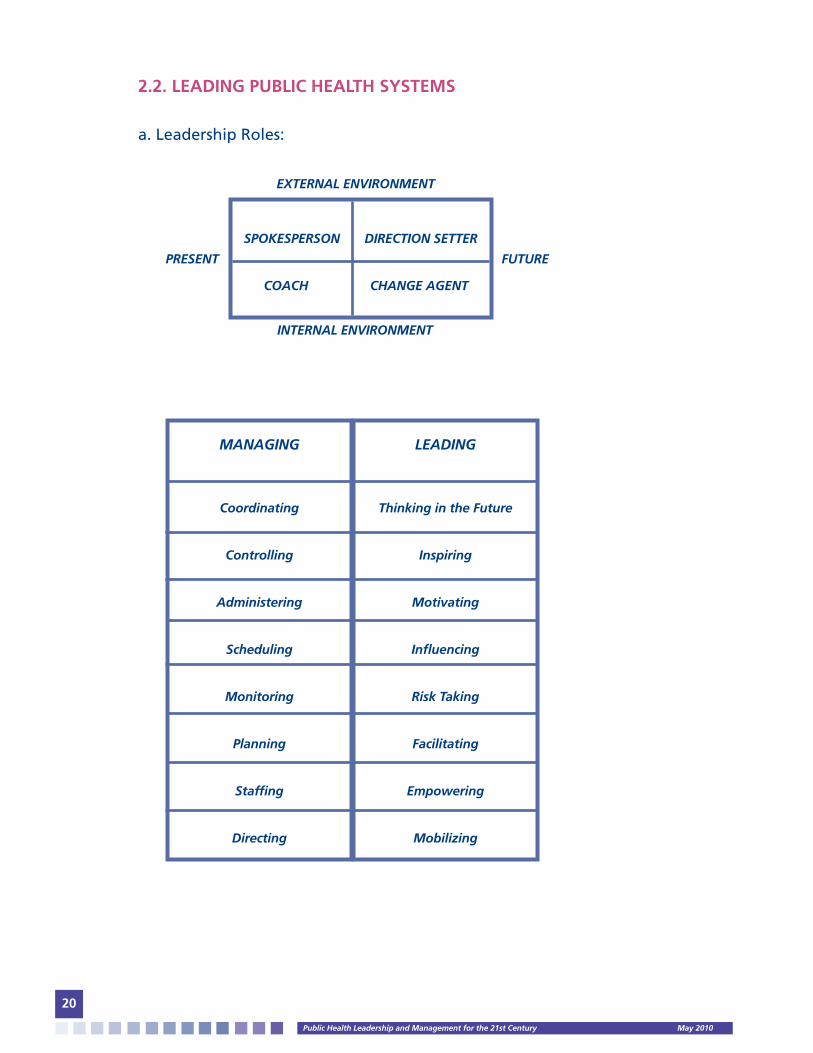
2.2. LEADING PUBLIC HEALTH SYSTEMS
a. Leadership Roles:
SPOKESPERSONDIRECTIONSETTER
COACH CHANGEAGENT
EXTERNALENVIRONMENT
PRESENT FUTURE
INTERNALENVIRONMENT
MANAGING
Coordinating
Controlling
Administering
Scheduling
Monitoring
Planning
Staffing
Directing
LEADING
ThinkingintheFuture
Inspiring
Motivating
Influencing
RiskTaking
Facilitating
Empowering
Mobilizing

PublicHealthLeadershipandManagementforthe21stCentury May2010
21
2.3. FORMULATING STRATEGY
a. Today’s Public Health Challenges:
b. Scientific Examples of Public Health Challenges in China:
• Rapidly emerging disease distribution –infectious respiratory disease to chronic disease—as
major causes of death (prior to SARS
• Unprecedented migration from rural to urban centers –30% to 40% of population in some
cities
• Population disparities and associated mental disease is the greatest economic challenge to
China by 2020 (WHO)
• High levels of anxiety, depression and stress in people who experience either a loss of real
income or a loss of income relative to others in their workplace or neighborhood (USC-CSCS)
• Exposure to foreign media (movies, TV, magazines, music) is associated with an increase in health
risk behavior –smoking, fast food consumption, etc.
Effectivepreparednessandresponseto21stcenturyPH
threats
Emergenceofnewandre-emergenceofolddiseases
ChangingdemographicsPopulationhealthdisparities
Emphasisonaccountabilityandperformance
Governmentandhealthdepartmentreorganization
Needforreliableandtimely
detection,science,communication,integration,
actionandcontainment
Explosionofinformationtechnology
Globalizationandrapidtransportationsystems
Enhancedroleofprevention
Invisibilityofpublichealth
Shiftingpublicexpectations

PublicHealthLeadershipandManagementforthe21stCentury May2010
22
2.4. LEADING AND MANAGING CHANGE
a. Paradigm Shifts:
2.5. DEVELOPING PUBLIC HEALTH ORGANIZATIONS
a. Developing Leaders:
• Treat people with trust and respect (support, recognize and reward staff)
• Build organizational capabilities (created aligned, learning organization; ensure coaching,
counseling, mentoring, training and appraisals)
• Transition management (embrace change; continuously scan horizon)
BehaviorsConsensusPatriarchalExclusiveNeedingfactsCompetitiveSolitaryvisionHierarchicalFunctionalskillsIndividualaccomplishmentsStructuralEpisodicControlAnalysisOutcome
PersonalcapacityDiscoveryEmbracingdiversityHolisticBefriendingambiguityCollaborativeCollectiveunderstanding&sharedvisionFlexible,horizontalLifelonglearningCommunitybuildingRelationalSustainableChaosandcreativitySynthesisProcess
LEADERS
Innovateanddeveloptheorganization
Askwhatandwhy
Eyeonthehorizon(future-oriented)
Seekflexibilityandchange
Problemfinders
Divergentthinkers
Influenceothersbytrust,persuasion&inspiration
Serveandempowerhumanbeings
Dotherightthing(EFFECTIVENESS)
MANAGERS
Maintainandoperatetheorganization
Askhowandwhen
Eyeonthebottomline(present-oriented)
Seekstabilityandcontrol
Problemsolvers
Convergentthinkers
Influenceothersbyrulesandsystems
Deployhumanresources
Dothingsright(EFFICIENCY)
PublicHealthLeadershipandManagementforthe21stCentury May2010
23
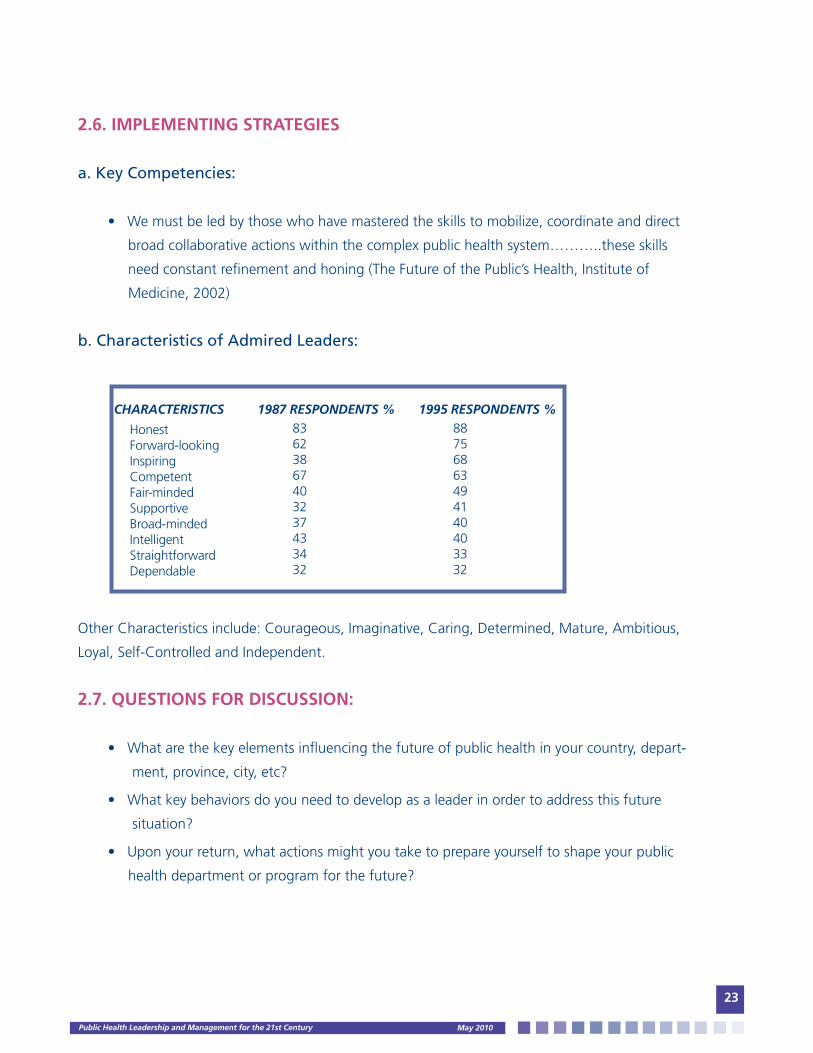
2.6. IMPLEMENTING STRATEGIES
a. Key Competencies:
• We must be led by those who have mastered the skills to mobilize, coordinate and direct
broad collaborative actions within the complex public health system………..these skills
need constant refinement and honing (The Future of the Public’s Health, Institute of
Medicine, 2002)
b. Characteristics of Admired Leaders:
Other Characteristics include: Courageous, Imaginative, Caring, Determined, Mature, Ambitious,
Loyal, Self-Controlled and Independent.
2.7. QUESTIONS FOR DISCUSSION:
• What are the key elements influencing the future of public health in your country, depart-
ment, province, city, etc?
• What key behaviors do you need to develop as a leader in order to address this future
situation?
• Upon your return, what actions might you take to prepare yourself to shape your public
health department or program for the future?
CHARACTERISTICS 1987RESPONDENTS% 1995RESPONDENTS%
HonestForward-lookingInspiringCompetentFair-mindedSupportiveBroad-mindedIntelligentStraightforwardDependable
83623867403237433432
88756863494140403332

PublicHealthLeadershipandManagementforthe21stCentury May2010
24
2.8. ACKNOWLEDGEMENTS:
• Michael F. Kipp, President, Kipp & Associates
• James R. Morgan, CEO, Strategy & Management Dynamics
• A. Paul Bradley Jr., President, The Bradley Group, Inc.
• American Management Association (AMA)
3. TEAM EXERCISE: CREATING INDIVIDUAL AND SHARED VISIONS
Break large group into small teams (5 or 10 people each). Each team appoints:
(1) a facilitator who will coordinate team discussions,
(2) a representative or reporter who will be responsible for later reporting back to the whole large group,
(3) a person(s) who will draw or paint a vision on flipchart paper that will be provided.
The facilitator will coordinate the group’s efforts to reflect or draw an image or idea on a flipchart of the dream
or vision of the team of their institution, community, province, city and/or a specific program or service for the
Year 2010. The facilitator will instruct team members to be creative and not to concern themselves with their
artistic abilities. The result of this process will be a shared vision of good health, quality services, exceptional
performance, a state-or-the-art health department, or any other theme.
All team members come back into the large group and the reporter from each small group will bring their
group’s shared vision to the front of the room, tape it to the wall and highlight images and ideas generated.
The reporter for the second small group will tape their action vision next to the previous groups and repeat
the process. When all shared visions are taped and all group reporters have reported, the result of this process
will be a “gallery of collaborative art” reflecting a variety of end goals, outcomes or horizons resulting from
the best efforts of public health leaders to protect and enhance the health status and wellbeing of individuals,
families, communities and/or the population at large. All program participants form a single line a conduct
a walk-through of the gallery of collective art. Once done, a discussion will take place regarding images and
ideas generated and the importance of visionary skills.
PublicHealthLeadershipandManagementforthe21stCentury May2010
25
Guiding Concepts and/or Questions:
• What an effective institution will look like in the Year 2010?
• What a healthy community will look like in the future?
• How will staff, institutions or communities achieve their vision)?
• How will program or service effectiveness be accomplished?
• Who will participate in the process –staff, institutions, communities, sectors of society?
Time:
• 30-45 minutes
Supplies:
• Flipchart pad and easel, thick markers, crayons and masking tape for each team
4. DISCUSSION: CONCEPT PAPER #1: DEVELOPING A VISIONARY LEADERSHIP APPROACH
5. BIBLIOGRAPHY
a. Required Readings
• Rowitz, Chapters 1, 2 and 3.
• Institute of Medicine of the National Academies: The Future of the Public’s Health. National
Academies Press. Washington, DC: 2003. pp. 1 – 18.
• Heifetz, Ronald A. & Linsky, Marty. The Challenge: In Leadership on the Line. Harvard
Business School Publishing, Boston, MA, 2002. pp. 1 – 31.
• Institute of Medicine of the National Academies: Insuring Americas’ Health: Principles and
Recommendations. National Academies Press. Washington, D.C., 2004. pp. 15 - 65.
• Hesselbein, Frances et al. Leading the Organization of the Future: Chapters 1, 2, 3: In The
Leader of the Future. The Drucker Foundation. San Francisco, CA, 1996. pp. 1 – 19.
• Hesselbein, Frances et al. Leading the Organization of the Future: Chapters 4, 5, 6: In The
Leader of the Future. The Drucker Foundation. San Francisco, CA, 1996. pp. 26 - 59. Institute
of Medicine of the National Academies: The Future of the Public’s Health. National
Academies Press. Washington, DC: 2003. pp. 19 - 45.
• Corrigan, Janet M., et al. Fostering Rapid Advance in Health Care: Learning from Systems
Demonstrations. Institute of Medicine, Washington, D.C. 2003. pp. 1- 26.

PublicHealthLeadershipandManagementforthe21stCentury May2010
26
b. Optional/Recommended Readings:
• Drucker, Peter F., et al. Looking Ahead: Implications of the Present. Harvard Business Review.
September – October 1997. pp. 15 – 27.
• Heifetz, Ronald A. & Linsky, Marty. The Response: Get on the Balcony & Think Politically: In
Leadership on the Line. Harvard Business School Publishing, Boston, MA, 2002. pp 32 – 76.
• Blank, Martin and Dazberger, Jaquieline. Creating and Nurturing Collaboration in
Communities.Washington DC: Institute for Educational Leadership, 1996. pp. 66 – 75.
• Buckinigiham, Marcus & Coffman, Curt. First, Break All the Rules: In What the World’s
Greatest
Managers Do Differently. New York, NY: Simon & Schuster, 1999. pp. 1 – 15.
• Vaill, Peter B. Permanent White Water: In Managing as a Performing Art, New Ideas for a
World of Chaotic Change. Jossey-Bass Publishers. San Francisco, CA. 1989. pp 1 -32.
• Glassman, Alan M. Rethinking Organization Stability as a Determinant for Innovation and
Diffusion. National Institutes of Health. pp. 132 – 146.
• Goleman, Daniel. What Makes a Leader? Harvard Business Review, November-December
1998. pp. 94 – 102.
• Allen, Kathleen E. et al. Rethinking Leadership. Kellogg Leadership Studies Project 1994-1997.
pp.40 – 62.
• Chrislip, David. Collaboration: The New Leadership: in The Healthcare Forum Journal.
November- December 1995, Vol. 38 #6. pp. 1 – 12.
II. MODULE 2: LEADING PUBLIC HEALTH INSTITUTIONS
1. LECTURE: TRANSFORMATIONAL LEADERSHIP:
a. Overview of Session:
• Discussion of leadership experiences and lessons to be learned from them
• Leadership fundamentals to be practiced in all leadership settings
• Leadership approaches to be used in concert in various settings
• Opportunity to set personal leadership objectives

PublicHealthLeadershipandManagementforthe21stCentury May2010
27
b. Management and Leadership:
• Management is about coping with COMPLEXITY TECHNICAL
Planning and budgeting CHANGE
Organizing and staffing
Controlling and problem-solving
• Leadership is about coping with CHANGE ADAPTIVE
Setting a direction CHANGE
Aligning people
Motivating and inspiring
c. What is expected of leaders?
• Improve Performance: Current and future
• Symbolize the Organization: Inside and Outside
d. Your experiences with leadership: Break into buzz groups to discuss:
• What have been your best and worst moments as a leader?
• What are the most important things you have learned about leadership from your
experiences?
e. Leadership fundamentals:
• Integrity
• High expectations
• Learning
These are required no matter what approach to leadership you use!!!
e.1. INTEGRITY:
• The leadership characteristic most often desired by subordinates
• What is integrity?
Being honest, trustworthy, fair, acting on principle
• Why is integrity crucial for leaders?
How can leaders promote integrity in their organizations?
⇓
⇓

PublicHealthLeadershipandManagementforthe21stCentury May2010
28
e.2. HIGH EXPECTATIONS:
• Leaders elicit better performance than subordinates thought possible
• High expectations of leaders can make the difference between a top company and an average
company
• Setting appropriately high expectations requires good judgment
How can anyone with low expectations be a leader?
e.3. LEARNING:
• Leaders promote learning
Current knowledge led to current performance
Learning creates potential for performance improvements
Automobile transmission analogy
• How can leaders learn and help their people to learn?
Without learning, you can’t have high expectations and integrity……..
f. Approaches to Leadership:
• Leader-based
• Relation-based
• Follower-based
g. LEADER-BASED LEADERSHIP:
• Influence in based on charisma, energy and ideas of the leader
• How? By establishing a vision, using symbols and inspiring people
• Can create major change, but may make the organization dependent on the leader

PublicHealthLeadershipandManagementforthe21stCentury May2010
29
h. What is a vision?
• A vivid concept of what an organization could be
• A sign of a leader who is forward-looking and inspiring
• A powerful image that must be communicated and reinforced
• A yardstick for measuring progress
i. Symbols of leadership:
• Communicate messages that cannot be communicated in words
• May either reinforce or distract from values and vision
• Are often perceived even when not intended
k. Symbols:
l. RELATIONSHIP-BASED LEADERSHIP:
• Influence is based on trust, respect and mutual obligation
• How? By building strong relationships
• Addresses differences among people
• Time-consuming
• Creates a lasting ability to get things done
• Relationship-based Leadership is not limited to use with subordinates
MEANING
• Equality or status differences• What is important• Openness to ideas (or not)• Continuity with past (or not)• What do we stand for?
TYPES
• Awards• Furniture• Types of dress• Presence or absence at events• Graphic identity• Where meetings are held

PublicHealthLeadershipandManagementforthe21stCentury May2010
30
m. Factors influencing Relationship-based Leadership:
• You (as boss, subordinate, colleague
• Relationship-building skills
• Effort to build relationship
• Other (as boss, subordinate, colleague)
• Relationship-building skills
• Effort to build relationship
• Similarly (demographic, personality)
• Situation (opportunity to interact, time pressure)
• How have your relationships been shaped?
n. FOLLOWER-BASED LEADERSHIP:
• Leading people to lead themselves
• Develops next generation of leaders
• The leader empowers, coaches, facilitates and gives up control
• Makes the most out of follower capabilities
• Follower capability and commitment is crucial
o. Empowerment:
• Strengthening employees SENSE OF EFFECTIVENESS
• Self-confidence
• Personal control over decisions
• And then granting them the AUTONOMY to assume more responsibility
p. From Leadership on the Line
• “Leadership is an improvisational art. You may have an overarching vision, clear, orienting
values, and even a strategic plan, but what you actually do from moment to moment cannot
be scripted. TO BE EFFECTIVE, YOU MUST RESPOND TO WHAT IS HAPPENNING (page 73)”.
• How accurate is this statement for public health leadership?
• Which leadership approach is most consistent with this requirement?

PublicHealthLeadershipandManagementforthe21stCentury May2010
31
q. Developing and approach to leadership: You should consider:
• Your capabilities
• The capabilities of your followers
• The organization’s needs and culture
r. Setting personal objectives for leadership development:
• Please write down one or two objectives for improving your leadership performance over
the next two months
• You will have the opportunity to share these with the class
s. Acknowledgements:
• Jim Dean, Associate Dean of Executive Education Program, Kenan-Flager Business School,
University of North Carolina, Chapel Hill.
t. Questions and Answers Session
2. INDIVIDUAL SELF-ASSESSMENT EXERCISE: LEADERSHIP AND MANAGEMENT
This is a self-assessment tool based upon ideas presented by Burt Nanus in his book Visionary
Leadership (Jossey Bass Publishers, 1992) and Burn Nanus and Warren Bennis in their book Lead-
ers: The Strategy for Taking Charge (Harper & Row, 1985). The qualities and behaviors of execu-
tives that act in a managerial capacity are listed in the left hand column. The qualities and be-
haviors of executives that act in a leadership capacity are listed in the right hand column. Please
indicate for each pair the approximate percent of time in a typical day (or a week, or a month)
that you devote to each capacity, with each line totaling 100% (see next page).

PublicHealthLeadershipandManagementforthe21stCentury May2010
32
Final Task: Calculate the overall time you spend in managerial and leadership activities and list reasons or
any obstacles that may prevent you from spending more time on leadership.
MANAGEMENT
Maintaining and operating the organization
Scheduling and coordinating (asking how and when)
Focusing on bottom line (present oriented)
Promoting organization stability and control
Problem-solving, dealing with crises
Optimizing resources, maintaining quality
Directing people, seeking compliance
Basing decisions on facts, systems procedures
Deploying human resources, forming teams/programs
Doing things right, seeking efficiency
TOTALS
PERCENT LEADERSHIP
Innovating and developing the organization
Policy and strategy forming (asking what and why)
Focusing on long-term (future oriented)
Promoting flexibility and change
Problem-finding, seeking opportunities
Renewing, transforming the organization
Inspiring people, seeking commitment
Basing decisions on trust, intuition, vision
Serving, developing and empowering people
Doing the right thing, seeking effectiveness
TOTAL
100%
100%
100%
100%
100%
100%
100%
100%
100%
100%
100%
PERCENT

PublicHealthLeadershipandManagementforthe21stCentury May2010
33
3. LECTURE: PUBLIC HEALTH LEADERSHIP PRINCIPLES (PHLP)
a. Concept of Change:
“In a society capable of renewal, LEADERS not only welcome the FUTURE and the changes it
brings but believe they can have a hand in SHAPING that future.
J.W. Garner, Self-Renewal”.
b. 21st Century Challenges:
• IDENTITY CRISIS in public health agencies and professionals
• Public’s LACK OF AWARENESS of the nature and accomplishments of public health
• Parents and friends still ask public health professionals WHAT THEY DO for a living
c. Definition of Leadership:
• Leadership is CREATIVITY IN ACTION
• It is the ability to see the PRESENT in terms of the FUTURE while maintaining respect for the
PAST
d. Public Health Leadership Principles (PHLP):
PHLP #1: The public health infrastructure must be strengthened by utilizing the CORE FUNCTIONS
OF PUBLIC HEALTH and its ESSENTIAL SERVICES as a guide to the change that should occur.

PublicHealthLeadershipandManagementforthe21stCentury May2010
34
PHLP #2: The goal of public health is to IMPROVE THE HEALTH of each person in the community.
PHLP #3. COMMUNITY COALITIONS need to be built to address the community’s public health
needs.
PHLP #4. LOCAL, REGIONAL AND NATIONAL public health leaders must WORK TOGETHER to
protect the health of all citizens regardless of gender, race, ethnicity or socioeconomic status.
PHLP #5. Rational community health planning requires collaboration between public agency
LEADERS AT ALL LEVELS.
PHLP #6. Novice public health leaders must LEARN LEADERSHIP TECHNIQUES AND PRACTICES
from experiences public health leaders.

PublicHealthLeadershipandManagementforthe21stCentury May2010
35
PHLP #7. Leaders, both born and made, must CONTINUOUSLY work to DEVELOP their LEADERSHIP
SKILLS.

PublicHealthLeadershipandManagementforthe21stCentury May2010
36
PHLP #8. Leaders must be committed not only to lifelong learning but to their own PERSONAL
GROWTH.
PHLP #9. PHYSICAL, PSYCHOLOGICAL, EMOTIONAL, EOCNOMIC AND SOCIAL HEALTH are all
elements of the health of a community.
PHLP #10. Public health leaders should THINK GLOBALLY and ACT LOCALLY
PHLP #11. Public health leaders need to be good managers

PublicHealthLeadershipandManagementforthe21stCentury May2010
37
PHLP #12. Public health leaders need to WALK THE WALK (do first what the ask of others).
PHLP #13. Public health leaders need to be PROACTIVE not reactive.

PublicHealthLeadershipandManagementforthe21stCentury May2010
38
PHLP #14. EACH LEVEL of the public health system has a NEED FOR LEADERS.
PHLP #15. Public health leaders must PRACTICE WHAT THEY TEACH.

PublicHealthLeadershipandManagementforthe21stCentury May2010
39

PublicHealthLeadershipandManagementforthe21stCentury May2010
40
e. Questions and Answers Session
4. DISCUSSION: CONCEPT PAPER #2: DEVELOPING EMPOWERED LEADERS
5. LECTURE: SWOT ANALYSIS

PublicHealthLeadershipandManagementforthe21stCentury May2010
41
6. TEAM EXERCISE AND/OR SELF-DIRECTED STUDY PROJECT AND PAPER #1: THE SWOT ANALYSIS
A Needs Assessment is a fundamental component of any Strategic Planning process. This is an ap-
praisal of the key forces that influence the success the organization will have in achieving its mis-
sion and goals. These forces may pose either an opportunity or a threat to the organization, such as
changes in economic conditions, population, technology, environment, or statutes. Some planers call
this element an Environmental Scan. However, many planers use a SWOT Analysis to determine both
internal and external factors that could significantly affect the achievement of the general goals and
objectives
A SWOT Analysis is a strategic planning exercise that gathers information that is used to look at ways
to converge and accentuate Strengths and Opportunities and minimize Weaknesses and Threats. This
is vital to any strategic plan because it allows planners to systematically and coherently steer clear of
obstacles to success in the strategic planning process.
• Strengths are strong attributes or inherent assets;
• Weaknesses represent faults and defects in our programs, services, policies or procedures;
• Opportunities highlight favorable circumstances or chances for progress, expansion or advance
-ment;
• Threats describe situations or risks that delay, stop or damage our image, programs or services.
Team Exercise:
The class conducts a rapid needs assessment of the China CDC, the Ministry of Health or any other
institution. The class is divided into four teams. Each team is responsible for one component of the

PublicHealthLeadershipandManagementforthe21stCentury May2010
42
SWOT Analysis. Each team identifies at least five issues related to each component. Each team
records findings and conclusions on a flip chart and a representative or reporter presents a sum-
mary to the entire class, thus creating a quick SWOT Analysis for teaching, learning and discussion
purposes.
Supplies:
Flipchart pad and easel, thick markers and masking tape for each group.
Time:
30 to 45 minutes including individual team discussions and presentations from 4 reporters.
7. BIBLIOGRAPHY
Required Readings:
• Rowitz, Chapters 4 and 14.
• Hesselbein, Frances et al. Leading the Organization of the Future: Chapters 7 & 8: In The
Leader of the Future. The Drucker Foundation. San Francisco, CA, 1996. pp. 71 - 81.
• Zaleznik, Abraham. Managers and Leaders: Are they Different? Harvard Business Review.
March – April, 1992. pp. 2 - 11.
• Institute of Medicine of the National Academies: The Future of the Public’s Health. National
Academies Press. Washington, DC: 2003. pp. 46 - 95.
• Edenet, Jill et all. Leadership by Example: Coordinating Government Roles in Improving
Health Care Quality. Institute of Medicine, Washington, D.C., 2002. pp. 56 – 128.
• Hesselbein, Frandes et al. Future Leaders in Action: Chapters 9, 10, 11: In The Leader of the
Future. The Drucker Foundation. San Francisco, CA, 1996. pp. 90 – 111.
• Hernandez, Lyla. Editor. Who will keep the Public Healthy? Institute of Medicine,
Washington, D.C., 2002. pp. 1 – 16.
• Pearson, Andrall E. Six Basics for General Managers. Harvard Business Review.
July – August, 1989. pp. 1-8.
• Institute of Medicine of the National Academies: The Future of the Public’s Health. National
Academies Press. Washington, DC: 2003. pp. 97 – 177.

PublicHealthLeadershipandManagementforthe21stCentury May2010
43
Optional/Recommended Readings:
• Longest, Beaufort B., et al. Management and Managers: In Managing Health Services Organiza-
tions and Systems, 4th Edition. Health Professions Press. Baltimore, MD. 2000. pp 1 – 17.
• Katz, Robert L. Skills of an Effective Administrator. Harvard Business Review. September –
October, 1994. pp. 1-12.
• Charan, Ram and Colvin, Geoffrey. Why CEOs Fail. Fortune. June 21, 1999. pp. 69-82.
• Heifetz, Ronald A. & Linsky, Marty. The Response: Hold Steady: In Leadership on the
Line. Harvard Business School Publishing, Boston, MA, 2002. pp 124 – 141.
• Heifetz, Ronald A. & Linsky, Marty. The Response: Orchestrate the Conflict & Give the
Work Back: In Leadership on the Line. Harvard Business School Publishing, Boston, MA, 2002.
pp 102 – 123.
• Goleman, Daniel. What Makes a Leader? Harvard Business Review, November – Decem-
ber 1998. pp. 94 – 102.
• Hersey Paul and Kenneth H Blanchard. 1976. Leader Effectiveness and Adaptability
Description. The 1976 Annual Handbook for Group Facilitators. pp. 1 – 14.
• Kotter, John P. What Leaders Really Do. Harvard Business Review, May – June 1990. pp.
3-11.
III. FORMULATING STRATEGY
1. LECTURE: LEADERSHIP APPLICATIONS IN PUBLIC HEALTH
a. USA Vision for Year 2010: Healthy People in Healthy Communities
b. The Mission of Public Health: “……to fulfill society’s interest in assuring the conditions in
which people can be healthy, The Future of Public Health, Institute of Medicine”.
c. Approach and Rationale (The National Academies: Advisers to the Nation on Science, Engi-
neering and Medicine, and The Institute of Medicine):
• Health is a public good and a social goal of many sectors and communities

PublicHealthLeadershipandManagementforthe21stCentury May2010
44
• Government has fundamental, statutory duty to assure the health of the public, BUT
• Government cannot do it alone
• There is a need for inter-sectoral engagement in partnership with government
d. Areas of Action and Change (The Future of the Public’s Health in the 21st Century, Institute of
Medicine):
• FOCUS on population health including the multiple determinants of health
• STRENGTHEN the governmental public health infrastructure
• BUILD inter-sectoral partnerships
• DEVELOP systems of accountability
• MAKE evidence the foundation of decision-making
• IMPROVE communication
e. Determinants of Population Health

PublicHealthLeadershipandManagementforthe21stCentury May2010
45
f. The Public Health System:
g. Core Functions of Public Health
• ASSESSMENT: identification of health problems
• POLICY DEVELOPMENT: identification of possible solutions
• ASSURANCE: Implementation of solutions (programs and services)
g.1. ASSESSMENT

PublicHealthLeadershipandManagementforthe21stCentury May2010
46
g.2. POLICY DEVELOPMENT
g.3. ASSURANCE

PublicHealthLeadershipandManagementforthe21stCentury May2010
47
h. Core Functions of Public Health and 10 Essential Public Health Services

PublicHealthLeadershipandManagementforthe21stCentury May2010
48
i. Relationship of USA Public Health Approach to Public Health Practice
j. Public Health Leadership Framework for the 21st Century: A SYSTEM FOR SUCCSS

PublicHealthLeadershipandManagementforthe21stCentury May2010
49
k. Questions for Discussion
• What are the three core functions of public health?
• What are the similarities and differences between organizational practices and the essential
services of public health?
• What leadership activities are required to implement the core functions of public health?
l. Acknowledgements:
• Healthy People 2010
• Institute of Medicine
• The National Academies
• Louis Rowitz’ Public Health Leadership
m. Questions and Answers Session
2. CLASS EXERCISE: SYSTEMS THINKING
a. Class Discussion: Systems Thinking

PublicHealthLeadershipandManagementforthe21stCentury May2010
50

PublicHealthLeadershipandManagementforthe21stCentury May2010
51
b. Class Exercise: Systems Thinking
Supplies:
• 4 system puzzles
Time:
• 30 – 45 minutes
Class Exercise:
• The class is divided into three or four groups. Each group is given a Systems Puzzle that must be
assembled as soon as possible. The following discussion is held once all puzzles have been
correctly assembled.
Discussion:
Systems thinking addresses how components of a whole- such as departments in an organization- con-
nect and relate to one another. The whole is the “system” and the components are “sub-systems”. A
major focus of system thinking is the relationships or “forces” within and between sub-systems, as well
as forces acting on the whole system.
Ludwig von Bertalanffy (1901- 1972), early pioneer of general systems theory, was one of the most
important theoretical biologists of the first half of the 20th century. His work has led many others to
view organizations as organisms (rather than machines) having diverse parts that function together as
a whole to maintain overall vitality and activity. When we view an organization in this way, we come
to understand how leaders can influence the qualities of connection and relatedness that influence the
vitality of organizational life.
HOW DO SYSTEMS BEHAVE?
1. Systems behave as though they are persons with lives of their own.
2. Systems regularly act to preserve themselves. They do this by resisting or adapting to
change.

PublicHealthLeadershipandManagementforthe21stCentury May2010
52
3. Systems maintain both external and internal boundaries.
4. Systems are always internally connected.
5. Systems assign specialized roles to their members.
6. Systems develop rules and rituals to bond members to one another and thus to
maintain and preserve the group.
7. What actually happens in a system is what the system intends to happen.
LEADERS USE SYSTEMS THINKING TO…
• Remember that no sub-system exists independent of another. Leaders consider how the
tensions of interconnectedness and interdependence play and influence all sub-systems as
well as the whole system.
• Focus on the “goodness of fit” between members of a system, not on individual strengths
and weakness.
• Regard the actual and potential adaptability of the system, not just what challenges and
problems it faces.
• Consider the states of equilibrium and disequilibrium versus stability.
• Notice that many situations require managing, not solving.
• Regard ambiguity and uncertainty as not only sources of anxiety, but of creativity and growth
too.
• Consider that demands for many “first order” responses may indicate the need for “second
order” responses.
3. DISCUSSION: CONCEPT PAPER #3: BUILDING INTERNAL AND EXTERNAL PARTNERSHIPS

PublicHealthLeadershipandManagementforthe21stCentury May2010
53
4. LECTURE: LEADERSHIP AND THE PLANNING PROCESS
a. Quote:
• “We live in a world where NO ONE IS IN CHARGE. No organization, or institution has the legitimacy,
power, authority, or intelligence to act alone on important public issues and still make substantial head-
way against the problems that threaten us all. J. M. Bryson and B.C. Crosty, Leadership for the Common
Good”.
b. Leadership and Planning:
• No matter what changes occur in the world of public health, PLANNING will occupy much of
the work of their leaders.
• STRATEGIC THINKING SKILLS are essential for all varieties of planning.
• Strategic planning must be driven by the big picture –the leader’s vision of the future.
c. Community Health Planning:
• Use approach that generates INNOVATIVE public health STRATEGIES
• Keep in mind CORE FUNCTIONS, ORGANIZATIONAL PRACTICES AND ESSENTIAL PUBLIC HEALTH
SERVICES.
• Develop outcome scenarios for those engaged in planning to have options to choose from.
d. Planning Steps: Planning does not eliminate change but rather fosters change. Planning is a form
of RATIONAL DECISION MAKING:
• Decide on GOALS AND OBJECTIVES
• Determine CONSTRAINTS
• Figure out what ACTIONS, POLICIES and PROGRAMS to implement
e. Planning Responsibilities: Assessment is a pre-requisite for planning.
• USE core functions of public health as a foundation
• LEARN different planning methodologies
• DETERMINE actions necessary to achieve community health goals and objectives
• USE premising and scenario building to discover innovative public health strategies
• BE INVOLVED in formal planning activities
• CREATE community partnerships to carry out planning
PublicHealthLeadershipandManagementforthe21stCentury May2010
54
f. Planning Models: Planning models, individually or jointly, are all useful for turning a vision into
programs and services.
• Continuous Quality Improvement (CQI)
• Re-engineering
• Re-inventing government
• Strategic Planning
f.1. CONTINUOUS QUALITY IMPROVEMENT
• Related to Total Quality Management (TQM)
• “|The culture of the organization is defined by and supports the constant attainment of
CUSTOMER SATISFACTION through an integrated system of tools techniques and
training, A.V. Feingenbaum”.
f.2. RE-ENGINEERING
• Restructuring of an organization
• “The RAPID AND RADICAL REDESIGN of strategic, value-added business processes –an
the systems, policies, and organizations structures that support them—to OPTIMIZE THE
WORK FLOWS AND PRODUCTIVITY of an organization, Manganelli and Klein”.
f.3. RE-INVENTING GOVERNMENT
• The use of ENTREPRENEURIAL TECHNIQUES by those in the public sector.
• “The fundamental TRANSFORMATION OF PUBLIC SYSTEMS AND ORGANIZATIONS to
create dramatic increases in their effectiveness, efficiency, adaptability, and capacity to
innovate, Osborne and Plastrik”.
f.4. STRATEGIC PLANNING
• Review PARTICIPATORY STRATEGIC PLANNING Lecture

PublicHealthLeadershipandManagementforthe21stCentury May2010
55
g. Strategic Planning Terms:
h. Strategic Planning Guidelines: A Team Process:
• Set a DEALINE
• Consider how to get the PLAN APPROVED
• Create a SCHEDULE for the planning process
• DISSEMINATE the results (plan)
• Decided on techniques to EVALUATE PROCESS
i. Community-Oriented Health Systems Planning
VISION
STRATEGIES
GOALS
MISSION
TACTICS
OBJECTIVES
Community-Oriented Health Systems Planning
COMMUNITY PROVIDERS
NEEDS ASSESSMENT
SYSTEM DESIGN
SYSTEM PERFORMANCE
ASSESSMENT
ORGANIZATIONAL PERFORMANCE
ASSESSMENT
NEEDS ASSESSMENT
SYSTEM DESIGN

PublicHealthLeadershipandManagementforthe21stCentury May2010
56
h. Public Health Leader’s Responsibilities:
• LEARN the benefits of planning
• PERFORM a stakeholder analysis
• EXPAND strategic planning process to community
• REMAIN optimistic and motivate others
• Do homework to PREPARE for each step
• BE REALISTIC about possibilities
• PERFORM assessment of organizational capability
j. Public-Private Partnerships:
• Public health agencies LEAD THE WAY but CANNOT CARY OUT ALL PUBLIC HEALTH
ACTIVITIES needed to protect and improve the health of a community.
• New types of alliances and partnerships:
Joint Ventures
Research sharing
Community-based projects and programs
Semi-structured alliances
k. Public Health Leader’s Responsibilities:
• Develop public and private relationships
• Share power and responsibilities
• Become involved in community activities
• Join local community groups and organizations
• Act to gain the trust of the community
l. Conclusions:
• The NEEDS of the public are constantly CHANGING.
• Public health agencies must RESPOND to the changes.
• The first step in responding adequately is to develop a PLAN OF ACTION.
• Creating a VISION is not enough. A STRATEGY is needed
m. Questions and Answers Session

PublicHealthLeadershipandManagementforthe21stCentury May2010
57
5. LECTURE & CLASS EXERCISE: ASSET-BASED COMMUNITY DEVELOPMENT
a. What determines health?
1. Individual behavior
2. Social relations
3. Physical environment
4. Economic status
5. Access to health care
1 to 4 are least affected by traditional public health interventions but often determine community
health.
b. Link between Associational Communities and Health:
• “SOCIAL CONNECTEDNESS is one of the most powerful determinants of our weel-being,
Robert Putnam, Harvard University”.
c. Health System Tool
PublicHealthLeadershipandManagementforthe21stCentury May2010
58
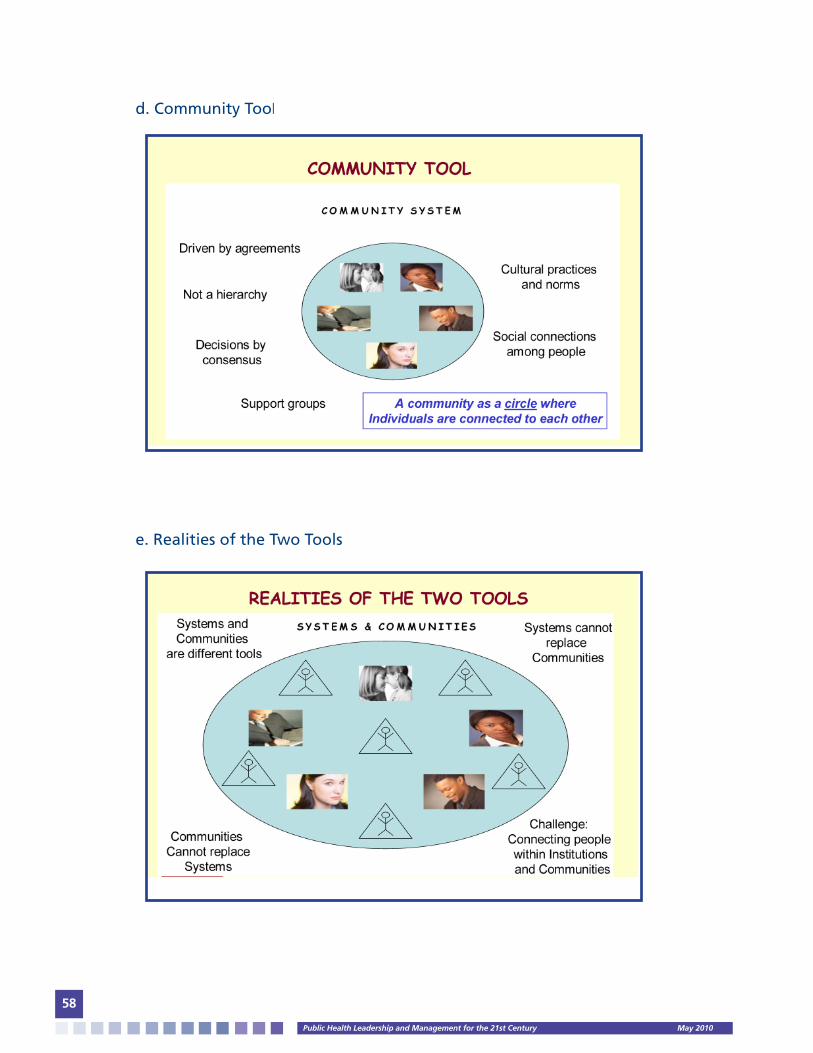
d. Community Tool
e. Realities of the Two Tools

PublicHealthLeadershipandManagementforthe21stCentury May2010
59
f. Two Tools for Well-Being
h. Half Empty or Half Full?

PublicHealthLeadershipandManagementforthe21stCentury May2010
60
i. Asset-Based Community Development:
• “A way of seeing communities as rich in the TALENTS, ABILITIES and CAPABILITIES of its
PEOPLE, VOLUNTARY ASSOCIATIONS and INSTITUTIONS, John McKnight, Northwestern
University”.
j. Local Assets:
• INDIVIDUALS: the talents, gifts, skills and capacities of local residents
• LOCAL CITIZEN ASSOCIATIONS: small, face to face groups where members do the work
• INSTITUTIONS: non-profits, government and businesses that can support community
development work
k. Neighborhood Needs Map

PublicHealthLeadershipandManagementforthe21stCentury May2010
61
l. Neighborhood Assets Map
m. Question? Who are the individuals, local citizen associations and institutions in your
community?
n. Community Needs Matrix
PublicHealthLeadershipandManagementforthe21stCentury May2010
62
o. Community Assets Matrix
p. Community Assets Map:

PublicHealthLeadershipandManagementforthe21stCentury May2010
63
q. Commuinity Assets Map:
6. LECTURE: PARTICIPATORY STRATEGIC PLANNING
a. What is Strategic Planning?
• “An orderly PROCESS for ENVISIONING an organization’s desired FUTURE and determining the
required ACTIONS to attain that future, Strategic Planning Concepts”.
• “Strategic Planning is the PROCESS by which the GUIDING MEMBERS of an organization
ENVISION its future and develop the necessary PROCEDURES and OPERATIONS to achieve that
future, EnTarga Business Planning”.
• “If I ran my BUSINESS like you run the GOVERNMENT, I’d be out of business in less than a year.
Can’t you run the government more like a business, GPRA 1993”.
GIFTS OFINDIVIDUALS
CITIZEN’SASSOCIATIONS
LOCALINSTITUTIONS
TEACHER’SUNION
PTA
SORORITIES
MASTERGARDENERS
SIERRA CLUB
NATIVE PLANT SOCIETY
TENANTASSOCIATION
KARATECLUB
SCOUTS
ST. SOPHIA’SCHURCH
BOOK CLUB
MAY: Artist & Yoga Practitioner
MARK: Bilingual & Carpenter
BRIAN: Coach & Organizer
JUAN: Cook & Soccer Player
KIM: Gardener & Power Walker
LAURIE: Writer & HerbalistLILIA:
Bike riding & Repair
CITYPARKS
SCHOOLDISTRICT
GROCERYSTORES
BOYS & GIRLS CLUB
FARMER’S MARKET
VENDINGMACHINE
OPERATORS
ASIAN-AMERICAN
COMMUNITYCENTER
AMERICAN LUNGASSOCIATION
YMCA
POLICEDEPARTMENT
DAIRYCOUNCIL
PUBLICLIBRARY
FITNESSCENTERS
COMMUNITY ASSETS MAP

PublicHealthLeadershipandManagementforthe21stCentury May2010
64
• “Strategic Planning is a PROCESS by which an organization can become all it wants to
become”.
• “Strategic Planning involves the future impact of present decisions”.
• “Planning is the rational determination of where you are, where you want to go, and how
you will get there”.
b. What is Strategic Planning? Preferred Definition:
• “Strategic Planning is a CONTINUOUS and SYSTEMATIC PROCESS, where PEOPLE make
DECISIONS about intended future OUTCOMES, how outcomes are to be accomplished,
and how SUCCESS is measured and evaluated, Phillip Blackberry 1993”.
c. Key Words:
• Continuous
• Systematic
• Process
• People
• Decisions
• Outcomes
• Success
d. Approaches to Planning:
• REACTICE: Past-oriented
• INACTIVE: Present-oriented
• PREACTIVE: Predict the future
• PROACTIVE: Create the future

PublicHealthLeadershipandManagementforthe21stCentury May2010
65
e. Question? What are the BENEFITS of Strategic Planning?
1. Focus is placed on IMPORTANT THINGS
2. Raise an awareness and impact of CHANGING ENVIRONMENT
3. Analyze the internal business CULTURE
4. Become aware of organization’s POTENTIALS
5. Identify and analyze available OPPORTUNITIES
6. May bring about NEEDED CHANGE
7. Identify STRATEGIC ISSUES
8. Set more REALISTIC OBJECTIVES
9. Obtain better information for DECISION-MAKING
10. Accelerate and improve GROWTH
11. Identify POOR PERFORMING AREAS
12. Gain control of operational PROBLEMS
13. Develop better COMMUNICATIONS
14. A ROAD MAP of location and direction
15. Better INTERNAL COORDINATION of activities
16. A FRAMEWORK for budgets and operational plans
17. Gain a SENSE OF SECURITY among employees
f. Question? What are the pitfalls to Strategic Planning?
1. Jumping from mission formulation to strategy development
2. Top management fails to communicate strategic plan
3. Management rejecting the formal planning mechanism
4. Failing to use the plans as a standard for measuring performance
5. Top management delegating function to a planner
6. Failure to create a climate which is collaborative
7. Not treating planning as a integral part of the whole process
8. Insufficient time spent on planning due to current problems
9. Becoming so formal that process lacks flexibility and creativity
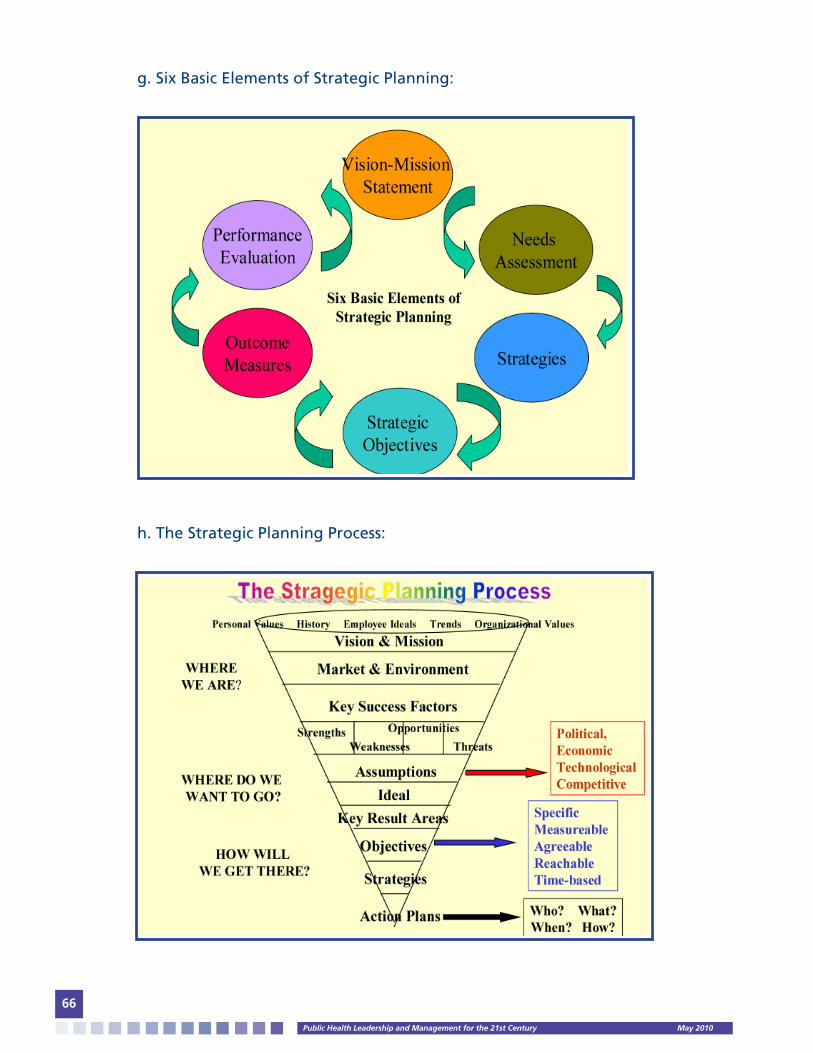
PublicHealthLeadershipandManagementforthe21stCentury May2010
66
g. Six Basic Elements of Strategic Planning:
h. The Strategic Planning Process:
PublicHealthLeadershipandManagementforthe21stCentury May2010
67
i. Questions and Answers Session
7. CLASS DISCUSSION: CONCEPT PAPER #4: BUILDING SUPPORT FOR A STRATEGIC PLAN
8. SELF-DIRECTED STUDY PROJECT & PAPER #2: CREATING A STRATEGIC AND AN IMPLEMENTATION PLAN
Required Readings:
• Rowitz, Chapters 6 and 10 and 15.
• Institute of Medicine of the National Academies: Setting the Course: A Strategic Vision for
Immunizations. Los Angeles, CA., 2003. pp. 1- 38.
• Hamel, Gary. Strategy as Revolution. Harvard Business Review. July – August 1996. pp. 21 – 33.
• Institute of Medicine of the National Academies: The Future of the Public’s Health. National
Academies Press. Washington, DC: 2003. pp. 178 – 211 and 212 – 267.
• Hesselbein, Frandes et al. Future Leaders in Action: Chapters 12, 13, 14 & 15: In The Leader of
the Future. The Drucker Foundation. San Francisco, CA, 1996. pp. 121 – 141.
• David, Jonathan R. et al. Strategic Planning: in Public Health Systems and Emerging Infections.
Institute of Medicine, Washington, D.C., 2000. pp. 1 – 28 and 68 – 74.
• Gray, Daniel H. Uses and Misuses of Strategic Planning. Harvard Business Review.
January – February 1986. pp. 88 – 97.
• Mintzberg, Henry. The Rise and Fall of Strategic Planning. Harvard Business Review,
January – February, 1994. pp 107 – 114.
Optional/Suggested Readings:
• Berkowitz, Eric. 1996. Marketing Strategy: In Essentials of Health Care Marketing. pp. 3 – 38.
• Berry, F.S., & Wechsler, Barton. State Agencies Experience with Strategic Planning. Public
Administration Review. March – April, 1995, Vol. 55, No 2. pp. 159 – 168.
• Ginter, Swayne. Developing Strategic Alternatives and Strategic Choice: In Strategic
Management of Health Care Organizations. 2002. pp. 191-249.
• Collins, J.C., & Porter, J.I. Building Your Company’s Vision. Harvard Business Review.
September – October 1996. pp. 64 – 77.
• Heifetz, Ronald A. & Linsky, Marty. Body and Soul: In Leadership on the Line. Harvard
Business School Publishing, Boston, MA, 2002. pp 163 – 225.
• Ghosh, Shikhar. Making Business Sense of the Internet. Harvard Business Review. March –
April 1998. pp. 16 – 34.

PublicHealthLeadershipandManagementforthe21stCentury May2010
68
• Porter, Michael E. What is Strategy? Harvard Business Review. November – December 1996.
pp. 1 – 22.
IV. LEADING AND MANAGING CHANGE
1. LECTURE: LEADERSHIP AND ORGANIZATIONAL CULTURE
a. The historical leadership question:
• What should the leader of the future be like?
b. What is not new:
• Leadership depends on organizational dynamics:
-Specific Situation
-Task to be performed
-Characteristics of the leader’s subordinates
Organizations have different needs and problems at different stages in their evolution
c. Relationship between the Leader and the Organization:
• Organizations are DYNAMIC SYSTEMS:
-They have a life cycle with unique challenges and implications for leadership behavior:
--ENTREPRENEURS: people who create organizations
--CHIEF EXECUTIVE OFFICERS, PRESIDENTS OR EXECUTIVE DIRECTORS: people who run
organizations
d. Four challenges that will not change:
1. Creating
2. Building
3. Maintaining, and
4. Changing (evolving) organizations to new forms

PublicHealthLeadershipandManagementforthe21stCentury May2010
69
d.1. CREATING: THE LEADER AS ANIMATOR
• Supply the ENERGY to get the organization off the ground:
-Try one approach after another
-Face repeated failures
-Transmit energy to subordinates
• Energy born out of strong PERSONAL CONVICTIONS
-Motivate entrepreneurs
-Builds excitement in others
• Leaders breath life into the organization (ANIMATORS)
d.2. BUILDING: THE LEADER AS CREATOR OF CULTURE
• Entrepreneur’s beliefs, values and basic assumptions are transferred to the mental models of
the subordinates:
-Hiring and keeping similar staff
-Training and building relationships with staff (thinking and feeling)
-Behaving as a role model
• The leader’s personality becomes embedded in the culture of the organization
• CULTURE DEVELOPMENT:
• Once culture is embedded in the organization, it cannot easily be changed
Excellence,quality,
clarity,highproductivity,efficiency,greatcustomerservice,responsiveness,opportunities,reliability,
commitment
Conflicts,inconsistent
policies,unevenpatternsofstrengthsandweaknesses,low
productivityandmorale,frustration,staffturnover
PublicHealthLeadershipandManagementforthe21stCentury May2010
70
d.3. MAINTAINING: THE LEADER AS A SUSTAINER OF CULTURE
• What was good for the YOUNG ORGANIZATION (high energy level and compulsive vision
of its founders: creators and builders) may become a liability as the organization finds that it
needs to:
-Stabilize itself
-Become more efficient
-Deal with the fact that its products have become commodities (services)
-Evolve new generations of leaders for the future
• CULTURE TRANSITION PROBLEMS:
1. The founder-builder does not want to let go of the leadership role or is emotion-
ally incapable of doing so.
2. The founder-builder creates a variety of organizational processes that prevent the
growth of the next generation of leader
• Problem: Prevent or undermine potential successors from learning or taking over
• APPROACH OF SUCCESSFUL LEADERS
-Successful leaders at this stage either:
--Have enough personal insight to GROW with the organization and CHANGE their
own outlook, or
--Recognize their own limitations and permit OTHER FORMS OF
LEADERSHIP to emerge
• Judgment and wisdom are most critical at this stage of organizational evolution

PublicHealthLeadershipandManagementforthe21stCentury May2010
71
d.4. CHANGING: THE LEADER AS CHANGE AGENT
• The rate of change of technological, economic, political and socio-cultural environmental
forces leaders to think like change agents:
-Challenge 1: How to acquire new concepts and skills
-Challenge 2: How to unlearn the things that no longer serve us well
--Anxiety, defensiveness and resistance to change
e. In Problematic Organizations…….
• Leaders need EMOTIONAL STRENGTH to be supportive of the organization while it unlearns pro-
cesses previously successful (PSYCHOLOGICAL SAFETY)
• Leaders need a TRUE UNDERSTANDING of cultural dynamics and the properties of their own orga-
nization culture
• Therefore:
--Leaders cannot arbitrarily change culture
--Leaders evolve culture by building on its strengths and letting weaknesses atrophy
over time
f. Culture Change = Cognitive Redefinition
1. NEW SEMANTICS: redefining individualism
2. BROADEN PERCEPTIONS: expanded mental model of individualism that includes collaborative work
3. NEW JUDGMENT AND EVALUATION STANDARDS: change negative competitive behavior to
positive collaborative behavior
Culture is “changed” ---in reality, EXPANDED, through changes in various key concepts in the mental
models of people who are the main carriers of culture
g. Enlarged and Broadened Mental Models:
Example 1: A native of GUATEMALA becomes American. He/she does not give up being Guatemalan
but adds what it means to be American to his personality.

PublicHealthLeadershipandManagementforthe21stCentury May2010
72
Example 2: An organization built on INDIVIDUAL INCENTIVES does not accept teamwork:
• Reward individuals for helping others and contributing to other projects:
-Deep individualism is acknowledged
-Concept is broadened to include working with others, building trusting relationships
and opening communication across boundaries
h. Culture Transformation:
• A genuine change in the leader’s behavior:
-Walk the Walk and Talk the Talk
• Leaders undergo a personal transformation as part of the total change process
i. Successful Survival Characteristics:
• A COMMITMENET to:
-Learning
-Change
-Staff, communities and stakeholders
-Building a healthy, flexible organization
• Without such culture core organizations cannot survive in the long run
j. A look toward the future:
• BUILDERS have a strong vision, conviction and energy to create an organization
• MAINTAINERS have great judgment, wisdom and skill to develop teams to institutionalize
processes
• CHANGERS have learning ability and personal flexibility to evolve and change organizations

PublicHealthLeadershipandManagementforthe21stCentury May2010
73
k. Perpetual Learning:
• Institutions of the past may be obsolete requiring new forms of governance to be learned
• Learning is an ongoing process not a one-time event
• Perpetual learning and change will remain CONSTANT
l. Characteristics of Future Leaders:
1. Extraordinary levels of perception and insight
2. Extraordinary levels of motivation
3. Emotional strength to manage their own and other’s anxiety
4. Skills in analyzing cultural environments
5. Willingness and ability to involve others and elicit their participation
6. Willingness and ability to share power and control according to people knowledge and skills
m. Leadership: An Emerging Function:
n. The Leader of the Future:
1. Can lead and follow
2. Is central and marginal
3. Is fluid within the hierarchy of the organization
4. Is individualistic and a team player
5. Is a perpetual learner
FUTURE
LeaderswillbePERPETUAL
DIAGNOSTICIANSabletoempowerdifferentpeople
atdifferenttimesandletemergingleadership
flourish
TODAY
Theprocessofappointingleadersisacritical
functionofboardofdirectors,electorates,
governmentagencies,etc.
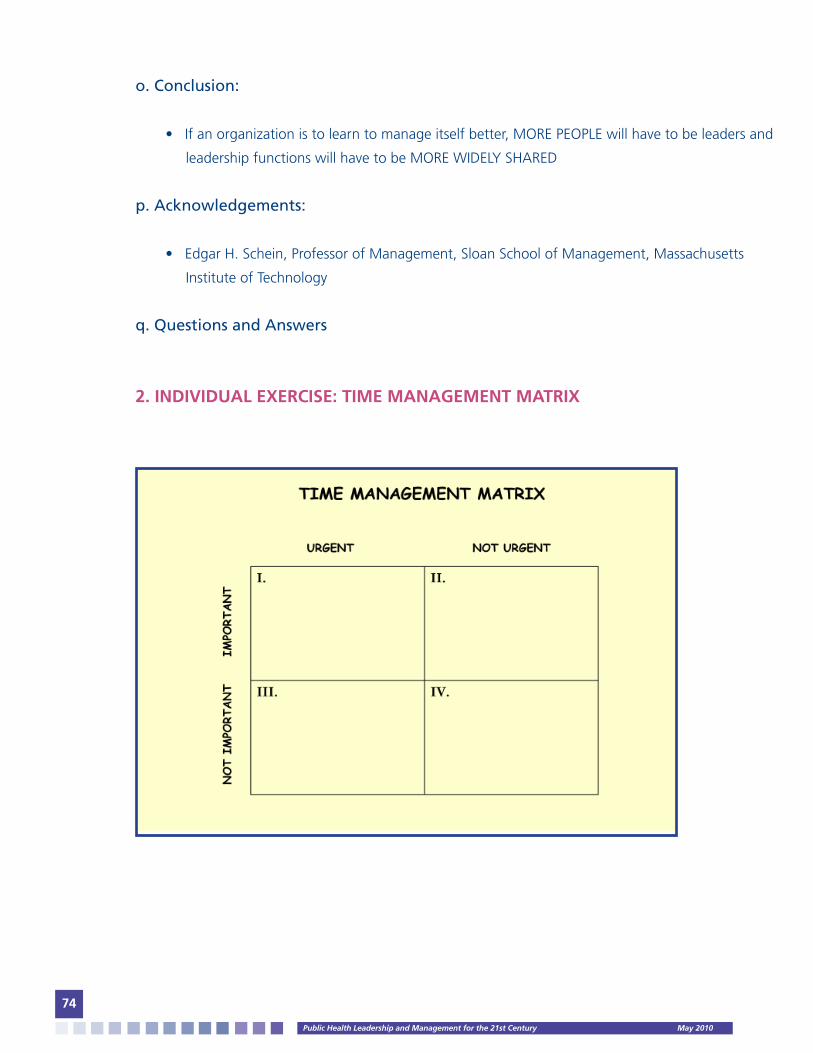
PublicHealthLeadershipandManagementforthe21stCentury May2010
74
o. Conclusion:
• If an organization is to learn to manage itself better, MORE PEOPLE will have to be leaders and
leadership functions will have to be MORE WIDELY SHARED
p. Acknowledgements:
• Edgar H. Schein, Professor of Management, Sloan School of Management, Massachusetts
Institute of Technology
q. Questions and Answers
2. INDIVIDUAL EXERCISE: TIME MANAGEMENT MATRIX

PublicHealthLeadershipandManagementforthe21stCentury May2010
75

PublicHealthLeadershipandManagementforthe21stCentury May2010
76
3. LECTURE: PEACETIME MANAGEMENT AND WARTIME LEADERSHIP
a. Peacetime Conditions:
• Predictable events
• Sense of comfort and control
• No crisis or chaos
• Top-down approach
• Standard procedures
• No major change is needed
• People are content with what already exists
• Change involved gentle “tweaking” of the system
b. Peacetime Management:
• Incremental modification of what already exists
• No major disruption or emotional consequences
• No sense of urgency
• Leaders occupy positions that have power
c. Problem or Challenge:
• Common conflict between those who want to lead others through a major change as though
it were wartime and those who refuse to become followers, insisting that it is still peacetime.
d. Wartime Conditions:
• Change and transition
• Crisis and urgency
• Uncertainty and turbulence
• Fear, apprehension and exhaustion
• Downsizing and ongoing reorganization
• Budget deficits and spending cuts
• Get more done and faster with less staff

PublicHealthLeadershipandManagementforthe21stCentury May2010
77
e. Wartime Conditions in the Health Sector in Los Angeles:
• Health disparities: infant mortality, diabetes, HIV infections
• Overweight and obesity
• Bioterrorism, SARS, emerging infectious disease outbreaks
• 2.8 million emergency room visits per year
• 3.1 million people with no medical insurance
• 35% with no dental insurance
• 236,000 homeless people
f. Wartime Conditions in the Health Sector in Service Planning Area 3 & 4 (or the spe-
cific geographical area where course is being or training is taking place):
• CLASS DISCUSSION:
-What are the public health challenges, issues or problems that make the current health sector
in your jurisdiction a wartime situation?
g. Wartime Leadership:
• Problem or Challenge: We have to learn to become wartime leaders, people who embrace ma-
jor change because they see far more opportunity than threat in turbulence.
Wartime Leadership:

PublicHealthLeadershipandManagementforthe21stCentury May2010
78
Desired Future:
g. Psychological Leadership: An Emotional Bond:
LEADERSGENERATE
Convictionthatthefuturewillbebetter
• FRIGHTENED • VACILLATING• HESITATION• WEAKNESS• FLOUNDERING• COWARDICE
• CYNICISM
PSYCHOLOGICALLEADERSHIP:ANEMOTIONALBOND
• COMPETENCE • CERTAINTY• ACTION• STRENGTH• EXPERTISE• COURAGE
• OPTIMISM

PublicHealthLeadershipandManagementforthe21stCentury May2010
79
h. Leadership Characteristics of the Future
i. A Learning Organization:
• WHAT THEY SAY• TITLE AND POSITION • WHAT THEY CONTROL• GOALS THEY SET
• WHAT THEY DELIVER• EXPERTISE AND COMPETENCE• WHAT THEY SHAPE• MIND SETS THEY BUILD
LEADERSHIPOFTHEFUTURE
PeopleareknownMOREfor...PeopleareknownLESSfor...
Peopleareknownforgreatpersonalcredibilityandorganizationalcapabilities
MOSTDIRECTLEADERSHIP
ALEARNINGORGANIZATION
LESSDIRECTLEADERSHIP MOSTINDIRECTLEADERSHIP
• Commands• Decision about resources & Promotion • Personal Guidance of Individuals & Teams
• Communicates & Inspires Vision & Values • Listens to & Cares for Followers • Leads By Personal Example
• Creates Conditions of Freedom • We Did it Ourselves
• Many Leaders

PublicHealthLeadershipandManagementforthe21stCentury May2010
80
4. CONCEPT PAPER #5: IMPLEMENTING ADAPTIVE LEADERSHIP
5. LECTURE: MANAGING PERSONAL AND ORGANIZATIONAL CHANGE
a. The Way Change Happens:
• The single biggest impetus for change in an organization tends to be a new manager in a key
job who sees that the status quo is unacceptable
b. The Change Grid:
c. Change Style Preferences:
80%LEADERSHIP
•Establishingdirection
•Aligning
•Motivating
•Inspiringpeople
20%MANAGEMENT
•Planning
•Budgeting
•Organizing
•Problemsolving
DENY
RESIST
EXPLORE
COMMIT
EXTERNAL/ENVIRONMENTPAST
PAST FUTURE
FUTURE
INTERNAL/SELF
CONSERVERS
ACCEPTthestructure
PREFERchangethatisincremental
PRAGMATISTS
EXPLOREthestructure
PREFERchangethatisfunctional
ORIGINATORS
CHALLENGEthestructure
PREFERchangethatisexpansive
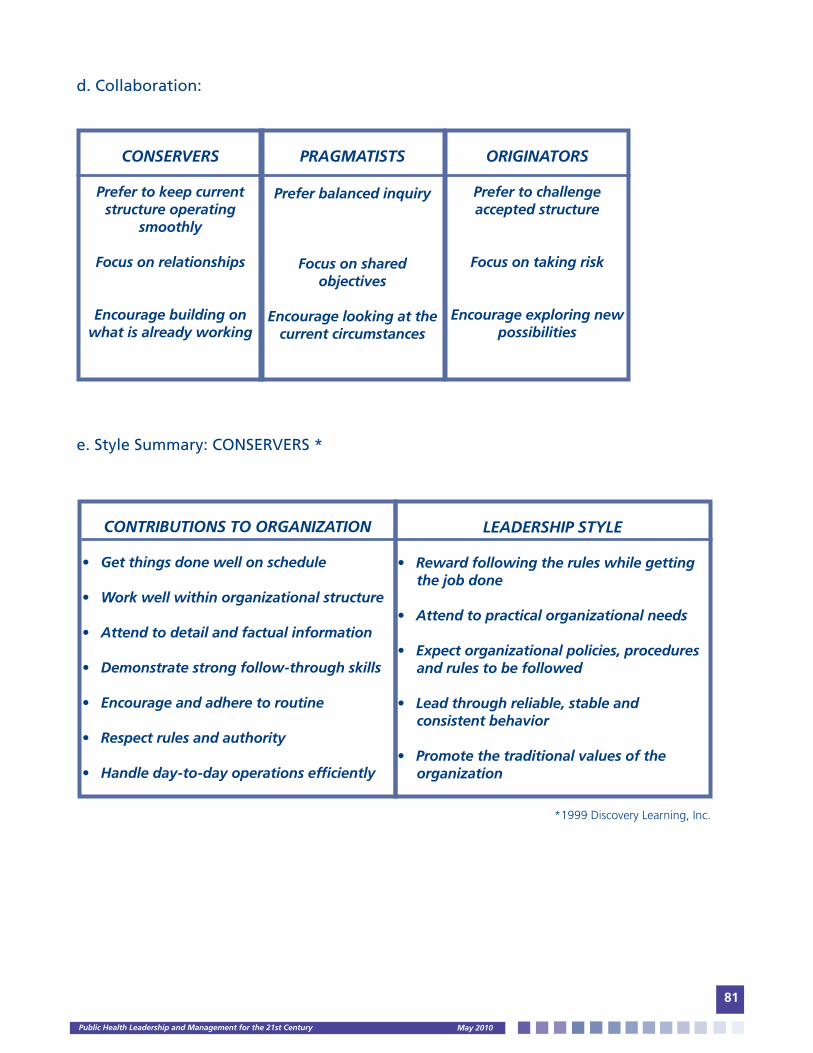
PublicHealthLeadershipandManagementforthe21stCentury May2010
81
CONSERVERS
Prefertokeepcurrentstructureoperating
smoothly
Focusonrelationships
Encouragebuildingonwhatisalreadyworking
PRAGMATISTS
Preferbalancedinquiry
Focusonsharedobjectives
Encouragelookingatthecurrentcircumstances
ORIGINATORS
Prefertochallengeacceptedstructure
Focusontakingrisk
Encourageexploringnewpossibilities
d. Collaboration:
e. Style Summary: CONSERVERS *
*1999 Discovery Learning, Inc.
CONTRIBUTIONSTOORGANIZATION
•Getthingsdonewellonschedule
•Workwellwithinorganizationalstructure
•Attendtodetailandfactualinformation
•Demonstratestrongfollow-throughskills
•Encourageandadheretoroutine
•Respectrulesandauthority
•Handleday-to-dayoperationsefficiently
LEADERSHIPSTYLE
•Rewardfollowingtheruleswhilegettingthejobdone
•Attendtopracticalorganizationalneeds
•Expectorganizationalpolicies,proceduresandrulestobefollowed
•Leadthroughreliable,stableandconsistentbehavior
•Promotethetraditionalvaluesoftheorganization

PublicHealthLeadershipandManagementforthe21stCentury May2010
82
f. Style Summary: PRAGMATISTS *
CONTRIBUTIONSTOORGANIZATION
•Addressneedsastheyarise
•Getthingsdoneinspiteoftherules,notbecauseofthem
•Negotiateandencouragecooperationandcompromise
•Takearealisticandpracticalapproach
•Drawpeopletogetheraroundacommonpurpose
•Organizeideasintoaction
•Haveshortandlong-rangeperspectives
LEADERSHIPSTYLE
•Facilitateproblemsolvingamongpeople
•Useandadaptpastexperiencestosolvecurrentproblems
•Buildcooperationratherthanexpectingit
•Useafacilitativeapproachinmanagingpeopleandprojects
•Encouragetheorganizationtohavecongruencebetweenvaluesandactions
*1999 Discovery Learning, Inc.
g. Style Summary: ORIGINATORS *
CONTRIBUTIONSTOORGANIZATION
•Understandcomplexproblems
•Bringstrongconceptualanddesignskills
•Pushtheorganizationtounderstandthesystemasawhole
•Supportandencouragerisktakingbehavior
•Providefuture-orientedinsightsandvision
•Serveascatalystsforchange
•Initiativenewideas,projectsandactivities
LEADERSHIPSTYLE
•Catalystsforsystemicchange
•Energeticandenthusiastic
•Providelong-rangevision
•Conceptualizeandbuildnewmodels
•Constantlyreorganizethewholesystem
•Liketobeinchargeofthestart-upphase
•Preferuniqueleadershiprolestoconventionalroles
•Managemorethanonetaskathesametime
*1999 Discovery Learning, Inc.

PublicHealthLeadershipandManagementforthe21stCentury May2010
83
h. Organizational Change:
• Leaders alter the way their organizations do business to cope with CHANGE:
-Total Quality Management
-Reengineering
-Reinventing Government
-Mergers and Acquisitions
-Turnarounds
• No organization ---large or small, local or global—is immune to change
i. Eight Steps to Transform an Organization:
1. Establish a sense of URGENCY
2. Form a powerful guiding COALITION
3. Create a VISION
4. COMMUNICATE the vision
5. EMPOWER OTHERS to act on the vision
6. Plan for and create SHORT TERM WINS
7. CONSOLIDATE IMPROVEMENTS and produce still more change
8. INSTITUTIONALIZE new approaches
• Leading by example is essential to communicating a vision
• Leaders balance short-term results with long-term vision
j. Four Sources of Failure:
1. Writing a memo instead of lighting a fire
2. Talking too much and saying too little
3. Declaring victory before the game is over
4. Looking for someone to blame in the wrong places
• These common mistakes suggest THREE KEY TASKS FOR CHANGE LEADERS
j.1. TASK #1: MANAGING MULTIPLE TIME LINES
• TIME: key strategic resource
• Meaningful change takes time

PublicHealthLeadershipandManagementforthe21stCentury May2010
84
• Create Short-Term Wins
--Effective leaders make organizational change an ongoing, multiphase process
j.2. TASK #2: BUILDING COALITIONS
• Engaging the RIGHT TALENT
• Growing the COALITION strategically
• Working as a TEAM, not just a collection of individuals
--Leaders face resistance and must win the support of employees, partners, customers and
investors
j.3. TASK #3: CREATING A VISION
• CLEAR intention
• APPEALING to stakeholders
• AMBITIOUS yet attainable
--A vision of the future is more emotional than rational
k. CONCLUSION:
• Leaders exist at all levels of an organization
• They are interested in a noble cause
• They see things with fresh eyes and challenge the status quo
• They connect people’s everyday work to a larger purpose
• They continue to take risks and are open to people and ideas
• They are driven by goals bigger than what any individual can accomplish and invest tremendous
talent, energy and caring in their change efforts
• However, the most notable trait of great change leaders is their quest for learning.
l. Questions and Answers Session.

PublicHealthLeadershipandManagementforthe21stCentury May2010
85
6. CASE STUDY: THE U.S. CENTER FOR DISEASE PREVENTION AND CONTROL (CDC) FUTURES INITIATIVE
a. The Futures Initiative: Achieving Health Impact
b. Why Change Now?
• Aging population
• Emerging global infectious diseases
• Obesity
• Development of public health workforce and infrastructure
• Health disparities
c. Strategic Imperatives:
• Health impact
• CDC will be a customer-centric organization
• Public health research
• Leadership for the nation’s health system
• Global health
• Effectiveness and accountability
d. Health Protection Goals:
• PREPAREDNESS: People in all communities will be protected from infectious, environmental and
terrorist threats
• HEALTH PROMOTION AND PREVENTION OF DISEASE, INJURY AND DISABILITY: All people will
achieve their optimal lifespan with the best possible quality of health in every stage of life
e. Organizational Design Principles:
• Strategy and goals derive from population health assessments (customers’ health) to achieve
health impact
• Strategy and goals drive agency’s priorities and allocations
• Emphasis on research and innovation
• Health protection “marketing”
• Consolidation of business and other cross cutting services

PublicHealthLeadershipandManagementforthe21stCentury May2010
86
f. Life-Stages
• INFANT: By 2015, the U.S. is one of five countries with the highest rates of infant survival (Baseline
28th, 1999).
• CHILD: By 2015, mortality is reduced 20%, saving an additional 800 lives per year
(NCHS Baseline).
• TEEN: By 2015, at least 95% of adolescents practice behaviors which protect them from illness
and injury now and in the future (NHIS Baseline)
• ADULT: By 2015, at least 90% of adults have a healthy weight (NHANES Baseline)
• SENIOR: By 2015, average lifespan of older Americans is increased by 2 years
g. The New CDC Organizational Chart

PublicHealthLeadershipandManagementforthe21stCentury May2010
87
h. Coordinating Center Roles
• Minimize silos
• Identify and capitalize on opportunities for coordination of research
• Decrease duplication and redundant activities
• Provide leadership, management and accountability for cross-center goals
i. Center Roles:
• Foundation of CDC’s scientific knowledge
• Accountable for quality of programs
• Meet statutory requirements
• Maintain center’s identities and disease prevention loci
j. CDC’s Futures:
FROM
Focus on process
Primary focus on infectious disease and preparedness
Disease specific, fragmented global approach
Inefficient work processes
Silos organization
No overall measure of success
Lack of customer segmentation
Limited partner capacity (state and local health departments)
Minimal applied research
Fragmented approach to customers and partners
Difficult to do business with
TO
Focus on health impact
Primary focus on infectious disease, preparedness and prevention
Comprehensive integrated global approach
Efficient work processes
Integrated coordinating centers (maintaining specialization)
Clearly articulated goals and performance measurement
Segmented customer approach
Strong partner network: (a) revitalized state and local health departments, and (b) media, business, health care delivery, schools, communities
Increase external/internal agenda
Integrated approach to customers and partners
Easy to do business with (standard of good goverenment)

PublicHealthLeadershipandManagementforthe21stCentury May2010
88
k. CDC’s Futures Initiative: VISION: IMAGINE A TIME WHEN:
• Every infant is born healthy
• All children go to school safe, healthy and ready to learn
• All people have the knowledge, ability and support to make healthy choices
• All people live in communities that are protected from infectious, environmental and terrorism
health threats
• All people live their full life expectancy and achieve lifelong independence
• All people are satisfied with their health status
l. Communicate:
• Futures Initiative: IMPROVING HEALTH IMPACT
• http://www.cdc.gov/futures
m. Questions and Answers Session
7. LECTURE: SERVANT LEADERSHIP:
a. Questions:
• What is Leadership? What is Servant Leadership?
b. Becoming a Servant Leader: Do you have what it takes? Ten Principles of Servant
Leadership:
• Listening
• Empathy
• Healing
• Awareness
• Persuasion
• Conceptualization
• Foresight
• Stewardship
• Commitment to the Growth of People
• Building community

PublicHealthLeadershipandManagementforthe21stCentury May2010
89
c. The Leader Who Serves:
d. Servant Leaders: Characteristics
• Listen and learn from those they lead
• Work at making themselves available
• Their door is always open
• Talk and listen to people at all levels of the organization
• Walk a mile in the other person’s shoes
• Become frantic learners
• Avoid the trap of success –the arrogance of ignorance
• Promote diversity recognizing people’s differences strengthens the group
• Are value-driven and performance-oriented
• Lead people to do things the right way and to do the right thing
• Acknowledge no one person can accomplish the task alone
WILLTHELEADERPLEASESTANDUP?
NOT
•Personwithmostdistinguishedtitle
•Highestpaidpersoninthegroup
•Personwithbestcarorhome
•Personwhopromoteshim/herself
•TheAdministrator
•Thetaker
•Thetalker
BUT
•Rolemodel
•Risktaker
•Servant
•Promoterofothers
•Theinitiator
•Thegiver
•Thelistener
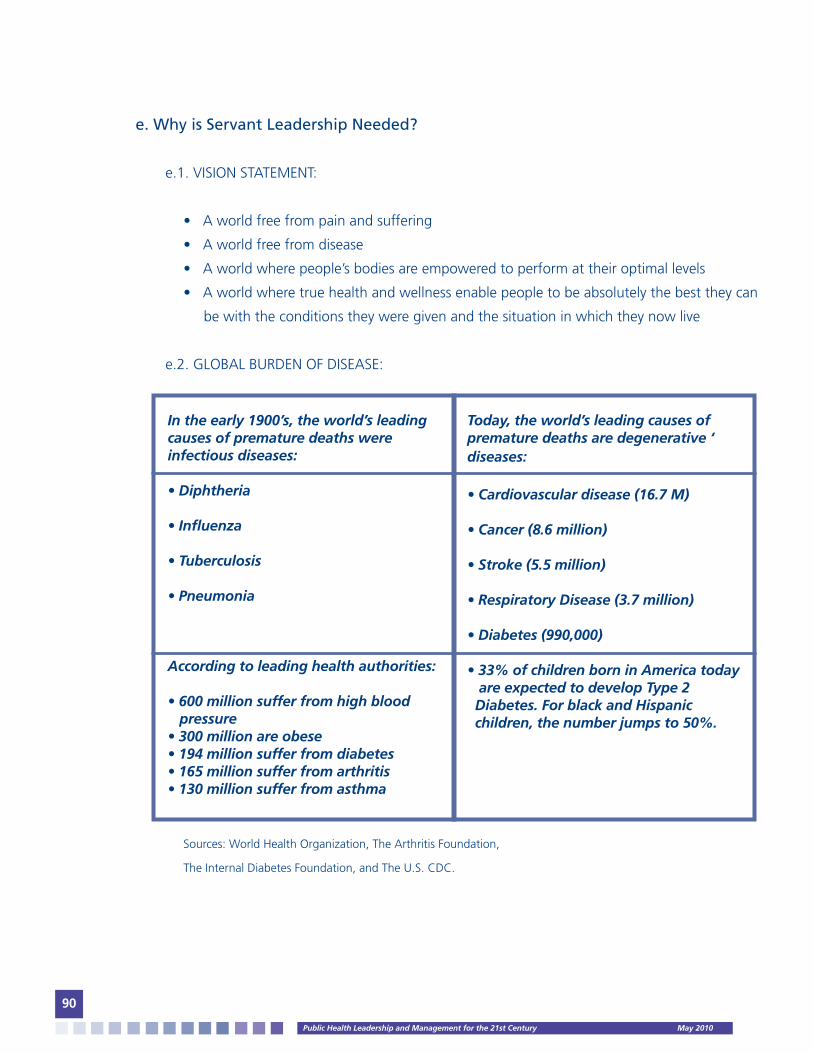
PublicHealthLeadershipandManagementforthe21stCentury May2010
90
e. Why is Servant Leadership Needed?
e.1. VISION STATEMENT:
• A world free from pain and suffering
• A world free from disease
• A world where people’s bodies are empowered to perform at their optimal levels
• A world where true health and wellness enable people to be absolutely the best they can
be with the conditions they were given and the situation in which they now live
e.2. GLOBAL BURDEN OF DISEASE:
Sources: World Health Organization, The Arthritis Foundation,
The Internal Diabetes Foundation, and The U.S. CDC.
Intheearly1900’s,theworld’sleadingcausesofprematuredeathswereinfectiousdiseases:
•Diphtheria
•Influenza
•Tuberculosis
•Pneumonia
Accordingtoleadinghealthauthorities:
•600millionsufferfromhighbloodpressure•300millionareobese•194millionsufferfromdiabetes•165millionsufferfromarthritis•130millionsufferfromasthma
Today,theworld’sleadingcausesofprematuredeathsaredegenerative‘diseases:•Cardiovasculardisease(16.7M)
•Cancer(8.6million)
•Stroke(5.5million)
•RespiratoryDisease(3.7million)
•Diabetes(990,000)
•33%ofchildrenborninAmericatodayareexpectedtodevelopType2Diabetes.ForblackandHispanicchildren,thenumberjumpsto50%.

PublicHealthLeadershipandManagementforthe21stCentury May2010
91
e.3. MAIN CHRONIC DEGERATIVE CONDITIONS:
• Heart disease
• Cancer
• Stroke
• Diabetes
• Osteoporosis
• Arthritis
• Alzherimer’s
• Obesity
e.4. CHANGE IN MENTAL MODEL:
e.5. DEFINING THE PROBLEM: GLOBAL
• 1/10 people (10%): World Mortality: INJURIES
• 3/10 people (30%): World Mortality: INFECTIOUS DISEASES
• 6/10 people (60%): World Mortality: CHRONIC DISEASES
• 7/10 people (70%): USA Mortality: CHRONIC DISEASES
• 8/10 people (80%): Los Angeles Mortality: CHRONIC DISEASES
e.5. DEFINING THE PROBLEM: MACRO
• Government has a duty to assure the public’s health
• Government cannot do it alone, other sectors have a role to play
• Need for inter-sectoral engagement
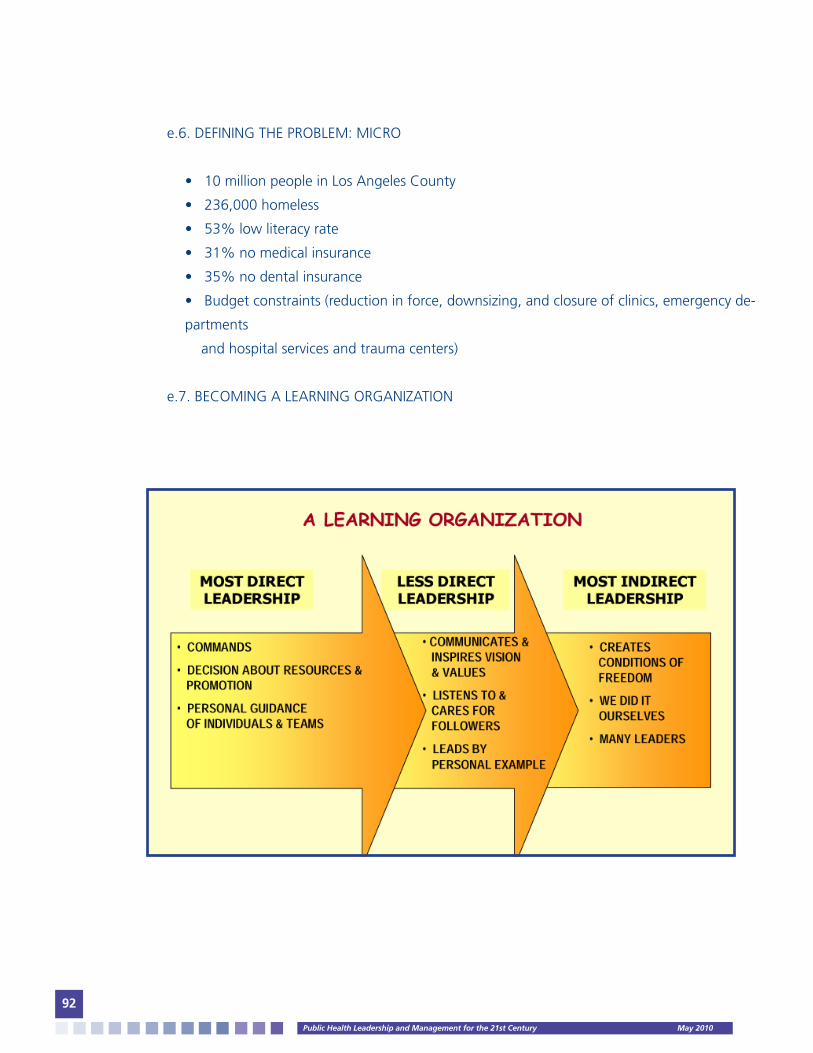
PublicHealthLeadershipandManagementforthe21stCentury May2010
92
e.6. DEFINING THE PROBLEM: MICRO
• 10 million people in Los Angeles County
• 236,000 homeless
• 53% low literacy rate
• 31% no medical insurance
• 35% no dental insurance
• Budget constraints (reduction in force, downsizing, and closure of clinics, emergency de-
partments
and hospital services and trauma centers)
e.7. BECOMING A LEARNING ORGANIZATION

PublicHealthLeadershipandManagementforthe21stCentury May2010
93
e.8. SPA 3 & 4 ORGANIZATIONAL CHART (Service Planning Area 3 (San Gabriel Valley) and Service
Planning Area 4 (Metropolitan Los Angeles)

PublicHealthLeadershipandManagementforthe21stCentury May2010
94
f. Questions and Answers Session
8. CLASS DISCUSSION: CONCEPT PAPER #6: COMMUNICATING CHANGE
9. BIBLIOGRAPHY
Required Readings:
• Rowitz, Chapter 11 and 12.
• Labovitz, George et al. The New Leadership: Taking Charge of Change. Organizational Dy-
namics, Inc. Burlington, MA. 2000. pp. 1 - 8.
• Institute of Medicine of the National Academies: Transforming Institutional Climate to En-
hance Diversity: in In the Nation’s Compelling Interest: Ensuring Diversity in the Health Care
Worforce. Washington, D.C. 123 – 152.
• Hesselbein, Frandes et al. Learning to Lead for Tomorrow: Chapters 16, 17, 18, & 19: In The
Leader of the Future. The Drucker Foundation. San Francisco, CA, 1996. pp. 149 – 189. Institute
of Medicine of the National Academies: The Future of the Public’s Health. National Academies
Press. Washington, DC: 2003. pp. 268 – 306.
• Institute of Medicine of the National Academies: The Future of the Public’s Health. National
Academies Press. Washington, DC: 2003. pp. 307 – 357.
• Hesselbein, Frandes et al. Learning to Lead for Tomorrow: Chapters 20, 21, 22, 23: In The
Leader of the Future. The Drucker Foundation. San Francisco, CA, 1996. pp. 199 – 227.
• Kohn, Linda T. Academic Health Centers: Leading Change in the 21st Century. Institute of
Medicine, Washington, D.C., 2003. pp. 1 – 20 and 87 – 110.
• Duck, Jeanie D. Managing Change: The Art of Balancing. Harvard Business Review. 1993.
71(6):109-118.
Optional/Suggested Readings:
• Kotter, John P. Leading Change: Why Transformation Efforts Fail. Harvard Business Review
1995. 73(2): 59-67.
• Conger, Jay A., et al. Leader’s Change Handbook: An Essential Guide to Setting Direction and
Taking Action. San Francisco, CA. Jossey-Bass Publishers, 1999. pp. 1 – 45.
• National Institutes of Health. Accountability, Administration and Leadership: Organizational
Change to Meet New Challenges: in Enhancing the Vitality of the National Institutes of Health:.
Bethesda, MD., 2003. pp. 102- 120.
• Kotter, John P. What Effective Managers Really Do. Harvard Business Review. March – April

PublicHealthLeadershipandManagementforthe21stCentury May2010
95
1999. pp. 3 – 12.
• Deal, Terrence E. and Bolman, Lee G. Reframing Organizations: Artistry, Choice and Leadership.
Jossey-Bass Publishers, San Francisco, CA. pp. 176 – 211.
• Kanter, Rosabeth Moss. Mastering Change in Learning Organizations. 2002. pp. 65 – 76.
• Sull, Donald N. Why Good Companies Go Bad. Harvard Business Review. July – August 1999.
pp. 73 – 85.
V. DEVELOPING PUBLIC HEALTH ORGANIZATIONS
1. LECTURE: BUILDING A LEARNING ORGANIZATION
a. Old Truisms and Refrains:
• No significant change occurs unless it is driven from the TOP
• There is no point in starting unless the DIRECTOR is on board
• Nothing will happen without TOP-MANAGEMENT BUY-IN
--Status Quo Mentality = The Way Things Are
b. Two Views of Leadership: View #1
• Only top management can initiate change
-Unwillingness to give up a familiar mental model
-self-protection (hold someone else responsible)
c. Two Views of Leadership: View #2
• Little significant change can occur if it is driven from the top
-Compliance
-Commitment
• There is no substitute for commitment in bringing about change

PublicHealthLeadershipandManagementforthe21stCentury May2010
96
d. Top Management Approaches and Outcomes:
e. Enhanced Learning Capabilities:
• Systems thinking
• Improving mental models
• Fostering dialogue
• Nurturing personal vision
• Building shared visions
--Leaders lead through developing new skills, capabilities and understandings
f. Three Essential Types of Leaders:
f.1. LOCAL LINE LEADERS:
-Undertake meaningful experiments to test whether new learning capabilities lead to
improved business results
--Designers
--Teachers
--Stewards
-There is no better way to learn than to teach
TOP-MANAGEMENTAPPROACH
• Reorganization
• Downsizing
• Reengineering programs
• Cost reduction programs
OUTCOMESMANAGEMENTFAILSDUETO:
• Fear and defensiveness
• No imagination or commitment
• No change in the way people think of understanding of trust and interdependence
• No enhancement of intelligence and skills

PublicHealthLeadershipandManagementforthe21stCentury May2010
97
f.2. EXECUTIVE LEADERS:
• Support line leaders
• Develop learning infrastructures
• Lead by example
--Protectors
--Mentors
--Thinking Partners
• Building Operating Environment for Learning:
-Executive Leaders:
--Articulate guiding ideas
--Develop learning infrastructure
--Create environment conducive to change
--Build self-directed work teams
• Leaders embrace staff empowerment
f.3. INTERNAL NETWORKERS
• Messengers and communicators of ideas
• Move freely about the organization
• Find people who want change
• Aid in diffusion of new learning
-No power is power
g. Question for Discussion or Class Exercise:
• Who are the LOCAL LINE LEADERS, EXECUTIVE LEADERS and INTERNAL NETWORKERS in your
organization?

PublicHealthLeadershipandManagementforthe21stCentury May2010
98
h. Conclusion
• The challenges of SYSTEMIC CHANGE where hierarchy is inadequate will push organizations
to NEW FORMS OF LEADERSHIP based on new principles
• These challenges cannot be met by isolated heroic leaders. They will require a unique mix of
DIFFERENT PEOPLE, in DIFFERENT POSITIONS, who LEAD IN DIFFERENT WAYS.
LOCALLINELEADERS
EXECUTIVELEADERS
INTERNALNETWORKERS
LOCALLINELEADERS
Supervisors,chiefs,headsofprograms,projectsorunits
EXECUTIVELEADERS
Ministers,directors,deputydirectors
INTERNALNETWORKERS
Seniormanagers,projectmanagers,co-facilitators,
learninghistorians,internalconsultants,trainers,personnel
staff,front-lineworkers

PublicHealthLeadershipandManagementforthe21stCentury May2010
99
i. Acknowledgements:
• Peter M. Senge, Director, Center for Organizational Learning, Sloan School of Management,
Massachusetts Institute of Technology
j. Questions and Answers Session
2. LECTURE: CREATING ORGANIZATIONS WITH MANY LEADERS
a. LAO TSU:
“The very highest leader is barely known by men
Then comes the leader they know and love
Then the leader they fear
Then the leader they despise
The leader who does not trust enough will not be trusted
When actions are performed without unnecessary speech, the people say,
WE DID IT OURSELVES”
b. A Learning Organization:

PublicHealthLeadershipandManagementforthe21stCentury May2010
100
c. Three Approaches to Empowering Many Leaders:
c.1. DELEGATING WITHIN A TRADITIONALLY HIERARCHY
• Limited scope for big-picture or cross-functional thinking
• Delegation is a good first step, but it does not fully meet the needs of information-age
organizations
c.2. CREATING COMMUNITY
• Sense of freedom
• Elective participation
• Common worth
• Information sharing
• Appreciation for gifts of ideas, courage and self-appointed leadership
-Community occurs most easily when FREE PEOPLE with some sense of EQUAL WORTH join
together VOLUNTARILY for a COMMON ENTERPRISE
c.3. LIBERATING THE SPIRIT OF ENTERPRISE
• Innovating
• Seeing things in new ways
• Changing the ways in which things are done
• Replacing hierarchy with indirect methods of leadership
--Greater freedom
--More accurate resource allocation
--Focus on the common good
-Leaders that create a SELF-ORGANIZING SYSTEM motivate followers to excel and
serve people
d. Models of New Forms of Leadership:
• Successful Nations (astounding economic growth after the introduction of free markets)
-China -Singapore
-South Korea -Peru
-Chile

PublicHealthLeadershipandManagementforthe21stCentury May2010
101
.e. Current Debate:
• Information-age leaders will change the debate to USERS CHOICE: Customer-focused service
f. Creating Space for More Leaders:
• Phase I: Organization as HIERARCHY, where the key tool is delegation
• Phase II: Organization as COMMUNITY, where the key tools are worthwhile vision and values, a
gift economy
• Phase III: Organization as ECONOMY, where the key tools are free enterprise, education and
effective leadership of core businesses
g. Future-Focused Leadership:
h. CONCLUSIONS:
• The greater legacy of future leaders will be the LIBERATION of organizations to a higher level of
productivity, innovation and service.
• By listening to their followers, future leaders will become DESIGNERS of the game who brings
out the best in others.
• When leaders do their job of indirect leadership well, the people will say, WE DID IT OURSELVES.
CENTRALIZATIONVERSUSDECENTRALIZATION
MONOPOLYVERSUSUSERSCHOICE
THEORGANIZATIONOFTHE
FUTUREWILLBE:
•Communitiesofentrepreneurs
•Structuredfrommanysmallerinteractingenterprises
•Eachenterpriserequiringleadership
THEROLEOFTHELEADERWILL
BETO:
•Createandcommunicatevisionandvalues
•Createsystemsthatsupportandguideautonomy

PublicHealthLeadershipandManagementforthe21stCentury May2010
102
.
i. Acknowledgements:
• Gifford Pinchot, Author, Speaker & Consultant, Why You Don’t Have to Leave the
Corporation to Become an Entrepreneur
• The End of Bureaucracy and The Rise of the Intelligent Organization
j. Questions and Answers Session
3. CLASS DISCUSSION: CONCEPT PAPER #7: CREATING AN ENVIRONMENT FOR INNOVATION
4. LECTURE: DEVELOPING A PERFORMANCE ORIENTED CULTURE
a. Leadership Behavior and Organizational Performance:
• Shapers and keepers of performance-oriented cultures
b. Speaking a Different Language:
• Example #1: Chief Executive Officer of Bank One:
“……managing an UNCOMMON PARTNERSHIP that fosters maximum local autonomy for
•Commander
•Controller
•Decisionmaker
•Assimilationofpower
•Telleroftruths
•Identifyandconstantlycommunicatevalues
•Shapevaluestoenhanceperformance
•Ensurestaffcapability
•Livethecommonlyheldvalue
•Listenagreatdealoftime
•Speakadifferentlanguage

PublicHealthLeadershipandManagementforthe21stCentury May2010
103
..carefully selected managers combined with effective centrally provided services and common perfor-
mance measures”.
• Example #2: Chairman of the Board of ServiceMaster:
“……looked for a SERVANT’S HEART as the primary criterion in the selection of his successor
to serve as Chief Executive Officer”.
• Example #3: Executive Director of Girl Scouts:
“……ensuring that the organization remains MISSION-FOCUSED, VALUE BASED and
DEMOGRAPHICS-DRIVEN (diversity-driven)”.
• Example #4: Chief Executive Officer of Southwest Airlines:
“…..talks about hiring as a NEAR RELIGIOUS EXPERIENCE”
• Tough talk has not produced the kind of results that these leaders have delivered
c. Listening versus Telling:
• Example #1:
Frontlinemanagersaretrainedtolistentotheneedsofcustomers
Witheachsucceedingpromotionpeopletendtotellmoreandlistenless
Thosewhoperformwellaregenerallyrewardedwithpromotionsawayfromcustomers
⇓
⇓

PublicHealthLeadershipandManagementforthe21stCentury May2010
104
d. Listening versus Telling:
BANKONE
•Listenstorequests
•Connectspeoplewithresources
•Watchesperformancenumbers
SERVICEMASTER
•Adayofworkinthefieldcleaningfloors,wallsandtoilets,andservicefoodtostaffandcustomers
SOUTHWESTAIRLINES
•Opendoorpolicy
•Goestoemployees
•CapitalizesalwaysonEmployees
e. Listening versus Telling:
• A leader does not use information to take action against someone, more often, he/she uses it
to:
-Launch new initiatives
-Put people in touch with each other for mutual assistance and support
• As long as information is used in this manner, organizations respond and perform
f. Living the Values:
• Organizations that embrace values that honor and support ADAPTABILITY claim success and
longevity.
-Sensitivity to the needs of customers, employees, supplies and other important
constituencies
• Adaptability requires a different set of leadership behaviors
BANKONE
•PeopleWhoCare
•Face-to-Faceopportunitiestolisten
GIRLSCOUTS
•Helpingeverygirlachieveherfullpotential
SERVICEMASTER
•Tohelppeopledevelop(endgoal)
•Togrowprofitably(ameansgoal)
•Extensivecharitywork
SOUTHWESTAIRLINES
•EmphasisonFamily(customersandemployers)
•CEOand>90%ofemployeesengagedincharitywork
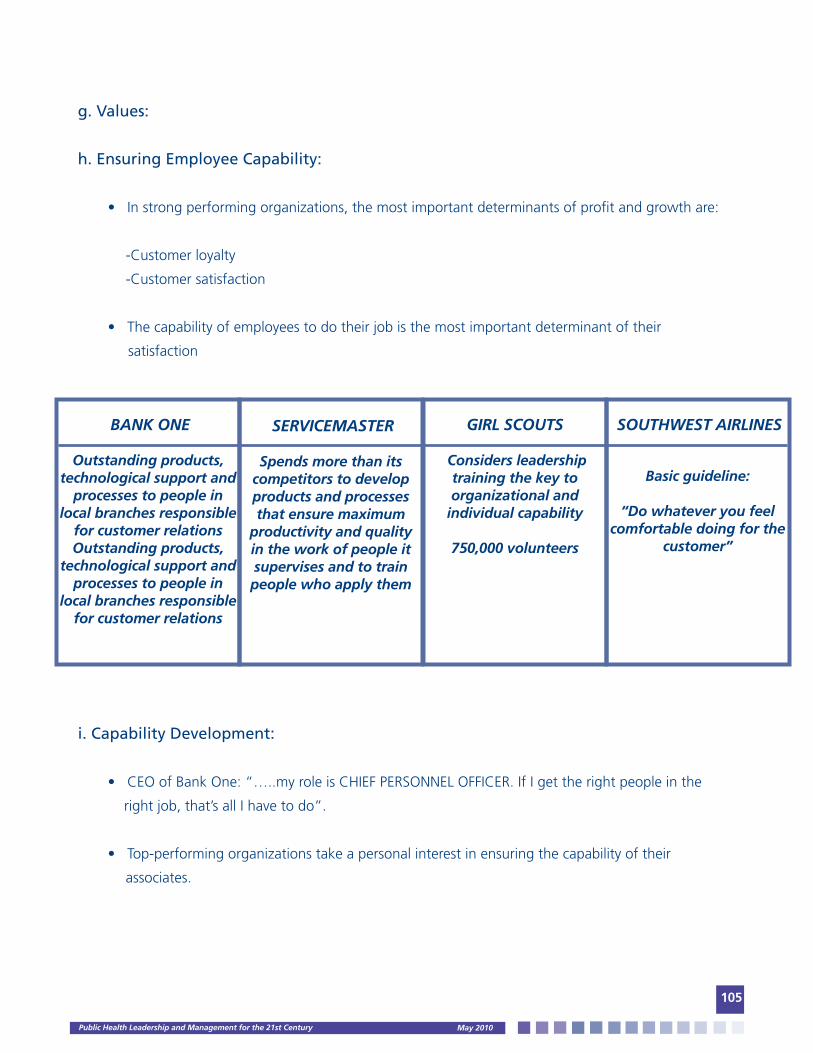
PublicHealthLeadershipandManagementforthe21stCentury May2010
105
g. Values:
h. Ensuring Employee Capability:
• In strong performing organizations, the most important determinants of profit and growth are:
-Customer loyalty
-Customer satisfaction
• The capability of employees to do their job is the most important determinant of their
satisfaction
i. Capability Development:
• CEO of Bank One: “…..my role is CHIEF PERSONNEL OFFICER. If I get the right people in the
right job, that’s all I have to do”.
• Top-performing organizations take a personal interest in ensuring the capability of their
associates.
BANKONE
Outstandingproducts,technologicalsupportand
processestopeopleinlocalbranchesresponsible
forcustomerrelationsOutstandingproducts,
technologicalsupportandprocessestopeoplein
localbranchesresponsibleforcustomerrelations
GIRLSCOUTS
Considersleadershiptrainingthekeytoorganizationaland
individualcapability
750,000volunteers
SERVICEMASTER
Spendsmorethanitscompetitorstodevelopproductsandprocessesthatensuremaximum
productivityandqualityintheworkofpeopleitsupervisesandtotrainpeoplewhoapplythem
SOUTHWESTAIRLINES
Basicguideline:
“Dowhateveryoufeelcomfortabledoingforthe
customer”
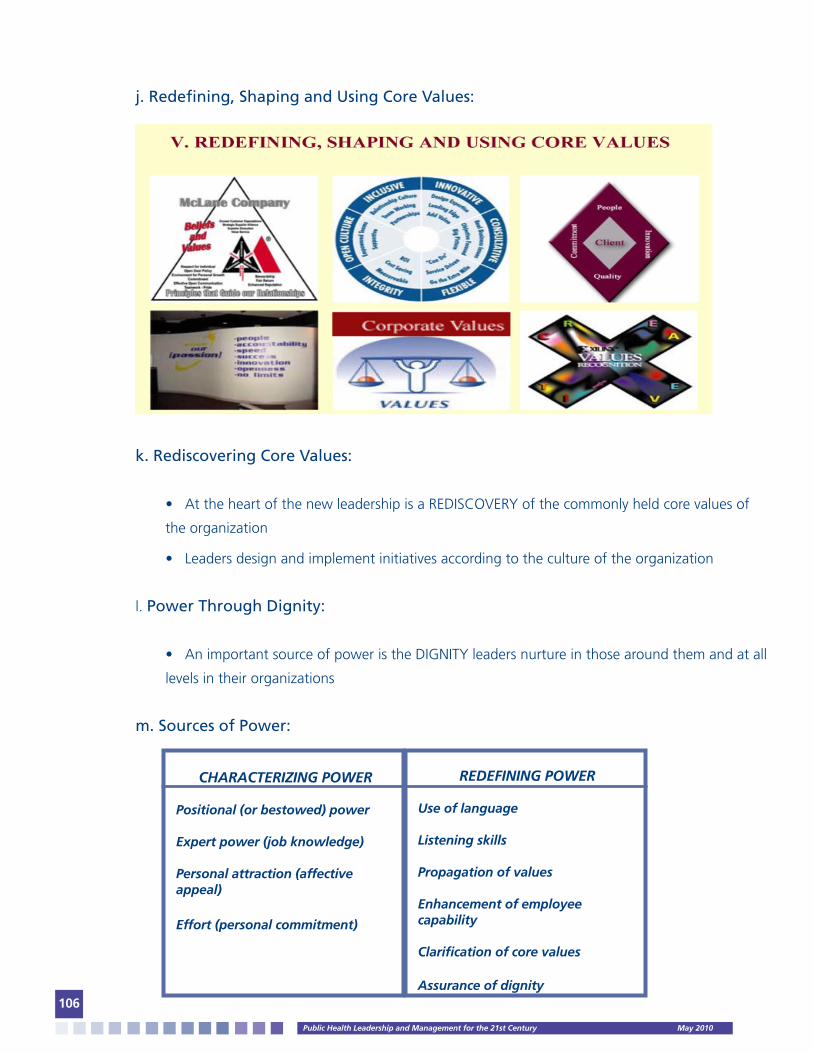
PublicHealthLeadershipandManagementforthe21stCentury May2010
106
j. Redefining, Shaping and Using Core Values:
k. Rediscovering Core Values:
• At the heart of the new leadership is a REDISCOVERY of the commonly held core values of
the organization
• Leaders design and implement initiatives according to the culture of the organization
l. Power Through Dignity:
• An important source of power is the DIGNITY leaders nurture in those around them and at all
levels in their organizations
m. Sources of Power:
CHARACTERIZINGPOWER
Positional(orbestowed)power
Expertpower(jobknowledge)
Personalattraction(affectiveappeal)
Effort(personalcommitment)
REDEFININGPOWER
Useoflanguage
Listeningskills
Propagationofvalues
Enhancementofemployeecapability
Clarificationofcorevalues
Assuranceofdignity

PublicHealthLeadershipandManagementforthe21stCentury May2010
107
n. Relational Power:
• The power of top leaders lies in their ABILITY TO FOSTER RELATIONSHIPS, both between
themselves and others and among others
o. CONCLUSION:
• There is a strong linkage between LEADERSHIP, CULTURE AND PERFORMANCE.
• In short, STATE OF THE ART LEADERSHIP delivers OUTSTANDING ORGANIZATIONAL RESULTS.
p. Acknowledgements:
• James L. Heskett, UPS Foundation Professor of Business Logistics, Graduate School of Business
Administration, Harvard University &
• Leonard A. Schlesinger, George Fisher Baker Jr. Professor of Business Administration, Associate
Dean and Director of External Relations, Harvard University
q. Questions and Answers Session
4. TEAM EXERCISE: X – Y SIMULATION: WIN AS MUCH AS YOU CAN
1. Teams
1. 4 groups
2. Separate physically
3. Each team gets ten ballots
2. Rules
1. Limit communications
2. Name of the game: Win as Much as You Can
3. Won’t answer further questions
4. Tally sheet/payoff schedule handout (ten rows)

PublicHealthLeadershipandManagementforthe21stCentury May2010
108
3. Prepare Flip Chart:
Start Game
• “1 minute to cast your ballots for round 1”
• Collect and post scores
• Round 2, etc.
Variation of Rounds
• Bonus rounds
• Send a delegate out of the room at round 5 & 9
Debrief
Rate your team’s satisfaction with the process (1—5)
Rate your team’s satisfaction with the product (1—5)
TEAMS/ROUNDS
T1
Vote/Payoff/Cum
T2
T3
T4
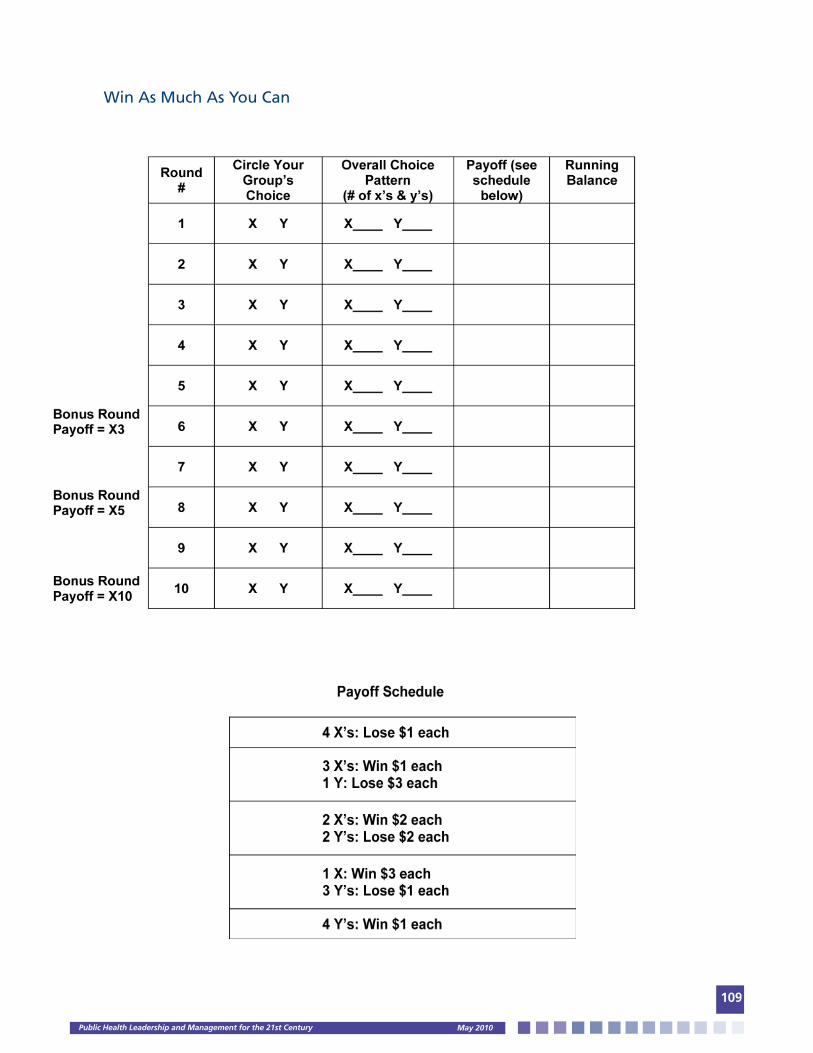
PublicHealthLeadershipandManagementforthe21stCentury May2010
109
Win As Much As You Can

PublicHealthLeadershipandManagementforthe21stCentury May2010
110
“Win As Much As You Can” Debrief
I. Who won? Who is the you in Win As Much As You Can?
II. How do you feel about your team’s performance? How do you feel about the other team’s
performance?
III. What factors made it difficult for your group to work cooperatively with the other groups in
this activity? How did the other team’s behavior influence your team’s behavior?
IV. What could have been done to raise the level of trust among the groups?
V. What analogous conditions create dysfunctional competition or conflict in situations at work?
VI. When the game was over, was it really over?
VII. What could be done on real life situations to minimize destructive competition and conflict
between groups?
VIII. Have each person write down one learning point that they can take back to work.
IX. If everyone in China CDC or MOH votes “X”, who wins?

PublicHealthLeadershipandManagementforthe21stCentury May2010
111
6. CLASS DISCUSSION: CONCEPT PAPER #8: CREATING SELF-DIRECTED WORK TEAMS
7. SELF-DIRECTED STUDY PROJECT AND PAPER #3: IQ (INTELLIGENCE QUO-TIENT), EQ (EMOTIONAL INTELLIGENCE), AND SQ (SPIRITUAL QUOTIENT)
8. BIBLIOGRAPHY
Required Readings:
• Rowitz, Chapter 2 and 13.
• Giener, Ann C. and Knebel, Elisa. The Core Competencies needed for Health Professionals: in
Who will keep the public healthy? Institute of Medicine, Washington, D.C., 2002. pp. 45 - 74
• Institute of Medicine of the National Academies: The Future of the Public’s Health. National
Academies Press. Washington, DC: 2003. pp. 358 – 402.
• National Public Health Leadership Network. The Public Health Leadership Framework. NPHLN,
2000. pp.1 – 10.
• Drucker, Peter F. Managing Oneself. Harvard Business Review. March – April 1999. pp. 92 – 108.
• Lau, C.M.., et al. A Shared Approach to Understanding Organizational Culture Change: In
Research in Organizational Change and Development, 2003. Volume 14: 225-256.
• Norman, Alex J. Managers’ Choices : Building Teams for Effectiveness in Public Service
Organizations. Pp. 1 –18.
• Aspden, Phillip, et al. Federal Leadership and Public/Private Partnerships: in Patient Safety:
Achieving a New Standard. Institute of Medicine, Washington, D.C., 2004. pp. 71 – 92.
• Keys, Paul R., and Norman, Alex J. Organizational Development in Public Services: The Irresistible
Force Meets the Immovable Object. The Haworth Press, INC., 1992. pp. 147 – 165.
Optional/Suggested Readings:
• Longest, Beaufort B., et al. Organizational Change:,In Managing Health Services Organizations
and Systems, 4th Edition. Health Professions Press. Baltimore, MD, 2000. pp. 78 – 91.
• Marks, Michell Lee and De Meuse, Kenneth P. Resizing the Organization. The Realities of
Resizing. 2003. pp. 123 – 135.
• French, Wendell L., and Bell, Cecil L. Definitions of Organizational Development: In
Organizational Development. Behavioral Science Interventions for Organization Improvement,
4th ed. Upper Saddle River, New Jersey, 1990. pp. 28 – 41.

PublicHealthLeadershipandManagementforthe21stCentury May2010
112
• Champy, James A. Preparing for Organizational Change: In The Organization of the Future
by Frances Hesselbein, et al. Jossey-Bass Publishers, 2000. pp. 89 – 104.
• Giener, Ann C. and Knebel, Elisa. Challenges Facing the Health System: in Who will keep
the public healthy? Institute of Medicine, Washington, D.C., 2002. pp. 45 – 74.
• Herzberg, Frederick. One More Time: How do you Motivate Employees? Harvard Business
Review, September – October, 1997. pp. 28 – 42.
• Drucker, Peter F. Managing Oneself. Harvard Business Review. March – April 1999. pp. 92 – 108.
• Butler, Timothy, and Waldroop, James. Job Sculpting: The Art of Retaining Your Best People.
Harvard Business Review. September – October, 1999. pp. 3 – 23.
VI. IMPLEMENTING STRATEGY
1. LECTURE: THE FIVE FUNDAMENTAL PRINCIPLES AND TEN COMMITMENTS OF EXEMPLARY LEADERSHIP:
a. Principle #1: CHALLENGE THE PROCESS
• Search for Opportunities
• Experiment and Take Risks
-Leaders forge into new territory and solve challenges by creating change
b. Principle #2: INSPIRE A SHARED VISION
• Envision the Future
• Enlist Others
-Visionary leaders always have an eye toward the big-picture –the possibilities
c. Principle #3: ENABLE OTHERS TO ACT
• Foster Collaboration
• Strengthen Others
-Leaders concentrate on making it easier for others to act
d. Principle #4: MODEL THE WAY
• Set the Example
• Plan Small Wins
-Leaders do first what they ask others to do
PublicHealthLeadershipandManagementforthe21stCentury May2010
113
e. Principle #5: ENCOURAGE THE HEART
• Recognize Individual Contributions
• Celebrate Accomplishments
-Leaders encourage people to carry on during tough times when everyone feels like
giving up
f. Collaborative Leadership:
• Leadership is shared
• Capacities are recognized and used
• Ideas of all members are heard and respected
• Success is celebrated
• New members can take on leadership roles
-Individuals have invaluable contributions to make as leaders
g. Who Can Be a Collaborative Leader? In collaborative work, there is room for a vari-
ety of leadership styles:
• Keep the big picture in sight
• Think through details
• Carry out day-to-day tasks
• Bring others on board
• Recognize success
-Collaboratives need a mix of “movers and shakers”
h. Are Leaders Born or Made?
• Some people naturally assume leadership in groups BUT leadership skills can be developed
over time
-It is essential to establish an environment conducive to nurturing new leadership
i. Who Are You As a Leader?
• Leadership begins with self-discovery and understanding your personal leadership style
-Leaders exhibit distinct practices that vary little from industry to industry
PublicHealthLeadershipandManagementforthe21stCentury May2010
114
2. CLASS EXERCISE: COLLABORATIVE LEADERSHIP *
Introduction:
Look around the room at the signs on the wall. They represent five principles of the kind of leader-
ship that is most successful in communities. You could also call these “leadership styles.”
• Challenge the Process
• Inspire a Shared Vision
• Enable Others to Act
• Model the Way
• Encourage the Heart
Instructions:
Please get up from your seats and walk to the sign that best represents your current leadership style.
We’re going to ask some of you to share why you chose that principle or style and perhaps give us an
example. For example if you choose “encourage the heart,” you might give an example of a commu-
nity celebration in which you honored community members for their contributions.
• What were some of your experiences with this activity?
• Was it was or difficult to pick a style?
• Were there any insights or surprises you’d like to share?
• Was it difficult to come up with an example?
• What are some of your feelings about a group of people with these leadership traits?
• How did you feel about the example?
Now walk under the sign that represents a principle or style of leadership you wish to work on or
grow in. Please share why you chose this principle and a way in which you might start to make
this change.
* Taken/adapted from the Los Angeles County Department of Health Services’ Office of Organiza-
tional Development and Training and the Public Health Institute’s Center for Collaborative Planning.
PublicHealthLeadershipandManagementforthe21stCentury May2010
115
3. LECTURE: CAPSTONE INITIATIVES AND ACTION LEARNING:
3.1. COLLABORATIVE LEADERSHIP CHANGE PROJECTS
a. Public Health Intelligence & Leadership Learning Principle:
• Adults learn by doing:
-I hear and I FORGET
-I see and I REMEMBER
-I do and I UNDERSTAND
--Confucius 551 – 479 B.C.
b. Why a Capstone Project?
• The measure of a SUCCESSFUL EDUCATION will be in the ability of the students to CONNECT
THE THREADS between public health intelligence and leadership courses and their own experi-
ences, abilities and talents and effectively APPLY THEM TO THE WORK THEY CURRENTY PERFORM
in their institutions and communities
c. Key Concepts:
• Improve institutional performance and community health through:
1. Team work
2. Collaboration
3. Partnerships
4. Leading change efforts
d. What is a Capstone Project?
• An applied learning experience where STUDENTS WORK ON AND RESOLVE A PUBLIC HEALTH
ISSUE, CHALLENGE OR OPPORTUNITY using an action learning approach
1. Deeply understand a real problem
2. Take wise actions
3. Reflect on what is learned

PublicHealthLeadershipandManagementforthe21stCentury May2010
116
e. Who is involved in the Capstone Project?
• Self-directed WORK TEAMS that will be formed during the Public Health Intelligence and
Leadership Program
f. When will the Capstone Project take place?
• Activities, timing, implementation, reporting and deliverables will be determined by China
CDC and MOH with support from USC
g. How will the Capstone Project be completed?
• Proposal Format and Guidelines:
1. Title
2. Team Members
3. Executive Summary
4. Public Health Issue, Challenge or Opportunity
5. Vision for Change
6. Stakeholders
7. Expected Outcomes
8. Strategy and Action
9. Sustaining the Change
10. Support Needed
g.1. Public Health Issue, Challenge or Opportunity
• What is the change that needs to happen?
• How is collaboration needed to make it happen?
• Is there a state of urgency and, if not, how will a felt sense of urgency be established?
• What is the context –department/program, internal/external stakeholders—in which the
change needs to happen?
g.2. Vision for Change:
• What will the CHANGE look like when you get there?

PublicHealthLeadershipandManagementforthe21stCentury May2010
117
g.3. Expected Outcomes:
• What two or three SHORT-TERM GOALS will you want to reach ---benchmarks or measures
of success?
g.4. Stakeholders:
• Who needs to be part of the change leadership team?
• Who are the major internal and external stakeholders?
g.5. Strategy and Action Plan:
• What in the culture will support or hinder the change?
• What is the strategy for strengthening those aspects of the culture that will support the
change?
• What is the strategy for weakening those aspects of the culture that will hinder the change?
• What is the proposed communication strategy with those who need to be kept informed and
with stakeholders?
g.6. Sustaining the Change:
• What is the proposed STRATEGY to sustain the change and promote continuous learning?
g.7. Support Needed:
• What RESOURCES or support will be needed to be effective and when will they be needed?
h. Sample Capstone Projects: Los Angeles:
• Reducing Animal Bites in Los Angeles County
• Enhanced Performance in Community Health Improvement Initiatives
• Integration of Performance Measures
• Promoting Public Health Initiatives
• Introduction of an Evidence-Based, Collaborative Community Change Approach to Improved
Birth Outcomes in Los Angeles County
• Public Health Measures: Improving Alcohol and Drug Program Administration Effectiveness
• Environmental Health: Collaboration for Change
• New Methodology for Public Health All Hazards Planning
PublicHealthLeadershipandManagementforthe21stCentury May2010
118
• Region-Specific Disaster Roles and Responsibilities
• Knowledge Exchange Enhancing the Public’s Health
• Improving the Public Health Emergency Preparedness of Vulnerable Populations in Los Angeles
County through Program-Division-Community Collaboration
• Forging a New Division of Communicable Disease Control and Prevention
• Mentoring for Health Facilities Inspection Division Staff
• Expanding Cervical Cancer Screening in STD Clinics
• Collaborative Model for the Advancement of Information Technology in Public Health for Los
Angeles County: Integrated Disease Management Demonstration Project
i. Capstone Project Question:
• What is the PUBLIC HEALTH ISSUE, CHALLENGE OR OPPORTUNITY in your institution or com-
munity that YOU WOULD LIKE TO ADDRESS with the support and HELP OF YOUR COLLEAGUES
in order to ADVANCE THE HEALTH AND WELL-BEING OF PEOPLE and/or ENHANCE THE EFFEC-
TIVENESS OF YOUR PROGRAMS AND SERVICES?
j. Acknowledgements:
• The Center for Collaborative Planning, Public Health Institute
• The Los Angeles County Public Health Leadership Institute
k. Questions and Answers Session
3.2. LECTURE: ACTION LEARNING
a. What is Action Learning?
• Action Learning is a structured process for WORKING ON REAL PUBLIC HEALTH PROBLEMS in
TEAMS to IMPROVE PUBLIC HEALTH and DEVELOP THE PARTICIPANTS
b. In Action Learning:
• Leaders become “comrades in adversity”
• Leaders understand a problem through REFLECTING ALOUD together its causes: PROBLEM-
FRAMING OR CLARIFICATION
• Leaders reflect together about effective and “wise” actions: PROBLEM-SOLVING OR
RESOLUTION
• Leaders TAKE ACTION and reflect on how effective the actions were and what should be
done next
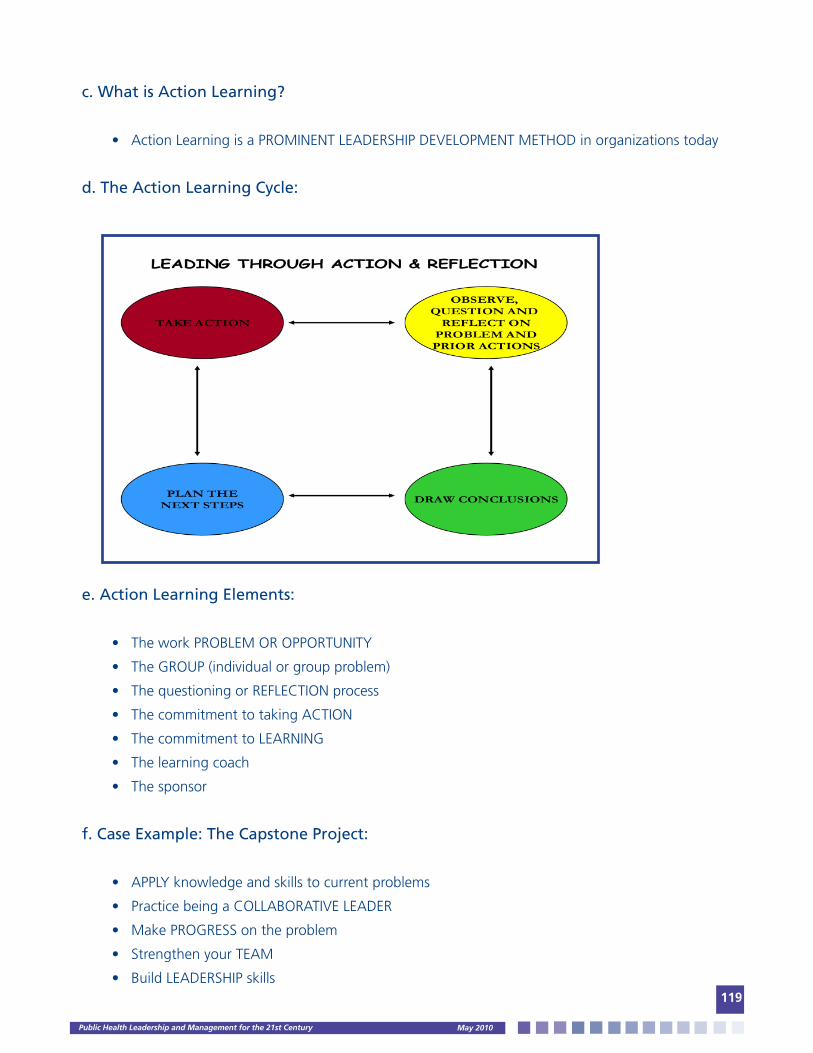
PublicHealthLeadershipandManagementforthe21stCentury May2010
119
c. What is Action Learning?
• Action Learning is a PROMINENT LEADERSHIP DEVELOPMENT METHOD in organizations today
d. The Action Learning Cycle:
e. Action Learning Elements:
• The work PROBLEM OR OPPORTUNITY
• The GROUP (individual or group problem)
• The questioning or REFLECTION process
• The commitment to taking ACTION
• The commitment to LEARNING
• The learning coach
• The sponsor
f. Case Example: The Capstone Project:
• APPLY knowledge and skills to current problems
• Practice being a COLLABORATIVE LEADER
• Make PROGRESS on the problem
• Strengthen your TEAM
• Build LEADERSHIP skills
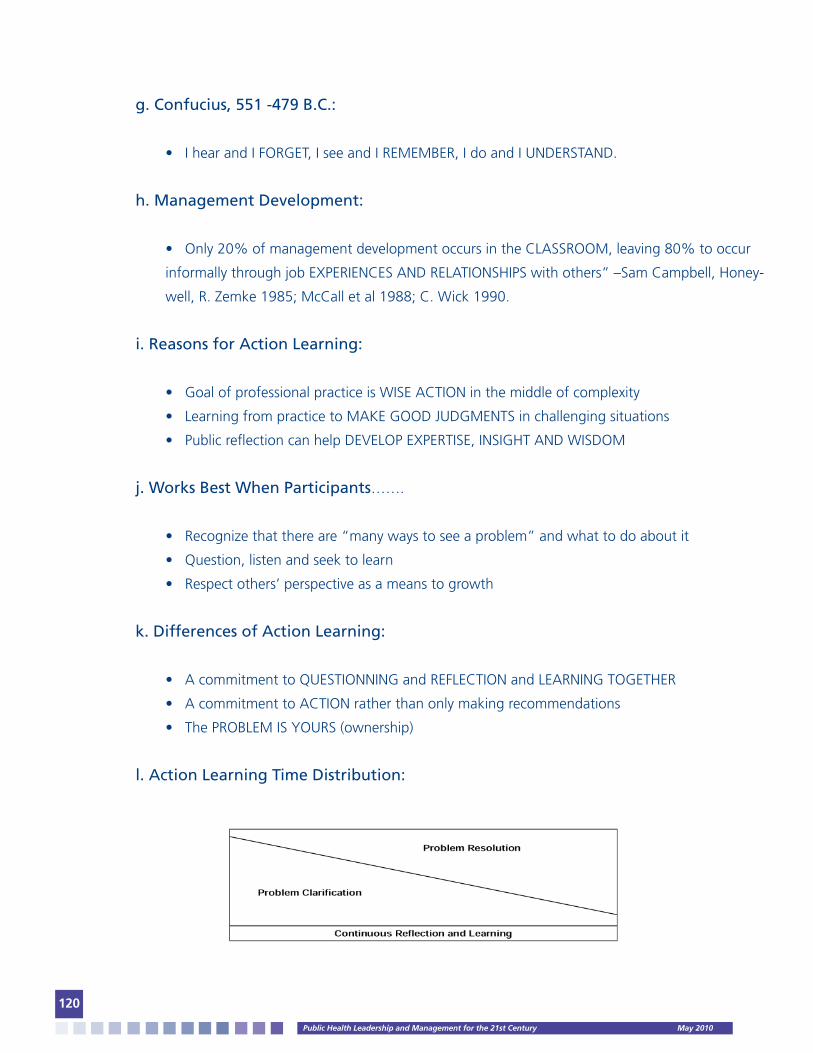
PublicHealthLeadershipandManagementforthe21stCentury May2010
120
g. Confucius, 551 -479 B.C.:
• I hear and I FORGET, I see and I REMEMBER, I do and I UNDERSTAND.
h. Management Development:
• Only 20% of management development occurs in the CLASSROOM, leaving 80% to occur
informally through job EXPERIENCES AND RELATIONSHIPS with others” –Sam Campbell, Honey-
well, R. Zemke 1985; McCall et al 1988; C. Wick 1990.
i. Reasons for Action Learning:
• Goal of professional practice is WISE ACTION in the middle of complexity
• Learning from practice to MAKE GOOD JUDGMENTS in challenging situations
• Public reflection can help DEVELOP EXPERTISE, INSIGHT AND WISDOM
j. Works Best When Participants…….
• Recognize that there are “many ways to see a problem” and what to do about it
• Question, listen and seek to learn
• Respect others’ perspective as a means to growth
k. Differences of Action Learning:
• A commitment to QUESTIONNING and REFLECTION and LEARNING TOGETHER
• A commitment to ACTION rather than only making recommendations
• The PROBLEM IS YOURS (ownership)
l. Action Learning Time Distribution:

PublicHealthLeadershipandManagementforthe21stCentury May2010
121
m. Capstone Project Question:
• What is the public health issue, challenge or opportunity in your institution or community that
you would like to address with the support of your colleagues in order to advance the health and
well-being of people and/or enhance the effectiveness of your programs and services?
n. Acknowledgements:
• Public Health Leadership Institute, Los Angeles County Department of Health Services
• Center for Collaborative Planning, Public Health Institute
• National Public Health Leadership Institute, University of North Carolina, Chapel Hill
o. Questions and Answers Session
p. KEY STEPS IN A CHANGE IMPLEMENTATION PROCESS (Source: Leading Change, Jef-
frey & Linda Russell, 2003):
These are the core elements of any successful plan for implementing organizational change. Some of
the key questions that the change implementation plan should address are identified.
Create a leading change design team: Who must be involved in helping you move your organization
or work area in a new direction? What areas, teams, or individuals should be involved in designing the
change?
Establish a sense of urgency for change: What are the forces causing the change and what is the
impact of these forces on the organization’s future success? Why is there a need for change? What de-
partments, units, teams, or individuals are affected and to what degree? Do the forces causing change
suggest a modest, incremental or transformational change? What are the consequences to the organi-
zation of not responding effectively to these forces?
Develop a vision for the change: What is the change that needs to occur? What do we need to ac-
complish or achieve as a result of the change? What problem are we trying to solve? What will the
outcomes of the change look like?
Define the impacts on those affected by the change: What are the potential pros and cons of the
change for the organization, departments, units, teams, and individuals? Who benefits and who loses?
Are customers or other stakeholders affected and to what extent?

PublicHealthLeadershipandManagementforthe21stCentury May2010
122
Create your strategy and action plan: How will you raise awareness of the need for change? How
will the losses be reduced, eliminated, or managed? How will employees and other stakeholders be
involved in developing the change vision and strategy? What actions will build commitment to the
change? How will the benefits from the change be realized? What actions need to occur, when
should they occur, and who should take the lead in taking them? What is the implementation time-
line?
Identify measures of success: How will the success of the planned change be evaluated? What are
the key indicators or measures of success? What benchmarks along the way will be used to help
track the progress the organization is making?
Develop your communication strategy: Who needs to be kept informed of the change vision and
strategy? What are the methods for communicating with these key stakeholders? What is the ideal
frequency of the communications about the change and the progress being made?
Develop your strategy to sustain the change and promote continuous learning: What is your plan for
building change leadership skills and knowledge in leaders, managers, supervisors, employees, and (if
appropriate) customers and other key implementation strategy? What other methods have you put in
place to sustain the change and foster continuous improvement?
4. CLASS DISCUSSION: CONCEPT PAPER #9: TURNING VISION INTO ACTION
5. LECTURE: CRISIS AND EMERGENCY RISK COMMUNICATION
a. GOAL: Tools for speaking during an intense public-safety emergency to the:
• Public
• Media
• Partners
• Stakeholders
-The RIGHT MESSAGE at the RIGHT TIME is a RESOURCE MULTIPLIER: it helps response
officials get their job done.

PublicHealthLeadershipandManagementforthe21stCentury May2010
123
b. Learning Outcomes: Acquire the following understanding:
• The psychology of communication in a crisis
• Your role as a spokesperson
• Working with media during a crisis
• Public health law and the media
c. Communicating in a Crisis is Different: In a crisis, all affected people:
• TAKE information differently
• PROCESS information differently, and
• ACT on information differently (Reynolds 2002)
-The way we normally communicate with people may not be effective during and after a crisis
d. Success of Operational Response Depends on:
• AMOUNT and
• SPEED of relevant official information received
-Real, measurable effect on the well-being of people depends on the WORDS you say and their
SPEED and SINCERITY
e. Five Things the Public Wants:
1. Gain facts needed for protection
2. Make well-informed decisions
3. Have an active role in response and recovery
4. Act as a watch-guard over resources
5. Recover or preserve well-being and normalcy
-The public wants to know what you know
f. Leaders Lead with Goals in Mind:
• Decrease illness, injury and deaths
• Execute response and recovery plans with minimal resistance
• Avoid misallocation of limited resources
• Avoid wasting of resources

PublicHealthLeadershipandManagementforthe21stCentury May2010
124
g. Communication Decisions:
• What to release
• When to release it
• How to release it
• Where to release it
• Whom to release it
• Why release it
-Well-prepared leaders have COMMUNICATION PLANS and resources in place…….PLAN NOW
h. FIVE COMMUNICATION FAILURES:
1. Mixed messages from multiple experts
• People don’t want to JUST PICK ONE of many messages, they want the BEST ONE or the
RIGHT ONE to follow
• Cumulative, consistent messages may drown out conflicting messages
2. Information released late
• If we can not give people what they need when they need it, others will
3. Paternalistic attitudes
• Help the people to reach the SAME CONCLUSION you did
• Never tell people DON’T WORRY
4. Not countering rumors and myths in real time
• The media will report rumors and hoaxes unless you can ANSWER QUICKLY why it is FALSE
5. Public power struggles and confusion
• All PARTNERS need to have clearly defined ROLES AND RESPONSIBILITIES
• Turf wars need to end at the moment a crisis begins
PublicHealthLeadershipandManagementforthe21stCentury May2010
125
i. FIVE COMMUNICATION SUCCESS STEPS
1. Execute a solid communication plan
• The public judges the success of your operation by the success of your COMMUNICATION
• Well-prepared leaders have COMMUNICATION PLANS and resources in place…..PLAN NOW
2. Be the first source of information
• The public uses the speed of information flow as a MAKER FOR YOUR PREPAREDNESS
• The FIRST MESSAGE people receive carries more weight
3. Express EMPATHY early
• The public will not be open until EMPATHY is expressed
4. Show competence and expertise
• The public assumes you are COMPETENT until proven otherwise
5. Remain honest and open
• Any INFORMATION is empowering
• UNCERTAINTY is more difficult to deal with than bad news
• People go to MULTIPLE SOURCES of information
• The FASTER bad news are given the BETTER
j. What People Feel in a Disaster:
1. Fear
2. Anxiety
3. Confusion
4. Dread
5. Hopelessness
6. Helplessness
7. Uncertainty
• Psychological barriers interfere with the COOPERATION and RESPONSE from the public

PublicHealthLeadershipandManagementforthe21stCentury May2010
126
k. Troublesome Expected Behaviors:
1. Dependence on special relationships
2. Worried Well
3. Multiple unexplained physical symptoms
4. Stigmatization
• Leaders confront behaviors in their communication to the public
l. Audience Judgments of Messages:
1. Speed of communication
2. Trust and credibility of the message
3. Empathy and caring
4. Competence and expertise
5. Honesty and openness
6. Commitment
7. Accountability
m. Employ the STARCC Principle: Your message in a crisis must be:
• Simple
• Timely
• Accurate
• Relevant
• Credible
• Consistent
n. Working with the Media: DISASTERS ARE MEDIA EVENTS
• The primary tool to get public safety messages to people in a hurry
• They know their audiences better than you do
-We need media involved during a crisis. Consider them in your planning.

PublicHealthLeadershipandManagementforthe21stCentury May2010
127
o. Early Media Mistakes:
1. Play favorites or hold grudges
2. Set arbitrary new rules to interact with official response group
3. Tell the media how to do their job
-BOTTOMLINE: They are going to be there whether we like it or not
p. What Reporters Want: EXPECT:
• Honest answers
• Timely release of information
• Quick squashing of rumors
• Commitment to availability and updates
• Subject matter experts
• Their calls to be returned
• State you do not have the answer
• Consistent messages
• Understanding of how media works
• Respectful treatment
q. Media Changes:
• Verification of facts goes down
• They abandon their adversarial role early in the crisis
• Many of them will lack scientific expertise
-Take the Media to SCHOOL: More information = More Factual.
-Less information = More Interpretative.
r. Successful Press Conferences:
• It’s a fast breaking crisis and the public is clamoring to know who is in charge
• You have an urgent message or recommendation
• You have promised regular updates
• You have news

PublicHealthLeadershipandManagementforthe21stCentury May2010
128
s. Writing for the Media in a Crisis:
• The mistake response officials make is waiting to release information until all the facts are in.
1. Release what you know
2. Acknowledge what you don’t know, and
3. State ho you are getting the answers
t. The Expected Questions:
• What happened?
• Are my family and I safe?
• What have you found that may affect me?
• What can I do to protect myself and my family?
• Who caused this?
• Can you fix it?
• Who is in charge?
• Has this been contained?
• Are victims being helped?
• What can be expected, right now and later?
• What should we do?
• Why did this happen?
• Did you have forewarning?
u. The Leader as a Spokesperson:
• Saves lives
• Reduces anxiety and fear
• Helps people recover more quickly
-A CREDIBLE SPOKESPERSON can influence behaviors that could be life saving
v. What Makes a Good Spokesperson:
• Expression of empathy
• Risk saying I don’t know, we’re working on it
• Telling the truth
• Confidence without arrogance
• Appropriate emotion

PublicHealthLeadershipandManagementforthe21stCentury May2010
129
• Modulated voice
• Direct eye contact
• Humility or a lack of defensiveness
-Always remember who the audience is……..people hurt, confused, anxious and possibly
angry……not the media!!!
w. Basic CERC Tenets:
1. Give anticipatory guidance
2. Be regretful, not defensive
3. Acknowledge people’s fears
4. Acknowledge the shared misery
5. Express wishes
6. Panic is less common than imagined
7. Be willing to address “what if” questions
x. Know Your Stakeholders
• Stakeholders are identifiable groups of people or organizations who can be reached in ways
other than through the media
• Stakeholders are people or organizations with a special connection to you and your involve-
ment in the emergency
y. Three Categories of Stakeholders:
1. Advocates
2. Adversaries
3. Ambivalents
-Anticipate stakeholder’s reaction and develop a stakeholder’s communication plan
z. Importance of Stakeholders:
• They may know what you need to know
• They may also be able to help communicate your message for the media

PublicHealthLeadershipandManagementforthe21stCentury May2010
130
aa. Five Mistakes Toward Stakeholders:
• Inadequate access
• Lack of clarity
• No energy for response to them
• Too little too late
• Perceptions of arrogance
bb. Media Law:
• Learn what legal rights the media have or do not have in a crisis. Consult a media expert if
you do not know
• The media has the constitutional right to acquire news from any source by any lawful means
• The media are given no constitutional right to special access (crime scenes, disaster scenes,
police stations, hospital laboratories, and places restricted to the public).
• The media’s access may be restricted if it interferes with legitimate law enforcement actions
• The media may have access to what is available an open to the public historically
• Articulate, before the crisis, the principles of public information you embrace
cc. Keeping Fit for Duty in a Crisis:
• RELIEVE STRESS: 15-minute walk, talk to someone, take a “brain break”, do deep breathing
exercises, eat nutritional foods, avoid caffeine and alcohol, get as much sleep as possible, etc.
• More than 24 hours without sleep = job performance equivalent to that of someone legally
drunk.
dd. Acknowledgements:
• U.S. Department of Health and Human Services (HHS)
• Centers for Disease Control and Prevention (CDC), CDC Office of Communication (OC), Office
of the Director (OD)
ee. Questions and Answers Session
PublicHealthLeadershipandManagementforthe21stCentury May2010
131
6. LECTURE: RISK AND HIGH STRESS COMMUNICATION
a. Definition:
• A science-based approach for communicating effectively in:
1. High-Concern
2. High Stress
3. Emotionally Charged, or
4. Controversial Situations
b. Literature Review:
• 8000 Articles in Peer Reviewed Journals
• 2000 Books
• Reviews of Literature by Major Scientific Organizations
--USC National Academy of Sciences
--Royal Society of Great Britain
c. Key Messages
1. Risk Communication is a science-based discipline
2. High stress, high concern situations CHANGE THE RULES OF COMMUNICATION
3. Key to communication success is PREPAREDNESS, PLANNING AND PRACTICE
d. 9/11 Major Lesson Learned (2001):
• “……the major public health challenges since 9/11 were not just clinical, epidemiological or
technical issues. The major challenges were COMMUNICATIONS. In fact, as we move into the 21st
century, communications may well become the CENTRAL SCIENCE OF PUBLIC HEALTH PRACTICE”.
--Edward Baker, MD, MPH, Assisstant Surgeon General, USA, 12/2001
e. Lessons Learned from Great Risk Communicators
1. Alexander the Great
2. Julius Ceasar
3. Napoleon Bonaparte
4. Wiston Churchill
5. Rudy Giuliani
6. Julie Gerberding

PublicHealthLeadershipandManagementforthe21stCentury May2010
132
f. Trust Determination Factors in High Concern Situations
g. Mental Noise Theory: Reduced Attention Span
• When people are stressed or upset, they often lose as much as 80% of the information that is
communication to them
h. High Risk Communication Principles (Tactics)
h.1. APP Rule: ANTICIPATE, PREPARE AND PLAN
• Great risk communicators know the answers of at least 95% of the questions
Listening,Caring,Empathy
Honesty,Transparency
Competence,Expertise
Dedication,Commitment
50%
15-20%
15-20%
15-20%
ARPRule
Ruleof3’s
P&RRule
27/9/3Template
AGL-4
CCOTemplate
YesNoTemplate
1N=3PRule
2XMessageEnhancements

PublicHealthLeadershipandManagementforthe21stCentury May2010
133
h.2. Everything in threes: RULE OF 3’s
• Three key messages
• Key messages repeated 3 times
• Each message supported by 3 supporting messages
h.3. Speak briefly in threes: 27/9/3 TEMPLATE:
• 27 words
• 9 seconds
• 3 messages
h.4. Use simple language: AGL-4 Rule
• Average grade level minus 4 years
h.5. Demonstrate feelings, determination and hope: CCO TEMPLATE
• Compassion
• Conviction
• Optimism
h.6. Use positive counterarguments: 1N – 3P RULE
• For 1 Negative use 3 Positive Statements
h.7. Don’t get involved in a battle with reporters: YES NO TEMPLATE
• You ask me a YES or NO question
• It would be difficult for me to answer YES or NO
• What I can address is the issue………which is…….
h.8. Double the attention span of audiences: 2X MESSAGE ENHANCEMENTS
• Personal stories
• Visuals
• Credible third parties

PublicHealthLeadershipandManagementforthe21stCentury May2010
134
7. TEAM EXERCISE: WEST NILE VIRUS MESSAGE DEVELOPMENT
a. West Nile Virus Transmission Cycle
b. Message Map

PublicHealthLeadershipandManagementforthe21stCentury May2010
135
c. West Nile Virus Summary
d. Acknowledgements:
• Dr. Vincent Covello, Director, Center for Risk Communication
• David Steffen, Director, National Public Health Leadership Institute, University of North Carolina,
Chapel Hill
8. CLASS DISCUSSION: CONCEPT PAPER #10: BECOMING CUSTOMER CENTRIC

PublicHealthLeadershipandManagementforthe21stCentury May2010
136
9. BIBLIOGRAPHY
Required Readings:
• Rowitz, Chapter 2 and 16
• National Research Council. Measuring Health Performance in the Public Sector.
Washington, D.C., 1999. pp. 1 – 48.
• Chrvala, Carole A., et al. Leading Health Indicators for Healthy People 2010. Institute of
Medicine, Washington, D.C., 1999. pp. 1 – 24.
• Ginter, Swayne. Control of the Strategy: Strategic Management of Health Care
Organizations. 2002. pp. 370 – 392.
• Institute of Medicine of the National Academies: Informing the Future: Critical Issues in
Health: Assuring the Public’s Health. 2nd. Edition. Washington, D.C. pp. 63 – 80.
• Hesselbein, Frandes et al. Executives on the Future of Leadership: Chapters 28, 29, 30,
31: In The Leader of the Future. The Drucker Foundation. San Francisco, CA, 1996. pp.
241 - 311. Kouzes, James and Posner, Barry. The Five Fundamental Principles and Ten
Commitments of Leadership: In The Leadership Challenge, 1995. pp. 15 – 29.
Optional/Recommended Readings:
• Institute of Medicine of the National Academies: Informing the Future: Critical Issues in
Health: Health Care Delivery Systems and Performance Capabilities.. 2nd. Edition.
Washington, D.C. pp. 81 – 100.
• Bensaou M., and Earl, Michael. The Right Mind-Set for Managing Information
Technology. Harvard Business Review. September – October 1998. pp. 26 – 44.
• Institute of Medicine of the National Academies: Imedical Innovation in the changing
health care marketplace. Washington, D.C. 2002. pp. 1 – 42.
• Hesselbein, Frandes et al. Executives on the Future of Leadership: Chapters 28, 29, 30,
31: In The Leader of the Future. The Drucker Foundation. San Francisco, CA, 1996. pp.
241 - 311.
• Bensaou, M., and Earl, Michael. The Right Mind-Set for Managing Information
Technology. Harvard Business Review. September – October 1998. pp. 7 – 29.
• Deal, Terrence E. and Bolman, Lee G. Reframing Organizations: Artistry, Choice and
Leadership. Jossey-Bass Publishers, San Francisco, CA 176 – 211.
• Rossy, Gerard L., et al. Tailored Management Development as a Vehicle for Strategy
Implementation. California State University, Northridge, CA. pp. 641 – 651.

PublicHealthLeadershipandManagementforthe21stCentury May2010
137
INSTITUTE FOR HEALTH PROMOTION & DISEASE PREVENTION RESEARCHKeck School of MedicineUniversity of Southern California (USC)1000 South Freemont Avenue, Unit 8 Alhambra, California 91803http://mph.usc.edu/ipr/http://mrcalderon.com
© 2008 INSTITUTE FOR HEALTH PROMOTION & DISEASE PREVENTION RESEARCH