public health in the americashist.library.paho.org/english/pub/pbos177.pdf · 1940 was a prudent...
TRANSCRIPT
PUBLIC HEALTHIN THE AMERICAS
HEADOUARTERS OF SOME LATIN AMERICAN DEPARTMENTS OF HEALTH
PAN AMERICAN SANITARY BUREAU . ..WASHINGTON, D. C.
Publication No. 177, June, 1942
M
#1" Pib!
II� ,LEI

FUNCIONARIOSDE LA
OFICINA SANITARIA PANAMERICANA
(OFFICERS OF THE PAN AMERICAN SANITARY BUREAU)
DIRECTORDR. HUGH S. CUMMING
Surgeon General (Retired) U. S. Pujlic Health 2ernsi
VICEDIRECTO RDR. JOÁO DE BARROS BARRETO
Brasil
CONSEJEROS (COUNSELORS)DR. MIGUEL SUSSINI
Araentina
DR. ANTONIO PEÑA CHAVARRtACosta Rica
DIRECTOR AUXILIAR (ASSISTANT DIRECTOR)DR. EDWARD C. ERNST
Sevicio de Sanidad Pdblica de lo8 Estados Unidos
SECRETARIO (SECRETARY)
DR. ARISTIDES A. MOLLRedaa"o, Cientifico. Boletín de la Oficina Sanitaria Panamericana
VOCALES (MEMBERS)DR. ATILIO MACCHIAVELLO
Chile
DR. LUIS MANUEL DEBAYLENicaragua
DR. A. L. BRICEÑO ROSSIVenezuela
DR. DAGOBERTO E. GONZÁLEZPertl
DR. MANUEL MARTINEZ BÁEZMlxico
DR. PEDRO MACHADOCuba
DR. JUAN ANTONIO MONTALVANEcuador
NMIEMBROS DE HONOR (HONORARY MEMBERS)DR. JORGE BEJARANO, Presidente de Honor
Colombia
DR. CARLOS ENRIQUE PAZ SOLDÁNPera
DR. LUIS GAITANGuatemala
COMISIONADOS VIAJEROS INGENIEROS SANITARIOS(TRAVELING REPRESENTATIVES) (SANITARY ENOINEERS)DR JOHN D. LONG SR. EDWARD D. HOPKINSDR JOHN R. MURDOCK SR. WALTER N. DASIIIELLDR. ANTHONY DONOVAN SR. WILLIAM BOAZDR. HENRY HANSONDR. VERNON W. FOSTERDR. JOSEPH S. SPOTO
Cover: Top: Building of the Department of Health (Dirección General de Sanidad) of Guate-mala: Ministry of Publie Health, Labor and Social Welfare (Ministerio de Salud Pública, Trabajoy Prevision Social) of Peru; Center: Ministry of Publie Health and Social Welfare (Secretaríade Salud Pública y Protección Social) of Costa Rica; Ministry of Labor, Health and Social Wel-fare (Ministerio del Trabajo, Salubridad y Previsión Social) of Bolivia.; Ministry of Health andSocial Assistance (Ministerio de Sanidad y Asistencia Social) of Venezuela; Below: Ministry ofHealth and Welfare (Secretaría de Sanidad y Beneficencia) of the Dominican Republic; Depart-ment of Public Health (Departamento de Salubridad Pública) of Mexico.

PAN AMERICAN SANITARY BUREAU
OFICINA SANITARIA PANAMERICANAPUBLICATION NO. 177 . JUNE, 1942
Public Health in the Americas
WASHINGTON, D. C.
U. S. A.

PTONEERS IN PUBLIC HEALTH IN AMERICA
CARLOS CHAGAS
(1879-1934)
JosÉ HIPÓLITO UNANUE
(1755-1833)
EDUARDO LICÉAGA
(1839-1920)
CARLOS J. FINLAY
(1833-1915)
WALTER WYMAN
(1848-1911)
ii
-

PIONEERS IN PUBLIC HEALTH IN AMERICA
JUAN GUITERAS
(1852-1925)
MIGUEL COUTO
(1864-1934)
DANIEL A. CARRIÓN(1858-1885)
LuIs M. RAZETTI
(1862-1932)
iii
JOSE PENNA
(1855-1919)

PIONEERS IN PUTBLIC HEALTH IN AMERICA
OSWALDO CRUZ(1872-1917)
GUILLERMO RAMWSON
FRANCISCO DE S.C. Y ESPEJO(1740-96)
WILLIAM C. GORGAS(1854-1920)
JosÉ M. VARGAS

PIONEERS IN PUBLIC HEALTH IN AMERICA
EMILIO R. CoNI(1855-1928)
RAFAEL RANGEL
(1877-1909)
Luis MORQUIO(1867-1935)
JUAN J. ULLOA(1859-1913)
y

PIONEERS IN PUBLIC HEALTH IN AMERICA
ALEJANDRO DEL RíO
(1867-1939)
TOMÁS G. PALOMO(XIX Century)
CARLOS DURÁN(XIX Century)
FACUNDO YNSFRÁN(XIX Century)
vi
TABLE OF CONTENTS
PAGE
Pioneers in Public Health in America ................... 1................. ii-vi
Pan-American Health Day (Dr. Hugh S. Cumming) ....................... . viii
Public Health in Argentina (Dr. Juan Jacobo Spangenberg) ................ 1
Recent Medical Advances in Argentina (Dr. B. A. Houssay) ................ 1
Public Health in Bolivia (Dr. Abelardo Ibáñez Benavente) ................. 12
Developments of Medicine and Science in Present-Day Brazil (Dr. AfranioPeixoto) ............................................................... 14
Public Health in Chile (Dr. Pedro Aguirre Cerda) .......................... 18
Public Health Progress in Colombia (Ministry of Labor, Health and SocialWelfare .............................................................. 20
Public Health in Costa Rica (Dr. Mario Luján Fernández) ................. 22
Public Health in Cuba (Dr. Alberto Recio) ................................ 25
Public Health in the Dominican Republic (Dr. Wenceslao Medrano H.) ...... 29
Public Health in Ecuador (Dr. Leopoldo Izquieta Pérez) ................... 31
Public Health in El Salvador (Drs. Victor Arnoldo Sutter and M. ZúñiigaIdiáquez) ......... ..................................................... 33
The Evolution of Public Health in Guatemala (Dr. Luis Gaitán) ........... 36
The National Health & Social Welfare Service of Haiti (Dr. Louis Hippolyte). 38
Haitian Epidemics (Dr. Rulx Léon) ....................................... 40
Public Health in Honduras (Dr. Pedro H. Ordóñez Díaz) ................... 41
Some Important Data on Public Health in México (Drs. Víctor FernándezManero and Alberto P. León) .......................................... 43
Pan American Health Day (Dr. Luis Manuel Debayle) ..................... 48
Public Health in Paraguay in the Twentieth Century (Dr. Gerardo Buonger-mini) .......................... ............................... 48
Public Health in Peru (Fiscal Year 1940-41) (Dr. Manuel Prado) ........... 53
New Objectives for the Coordinative Work of the Pan American SanitaryBureau, Washington (Dr. Carlos Enriquez Paz Soldán) ................. 55
Public Health in the United States (Dr. Thomas Parran) .................. 57
Public Health in Uruguay: 1901-1941 (Dr. Rafael Schiaffino) ................ 62
Outline of Public Health in Venezuela (Dr. M. Lares Gabaldón) ............ 66
Some Pan American Public Health Pioneers .............................. 69
vii
PUBLIC HEALTH IN THE AMERICAS
In honor of the Second Pan American Health Day (December 2, 1941), NationalHealth Authorities and other prominent sanitarians of the Americas were in-vited to prepare, for publication in the Boletin de la Oficina Sanitaria Panamer-icana, articles on the history, development and present status of public health intheir respective countries, or on some other subject proper to Pan AmericanHealth Day. The reports received were so interesting that it was decided toreprint the translations in a separate booklet for the convenience of studentsin this field.-EDIToR.
PAN AMERICAN HEALTH DAY
An excellent proof that the creation of Pan American Health Day in1940 was a prudent and wise initiative, was its wide celebration in allthe American Republics, with the cordial and effective participation ofboth Governments and people.
A glimpse at the activities which took place on this day last year,as well as at those already planned for this, show how united all ourcountries are in their faith in Public Health as an instrument for theprotective strengthening of our people. The celebration this yeartakes on added importance in view of the crisis through which the worldis passing, a crisis which threatens ever more closely our own countries.In these moments of unrest and alarm, when National Defense is nolonger a theory, but an inevitable necessity, we must strive moreearnestly than ever to strengthen the biologic factor: Man himself,since on him will depend the final success of our efforts in the struggleswhich lie ahead.
Let us therefore make December 2 an occasion not only for renderingtribute to the pioneers of the past and for emphasizing, as we havedone before, the importance of public health work, but also, and aboveall, for stressing the fact that it is only through Health and Sciencethat the future may be confronted with security, and a humanity createdand maintained which may fearlessly defy the risks which menace us.
Health, the treasure of the rich, the happiness of the poor, and thenecessity of all, stands today as the greatest asset available to men intheir defense of the right to Liberty and to Life. Pan AmericanHealthDay indeed takes on new significance and value in this momentous year.-HUcGH S. CUMMING, Director of the Pan American Sanitary Bureau.
viii

PUBLIC HEALTH IN ARGENTINA
By DR. JUAN JACOBO SPANGENBERG
President of the National Department of Health
Cardiovascular diseases are today one of the fundamental public health prob-lems of Argentina. They are responsible for the greatest number of deaths-about 28,000 a year (267 per 100,000) in the cities, and a somewhat smaller numberin the rural regions. The economic loss, including medical aid required andpotential earning capacity, has been estimated at 100 million pesos annually;40% of retirement for disability is due to these conditions. The NationalDepartment of Health has recommended to the Executive Authorities the fol-lowing preventive measures: compulsory periodic medical examinations, special-ized medical service, and professional orientation.
Since the enactment of the Compulsory Vaccination Law in 1904, smallpoxhas definitely been banished from the country. The few cases reported havebeen from frontier regions. In 1940, 1,565,315 doses of smallpox vaccine weredistributed gratuitously, and 721,535 inoculations including re-vaccinations,were registered. No cases of smallpox were reported during this year.
Diphtheria vaccination is now obligatory for all children between the ages of9 months and 12 years. Even before this action was taken, the National Depart-ment of Health manufactured diphtheria vaccine, first the three-dose toxin-antitoxin, and finally a single-dose type, which it distributed free throughout thecountry for voluntary use. But the results were satisfactory only where localregulations made immunization compulsory. It is expected that equally goodresults will be obtained throughout the country, following the new nationalcompulsory legislation.
RECENT MEDICAL ADVANCES IN ARGENTINA
By Dr. B. A. HOUSSAY
Director of the Institute of Physiology, University of Buenos Aires
It is difficult, or, rather, impossible, to report in a few pages the most importantscientific contributions of the last few years in Argentina. The brief reviewwhich follows must, of necessity, suffer from inevitable omissions and too muchcondensation. Since not all the meritorious achievements can be mentioned,only some of the best-known or most important will be cited, without this sig-nifying any detraction from those which could not be included because of lackof space.
The role of the anterior pituitary in carbohydrate metabolism and in diabetes,was discovered in our Institute of Physiology. Until 1929 the known facts werethat diabetes is common in acromegaly (32% of cases) and that the extract of theposterior lobe is hyperglycemic. In our Institute the following phenomena wereobserved illustrating the physiologic role of the anterior lobe:
(A) Hypophysectomy or ablation of the anterior lobe causes: (1) a strongsensitivity to the hypoglycemic or toxic action of insulin (Houssay and Magenta,1924-1929), and to that of other hypoglycemic agents such as phloridzin or fasting(Houssay and Biasotti, 1930); (2) attenuation of the intensity of pancreatic andphloridzinic diabetes (Houssay and Biasotti, 1930); (3) rapid drop in glycemia and
1
HEALTH AUTHORITIES OF THE AMERICAN REPUBLICS
DR. JUAN JACOBO SPANGENBERG DR. A. IBÁÑEZ BENAVENTE
(Argentina) (Bolivia)
DR. JoAX DE BARROS BARRETO
(Brasil)
DR. ANSELMO GAITÁN U. DR. MARIO LUJÁN FERNÁNDEZ
(Colombia) (Costa Rica)
PUBLIC HEALTH IN THE AMERICAS 3
in glycogen during starvation (1924 and 1930) observed even in animals withoutpancreas. This condition may be prevented with a protein and carbohydratediet, but not by a fatty diet.
(B) The anterior pituitary extract produces the following effects, which areobserved even in the absence of the pituitary and of the pancreas: (1) increasedresistance to insulin (Houssay and Potick, 1929; Di Benedetto, 1932) and to otherhypoglycemic agents such as phloridzin (Houssay and Biasotti, 1933) impedesthe drop in glycemia and glycogen in hypophysioprivous animals during fasting;(2) it aggravates pancreoprivous diabetes and rapidly results in death followingcoma with acidosis and severe ketosis (Foglia & col., 1937); (3) it aggravatesattenuated pancreatic or phloridzinic diabetes in pancreoprivous animals lackingthe pituitary, and also Sandmeyer's diabetes (Houssay, Biasotti, & Rietti, 1932);(4) it causes a typical diabetes in normal dogs (Houssay, Biasotti & Rietti, 1932),which at first is of extrapancreatic origin, but the islands of Langerhans are sooninjured (Porto 1941) and the output of insulin is enormously reduced (Houssay& collaborators, 1936 and 1941); (5) at times the animal remains definitely diabeticafter suspension of the anterior pituitary injections, because of the destructionof the islands of Langerhans, a phenomenon which was first demonstrated in dogswith a reduced pancreas (Houssay, Biasotti & Rietti, 1932) and later in dogs witha whole pancreas (Young, 1937). It is not unusual to see all of these facts quotedwith errors of date and authorship in North American publications and in theLatin American ones which copy them.
General clinics of the "General Rodriguez" Colony-Hospital for Leprosy,Buenos Aires, Argentina, opened on the Second Pan American Health Day.
Hypertension of renal origin has been intensively studied in our Institute from1937 to date. A kidney in which ischemia has been produced discharges renin,which, by acting on the serum globulins (in vitro or in vivo) produces hipertensin(Braun Menéndez, Fasciolo, Leloir and Mufñoz, 1939). Grafting the kidney,by vascular union, into a nephrectomized dog, it is observed that the blood pres-sure rises in 5 or 10 minutes; a phenomenon which is not seen following the graft-ing of a normal kidney (Houssay & Fasciolo 1937). The venous blood of theischemized kidney contains abundant renin, which may be accurately measured,and which produces hipertensin in the circulating blood (Houssay and Taquini,1938; Braun Menéndez and Fasciolo, 1939). Hipertensin was first isolated fromthis blood, and then prepared in vitro in 1939. These findings are often omitted

4 PAN AMERICAN SANITARY BUREAU
from North American publications. A complete review of the work was pub-lished in 1940, and two papers on it have appeared in England and two in theUnited States. Cases of renin specificity are known, whereas hipertensin isequally active from toads to man. The pharmacology of hipertensin has beenstudied by Ludueña, Foglia, Braun Menéndez, and collaborators. Renin isdestroyed by the kidney and by all the tissues; hipertensin by a hipertensinase.During shock (Dexter) and severe hypotension (Huidobro), a discharge of renininto the blood has been shown.
Fluorosis has been found in different parts of Argentina, causing mottledenamel (Damon, Muñoz, Erausquin, Mácola), and if the quantity of fluorine indrinking water is large, ostealgia and osteopetrosis (Capizzano & col., Pasqualini).
Plasma potassium, its role and regulation, have been studied a great deal byMarenzi, Gerschman, Houssay, and Moglia, and an important monograph byGerschman was published in 1939. Cicardo has investigated the liberation ofpotassium from the striated or smooth muscle by acetylcholine, and the role of
Palermo water plant, Public Sanitation Works Department, Buenos Aires,Argentina
potassium in muscular activity. Zwemer (1941) has been working on the physio-logic and pharmacologic action of potassium.
The normal and pathologic physiology of urobilin and bilirubin has beenthoroughly studied by Royer and by López García and Castex, who have madeknown valuable methods of quantitative clinical examination of blood, bile andurine. Royer has investigated the biliar vesicle function through laparoscopy andintravesical injection of opaque substances. Operative cholangiography hasbecn the subject of important research by Mirizzi. Bengoles and Velazo Suárezhave methodically studied the physio-pathology of the bile ducts.
The anterior pituitary in thyroprival cases shows a decreased gonadotropieand thyrotropic activity (Reforzo). As the result of intense thyroid treatmentthe pituitary exerts a marked thyreo-depressive action (Reforzo).
Important studies of the sex hormones have been made in dogs (Arenas andSammartino), toads (Inés L. C. de Allende), and weasels (Martínez Esteve).During continuous estrogen treatment a cyclic vaginal response is observed (DelCastillo and Di Paola). The interrelation of the ovary and the anterior pituitaryhave been studied by Peralta Ramos and Colombo, Fels, Del Castillo and Sam-

PUBLIC HEALTH IN THE AMERICAS 5
martino and others. Araya maintains that ovulation and menstruation aretotally independent phenomena, but Sammartino's careful observations havealways shown a typical correlation between the condition of the endometriumand that of the ovary.
The inter-action of the anterior pituitary of mammals and batrachia with thethyroid, suprarrenal glands, gonads, parathyroids, spleen, thymus, etc., has beenthoroughly studied at the Institute. The pituitary of the toad has been observedduring its seasonal variations (Masselin, Novelli), in its action on mammals(Foglia) and on the suprarenals (Porto). Pasqualini demonstrated that insipidpolyuria of the toad was observed in the absence of the thyroid or of the anteriorlobe. Stoppani (1941) carried out a very complete investigation of the regula-tion of color in batrachians and of the pharmacology of various modifying agents.
"Santa María" National Tuberculosis Sanatorium, Córdoba Province,Argentina
The average hemoglobin in man is about 15.5 gm and in women, from 13.8 to14.2, in various parts of the country (Orías, Parodi, Gargiulo, Meccheri). Quan-titative studies on vitamin K and its deficiency in certain pathologic conditionshave been made (Banfi, Tanturi, Bay and others).
The functions of the suprarenals have been studied in Rosario and in BuenosAires. In the latter city, Pinto and Vaccarezza have worked on the relationshipbetween the suprarenals and thc sex hormones. The initial disturbances followingmedulliadrenal excision are due to a passing hypofunction of the cortex, which isprevented or remedied by desoxicorticosterone (Foglia and Gerschman). Thecorticosuprarenal syndromes and their hormone or surgical treatment have beenthe subject of much study by del Castillo and his co-workers.
A great deal of interest has been shown in the thymus. It has been demon-strated that its extracts or ablation do not affect growth (Chiodi). The sex

6 PAN AMIERICAN SANITARY BUREAU
(Chiodi) or suprarenal (Houssay, Pinto and del Castillo) hormones moderate itsdevelopment, whereas those of the thyroid inerease it (Reforzo and Pinto).Involution of the thymus occurs at the same time and with a similar curve innormal and castrated animals (Chiodi).
The Institute of Nutrition, under the energetic direction of Professor Escudero,carries on a multiplicity of activities. The nutrition courses of the School ofMedicine are given there; it has a School of Dietetics, a polyclinic, infirmaries,ordinary and research laboratories, and maintains lunchrooms. It is one of theinstitutions best endowed financially. Its research work has included humannutrition, child dietetics, milk, national foods, and vitamin C in various foods.
The avitaminoses are rare in Argentina. Only 8 cases of B1 deficiency havebeen observed (Dassen, Cossio, Soldatti and Taquini.), although the circulatorysymptoms of this condition have been well studied experimentally, in dogs (Sol-dati, 1940). Only six cases of pellagra have been reported to date (Castellanos,Repetto). Scurvy is very uncommon. Severe rickets is rare, but X-ray symp-toms, usually transitory, have been found in 30% of cases (Garrahan). Sys-tematic research on child nutrition has been carried out (Garrahan, Schweitzer,Escudero, Gaing). Extensive statistical surveys of the height and weight oftens of thousands of school-age children in Buenos Aires have been made (Olivieriand Perlina Winocur).
The Institute of Cancer (officially known as the Institute of ExperimentalMedicine) directed by Prof. A. H. Roffo, is well supplied with resources andequipment for the care and surgical and radiotherapeutic treatment of malignanttumors. Branches of the Institute have been established in the interior. Experi-mental investigations have been made of the cancerigenic action of various tars(coffee, tea, mate, tobacco), of derivatives of irradiated cholesterol, and of dietsbased on cooked fats, and of the production of cutaneous cancer in rats repeatedlysubjected to the action of the sun or of ultra-violet rays. Dr. Roffo believes thatcholesterol increases in the skin through the action of the sun, and accumulatesstrongly in pre-cancerous lesions, producing cancerigenie substances throughactinic action. He has carried on an extensive campaign against the danger, ascancerigenic agents, of the use of tobacco, of excessive sun-bathing, and of theheavy pollution of the air by the unconsumed combustible products used inautomobiles.
The Bacteriologic Institute of the National Department of Health, directedby Prof. Alfredo Sordelli, is the national public health laboratory. It preparessera, vaccines, and hormones, and is the center for microbiologic diagnosis. Toit is due the knowledge of the extension and importance of the following con-tagious diseases in Argentina: brucellosis; bacillary dysentery and entericdiseases; sylvatic plague; psittacosis; human trypanosomiasis (first Argentinecase); uncinariasis; leptospira in rats; Listerella; influenza; and exanthematictyphus (frontier area). The Virus Laboratory (Dr. Taylor, of the RockefellerInstitute) is studying viruses, especially that of influenza. Among the bovineare found B. chauveaui and B. hemolyticus. Of the principal original contribu-tions and studies of the Institute, mention may be made of the following: (1)discovery of Clostridium sordelli; (2) study of the toxins and antitoxins of gangrenegerms; (3) study of the chemical nature of the heterogenetic antigen; (4) rapidpreparation of antitoxic sera of high value, which do not cause serum-sickness;(5) pharmacodynamics and immunology of the venom of snakes, spiders andscorpions; (6) isolation and properties of alkaloids of plants of native plants;(7) endemic goiter, its relation to iodine, and its prevention; (8) trypanosomiasis;(9) diagnosis and epidemiology of psittacosis; (10) rapid diagnosis and prophylaxisof diphtheria; (11) anthrax antigen and antitoxin; (12) medical entomology

HEALTHI AUTHORITIES OF THE AMERICAN
DR. ALBERTO RECIO
(Cuba)
DR. THOMAS PARRAN
(Estados Unidos)
DR. VICTOR ARNOLDO SUTTER
(El Salvador)
DR. L. IZQUIETA PÉREZ
(Ecuador)
DR. Louis HIPPOLYTE
(Haití)
REPUBLICS
1 b
7N

8 PAN AMERICAN SANITARY BUREAU
(mosquitoes, triatoma, Ixodes); (13) mycology, and so on. The Institute waschosen by the Pan American Sanitary Conference in Bogota (1938) to be thedistributing center of international biologic standards for South America.
Outstanding pathological studies include those on syphilis of the lung(Elizalde), ovarian tumors (Sammartino, in the Service of Prof. Ahumada),feminine genital anaphylaxis (Murray), bone tumors (Brachetto Brian), hemo-pathies (Bianchi, Pavlovsky), hydatidosis (Itoiz), and the kidney (Monserrat).In neurology, we have the work of del Río Hortega on tumors of the nervoussystem, that of Balado on the external geniculate body, and the studies on struc-ture and funetion of the nervous system (Acta Neurobiologica of Chr. Jakob),aphasia (Victoria, Dimitri), and encephalography (Odoriz, Caprile).
A number of discoveries have been made in the field of parasitology since thefinding of the coccidioides by Posadas and Wernicke (1890) and of the Rhino-sporidium (Seeber, 1900; 5 cases found in the country). Hydatidosis has beenthe subject of fundamental research by Cranwell and Herrera Vegas (1901),and more recently, by Castex and Greenway; the diagnosis by complement-deviation has been studied by Imaz Apathie and Lorentz (1908). Echinococcusalveolaris is rare, and was investigated by Viñas and Llambías. A center for thestudy of Hydatidosis has been created under the direction of Dr. Ivanisevich,and the Argentine Medical Association has sought the passage of a law for pre-vention of the disease.
In cutaneous American leishmaniasis notable results have been obtainedthrough intramuscular use of fuadin (Mazza), and with fuadin and yatren (3%intravenously) in the mucous forms; the treatment is shortened by using atebrinintramuscularly or infiltrating it in the ulcerated area (Mazza). Visceral leish-maniasis, reported by Mazza (1926) and the existence of which was later doubted,has been found in various foci in the Chaco (Romaña and Chagas) or other areas(Mazza).
The mosquitoes of Argentina were studied by Lynch Arribalzaga, Neiva, andPetrochi, and more recently, by Shannon and del Ponte. Hookworm disease hasbeen the subject of much investigation; Fulleborn (1927) and Orías (1930) ob-served that the hemoglobin is normal in infected areas when nutrition is good, asis generally the case. Intestinal amebiasis has also been widely studied (Castexand Greenway, 1928 to 1934). The pharmacologic action of emetine was thor-oughly worked out by Guglielmetti (1916 to 1919). Prof. Bacigalupo is the authorof a series of papers on (1) Hymnenolepis nana, fraterna, and diminuta and dis-covery of its development in various intermediary hosts (2) new intermediaryhost of Gongylonema neoplasticum; (3) discovery of Limnaea viatrix D'Orb. asthe intermediary host in distomiasis due to Fasciola hepatica; (4) emetin treat-ment of Giardia infestation; (5) demonstration of Bartonella muris in Argentina;(6) development of the microfilaria of the dog in Taeniarhynchus titillans, etc.
Now that the disease is known, more than 500 cases of human trypanosomiasiscaused by Schizotrypanum cruzi have been discovered. The diagnosis is orientedby the unilateral ocular lesion which E. Díaz and E. Chagas call "Romaña'ssign," but which Mazza says has been known since Carlos Chagas. Accordingto Mazza and his co-workers in the Mission of Regional Pathology Studies of theUniversity of Buenos Aires, dacryo-adenitis (with parasites) is endogenous, andnot on the site of primary inoculation (although Romaña produced it experi-mentally in monkeys). The local lesion at the site of inoculation they call "inocu-lation chagoona" to distinguish it from the hematogenic chagomas. Eruptionshave been observed, called schizotrypanids, morbillous, urticarious, or erythre-matic in appearance. Bayer 9706 is considered a specific, and as life-saving(100 mg. Kg) in cases of meningo-encephalitis. The Sanarelli-Schwartzman

PUBLIC HEALTH INI THE AMERICAS 9
phenomenon has been obtained in the dog, with S. cruzi. There is a histiocyticlesion of the liver typical of the disease, permitting diagnosis by viscerotomy.The cardiac histology in cardiopathies has been studied, as have also a number ofnew insect vectors, and natural infection has been found in the dog (1926) andother canines, the cat (1926), and various armadillos, marsupials, weasels, bats,and squirrels.
Under the leadership of Prof. C. Fonso Gandolfo the Department of InfectiousDiseases of the University has followed three main lines of activity: (1) teachingand research; (2) preparation of specialized physicians; (3) preventive medicine
and public health. Every year students are taken on expeditions lasting severalweeks, into the zones afflicted by the most endemic diseases, and which have theleast medical attention.
The Schools of Medicine of Argentina have been gradually preparing for the
training of specialists in various fields, awarding certificates of competence oncompletion of the course. Such advanced training is already available in legalmedicine, hygiene, tuberculosis, contagious diseases, and anesthetics.
The National Academy of Medicine has an Institute of Physical InvestigationApplied to Human Pathology, under the direction of Prof. M. R. Castex, whosework is mentioned below.
The Institute of Tuberculosis Research directed by Prof. Roque Izzo, is es-
tablished in modern quarters, and carries on such multiple activities as teaching,polyclinic and hospital care, research, and anti-tuberculosis education. Researchhas been mainly directed to the biochemical studies in tuberculosis. The chemi-
cal and pathologic sections are well-equipped and under competent personnel(Irigoyen, Marenzi, Porto).
The Institute of Hygiene of the School of Medicine, under the direction of
Prof. A. Zwanck, provides professional training for physicians and public healthnurses, and has just recently started a post-graduate course in hygiene for physi-cians, which at present is given in the evening (6 to 8).
In anatomy, Prof. P. Belou has published sizeable volumes on the anatomicrevision of the arterial system by means of stereoradiography, and has madefrequent good-will trips to other American countries. Prof. J. J. Cirio has dealtwith the classification of the extension and flexion movements. In Cordoba,Prof. Fracassi has devoted his attention preferably to the vascular system.Histology is still feeling the influence of the late Prof. P. Rojas: Varela and hisdisciples are concerned with hematology; de Robertis with the cytophysiologyof the liver, thyroid, and parathyroid; Szepsenwol with the study of the differ-entiation factors of the neurons and ontogeny of the forms of contraction of thestriated muscle; and Novinski with the chemistry of embryology.
An interesting method of radiographic examination of the lung is Politzer's"digraphy," which gives a highly instructive impression of movement. Theseparate examination of lung function, made by Vaccarezza, Lanari, Bence andLabourt, has permitted them to study spirometry, respiratory interchange. andresidual air. The curve of the composition of alveolar air in time function hasbeen investigated by Marenzi and his co-workers. Important and well-docu-mented monographs have appeared on spontaneous pneumothorax (Castex andMazzei), pulmonary atelectasis (Castex, Palacio and Mazzei), and pulmonarycancer (Palacio and Mazzei, Loizaga, etc.). The surgical treatment of tubercu-losis, and thoracoplasty have originated individual methods and technique(Finochietto, Aguilar, Brea, Taiana). Surgery of lung cancer is practiced mainlyby Professors Ceballos and Arce. Prof. Arce, who has just been placed in chargeof a course in thoracic surgery, with its own institute, praises the advantages

10 PAN AMERICAN SANITARY BUREAU
of preoperatory pneumothorax, the priority in authorship of which he hasrevindicated.
Cardiology is a clinical branch which has received a great deal of attention inArgentina, especially the use of modern methods of examination. Most of theoriginal articles are published in the journal of the Argentine Cardiology Society,and among them should be mentioned: (1) numerous important studies of phono-cardiography (Battro, Cossio, González Sabathié, Pereira, Caeiro) and the publi-cation, in Spanish and English, of the book by Braun Menéndez and Orías, "Heartsounds in normal and pathologic conditions." Its excellent illustrations of thefour heart sounds have been reproduced in physiology texts of various countriese(2) gallop rhythm (Battro, Braun Menéndez and Orias); (3) sounds of themitral valve (Battro and Braun Menéndez, Cossío); (4) myocardiac infaret(Martínez, Cossío, Padilla, Bosco); (5) electrocardiography of blocks and para-rrhythmia (Vedoya); (6) limitations of cardiac percussion (Cossío); (7) affectionsof the peripheral circulation (Di Ció) and surgical treatment (Diez, Introzzi);(8) role of the diencephalon and pituitary in the regulation of arterial pressure(Braun Menéndez, Orías); (9) exact diagnosis, by graphic methods, of the lesionscausing asynchronisms through branch block (Braun Menéndez, Solari, Orías,Battro), or extrasystole (Battro, Castex and González Segura); (10) esophagealpulses and sounds (Taquini); (11) physiopathologic study of heart disease charac-terized by cyanosis (Ayerza, Berconsky and Solari, Capdehourat and Castex,Arrillaga); (12) electrocardiogram of men at high altitudes (Capdehourat); (13)carbogen in circulatory affections (Castex and Di Ció); (14) action of histamineon the cutaneous vessels in malignant hypertonia (Battro, Castex and GonzálezSegura); (15) clinical studies of hypertension (Moia, Cossió); (16) pharmacologyof quinidine (Arrillaga, Guglielmetti and Waldorp); (17) action of acetylcholineby the arterial, humeral, or carotid route (Battro and Lanari), and many others,which cannot be included because of lack of space.
Dermatologists have given much attention to combating leprosy. The earlyefforts of Sommer and Aberastury, carried forward by Baliña, Fidanza, Puente,and Fernández, have brought about the opening of large modern leprosaria invarious parts of the country (Posadas, Isla del Cerrito, Córdoba, Rodríguez, etc.).In the scientific realm, Balifia has been interested in the classification of clinicalforms; Fernández in leprous allergy, the leprolin test, diagnosis and treatmentproblems, and histopathology; and Pierini, in the histamine test. The derma-tologists have also succeeded in having prostitution prohibited, and in securingthe establishment of numerous venereal disease dispensaries, and a considerablereduction in the incidence of syphilis has been observed. Studies in the derma-tological field have been stimulated by the teaching activities of ProfessorsBaliña, Fidanza, and Fernández, and Buenos Aires has two active societies withbranches in Rosario and Córdoba. Among the most original contributions maybe mentioned: the demonstration by Aubrun (1931) that the so-called "experi-mental pelade" of Max Joseph is due to the scratching originated by pruritusfrom partial denervation; Negroni's curative vaccine for actinomycosis (1932-1936) and studies of cutaneous mycoses; Balifia's demonstration of the traumaticorigin of liminal alopecia (1932-1937); Puente's observation of the frequency ofglandular cheilitis among Celtic groups (1934-1936) and studies on Riehl's melano-sis (1941), and Pierini's studies on the frequency of pigmentary dermatosis dueto cosmetics (1941).
In Rosario there has been rapid progress in the quality of medical investigations.Constant improvement has been observed in the various medical branches, suchas Medicine (Alvarez, Staffieri); Surgery (Cames. Tejerina); Gynecology (Araya,Borrás); Cardiology (González Sabathié); Dermatology (Fernández); Ophthal-mology (Weskamp); Neurology (Fracassi); Psychiatry (Foz, Ciampi) and others.

PTJBLIC HEALTH IN THE AMERICAS 11
The work done in the Institute of Pathologic Anatomy (Cid, Picena, Ocafa) isvery important.
The Institute of Physiology of the School of Medicine of Rosario has pub-lished 80 original articles in the last 10 years, in addition to didactic publicationsand journals. Among the most important have been those on: (1) the fact thatenervation does not atrophy the suprarenal gland (Sgrosso) and reduces thesecretion of adrenalin to infinitesmal quantities which may nevertheless bemeasured with adequate methods (Lewis and Prieto); (2) adrenalin-secretorysubstances (Lewis, Ludueña); (3) isolation (Reti) and pharmacology (Lewis,Ludueña) of the alkaloids of various kinds of cacti; (4) vitamin A and carotenes;(5) diabetes and the suprarenals (Lewis and Turcatti); (6) respiration of thetissues (De Meio); (7) factors modifying the action of the gonadotropins (Bar-man); (8) volume of the blood (Levin), etc.
The Institute of Pharmacology in Rosario is the only one permanently func-tioning in Argentina. Among the principal studies realized there have beenthose on: (1) treatment of hydrocyanide poisoning (Hug); (2) pharmacology ofsympathomimetic amines on blood pressure and the penile retractor, sensitiza-tion by ephedrin, cocaine, or pyrogalol (Ludueña); (3) microdosage of mercury(Llacer); (4) treatment of mercury poisoning by rongalita (Hug); (5) studies offibrinogen (Chiodin); (6) adrenalin-secretory action of potassium (Hug); and (7)erythrin alkaloids (Hug, Deulofeu, Cicardo).
Córdoba has an important research center: the Institute of Physiology directedby Prof. Oscar Orías, where studies have been carried out on: (1) heart sounds inadults, children, the fetus, and pregnant women; (2) sex endocrinology of thetoad and comadreja (weasel); (3) pharmacology of Fagara coco, Nierembergiahippomanica, and Lycopodium saururus; (4) pharmacology of snake venom; (5)acetylcholine and vagal escape; (6) electrocardiography; (7) ventricular fibrilla-tion; (8) blood groups; and (9) vital capacity. Among the collaborators areI. L. C. de Allende, A. Segura, S. Amuchástegui, I. Pereira, E. Moisset de Espanés,E. Soaje Echagúe, and others.
The Institute of Tuberculosis, directed by Prof. G. Sayago, provides a greatdeal of hospital care, and teaching, and has a full-time bacteriologist (F.Schwarz). The various Services of the School of Medicine are in constant prog-ress, including those of Surgical Clinic (P. L. Mirizzi and J. M. Allende), MedicalClinic (T. Castellanos and J. M. Allende), Pediatrics (J. M. Valdés), Anatomy(H. Fracassi), Obstetrics (C. Lascano), Ophthalmology (Ureta Zavalía), Oto-rhinolaryngology (H. Walker), and others. Among the most important recentpublications are the book by Prof. P. L. Mirizzi on "Physiopathology of the liverand bile ducts, operative cholangiography," 1939, and that of Prof. Rámon A.Brandán on "Climatology of Córdoba Province," 1940. Brandán has devotedmore attention than any other worker to the medical climatology of Argentina.
It would be impossible to review the developments in Surgery, Obstetrics,Pediatrics, and the medical (INeurology, Psychiatry, Gastroenterology) andsurgical (Urology, Ophthalmology, Otorhinolaryngology, Orthopedics) special-ties, due to lack of time, of space, and of competence on the part of the narrator,since these branches would require an extensive exposition.
Original research in medicine in Argentina has been steadily developing inquantity and quality. It is most desirable that all the American countriesshould know the scientific work being done in each, in order to avoid tendenciestoward provincial localism, or toward an imperious disregard of one's neighbors.Mutual knowledge, objective and serious criticism, moderation in the use of re-ciprocal praise, the exchange of teachings, and mutual assistance, should berapidly and intensely increased, for the sake of the consolidation of the friend-ship and medical and public health progress of the Pan American countries.

12 PAN AMERICAN SANITARY BUREAU
PUBLIC HEALTH IN BOLIVIA*
By Dr. ABELARDO IBÁIEZ BENAVENTE
Minister of Labor, Public Health, and Social Welfare
In November, 1940, the Department of Hygiene and Public Health was con-solidated with the Department of Labor and Public Welfare. The problem ofpublic health in Bolivia is aggravated by such factors as the heterogeneity of thepeople, with a corresponding diversity of languages and customs, lack of educa-tion, inadequate means of communication, great distances separating a large partof the population from urban areas, low standards of living accompanied by poorhousing and nutrition deficiencies, venereal diseases, alcoholism, and the im-moderate use of coca.
The present plan provides for both preventive and therapeutic measures,and is to be extended to all sections of the country. The following services andinstitutions are to be established: traveling clinics, to supplement the presentinadequate systern of health stations located ini certain municipalities; increasedhospital facilities, including the construction of a new hospital in La Paz (1,000beds), and another in Oruro (300 beds), tuberculosis sanatoriums in La Paz andCochabamba, seven hospitals in other communities, three frontier hospitals, asanatorium at Buenaventura, a national leprosarium on San Silvestre Island inthe Mamore River, and three temporary leprosaria, one national insane asylumin Sucre, maternity hospitals in Cochabamba and Puerto Suárez, and a hospitalfor malaria cases in Mizque. (At present Bolivia has 37 hospitals with a totalof 3,363 beds.)
Since almost all of the public health personnel has had no special training,there is urgent need for the creation of a public health institute together with amedical school for the preparation of hygienists, sanitary engineers, laboratorytechnicians, radiologists, and similar specialists. An appropriation for thisprogram is included in the 1942 budget.
Malaria, perhaps the greatest cause of sickness and death in Bolivia is preva-lent in 80% of her territory. The Government has appropriated the followingamounts for control work: 500,000 bolivianos for Tarija, Sucre and the Yungas ofLa Paz; 1,000,000 for Cochabamba and vicinity; 300,000 for Mizque,' in additionto the profits of the National Quinine Factory. The latter now furnishes quinineto the most severely stricken areas, and its production is to be increased from thepresent average of 100 kg. to 1,000 kg. per inonth.
One of the consequences of the Chaco War was the migration to the urbanareas of rural people who had little immunity to certain diseases. Tuberculosisspread very rapidly among them. In 1935 two small hospitals, several tuber-culosis dispensaries, and a preventorium for children born in tubercular homes,were established. Lack of funds has prevented the construction of additionalfacilities. Thc mligration also resulted in an increased spread of venereal dis-ease, for which treatment in the contagious period is now compulsory. Pre-marital examinations are made free of charge, upon request.
There are sporadic outbreaks of yellow fever and plague in the forest regions,but they do not reach the stage of major epidemics. The Government supportsan anti-plague service, and contributes to the yellow fever control service main-tained in collaboration with the Rockefeller Foundation.
* Taken from the Report of the Minister from August 1940 to date, presented to the National Congress.l The rate of exchange of the boliviano on Dec. 6, 1941, was 43 to one dollar.

PUBLIC HEALTH IN THE AMERICAS 13
To combat goiter, which is now common in a large area of the country, theGovernment plans to establish a salt monopoly to insure the necessary iodinecontent in all table salt.
From 98% to 100% of the Bolivian population, including children, suffer fromintestinal parasites-hookworm being the most common. Joint commissions ofdoctors and constructors are being planned, to supervise the provision of latrinesfor all houses in the affected regions.
A large scale vaccination program is being tried in an effort to conquer typhus,which causes thousands of deaths every year. The establishment of compulsoryvaccination against typhoid fever has resulted in a marked decrease in this dis-ease. Smallpox has disappeared almost entirely from urban communities.
Building of the Ministry of Labor, Public Health, and Social Welfare, of Bolivia
It is estimated that 90% of the people suffer from malnutrition. The nucleusof a National Institute of Nutrition has been created, and plans are being madeto establish facilities for feeding expectant mothers and children, and also asystem of popular restaurants.
A four year public health plan has been formulated calling for the allocationof 12% of the national budget to health purposes. Thc proportion is to be i¡i-creased to 20% by the fourth year. A national orphanage-school with a capacityfor 700 to 800 children, including war orphans, was opened in May, 1941. InSucre, 150 abandoned children and war orphans are being cared for; in Oruro,250, in Cochabamba, 400; and there are National Child Welfare units in Potosi,Santa Cruz, Tarija, Trinidad, Tupiza, Uyuni, Vallegrande, Camargo and Roboré.
To relieve the acute housing crisis, the Department of Public Welfare willsoon begin the construction of 150 houses in La Paz, and 50 in Oruro. Theseprojects are only the beginning of a national housing program.
14 PAN AMERICAN SANITARY BUREAU
DEVELOPMENT OF MEDICINE AND SCIENCE INPRESENT-DAY BRAZIL*
By Dr. AFRANIO PEIXOTO
Professor in the University of Rio de Janeiro
The scientific and medical development in Brazil in the last forty years has ofnecessity depended on the social, economic, and political conditions of the countryand of the world. During this period there have occurred two disastrous wars,originating in quarrelsome Europe as the result of the spirit of political imperial-ism which ought to be out-moded.... But it seems that in the European tradition,this is not to be. There progress has a warlike tradition with which it is in-separably mixed. The fashion reaches America, and with it, the necessity fordefense. The internal conflicts in America have been imitations of Europeanones; as have been our would-be (sometimes civilian) Napoleons. Americanscientific progress, and with it that of Brazil, reflects these world upheavals....
Nevertheless, it has its Continental aspects. Spain was not able to exterminateyellow fever, even though Carlos J. Finlay had pointed out the way. The Frenchfailed economically in Panama because they had failed scientifically. ThenAmerica came forward with her own resources. In 1900 the American commissionappointed by Sternberg and composed of Walter Reed, James Carroll, AristidesAgramonte, and Jesse Lazear fixed the responsibility for yellow fever (whichEurope called "American typhus") on a striped mosquito, identified by Howardas Aedes aegypti-the same mosquito singled out by Finlay. Acting on his con-vietions of this demonstrated truth, Gorgas sanitated Cuba. Other confirma-tions followed, with the experiences of Juan Guiteras (1901) in Las Animas, Cuba;of Pereira Barreto, Adriano de Barros, and Silva Rodrigues, under the inspirationof Emilio Ribas and Adolfo Lutz in S. Paulo, Brazil (1903); of Parker, Beyer, andPothier (1903) and Rosenau, Parker, Francis, and Beyer, in New Orleans, U. S. A.;and, finally, of Marchoux, Salimbeni and Simond, of the Pasteur Institute ofParis, working in Rio de Janeiro (1903). The supreme sacrifice was not lacking:Lazear, bitten by a mosquito in a sick-ward, and Miss Mass, a nurse who volun-teered for some of Guiteras' experiments, died of yellow fever; two others diedduring the Guiteras experiments, and two more in those of Oswaldo Cruz, Mar-choux, Salimbeni and Simond. Other experimentors, such as Carroll and Moran,became seriously ill, proving the transmission of the virus by the mosquito.
The work bore fruit: W. C. Gorgas cleaned up Habana (1901); then J. H. Whitedid the same for New Orleans, Eduardo Liceaga for Vera Cruz, Carneiro deMendonQa for Rio de Janeiro (1903-8), Sir Rupert Boyce for the English Antilles,Gorgas and Carter for Panama, Lyster for Central America, Connor for Ecuador,Hanson for Peru. In 1908, after Rio de Janeiro was freed from yellow fever, camethe turn of Manaus and Belem (1913), with the work of Teofilo Torres and Pedroso.
The new theory was not accepted in Brazil without a struggle. Argumentsbecame fanatic. Professor Rocha Faria was severely criticized in medical sciencefor not admitting the exclusive role of the Aedes aegypti (then known as Stegomyiafasciata) in the transmission of yellow fever.... Ironically, today a number ofspecies have been shown to transmit the virus in Africa, in the West Indies, andin South America. In the jungle, Aedes aegypti is.actually absent.... Aedesscapularis, A. fluviatilis, A. leucolelaenus, and even one of another genus, Haema-gogus capricorni, have justified Rocha Faria in his protest against public healthfanaticism. None the less, such fanaticism-the "believe or die" policy-hadits uses. It brought about the sanitation of America.
* For additional, extensive reports on public health in Brazil see the articles by Barros Barreto andParreiras in forthcoming issues of the BOLETIN.

PUBLIC HEALTH IN THE AMERICAS 15
But the victory proved deceptive. Yellow fever, once the battle-or thearmed sanitary truce-had ended, returned. It came from Northeastern Brazilto Rio de Janeiro, in 1928-29. And, significantly, this once-so-urban diseasebecame suburban. It was eradicated by Clementino Fraga. But yellow feverwas not done. It reappeared not long ago (1932) as jungle yellow fever, reportedfrom Colombia, Venezuela, Brazil, Bolivia . . . by experts of the RockefellerFoundation, headed by Fred. L. Soper. In Brazil serious studies were made byBeaurepaire de Aragao. Yellow fever: first urban, then suburban, then sylvatic-these the avatars. An epizootic among wild animals, eventually spread to man. . .at times domesticated among us, causing epidemics . . . such is the presenttheory. When these epidemics are conquered, the focus remains, as does thedanger. An armed sanitary truce must be enforced-the mosquito-killer, theinspection of foci, viscerotomy, immunity tests-these are the weapons.
To meet the danger, new methods have been introduced, nearly all of themAmerican. First, the experiments with tremendously infective yellow fever virus,in the blood: their price the laboratory martyrdom of Adrian Stokes, HowardCross, Hideyo Noguchi, William A. Young, Paul Lewis, Theodore Hayne, Mau-rice Wakeman.... The macacus rhesus monkey is discovered susceptible (Stokes,Bauer, Hudson), as are other monkeys: Cubus macrocephalus (Davis and Shan-non), M. cynomolgus (Aragao), and M. speciosus (Aragáo). Even better, thewhite rat, through intra-cerebral injection (Max Theiler). Viscerotomy, usedby Soper and the Rockefeller workers, followed by the anatomic-pathologicexamination of cases dying of strange fevers, proved that yellow fever was spreadthrough much of South America, up to the Bolivian highlands, involving all ofBrazil, Colombia, Venezuela, the Guianas....
Then came the vaccines, convalescent serum, autolysated organs. The lastword has not yet been spoken. The identity of American and African virus iscertain. The identity of jungle, suburban, and urban yellow fever, unquestion-able. The struggle, and the studies which prepare the means for the struggle,go on. America has taken the matter in hand, dispensing with the aid of for-eigners.
Oswaldo Cruz had in Brazil another and greater influence: he introduced thelaboratory into clinical medicine, and made from a serum-therapy institute aschool of experimental medicine. A revolutionary measure was the regulationmaking smallpox vaccination compulsory in Rio in 1906 (Arnoldo Vieira de Car-valho had already thus eradicated the disease from Sao Paulo). Disciples ofCruz made memorable discoveries: Rocha Lima found the Ricketzia prowazeki,cause of exanthematic typhus; Gaspar Viana developed the treatment of cutane-ous leishmaniasis by antimony tartrate; Arthur Neiva anticipated Nocht inobserving the quinine-resistance of the hematozoon; Carlos Chagas discoveredAmerican trypanosomiasis; Beaurepaire de Aragáo made hundreds of scientificcontributions of inestimable value; Cardoso Fontes demonstrated the filterabilityof the tuberculosis virus (1911), anticipating Vaudremer (1922) by 11 years. Theschool of Sao Paulo, under Emilio Ribas, Adolfo Lutz, and Paula Souza, has like-wise had a far-reaching influence.
An enfeebled pestilence is not a danger past. Caroco fever or ingua de frio(Amadeu Fialho, Antonio Periassú) is a frustrate, ambulatory form of plaguewhich may eventually become acute and fatal.... Smallpox appears in the interiorin its mild form of alastrim.... Trachoma, which we allowed to enter from theMediterranean, with Syrian and Italian immigrants, is spread over Sao Pauloand Minas, and has a focus in Ceara (Sanson).... Snake bites, which killed orpoisoned around 5,000 persons a year, were combated with specific serums devel-
16 PAN AMERICAN SANITARY BUREAU
oped by Vital Brazil, and nmade known in the United States by Afranio doAmaral.
During the last 40 years tuberculosis has shown no change. Culpable aremalnutrition, over-crowded, unihygienic housing, lack of knowledge of modernmethods of diagnosis and treatment. First came the costly sanatoria for therich, and then those for the poor, inadequate because they are not supplementedby economic assistance for the inmates, early treatment, and security for thefamily. Our tuberculosis mortality is 250 per 100,000; that of the United Statesis 47. Manoel de Abreu invented the system of taking a photograph of a radio-scopic image, so that instead of the cost of 20$000 or $1.00 for an X-ray, the ex-pense is only 200 reis, or 1 cent, for an "Abreugraph" (Sayago).... The wholepopulation could be surveyed this way, and the pre-tuberculous or cases withoutsymptoms (Aloysio de Paula), the declared cases (Assman-Redeker early infil-trations, without fusion), and the open, cavernous, contagious cases, discovered.
Air view of A. gambiae foci on the Ceará coast, Brazil
... All these might be treated surgically, with the rudimentary Forlanini method,or even more serious operations (costal, pleural, etc.), the surgery being supple-mented by proper feeding and vitamins. The tuberculosis problem of today isone of diagnosis and treatment guided by the X-rays. Adequate nutrition,proper housing, hygiene, complete the program. It is in the hands of an intelli-gent though not extravagant government. It will cost something, of course, toovercome the antiquated medical routine .... The general measures, housing,nutrition, avoidance of contagion, have given results the world over. Brazilremains behind, with her heavy burden of tuberculosis. ... It has not decreased;it actually increases.... I do not wish to omit this note of warning, because thepublic good is worth the sacrifice of some restraints. There can be no patrioticreservations against this disease....
Likewise with lcprosy. It was disregarded, because it seemed tending todisappear, in certain regions, as in Bahia. Its contagiousness appeared to belimited. But the constant foci, in Para and Maranhao, had their counterparts,in Sao Paulo and Minas. The estimated number of lepers was increasing. Adolfo
PUBLIC HEALTH IN THLE AMERICAS 17
Lutz calculated them at 10,000; Valverde, at 15,000; Pupo, at 27,000; Lindenberg,at 30,000; Eduardo Rabelo gave the figure 50,000. This is high indeed: higherthan the 5,000 of Colombia; the 9,000 of Madagascar; the 11,000 of the DutchIndies; the 15,000 of the French Indies; the 40,000 of Japan; it is exceeded by the100,000 of British India. But in proportion to density of population, India's400 million to our 40 million, Brazil has the unenviable record for the highestamount of leprosy in thc world. Considering the magnitude of the problem,little has been done. There are some model leprosaria, in Sao Paulo, in Minas,in Espirito Santo, and in Rio; others are being built in the northern part of thecountry, but these are almost nothing, reaching two or three thousand out of ourmany.* Meanwhile, Souza Araujo, familiar with the international problem ofleprosy, has been as one vainly crying in the wilderness. Wc are not attracted bythe idea of isolation, even partial isolation, which has accomplished so much,
Headquarters of Federal Health Officer, Fortaleza, Ceará
from Norway to the Philippines .... We are waiting for treatment-for rapidtreatment.
Let us close on the brighter note of a great sanitary triumph. The rapidaerial-maritime advice-boats brought to us at Natal, from Dakar, the worstpossible immigrant. No heretical, communistic, or nazi invasion could be asdangerous as the invasion of Anopheles gambiae, the deadly African mosquitowhich was identified here in 1930 by Dr. R. C. Shannon. Other malaria-carryinganopheles transmit the disease in a bare 5% of bites; the gambiae, in 100%. Asmall demonstration was the epidemic in Natal and vicinity, with tens of thou-sands of deaths (at least 40,000 cases, 8,000 deaths). Souza Pinto estimated theannual number of deaths in Brazil from malaria at 8,000, with about 800,000 cases.(Barros Barreto multiplied these figures by ten.) What then would the spreadof A. gambiae mean to Brazil? Ruin, utter and complete! And to the rest of thecontinent? The United States understood, and in defending herself, defended thecontinent. In cooperation with the Brazilian Government, which shared in the
*Eunice Weaver (Bol. Of. San. Pan., June 1942, p. 569), reports that about 23,000 out of some 30,000known lepers are or soon will be interned in leprosaria, and describes the active campaign now beingwaged against the disease.
18 PAN AMERICAN SANITARY BUREAU
expenses, the Rockefeller Foundation undertook the extermination of the Anophe-les gambiae, which had already reached -Ceará. In 1941 the miracle was an-nounced . . . the unwanted invader had been eradicated from America; the leastdesirable of the undesirables was gone.
To review other developments: Our geology and archaeology, derived fromFederico Hartt, Orville A. Derby, and John Casper Branner, had worthy succes-sors in Arrojado Lisboa, Calogeras, Gonzaga de Campos, Eusebio de Oliveira,Betim Paes Leme. In phytography Lindmann, Lutzelberg, Hueber, Sampaio,Hoehne, won distinction, as did Goeldi, von Ihering, Melo Leitao, and CostaLima in zoology. Roquete Pinto, in "Rondonia" made the finest ethnographicjourney of our times, as von Martius and von den Stein did in other days. MiguelOsorio is our Number One physiologist, as a result of his original findings. Dec-ades ago Nina Rodrigues created a school, not only of experts in legal medicine,but also of anthropologists and ethnographists, a school which preceded themodern "Africanology" of the American Herskovits. Arthur Ramos is our major"negrologist." In another field, that of fingerprint identification, LeonidioRibeiro discovered the precariousness of these marks in various nervous diseases,in leprosy, in certain manual professions, and opened a new chapter in medicine,"dactylodiagnosis." Finally, Anisio Teixeira brought from North Americatheir educationalist enthusiasm, and has become our Dewey, not only because ofhis practical achievements, in Baia and Rio, which his opponents were unable todestroy, but also because of the written and otherwise disseminated proselyticinfluence, both of himself and of his numerous followers.
This rapid review is, or has attempted to be, an act of faith on the part of Brazil,an expression of confidence in our continent. We in America are capable of a fewthings. The United States of North America, our oldest brother, is taking theplace of our old and decrepit mother, suffering, poisoned Europe.... Our newerbrothers all have something to offer. Brazil is an honor to her family.
PUBLIC HEALTH IN CHILE
By DR. PEDRO AGUIRRE CERDA
President of the Republic
Thanks to the excellent work of the Public Health Service Chile has been freeof epidemics since the end of 1939. There have been only one or two sporadic casesof typhus. Whereas in 1938, 70% of the conscripts serving in Arica contractedmalaria, in 1940 there was not a single case. The malaria control services arebeing extended to the Lluta Valley.
Maternal and child welfare, including nutrition, have received special consider-ation, and it is hoped that within two or three years the present high infant mor-tality rate will be greatly decreased.
Through the social security (compulsory insurance) program protection isprovided against the risks of sickness, disability, old age, widowhood, and or-phanage, and attempts are being made to extend medical care to the families of theinsured. At present, the Social Security Fund cares for the children of the in-sured until they are two years of age. A complete cycle of medical attention isbeing planned to care for the mother from the beginning of pregnancy, and for thechild from birth until he is old enough to work. He then becomes eligible in hisown right for medical service throughout his lifetime. By this means 3,600,000
PUBLIC HEALTH IN THE AMERICAS 19
persons will be eligible for medical benefits, including 200,000 children who arenow excluded. It is suggested that merging the medical section of the SocialSecurity System with Public Assistance would make this plan more feasible.
The Goverament, through the Popular Housing Department, is doing its ut-most to solve the acute housing problem. Low-cost, hygienic, comfortable homeshave already been constructed for workers in 17 cities. The Housing Depart-ment's policy is to establish its communities within urban limits so that the people
:t·;~1 y
'Iwo views of garbage burial in Viñia del M4ar, Chile
may more economically enjoy paved streets, electric light, pure water, gas, andsewage disposal, as well as the opportunities for spiritual, intellectual and phys-ícal activity offered by schools, thcaters, and libraries.
The popular restaurants (33, excluding those dependent on the UnemploymentCommission) served approximately 2,000,000 meals to 1,000,000 people in 1939;and 4,000,000 meals to 1,200,000 people in 1940. During 1940 this Service, withl thecooperation of municipalities and School Aid Councils, furnished breakfast andlunch to the primary school children, supplying 1,500,000 rations.
20 PAN AMERICAN SANITARY BUREAU
Tlie birthday of the pattriot General Bernardo O'Higgins has been set aside forthe solicitation of funds and goods for the needy, and in Santiago 1,500,000 pesosand a large quantity of supplies were collected.
The State does not have sufficient resources to establish rehabilitation schoolsfor certain unfortunates, but 500,000 pesos have been allocatedto eachof the threenational vocational workshops established in 1940 (to aid deserted mothers, chil-dren, and handicapped persons). Thos- for children and the handicapped areoperating at full capacity, with very satisfactory results, and that for motherswill be opened in 1941.
PUBLIC HEALTH PROGRESS IN COLOMBIA
Ogficial Report from the Ministry of Labor, Health and Social Welfare
Colombia has not lagged behind in the steady march of public health progress.The different administrative systems which she has adopted, each seeking tooutdo the other, have placed her on an equal position with the rest of the Americanrepublics, particularly since the beginning of the Pan American Sanitary Con-ferences.
At first (some 50 years ago), there existed a central office called the SuperiorBoard of Health, which limited its activities to the distribution of smallpoxvaccine and consideration of the public health problems of the Capital. Theseproblems were solved in an empirical or romantic fashion, in spite of the scientificreputation of the members of the Board. This board was followed by a CentralBoard of Hygiene, and then by the present National Department of Health,which gained in prestige through its increased range of action although as a de-pendency of various ministries.
After having been a part of the Ministries of Government and Education andPublic Health, it became autonomous in 1932 as the National Department ofHealth. There then began an era of health commissions and units which havebrought the benefits of public health to all parts of the country. It is only just torecall, however, that already when the National Public Health Department was apart of the Ministry of Agriculture and Commerce, the Minister at that time,Señor Dn. Jesús del Corral, a man of energy and understanding, had secured thecooperation of the Rockefeller Foundation for a campaign against hook-worm.
When the Ministry of Labor, Health and Social Wclfare was created, publichealth attained its due recognition. The present organization has cooperativerelations with such organizations as the Fomento Municipal (Municipal Im-provement Fund), which is providing a large number of cities with water supplyand sewage systems, and slaughterhouses; the Department of Social Welfare,which exercises supervision over charitable bequests, which in this traditionallygenerous country reach a considerable amount; the Child and Maternal WelfareDepartment, which is a model of its kind; and an effective tuberculosis controlcampaign. It is firthermore well known that Colombia's anti-leprosy campaignis a model from various points of view including treatment, cure, and research,for which it has excellent facilities.
Research.-Colombia has a number of research institutions which place it on ahigh level in this field. Thanks to the general organization of the Ministry, socialproblems and those of preventive medicine always find prompt consideration andsolution.

PUBLIC HEALTH IN THE AMERICAS 21
Tuberculosis.-The increased range and diversity of activities in tuberculosiscontrol are shown by the statistics. Thus, the number of dispensaries has in-creased from 3 in 1936 to 4 in 1937 and to 27 in 1940; the number of persons attend-ing the dispensaries has grown from 10,000 in 1936 to 139,854 in 1940. In 1941 anadmirably equipped sanatorium was completed in Bogotá, which will be opened inJanuary, 1942. The "La Maria" sanatorium in Medellín is being enlarged.
Yellow Fever.-In yellow fever rescarch notable progress has been made. In1939 a laboratory was built and fully equipped. The vaccine produced by thislaboratory has been requested by a number of foreign countries.
Leprosy.-Much progress has been made in the campaign against leprosy andthe National Health Laboratory is producing high quality esters, so that Colombiahas an excellent supply of these materials. In fact a number of Central andSouth American countries have ordered the products of this Laboratory. Thewelfare of the healthy children cf lepers has received attention through the
Aeration tank, water supply plant, Bogotá, Colombia
construction of several hornmes for them, and the three leprosaria of the countryhave been considerably improved in recent years.
Child and maternal welfare.-The Child and Maternal Welfare Services havebeen considerably extended, and include gotas de leche (milk stations) nurseryhomes, nursing rooms, kindergartens, children's hospitals,healthy children clinics,school dental services, pre-natal and maternity services. There were more than800 such institutions in operation in 1940 with a total of 612,492 persons in at-tendance.
Sanitary commissions.-The local sanitary commissions and units, numberingmore than 100, actively carry on two kinds of services, 1, preventive, designed toinsure the sanitation of the environment and 2, curative, through the furnishingof medical and social care on a limited basis.
Rural sanitation.-In recent years rural hygiene work has been intensified,especially among coffee plantation workers, and several excellent health centershave been established in the coffee regions.

22 PAN AMERICAN SANITARY BUREAU
General health.-Energetic scientific campaigns are being carried on againstmalaria, yaws, bartonellosis, and venereal diseases. As a further means ofimproving thc general health, the Government is undertaking an activc campaign
Sanitation of Cúcuta, Colombia: Above: Drainage of standing water in streetgutters; below: canalization of a stream on outskirts of city.
to provide sanitary water and sewage systems in the different cities of the country,and more than 200 such systems are already being installed.
Narcotic control.-An appreciable degree of success has been obtained in thenarcotic control campaign, and the Secretary of State of the United States hassent Colombia congratulations for her work in this field.
PUBLIC HEALTH IN COSTA RICA
By Dr. MARIO LUJÁN FERNÁNDEZ
Secretary of Public Health and Social Welfare
Costa Rica has some 656,129 white inhabitants, and only 5,000 Indians, a condi-tion which has been very favorable to her organization, cultural development,and public health progress.

PUBLIC HEALTH IN THE AMERICAS 23
Public health work began in 1914, with the creation of the School HealthDepartment. In 1916 the first Hookworm Control Department was established,the forerunner of the present organization. In 1921, the Undersecretariat ofHealth came into being, followed by the promulgation in 1923 of the Public HealthLaw, which is still in force. In 1928 the Secretariat of Public Health and SocialWelfare was created, and the most important technical divisions were developed.The Secretariat now operates through coordinated and centralized services of:Epidemiology, Sanitary Engineering, Rural Hygiene (health units), SchoolHealth, Child and Maternal Welfare, Institute of Hygiene, Tuberculosis control,Venereal Disease control, Malaria campaign, Health Education, Vital Statisticsand, finally, the supervisory social assistance service, under the Department ofSocial Assistance and Protection. To carry public health to all parts of thecountry, there are 23 health units, three traveling clinics, three rural assistancecenters, eight rural maternity hospitals, and 17 official treatment centers.
Funds.-Public health budgets have reached encouraging figures: 1928,1,407,932.09 colones (4% of the national budget); 1930, 1,162,523.58 (3.2%); 1935,
Left: Department of Health and Welfare, Costa Rica; right: tuberculosiscontrol office.
1,802,922.97 (4.8%); 1939, 2,336,114.79 (5.5%), and 1940, 2,445,320.94 (5.4%).Furthermore, the welfare services have a present budget of 12,450,000 colones,the administration of which has been in the hands of the Secretariat of Healthsince 1940, when the Law of Social Assistance and Protection was promulgated.Supervisory work was begun by the National Health Council, now no longer inexistence (1936-1940).
The health units, which are the pivot of the organization, and the SanitaryEngineering and Epidemiology Services, have carried out health programs innearly all the country. Around 24,575 sanitary latrines have been built, anidmany drainage and other malaria control projects have been completed in thelowlands. Malaria is not a primary public health problem. During recent yearsthe preventive aspect of public health has been stressed, and from 1937 to 1941 theEpidemiology Service vaccinated 7,205 children against diphtheria, and 12,363against typhoid. Each health unit has a vaccination program, oriented throughthe Vital Statistics reports, and also maintains a public hygiene campaign,through the medium of cantonal health inspectors.

24 PAN AMERICAN SANITARY BUREAU
Tuberculosis.-Tuberculosis control work, which is under a central authority,is carried on through preventive services, dispensaries, a preventorium, travelingclinic for the finding of incipient cases, sanatorium for adults and children, socialworkers, and so on. At the present time, (January 1941), 72,795 persons havebeen examined.
Venereal disease.-For venereal disease control there are dispensaries funetion-ing as annexes to the first-class health units. This problem is a very serious one,and much remains to be done.
Nursing.-Costa Rica has at present 140 nurses, working in three sections:obstetrics, social workers, and school nurses. It is hoped to create a group ofall-round public health nurses, and the first step has been taken with the establish-ment of the Department of Visiting Nurses and Social Service.
Rural health center, Paraíso, Costa Rica
Child and maternal welfare and school hygiene.-Child and maternal and schoolhygiene has been developed on the public health and social welfare plane through:prenatal clinics (36), rural maternity hospitals, rural midwife service, nutritioncenters, gotas de leche (milk stations), infant clinics, school physicians, and schoolclinics.
Vital statistics.-The Vital Statistics Department, recently reorganized,maintains up-to-date information on the fundamental health problems: generalmortality, child and maternal mortality; control of communicable disease;medical attention, and so on. Morbidity services are now being extended so as tofurnish additional data as a guide for public health campaigns. Costa Ricanpublic health authorities wish to base their activites upon accurate informationso as not to waste their efforts. General death rate: 1901-1905, 26; 1906-1910, 27;1911-1915, 25; 1916-1920, 29; 1921-1925, 24; 1926-1930, 23; 1931-1935, 21; 1936-1940,18. Infant death rate: 1916-1920, 203; 1921-1925, 232; 1926-1930, 178; 1931-1935,

PUBLIC HEALTH IN THE AMERICAS 25
159; 1936-1940, 137. Principal causes of death: malaria: 1901-1905, 33; 1906-1910,56; 1911-1915, 53; 1916-1920, 100; 1921-1925, 96; 1926-1930, 198; 1931-1935, 202;1936-1940, 115; tuberculosis: 1901-1905, 77; 1906-1910, 87; 911-1915, 81: 1916-1920,92; 1921-1925, 84; 1926-1930, 92; 1931-1935, 87; 1936-1940, 81; typhoid: 1906-1910,24; 1911-1915, 20; 1916-1920, 12; 1921-1925, 18; 1926-1930, 18; 1931-1935, 13; 1936-1940. 10.
Improvements.-Infant mortality has dropped from 258.4 in 1925 to 132.4 in1940. Costa Rica's birth rate, which has shown little variation in the last 25years, is now one of the highest in the world. Increase: 1920, 11; 1940, 25.6.
Construction.-A Department of Public Health Architecture has been created,to bring greater harmony into building construction.
Other services.-Among the auxiliary services may be mentioned the NarcoticsControl, Pharmacy, Maritime Sanitation, Aerial Sanitation, and Juridical sec-tions, and the School of Hygiene for public health personnel.
Problems to be solved.-The problems still awaiting solution are those commonto other Caribbean countries: (1) soil sanitation, involving sewers, latrines, wastedisposal; (2) nutrition, for which a Council has been created; and (3), the mostimportant, driniking water supplies.
Water.-With the cooperation of the Pan American Sanitary Bureau, theSecretariat has secured the promulgation of a Law on Drinking Water Supplies,which representes an important forward step, since the control of water suppliesshould be in the hands of the national department of health.
Program.-Costa Rica's public health program contemplates, therefore, thefulfillment by health units of their three chief functions: Hygiene, Prevention,Assistance; the transformation of present aqueducts into safe water supplysystems; the development and extension of the tuberculosis control campaignin all social groups; thc energetic continuance of the soil sanitation progranm;and, finally, a favorable solution of the venereal disease problem, for the sakeof Costa Rica's people.
Social security.-Another far-reaching action was the promulgation, alongwith the Drinking Water Supplies Law, of the Social Security Law. It is hopedthat Social Security may be brought into operation without affecting vital publichealth services, and it is believed that this can be done, since the Costa Ricanhealth organization already has the scientific, preventive medical, and publichealth equipment which will enable it to develop without duplication of services.
The Costa Rican government proposes to raise the national standard of healththrough positive public health and social action, and to this end it has the publichealth organization already here described, and the prospective influence ofsocial security.
PUBLIC HEALTH IN CUBA
By Dr. ALBERTO RECIO
Director of Health
The Island of Cuba, and particularly the city of Habana, were considered incolonial times the Inferno of America. Yellow fever, malaria, smallpox, dysen-tery, typhoid fever, tetanus of the newborn, glanders, and even cholera and otherdiseases periodically decimated its population, from the days of the Conquest
26 PAN AMERICAN SANITARY BUREAU
until the year of Independence. During the Intervention Government of theUnited States, after the country was frced from Spain in 1899, sanitation wasbegun and campaigns were waged against the prevailiing epidemic and endemicdiseases.
The Provisional Military Government lasted for two years and five months,and was under the direction of a physician, General Leonard Wood, who con-sidered the improvement of the precarious health of an impoverished people thegreatest of his duties. In this bricf period the bases were laid for a public healthorganization which, carried to completion by succecding administrations, soonconverted the former Inferno into one of the most prosperous and healthy tropicalregions in the world. Besides thc subjection of Habana to the most thoroughcleaning ever given a city, the program saw the organization in 1900 of two sani-tary inspection services, in the charge of 100 Cuban physicians and directed byMajor William Gorgas, and also the establishment of the Services of Sanitationand Disinfection, Statistics and Demography, and Orders, Archives, and Corre-
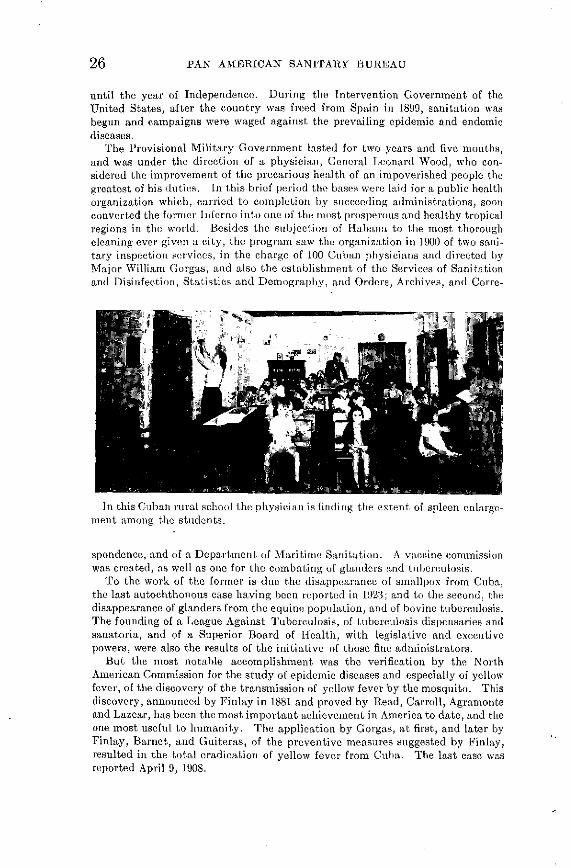
In this Cuban rural school the physician is finding the extent of spleen enlarge-ment among the students.
spondence, and of a Department of Maritime Sanitation. A vaccine commissionwas created, as well as one for the combating of glanders and tuberculosis.
To the work of the former is due the disappearance of smallpox from Cuba,the last autochthonous case having been reported in 1923; and to the second, thedisappearance of glanders from the equine population, and of bovine tuberculosis.The founding of a League Against Tuberculosis, of tuberculosis dispensaries andsanatoria, and of a Superior Board of Ilealth, with legislative and executivepowers, were also the results of the initiative of those fine administrators.
But the most notable accomplishment was the verification by the NorthAmerican Commission for the study of epidemic diseases and especially of yellowfever, of the discovery of the transmission of yellow fever by the mosquito. Thisdiscovery, announced by Finlay in 1881 and proved by Read, Carroll, Agramonteand Lazear, has been the most important achievement in America to date, and theone most useful to humanity. The application by Gorgas, at first, and later byFinlay, Barnet, and Guiteras, of the preventive measures suggested by Finlay,resulted in the total eradication of yellow fever from Cuba. The last case wasreported April 9, 1908.

PUBLIC HEALTH IN THE AMERICAS 27
When the Republic was restored in 1902, Finlay and Barnet succeeded Gorgasand his assistant Furbush, and extended the benefits of public health to the w holecountry. The Superior Board of Health, whose decrees were executive in nature,in 1906 promulgated the Sanitary Ordinances, applicable to municipalities.Attention was given to tuberculosis, diphtheria, and other diseases, and the Na-tional Laboratory was organized.
Municipal sanitary administration was confided to local boards. Their ineffi-ciency demonstrated the necessity of nationalizing health services, and a decreesuggested by Major Jefferson R. Kean was issued creating the National Depart-
Thanks to the efforts of the Marianao, Cuba, Health Unit, many homes arenow equipped with this type of sanitary privy, with its platform and box ofprecast concrete and the seat and cover of varnished wood.
ment of Health, supported by funds appropriated by the Central Government plus10% of municipal revenues. This system proved very effective, and a number ofdifficult public health campaigns were carried out. In 1909 the Department waselevated into the Secretariat of Health and Welfare, today known as the Ministryof Public Health and Social Welfare.
The Ministry is divided into the Department of Health and that of SocialWelfare. These two divisions, with their 126 local offices and 35 hospitals (whichcare for 13,441 patients) and numerous dispensaries, have been able to keep themortality, morbidity, and epidemiological rates down to a low level comparableto that of the most progressive nations.
28 PAN AMERICAN SANITARY BUREAU
Yellow fever disappeared from Cuba in 1908, smallpox in 1923. Bubonicplague, wlhich invaded the island in 1912 and 1914, was rapi(lly eradicated. Theworld pandemic of influenza, which reached Cuba in 1918, did not show its cus-tomary severity. Diphtheria has greatly decreased, and malaria has also beenmuch reduced, and is confined to thinly-populated rural areas. Only infantilegastro-enteritis, intestinal parasitoses, and typhoid fever remain as problemsto be solved, and they, along with tuberculosis, syphilis, leprosy, and other so-called social diseases, are today the chief objects of attack by the Ministry.
The prolonged economic crisis suffered by Cuba since 1920, and the politicaluphcavals of 1930-1933 disrupted public health machinery. But in view of thedangers of deficient public health activity, there was created the CorporativeCouncil of Education, EIealth, and Welfare, to which must be credited ninnybrilliant initiatives and accomplishments. It functioined until October, 1940,when its various divisions were absorbed into the Ministries of Education anlPublic Health and Social Welfarc.
The Corporative Council of Education, Health, and Welfare, was composed ofthe 1,200 civil-rural schools and 40 educational missions, the Institute of Tech-nology, the rural homes for children, thc child guidance centers, a TechnicalRural Health Service, a National Tuberculosis Council, a Foundation for theControl of Leprosy, Syphilis, and Venereal Diseases, and the Finlay Institute,with its School of Public Health and Tropical Medicinc.
The Techlinical Rural Health Service was devoted, as the name implies, chieflyto rural problems. It began by giving adequate training to all its personnel,creating a body of public health experts and specialists. It then undertook anumber of projects including the codification of public health laws and ordinances,for the preparation of a Sanitary Code; a public health survey of the whole Re-public; organization of the Vital Statistics Department; improvement of thecontrol of food and drugs and of drug manufacture; campaigns against prevailingdiseases; supervision of foods, beverages, and aqueducts and other water supplysystems; health education; intensification of international cooperation in publichealth; creation of a Scientific Research Center; and the preparation of programsfor future action.
The National Tuberculosis Council is responsible for the fact that throughoutthe Republic there are tuberculosis dispensaries, sanatoria, and hospitals, andfor an impressive amount of educational worl. Its functions include not onlythe finding, isolation, and care of patients, but also the education of the public,the instigation of laws establishing social security coverage for tuberculosis,readaptation for work, post-sanatorium aid, traveling dispensaries, sanitation ofdwellings, and so forth. The Constructions Section has improved existing hos-pitals and dispensaries and has begun the construction of two magnificent sana-toria: that of Tope de Collantes, in the Trinidad hills, 800 meters above sea level,which has a capacity of 600 beds; and the other, in Habana, for children, capacity500.
The Leprosy Foundation has brought to light the number of existing cases;it has improved the national leprosarium and begun the construction of another,in the eastern part of Cuba, and has also carried on an excellent campaignagainst yaws.
Another excellent measure of the Provisional Revolutionary Government wasthe creation of the National Public Assistance Corporation, which supervises theactivities of private Welfare institutions and also some official ones, gives aid tonumerous institutions, and tends to the maintenance of the vocational schools.
Since 1936 the Rockefeller Foundation, in cooperation with the Cuban Govern-ment, has carried on an energetic campaign against malaria. Its technicianshave succeeded in controlling the disease in certain areas. Thcey hayve completed
PUBLIC HEALTH IN THE AMERICAS 29
model anti-mosquito projects, and organized, in a town of 60,000 inhabitants, amodel sanitary unit whose program serves as a practical school for local officers.
Vital statistics.-General death rate (per 1,000 population): 1902-1911, 14.4;1926-1935, 11.4; birth rate, 30.8 and 23.4 respectively; marriage rate, 6.5 and 4.2;infant mortality (per 1,000 live births), 136.2 and 100.2. The lowest mortalityrate was that for 1902 (9.8), and the highest, that of 1920 (17.2). In 1898, thedeadly policy of concentration caused the mortality rate to rise to 89.2 per 1,000inhabitants.
Disease mortality.-(Rates per 100,000 population): Typhoid and paratyphoid,1902-1911, 15.6; 1926-1935, 14.5; diphtheria, 8.2 and 2.8; whooping cough, 6.5 and3.2; scarlet fever, 2.4 and 0.05; smallpox, 0.04 and 0; measles, 4.3 and 1.6; malaria,47.8 and 20.9; yellow fever, 0.6 and 0; leprosy, 1.6 and 0.8; syphilis, 3.3 and 4.4;cancer, 39.8 and 42; respiratory tuberculosis, 169.6 and 77; other forms of tubercu-losis, 17.5 and 4.9; enteritis in children under 2, 197.5 and 153; iii persons over 2,62.1 and 61.6.
Funds.-The public health appropriations have varied from 1.50 pesos percapita in 1910 to 2.15 in 1918-19, and 0.55 in 1933-34; the present figure is 1.10.The various agencies of the Corporative Council of Education, Health and Wel-fare which were absorbed by the Ministry of Public Health and Social Welfare,had their own budget of $2,186,788, which increases the per capita expenditurefor health for the present year to 1.75 pesos.
PUBLIC HEALTH IN THE DOMINICAN REPUBLIC
By Dr. WENCESLAO MEDRANO H.*
Minister of Heallh and Welfare
History.-The public health service of the Dominican Republic might well becalled the oldest in America, since Hispaniola was the first European settlementin the new world. The island's first great medical problem was probably thesevere epidemic of smallpox in 1519. However, before that time the first Americanhospital, San Nicolás, had already been founded, in Santo Domingo.
Constant attempts were made to improve the health of the colony. It had itsphysicians, and even a school of medicine in the University founded in 1538. Inadldition to hospitals, there were municipal physicians, among them such medicalwriters as Méndez Nieto, and Fernando Diez Leiva, author of "Antiaxiomasmédicos morales y filosóficos" (Moral and Philosophical Medical Axioms), 1682.Diez Leiva was, according to the title page of his work, "physician of the city ofSanto Domingo."
However, there was no specialized public hcalth service either during thecolonial period or during that of Haitian domination (1822 to 1844). Nor wassuch an organization createdt upon the establishment of the Republic in 1844,although the Government was always concerned with public health. After 1845public health became a municipal responsibility. Tlihe law of municipal govern-ment of that year provided in articles 13 and 27 for sanitary police and cleanliness,the supervision of markets and food warehouses, the preparation and preservationof vaccine, precautionary measures against epidemics, improvement of streetsand public plazas, and anything else which could contribute to public health andcleanliness, and finally, for the establishment of welfare institutions.
The police department had public health duties. The Police Ordinances of1845 contained two chapters affecting health, I, Public Cleanliness and IV, Public
* Dr. Wenceslao Medrano H. has been succeeded by Dr. Darío Contreras.
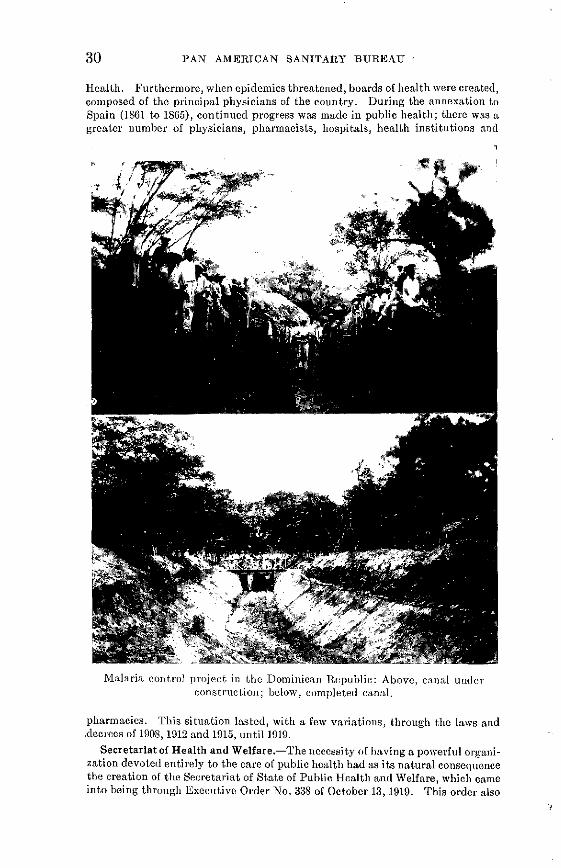
30 PAN AMERICAN SANITARY BUREAU
Health. Furthermore, when epidemics threatened, boards of health were created,composed of the principal physicians of the country. During the annexation toSpain (1861 to 1865), continued progress was made in public health; there was agreater number of physicians, pliarmacists, hospitals, health institutions and
q
Malaria control project in thle Dominican Republic: Above, canal underconstruction; below, completed canal.
pharmacies. This situation lasted, with a few variations, through the laws and.decrees of 1908, 1912 and 1915, until 1919.
Secretariat of Health and Welfare.-The necessity of having a powerful organi-zation devoted entirely to the care of public health had as its natural consequencethe creation of the Secretariat of State of Public Health and Welfare, which cameinto being through Executive Order No. 338 of October 13, 1919. This order also

PUBLIC HEALTH IN THE AMERICAS 31
contained the regulations for the organization of the new department. At thepresent time the public health service functions under regulations adopted inJanuary 1938. During the last few years the public health service has reached itsmaximum efficiency and has complied rigorously with the provisions of the excel-lent Code of Sanitary Procedure of 1938 (approved in December, 1937).
Public Health Campaigns.-The public health service has carried on its ruralsanitation work through the provincial health authorities and through the 16 ruraldispensaries of the Republic. Treatment is furnished for the endemic diseases ofthe area: malaria, hook-worm. syphilis, yaws and tropical ulcer.
Tuberculosis.-On Pan American Health Day, 1940, the National LeagueAgainst Tuberculosis was installed. This organization is in charge of the cam-paign against tuberculosis, and under the auspices of the Secretariat of Health andWclfare it has secured a considerable number of members and has been able tocollect a large amount of money. This has been used to purchase equipment forthe first tuberculosis hospital (100 beds), now almost completed.
Child and Maternal Welfare.-On January 5, 1941, the National Board ofMaternal and Child Welfare, created by Law No. 367 of November 15, 1940, wasinaugurated. Among its activities have been the installation of two milk stations,enlargement of the maternity ward of the Padre Billini Hospital to a capacity of60 beds, construction of the Maternity Hospital of San Francisco de Macoris(30 beds), and enlargement of the Julia Molina Maternity Hospital (30 beds).
Children's Hospital.-The Ramfis Children's HEospital (150 beds) was in-augurated January 6, 1938 and is meeting a long-felt need, as the first children'shospital in the Republic.
PUBLIC HEALTH IN ECUADOR
By Dr. LEOPOLDO IZQUIETA PÉREZ
Director General of HIealth
Although we are far from pretending that Ecuador has attained to a completedegree of public health advancement, we can say that it has progressed to thcepoint from which the future may be regarded without anxiety. In former timesthere was full justification for the apprehension felt by foreigners and also by theinhabitants of the interior of the country, on arriving in Guayaquil, since thou-sands of persons in both categories perished there of yellow fever. And, as ifycllow fever were not enough, there came another pestilence of terrifying propor-tions: bubonic plague, which appeared in 1908 and found a favorable atmosplicrefor its propagation in Guayaquil and in the rest of Ecuador.
In those days there was in Guayaquil a so-called Board of Health, composed ofbeterogenous elements, many of whom were amateurs in medicine and in theirknowledge of hygiene. This Board met from time to time to issue regulations ofmore or less effectiveness. In 1908, on the heels of the bubonic plague invasion,the National Government appointed as the first Director General of Healththe North-American physician, Dr. Bolivar J. Lloyd. Dr. Lloyd immediatelyproceeded to organize the sanitary defense of the country. He was succeededin his task by Dr. Luis Felipe Cornejo Gómez, whlio carried tbe work forward,as did his successor, Dr. León Becerra. Tlhe latter administration saw the visitof the famous North American commission composed of Drs. W. C. Gorgas,Juan Guiteras, and R. Carter, in 1916, and of a later Colmmission including Drs.Rendall, Lebredo, Eliot, Rcdembourg, and Noguchi. Dr. Becerra was followedby Dr. Wenceslao Pareja, and he by Dr. Luis Mariano Cueva, who died in 1931.
32 PAN AMERICAN SANITARY BUREAU
Dr. Sayago occupied the post for a short time, when he was succeeded by Dr.Leopoldo Izquieta Pérez, the present Director.
The public health movement in Ecuador, then, really began in the twentiethcentury (in 1908). The establishment of the contagious disease hospital; theactive anti-rat campaigns; the urban and maritime disinfections and the mem-orable fight against yellow fever with the aid of the Rockefeller Foundation, wereaccomplishments of the dawn of this period. The development of our publichealth work has been a rapid one: it has seen the founding of new institutions;the struggle against our extremely high disease rate; and the execution of thenecessary hygienic measures to these ends. There is still much to be done, andone of the most important problems is that of providing safe drinking water insufficient quantities for Quito and Guayaquil. Another urgent need of Guayaquil,chief port of the Republic, is the leveling of its terrain, since the present irregu-larities permit the collection of stagnant water and the consequent breeding ofmosquitoes.
Guayquil General Hospital
It is imperative that Guayaquil carry out in the near future a number of sani-tation projects, including the completion of street paving; construction of wharvesalong the river bank; drainage and drying of the swamps surrounding the city;the canalization of the Estero Salado; the destruction of neighboring manglaresor mangrove swamps; and, finally, the promulgation of new laws and ordinancesregulating new building construction in the city. To these measures must beadded an active campaign against malaria, the establishment of tuberculosissanatoria, and of dispensaries for the treatment of hookworm. An importantinfluence in this work will be the newly created National Institute of Hygiene,in Guayaquil (See the Bolelin for Sept., 1941, p. 892), which will serve the wholeRepublic.
It is high time that we undertake to solve our problems, because isolation doesnot fit in with other civilized communities. Peoples should maintain a mutualunderstanding and aid each other. We hope tlihat the efforts of all the countrieswho are doing their best to progress diiring this crucial period of history, will becrowned with success. The Continent of Peace ought indeed to outstrip in itshygienic advancement and safeguards, the other continents which are engaged inself-extermination. Great benefits await us under the firm leadership of our
,,,

PUBLIC HEALTH IN THE AMERICAS 33
Governments and the discipline of our people, who will not fail us in the work ofcommunity and solidarity.
Funds.-Public health budgets have been progressively increased. Theconservation and defense of human capital has been at all times and in all coun-tries the chief concern of Governments. Despite great difficulties, the Ecuadorianhealth budget has finally reached 2,300,000 sucres. While this figure does notreach the amount proposed by the Third Pan American Conference of NationalDirectors of Health, it at least represents an earnest effort toward improving thesanitary condition of the country. The amounts appropriated for public health
Guayaquil Clinic
in Ecuador have risen from 220,000 sucres in 1922 to 263,006 in 1925, 591,080 in 1930,773,000 in 1935, 2,031,440 in 1940, and 2,300,000 in 1941.
General and Infant Mortality.-The general deaths have varied from 51,584in 1928 to 44,385 in 1930, 46,193 in 1935, and 62,183 in 1940; and the infant deathsfrom 14,984 to 13,881, 14,361, and 18,839, respectively. In 1940 the principal causesof death were: whooping cough, 7,134; malaria, 4,847; tuberculosis, 2,263; dysen-tery, 1,199; measles, 814; typhoid, 405; tetanus, 207; syphilis, 80; hookworm, 65;smallpox, 42; plague, 14; and leprosy, 13.
PUBLIC HEALTH IN EL SALVADOR
By Drs. VICTOR ARNOLDO SUTTER and M. ZIÑ\IGA IDIÁAQUEZ
Director, and Secretary, respectively, Nationa2 Department of Health
The Public Health Service of El Salvador came into existence at the turn of thecentury, with the promulgation of the first Sanitary Code, on May 30, 1900, duringthe Presidency of General Tomás Regalado. The distinguished physician, par-liamentary orator, and author, Dr. Rubén Rivera, was at that time Minister ofGoveranment. In accordance with the Codc, the first Superior Council of Healthwas appointed on July 23 of that year. Its members included the eminent physi-cians Drs. Tomás G. Palomo, surgeon; Carlos Bonilla, clinician, teacher of futuregenerations, writer, and poet; and Francisco Guevara, physician, pharmacist, andoutstanding surgeon.
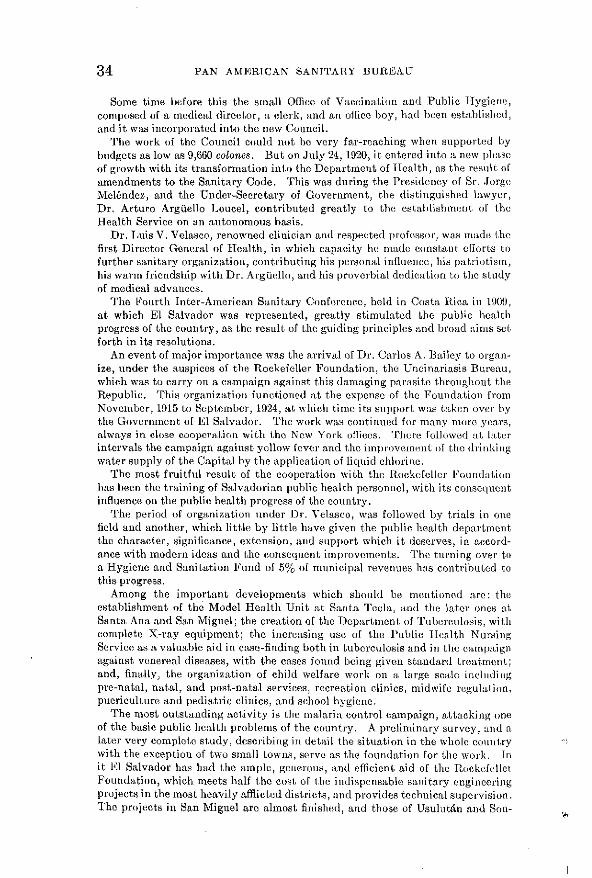
34 PAN AMERICAN SANITARY BUREAU
Some time before this the small Office of Vaccination and Public Hlygienc,composed of a medical director, a clerk, and an office boy, liad been establislicdl,and it was incorporated into thc new Council.
The work of the Council could not be very far-reaching when supported bybudgets as low as 9,660 colones. But on July 24, 1920, it entered into a new plhaseof growth with its transformation into thc Department of Health, as the result ofamendments to the Sanitary Code. This was during the Presidency of Sr. JorgeMeléndez, and the Under-Secretary of Government, the distinguished lawyer,Dr. Arturo Arguello Loucel, contributed greatly to the establishment of theHealth Service on an autonomous basis.
Dr. Luis V. Velasco, renowned clinician and respected professor, was made thcfirst Director General of Health, in which capacity he made constant efforts tofurther sanitary organization, contributing his personal influence, his patriotism,his warm friendship with Dr. Argiello, and his proverbial dedication to the studyof medical advances.
The Fourth Inter-American Sanitary Conference, held in Costa Rica in 1909,at which El Salvador was represented, greatly stimulated thce public healthprogress of the country, as the result of the guiding principles and broad aims setforth in its resolutions.
An event of major importance was the arrival of Dr. Carlos A. Bailey to organ-ize, under the auspices of the Rockefeller Foundation, the Uncinariasis Bureau,which was to carry on a campaign against this damaging parasite throughout theRepublic. This organization functioned at the expense of the Foundation fromNovember, 1915 to September, 1924, at which time its support was taken over bythe Government of El Salvador. The work was continued for many more years,always in close cooperation with the New York offices. Thcre followed at laterintervals the campaign against yellow fever and the improvement of the drinkingwater supply of the Capital by the application of liquid chlorine.
The most fruitful result of the cooperation with the Rockefeller Foundationhas been the training of Salvadorian public health personnel, with its conscqucntinfluence on the public health progress of the country.
The period of organization under Dr. Velasco, was followed by trials in onefield and another, which little by little have given the public health departmentthe character, significance, extension, and support which it deserves, in accord-ance with modern ideas and the consequent improvements. The turning over toa Hygiene and Sanitation Fund of 5% of municipal revenues has contributed tothis progress.
Among the important developments which should be mentioned arc: theestablishment of the Model Health Unit at Santa Tecla, and the later ones atSanta Ana and San Miguel; the creation of the Department of Tuberculosis, withcomplete X-ray equipment; the incrcasing use of the Public IIcalth NursingService as a valuable aid in case-finding both in tuberculosis and in the campaignagainst venereal diseases, with the cases found being given standard treatment;and, finally, the organization of child welfare work on a large scale includingpre-natal, natal, and post-natal services, recreation clinics, midwife regulasion,puericulture and pediatric clinics, and school hygiene.
The most outstanding activity is the malaria control campaign, attacking oneof the basic public health problems of the country. A preliminary survey, and alater very complete study, describing in detail the situation in the whole countrywith the exception of two small towns, serve as the foundation for the work. Init El Salvador has had the ample, generous, and efficient aid of th RocklefellclFoundation, which meets half the cost of the indispensable sanitary enginceringprojects in the most heavily afflicted distriets, and provides technical supervision.The projects in San Miguel are almost finished, and those of Usulután and Son-
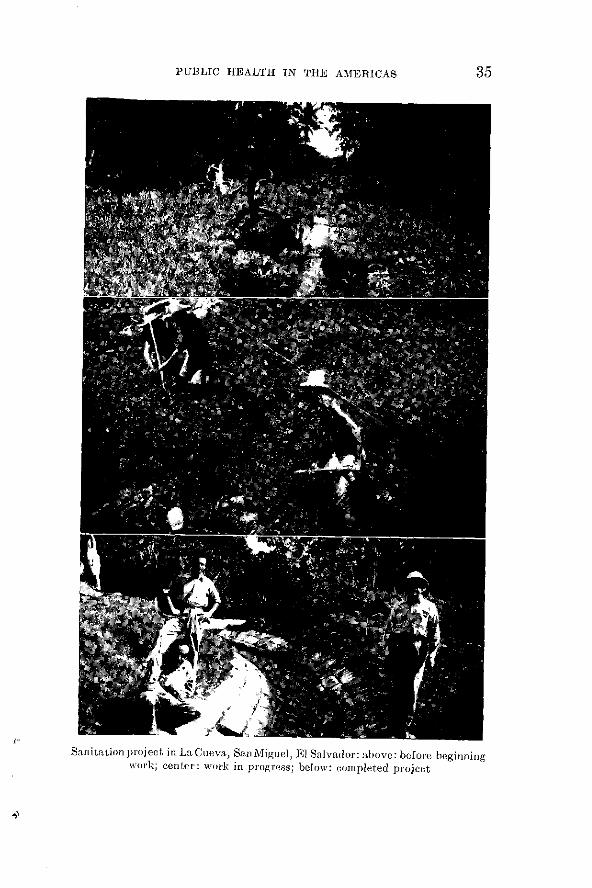
PUBLIC HEALTH IN THE AMlERICAS 35
Sanitation project i¡n La Cueva, San Miguel, El Salvador: above: before beginningwork; center: wvork in progress; below: completed project

36 PAN AMERICAN SANITARY BUREAU
sonate are to bcegin immediately. The decrease in the death rate from 1924 to1940, and especially in the last three years, speaks well for the work of the PublicHealth Service.
Urgent needs.-The most urgent task for the future is to develop amply andcompletely the interesting work which has already been undertaken.
Funds.-The general budgets for health expenditures in El Salvador havevaried from 27,560 colones in the fiscal year 1901-1902, to 22,400 in 1905-1906,30,260 in 1910-1911, 60,620 in 1915-1916, 152,050 in 1920-1921, 197-120 in 1925-1926,369,120 in 1930-1931, 210,000 in 1935-1936, and 388,126 in 1940-1941. The averagesby periods have been 23,784 colones in 1901-1911, 60,398.80 in 1911-1920, 180,026.66in 1920-1926, and 293,948.06 in 1926-1941.
Population.-The population of the Republic has increased from 1,287,395inhabitants in 1924, to 1,459,594 in 1930, 1,597,564 in 1935, 1,744,535 in 1939, and1,787,930 in 1940.
General mortality.-The total number of deaths has varied from 33,047 (25.7)in 1924, to 31,490 (21.6) in 1930, 38,884 (23.7) in 1935, 31,656 (18.1) in 1939, and31,242 (17.5) in 1940.
Infant mortality.*-1930, 10,329; 1935, 8,617; 1939, 8,289; 1940, 9,019.Causes of death.-Malaria: 1924, 3,189 (248); 1930, 3,115 (213); 1935, 4,470
(280); 1939, 3,418 (196); 1940, 3,325 (186); diarrhea-enteritis, under 2 years: 1,821(141), 2,467 (169), 3,587 (225), 2,349 (135), and 2,791 (156) respectively; tuberculo-sis: 478 (37), 529 (36), 765 (48), 743 (43), and 698 (38.5); pneumonia: 766, 661,1,414, 1,918, and 1,674; measles; 119, 350, 1,315, 1,863, and 1,276.
THE EVOLUTION OF PUBLIC HEALTH IN GUATEMALA
By Dr. LUIS GAITÁN
Sub-Director of Public Health
History.-The history of medicine in Central America was in the beginningthe history of the plagues, obstacles, and catastrophes which confronted Govern-ments in their efforts to safeguard their people. The construction of hospitalsand asylums to meet immediate needs, was the first public health developmentdescribed in the ordinances and chronicles of the past century. At that time,public health and bygiene were not branches of an exact science, based on social,epidemiological and mathematical principles, but consisted of ordinances, sug-gestions, or regulations issued by the authorities of the Central-American Federa-tion, through its municipalities.
The oldest Central American public health ordinance is that published underTitle II, Law V, No. 314, October 2, 1839, of the First Book of Laws of the NationalSovereignty, which read as follows:
"Article 28.-In the case of pestilence, all proper measures to relieve the necessities of the people shalbe taken.
"Art. 42.-The Sanitary Police are ermpowered to deal with matters of correction and secsurity; theyshall bestrictly obligated to prevent and remove anything which may prejudice public health; they shallsee to the cleaning of the streets, plazas, and markets, watch over the quality of foods of all kinds, andshall effectively bring about the dryixng up or drainage of stagnant or unhealthy pools of water.
"Art. 45.-In cases of pestilence, the Municipalities shall irmmnediately report to the Corregidor of theDepartment, but this shall not relieve them of the duty of immediately organizing Boards of Health andof providing assistance to the inhabitants.'
*Stillbirths have been excluded from deaths from O to 1 year.

PUBLIC HEALTH IN THE AMERICAS
Population.-Another early undertaking was the appointment of a Committeefor the taking of the First Census of the Republic. In 1825 the State of Gua-temala, in the Central American Federation, had 318,215 inhabitants; in 1893 thecountry had 1,364,678; in 1903, 1,842,134; in 1921,2,004,900, and in 1940, 3,284,189.
Thc population of Guatemala has increased, therefore, one million in the last20 years, a fact which demonstrates more than any other, the progress realized
UIm r_,
i : ?A 1
Workers' housing in Guatemala
thanks to its present wise laws and regulations and to its cultural and scientificrelations with the United States and Europe. The advance of the public healthsciences, the eradication of yellow fever, the quarantine of ports and internationalconventions, as well as the sanitation of Cuba and Panama, have permitted theutilization of natural resources and the growth of population.
Mortality.-Another factor which must be taken into account is the generalleath rate. In 1865 the average annual mortality was 30 deaths per 1,000 in-
37

38 PAN AMERICAN SANITARY BUREAU
habitants. Today, thanks to the degree of public health organization and itsconstant vigilance this average has dropped to 19 per 1,000. The typhoid fevermortality has decreased from 23.3 per 100,000 in 1930 to 6.7 in 1940, and the small-pox rate from 1.1 in 1931 to 0.22 in 1940.
Funds.-Appropriations for sanitation and public health have increased froman annual average of 4,267 quetzales during 1900-1909, and 3,621 in 1910-1919, to33,975 in 1920-1929, 194,910 in 1930-1940, and 115,967.05 in 1940.
Health index.-The general basis for estimating the public health index is thedisappearance of the pestilential diseases which were so devastating in the lastcentury: hospital septicemias, smallpox in the villages and rural areas, typhusfever, and finally, malaria in the lowlands. Fortunately, many of these plagueshave vanished forever, and smallpox, which was formerly a terrible enemy whichno one escaped, today is responsible for but an insignificant mortality, and casesbecome more and more uncommon. This victory is the result of patient effortbeginning May 12, 1824, when the Public Health department of Guatemala madevaccination compulsory. (Vaccination was practiced in the hospitals of theKingdom of Guatemala in 1804, by the protomédico or royally appointed physicianDr. Narciso Esparragosa y Gallardo.) In 1840 more adequate regulations wereestablished: these were confirmed in 1871 by the liberal laws, and reaffirmed bythe present sanitary regulations.
National Vaccine Institute.-During the period from 1909 to 1940, the NationalInstitute of Vaccine prepared a total of 18,021,307 doses of smallpox vaccine, whichwere widely distributed throughout the Republic. On more than one occasion,supplies have been sent to neighboring Republics.
Vital index.-The vital index (excess of births over deaths) of Guatemala hasfluctuated, on the average, between 15 and 22, since 1871.
This brief sketch affords an idea of the biologic potentialities of Guatemalaand is a testimony of the abilities of her native races to develop and grow towardgreater progress and culture, when their health is protected and their vital needsare assured by preventive medicine and social hygiene.
THE NATIONAL HEALLTH AND SOCIAL WELFARESERVICE OF HAITI
By DR. LOUIS -IIPIOLYTE*
Director General, National Service of Ilygiene and Social Welfare
The National Service of Hygiene and Social Welfare of HIaiti was re-organizedin 1919 and has since come to be one of the most important administrative branchesof the Government.
The Service has developed gradually and has become an organization whichfunctions on a rational basis and which renders inestimable services to the urbanand rural population.
The Service extends its activities throughout the Republic by means of 11hospitals and 125 rural clinics, all of them housed in buildings constructed withinthe last twenty years.
One of the most important parts of the program is public assistance, giventhrough the hospitals and rural clinics and constituting a campaign against thethree principal diseases afflicting the population: malaria, treponematosis andtuberculosis. These three conditions are responsible for the greatest number ofdeaths in Haitian hospitals. The sanitation service funetions in accordance with
* Dr. Lonis Hippolyte has been succeeded by Dr. Jules Thébaud.
PUBLIC HEALTH IN THE AMERICAS
legislation based on the principles of hygiene and undertakes extensive projectsin different parts of the country. The maritime and domestic quarantine service
.1.- - - 111 U I i3 1 l
Above: Partial view of the court of the General Hospital, Port-Au Prince, HaitiCenter: Child assistance center, social assistance service, Cap-Haitien
Below: Rural health clinic, Léogane, Haiti.
is organized according to the precepts of the Pan American Sanitary Code, ratifiedby Haiti on June 21st 1928. Another function of the Service is the teaching of
-`-------
39
;717,- t.i "; , i,~
40 PAN AMERICAN SANITARY BUREAU
medicine, which was reorganized with the assistancc of the RockefellerFoundation.
Since .1919 the I-aitian Government has opened a school of nursing whichfurnishes to the hospitals, whose importance increases daily, a corps of intelligentand devoted nurses. It has also created the maternal andl child welfare services,the service of health education, which is carried on by the radio, schools, andpress, and finally, the social assistance services which include a number of estab-lishments for the shelter of the poor, the aged, and children.
The Haitian Public Health Service has always been characterized by its will-ingness to encourage the efforts of private initiative in behalf of suffering hu-manity. Thus it has recently facilitated the establishment of an institute ofradio-therapy, a really important development in the annals of Haitian medicine.It is almost unnecessary to point out the service which this truly humanitariancenter is giving to the people of Haiti, especially to the poorer ones whose meansdo not permit their seeking treatment abroad.
A recent development which should assist greatly in the control of malaria isthe creation of a division entirely devoted to this work. This was made possiblethrough the aid of the Rockefeller Foundation, an assistance for which I takethis occasion to express our appreciation. The Foundation has been cooperatingwith the Service in malaria control for about one year.
During the period since its reorganization the Haitian Public Health Servicehas funetioned to the height of its resources and done all that was in its power toimprove the living conditions of Haitian citizens and to safeguard their moraland material well-being, in spite of a lack of sufficient funds.
There is much which still remains to be done and the Service has outlined anumber of objectives to be attained as soon as possible, including: (a) revisionof the narcotics control legislation, (b) isolation of lepers, (c) finding of tuber-culosis cases and construction of sanatoria, (d) establishment of a social assistancefund, (e) further development of the Child Welfare Service, (f) improvements inrural hygiene, and (g) intensification of malaria control through sanitary en-gineering.
Budget.-1919-1920, 1,341,000 gourdes; 1924-1925, 1,845,882; 1929-1930, 3,903,-220.92; 1934-1935, 2,702,740.46; 1939-1940, 2,616,769.30; 1940-1941, 2,616,769.30.
HAITIAN EPIDEMICS
By Dr. RULX LÉON
Ex-Secretary of State in charge of the Public Health and Social Assistance Service
Several severe smallpox epidemics occurred in Haiti during early times, in-cluding those in 1518, 1738, 1740 and 1741. Treatment in 1518 consistedchiefly in having patients bathe in the river. But in 1825, when another out-break appeared, soldiers were ordered to be vaccinated. In 1881-1882 and 1920Haiti was again severely stricken but it was only in 1920 that the people beganto take seriously vaccination and isolation as a means of combating the disease.
The first cases of yellow fever, imported from Martinique, were reported inHaiti in 1691. Epidemies occurred in 1733, 1735, 1739, 1743, 1745 and 1746. Verysevere were those in 1798, 1802, 1803 and 1804, according to such writers as Pois-sonier Desperrieres, Ch. F. Roux, Victor Bally, Delmas, Descourtilz, LouisJoumaron and François Moulié. No further epidemies of yellow fever occurredin Haiti, although a few sporadic cases were reported from time to time, confinedto the white colony. Dr. Georges Smith, first President of the Board of Health,
PUBLIC HEALTH IN THE AMERICAS 41
wrote in 1861 that during the 20 years of his practice in Haiti, he never had a fatalcase of yellow fever in a negro or in anyone with African blood and that althoughsuch individuals contracted the disease, they usually recovered very quickly.
Epidemics of malaria and of typhoid, sometimes difficult to distinguish withoutlaboratory aid, have also been reported in Haiti, in 1739, 1742, 1744 and 1766.The independence of Haiti brought about no noticeable change in this regard.In 1817 and 1818 there was much malaria, and it was especially severe at Port-au-Prince. Alexandre Pétion, founder of the Haitian Republic and friend of Si¡¡ onBolívar, died during this epidemic.
Among the endemic diseases which often proved fatal may be mentionedmumps, very common in 1740, (Pouppée Désportes), and measles, prevalent in1741 (Damien Chevallier) and 1889. There were many cases of rabies in bothdogs and humans in 1762, 1768 and 1852. An influenza epidemic, with pulmonarycomplications, occurred in 1852. Three years ago Port-au-Prince had its secondepidemic of diphtheria since 1892, and in 1935 anthrax made its first serious ap-pearance since 1775.
PUBLIC HEALTH IN HONDURAS
By Dr. PEDRO H. ORDÓOEZ DIAZ
Director General of Health
History.-Public health development in Honduras began in 1910 with thepromulgation of the Sanitary Code. The Public Health Council established bythis Code commenced to function in 1914.
Prior to 1910, public health was regulated by a series of provisions in the PoliceLaw and in the Law of Municipalities, and by executives who gave facilities to themunicipalities and to police authorities to order the cleaning of streets and ofpublic and private premises, to employ the Jenner vaccine in periods when small-pox was epidemic, and for the establishment of isolation hospitals administeredby welfare boards. All these measures were made public by proclamation.
In 1911 the Venereal Disease Prevention Offices were created, and in 1912 theJenner Vaccine Institute and the Veterinary Section. In 1917 a number ofamendments were made in the Sanitary Code. The Department of Health wascreated as a dependency of the Superior Council of Health, and the Republic wasdivided into five sanitary zones. The Council functioned until June 1920, whenthe Department of Health was given ample facilities for carrying out an effectivepublic health program.
Present organization.-At the present time public health administration comesunder the Ministry of Government, Justice, Health and Welfare, with its Depart-ment of Health, Secretariat of Health, and Divisions of General Prophylaxis,Tropical Diseases, Laboratories and Biologic Institute, Sanitary Engineering,Sanitary Police, and Sanitary Delegations.
Legislation.-The Constitution of Honduras contains the following provisionsregarding public health:
Every person's home is inviolate territory, which may not be invaded exceptby the authorities in cases of fire, earthquake, flood, epidemic, or other similarcatastrophe, and for the purposes of health inspections or visits; women are notpermitted to engage in unhealthful or dangerous work or in industrial night workafter six o'clock, in commercial establishments; children of less than 12 years ofage may not hire out for work, and those between 12 and 16 may not work longerthan 6 hours per day; large industrial enterprises are required to establish hos-pitals at their factories for the care of industrial accidents and sickness among

42 PAN AMERICAN SANITARY BUREAU
their employes; it is the duty of the State to guard the public health and hygienicwell-being of the nation; and finally, the family, as the foundation of society, isunder the protection of the State.
Necessities.-The most urgent public health necessities of Honduras are anenergetic campaign against malaria, intestinal parasitoses, pulmonary tuberculo-sis, and venereal diseases. The Department of Health has taken some steps tocombat these diseases, which decimate the population, but since they are problemsof such enormous extension, their solution has never been accomplished.
Funds.-The public health budget for the fiscal year 1921-1922, the oldest forwhich figures were available, amounted to 79,260 lempiras for activities andsalaries of public health personnel. The 1941-42 budget amounts to 164,760lempiras.
Vital statistics (fiscal year 1939-40).-General death rate, 16.38 per 1,000population; infant mortality, 103.38 per 1,000 births; deaths from typhoid and
D'Antoni Hospital, La Ceiba, Hondouras
paratyphoid, 77 (6.9 per 100,000); malaria and other fevers, 5,972 (538); pulmonarytuberculosis, 317 (28.6); intestinal parasitoses, 853 (77); diarrheas, 699 (63.1);dysenteries, 517 (46.7); pneumonia, 600 (54.2). According to the June 30, 1940census, the population of Honduras was 1,107,859.
Institute of Biology.-The Biologic Institute has begun to secure good resultswith the preparation of the typhoid and paratyphoid vaccine being used pre-ventively in various parts of the Republic. It also manufactures smallpox andanti-rabies vaccine, and cooperates with the Health Laboratory in confirming thediagnosis of contagious diseases through bacteriological examinations and sero-logic tests, and aids in the control of the quality of certain foods which may serveas means of transmission of disease.
Future of public health.-For the future improvement in public health we mayhave the assistance of an improvement in the economic situation. Honduras isalways ready to cooperate with the Pan American Sanitary Bureau in the solutionof the public health problems of the Continent.

PUBLIC HEALTH IN THE AMERICAS 43
SOME IMPORTANT DATA ON PUBLIC HEALTH INMEXICO
By Drs. VICTOR FERNÁNDEZ MANERO and ALBERTO P. LEON
Chief and ex-Secretary, respectively, of the Department of Public Heallh
Most notable developments.-The first Public Health Council of Mexico wascreated in 1841, and was purely advisory in nature. On July 14, 1891, the firstSanitary Code was promulgated, granting executive authority to the SuperiorCouncil of Health. An amended Code was issued September 10, 1894, definingthe jurisdictions of Federal and Local public health authority, and placing theformer in the hands of the Superior Council of Health. WVhen the new Consti-tution was adopted in 1917, the Department of Public Health was created onFebruary 5, as an autonomous body, directly under the President of the Republic.The general Regulations for the Department were issued December 19, 1924, ap-pearing in the Diario Oficial for January 21, 1925. Amendments to the SanitaryCode, March 6, 1926, increased the powers of the Department in public healthmatters; the new Code was published in the Diario Oficial of July 8 and 9 of thatyear. In 1926, the Regulations for the Council of Public Health were also adopted.January, 1927, saw the creation of the first (32) Federal Health Delegations in theStates. In January, 1929, the Office of Rural Hygiene and Sanitary Services ofthe Interior was established, and also the Service of Visiting Sanitary (or PublicHealth) Nurses. In 1931, the first Coordination of Federal and Local SanitaryServices was organized to strengthen public health activity by the cooperation ofFederal and Local governments, particularly the services in rural zones. In1935, the Ejidal Public Health Services (Scrvices in the Ejidos, or communalvillages patterned after the old Indian system), and the Coordinated Serviceswere expanded to include 22 States. The Cooperative Office of Health Services inthe Federal District was created the same year, in order to separate the localpractical work from the administrative services for the Republic as a whole. ANational Housing Commission was appointed in 1938. In 1934, there were 182Health Offices in the States, and these had been increased by 1940 to 698, of which108 were social medicine and rural hygiene units. The number of public healthnurses employed in these Health Offices rose from 383 in 1934 to 1,390 in 1940.
Health education.-When the National School of Medicine was organized in1833, a course in hygiene was included with that of physiology, the first time inwhich hygiene was taught in Mexico. In 1867 a separate chair of hygiene wascreated and made compulsory for medical students; the first instructor was Dr.Ladislao de la Pascua. In 1922 the School of Public Health was founded, but itseducational activities began in May, 1925. In this year, the Office of Propagandaand Health Education was created.
Communicable Diseases.-In 1902 a Commission on Epidemiology was addedto the Superior Council of Health, and its duty was the prevention of communi-cable disease. In that same year Dr. Eduardo Licéaga, first President of theCouncil, proposed an energetic campaign against the Aedes aegypti mosquito.The project, Regulations, and plans were approved in 1903, and the work wasbegun in September in the Port of Veracruz, being extended to other ports andcities a few months later. By December 1904, three months had passed since acase of yellowfever had been reported in Veracruz, and on October 25, 1906, theSuperior Council of Health reported that not a single case had appeared in thewhole country. Also in 1902, at the suggestion of the Superior Council of Health,the President of the Republic asked the States to make smallpox vaccination com-pulsory. On March 27, 1925, the Regulations on Vaccination and Re-vaccination
PAN AMERICAN SANITARY BUREAU
HEALTH AUTHORITIES OF THE AMERICAN REPUBLICS
DR. P. HI. ORDÓÑEZ DÍAZ(Honduras)
DR. GERARDO BIJONGERMINI
(Paraguay)
DR. VÍCTOR FERNÁNDEZ MANERO
(México)
DR. LUIS M. DEBAYLE
(Nicaragua)DR. CONSTANTINO CARVALLO
(Perú)
44
ii
Y .
PUBLIC HEALTH IN THE AMERICAS 45
were issued, making vaccination compulsory for all inhabitants of the country.On October 20, 1902, an epidemic of bubonic plague appeared for the first time inMexico (port of Mazatlán). Its control is one of the most interesting and eloquentexamples of victory over this disease. By March 15, 1903, the epidemic had beencompletely controlled; there were no more cases. In April, 1911, two years afterNicolle had demonstrated the role of Pediculus vestinmenti as a vector of exanthe-matic lyphus, a de-lousing campaign was begun in Mexico. In 1920 an epidemic
Above: Partial view of tuberculosis sanatorium in Huipulco, D.F., MexicoBelow: Main canal of malaria control product at Agua Azul
and San Carlos, Guadalajara, Jalisco, Mexico
outbreak of bubonic plague occurred in the port of Veracruz; it was brought undercontrol by the middle of the same year. In April, 1924, a campaign against hook-worm was undertaken in collaboration with the Rockefeller Foundation. A Com-
mission for the study of pinto was appointed in 1929, as was another for the study
and control of onchocerciasis. In 1938 a beginning was made in the combating ofmeasles through the use of convalescent serum or by the attenuation or modifica-
tion of the virus by placental extract; active immunization against diphtheria
46 PAN AMERICAN SANITARY BUREAU
with alum-precipitated toxoid was initiated, and the epidemiological investigationof brucellosis was begun. In 1940 a hospital was completed in Huixtla, Chiapas,for onchocerciasis patients in the endemic area; and another was opened in Ar-celia, Guerrero, for pinto cases, this likewise being in the endemic zone. In thesame ycar a Medical-Public Health Service for the prevention of trachoma wascreated in Nacimiento, Muzquiz (Coahuila), and the study of the prevalence inMexico City of the different types of pneumococci was undertaken.
Tuberculosis.-In 1900 Dr. Licéaga founded the first National TuberculosisAssociation. In 1918 the first tuberculosis dispensary was opened in Mexico City,and in 1929 the construction of the Huipulco Tuberculosis Sanatorium and fivedispensaries in Mexico City was begun. Dispensaries were also opened in theStates of Tamaulipas, Veracruz, Guanajuato, Sinaloa, and Coahuila. The Na-tional Tuberculosis Control Committee, created by Presidential decree November10, 1939, began its work in January 1940. The first preventorium was foundedthat same year in Mexico City. The National Committee instituted a financialcampaign in 1941, collecting 4,000,000 pesos through public cooperation, and be-ginning the construction of three hospitals with a total capacity of 1,100 beds, apreventorium in Mexico City for 300 children, and a 300-bed children's tubercu-
Ejidal Clinic, San Pedro, Coahuila, Room in the Ejidal Clinic atMexico Matamoros, Coah., Mexico
losis hospital. The First Regional Conference on Tuberculosis was celebratedthe same year in Guanajuato.
Venereal Disease.-The first Regulation on Prostitution and the Registrationand Health Inspection of prostitutes was prornulgated in 1918, and the first dis-pensary was opened. The first 12 venereal disease dispensaries in the States werefounded in 1924, and a consultative service for venereal disease cases was createdin each health unit. In 1933 the Venereal Disease Control Campaign Service wasestablished in the Department of Public Health, combining under one administra-tion the various institutions in this field. Legal prostitution was abolished in1940, and the operation of houses of prostitution and the transmission of venerealdisease were included as crimes under the Penal Code. A Service of SocialWorkers was created in that year to assist in the campaign.
Malaria.-Permanent malaria control engineering projects were begun in 1934.In 1935 a Presidential decree declared the malaria control campaign to be of publicutility, and the importation of quinine and its derivatives was rnade duty-free.Studies for the cultivation of cinchona were begun. In 1940, 761,935 pesos hadbeen spent for malaria control.
Leprosy.-The Leprosy Prevention Servicc was created in 1929, and the Na-tional Leprosy Prevention Regulations were issued. The first leprosy censuswas made the same year. In 1939 the first Leprosarium, "Dr. Pedro López," inZoquiapán, D. F., was opened. The Sarabia (Guanajuato) Leprosarium was

PUBLIC HEALTH IN THE AMERICAS 47
built in 1940. In 1941 the First Regional Leprosy Conference was held in thatState.
Maritime sanitation.-On December 16, 1905, the resolutions of the II PanAmerican Sanitary Convention regarding maritime and international sanitationwere approved, and they were later ratified by the Senate. The first MaritimeSanitation quarantine station was opened February 11, 1906, in the Port of Vera-cruz. In 1938 construction was begun on the Manzanillo quarantine station,and it was inaugurated in 1940.
Sanitation.-Mexico City's first modern drainage system was begun in 1901 atthe initiative of the Superior Council of Health. The first Regulations on Sani-tary Engineering were issued January 1, 1904. In 1939 the National DrinkingWater Division was created in the Department of Public Health. From 1934 to1940, drinking water services were installed in 337 small towns, at a cost of5,500,000 pesos, and benefiting 415,000 persons.
Food Hygiene.-When the Superior Council of Health was created in 1891. aCommission of Food and Beverage Hygiene was included in its organization.In 1902 the first provisions on milk and bread hygiene were adopted, and 1918 sawthe promulgation of the first Regulation on the Production, Sale, and Distributiorof Milk, the Regulation on Production and Sale of Foods and Beverages, andthe Market Regulation.
Child welfare.-The first child welfare center was founded January 1, 1925,and named in honor of Dr. Eduardo Licéaga. In May, 1929 the Child HygieneService was founded, and various child welfare centers were opened in MexicoCity and in some of the States. In that same year the National Child ProtectionSociety, not an official organization, was created. Under its auspices the Mater-nity Home, six home-schools, and seven child centers were established. TheDepartment of Social Assistance for Children was created June 30, 1937, andplaced in charge of child welfare work in the Republic. On December 30, 1939,the Secretariat of Public Assistance came into being, and among its functions areassistance to mothers and children, and child hygiene.
Industrial hygiene.-When the Superior Health Council was created in 1891,it included a Commission on Factory and Industrial Hygiene. In 1929 the In-dustrial Hygiene and Social Prevision Service was established, and placed incharge of Federal action in this field.
Institute of Hygiene.-The Institute of Hygiene, which manufactures thebiologic products used in the prophylaxis of communicable disease, was foundedMay 1, 1895, as the National Bacteriological Institute, a dependency of theBacteriology Section of the Anatomy-Pathology Museum. In 1921 it was re-organized and enlarged under its present name, being a part of the Departmentof Public Health.
Institute of Public Health and Tropical Disease.-The construction of thisInstitute was begun in 1935, and it was inaugurated in 1939.
Important Activities.-Among other important activities of recent years havebeen: the discovery of the causative agent of mal del pinto; adoption of simultane-ous active and passive immunization against diphtheria; preparation of typhusvaccine in adequate quantities and at low cost; and the preparation of an alum-precipitated typhoid-paratyphoid vaccine (T.A.B.), to be administered in asingle dose.
Most important needs.-To judge by the mortality statistics, Mexico's mostimportant health problems at present are the prevention of water-borne diseases,pneumonia, malaria, and tuberculosis.
Future program.-The program for the future must, of necessity, be based onthese four problems, thus including: (1) increased efforts to prevent the trans-
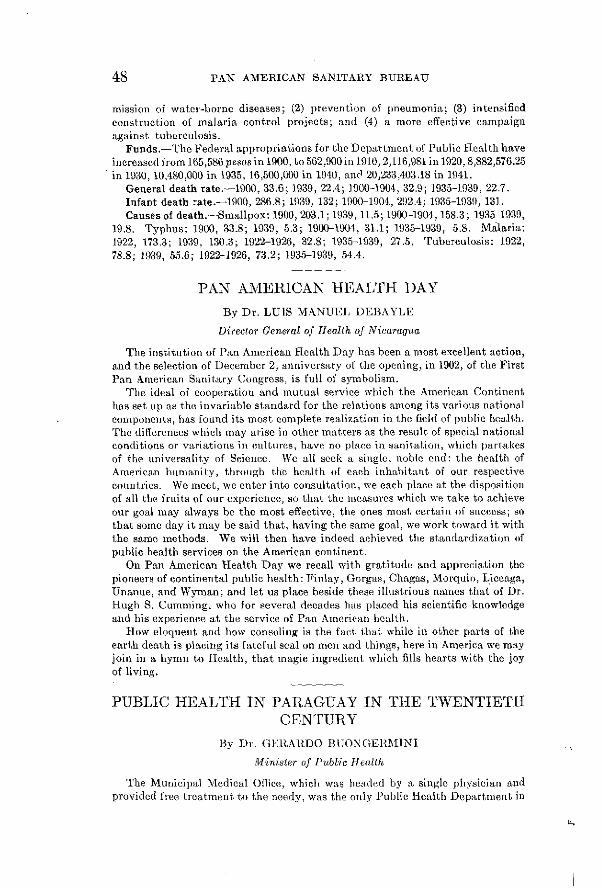
48 PAN AMERICAN SANITARY BUREAU
mission of water-borne diseases; (2) prevention of pneumonia; (3) intensifiedconstruction of malaria control projects; and (4) a more effective campaignagainst tuberculosis.
Funds.-The Federal appropriations for the Department of Public Health haveincreased from 165,586 pesos in 1900, to 562,900 in 1910, 2,116,981 in 1920, 8,882,576.25in 1930, 10,480,000 in 1935, 16,500,000 in 1940, andc 20,233,403.18 in 1941.
General death rate.-1900, 33.6; 1939, 22.4; 1900-1904, 32.9; 1935-1939, 22.7.Infant death :ate.-1900, 286.8; 1939, 132; 1900-1904, 292.4; 1935-1939, 131.Causes of death.-Smallpox: 1900, 203.1; 1939, 11.5; 1900-1904, 158.3; 1935-1939,
19.8. Typhus: 1900, 33.8; 1939, 5.3; 1900-1904, 31.1; 1935-1939, 5.8. Malaria:1922, 173.3; 1939, 130.3; 1922-1926, 32.8; 1935-1939, 27.5. Tuberculosis: 1922,78.8; 1939, 55.6; 1922-1926, 73.2; 1935-1939, 54.4.
PAN AMERICAN HEALTH DAY
By Dr. LUIS MANUEL DEBAYLE
Director General of Health of Nicaragua
The institution of Pan American Health Day has been a most excellent action,and the selection of December 2, anniversary of the opening, in 1902, of the FirstPan American Sanitary Congress, is full of symbolism.
The ideal of cooperation and mutual service which the American Continenthas set up as the invariable standard for the relations among its various nationalcomponents, has found its most complete realization in the ficld of public health.The differences which may arise in other matters as the result of special nationalconditions or variations in cultures, have no place in sanitation, which partakesof the universality of Science. We all seek a single, noble cnd: the health ofAmerican humanity, through the health of each inhabitant of our respectivecountries. We meet, we enter into consultation, we each place at the dispositionof all the fruits of our experience, so that the measures which we take to achieveour goal may always be the most effective, the ones most certain of success; sothat some day it may be said that, having the same goal, we work toward it withthe same methods. We will then have indeed achieved the standardization ofpublic health services on the American continent.
On Pan American Health Day we recall with gratitude and appreciation thepioneers of continental public health: Finlay, Gorgas, Chagas, Morquio, Liceaga,Unanue, and Wyman; and let us place beside these illustrious names that of Dr.Hugh S. Cumming, who for several decades has placed his scientific knowledgeand his experience at the service of Pan American health.
How eloquent and how consoling is the fact that while in other parts of theearth death is placing its fateful seal on men and things, here in America we mayjoin in a hymn to Health, that magic ingredient which fills hearts with the joyof living.
PUBLIC HEALTH IN PARAGUAY IN THE TWENTIETHCENTURY
By Dr. GERARDO BUONGERMI\NI
Minister of Public Health
The Municipal Medical Office, which was headed by a single physician andprovided free treatment to the needy, was the only Public Health Department in

PUBLIC HEALTH IN THE AMERICAS 49
Asunción until 1889. In that year the Chief Executive appointed a Council ofMedicine, which was composed of the majority of physicians then in practice(Flaviano García Rubio, Juan Vallori, Francisco Morra, Manuel Porras Pardo
1ANW a . . .. - ' -
Above: Local Health Unit or Center No. 1, Nicaragua, openel December 2,1940, on the First Pan American Health Day; Below: Child
WTelfare Clinic, General Somoza Health Unit
and Silvio Andreuzzi). The appearance of Bubonic Plague in 1889 (one of itsvictims was Doctor Benjamin Aceval) brought about the creation of the NationalCouncil of Hygiene, composed of four physicians and two pharmacists. Thisbody was in charge of river and domestic sanitary administration, and prepared
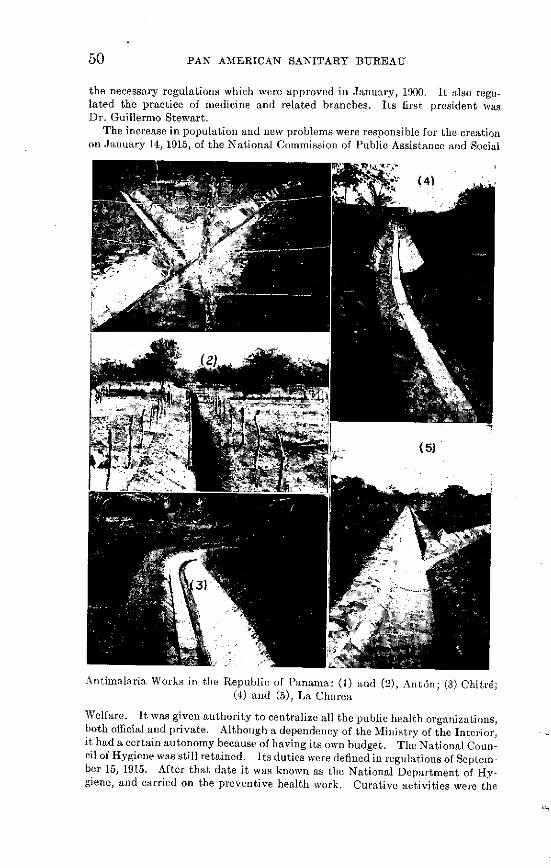
50 PAN AMERICAN SANITARY BUREAU
the necessary regulations which were approved in January, 1900. It also regu-lated the practice of medicine and related branches. Its first president wasDr. Guillermo Stewart.
The increase in population and new problems were responsible for the creationon January 14, 1915, of the National Commission of Public Assistance and Social
Antimalaria Works in the Republic of Panama: (1) and (2), Antón; (3) Chitré;(4) and (5), La Charca
Welfare. It was given authority to centralize all the public health organizations,both official and private. Although a dependency of the Ministry of the Interior,it had a certain autonomy because of having its own budget. The National Coun-cil of Hygiene was still retained. Its duties were defined in regulations of Septem-ber 15, 1915. After that date it was known as the National Department of Hy-giene, and carried on the preventive health work. Curative activities were the

PUBLIC HEALTH IN THE AMERICAS 51
function of the National Commission of Public Assistance. However, the 1917budget law combined the two under the name of Department of Hygiene andPublic Assistance. This arrangement lasted until the creation of the Ministryof Health on January 15, 1936.
During this period the medical profession of Paraguay in cooperation withthe health authorities founded the following institutions: National VaccineConservatory (organized by Professor David Lofruscio); National Institute ofBacteriology (Elmassian, followed by Migone, Urizar and Schenone); the LeprosyColony (Ricardo Odriosola, at that time Dean of the School of Medicine); theGota de Leche or Milk Station (Manuel Peña); Clinical Hospital (Damas de Cari-dad, or Ladies' Charitable Society); and the Maternity Hospital (J. P. Montero).The first campaign against hookworm was carried out under the direction ofDoctor Juan Francisco Recalde during the administration of Professor BenignoEscobar as Director of Public Assistance. Doctor Escobar succeeded in securingthe cooperation of a Rockefeller mission for a five year campaign against intestinalparasites.
The Medical Syndicate of Paraguay brought about compulsory medical servicein industries; the National Red Cross is the work of Doctor Andrés Barbero; theFirst Aid Service was created while Professor Cayetano Masi was Director of theDepartment of Health; the health centers, various regional hospitals, the ruralhealth posts, the School of Public Health Nursing, and other institutions are thework of the present Ministry.
Technical and economic difficulties have not permitted the complete organi-zation of the services and functions of the Ministry of Public Health, created in1936, which since 1937 has carried out its program of public health work as effec-tively as possible within the limits of its budget. The Ministry has been headedby Drs. Pedro Duarte Ortellado, Gerardo Buongermini P., Alejandro Dávalos,Ricardo Odriosola, and the second of these again occupies the post.
Adequate regulations have been adopted by the five Departments into whichthe public health funetions are divided. Among the legislation of a public healthnature are the laws requiring compulsory reporting of contagious diseases, andcompulsory pre-marital certificates; and new regulations on the practice ofpharmacy and related professions. The river, air and railway sanitary serviceshave been modified and enlarged, the Tuberculosis Prevention Service createdand an Epidemiology Service organized to carry out vaccination, disinfection,deratization, and control of malaria and yellow fever. Construction of a newbuilding for the Laboratory is almost finished. A campaign against blindnessand trachoma in the schools has been undertaken, as has one against malariawvhich has become a problem since about two years ago. Typhoid and small-poxvaccination are also carried on.
The Child Welfare Department regulates the functions of the School MedicalService, has reorganized the Milk Station Service, created the School of VisitingNurses and Midwives and a Laboratory attached to the Gota de Leche, and, underthe auspices of the International Institute of Child Welfare, it has organized astudy of infant mortality.
The Dental Department has services in the Capital and also in the interior,the latter attached to the regional hospitals, health units and sanitary posts,as dependencies of the Department of Rural Hygiene. It has organized theDental Supply Service and will continue new rural services as finances permit.
The Department of Public Assistance is in charge of the Permanent MedicalService, the Emergency Surgery and Traumatology Service, and the VenerealDisease Dispensary, and has suburban services in the Hospital of the Workers'Quarter.
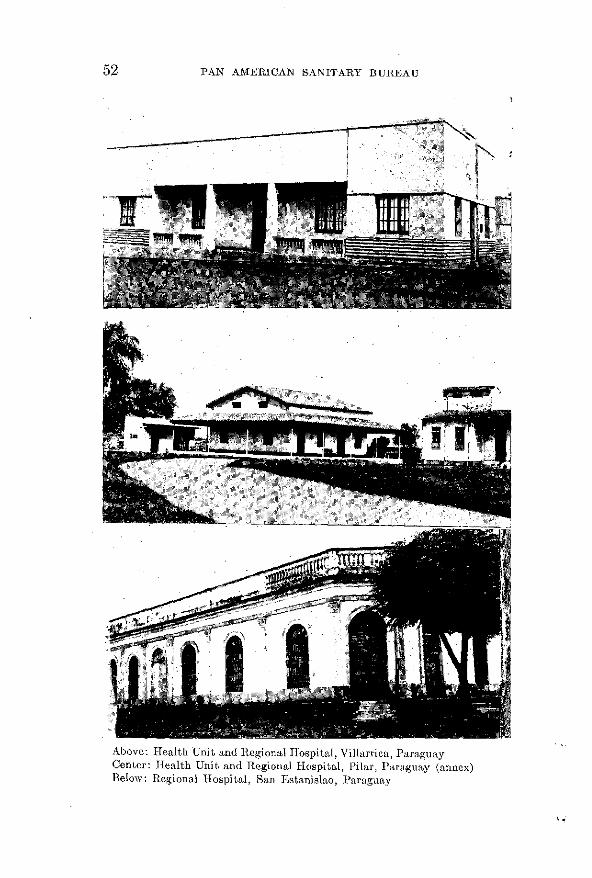
PAN AMERICAN SANITARY BUREAU
1 I I ·-: I1 m~~-I~
Above: Health Unit and Regional Hospital, Villarrica, ParaguayCenter: Health Unit and Regional Hospital, Pilar, Paraguay (annex)Belo\w: Regional Hospital, San Estanislao, Paraguay
52
PTIBLIC HEALTH IN THE AMERICAS 53
The Department of Rural Hygiene, which is directly under the Minister, hasdevoted the greatest possible attention to rural sanitation. It has built severalregional hospitals, organized sanitary posts in more than 100 towns and colonies,amplified the services in the principal cities, and so on. In addition to treatmentand preventive work, the rural services are in charge of death registration andlocal vital statistics information, and also supervise the medical and pharma-ceutical services of industrial establishments. The Ministry functions in con-nection with services of a medical-legal nature and with the Vital StatisticsDepartment, and a central office coordinates the operation of its different depart-ments through daily and monthly reports.
The Public Health Council, composed of the Directors of Departments andother high authorities of certain institutions in the country, assists in the solu-tion of problems submitted to its consideration at meetings presided over by theMinister.
The program for the future includes the following projects, some of which havealready been carried out: surcharge of postage and telegraph stamps, to helpfinance the malaria control campaign; compulsory social security, now understudy; reorganization of the Child Welfare Department; creation of hospitalcommittees in all rural localities, these to have the support of 15% of the muni-cipal revenues: creation of an Allergy Center; organization of the Department ofNutrition and Sanitary Engineering: and an additional tax on cigars and cigarettesfor the creation of an Institute of Cancer.
Funds.-1913, 394,560 pesos (curso legal or ordinary legal tender); 1915, 427,280;1921, 5,160,000 pesos curso legal and 48,000 pesos sealed gold; 1925, 6,380,600 and69,504; 1930, 6,712,680 and 27,400; 1935, 6,439,080 and 21,600; 1940, 43,775,400 and45,500.
Vital Statistics.-Births: 1905, 22.8; 1910, 27.4; 1915, 31.9; 1920, 32.5; 1925, 34.7;1930, 41.1; 1935, 34.6; 1939, 32.6; 1940, 39.9; General death rate: 1905, 12.9; 1910,16.7; 1915, 14.1; 1920, 25.4; 1925, 19.1; 1930, 16.6; 1935, 23.8; 1939, 13.9; 1940, 16.Infant death rate: 1914, 136.4; 1920, 202.4; 1925, 151.5; 1930, 109.5; 1935, 102.9;1939, 76.4; 1940, 85.6.
Causes of death.-Dysentery: 1905, 14; 1910, 6; 1915, 15; 1920, 22; 1925, 31;1930, 7; 1935, 330; 1939, 71; 1940, 51; tuberculosis: 1905, 103; 1910, 103; 1915, 128;1920, 128; 1925, 201; 1930, 190; 1935, 261; 1939, 202; 1940, 197; typhoid and para-typhoid: 1905, 44; 1910, 28; 1915, 19; 1920, 38; 1925, 51; 1930, 32; 1935, 58; 1939, 79;1940, 63.
PUBLIC HEALTH IN PERU (FISCAL YEAR 1940-41)By DR. MANUEL PRADO
President of the Republic
Among the important developments in public health in Peru duringthe past fiscal year have been the continuation of efforts to create a na-tional public health conscience; the creation of the National Department ofIndustrial Hygiene; the creation of a Commission to coordinate maternal andchild welfare activities in the country, and the expansion of such work, whichincludes among other things a program of rural hygiene and puericulture carriedon by the National Institute of Child Welfare, with its traveling clinic, the 225,420consultations given, the 54,181 luncheons furnished pregnant women at its Mother'sRestaurants; and the 292,000 liters of milk distributed to children in addition toother food, and medicine. Construction of a second children's hospital to supple-ment the efforts of the present one is under consideration. Another factor in

54 PAN AMERICAN SANITARY BUREAU
child welfare was the furnishing of 2,412,796 school lunches in the various prov-inces. The government is attempting to assure an adequate supply of medicinesat low cost, and commissions are studying the problem. Narcotic drug controlhas been reorganized. Social Security legislation is now actively in force, on thecompletion of the Workers' Hospitals in Lima and Ica provinces. Employers arestill required to furnish free medical and pharmaceutical assistance to workersnot covered by social security. Special health campaigns are under way in theNorthern departments, and 33 sanitary brigades have been created.
Tuberculosis work has been coordinated under the National TuberculosisService. Plans are being worked out for a system of dispensaries and travelingclinics throughout the country. The women's wing of the Jauja sanatorium has
N been completed, and the men's pavilion is to be enlarged. In connection with theanti-venereal disease campaign, a dispensary is to be established in Callao.
Antiplague campaign in Perú: Inoculated guinea pigs placed in glass jars
As a preventive measure against yellow fever, vaccination has been made freeand compulsory in certain areas. A National Malaria and Rural Hygiene Servicehas been created. The cooperation of the Rockefeller Foundation has beensecured for a demonstrative malaria control campaign in the Cosa valley. Effortsto prepare for settlement and exploitation of the Peruvian selva or tropical forestarea, under public health safeguards, have been intensified. Preliminary surveysare being made, and a central laboratory has been established in Iquitos whichwill serve the selva regions, and will also study the medicinal and vegetableresources of the area.
Peru has at present 62 hospitals with 8,636 beds, in charge of the Sociedades deBeneficencia (Welfare Societies), and efforts are being made to increase thesefacilities, which are recognized as inadequate. A number of public health officershave been sent abroad for special training. Pending the reorganization of coastalmaritime sanitation, certificates of exemption from fumigation may be issued

PUBLIC HEALTH IN THE AMERICAS 55
only in Callao, with the approval of the Plague Service, which has actively con-tinued its various anti-plague efforts.
The present budget for Public Health, 6,857,462 gold soles, although a 14%increase over the previous year, is not considered sufficient for the needs of thecountry, and it is hoped to increase it year by year.
NEW OBJECTIVES FOR THE COORDINATIVE WORKOF THE PAN AMERICAN SANITARY BUREAU,
WASHINGTONBy Dr. CARLOS ENRIQUE PAZ SOLDÁN
Honorary Member of the Pan American Sanitary Bureau, and Professor of Hygienein the Universily of San Marcos. Lima, Perú
An imperative duty of taking part in the celebrations of the Pan AmericanSanitary Bureau rests upon those of us who have been ideologically serving itfor almost two decades, who have watched, year after year, its uninterruptedprogress and its growing influence on the public health of this hemisphere, andwho look upon as our own the events which it commemorates and its triumphs,which are so closely bound up with the devotion of the workers in Washingtonwho, under the vise leadership of Dr. Hugh S. Cumming, have strengthened itand made it the Pole Star of American bio-social policy. It is not surprisingtherefore, that on Pan American Health Day we should say something about thenew objectives awaiting this institution which is representative of America'swill to live; which is at the same time her conscience and her light in everythingrelated to human health throughout the vast extent of the New World.
There are two tasks calling upon its coordinating and orientating activity, inthese hours of destruction through which Humanity is passing: to define suc-cinctly the Pan American concept of Public Health Law; and to present a pan-oramic picture of the biosocial conditions of labor in this continent.
American Public Health Law.-The definition of American Public Health Law,which is already in progress thanks to the initiative of the IV Pan AmericanConference of National Directors of Health, is not a tiresome undertaking, butrather a labor which will give new splendor to the biosocial policies of the Conti-nent. It is an attempt to surpass the Pan American Sanitary Code, which hasdone so much for the progress of our peoples. And this achievement would besought through giving all our countries a model Sanitary Code, capable of servingas a reference for daily public health activities. In this respect, a magnificentprecedent and an unsurpassable lesson was the work of the American PublicHealth Association in setting forth in October 1940 the "minimum functions de-sirable and the principles of organization for public health work."
But the drafting of this model Code requires preliminary studics which shouldbe carried forward without delay: the review of the public health history of ourpeoples, with a historical, objective, and impartial examination of what wascreated, improvised, or dreamed of in the desire for hecalth, during the centuriesof evolution of American society. How interesting it would be to know the wayin which each of the American Republics went through the four periods of de-velopment of public health policy: the empiric, the medical, the Pasteurian, andthe present, which we may call the social, thought it ought to be known as thehuman period.
In each of these periods and in each of our countries, what was the nature of theinstitutions which carried out the programs thus inspired? What was the part of

56 PAN AMERICAN SANITARY BUREAU
each of the authorities which successively played the leading role in the safe-guarding of the health of communities-the Church, the Community, the State,the Collective Group? What were the immediate objectives, and above all,how were they attained, with the consequent accumulation of valuable experi-ence? The answers to these and other questions would constitute a treasure-store of fundamental guides for the great task of the model codification of publichealth law in America.
How shall a model Pan American Code take into account the diversity in thecommon traditions of the Continent, without receiving from their teachings in-spiration and guides for the future? Surely these are reason enough for the PanAmerican Sanitary Bureau to organize the making of a preliminary, basic inven-tory before proceeding with the drafting of American Public Ilealth Law. Thecoordination of the reports on the historical evolution of public health legislationin America, and on the organizations which have tried to carry out such legisla-tion, would be a most fruitful work, bringing to the Bureau new and brighterlaurels.
Medico-social study of labor.-The second immediate task inviting the co-ordinating action of the Pan American Sanitary Bureau, is the medico-socialstudy of labor, as a vital problem, with the pointing out of objectives and of themeans of discovering the manner in which man goes about his work in Americain his cosmo-telluric environment.
Until the V Pan American Sanitary Conference, industrial hygiene had notreceived any attention from the sanitarians of the Continent. Only in Monte-video had the question received notice, with the passage of this resolution: "TheSixth Conference recommends that on the program of the next Conference, prob-lems of industrial hygiene be included among the agenda," a recommendationwhich was repeated by the VII Conference, without any definite steps being taken.But in Lima (1927), the following resolution was adopted: "The VIII Pan Ameri-can Sanitary Conference declares: that the health and well-being of the workingclass, are linked with the health and the economic progress of a country, and thatthe damages resulting from industry are injurious to the nation, decreasing theactual production, and above all, the future production of the population, under-mining its health, for which reason there is recommended to the various countriesof America the necessity of establishing within the health administration specialdivisions placed in charge of everything relating to labor and to industrial hy-giene, in order that workers may be placed in the best possible conditions of livingand working, in accordance with their physical and mental aptitudes."
The interpretation of this resolution would justify bur proposal that the Bureaustudy the results achieved by the recommended organization, and to what extentit has been put into practice by the different countries.
The IX Conference recommended, as a supplement to the Lima resolution,that a study of labor and its sanitary conditions in America be prepared for the XConference, but unfortunately this was not done.
Without fear of contradiction, it may be stated that we are ignorant in manyrespects concerning the actual sanitary conditions under which men work in theAmericas. It is true that in Europe much light has repeatedly been thrown onthis subject, but it must be recognized that those who have cast this light, havenot been conversant with the psychology and biology of our peoples. Thereforeit is highly desirable that the Pan American Sanitary Bureau, with the coopera-tion of all the American health authorities, should undertake to collect new bio-social information on these matters. Lest there should be some question as tothe coordinating action which such a study would represent, we shall outline whatwe mean by the biosocial study of labor.
..i

PUBLIC HEALTH IN THE AMERICAS 57
We have for many years taught that work is, fundamentally, a natural biologicfact, grounded in the condition of man: in the sweat of thy brow shalt thou labor,God's decree for man; in sorrow shalt thou bring forth thy children, His sentencefor women. Two aspects of labor: one assuring the sustenance of today, theother, the immortality of the species.
American public health has done and is doing much to prepare wonoan for herlabor, in its essence: maternity. But it has not been as eager to bring within itsfold the labor of men. And this is what should be attempted: to bring this prob-lem into the private camp of the sanitarians, rather than let it continue theproperty of the politicians and lawyers, who are not always aware that the basisof their allegations must be a biologic one. The medical sociologist looks atlabor from another viewpoint, which allows him to perceive its complex andmultiple aspects. He is interested in knowing the worker; in evaluating his trans-forming and psychic capacity; in establishing the techniques which will betterdominate the geocosmic atmosphere conditioning work; in understanding in-timately the combination formed by human power and the resistance of things;in foreseeing the economic, social, and political consequences of this meeting offorces; and in indicating how from this examination the juridical treatment mayarise, so that the written standards shall be just, and shall foresee accidents,illnesses, fatigue, and conflicts of all kinds, and shall, above all, elevate work tothe superior rank to which it belongs: these are the horizons of this investigator,which attract his efforts as a man versed in the knowledge of man.
The wisdom of the public health authorities of our Republics render anyfurther insistence on these points unnecessary. What has been expressed hereis more than enough to fulfill our pleasant and self-imposed task, of indicating,on the Second Pan American Health Day, some objectives for the future labor ofthe consecrated body known as the Pan American Sanitary Bureau.
PUBLIC HEALTH IN THE UNITED STATES
By Dr. THOMAS PARRAN
Surgeon General, U. S. Public Health Service
The most important advance in public health in the United States since theturn of the century has been the development and strengthening of permanent,professional health organization at Federal, State and local levels.
The Public Health Service-the first Federal agency concerned with health-was established by Congress as the Marine Hospital Service in 1798. From anorganization concerned only with the care of American seamen, the MarineHospital Service developed gradually to become the U. S. Public Health Servicein 1902. Today it is concerned with the health of 130,000,000 men, women andchildren.
With the passage of the Social Security Act in 1935, the Public Health Servicewas enabled to play the most direct part in its history in improving the healthservices of the 48 States and the Territories. The health provisions of the Actmade available Federal funds to be allotted in grants-in-aid to the States forpublic health work. To become eligible for these funds, the States were requiredto submit health programs for approval by the Surgeon General of the PublicHealth Service according to standards set by him and the Conference of Stateand Territorial IIealth Officers. One requirement held that the State programswere to be carried out by full-time, professional workers. Provision was made forthe training of State personnel in qualified professional schools at Federal ex-
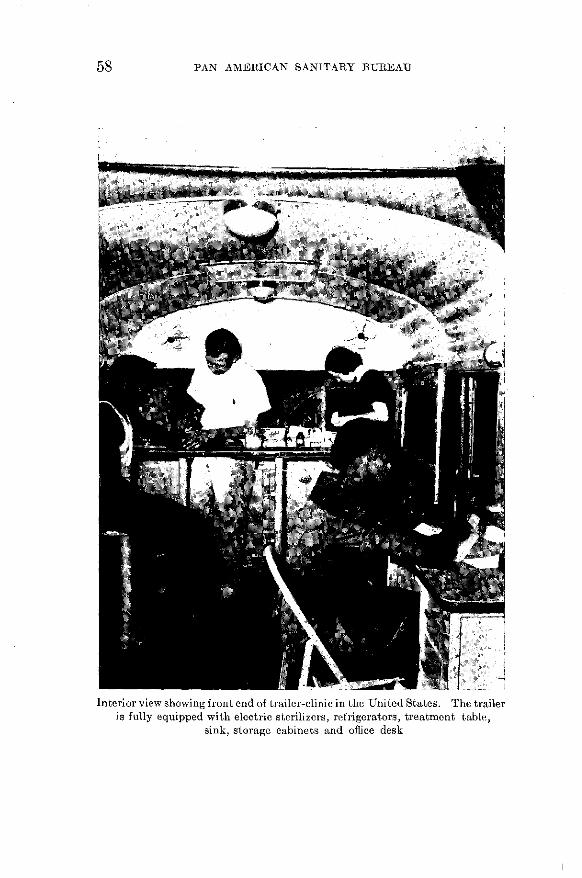
58 PAN AMERICAN SANITARY BUREAU
u ~~~~~~~~---,1 'Interior view showing front end of trailer-clinic in the United States. The trailer
is fully equipped with electric sterilizers, refrigerators, treatment table,sink, storage cabinets and office desk
1 1

PUBLIC HEALTH IN THE AMERICAS 59
pense. During the period 1936-41, a total of $47,333,000 was paid to the Statesand Territories by the Federal government under Title VI of the Act, which per-tained to public health services. So great was the stimulation of Title VI, thatthe States and localities themselves budgeted $30,438,399 more for public healthin the fiscal year 1942 than they spent in 1935. The Federal contribution for1942 indeed, amounts to only 12.4 percent of the total $97,458,330 appropriated.
The increase in full-time county health departments has been one of the mostnotable effects of the Act. In 1935, only 594 of the 3,000 counties were served byfull-time health units; in 1941 the number was 1,655. More than 7,000 doctors,nurses, engineers and laboratory technicians have received specialized trainingin public health through Social Security funds.
Here was a concrete foundation for the national defense health program, nowprogressing so splendidly.
In May, 1938 Congress passed the Venereal Disease Control Act-a secondmajor step toward a national health program. Here again Federal funds weremade available to the States through grants-in-aid under the administration ofthe Public Health Service, although the Venereal Disease programs were admin-istered by the States themselves. Under the Act, public clinics increased from1,122 in 1938 to 3,088 in 1941. During the past five years, clinic treatments forvenereal disease increased from 2,122,000 to 10,178,000. Today every State pro-vides free anti-venereal drugs and laboratory diagnostic services to doctors.Venereal disease is now definitely decreasing under the first national controlprogram in the United States.
Another notable advance was the founding of the National Cancer Institute,in 1937. In that year the National Cancer Act established the Institute and aNational Advisory Cancer Council in the Public Health Service. Funds wereprovided for a comprehensive research program at the Institute and to expandresearch in other scíientific institutions.
Here was the first, organized Federal attack on cancer. The Institute broughttogether the nation's best scientific thought to select and advance the most
promising lines of research. The training program seeks to overcome the presentshortage of cancer specialists. It provides qualified physicians and researchscientists with an opportunity to specialize in cancer research and therapy. TheAct also provided for the purchase of approximately 9 grams of precious radiumfor loan to hospitals and clinics. In these institutions the radium is used to treatpatients. No charge is made to patients for the use of Federally-owned radium.Meanwhile at the National Cancer Institute more lines of cancer research areunder investigation than in any other laboratory in the world.
The three programs under Title VI of the Social Security Act, the VenerealDisease Control Act and the National Cancer Act represent the most recent ad-vances in public health in the United States. The principle of Federal coopera-tion with the autonomous State and Territorial health departments underlieseach of these progressive programs.
There has been a beginning toward unification of Federal health and welfareactivities. The U. S. Public Health Service, the Food and Drug Administration,the Social Security Board and the U. S. Office of Education were brought underone administration-the Federal Security Agency-in 1939.
The present national emergency has further extended Federal health activityin the States and Territories under the administration of the Public HealthService.
Water purification systems, sewage and garbage disposal plants, hospitals andhealth centers are being built by the Federal Government in defense areas wherethe Service believes them necessary. Qualified professional personnel, paid by

60 PAN AMERICAN SANITARY BUREAU
the Federal government, are sent into States and localities where needs have ad-vanced beyond the capacity of local authorities.
An important step has been taken with the decision of the President to rehabili-tate young men rejected by the military services because of correctible physicaldefects. Examination of the first million of these young men for venereal dis-ease has provided the first, large scale estimate of the extent of syphilis amongthe general population.
Technical guidance, money and personnel expert in industrial hygiene havebeen provided to control hazards and promote health among workers in the greatdefense industries.
The science of nutrition, born only 20 years ago, has shown us that food ismedicine-preventive medicine. In 1940,a national nutrition program was set
Anti-malarial work in the United States: left, taking a reading of wind velocityon the surface of the water; center, taking a reading of rainfall;
right, dipping for mosquito larvae
in motion. If it be carried out fully, the people will attain levels of health,vigor and efficiency which have in the past seemed unattainable. The programcontemplates increased research, and the production and consumption of moreof the foods which provide the defensive vitamins and minerals; less of the foodswhich are lacking in these elements.
We ought perhaps now to pause for a moment of recollection before we considerthe future of public health in the United States. We have seen the acute, com-municable diseases virtually conquered. We have seen organization and exten-sion of full-time public health agencies in all the States, aided by an active Federalservice. An attack has begun on venereal disease. A program for better nutri-tion is being developed. National defense has sped health services by a decadeand there is support for the rehabilitation of young men eligible for military serv-ice except for minor physical defets.
PUBLIC HEALTH IN THE AMERICAS
J1
HEALTH AUTHORITIES OF THE AMERICAN REPUBLICS
DR. WENCESLAO MEDRANO
(Rep. Dominicana)
DR. FÉLIX LAIRET HIJO
(Venezuela)
H. DR. J. C. MussIO FOURNIER
(Uruguay)DR. RAFAEL SCHIAFFINO
(Uruguay)DR. ARMANDO CASTILLO PLAZA
(Venezuela)
61
4I
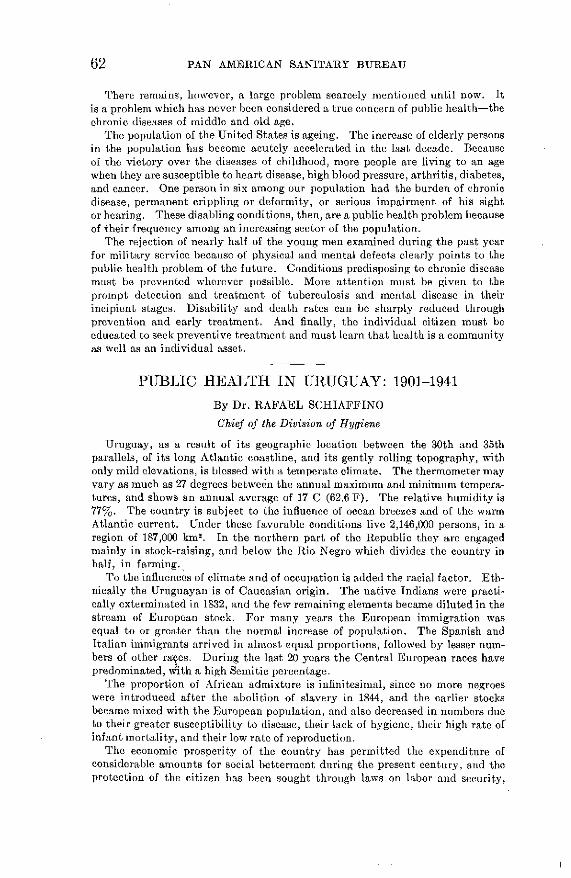
62 PAN AMERICAN SANITARY BUREAU
There remains, however, a large problem scarcely mentioned until now. Itis a problem which has never been considered a true concern of public health-thechronic diseases of middle and old age.
The population of the United States is ageing. The increase of elderly personsin the population has become acutely accelerated in the last decade. Becauseof the victory over the diseases of childhood, more people are living to an agewhen they are susceptible to heart disease, high blood pressure, arthritis, diabetes,and cancer. One person in six among our population had the burden of chronicdisease, permanent crippling or deformity, or serious impairment of his sightor hearing. These disabling conditions, then, are a public health problem becauseof their frequency among an increasing sector of the population.
The rejection of nearly half of the young men examined during the past yearfor military service because of physical and mental defects clearly points to thepublic health problem of the future. Conditions predisposing to chronic diseasemust be prevented wherever possible. More attention must be given to theprompt detection and treatment of tuberculosis and mental disease in theirincipient stages. Disability and death rates can be sharply reduced throughprevention and early treatment. And finally, the individual citizen must beeducated to seek preventive treatment and must learn that health is a communityas well as an individual asset.
PUBLIC HEALTH IN URUGUAY: 1901-1941
By Dr. RAFAEL SCHIAFFINO
Chief of the Division of Hygiene
Uruguay, as a result of its geographic location between the 30th and 35thparallels, of its long Atlantic coastline, and its gently rolling topography, withonly mild elevations, is blessed with a temperate climate. The thermometer mayvary as much as 27 degrees between the annual maximum and minimum tempera-tures, and shows an annual average of 17 C (62.6 F). The relative humidity is77%. The country is subject to the influence of ocean breezes and of the warmAtlantic current. Under these favorable conditions live 2,146,000 persons, in aregion of 187,000 km2 . In the northern part of the Republic they are engagedmainly in stock-raising, and below the Rio Negro which divides the country inhalf, in farming.
To the influences of climate and of occupation is added the racial factor. Eth-nically the Uruguayan is of Caucasian origin. The native Indians were practi-cally exterminated in 1832, and the few remaining elements became diluted in thestream of European stock. For many years the European immigration wasequal to or greater than the normal increase of population. The Spanish andItalian immigrants arrived in almost equal proportions, followed by lesser num-bers of other races. During the last 20 years the Central European races havepredominated, wÑith a high Semitic percentage.
The proportion of African admixture is infinitesimal, since no more negroeswere introduced after the abolition of slavery in 1844, and the earlier stocksbecame mixed with the European population, and also decreased in numbers dueto their greater susceptibility to disease, their lack of hygiene, their high rate ofinfant mortality, and their low rate of reproduction.
The economic prosperity of the country has permitted the expenditure ofconsiderable amounts for social betterment during the present century, and theprotection of the citizen has been sought through laws on labor and security,
PUBLIC HEALTH IN THE AMERICAS 63
maternal and child protection, old age pensions, pensions for various groups ofindividuals, and so on.
Above: Montevideo's first hospital, founded by Mateo Vidal in 1781; below:Clinical Hospital, the most modern in the city.
At the beginning of the century public health was centered in the Council ofHygiene which, in addition to the regulation of the medical prófession, was in
64 PAN AMERICAN SANITARY BUREAU
charge of the sanitary condition of the country and of international health; andin the Council of Public Assistance, which administered the hospitals and poly-clinics for the needy. By a law of November 7, 1910, the regional hospitals wereincluded, so that this organization was in charge of all welfare work in the country.On October 15, 1931, the two councils were merged by law into a single Council,and then into the Ministry of Public Health. Later the Children's Council wastransferred from the Ministry of Health to that of Public Instruction.
At the beginning of the present century the sewage system of Montevideo wasmodernized, and this was followed by the installation of water supply and sewagesystems in Salto, Paysandú, and Mercedes. In 1916 the Department of SanitaryWorks was founded, under the Ministry of Public Works, and since that time it hasspent 20,000,000 pesos in the provision of safe water to 117 more cities and towns,and in the construction of sewage systems in 17 important cities. The pavingof streets is a function of the municipalities, which have spent a great deal on suchimprovements.
At the present time the welfare facilities of the country include 56 hospitalswith 9,800 beds. The budget of the Ministry amounts to 8,560,332 pesos, of whichthe preventive expenditures amount to but little over half a million, the restgoing to welfare.
Public Health organization is carried out through the Division of Hygiene,which has medical health delegates in the 19 departments, and nurses who assistin their duties. The Division includes the sections of Vital Statistics, Domesticand International Sanitation; Health Education; Sex Hygiene; Rabies Pro-phylaxis; Preventive Clinics; Industrial Hygiene; School and Lyceum Hygiene;Hygiene of Nutrition; Control of Narcotics, and so on. The campaign againsttuberculosis operates directly under the Minister.
Public health indexes have improved notably since the beginning of thiscentury.
Vital statistics.-Population, 1901, 964,577; 1939, 2,146,545; births, 31,703(32.8 per 1,000 population) and 42,862 (19.9) respectively; marriages, 4,480 (4) and15,001 (7); general deaths, 12,504 (13) and 19,341 (9). General and infant deathrates by five year periods: 1901-1905, 12.9 and 103; 1906-1910, 13.9 and 106;1911-1915, 12.9 and 10.5; 1916-1920, 13.4 and 11.1; 1921-1925, 11.5 and 10.1; 1926-1930, 10.6 and 98; 1931-1935, 10.3 and 95; 1936-1939, 9.7 and 92. Tuberculosismortality: 1901-1905, 113; 1936-1939, 109. Typhoid mortality: 1901-1905, 18;1936-1939, 8.2.
Uruguay has neither malaria nor hookworm. During the present century therehas been no epidemic of yellow fever or of other tropical diseases. However, inthe last few years more than 100 cases of Chagas' disease have been reported,with very low mortality.
Diphtheria has been epidemic since 1919, with the following mortality: 1921-1925, 4.8 per 100,000; 1926-1930, 6.6; 1931-1935, 14.8; 1936-1939, 10.9. Cancer ratesare steadily rising, due in part to more accurate diagnosis. Tetanus, anthrax,and other contagious diseases cause less than 100 deaths a year. Uruguay has1,800 physicians, of whom 1,200 are located in the capital.
The favorable state of the public health now awaits the benefits which shouldresult from the adoption of the Sanitary Code which, drafted in accordance withmodern principles, is now pending the approval of Parliament.
In the international field, Uruguay has cooperated with the Pan AmericanSanitary Bureau, and has likewise taken part in the meetings of the Health Sectionof the League of Nations, and of the International Office of Public Health of Paris,and has adhered to the various international conventions.

PUBLIC HEALTH IN THE AMERICAS
r
a
F: ;B 1. .
v i t
li ~~~~>
' !~~~~~b
¡, 58~ ~~5., : 9
,d;
42 9 g
65
lo
!Nwau -la
lap
1tu

66 PAN AMERICAN SANITARY BUREAU
OUTLINE OF PUBLIC HEALTH IN VENEZUELA
By Dr. M. LARES GABALDON
Chief of the Service of Information and Health Education, of the Ministry ofHealth and Social Welfare
Venezuelan public health organization had its beginning March 17, 1909,with the creation of the Public Health Commission. In November, 1911, theNational Office of Health was inaugurated, with its Institute of Hygiene and itsChemistry, Bacteriology, and Parasitology Laboratories. In 1926 the firstvenereal disease dispensary was opened, in Caracas, and a Sanitary EngineeringCommission was appointed. The first tuberculosis dispensary was opened in 1928.
In 1929 the National Health Office increased its activities, with the creation oflaboratories for water analysis, physiotherapy, and radium therapy (this lastconstituting the beginning of the campaign against cancer). At this same timethe studies of malaria and hookworm were carried forward, with the collaborationof the Rockefeller Foundation; the School Inspection Service was organized, and a"National Sanitary Conference" was set up to study national public healthproblems.
With the establishment of the Ministry of Public Health, Agriculture andHusbandry, in August, 1930 a transformation of Venezuelan public health organi-zation was begun, which was intensified with the creation in 1936 of two newMinistries: that of Public Health and Social Welfare, and that of Agriculture andHusbandry. Since then sanitary services have multiplied rapidly, with theopening of tuberculosis, venereal disease and maternal and child welfare dis-pensaries and clinics, under their respective Divisions of the Ministry. In 1936the Divisions of Yellow Fever Prevention and of Malaria were created, the latterhaving an annual budget of 3,000,000 bolívares.
In 1938 the Department of Health, of the Ministry, was reorganized, and theexisting Health Offices were transformed into Health Units or Centers. In thesame year the School Hygiene Service, and the Divisions of Epidemiology andStatistics, Laboratories, Sanitation, and Sanitary Inspection, and Health Units,were organized, and the National Institute of Health, with its own autonomouspersonnel and appropriation, was founded.
Malaria.-The Malaria Division, organized in July 1936, has its headquartersin Caracas, and includes four sections: Epidemiology, Local Malaria Control andQuinine Distribution Commissions, Malaria Engineering, and Administration.A malaria survey is at present being made; it has already been completed for eightof the 20 States, and it is hoped that it will be finished by December, 1942. Themost important vectors are A. darlingi, particularly in the interior, and A. albi-manus on the coast. The 1,707 distributing agencies in 1,111 centers of population,distribute from 2,000 to 2,500 kg. of quinine sulfate annually, in tablets for indi-vidual treatment. Malaria control engineering projects have been carried out in10 cities, and in Maracay the index of infection was thus reduced to zero. Theestablishment of a School of Malariology for physicians and engineers is nowunder consideration.
Tuberculosis.-Since the creation of the Tuberculosis Division in July, 1936,23 services have been established, with tuberculosis dispensaries in the greaterpart of the principal cities. These attempt to solve the problem of tuberculosiscare, since the number of beds available is not sufficient. The Simon BolívarTuberculosis Sanatorium has been functioning for a year and a half, and anotherlarge one is under construction in Mérida. The Federal Government, in coopera-tion with the Statcs, has endeavored to secure the installation of tuberculosis

PUBLIC HEALTH IN THE AMERICAS 67
vio a u
Above: Model housing, 400 dlwellinp-s, fer individuals whose insanitary homesin an old swampy and unhealthful quarter of Puerto Cabello,
Venezuela were razed.Below: Venezuelan small-town hospital
Canal of 25,000 liters per second capacity, lined with prefabricatedconcrete; located south of Maracay, Venezuela

68 PAN AMERICAN SANITARY BUREAU
wards in various hospitals in the country. Venezuela's Tuberculosis Societysponsored the First National Tuberculosis Congress, in 1938, the First Tuber-culosis Jornadas (Meetings), in 1940, and is preparing for the Second NationalTuberculosis Congress, to be held in Maracaibo in 1942.
Maternal and child welfare.-The Division of Maternal and Child Welfare,organized in 1936, has among its facilities the Institute of Puericulture and 40 milkstations in Caracas, which are attended by 161 mothers and 1,387 infants daily.In 1940, 517,205 liters of milk were distributed. The Institute and centers alsotrain physicians and nurses in puericulture. The work of the Division has beenextended to rural areas, and the mortality from infant tetanus has decreased from2,411 in 1923 to 202 in 1910. In November, 1936, the Venezuelan Child Councilwas created as a coordinating center, and it already has at its disposal observationclinics for children, nursery homes, and an Institute of Re-adaptation for childrenunder 12.
Venereal disease.-The Venereal Disease Control Division operates six dis-pensaries in Caracas and 47 throughout the rest of the Republic. Venezuelanlaws authorize compulsory treatment of venereal diseases during the contagiousperiod.
School hygiene.-This Service, organized in 1939, at present has a staff of sevenphysicians, four medical specialists, seven dentists, 12 hygienists and 16 assistants,who work through 12 district centers. A number of school lunchrooms, and twochildren's camps, one maritime and the other inland, have been installed.
Hookworm.-Hookworm was first identified in Venezuela in 1903. Some yearslater the control campaign was begun, and the work is carried on with intensitythroughout most of the country, including especially health education, designingof new types of latrines, setting up of shops for the manufacture of latrine parts,and so on.
Sanitary engineering.-Since its reorganization in 1936, thc Division of Sani-tary Engineering provides consultation service, inspection and supervision ofsanitary engineering projects, and the direction of soil sanitation work.
Yellow fever.-This Service, which was set up in 1937, has devoted particularattention to the study of yellow fever immunity in Venezuela and to the organiza-tion of a viscerotomy service for control purposes in regions in which the diseasehas been shown to have been present in former years.
Nutrition.-A Committee on Nutrition was recently appointed, to makepreliminary studies preparatory to the organization of a Division of Nutrition.
Pharmacopoeia.-A special Commission has edited the Venezuelan Pharma-copoeia, which will soon be published and will meet an urgent need.
Foods.-A scientifically trained force of inspectors exercises daily supervisionover meat, milk and millk products, from the sources of supply to the retail stores,and results have been very satisfactory since the inauguration of the servicefour years ago. A program has been drawn up so that each technical service will beplaced in the charge of specialists, providing for a decentralization of work withinthe Ministry. The base of action will then be each health unit, in which all thepublic health services of the country are represented according to the needs of eachregion.
Funds.-The Venezuelan public health appropriations have increased from757,112 bolivares in the fiscal year 1900-01, 362,502 in 1904-1905, 487,191 in 1909-1910, and 207,137 in 1914-15, to 1,972,921 in 1919-20, 2,319,317 in 1924-25, 5,054,026in 1929-30, 5,004,478 in 1934-35, 19,959,752 in 1939-40, and 17,959,752 in 1940-41.
Vital statistics.-General deaths: 1905, 58,343; 1909, 53,364; 1936, 57,876; 1939,67,757; 1940, 61,557; infant deaths, 11,480, 6,422, 13,244, 17,058, and 16,234 re-spectively; tuberculosis, 5,270, 3,537, 3,256, 3,566, and 3,510; typhoid, 1,482,1,231, 269, 312, and 321; malaria, 9,015, 9,268, 2,225, 1,423, and 1,261.
SOME PAN AMERICAN PUBLIC HEALTH PIONEERS*
CARRIÓN, DANIEL, A. (1858-1885), Peruvian medical student who proved by hisdeath in the interests of science the identity of verruga peruana andOroya fever, now known as Carrión's Disease or Bartonellosis.
CHAGAS, CARLOS (1879-1934), Brazilian sanitarian and research worker; dis-covered American Trypanosomiasis or Chagas' Disease.
CoNi, EMILIO R. (1855-1928), Argentine pioneer in child welfare, tuberculosiscontrol, and vital statistics organization.
COUTO, MIGUEL (1864-1934), "Prince of Brazilian Medicine," best rememberedfor his influence as a teacher.
CRuz, OSWALDO GONCALVES (1872-1917), Brazilian sanitarian; eradicated yellowfever froil Rio de Janeiro; long Director of the Institute now bearinghis name.
DEL Rio, ALE.IANDRO (1867-1939), Chilean sanitarian and pioneer in social as-sistance and welfare.
DURÁN, CARLOS (graduated 1874), of Costa Rica, physician and statesman;founder of laboratory, school of nursing, tuberculosis sanatorium.
ESPEJO, FRANCISCO JAVIER EUGENIO )E SANTA CRUZ Y (1740-96), Ecuador,public health pioneer, foe of quackery, first public librarian and journalistof Ecuador, died in jail as an enemy of Spanish rule.
FINLAY, CARLOS J. (1833-1915), Cuban hygienist, discover of the transmission ofyellow fever by the Aedes aegypti mosquito (1881).
GORGAS, WILLIAM CRAWFORD (1854-1920), U. S. Army Medical Officer, who sani-tated Habana and the Canal Zone and aided in the solution of yellowfever and other public health problems in other American countries andAfrica.
GUITERAS, JUAN (1852-1925), Cuban sanitarian, yellow fever research worker,and public health worker in both Cuba and the United States.
LICÉAGA, EDuARDO (1839-1920), Mexican public health leader and educator who,among other things, freed his country of plague and yellow fever.
MORQUIO, LuIs (1867-1935), Uruguayan pediatrician, initiator of and leader inmany developments in child care, and perhaps most influential as ateacher.
PALOMIO, ToMÁ.s G. (XIX century), sanitarian and statesman; of El Salvador;first president of Superior Board of Health (1900).
PENNA, JOSÉ (1855-1919), Argentine hygienist and teacher; founder of hospitals,dispensaries, the bacteriological institute, and national quarantineservice.
RANGEL, RAFAEL (1877-1909), founder of modern Venezuelan parasitology.RAWsoN, GUILLERaIO (1821-1890), of Argentina, physician, statesman, and sani-
tarian; son of a U. S. Navy Surgeon.RAZETTI, LUIS M. (1862-1932), Venezuelan surgeon, obstetrician, and medical
sociologist.ULLOA, JUAN J. (1859-1913), Costa Rica sanitarian and statesman; organizer of
local medical care for the poor.UNANUE, JosÉ HIPÓLITO (1755-1833), of Peru, physician, statesman, philosopher,
* See also Pub. 159 of the Pan American Sanitary Bureau, "Some Pan American Pioneers inPublic Health," and "The Pan American Sanitary Bureau, its Origin, Development and Achieve-ments," by A. A. Moll, Bol. of San. Pan., Feb. 1942, p. 141, for other pioneers. Additional infor-mation may be obtained from these publications and from the Pan American Sanitary Bureau.
69
70 PIONEERS IN PUBLIC HEALTH
friend of Bolívar and San Martín, and one of the fathers of Americanmedicine.
VARGAS, JOSÉ MARIA (1786-1854), Venezuelan surgeon, research worker, patriot,and statesman; jailed and exiled by the Spaniards but later Presidentof the Republic.
WYMAN, WALTER (1848-1911), as Surgeon General of the U. S. Public HealthService and first Director of the Pan American Sanitary Bureau didmuch to establish public health on a national and international basis.
YNSFRÁN, FACUNDO D. (XIX cent.), Paraguayan sanitarian, founder of theDepartment of Health and of the School of Medicine.

PUBLICATIONS OF THE PAN AMERICAN SANITARY BUREAU
No. 1.-Prevención de las Enfermedades Transmisibles. 60 páginlas.
No. 3.-Higiene Pre-natal. 7 páginas.No. 5.-Ordenanza Modelo para Leche. 11 páginas.
No. 7.-Organización del Servicio (lde Sanidad Pública de los Estados Unidos. 26 páginas.
No. 9.-La Profilaxis del Bocio Endémico. 10 páginas.
No. 17.-Conservación de la Vista. 6 páginas.No. 19.-Colecta, Examenl e Identificación de las Pulgas Murinas. 11 páíginas.
No. 23.-lMeningitis Cerebroespinal Epidémica (Meningocócica). 4 páginas.
No. 25.-Amígdalas y Adenoides (Vegetaciones Adenoideas). 6 p:lginas.
No. 26.-Tifoidea: Sa Causa y Profilaxia 4 páginas.No. 30.-Tratailiento del Paludisimo. 4 páginas.
No. 36.-Noimenclatura Interíascionsal de las Cansas de Muerte. 16 páginas.
No. 37.-El Interrogatorio en el Diagnóstico Precoz de la Tubcrculusis Pulmuonar 3 páginas.
No. 43.-Código Sanitario Panamericano. 23 páginas.
No. 45.-.-La Declaración Obligatoria del Embarazo. 10 páginas.
No. 46.-La l)ifteria en el Trópico. 15 páginas.
No. 47.-Los Censos en Sanidad y en Epidemiología. 13 págiinas.
No. 48.-Higiene Cornltal parL el Pre-escolar. 5 páginales.
No. 49.-El Diagnóstico de la Fiebre Amnarilla. 14 páginas.
No. 50.-Acta Final, II Conferenciat Panamericana de Directores N:iciouiales de Saniidad 16 páginas.
No. 51.-Milk. 8 pages.
No. 52.--Souminay of Proecediíngs, 11 Pan Amrnericanu Confeeiince of N:stilal l)irectors of llealth 14
p:ages.No. 53.-Vacunación Antidiftérica. 8 pá:iginas.
No. 55.-A I.Lceta Anti-larvaria no Impaludismo. 6 págiiias.
No. 57.-Diagmióstico Retrospectivo (de la Fiebre Amariilla. 6 ¡)iígiias.
No. 58.--El Problema de la Aliientación eii el Uruguay. 9 paginas.
No. 61.-lrmmuizaciiS Profiláctica <le los Recié.n Naciils ceui BCG. 22 pgíinas.
No. 62.-- pideumiologia de la Lepra. 5 páginas.
No. 65.-La Iligienie Menital. 11 págiíías.
No. 70.-1)iagnóstico de la Tuberculosis. 6 páginlas.No. 82.-Narcomania. 46 páginas.No. 88.-Antirratización de los Buques. 40 páginas.
No. 90.-Control de las Enfermedades Transmisibles. 70 páginas.
No. 97.-Acta Final, Novena Conferencia Sanitaria Panamericana. 20 p:íginas.
No. 98.-El Problema de la Fiebre Amarilla en América. 10 páginas.
No. 9;.-Profilaxia de la Fiebre Amarilla. 6 páginas.
-No. 101.-Ninth Pan American Sanitary Conference. 8 pages
No. 102.-El Saneamiento del Suelo. 17 páginas.
No. 103.-Report of the Director of the Pan American Sanitary Bureau. 8 pages.
No. 104.-Profilaxia y dominio del paludismo. 24 páginas.
No. 105.-Fumigación de buques. 14 páginas.
No. 106.-Snake-Bites. 10 pages.No. 108.-Las Repúblicas Americanas ante las Convenciones Internacionales de Sanidad 5 páginas.
No. 109.-La Lucha Antivenérea. 27 páginas.
No. IíO.-Third Pan American Conference of National Directois of Healthi-Summary of Proceedings.
10 pages.
No. 111.-Venenos Antirrata. 4 páginas.
No. 112.-Tratamiento Anti-Leprotico. 14 páginas.
No. 113.-Pautas de Organización Sanitaria. 12 páginas.
No. 118.-Servico de Peste. 6 paginás.
No. 121.-Actas de la Tercera Conferencia Panamericana de Directores Nacionales de Sanidad.
396 páginas.
No 125.-Pautas para Abastos de Agua. 16 páginas.
No. 126.-Décima Conferencia Sanitaria Panamericana, Acta Final. 20 paginas.
No. 127. -Lepra: Epidemiología-Clasificación-Tratamieito. 17 páginas.
No. 128.-A Classificavao da Lepra. 5 páginas.
No. 129.-Final Act: Tenth Pan American Sanitary Conference. 13 pages.
No. 130.-Dixiéme Conference Sanitaire Panaméricaine: Acte Final. 20 pages.
No. 131.-X Conferéncia Sanitária Panamericana: Ata Final. 12 páginas.
No. 132.-Modelos de Certificados de Defunción, de Nacimiento Viable, y de Defunción Fetal. 4 pá-
ginas.
No. 133.-Tenth Pan American Sanitary Conference. 14 pages.
No. 134.-Los Preventorios en la Lepra. 8 páginas.No. 135.-Proyecto de Escalafón Sanitario. 12 páginas.
No. 136.-Actas de la Décima Conferencia Sanitaria Panamericana. 941 páginas.
No. 137.-Nomenclatura Internacional de las Causas de Muerte. 25 páginas.
No. 138.-La Enfermería Sanitaria. 10 páginas.
No. 139.-Mate. 8 pages.No. 140.-Alimentación. 22 páginas.
No. 141.-Sociedades e Instituciones Científicas de la América Latina (Scientific Societies and Instittl-
tions in Latin America). 50 páginas.
No. 142.-Demografía de las Repúblicas Americanas. 16 páginas.
No. 143.--Educación Sexual Destinada a los Padres. 9 páginas.
No. 144.-Estudio de Ciertas Cuestiones Relativas a las Vitaminas. 14 páginas.
No. 145.-Lo que Debemos Saber sobre Cáncer. 6 páginas.
No. 146.-A las Madres. 2 páginas.No. 147.-IV Conferencia Panamericana de Directores Nacionales de Sanidad: Acta Final. 9 páginas.
No. 148.-The Pan American Sanitary Bureau and its Cooperative Work in the Improvement of Milk
Supplies. 4 pages.No. 149.-Half a Century of Medical and Public Health Progress. 20 pages.
No. 150.-Medio Siglo de Adelanto en Medicina y Sanidad. 22 páginas.
No. 151.-IV Pan American Conference of National Directors of Health (Final Act). 8 pages.
No. 152.-Medical and Publio Health Journals of Latin America (Revistas de Medicina y Sanidad
de la América Latina). 51 páginas.
No. 153.-Annual Report of the Director of the Pan American Sanitary Bureau: 1939-1940. 34 pages
No. 154.-Reacción a la tuberculina. 6 páginas.
No. 155.-Informe Anual del Director de la Oficina Sanitaria Panamericana: 1939 1940. 39 páginas.
No. 156.-Pan American Public Health Quiz. 14 pages.
No. 157.-Epitome del Segundo Suplemento (1939) de la Farmacopea E.U. XI. 20 páginas.
No. 158.-Public Health and Medicine iii Stamps of the Americas. 7 pages.
No. 159.-Some Pan American Pioneers iii Public Health. 5 pages.
No. 160.-Scientific Institutions in Latin America: Part I. 47 pages.
No. 161.-Indices Sanitarios Panamericanos. 3 páginas.
No. 162.-IV Conferencia Panamericana de Directores Nacionales de Sanidad: Resumen de sus
labores. 29 páginas.No. 163.-Huertos escolares. 7 páginas.
No. 164.-Clave diagnóstica para la clasificación en columna (tabulación) de las causas de morbidad.
18 páginas.No. 165.-Contribuciones al estudio de la peste bubónica en el nordeste del Brasil. 331 páginas.
No. 166.-Health and Living Conditions in Latin America. 11 pages.
No. 167.-The Work of the Pan American Sanitary Buieau in Relation to Clhild Welfare. 4 pages.
No. 168.-La enseñanza médica en Estados Unidos. 22 páginas.
No. 169.-El lanzallamas en la lucha antipestosa. 9 páginas.
No. 170.-El entierro de la basura bajo un recubrimiento eficaz en Cristóbal. Zorna del Canal. 11
páginas.
No. 171.-Fourth Pan American Conference of National Directors of Health: Resumé. 26 pages.
No. 172.-Pautas mínimas para el saneamiento de las minas del Perú en lo relativo a viviendas. 8
páginas.No. 173.-La fiebre amarilla en las Américas. 15 páginas.
No. 174.-Diagnóstico y tratamiento de ciertas afecciones de los tropicos. 12 páginas.
No. 175.-Housing and Hospital Projects of Latin American Social Security Systems. 15 pages.
No. 176.-Annu al Report of the Director of the Pan American Sanitary Bureau: 1940-1941. 39 pages.
No. 177.-Public Health in the Americas. 70 pages.
Adresser toutes les demandes a M. le Directeur de l'Office Sanitaire Panaméricain.
Diirjanse todos los pedidos al Director de la Oficina Sanitaria Panamericana.
Todos os pedidos devem ser enderecados ao Diretor da RepartiQao Sanitária Panamericana
Address all requcests for publications to the Director of the Pan American Sanitary Bsureau.

THE PAN AMERICAN SANITARY BUREAU is an independent internationalpublic healthorganization. Itwas created bythe Second InternationalAmer-
ican Conference (1901-1902), organized by the First Pan American SanitaryConference (1902), and reorganized by the Sixth (1920). It is governed by aDirecting Council elected, together with the Director, at each Pan AmericanSanitary Conference, and supported by annual quotas contributed pro rata by allthe American Republics. The Bureau is interested primarily in the preventionof the international spread of communicable diseases, and also in the maintenanceand improvement of the health of the people of the 21 American Republics. Underthe provisions of the Pan American Sanitary Code (1924), it has become the centerof coordination and information in the field of public health, in the AmericanRepublics. It also acts as a consulting body at the request of national healthauthorities, carries on epidemiological and scientific studies, and publishes amonthly Bulletin, as well as other educational material. Pan American HealthDay is celebrated annually on December 2 in all American Republics. Addressall correspondence to the Director of the Pan American Sanitary Bureau, Wash-ington, D.C.