public health advocacy
DESCRIPTION
Public Health Advocacy. Causes of ill-health: the risk factor reduction!. Smoking - education, cessation supports, etc Alcohol - education, sensible/safe limits, etc Exercise - education, advise, etc Nutrition – education, Diet, the pyramid, etc - PowerPoint PPT PresentationTRANSCRIPT

F Howell, TCD 2009/2010 1
Public Health Advocacy

F Howell, TCD 2009/2010 2
Causes of ill-health: the risk factor reduction!
• Smoking - education, cessation supports, etc
• Alcohol - education, sensible/safe limits, etc
• Exercise - education, advise, etc
• Nutrition – education, Diet, the pyramid, etc
• RTA’s - education, driving schools, speed limits
• Etc etc etc etc
F Howell, TCD 2009/2010 3
Market justice orientation(1)
• Rugged individualism
• Self - determination
• Strong individual control/responsibility
• Limited individual obligation to the collective good
• Limited government involvement in social activity

F Howell, TCD 2009/2010 4
Market justice orientation (2)
• People act in their own best interest
• Assume risks knowingly and voluntarily
• Biological predisposition to illness
• Personal responsibility
• Blame the victim
F Howell, TCD 2009/2010 5
Blaming the victim
• Problems are as a result of unusual events/circumstances
• They are exceptional rather than universal
• Jogger - Central Park - New York
• Personal responsibility - the ENTIRE solution
• Victims are “others”

F Howell, TCD 2009/2010 6
Public Health Advocacy
Advocacy is a catch-all word for the set of skills used to create a shift in public opinion and mobilise the necessary resources and forces to support an issue, policy or constituency.
Advocacy is not just about lobbying Advocacy can be part of your day job!
F Howell, TCD 2009/2010 7
Public Health Advocacy
Refers to the process of overcoming major STRUCTURAL barriers as opposed to INDIVIDUAL barriers to Public Health goals.
Advocacy seeks to increase the power of people and groups and to make institutions more responsive to human needs.
F Howell, TCD 2009/2010 8
Types of Barriers
Political philosophies that devalue health and quality of life at the expense of economic outcomes
Political or bureaucratic opposition or inertia to health promoting legislative provisions
Political or bureaucratic opposition to the participation of consumers in healthcare planning
Marketing of unsafe and unhealthy products
F Howell, TCD 2009/2010 9
Targets of Advocacy
Policies and practices of Governments and Institutions
Government laws and regulations Commercial marketing practices of
industries Activities of counter health lobbying
groups

F Howell, TCD 2009/2010 10
Being an Advocate
Advocacy is an integral part of any prevention strategy
It is issue and policy orientated It is not primarily about changing
individuals behaviour
Upstream/downstream

F Howell, TCD 2009/2010 11
Key issues to consider• The use of evidence
• Using data to support argument
• Setting targets – short to long term
• Power assessment
• Tactics
• Continuous evaluation
• Media Advocacy

F Howell, TCD 2009/2010 12
Evidence is crucial
• Supported by systematic empirical evidence• Supported by cogent argument• Scale of likely health benefit• Likelihood that policy would bring benefits other than
health benefits• Fit with existing or proposed government policy• Possibility that the policy might do harm• Ease of implementation• Cost of implementation
F Howell, TCD 2009/2010 13
Data are importantstrong and credible data basegives a clear analysis of the issues
to be addressedbe user friendly with the data
Health policies can be made in the absence of evidence, or despite evidence

F Howell, TCD 2009/2010 14
“Targets”
Goal setting is criticalsense of direction, unifying theme,
end point long range - short termwhat steps are needed to achieve
each goalhelps long term thinking and focuses
on the real issues
F Howell, TCD 2009/2010 15
Advocacy can be threatening “If there is no struggle there is no
progress. Power concedes nothing without a demand.”
challenges staid notions, vested interests upstream forces might not like it
Advocacy requires assessment what about your own organisational health can I win, can we afford to lose assess assets and liabilities and plan
strategies building broad, cohesive coalitions
- resources, strengths and weaknesses.

F Howell, TCD 2009/2010 16
Professor Ivan Perry, UCC
Irish Indep 29 Oct, ’03
F Howell, TCD 2009/2010 17
The media connection
In our “mass-mediated” democracy public health battles are fought not only in the clinics and the courts, but also on the 10pm news, the front pages, financial section and even on 24 hour all talk radio
The mass media constitute an important part of the environment in which the selection, presentation, definition and discussion of public issues occur

F Howell, TCD 2009/2010 18
Media advocacy
Seeks to influence the selection of topics by the mass media and shape the debate about these topics
Ensures that the story is told from a public health perspective
If you don’t exist in the media, for all practical purposes you don’t exist

F Howell, TCD 2009/2010 19
Understanding media advocacy More an art than a science
Improves with practice understand the needs of journalists set media objectives that relate to your
goals be on the alert for stories that help your
issue Never do anything that would
compromise your credibility

F Howell, TCD 2009/2010 20
Case study
Smoke-free Irish Workplaces, Including Bars.

F Howell, TCD 2009/2010 21
Key issues• Smoke-free workplaces introduced 29th March 2004
• Campaign did not start on the 28th March 2004
• Capacity building for years
• Part of a comprehensive tobacco control package – – price, advertising, sales to children, tar and nicotine levels etc
F Howell, TCD 2009/2010 22
The 70s
• Active smoking harmful
• Smokers’ rights universal
• Environmental tobacco smoke (ETS), passive smoking, involuntary smoking – what is that?

F Howell, TCD 2009/2010 23
Environmental tobacco smoke- is it bad for you?• For the moment most, but
not all, the pressure to have the right to breathe smoke-free air must be based on aesthetic considerations rather than on known serious risks to health.
Editorial, BMJ, 1976.
Excuse me, Do you mind if I smoke?
No, only if you don’t mind if I fart

F Howell, TCD 2009/2010 24
The 80s
• Increasing awareness of tobacco control issues
• Advertising bans
• Health warnings on packs
• Sales to children
• ETS – could it be bad for you?
F Howell, TCD 2009/2010 25
Passive smoking – the evidence emerges
• 1982 - US Surgeon General. The health consequences of smoking: cancer.
– Reviewed 3 studies showing an increased risk of lung cancer in non-smoking women whose husbands smoked
– Conclusion - cautious
• 1986 - US Surgeon General. The health consequences of involuntary smoking.
– Reviewed 13 spousal studies
– Conclusion: Involuntary smoking is a cause of disease including lung cancer, in healthy non-smokers.

F Howell, TCD 2009/2010 26
• 1986 - US National Research Council. Environmental tobacco smoke: Measuring exposures and assessing health effects.
• 1986 - IARC. IARC monographs on the evaluation of of the carcinogenic risk of chemicals to humans: tobacco smoking.
• 1986 - UK DHSS. Fourth report of the independent scientific committee on smoking and health.
• 1986 - Australian NHMRC. Effects of passive smoking on health.
F Howell, TCD 2009/2010 27
The 90s• Increasing awareness of
adverse health effects of ETS
– Irrevocably changed balance of smokers’ rights versus non smokers’ rights
• Irish Legislation• Restrict consumption (non
smoking areas) in specified locationse.g. Public offices, schools, colleges, cinemas, theatres, taxis, health and child care facilities, “restaurants”
• Voluntary code for the workplace
F Howell, TCD 2009/2010 28
Further “action”
– Minister for Health Consultative Committee 1992• Employers/unions/officials
– Recommended Voluntary Code of Practice on Smoking in the Workplace
– Employers to be proactive– Published “Clean Air at Work”– Circulate it– Review in 12 months
F Howell, TCD 2009/2010 29
ASH Ireland• 1991-1992 – Irish Heart Foundation +Irish Cancer Society
discussion re tobacco control
• 1992 - ASH Ireland founded by IHF+ICS
• Admin Support (Ms Valerie Coghlan)• PR Support
• Advocacy for tobacco control– Media driven!
• Mission - ASH Ireland, in pursuance of a tobacco free society, aims to reduce the toll of disease, disability and death caused by tobacco use.
F Howell, TCD 2009/2010 30
1994 - Review of the effectiveness of the 1992 voluntary code
• Restructured Consultative Committee– Only 1,200 copies sent to employers– Poor awareness of the Code
• Recommend continue voluntary code as against legislation
• Further review in 2 years• Revised code of practice • Endorsed by employers/trade unions• Circulate widely

F Howell, TCD 2009/2010 31
Further action• 1994 Health Strategy: Shaping a healthier future
– Extend environmental controls over tobacco, especially those in the workplace
• 1995 Regulations extend places where smoking banned– Child care facilities /All Health care premises– Bingo/Bridge/Snooker – Public areas in retail financial agencies, Banks etc– Public areas in hairdressing salons/barber shops– Taxis and hackneys, aircraft/ferries– 50% of seating in restaurantWorkplaces still excluded!
F Howell, TCD 2009/2010 32

F Howell, TCD 2009/2010 33
…..As the evidence grew …the lobbying continued
• Issue focused as a health and safety issue• For all workplaces, including bars• Reach for the unreachable ? – deliberate strategy
• Not a consumer protection issue• Not a smoking reduction issue
• Politicians, public servants, trade unions targeted• Constant media linkage• International Research highlighted• International developments highlighted
– California, Canada, Australia, Finland

F Howell, TCD 2009/2010 34

F Howell, TCD 2009/2010 35
Outcome…..end of the 90s/start of the 2000
Parliamentary Enquiry 1999• Joint Oireachtas (Parliament)
Committee on Health and Children (multi- party)
• Heard evidence from wide range of groups: – Minister’s officials– European Commissioner– Public servants– NGOs– Tobacco Industry– Academics
F Howell, TCD 2009/2010 36
Parliamentary Enquiry 1999
• Rejected tobacco industry insistence that ETS not harmful to non smokers
• Recommended new national anti-smoking strategy, many far-reaching initiatives, including– Restrictions on workplace, including bars– New unit to deal solely with tobacco control issues
F Howell, TCD 2009/2010 37
• 2000 DOHC Report : Towards a tobacco free society– Recommended ban on smoking in workplaces, except bars– Establish Office of Tobacco Control (NB)
• 2000 June– Complete ban on tobacco advertising in print media came into
force• 2001 Joint Committee on Health and Children
– Reaffirms recommendation on ban on smoking in all workplaces• 2001 – The Public Health (Tobacco) Bill 2001,
– The provisions in the Bill allow the Minister for Health and Children to prohibit smoking in all places, including the workplace, by way of regulation.
– Allows the establishment of the Office of Tobacco Control

F Howell, TCD 2009/2010 38
Next steps…………build capacity
• Feb 02 –OTC Conference – specifically on passive smoke
– International Experts/ICTU/HSA involved– James Repace “……. Based on this study and my
own studies of the effects of ETS on such workers in Hong Kong and Boston, I would estimate that approximately 150 bar workers a year in Ireland will die from ill health caused by ETS."

F Howell, TCD 2009/2010 39

F Howell, TCD 2009/2010 40
Pressure from the lobbying front……………
• ASH Ireland concerned about silence from Health and Safety Authority
• ASH Ireland sends a series of FOI requests to Health and Safety Authority
• Evidence emerges that their Board (IBEC/ICTU reps) not very proactive on the issue
• Direct approach to Minister in charge, Mr. Tom Kitt TD
• He asks HSA to examine the possibility of banning smoking in workplace
F Howell, TCD 2009/2010 41
How extensive should workplace restrictions be?
• Health and Safety Authority (HSA) & OTC jointly commissioned independent scientists to review evidence on ETS.
• Chair Dr Shane Allwright, • Terms of reference
“To identify and report on the degree of consensus that exists among leading scientific authorities on the question of the hazard and risk posed by environmental tobacco smoke to human health in the workplace.”

F Howell, TCD 2009/2010 42
…………….. and
• June 2002 – IARC has concluded that involuntary smoking is carcinogenic to humans (Group 1).
• Nov 02 – Minister suggestions– Complete ban in workplaces/restaurants– Partial ban in pubs – when food served and to have specific
no-smoking areas
F Howell, TCD 2009/2010 43
and as a result…………………….
• Ridiculed by Vintners
• Bar workers trade unions furious!
• Opposition politicians go on the attack!
• NGO Community lobby harder!!And then……………………..

F Howell, TCD 2009/2010 44
Authors concluded
• ETS cause heart disease cancer and respiratory probs
• Employees need to be protected
•Ventilation is ineffective
•Legislative measures are required
30 th January 2003
Allwright Report
F Howell, TCD 2009/2010 45
What happened next……….
• Publicans condemned the Government's decision to announce a ban on smoking in all licensed premises from January 1st next.
• Unnecessary, unworkable, unenforceable
• 15 months of “fun”
F Howell, TCD 2009/2010 46
Anti-ban side• Bar owners – economic impact, compromise
proposals, ventilation• Employers organisation supported bar owners• Some senior Ministers tried to jump ship• Enstrom Kabatt study• Death of bar worker in New York• Tobacco industry intervention (minimal)• ++++

F Howell, TCD 2009/2010 47
Proposed Ban on Smoking in the WorkplaceDraft Tri-partite Position Statement (11th July 2003)
(and a cast of thousands!)
F Howell, TCD 2009/2010 48
Public Health Advocacy Campaign
If you don’t exist in the media, for all practical purposes you don’t exist
• Letters to the national papers
• National Radio
• Local Radio
• Sunday features
• Chat shows
• TV shows
• Etc etc
Anytime, anyplace, anywhere!
F Howell, TCD 2009/2010 49
Simple messages repeated +++• Health and Safety issue• ETS is a serious cause of ill health• All workers deserve protection• Ventilation does not work• Separate areas do not work• Smokers are reasonable• Provide assistance to help them quit if they wish to
• Not a consumer protection issue• Not a smoking cessation issue• Not a tobacco control issue

F Howell, TCD 2009/2010 50
OFFICE OF TOBACCO CONTROL
• Montague Communications have won a PR Excellence Award for our management of the Office of Tobacco Control's campaign to build public compliance with the smoke-free workplace legislation

F Howell, TCD 2009/2010 51
Irish Times, Oct 16, ’03

F Howell, TCD 2009/2010 52
Other helpers………• Trade union Movement• Health care professionals• Boston experience as against California• Minister for Health and Children visits New York• Political opposition previously tied in -‘silenced’• DOHC “Every cigarette is doing you damage” campaign• DOHC “Smoker’s quit line”• CMO Support• International tobacco control community• ++++++++++…………………………..
F Howell, TCD 2009/2010 53
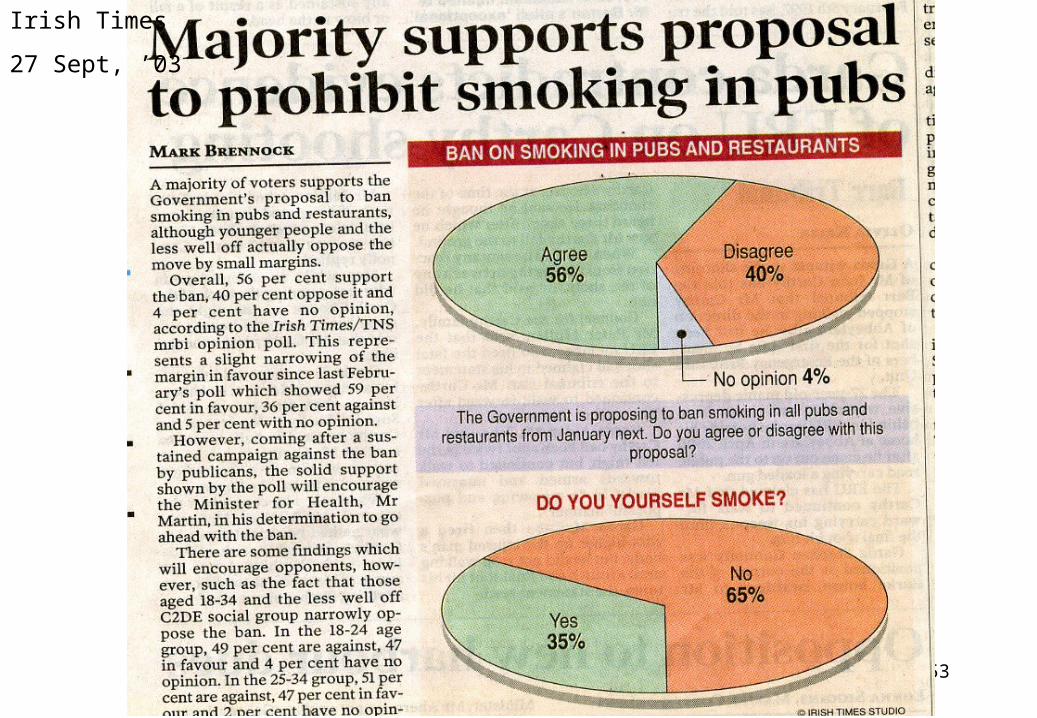
Irish Times
27 Sept, ’03

F Howell, TCD 2009/2010 54
March 29th 2004
The big day………………………what would happen??

F Howell, TCD 2009/2010 55
The Broadsheets Editorials
F Howell, TCD 2009/2010 56
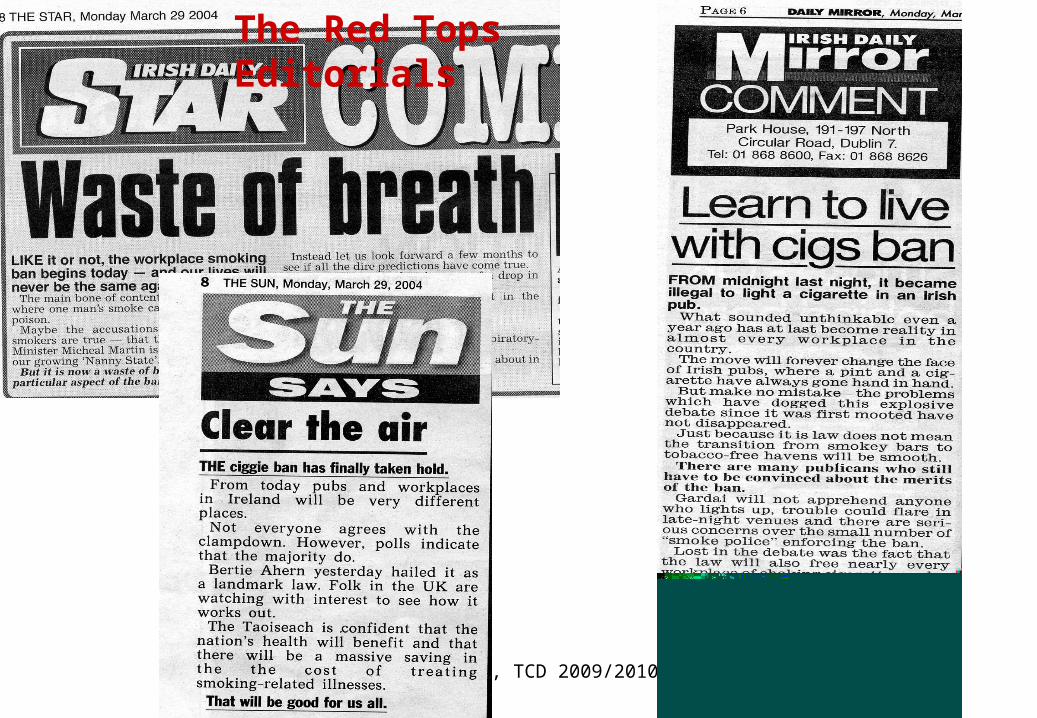
The Red Tops Editorials

F Howell, TCD 2009/2010 57
F Howell, TCD 2009/2010 58
Implementation of ban• Resounding and astonishing success - so far• Almost universal compliance, rural and urban• Self enforcing + Enforcement Officers• Media support
– Supportive editorials in both broadsheets and tabloids
• Bar owners –some angry, some not• Smokers
– Some angry– Opportunity to give up– Smoking less

F Howell, TCD 2009/2010 59

F Howell, TCD 2009/2010 60
High degree of public support• 93% think the law was a good idea, including
80% of smokers
• 96% of people feel the law is successful, including 89% of smokers
• 98% believe that workplaces are healthier, including 94% of smokers
• RTE New Year Poll 2004 – How was it for you?– Smoke-free law voted the no 1 high of 2004
F Howell, TCD 2009/2010 61
Compliance is very high
• 93% of all hospitality premises inspected were smoke free
• 92% of non hospitality sector were smoke free
• 96% of all indoor workers report working in smoke-free areas since the ban

F Howell, TCD 2009/2010 62
Why so successful?• Check back with New York and Boston • Keep the message simple !• 15th Month media debate • Most smokers don’t want to be smokers• Opportunity to quit• Most smokers are reasonable• Silent majority non-smokers, biding time• Onus on employer/owner to enforce• Most people are law abiding
F Howell, TCD 2009/2010 63
F Howell, TCD 2009/2010 64
Understanding advocacy
Governments/Institutions adopt policies in a climate of public readiness
Public health advocates need to shift public opinion in the right direction
Political action becomes compellingPolitical inaction becomes a liability

F Howell, TCD 2009/2010 65
Ireland Smokefree!