public health 2030: a scenario exploration supported by grants from:
TRANSCRIPT

Public Health 2030:A Scenario Exploration
Supported by grants from:

Introduction
• Public Health is “what we as a society collectively do to ensure the conditions for people to be healthy.”
• The Who, What, and How of public health is evolving – not always in consistent directions.
• Scenarios all exploring the factors shaping public health, and public health’s actions to consider alternative paths into the future.
2
The Public Health 2030 ProjectFunded by Robert Wood Johnson & Kresge Foundations following scenarios on Vulnerability 2030, Primary Care 2025 , and Health and Health Care 2032
• Explore key forces shaping public health
• Consider the future of public health functions, financing and sustainability
• Build expectable, challenging, and visionary scenarios that facilitate preparation, imagination, and aspiration
• Provide and widely distribute the scenarios as a tool for public health agencies, organizations, and schools
3
Developing the Scenarios
• Considered key drivers shaping public health• Developed expectable, challenging, and
aspirational forecasts for the drivers• Interviewed experts, Project advisers• Developed and used state and local Public
Health 2030 Scenarios• Developed national Public Health 2030 Scenarios
4
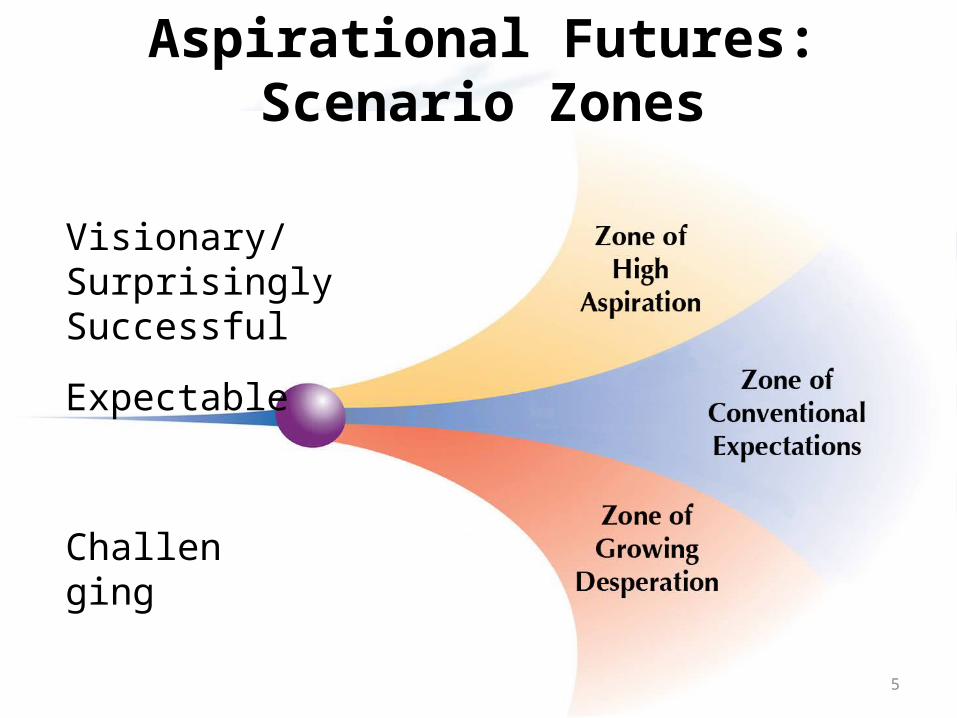
Aspirational Futures: Scenario Zones
Visionary/Surprisingly Successful
Expectable
Challenging
5

Public Health 2030: State & Local Scenarios
• Fargo Cass Public Health (ND)
• Boston Public Health Commission (MA)
• Cuyahoga County Board of Health (OH)
• Virginia Department of Health
6
National Public Health 2030 Scenarios
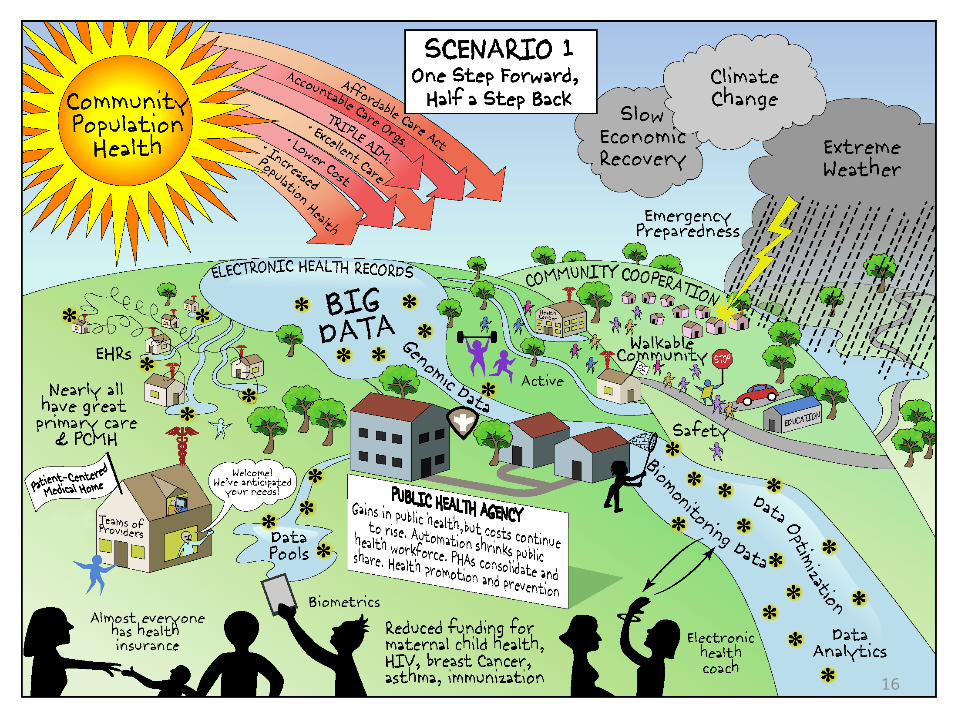
Scenario 1: One Step Forward, Half a Step BackSignificant advances in big data analytics, in access to and quality of health care; yet recurring fiscal and health challenges for communities and PHAs.
Scenario 2: Overwhelmed, Under-ResourcedEconomic and environmental challenges, infectious diseases increase, health care reform halted, public health constrained.
Scenario 3: Sea Change for Health EquityPHAs evolve into health development agencies. Economic stability and value and policy shifts toward equity support this evolution.
Scenario 4: Community-Driven Health and EquityInnovation in communities, alternative economics, transformation is accelerated through technology and recognition of economic and social injustice.
7
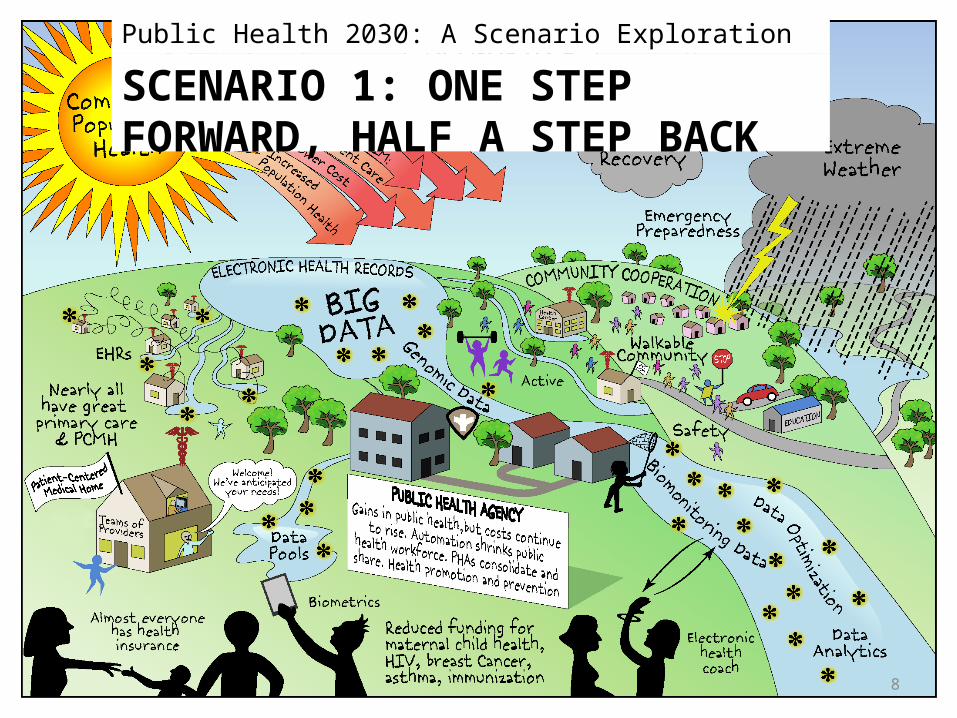
SCENARIO 1: ONE STEP FORWARD, HALF A STEP BACK
Public Health 2030: A Scenario Exploration
8
Scenario 1: One Step Forward, Half a Step Back
• Public health agencies (PHAs) advance capabilities in technology and big data analytics
• Public health is restrained by – High costs of health care – Variations in PHAs’ technological capabilities,
funding, services, and effectiveness
9
• Public health funding varies widely; Federal funding for health care programs reduced as access to health care improves– PHAs refocus on prevention and
improving community conditions
• PHAs consolidate and share services; most improve comparability and show positive returns on investment (ROI)
Scenario 1: One Step Forward, Half a Step Back
10
• Emergence of Big Data
• Improved surveillance and analysis
• PHAs provide quality control, and some “nudge” social networks toward better health
Scenario 1: One Step Forward, Half a Step Back
11
• When possible, PHAs– Automate inspections– Enhance population health monitoring– Improve emergency preparedness
• Some PHAs are confined to mandated services• Others are able to emphasize prevention
Scenario 1: One Step Forward, Half a Step Back
12

• More extreme weather events (EWEs) and vector-borne infections– E.g. Lyme disease and
dengue fever
• PHAs use simulations and gamification to prepare communities for emergencies
Scenario 1: One Step Forward, Half a Step Back
13
Triple Aim
Electronic Health
Records (EHRs)
• Health care reform largely implemented
• Expansion of Accountable Care Organizations (ACOs), Triple Aim, and Patient-Centered Medical Homes (PCMH)
• Care improved by knowledge technologies – Doc Watson, digital health coach
• PHAs focus on prevention, have varying roles with ACOs
Scenario 1: One Step Forward, Half a Step Back
14
Scenario 1: One Step Forward, Half a Step Back
• Health care costs continue to rise as access improves
• Social determinants not addressed
• No “game-changers”
• Continued disparities
15
16
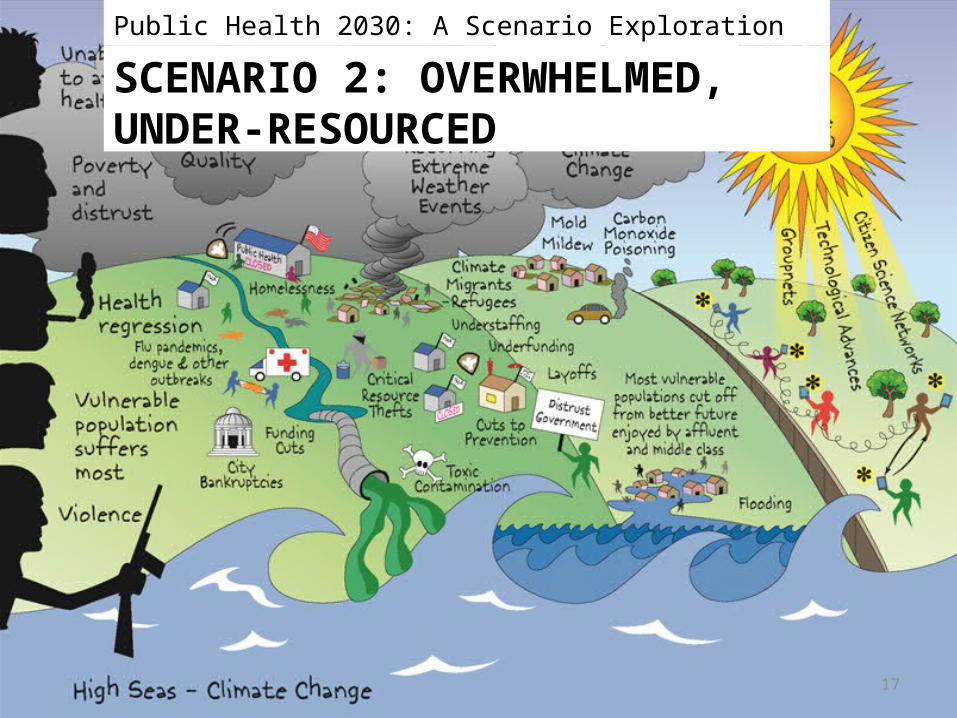
SCENARIO 2: OVERWHELMED, UNDER-RESOURCED
Public Health 2030: A Scenario Exploration
17

• Severe recessions in 2016 and 2023
• PHA funding reduced, many programs eliminated
Scenario 2: Overwhelmed, Under-Resourced
18

• PHAs blamed for lack of preparation and ineffective responses
• Public distrusts PHAs, federal government in general, and health care
Scenario 2: Overwhelmed, Under-Resourced
19

• Distrust grows, people refuse to get flu shots
• Highly virulent flu strain in 2020• Tens of thousands of people die
Scenario 2: Overwhelmed, Under-Resourced
20

• Citizen science and technology grow but serve affluent and reinforce disparities.
• PHA health care services cut while need grows.
• Excellent, personalized care for those who can afford it.
• Innovative private sector approaches to health for those who can afford them.
Scenario 2: Overwhelmed, Under-Resourced
21
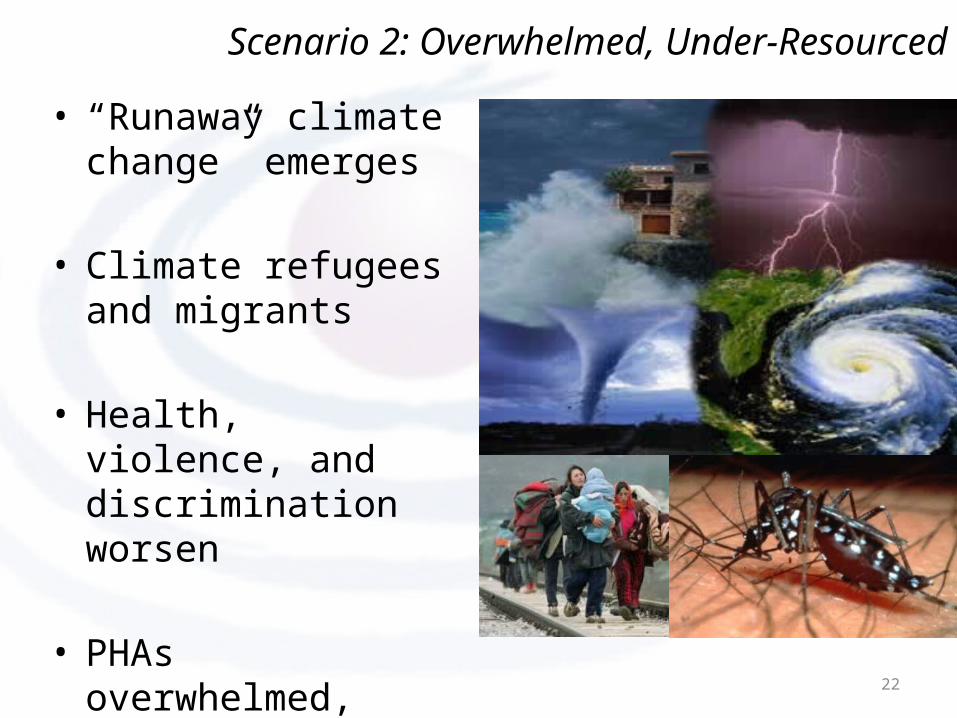
• “Runaway climate change” emerges
• Climate refugees and migrants
• Health, violence, and discrimination worsen
• PHAs overwhelmed, struggle to recover
Scenario 2: Overwhelmed, Under-Resourced
22

• PHAs understaffed, overwhelmed.
• Many universities shut down public health programs.
• Private sector innovations ignore disparities and vulnerability.
• Worsening disparities in health, quality health care access, effective prevention, and other public health services.
Scenario 2: Overwhelmed, Under-Resourced
23

24

SCENARIO 3: SEA CHANGE FOR HEALTH EQUITY
Public Health 2030: A Scenario Exploration
25
• Changes in values and demographics. • Funding improves for public health. • Public health pursues advanced analytics,
gamification, and multisectoral partnerships.• Improvements in housing, economic
opportunity, education, and other social determinants of health.
• Some disparities persist.• But in 2030, the vast majority of Americans
have attained greater opportunity for good health.
Scenario 3: Sea Change for Health Equity
26

• Support for “common sense” policy• Public support for opportunity, equity, and
fairness in policies and economics– National minimum wage, Health in All Policies
• Innovation and use of new tech for outcomes
Scenario 3: Sea Change for Health Equity
27
• Public health funding improves
• Economies gradually grow, reduce fiscal strains and cuts
• PHAs foster additional resources from business, foundations, ACOs
• Evaluations show positive ROI
• Congress restores Prevention Fund restored to $2B level in 2020, add 2% tax in 2022 on medical services
Scenario 3: Sea Change for Health Equity
28
• PHAs become chief health strategists, shift away from direct services
• Collaborative networks and partnerships
• Simulations, forecasts, analyses
• Spread best practices• Identify most cost-
effective and appropriate providers
Scenario 3: Sea Change for Health Equity
29
• Gaming changes communities’ awareness of and commitment to achieving health
• New tech developments are made to be affordable and culturally appropriate
• PHAs lead coalitions, recognized by the public has chief health strategists
Scenario 3: Sea Change for Health Equity
30
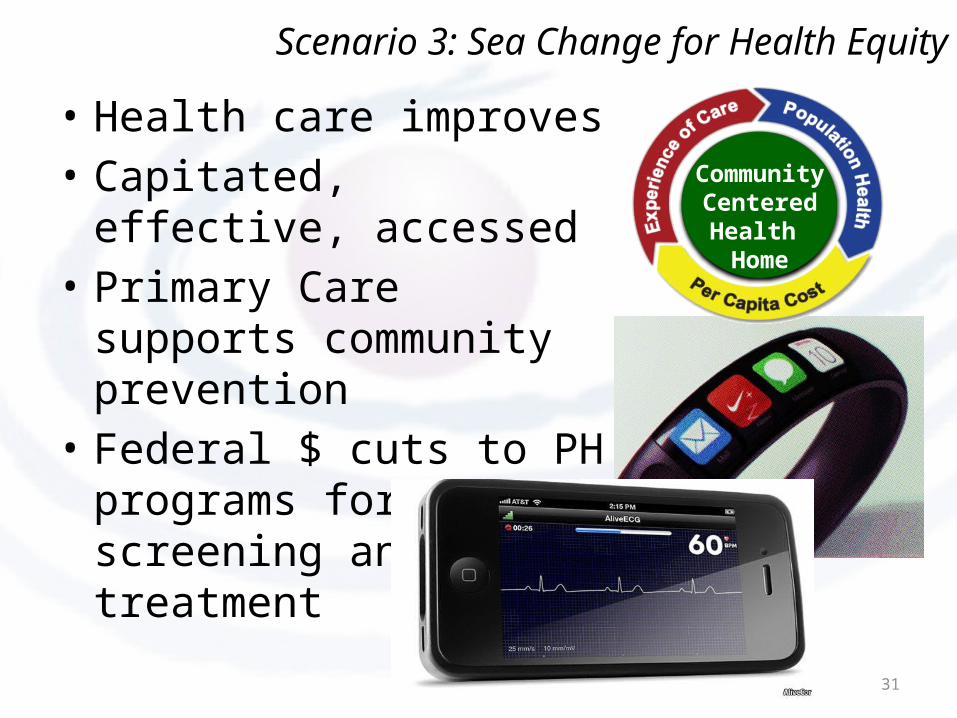
• Health care improves• Capitated, effective, accessed• Primary Care supports
community prevention• Federal $ cuts to PH
programs for screening and treatment
Community Centered Health Home
Scenario 3: Sea Change for Health Equity
31

By 2030,• Better health and health equity, less demand
for health care• Improved community conditions, esp. for low
income communities
Scenario 3: Sea Change for Health Equity
32

33
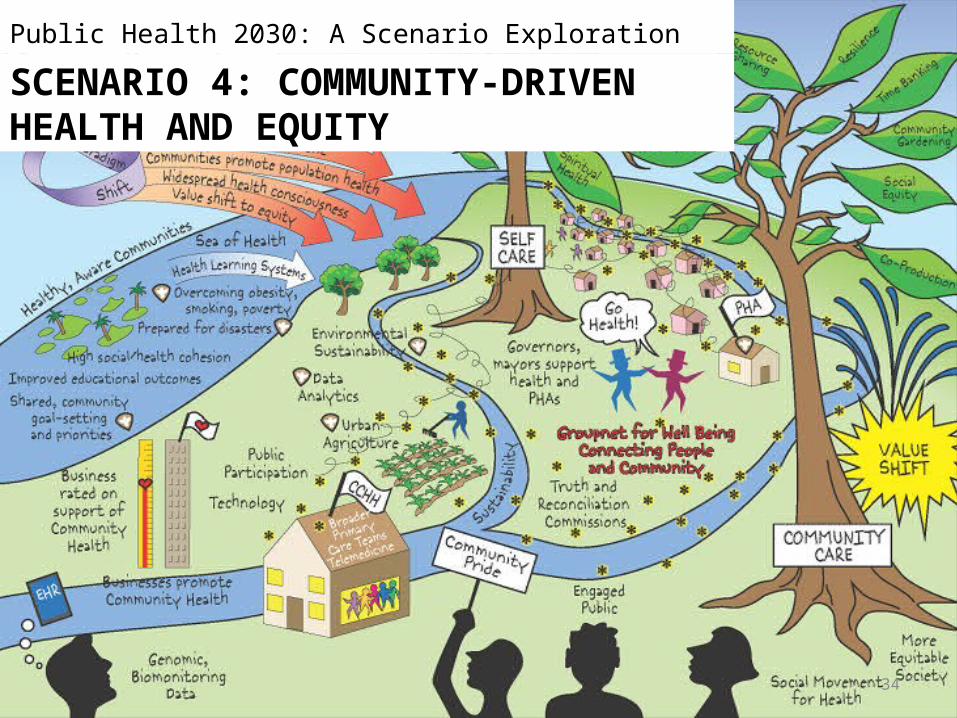
SCENARIO 4: COMMUNITY-DRIVEN HEALTH AND EQUITY
Public Health 2030: A Scenario Exploration
34
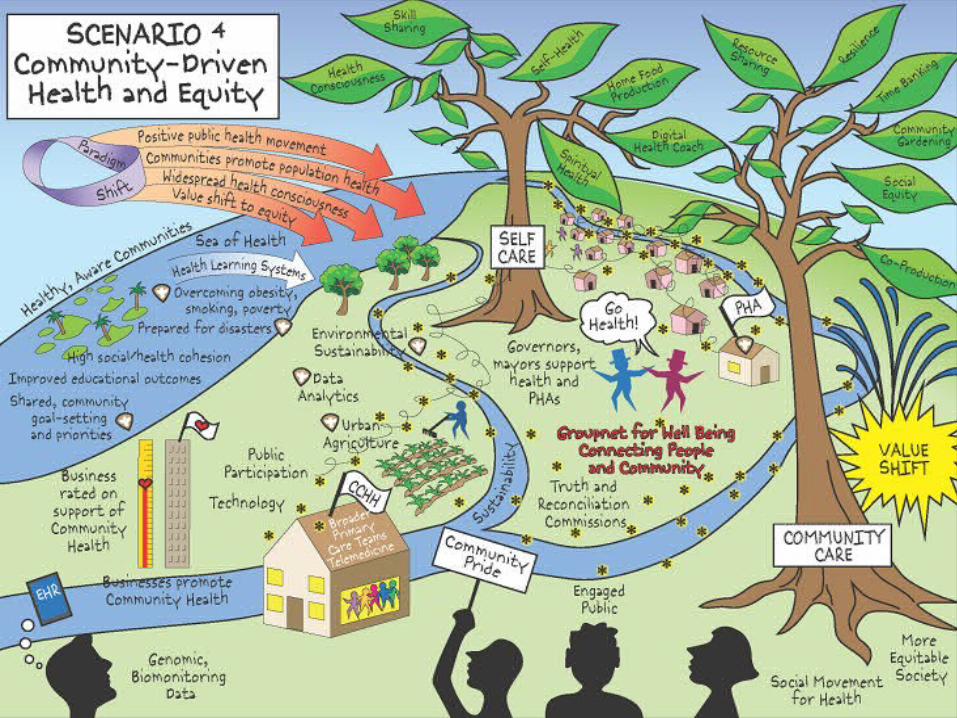
• Health improvement initiatives coalesce via technology and networks into a broad, national public health infrastructure.
• Value shift to equity was accelerated by another major recession and economic transformation.
• The nation tries to come to terms with its racial and socioeconomic histories, and tries to create a more equitable society.
• Public health sheds many functions and facilitates these movements to improve health.
Scenario 4: Community-Driven Health and Equity
35

• Groupnets used to improve behavioral health at the micro-level, often through “peer uplift”
• Community activity & organizations focused on health
• PHAs lead on information quality & community facilitation
Scenario 4: Community-Driven Health and Equity
36

• Health records integrated with other personal and community data to allow advanced health analysis and targeting
• Community health learning systems enhance PHAs’ roles as facilitators and health strategists
• Games and simulations improve community engagement and planning
Scenario 4: Community-Driven Health and Equity
37
• Environmental Health evolves
• PHAs work with communities, and partners to reduce environmental impact and expand renewable energy.
• Highly effective pre-event resilience games and simulations for Extreme Weather Events.
Scenario 4: Community-Driven Health and Equity
38
• Governments spend less and spend “smarter”• Unemployment accelerates shift to alternative
economics/new community economic models
Scenario 4: Community-Driven Health and Equity
39

• Economic and social justice movement progressed
• “Truth and Reconciliation” processes spread
• New legislation promotes social and economic fairness
Scenario 4: Community-Driven Health and Equity
40

• Public health graduates are trained for community engagement and advanced analytics
• PHAs serve as effective chief health strategists
• Disparities are reduced and the nation is largely unified in seeking to eliminate them
Scenario 4: Community-Driven Health and Equity
41
42
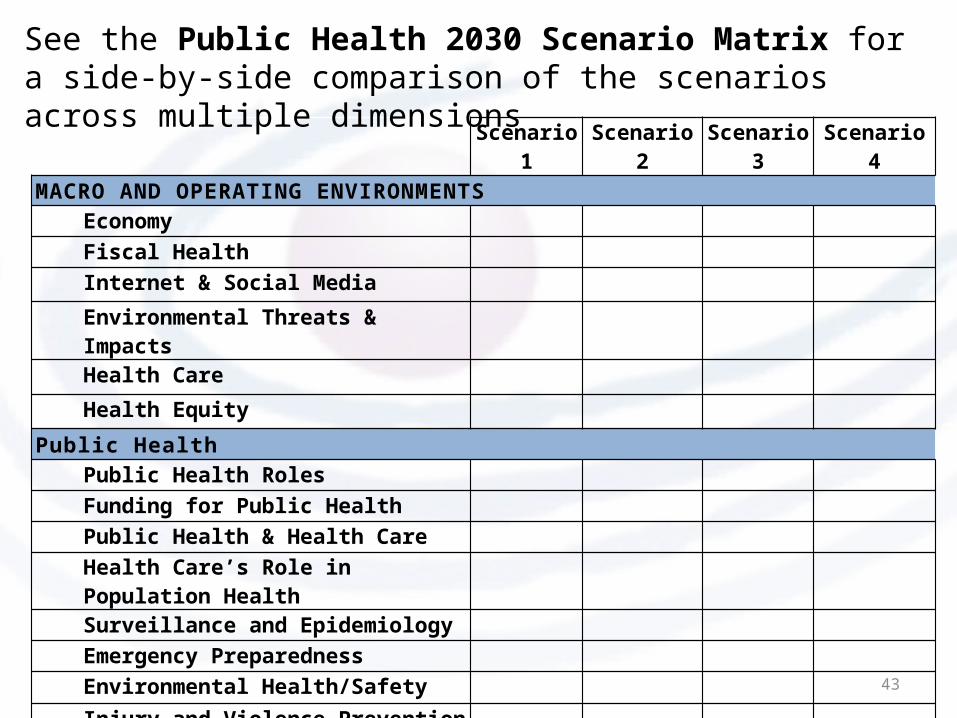
Scenario 1 Scenario 2 Scenario 3 Scenario 4
MACRO AND OPERATING ENVIRONMENTSEconomy
Fiscal Health
Internet & Social Media
Environmental Threats & Impacts
Health Care
Health Equity
Public HealthPublic Health Roles
Funding for Public Health
Public Health & Health Care
Health Care’s Role in Population Health
Surveillance and Epidemiology
Emergency Preparedness
Environmental Health/Safety
Injury and Violence PreventionEtc.
See the Public Health 2030 Scenario Matrix for a side-by-side comparison of the scenarios across multiple dimensions
43
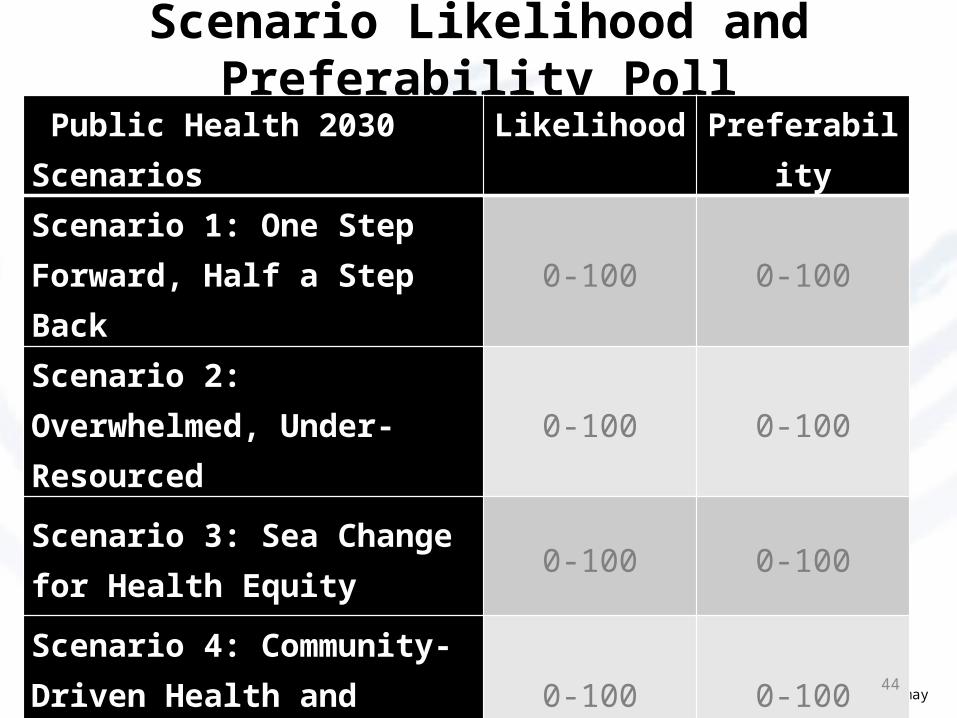
Scenario Likelihood and Preferability Poll
Please use the grid below to assess the likelihood and preferability of each scenario separately. •100% refers to highly likely or preferable. •0% means there is nothing desirable or preferable about a particular scenario. •Percentages can be from 0 to 100 in each cell. Columns or rows need not add up to 100%. For example, you may assign 60% for likelihood and 85% for preferability of a scenario.
Public Health 2030 Scenarios Likelihood Preferability
Scenario 1: One Step Forward, Half a Step Back 0-100 0-100
Scenario 2: Overwhelmed, Under-Resourced 0-100 0-100
Scenario 3: Sea Change for Health Equity 0-100 0-100
Scenario 4: Community-Driven Health and Equity 0-100 0-100
44

• Implications for public health in your city, county – your goals, directions, strategies?
• What are your expectations, fears and aspirations for public health?
• Other questions?
Implications/Questions
45

Public Health 2030 Recommendations
from the
National Workshop
March 6 & 7, 2014
46
47
Rec 1:
Transform Public Health Agencies into “Health Development Agencies” with Dedicated, Sustainable, and Sufficient Funding. 1A: Develop Dedicated, Sustainable, and Sufficient Funding1B: Implement Policies for the Systematic Use and Development of Evidence and Best Practices1C: Build Public Health Agencies' Role in Fostering Prevention and Health Promotion Strategies
Rec 2:
Partner in Health Care Transformation to Facilitate the Evolution from a Health Care System to a Health System
Rec 3:
Build the Capacity for Dialogue about Inclusion, Opportunity, and Equity
Rec 4:
Dialogue with Other Sectors to Support Innovation
Rec1: Transform Public Health Agencies into “Health Development Agencies” with Dedicated, Sustainable, and Sufficient Funding.
Conceiving of public health agencies as “health development agencies” is new. We believe that taking steps toward the realization of this endeavor will pave the path for developing and recruiting the people and resources needed to innovate, and to make major inroads into improving population health and eliminating health disparities.
48

The health development agency of 2030 will:• Identify problems and opportunities to improve
community health, • Catalyze and incentivize action by sectors within health
and outside health• Carry out some but not all of the traditional assurance
and protection functions of PHAs today• Promote health in the broader context, assure
inclusiveness, and are fully incorporated into community improvement processes
• Perform strong fiscal management (“No margin, no mission”)
49

The health development agency of 2030 will:• Learn and apply innovation principles from other
sectors and organizations• Leverage other stakeholders and resources from other
sectors to improve health and wellbeing• Have adequate funding for the necessary
infrastructure. • Employ staff with the interdisciplinary training and
skills needed to work with other stakeholders and support the agency’s role in fostering prevention and health promotion.
50
Rec1A: Develop Dedicated, Sustainable, and Sufficient Funding
Health development agencies will require dedicated, sustainable, and sufficient funding streams that lie outside of traditional categorical programs.
51
Rec1A: Action Steps
• Define with specificity what is needed for the health dev. agency, what it will cost, and accountability measures
• Review and support current efforts to define and estimate the costs of foundational capabilities and experiments in funding
• Define options for developing revenue streams to support the foundational capabilities
• Enable flexible use of grant funding. Expand federal block grant funding to dedicate a portion specifically to supporting the foundational capabilities
52
Rec1A: Action Steps
• Integrate standards for goodness (appropriateness and effectiveness) and fairness (equity) into grants and partnerships
• Design grant requirements to promote multi-sector participation and collaboration
• Promote National Public Health Accreditation
53
Rec1B: Implement Policies for the Systematic Use and Development of Evidence and Best Practices
Strong fiscal management and effectiveness will require continual and enhanced research, evaluation, and translation of policies, programs, and services. Moreover, evidence and best practices information on a few policies already exists but this information is not used systematically by PHAs and community organizations.
54
Rec1B: Action Steps
• Assure adequate data collection, analysis, and utilization to support the mission of public health agencies
• Develop metrics and tools to support policy and impact assessments
• Capture value and improved outcomes through a defined evaluation process
• Improve the systematic collection, growth, and use of evidence of what works in public health. Identify and disseminate existing best practices.
55
Rec1B: Action Steps
• Develop tools and resources for health development agencies to use that are equivalent to those used in economic development, but with community health improvement indicators as the outcome measures/ROI
• Design successive versions of the public health accreditation standards and measures to drive innovation
56

Existing sources for evidence-based practices to identify promising practices include:• The Practical Playbook (www.practicalplaybook.org)• Strategies for Reducing Health Disparities — Selected CDC-
Sponsored Interventions, United States, 2014 (http://www.cdc.gov/mmwr/preview/ind2014_su.html#HealthDisparities2014)
• Guide to Community Preventive Services (www.thecommunityguide.org/index.html)
• Healthy People 2020 • Compendium of Proven Community Based Prevention Programs (
http://tfah.org/report/110)• County Health Rankings• THRIVE tool (http
://thrive.preventioninstitute.org/thrive/index.php)• Various examples from state and local PHAs 57
Rec1C: Build Public Health Agencies' Role in Fostering Prevention and Health Promotion Strategies
…Public health agencies can provide this trusted leadership but will require the expansion of prevention research and subsequent publication and dissemination of findings, as well as improvements in workforce development and agency communications capabilities.
58
Rec1C: Action Steps
• Demonstrate the value of PHA leadership in fostering prevention & health promotion strategies to other stakeholders.
• Promote foundational capabilities of state & local public health agencies. Engage outside stakeholders in this conversation.
• Incorporate the necessary skills and competencies for these capabilities into training for public health professionals.
• Identify best practices already in existence that demonstrate these capabilities, and promote these practices.
59

Rec1C: Action Steps• Assure adequate IT capabilities, data collection,
analysis, and utilization to support these foundational capabilities.
• Enhance PHAs’ communication capabilities in the evolving Internet, social media, and broadcast era.
• Develop marketing skills to build support for and create coalitions in support of the "health development agency" concept.
• Assure that all PHA processes amplify hidden or muffled community voices.
• Expand prevention research, including enlarging the number of researchers focused on prevention.
60

Rec2: Partner in Health Care Transformation to Facilitate the Evolution from a Health Care System to a Health System
Specific trends in health care supporting this shift to emphasizing community health and prevention include:• Health care systems, particularly those pursuing the
Triple Aim…and…improving population health• The move away from fee-for-service payment toward
pay for value and global budgeting approaches adopted by both public agencies and private not-for-profit clinical entities
61
Rec2: Partner in Health Care Transformation to Facilitate the Evolution from a Health Care System to a Health SystemIn its role as chief health strategist, public health needs
to seize the opportunity and be at the table to offer strategic direction, facilitation, vision for prevention, advanced analytics, best practice knowledge on community health interventions, and (where relevant) services. Public health needs to share its experiences to ensure that new initiatives can build on learnings and successes. Public health also needs to share in the savings realized when prevention and health promotion bend the health cost curve downward.
62

Rec2: Action Steps
At the national and state levels• Identify specific models and best practices of effective
public health collaborations with health care systems • Develop tools and venues for educating health care
professionals and the broader health leadership community on the importance of taking a community-oriented approach and on the models and best practices
• State and local governmental public health agencies should build both the evidence- and practice-base for public health in collaboration with community partners
63
Rec2: Action Steps
At the local level• State and local public health agencies should
determine how they can best contribute to enhanced health provider efforts to improve population health
• Local health departments should facilitate discussions with and learning by health care providers about innovations and new models for joint public health/health care service delivery that represent opportunities for enhanced community health
• Identify health care leaders who are interested in and/or have a track record of addressing community needs
64

Rec2: Action Steps
At the local level• …PHAs should work with clinical partners to encourage
that Community Health Needs Assessment processes:– Collaborate with PHAs on comprehensive CHNAs.– Include robust analysis of community conditions and root
causes of health inequities.– Deploy big data analytics that uses public health and health
care data.– Work with communities to identify the community’s
concerns and priorities and build on these concerns to develop and implement plans to address community needs.
– Align with the voluntary Public Health Accreditation Board (PHAB) standards.
65

Rec3: Build the Capacity for Dialogue about Inclusion, Opportunity, and Equity
There are important value changes that public health agencies need to reinforce. The ability to frame a dialogue, both internal to the agency and external in the community, about the historical legacy and present day practices of racism and other "isms" is fundamental to understanding and addressing the root causes of health inequity and advancing community vitality.
66

Rec3: Action Steps
• Use dialogues to identify and promote fundamental aspirations of communities and residents, and use them to inform the work of public health agencies, including community health improvement plans and internal agency strategic plans. Integrate opportunities for dialogue on legacy and future-focused narratives into routine public health practice.
• Identify opportunities to dialogue with executive and legislative policymakers.
• Identify existing good examples of dialogues, disseminate them, and replicate them.
67

Rec4: Dialogue with Other Sectors to Support Innovation
Public health should facilitate mutual understanding of needs and perspectives, and tailor messages accordingly […] Public health also needs to seek lessons in innovation through these dialogues with other stakeholders and sectors.
68
Rec4: Action Steps
• Define and acquire the skills needed for effective dialogue with other stakeholders and sectors.
• Institutionalize measures for effective dialogue.• Adjust public health messages to reflect what
community stakeholders can hear and absorb.• Conduct dialogues with stakeholders and sectors
outside of public health ("Talk to somebody different").• Conduct one-on-one meetings with strategic
stakeholders.
69

Rec4: Action Steps
• Identify and pursue opportunities for dialogue with executive and legislative policymakers, as well as with the media.
• Identify innovative options that meet the needs and perspectives of multiple, diverse stakeholders and sectors.
• Catalyze Health Collaboratives comprised of influential champions who work to educate decision makers and the public about the critical importance of health development agencies’ work in ensuring the economic future of our country.
70

Rec4: Action Steps
• Market health development agencies by providing a clear and compelling case for and image of them. This should encourage stakeholders to come to health development agencies for consultation regarding prevention, health promotion, and disease management strategies, and to trust their evaluation processes related to the measurement of national, state, and local health outcomes.
71

Public Health 2030:A Scenario Exploration
Supported by grants from:
www.altfutures.org/publichealth2030