public expenditures in health. main principles establish market failures identify beneficiaries of...
TRANSCRIPT

Public Expenditures in Health

Main Principles
• Establish Market Failures
• Identify beneficiaries of expenditures
• Balance potential benefits with ability to deliver services
Health - Market Failures
• Public goods (pest control, sanitation, health education)
• Externalities (infectious disease control)
• Information advantage of doctors
• Insurance
Health - equity concerns
• Inequities in health status
• Inequities in benefits of services

The poor are sicker than other people: Under two mortality by “wealth”- Brazil, 1996
0
2
4
6
8
10
12
Poore
st 2 3 4 5 6 7 8 9
Riches
t
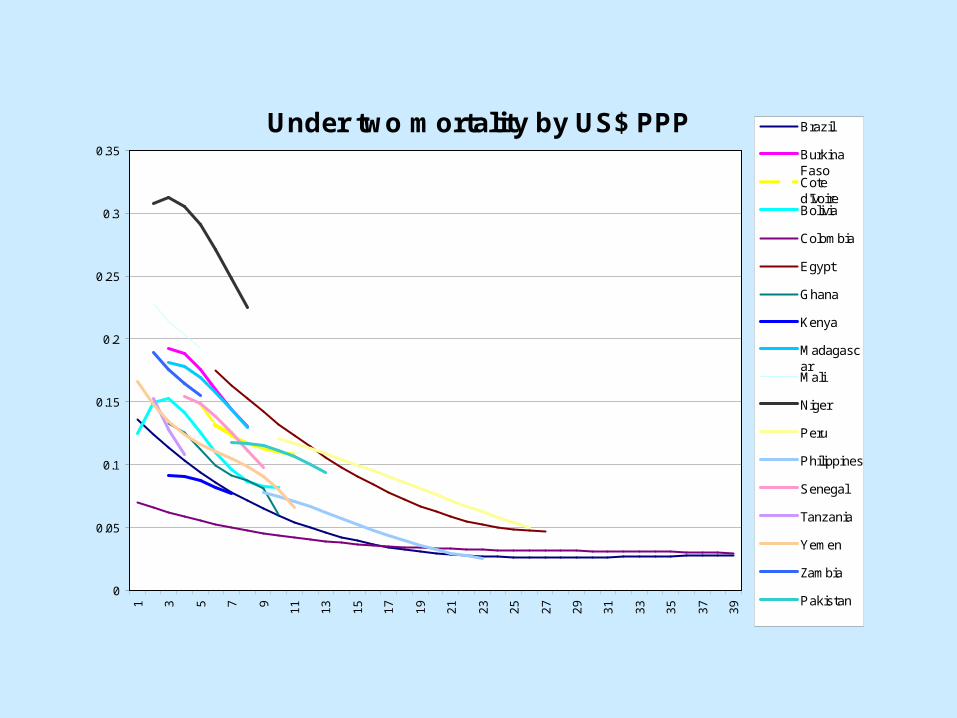
Under two mortality by US$ PPP
0
0.05
0.1
0.15
0.2
0.25
0.3
0.351 3 5 7 9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
Brazil
BurkinaFasoCoted'IvoireBolivia
Colombia
Egypt
Ghana
Kenya
MadagascarMali
Niger
Peru
Philippines
Senegal
Tanzania
Yemen
Zambia
Pakistan

Prevalence of disease by “wealth”: India 1992-3
0123456789
Poore
st II III
IV V VIVII
VIII IX
Riches
t
TB (x10)MalariaBlindness
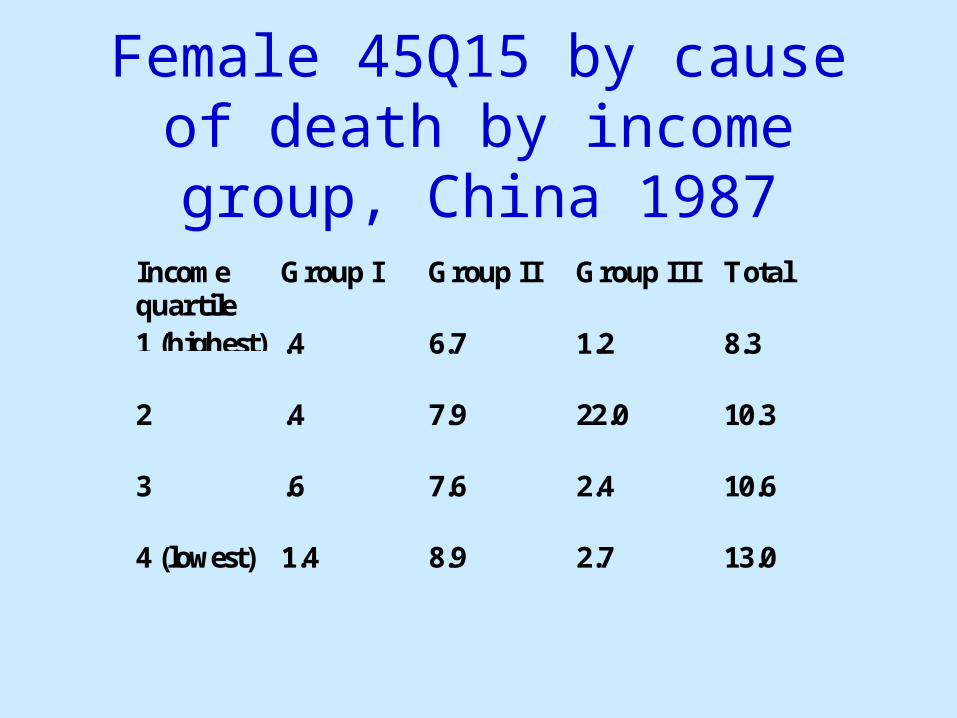
Female 45Q15 by cause of death by income group, China 1987
Incomequartile
Group I Group II Group III Total
1 (highest) .4 6.7 1.2 8.3
2 .4 7.9 22.0 10.3
3 .6 7.6 2.4 10.6
4 (lowest) 1.4 8.9 2.7 13.0

Health - Problems of Implementation
• Management challenge– Personnel placement– Quality of services
• Conscientious providers
• Maintenance of facilities
• Political Influence

Percentage of health centers without doctors by province: Indonesia
0
10
20
30
40
50
60

Absenteeism in primary facilities
05
1015202530354045
Uganda
Bangladesh
IndiaIndonesia
Ecuador
Peru
Teachers
Healthworkers
% a
bsen
t
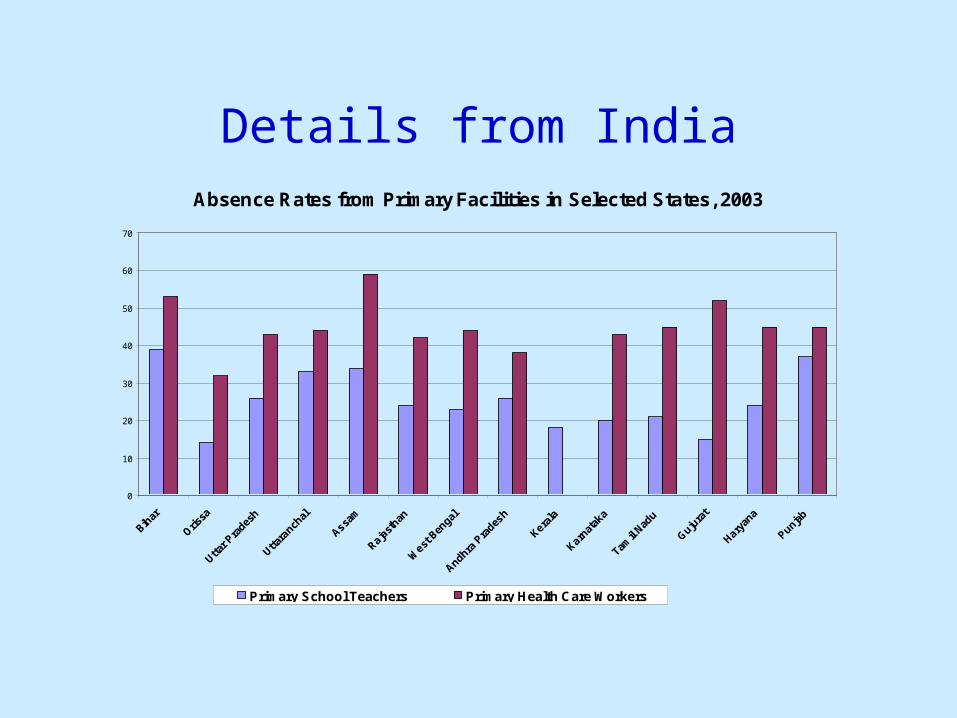
Details from IndiaAbsence Rates from Primary Facilities in Selected States, 2003
0
10
20
30
40
50
60
70
Bihar
Orissa
Uttar P
rades
h
Uttara
nchal
Assam
Rajast
han
West
Ben
gal
Andhra P
rades
h
Kerala
Karnat
aka
Tamil
Nadu
Gujura
t
Haryan
a
Punjab
Primary School Teachers Primary Health Care Workers
Health: Complementarity/ conflict between goals
• Public goods - strong complementarity
• Primary health care - modest efficiency effects (varies), potentially high equity effects, difficult management
• Hospitals - high efficiency, high potential but low actual equity effects, easier management(?)

In Brazil, the poor have worse sanitation facilities…
0
10
20
30
40
50
60
70
Poorest III V VII IX
Percent of households with no sanitation facilities
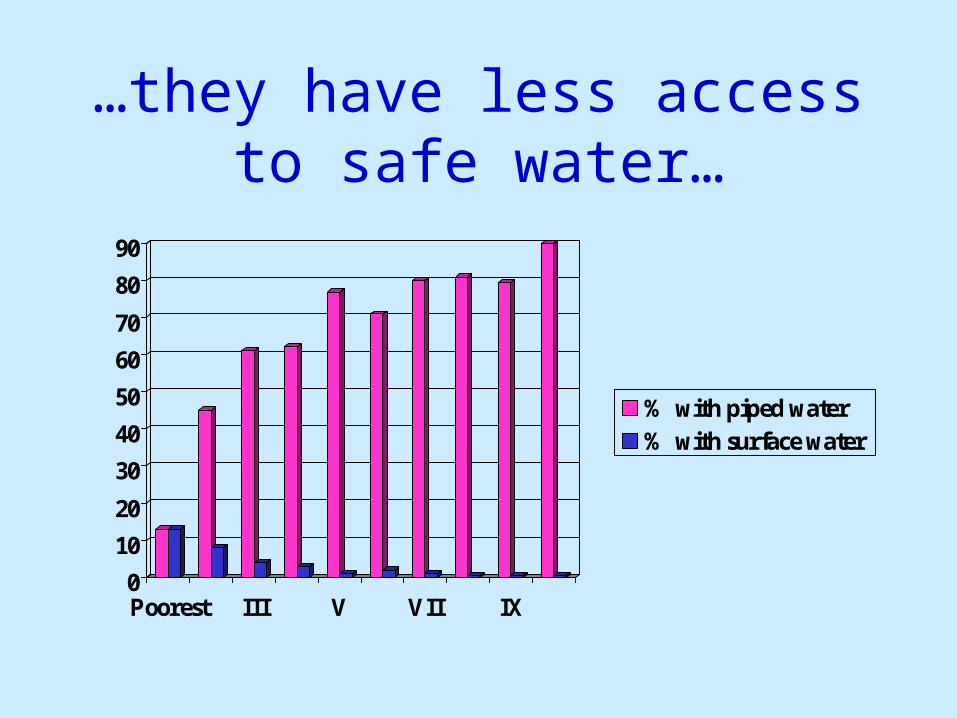
…they have less access to safe water…
0
10
20
30
40
50
60
70
80
90
Poorest III V VII IX
% with piped water% with surface water

…and this costs the lives of their children
0123456789
10
Good watersource andsanitation
Nosanitation
Bad water Both bad

Health: Complementarity/ conflict between goals
• Public goods - strong complementarity
• Primary health care - modest efficiency effects (varies), potentially high equity effects, difficult management
• Hospitals - high efficiency, high potential but low actual equity effects, easier management(?)

Determinants of infant mortalityVariable Malaysia PhilippinesIncome -1.06
(.97)-.223(.042)
Safe Water -.147(.05)
-.026(.027)
Immunization (DPT) -.113(.04)
-.018(.013)
Public medicalpersonnel per capita
1.03(.79)
Public health subsidy -.404(.113)
Subsidy income .041(.012)
Adjusted R2 .55 .988S.e. in parentheses
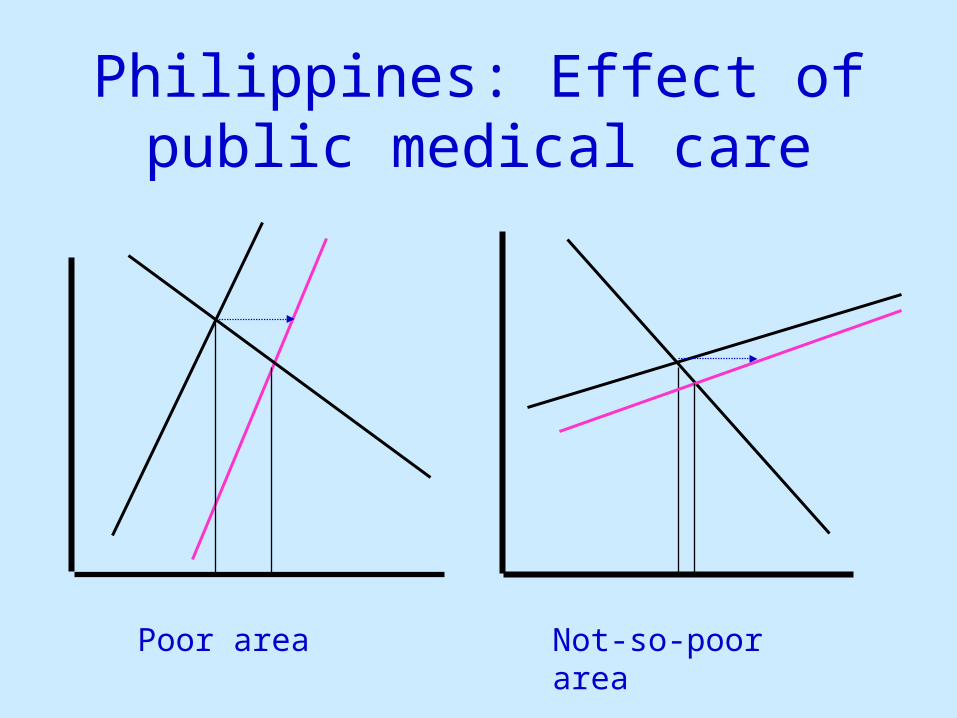
Philippines: Effect of public medical care
Poor area Not-so-poor area

Substitution between public and private providersCountry/Sample Policy change Increase in private
sector as a percentageof decrease in public
Price increasesBenin (rural) Community Health
Center fees61
Bolivia (urban)-adults Ministry of PublicHealth (MoPH) fees
33
Bolivia (urban)-children=15
“ “ 0
Bolivia (urban)-children= 4
“ “ 0
El Salvador (urban) –males
Ministry of Health fees 56
El Salvador (urban) –females
“ “ 50
Ghana Public facility fees 60Kenya (rural) – adults Government facility
fees (0 to 10Ksh)37
Nigeria – adults Public facility fees 100Pakistan (urban) –children = 5
Government clinic price 71
Increases indistance or time
Bolivia (urban) – adults Waiting time – MoPHfacilities
100
Bolivia (urban) –children = 15
Travel time - ““
20
Bolivia (urban) –children = 4
Waiting time- ““
20
Ghana Distance to nearestpublic facility
50
Kenya (rural) “ “ 44

Distribution of health care subsidies, Indonesia
020406080
100120140160180200
Poore
st 2 3 4 5 6 7 8 9
Riches
t
Hospital inpatientHospital outpatientHealth centerHealth sub-center
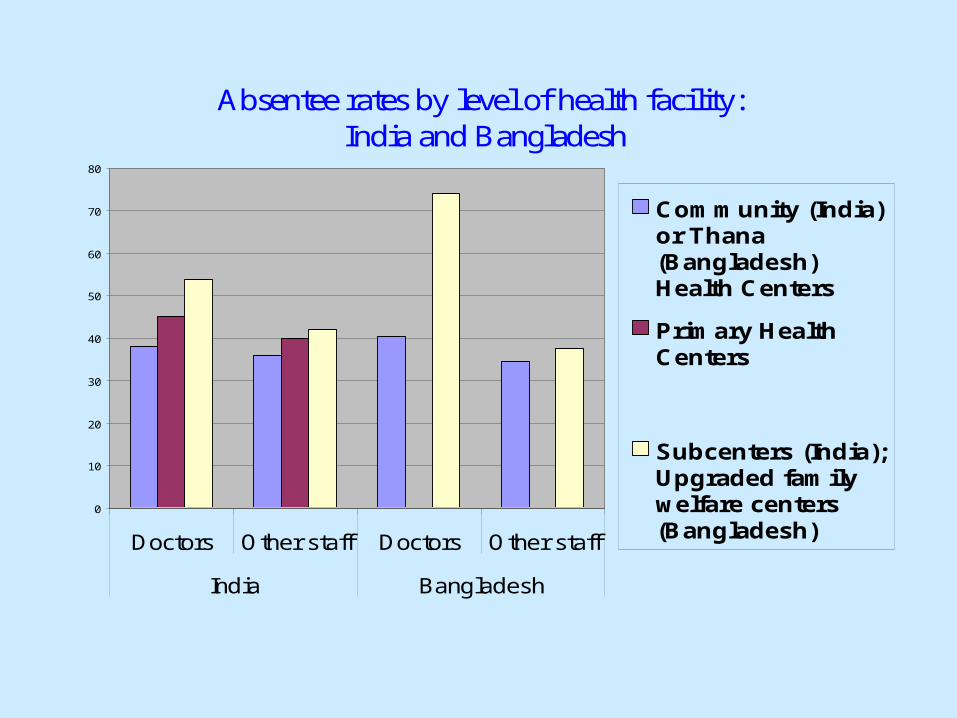
Absentee rates by level of health facility: India and Bangladesh
0
10
20
30
40
50
60
70
80
Doctors Other staff Doctors Other staff
India Bangladesh
Community (India)or Thana(Bangladesh) Health Centers
Primary HealthCenters
Subcenters (India);Upgraded familywelfare centers(Bangladesh)

Health: Complementarity/ conflict between goals
• Public goods - strong complementarity
• Primary health care - modest efficiency effects (varies), potentially high equity effects, difficult management
• Hospitals - high efficiency, high potential but low actual equity effects, easier management(?)

Value of insurance as a % of expected cost
0
10
20
30
40
50
60
Poorest 2 3 4 Richest
OutpatientInpatient
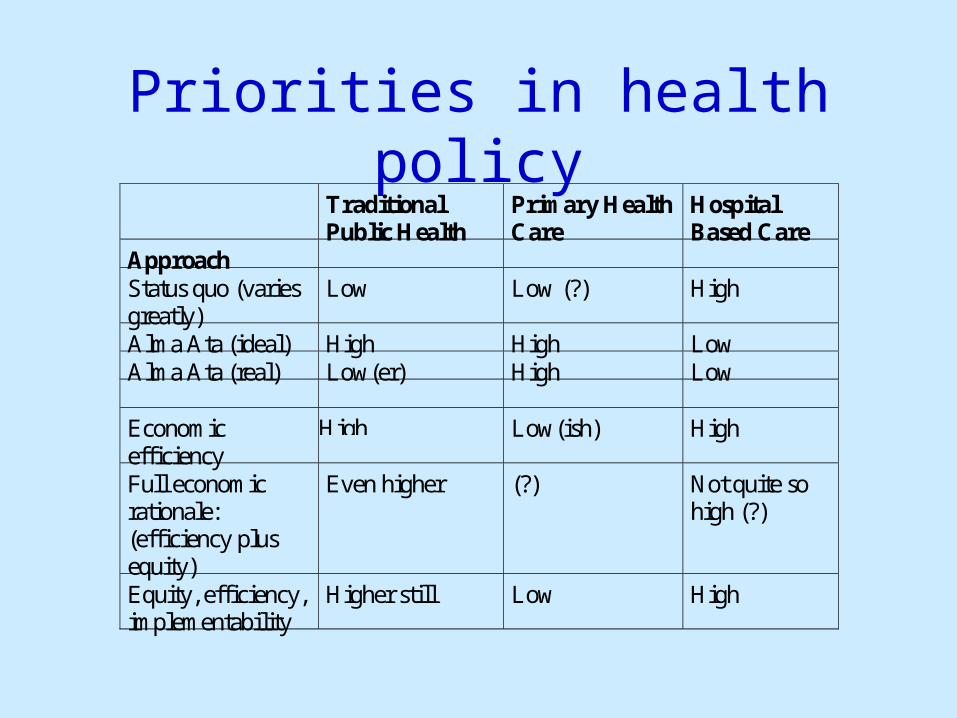
Priorities in health policyTraditionalPublic Health
Primary HealthCare
HospitalBased Care
ApproachStatus quo (variesgreatly)
Low Low (?) High
Alma Ata (ideal) High High LowAlma Ata (real) Low(er) High Low
Economicefficiency
High Low(ish) High
Full economicrationale:(efficiency plusequity)
Even higher (?) Not quite sohigh (?)
Equity, efficiency,implementability
Higher still Low High