psychosocial aspects of living with congenital heart...
TRANSCRIPT

Umeå University Medical Dissertations, New Series No 1532
Psychosocial aspects of living with congenital heart disease child, family, and professional perspectives
Anna-Lena Birkeland
Department of Clinical Sciences
Pediatrics
Child and Adolescent Psychiatry
Umeå University
901 87 Umeå
Umeå 2012

Responsible publisher under Swedish law: the Dean of the Medical Faculty
This work is protected by the Swedish Copyright Legislation (Act 1960:729)
© Anna-Lena Birkeland
ISBN: 978-91-7459-511-6
ISSN: 0346-6612
Cover picture: Annica Anca Elmberg, www.källbergelmberg.se
E-version available at http://umu.diva-portal.org/
Printed by: Print & Media
Umeå, Sweden 2012

Alla är en berättelse… som vi får lyssna till…


PROLOG
Mitt professionella fokus har varit psykosocial utredning, bedömning
och behandling av barn med hjärtfel och familjen runt dem. Jag har
fått ta del av och lyssnat på många berättelser från hjärtbarn, föräldrar
och familjer, var och en av dessa är i sig själva en studie av komplexitet,
anpassning, bemötande och samarbete. Detta kliniska arbete inom
barnhjärtsjukvård har gett mig kunskap om hjärtbarnens livsvillkor,
familjen, professionella utmaningar inom barnhjärtsjukvård samt om
sjukvårdens och samhällets förmåga och ibland, trots goda avsikter,
oförmåga att se och möta behovet av ett helhetsomhändertagande och
upprätthålla beredskap att möta komplexiteten på både individ,
grupp/familj och samhällsnivå. Genom arbetsprocessen med
avhandlingen har jag fått möjlighet att fördjupa och vidare utforska
några av de aspekter som jag identifierat i mitt kliniska arbete.


i
TABLE OF CONTENTS
Table of contents _________________________________________________ i
Abstract ________________________________________________________ iii
Populärvetenskaplig sammanfattning _______________________________ v
Original papers __________________________________________________ ix
Abbreviations ___________________________________________________ x
Thesis at a glance ________________________________________________ xi
Introduction _____________________________________________________ 1 Theoretical framework ________________________________________________ 2
Quality of life _____________________________________________________ 2 Stress - Coping____________________________________________________ 5 Psychosocial approach _____________________________________________ 6 Support _________________________________________________________ 7 Profession _______________________________________________________ 8 Team ___________________________________________________________ 9 Transition _______________________________________________________ 10
Methodological framework ________________________________________ 11 Quantitative methods _________________________________________________ 11
Structured interview: Study I ________________________________________ 11 Questionnaire: Study IV ____________________________________________ 12
Qualitative method ___________________________________________________ 12 Studies II–IV______________________________________________________ 12 Study II _________________________________________________________ 12 Study III _________________________________________________________ 13 Study IV _________________________________________________________ 13 Statistical analysis: Studies I and IV ___________________________________ 13
Ethics __________________________________________________________ 14
Aims of the study ________________________________________________ 15 Overview of the research process________________________________________ 16 Study groups ________________________________________________________ 16

i i
Results ________________________________________________________ 20 Study I: Complexity __________________________________________________ 20
Aim ___________________________________________________________ 20 Design and results ________________________________________________ 20
Study II: Coping ______________________________________________________ 21 Aim ____________________________________________________________ 21 Design and results _________________________________________________ 21
Study III: Profession ___________________________________________________ 22 Aim ____________________________________________________________ 22 Design and results _________________________________________________23
Study IV: Teams/PCTs _________________________________________________ 24 Aim ___________________________________________________________ 24 Design and results ________________________________________________ 25
Discussion _____________________________________________________ 26 Complexity _________________________________________________________ 26
Personal sphere __________________________________________________ 27 Interpersonal sphere ______________________________________________ 27 External sphere ___________________________________________________ 27
Coping – Stress _____________________________________________________ 28 Profession _________________________________________________________ 30 Teams/PCTs _________________________________________________________32
Methodological considerations and limitations _______________________ 34 Quantitative method _________________________________________________ 34 Qualitative method __________________________________________________ 35
General summary _______________________________________________ 37
Challenges for the future _________________________________________ 38
Acknowledgements _____________________________________________ 39
References ______________________________________________________41

i i i
ABSTRACT
Background
The vast majority of infants born with congenital heart disease (CHD) reach
adulthood because of the developments in cardiology in recent decades. This
thesis aims to describe the psychosocial situation of child/adolescent cardiac
patients and their families, investigate the situation faced by parents and siblings
initially and over time, investigate the approaches paediatric cardiologists use in
encountering the family, and describe the teamwork occurring in paediatric
cardiology teams (PCTs) in Sweden.
Theoretical framework: The theoretical framework was based on a quality of life
model applied to children, a stress-coping model, and a psychosocial approach
including support, profession, and teamwork.
Methods
The research combines quantitative data collection/analysis and qualitative
research interviews/content analysis.
Results
Complexity: The three grades of medical complexity differed regarding the
number and severity of psychosocial symptoms, the children with the most
complex CHD having the most severe symptoms. The most frequent symptoms in
the whole patient group regarding various spheres were: healthcare and
treatment-related needs in the external sphere, family symptoms in the
interpersonal sphere, and mental/psychosomatic symptoms in the personal
sphere.
Coping: Being informed of a child’s/sibling’s heart disease has emotional
consequences, so information, communication, and support are essential.
Breaking the news of a child’s disease can be described as a turning point still
significant after ten years. The professionalism of the doctor’s approach in
breaking the news is crucial.
Profession: Among paediatric cardiologists, how to break bad news to a family is
an important concern, evident in findings regarding the significance of trust and
confidence and the use of various emotional positions. Paediatric cardiologists
commonly wish to be skilled at handling this situation, and attaining the needed
skills calls for reflection, education, and sharing experience.

i v
Team: PCTs in Sweden aim and try to work in a structured way. In PCTs, there is
a need for leadership, resource coordination, coaching, and a forum for joint
reflection. Dependence on the physician on the team was identified in all PCTs.
The challenge of managing increasing complexity at both the family and system
levels requires interprofessional teams.
Conclusions
These studies illustrate the psychosocial complexity and the need of psychosocial
support. Emotional consequences, communication, information and support are
essential both for the children, parents/families and for the professionals. To
manage this complexity organizational alteration action plans are required. There
is a need for a forum to stimulate dialogue and common reflection in the local
PCT and at the regional and national centres.
Key words breaking bad news, children/adolescents, congenital heart disease,
communication, content analyse, coping, counselling, interprofessional team,
medical education, patient relationships, paediatric cardiology, professional role,
psychosocial inventory method, qualitative method, quantitative method stress,
teamwork

v
POPULÄRVETENSKAPLIG SAMMANFATTNING
Bakgrund
Sedan flera decennier har barnhjärtsjukvård genomgått en omfattande
utveckling. För 50 år sedan ledde obehandlat medfött hjärtfel till barns död i 60–
70% av fallen. Flertalet barn som är födda med hjärtfel når nu tonåren och
vuxenlivet tack vare den utveckling som skett inom barnhjärtkirurgi,
intensiv/nyföddhetsvård och barnkardiologi de senaste 40–50 åren. Idag kan
barn som tidigare bedömdes vara icke behandlingsbara ges en tillfredsställande
korrigering eller lindring. Nya metoder har revolutionerat behandlingen och
vården av dessa barn men också lett till livslång uppföljning för vissa hjärtbarn. I
denna nya grupp av patienter ingår t.ex. barn med s.k. enkammarhjärtan och de
barn/ungdomar som kan behöva genomgå hjärttransplantation. Erfarenhet från
vården av barn med hjärtfel tyder på att hjärtfelet inte alltid är det största
problemet för dessa patienter utan att de lever med frågor som avser livskvalitet
och den psykosociala situationen. Barn som behandlas för medfödda hjärtfel har
ofta en mycket speciell erfarenhet i livet och kan tvingas leva med olika besvär.
Många behöver ha kontakt under lång tid med hälso- och sjukvården.
Tillsammans med ökade investeringar i medicinsk teknik, behandling och vård av
barn med hjärt- sjukdom finns ett behov av att vidareutveckla och vidare utforska
det psykosociala området för dessa patienter.
Avhandlingens syfte: Det övergripande syftet med denna avhandling var att öka
kunskapen om den psykosociala situationen för barn med medfött hjärtfel (CHD)
och hur de professionella inom barnsjukvården möter barn och familjer som
drabbats av hjärtfel.
Avhandlingens specifika syften:
- att beskriva den psykosociala situationen för barnet/ungdomen och familjen
- att undersöka erfarenheter hos föräldrar och syskon vid beskedet om hjärtfel
och hur man hanterat detta över tid
- att undersöka förhållningssätt i mötet mellan barnkardiolog och familjen
- att beskriva de barnkardiologiska teamen (PCT) i Sverige och deras
förhållningssätt till att arbeta med barn med hjärtfel.
Teori Den teoretiska referensramen utgår från en livskvalitetsmodelll för barn, stress
och coping/anpassning samt psykosocialt förhållningssätt där stöd, profession
och team ingår.

v i
Metoder
Kvantitativa data och kvalitativa forskningsintervjuer har kombinerats.
Kvantitativ metod: Utifrån en livskvalitetsmodell har ett instrument tagits fram
för bedömning av den psykosociala situationen för barn med hjärtsjukdom.
Psykosociala symtom har registrerats. Formuläret delades in i sfärerna personell,
interpersonell och extern.
En enkät har skickats ut till samtliga barnhjärtteam i Sverige.
Kvalitativ metod: Kvalitativa forskningsintervjuer har genomförts med föräldrar,
syskon, barnhjärtläkare och barn-hjärtteam. Intervjudata har analyserats med
kvalitativ innehållsanalys där man systematiskt och strukturerat bearbetar
textdata för att se mönster och teman.
Resultat Komplexitet: De tre graderna av medicinsk komplexitet, skilde när det gäller
antal och svårighetsgrad av psykosociala symptom, där barn med mest komplexa
hjärtsjukdomarna hade de mest frekventa och de allvarligaste symptomen. De
vanligaste symptomen i hela patientgruppen i de olika sfärerna var vård och
behandlingsrelaterade behov i den externa sfären, familjesymtom i
interpersonella sfären och psykiska/psykosomatiska symtom i den personliga
sfären. De allvarligaste symptomen hittades i den interpersonella sfären där
familjesymtom utgjorde den mest allvarliga variabeln. Frekvensen av allvarliga
problem i den personliga sfären var 11% i patientgruppen.
Coping: Att få information om ett barns/syskons hjärtsjukdom får känslomässiga
konsekvenser och information, kommunikation samt stöd är viktigt. Beskedet om
barnets sjukdom kan beskrivas som en vändpunkt i familjernas liv som
fortfarande påverkar dem efter tio år. Läkarens professionella förhållningssätt att
ge besked och sättet att kommunicera är centralt.
Profession: Bland barnkardiologer är hur man ger svåra besked till familjen en
viktig angelägenhet. Tydligt i resultaten är användning av olika känslomässiga
positioner och betydelsen av tillit och förtroende mellan läkaren och
barnet/familjen. Det finns en gemensam strävan att uppnå kompetens att hantera
situationen, och det finns ett behov av reflektion, utbildning och utbyte av
erfarenheter.
Team: Barnhjärtteam i Sverige har ambitionen att arbeta på ett strukturerat sätt
ofta med en sjuksköterska som samordnare. Utmaningen att hantera den ökande
komplexiteten på både familj- och systemnivå kräver insatser av olika
professioner. Barnhjärtteamen möter svårigheter i t ex form av tidsbrist och
problem att samla hela teamet. Inom barnhjärtteamen, finns det ett behov av att
utveckla ledarskap, samordning av resurser, coachning och forum för gemensam
reflektion.

v i i
Slutsatser
De fyra studier som ingår i avhandlingen visar sammantaget på komplexiteten för
barn med medfödda hjärtfel, en komplexitet som både barnet, familjen och de
professionella lever med och måste hantera. Att få besked om barns hjärtfel är
stressande och känslomässigt påfrestande men hanterbart över tid.
Barnhjärtläkarens förhållningssätt har betydelse för föräldrarna och dennes sätt
att kommunicera är betydelsefullt. Emotionella konsekvenser, kommunikation,
information och olika former av stöd är väsentligt både för barn,
föräldrar/familjer och för de yrkesverksamma. För att hantera denna komplexitet
krävs stöd, professionalitet, systemförståelse, organisatorisk insikt och
handlingsplaner för att sätta hjärtbarnet i centrum. Det finns ett behov av forum
för att stimulera dialog och gemensam reflektion i de lokala barnhjärtteamen och
på regionala och nationella centra.
Nyckelord barn/ungdomar, coping, kardiologi teamarbete, kommunikation,
medfödd hjärtsjukdom, medicinsk utbildning, psykosocial symtominventering,
hjärtsjukdom, patientrelationer, rådgivning stress, profession

v i i i

i x
ORIGINAL PAPERS
This thesis is based on the following papers, which are referred to in the text by
their Roman numerals.
I. The complexity of the psychosocial situation in children and adolescents
with heart disease. Birkeland A-L, Rydberg A, Hägglöf B.
Acta Paediatrica 2005;94:1495–1501
Reprinted with permission from the publisher
II. Facing bad news: a case study focusing on of families having a child with
congenital heart disease. Birkeland A-L, Hällgren-Graneheim U, Rydberg A,
Hägglöf B, Dahlgren L.
In manuscript
III. Breaking bad news: an interview study of paediatric cardiologists. Birkeland
A-L, Dahlgren L, Hägglöf B, Rydberg A.
Cardiology in the Young 2011;21:286-291
Reprinted with permission from the publisher
IV. Teamwork in Swedish paediatric cardiology: a national exploratory study
examining function and dynamics. Birkeland A-L, Rydberg A, Dahlgren L,
Hägglöf B.
Accepted for publication

x
ABBREVIATIONS
AD/HD Attention-Deficit/Hyperactivity Disorder
CHD Congenital Heart Disease
CBCL Child Behaviour Check List
CAP Child and Adolescent Psychiatry
DSM IV Diagnostic and Statistical Manual of Mental Disorders IV
GARF Global Assessment of Relational Functioning (GARF) Scale
GUCH Grown-Up Congenital Heart disease
HO Habilitation Organization
HRQoL Health-Related Quality of Life
PCT Paediatric Cardiology Team
QoL Quality of Life
SOC Sense of Coherence
SOFAS Social and Occupational Functioning Assessment Scale
WHO World Health Organization

x i
THESIS AT A GLANCE
Aims Material and methods Results Conclusions
Study I.
Complexity
The complexity of
the psychosocial
situation in
children and
adolescents with
heart disease.
Published.
To describe the
psychosocial situation of
children/adolescents
with heart disease and
their families.
n = 9
Children/adolescents with
congenital heart disease
(CHD) were graded into
three categories with
respect to the complexity
of CHD.
Patients were compared
with age- and gender-
matched healthy controls.
A structured interview
model and clinical
evaluation was used to
collect data.
Results were presented as
means, medians, and
percentages. Differences
between groups were
analysed using contingency
analysis (Chi-square test).
The most frequent symptoms
were healthcare- and treatment-
related needs (71/97) in the
external sphere, family symptoms
(68/97) in the interpersonal
sphere, and mental and non-
cardiac-related somatic symptoms
(19/97) in the personal sphere.
Corresponding numbers in the
control group were treatment-
related needs (15/97), family
symptoms (9/97), and somatic
symptoms (25/97). In the patient
group, 50% of the symptoms were
evaluated as mild, 30% moderate,
and 20% severe. The frequency
of severe problems in the
personal sphere was 11% in the
patients and 1% in the controls.
The study illustrated the psychosocial
complexity and the need for
psychosocial support in the study
group.
The three grades of medical
complexity differed regarding the
number and severity of psychosocial
symptoms. Severe personal problems
were experienced in the most complex
group, indicating that the patients have
severe personal problems independent
of family problems.
In line with development of medical
treatment, the results indicated a need
for structured psychosocial
programmes based on the complex
psychosocial situation of children and
adolescents with heart disease and
their families.
Study II.
Coping
Facing bad news
- a case study
focusing on
families having
a child with
congenital heart
disease.
Manuscript
To explore the
experiences of parents
and siblings of children
with CHD during the
diagnostic phase and
how family members
dealt with the situation
over time.
n = 8
Children with CHD
representing three levels of
complexity from a patient
group of 97 children. Family
members were interviewed
on two occasions ten years
apart and data were
collected from eight semi-
structured interviews.
Qualitative content analysis
was used.
Main themes:
- Being informed of the diagnosis
evoked overwhelming feelings
- Ambivalence towards medical
interventions and technology
- Expressed need for professional,
social, and emotional support
- Pathways to new perspectives
- Outlook on life and future
changed over time
Receiving news of a child’s CHD could
be described as a turning point. How
the problems were evaluated and dealt
with varied over time. Despite marked
stress, living with and caring for a child
with heart disease proved
manageable. In both the short and
long terms, well-functioning
communication between the families
and medical personnel was described
as essential.
Study III.
Profession:
physician
Breaking bad
news: an
interview study
of paediatric
cardiologists,
Published.
To examine the
approach of paediatric
cardiologist in informing
and communicating with
the family and patient.
n = 9
Nine semi-structured
interviews were carried out
with paediatric
cardiologists.
Qualitative content analysis
was conducted.
Main themes:
- Method of providing information
- Emotional positions
- Creation of confidence
- Interaction
- Success and failure
- Strategies for handling the
situation
- Various themes/needs all
involved a need for reflection
- Development of teamwork is
required
Physicians were expected to cope with
the complexities of diagnoses and
decisions, while being sensitive to the
feelings of the parents, aware of their
own emotions, and able to keep all this
under control in the context of breaking
the bad news to the parents and
keeping them informed. These
conflicting demands created a need to
expand the professional role by
including more training in emotional
competence and communicative
ability.
Study IV.
Team: PCT
Teamwork in
Swedish
paediatric
cardiology:
a national
exploratory study
examining
function and
dynamics,
Accepted.
To describe PCTs in
Sweden, their
organization and
function, and to deepen
our understanding of
working in a PCT.
n = 30
Questionnaire sent to all 34
contact nurses for
paediatric cardiology in
Sweden.
n = 6
Focus group interviews with
PCTs selected by size and
location. Statistical and
content analysis were used.
Thirty of 34 PCT units completed
the questionnaire. The nurse was
coordinator in 17/26 units.
Main themes:
- Organization/ way of working working
- Function and task
- Attitude/approach
- Communication
The challenge was to meet and
manage the increasing complexity.
Structural/organizational limitations
and doctors’ working conditions were
crucial factors. The PCTs need
leadership, team coordination/
communication, support, continuing
education, and access to professional
management consultants. Fora for
dialogue and joint reflection are
needed in the local PCT and at
regional and international centres.

x i i

I n t r o d u c t i o n | 1
INTRODUCTION
Paediatric cardiology has been developing extensively for several decades. Fifty years
ago, children died from untreated congenital heart (CHD) disease in 60–70% of
cases. Today, however, most children born with CHD reach adolescence and
adulthood thanks to developments in cardiac surgery, interventional cardiology,
intensive/neonatal care, and general paediatric cardiology over the past 40–50 years
(1–3). Childhood conditions once deemed untreatable can now be adequately
corrected or alleviated (4). Treatment and care of patients with CHD have been
revolutionized by the introduction of new methods in surgery and anaesthesiology
and the development of specialized children’s intensive care units, though this has led
to life-long follow-up for some children with CHD (5). This new group of patients
includes children with single-ventricle heart defects and children/adolescents who
need to undergo cardiac transplantation (2, 6–10). Although the outcome of
corrective cardiac surgery is the key factor for survival, other factors such as
psychological and social issues are of great importance in terms of quality of life (11).
Clinical experience suggests that the cardiac defect is not always the most serious
problem facing these patients; instead, quality of life and the psychosocial situation
are the major issues in their lives (12). A holistic approach to care, psychosocial
assessment resources and psychosocial treatment, when appropriate, are important
determinants of the quality of life of the child, adolescent, and the family (11, 12).
Research into heart disease in children and adolescents has previously been
predominantly medically oriented; few psychosocial studies have been carried out in
this field, in contrast with the fields of childhood and adolescent experience of more
common diseases such as cancer, asthma, and diabetes.
Children treated for congenital heart defects often have a very special life experience
and may be forced to live with various difficulties and disabilities. Many require long-
term contact with the healthcare system, doctors, nurses, and paediatric cardiology
teams (PCTs) (13). Studies attempting to highlight quality of life in children with
CHD, as well as psychosocial studies, all identify a complex set of psychosocial
problems (14–17). This patient group also occasionally appears to have behavioural
and emotional problems. Various studies (17, 21-25) have found a higher frequency of
psychological problems in the group with complex congenital heart defects.
The situation of children with CHD and their families is often complex, resulting in a
complicated psychosocial existence involving hospitalizations, dependence on the
healthcare system, and stress to the patients, their parents, and families (26–28).
Professionals face constant challenges in meeting the needs of these children and
their families, helping them deal with the complexity of this situation. As the number
of patients who survive grows, so to does the need for both medical and psychological
care (17). At the same time that paediatric cardiac care is evolving, socioeconomic
changes are also occurring, for example, in the social insurance system. Such changes

2 | A n n a - L e n a B i r k e l a n d
affect the already vulnerable paediatric cardiac patients and their families (29, 30).
The lack of holistic care may therefore also have economic consequences for these
children and their families/parents, with the risk of worsening financial conditions
(31).
Along with increased investments in medical technology, treatment, and care for
children with CHD, the psychosocial situation of these patients needs further
development and exploration (17, 23, 32). Studies from a psychosocial perspective
with a focus on quality of life that highlight the need for further research in this area
reveal a psychosocial perspective in paediatric cardiac care, thereby contributing to
improved quality of life for children with heart disease and their families. Bio-
psychosocial models that integrate a biological perspective have increasingly been
advocated for evaluating the effects of healthcare. The World Health Organization
(WHO) has been involved in the development of such a system addressing quality of
life, namely, the ICF-C4 (33).
Theoretical framework
The theoretical points of departure are quality of life (QoL) (34), stress – coping (35,
36), and psychosocial approach (37) including support, profession, and teamwork.
Quality of life
The aim here was to describe the complexity of the situation and contribute to an
overall picture of the psychosocial situation of children with CHD. The QoL concept is
relevant because its definition is multifaceted, representing a complex composition of
various aspects of human life and of the individual’s perception of his/her life
situation – i.e., the culture and value systems in which people live as related to their
goals, expectations, benefits, and concerns (34). The QoL concept is integral to many
scientific disciplines and is interdisciplinary in nature, which enables and creates
opportunities for exchanging knowledge between disciplines and professions, such as
philosophy, sociology, economics, psychology, and medicine. This is a good starting
point from which to describe and understand the complexity of the psychosocial
situation of children with CHD.
Lindstrom presents a relevant theoretical summary of the QoL concept in The
Essence of Existence (34); the model used in the present thesis is based on parts of
Lindström’s theoretical model. In healthcare research, the conceptual content has
shifted towards the health-related quality of life (HRQoL) concept (38), which is a
multidimensional concept that includes domain related to physical, wellbeing and
social functioning. It goes further than direct measures of population health, and
focuses on the impact health status has on quality of life (38).
I n t r o d u c t i o n | 3
Various instruments and questionnaires have been developed to measure the child’s
HRQoL. Some instruments are designed to assess the effects of the treatment of a
disease, while others analyse how a particular disease affects QoL.
Examples of instruments for measuring QoL in children with chronic diseases
include PedsQoL (Paediatric Quality of Life Inventory) (39), DisabKids (40), and
Kidscreen (41). PedsQoL includes a specific cardiac module (42), and another
cardiac-specific HRQoL instrument is the Paediatric Cardiac Quality of Life
Inventory (PCQLI) (43). At the time that we planned this study, however, no such
instruments were normed for use in Sweden. We also hoped to capture QoL from a
broader perspective in order to characterize the complexity associated with children
with cardiac disease using a method that would allow us to measure and describe
their psychosocial situation in general. Moreover, the age range of the studied
children was large, and it was difficult to find an instrument that covered all ages.
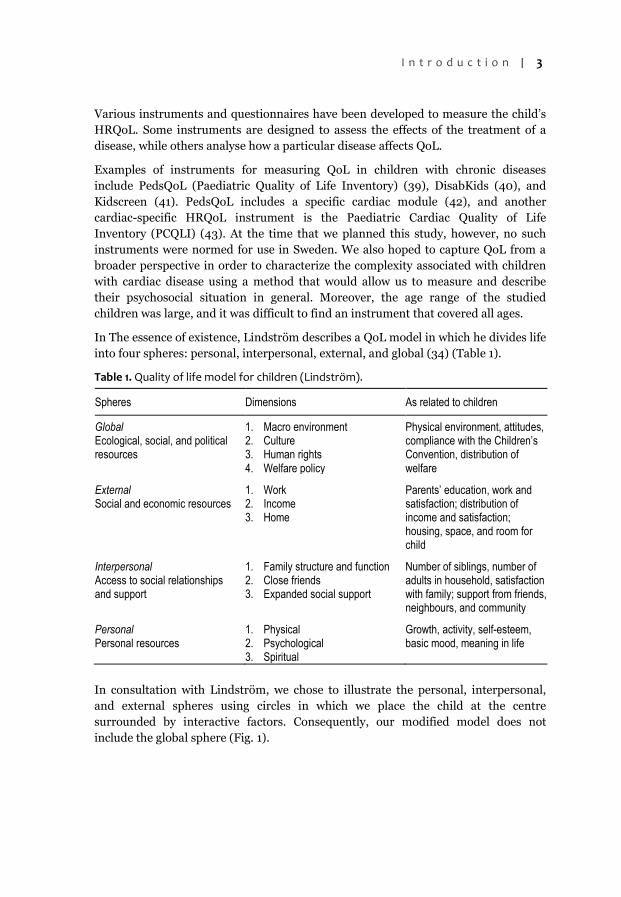
In The essence of existence, Lindström describes a QoL model in which he divides life
into four spheres: personal, interpersonal, external, and global (34) (Table 1).
Table 1. Quality of life model for children (Lindström).
Spheres Dimensions As related to children
Global Ecological, social, and political resources
1. Macro environment 2. Culture 3. Human rights 4. Welfare policy
Physical environment, attitudes, compliance with the Children’s Convention, distribution of welfare
External Social and economic resources
1. Work 2. Income 3. Home
Parents’ education, work and satisfaction; distribution of income and satisfaction; housing, space, and room for child
Interpersonal Access to social relationships and support
1. Family structure and function 2. Close friends 3. Expanded social support
Number of siblings, number of adults in household, satisfaction with family; support from friends, neighbours, and community
Personal Personal resources
1. Physical 2. Psychological 3. Spiritual
Growth, activity, self-esteem, basic mood, meaning in life
In consultation with Lindström, we chose to illustrate the personal, interpersonal,
and external spheres using circles in which we place the child at the centre
surrounded by interactive factors. Consequently, our modified model does not
include the global sphere (Fig. 1).

4 | A n n a - L e n a B i r k e l a n d
Personal
Interpersonal
External
Figure 1. Quality of life model for children.
According to Lindström, for life to be rich in quality, key components must be
included in the QoL concept and these areas of life must be important to the
individual. According to Table 1, Lindstrom’s model is covered by resources
distributed between four spheres/systems: personal/individual resources, family and
other interpersonal resources, social and economic resources, and social and political
resources. According to the model, families define QoL and what improves it. If
family members receive help with the problems for which they feel they need help, a
serious illness or handicap does not have to reduce their QoL.
In recent years, research has focused on understanding and describing QoL. We can
follow developments in this field in a review by Lindström and Eriksson (38). A key
researcher in this field is Antonovsky, who contributed to our understanding of
salutogenics (44). Antonovsky’s research focused on what causes people to become
and remain healthy, i.e., the origin of those factors that are salubrious or salutogenic.
The concept of sense of coherence (SOC) was Antonovsky’s answer to the question of
what renders life salutogenic (44, 45). According to Antonovsky (45), SOC is a global
orientation expressing a pervasive, enduring, and dynamic feeling of confidence that
the internal and external worlds are predictable, and that there is a high probability
that things will go as well as can reasonably be expected. SOC can be divided into
three components: comprehensibility, manageability, and meaningfulness. An

I n t r o d u c t i o n | 5
individual with a high SOC understands what is happening in a given situation, can
manage the situation, and sees meaning in what is happening, while an individual
with a low SOC perceives the situation as incomprehensible, unmanageable, and
meaningless. According to Antonovsky, comprehensibility refers to how a person
experiences internal and external stimuli, either in the form of order, clarity,
structure, and coherence, or as incoherent and inexplicable chaos and ambiguity.
Manageability refers to the capacity of an individual to cope with problems, using the
available personal or external resources. Meaningfulness is the third component of
SOC, and people with a high sense of meaningfulness feel it is worth dedicating
energy and commitment to solving problems. They view life with confidence and
believe that life has purpose and meaning (45, 46). The strength of Antonovsky’s
theory of SOC is that it focuses on a person’s entire “lifeworld” and how events and
circumstances shape how the individual sees him- or herself. Antonovsky believes it
is a person’s overall view of life and not one-time events that affect health. According
to Antonovsky, it is mainly the environment surrounding the individual that affects
health, and a low SOC can be changed with the right interventions. Converted to the
QoL concept, this means that, regardless of disease or other stress, a high sense of
context can contribute to a higher QoL.
Stress - Coping
Key life events such as divorce, grief, unemployment, illness, the addition of a new
family member, or the illness of a child may be consistent with the definition of
stressors and events to which the individual has no automatic response.
Karasek uses the demand–control model to describe how psychological and physical
stressors in life and the decision latitude of the individual affect health (47).
According to Karasek, experiences of stress are related to how well an individual
responds to two protective psychological mechanisms: the “alarm reaction” and
“adaptation”. The “alarm reaction” is the physical reaction that occurs when we are
confronted with dangers, such as information about the serious illness of a child.
“Adaptation” or coping means that we learn what stimuli in the environment no
longer pose a threat to us and adapt to this knowledge. It is crucial that people adapt
to such conditions, otherwise the risk of both psychological and physical collapse is
fairly great. When one of the “alarm reaction” or “adaptation” mechanisms does not
work, what we call stress arises. A situation characterized by high demands combined
with weak ability to control risk leads to stress and “strain”, a situation that the
individual and, in our case, the family wants to avoid. Karasek and Theorell (48)
divide the psychological demands of the sort experienced by the studied families into
two types: cognitive and emotional. People have to cope with situations they are
unprepared to cope with either cognitively or emotionally. The control in their model
also has two facets, involving the personal ability to cope with the situation that
arises, and the positive opportunity for growth. Even extremely pronounced negative
stress of the type addressed here can generate positive growth. Another measure of

6 | A n n a - L e n a B i r k e l a n d
negative stress is whether the individual personally experiences the conditions as
stressful and psychologically demanding.
Coping is defined as constantly changing cognitive and behavioural efforts to manage
specific external and/or internal demands that are appraised as taxing (49) or
exceeding one’s resources (50). A range of coping behaviours has been identified.
Lazarus et al. distinguish between problem-focused and emotion-focused coping:
problem-focused coping involves confronting a problem to reduce the effect of a
stressor, while emotion-focused coping involves dealing with the emotional distress
occasioned by the stressor.
A key element of the adaptation concept is that of successful coping. When an
individual and a family has encountered adversity and coped well with the challenge
of, for example, having a child with heart disease, they have used various individual,
family-related, or societal coping resources. All these capacities are defined as factors
that can promote good outcomes despite adversity. The capacity to overcome,
endure, or handle life problems in a productive way can also be described as
resilience, which also implies that individuals can develop and be strengthened by
adversity. Walsh et al. (51) define resilience “as the capacity to rebound from
adversity, strengthened and more resourceful … It is an active process of endurance,
self-righting, and growth in response to crisis and challenge … the ability to
withstand and rebound from disruptive life challenges” (p.4.). The SOC model of
Antonovsky with its holistic view of health fits well within a resilience model. From a
broader perspective, resilience depends on a bio-psychosocial model, as
genetic/hereditary and psychosocial resilient factors can promote good outcomes
even after very negative life experiences (52).
Compas et al. describe the relationships between coping and other reactions to stress
(53). Mackay (54) summarizes these relationships as follows: “Coping is a conscious
intentional response to stress. Coping is often invoked to represent competence and
resilience. However, these three terms have distinct meanings. Where coping refers
to adaptive response to stress, competence refers to the characteristics needed for
successful adaptation, and resilience is reflected in outcomes where competence and
coping” have been displayed (p. 105). In any case, over time, these terms and
concepts have formed the building blocks of our understanding of how individuals,
children, and families manage and adapt to stressful life events and living conditions.
Psychosocial approach
The psychosocial concept is included as part of the theoretical framework in this
thesis, and what follows is an overview of the concept and how it is used. The
Encyclopaedia Britannica and the Swedish National Encyclopedia describe the word
psychosocial as referring to the relationship between social factors and individual
beliefs and behaviour (55). The social conditions of an individual may cause
psychological reactions and vice versa. Factors that can affect the psychosocial

I n t r o d u c t i o n | 7
situation of an individual either negatively or positively include grief, joy, love,
illness, finances, work, and the surrounding environment.
Applying a psychosocial approach to clinical practice involves taking account of how
the social and psychological life environments of the individual influence the human
body; for example, physiological effects, behaviours, psychological, and physical
illness.
“Psychosocial” is not a new concept, but can be traced far back in the history of
professional social work (37). In 1941, the social work theoretician Gordon (56), a
representative of the diagnostic school, said: “We must study the whole... Without the
whole, we cannot understand the parts, nor can we understand the whole without the
parts”. She also coined the concept of “the person-in-the situation” with a particular
emphasis on the interaction between the person and the situation. Bernler and
Johnsson (37) define psychosocial work as the social work carried out with
individuals, families, and groups for preventive purposes; they also believe that
studying and understanding the figure/person in question/situation, as described by
Gordon, entail having a psychosocial approach.
The psychosocial approach entails seeing the individual in the context in which
physical, psychological, and social factors interact, having a crucial impact on the
development of a person’s identity and life situation. According to Bernler and
Johnson (37), this approach describes an understanding or attitude in working with
people. Psychosocial work, as described above, takes into account the personal,
interpersonal, and external spheres and, for change to occur, may require
interventions/support in one or more of these spheres.
To describe the practical work based on this approach, we talk about psychosocial
work/treatment, which can be said to be a generic term for the methods within social
work used in relation to individuals, families and groups for preventive or treatment
purposes (57). In the context of this thesis, the psychosocial approach encompasses
various methods for strengthening the resistance of the child/family to external
adversities and making changes in the social environment that would enable the
child/family to better cope with threatening situations (27).
Support
One resource in this effort to cope with stress and strain has been identified as “social
support”, a positive factor that is expected to have a dampening effect on perceived
stress (37). Many providers of medical, nursing, and psychosocial services state that
they use social support as a method. Epidemiological research defines social support
as the presence of people in the vicinity of the individual who can help the individual
with both emotional and practical problems. Bernler et al. believe that certain
activities must be taken to be able to call something support (37, 58). They argue that
support should not be considered just a method of work, but as a component of all

8 | A n n a - L e n a B i r k e l a n d
social work, from the first session to the last. In this context, support entails creating
a treatment relationship based on trust. Social support can be divided into two
components, i.e., emotional and professional support, so families may receive
support from friends and acquaintances, as well as from doctors and other healthcare
professionals.
The various methods of psychosocial work can be collectively defined as general
targeted interventions or preventive psychosocial work, that entail informing and
educating various types of groups (57, 58), for example, team development,
educational initiatives, and staff supervision. Psychosocial work in paediatric cardiac
care also aims to improve the psychosocial prognosis of the child and family subject
to the limitations imposed by the cardiac disease (57). The profession offers
individual and family-focused interventions including counselling, identification of
psychosocial situations, information, as well as support for the stresses, strains, and
interaction between involved parties.
Profession
A primary purpose of encounters between patients and professionals is to generate
feelings of trust. In today’s society, the various roles involved in the healthcare
professions, such as those of the doctor and nurse, must meet dual demands, i.e., for
professionalism in the sense of effective treatment based on scientifically proven
experience and for emotional skills when meeting with clients (59, 60). The
professionalism of the healthcare approach increasingly tends to include both
cognitions and emotions, and the discussion that the work should benefit the patient
(60). Consequently, the personal emotions and needs of healthcare staff must be held
in check in favour of displaying respect, interest, and warmth and taking a personal
approach (61).
Emotional work as a concept was recognized in 1979 by Hochschild (62). She
demonstrated that emotional work tended to be invisible, something that did not
count, a kind of voluntary work that, on top of ordinary professional tasks, was often
perceived as burdensome. Many professions have been studied from this perspective.
In a 2002 study of the working conditions of nurses, Bones (63) identifies change
processes in healthcare practices that influenced the emotional work of nurses and
how they perceive those changes (63). Bones found that the combination of
“invisible” emotional work and clinical/documentary work was perceived as
extremely stressful, but that some nurses managed to coordinate the two modes and
satisfy the conflicting expectations of their professional role.
In modern society, trust is increasingly contingent and vulnerable, particularly as it
pertains to the role of the doctor, who is highly dependent on real and perceived
professionalism. British sociologist Anthony Giddens describes this in terms of trust,
which has two faces: one assumes an objective and appropriate treatment, while the
other is based more on who a person is and his/her relationship to the professional

I n t r o d u c t i o n | 9
party. Giddens argues that modern society requires that people trust each other and
that this trust also applies to strangers. For example, patients have the right to expect
the same treatment from doctors and other healthcare professionals as do any other
people in the same situation. Society is quite simply based on this foundation, and
trust is the glue that creates societal cohesion and effectiveness. Consequently, if
meetings between a professional and a client fail because the professional does not
meet client expectations, trust in the professional will be shaken and, by extension, so
will trust in the entire profession and ultimately in professionals in general.
Something valuable is created in these meetings, which Giddens describes as “access
points”. People assume each other’s roles in these meetings, at best resulting in “joint
ventures” or at worst generating disappointment and distrust (64).
Team
The various professions involved in interprofessional work associated with children
with CHD are confronting a rapid increase in relevant knowledge. Because of this
knowledge proliferation, no single person can have even an overview of all existing
knowledge in the field. This means that case management requires interprofessional
teams consisting of representatives of various professions, who jointly handle the
complexity and associated challenges of the patient’s psychosocial situation (65, 66).
In this regard, paediatric cardiology teams (PCT) meet the needs of patients and their
families, as well as of the professionals involved in their care.
Teamwork can be viewed from various theoretical perspectives. From the
perspectives of organizational theory and efficiency management, teamwork can be
regarded in terms of decision-making, goal attainment, and interpersonal dynamics
(67, 68). A team can also be understood through the lens of group development
models in which the team is perceived as developing in more or less fixed sequential
stages (69). The concept of team is frequently used in healthcare without being
defined, but implicitly refers to a group of people who to some extent coordinate their
actions. How the terms “multidisciplinary”, “interdisciplinary”, and
“interprofessional” are used is complex and problematic, and they are not interpreted
uniformly or coherently in healthcare (70–72). In the multidisciplinary team,
consultations are arranged, but little or no communication occurs between the
various specialists. Interdisciplinary teamwork, while also based on individual
assessment, is followed by meetings in which team members seek consensus (73).
The theoretical framework of interprofessional teamwork, as mentioned above, is
extensive (74). Hall and Weaver (75) and Kvarnström (76) have discussed the
interaction and mutual dependency of team members, and their responsibility for
patient care, as a continuum extending from “multi” through “inter” to “trans”.
Freeth (77) defines teamwork as “the process whereby a group of people, with a
common goal, work together, often, but not necessarily, to increase the efficiency of
the task in hand” (p. 16). Overall, the team’s role is to see itself in a larger context,

1 0 | A n n a - L e n a B i r k e l a n d
reflecting on patient conditions, on team organization and mission, and on meetings
with patients, colleagues, and other professional (78, 79).
Transition
As one objective of this thesis is to elucidate the psychosocial complexity of the
situations of children with CHD and their families, transition in the context of CHD
could have been a theoretical framework (80). Transition is a middle-range theory
that covers the ambition to understand complex situations and represents a concept
that could also be used as a tool to describe and understand specific and practical
phenomena (80). In this thesis, however, we chose a theoretical framework
combining multiple theories that cover the ambition and aim of this thesis.

M e t h o d o l o g i c a l f r a m e w o r k | 1 1
METHODOLOGICAL FRAMEWORK
This thesis aims to build a deeper understanding of what children with heart disease
and their parents experience by highlighting in various ways the psychosocial
situation of children with cardiac disease. By combining qualitative and quantitative
methodologies and approaches, we broadened the database, resulting in a more
reliable basis for interpretation, improving the possibility of describing the target
group in terms of the complexity of heart disease and allowing for a deeper
understanding of this group’s needs (81–85). Specifically, we combined methods
involving both quantitative data collection and interviews. Quantitative methods
were used in studies I and IV, while qualitative methods in the form of qualitative
research interviews/themed individual and group interviews were used in Studies
II-IV.
Quantitative methods
Structured interview: Study I
The QoL model, previously described as part of the theoretical framework (Table 1,
Fig. 1), was operationalized, resulting in an instrument for assessing the psychosocial
situation of children with heart disease. The research group formulated a new
instrument because at the time of the study no standardized cardiac-specific
instrument for children was available and no single existing instrument could supply
the comprehensive information desired. In addition, except for one subject who was a
grown-up CHD (GUCH) patient, the studied children and adolescents were aged 0–
18 years, which made it difficult to find a scale that covered the entire age span.
Accordingly, an interview-based instrument using structured questions about
psychosocial symptoms was developed. The questionnaire was divided into items
covering the personal, interpersonal, and external spheres. The personal sphere
describes symptoms directly related to the child. The interpersonal sphere describes
symptoms related to the child’s immediate circle, i.e., family, friends, and school. The
external sphere describes symptoms related to medical care, social services, and
finances. Psychosocial symptoms were registered using the questionnaire. An
experienced clinical social worker interviewed the children and their parents. The
interviews covered the predetermined symptom areas. When developing the
assessment instrument, various rating scales and assessment instruments were used
to delineate and define issues such as CBCL (86, 87), definitions from DSM-IV (88),
diagnoses of certain diagnostic areas and the GARF relationship assessment (88),
and the SOFAS functional rating scale (88) from DSM-IV (88, 89).
The symptom areas assessed in the children were based on DSM-IV. GARF (88) was
used to describe family symptoms in the interpersonal sphere. Certain themes
regarding the interpersonal functional problems of the children were taken from the

1 2 | A n n a - L e n a B i r k e l a n d
SOFAS scale (Appendices I and II in Study I). Support for the above approach, citing
examples from various instruments, can be found in the Comprehensive Handbook of
Social Work and Social Welfare (90).
Symptom severity was evaluated and scored using a four-point Lickert scale ranging
from 0 to 3, where 0 indicates no symptoms, 1 mild symptoms, 2 moderate
symptoms, and 3 severe symptoms. A manual was formulated to guide the
questionnaire administration and to determine the weighting of the symptoms (Study
I, Appendix II).
Questionnaire: Study IV
This questionnaire comprised an inventory of 19 questions (Study IV, Appendix I).
Initially, background data were requested: respondent profession, size of catchment
area, number of children enrolled, and number of visits per year. Team organization
was covered by six items, followed by a question containing seven variables, relating
to team function and tasks. Under the heading “Way of working” was items about
meeting frequency, memos, documentation, and organized networking events.
Finally, inquiries were made about team members’ attitudes to teamwork, thinking
about teamwork, and views of what characterizes good teamwork.
Qualitative method
Studies II–IV
The method used to analyse the texts/interviews was interview analysis in the form of
qualitative content analysis (91). The actual process can vary, but the following
description according to Granheim and Lundman (92) applies to the process we used
to analyse the interview texts. The entire text (i.e., analysis unit) was first read
through several times to gain a sense of the whole. Particular sentences or phrases
containing information relevant to specific issues were selected; surrounding text was
included to preserve the context of these passages, which constituted meaningful
units. These meaningful units were condensed to shorten the text while retaining all
the content. The condensed meaningful units were coded and grouped into categories
reflecting the core message of the interviews. These categories represent the manifest
content. Finally, themes were formulated to reveal the latent content of the
interviews.
Study II
In this study, which was based on themes from the above-mentioned personal,
interpersonal, and external spheres (Fig. 1, Table 1), the parents and siblings of
children with CHD were interviewed on two occasions ten years apart. The
interviews, which were semi-structured and lasted two to two and a half hours, were

M e t h o d o l o g i c a l f r a m e w o r k | 1 3
all conducted by one of the authors. The interviews sought to trace the path of the
child and family through their experience of the disease and covered the following
topics: course of the disease, medical care, the child with heart disease, perspectives
of family members, and support. Follow-up interviews, also based on the three
spheres, were conducted with siblings and parents after ten years. Data were
analysed using content analysis.
Study III
Nine experienced paediatric cardiologists were interviewed for one and a half to two
and a half hours each. All interviews were carried out by one of the authors. The
interviews were semi-structured, covering five themes and including follow-up
questions and opportunities for the interviewee to add personal reflections – the
interviewed cardiologists were given great latitude to describe their experiences and
provide in-depth information (81). The main themes were the doctor’s self-
presentation, professional attitudes, and encounters with parents as well as the
messages they conveyed to patients and their families. These themes included topics
such as access to evidence-based knowledge, emotional reactions, and the balance
between proximity and distance in client meetings. Two researchers, a medical
sociologist experienced in qualitative data analysis and a paediatric cardiologist, read
and independently analysed the decoded data, identifying the main themes. Data
were analysed using content analysis.
Study IV
Six PCTs selected by size and location were studied via focus group interviews. The
focus group interview was considered a natural environment in which team members
could share their experiences and opinions and be inspired by each other (93). The
interviews, which lasted one and a half to two hours, were all carried out by one of the
authors. The interviews were semi-structured and team members were given great
latitude to describe their experiences and provide in-depth information (81). An
interview guide covered the following topics from the questionnaire: organization
and way of working, function/task, attitude/approach, communication, and
challenges facing the team. All data were subjected to qualitative content analysis (91,
92, 94, 95).
Statistical analysis: Studies I and IV
Results were presented as means, medians, and percentages. Differences between
groups were analysed using contingency analysis (chi-square test, Fisher’s exact test).
A p-value less than 0.05 was considered to be statistically significant. The Statistical
Package for the Social Sciences (SPSS/PC) and Microsoft Excel were used for
statistical analysis of the data.

1 4 | A n n a - L e n a B i r k e l a n d
ETHICS
All methods and the project as a whole were approved by the Research Ethics
Committee of Umeå University on 14 February 2000; additions to the project were
approved by the Regional Ethical Review Board of Umeå on 24 August 2010.
Before each questionnaire survey or interview, respondents were given information
about the purpose of the research, why we were interested in their participation, and
their rights as research participants, such as the right to withdraw from the study at
any time without specifying any reason and without affecting their right or access to
care and treatment. The information was provided orally in connection with visits to
the clinic and in writing by e-mail or regular mail.
While conversations/interviews could have therapeutic value, for example, by
facilitating the processing of past experiences, they could also rekindle past traumas.
The present interview studies were conducted by an interviewer with extensive
clinical experience in counselling; this ensured an approach to people and interview
material that included professional assessment during the session of the need for
follow-up. The ethical implications of the study did not entail any clear risk to the
respondents.

A i m s o f t h e s t u d y | 1 5
AIMS OF THE STUDY
The overall aim of the study was to increase our knowledge of the psychosocial
situation of children with CHD and of the professions handling them.
The specific aims were:
describe the psychosocial situation of the children/adolescents with CHD and
their families
explore the situation faced by parents and siblings initially and over time
investigate the approaches used in encounters between paediatric cardiologists
and the families of affected children
describe PCTs in Sweden and their approaches to their work
The specific aims to be achieved throughout the research process were addressed in
four studies exploring the three inner spheres of the QoL model (34) (Fig. 2).
Interpersonell
Extern
Personell
I
II
III
IV
I
I
II
I ComplexityII CopingIII ProfessionIV Team
Figure 2. Study I deals with the psychosocial complexity in personal, interpersonal and external spheres. In Study II, describing the strategies for mainly the surrounding family, the interpersonal and external spheres were explored. The paediatric cardiologists and the paediatric cardiology team, in the external sphere, are described in Study III and IV.

1 6 | A n n a - L e n a B i r k e l a n d
Overview of the research process
Clinical realities, together with the goals of treating children with CHD holistically
and of developing a more patient-centred approach, shaped the research team efforts
to inventory the psychosocial situation of children with CHD.
The inventory revealed the complex situation of children with CHD and their
families, in the personal, interpersonal, and external spheres, which illustrated and
clarified several levels of needs. The results indicated the complexity of the situation
in which children with heart disease and their families live (Study I). Children with
heart disease, along with their parents and siblings, have to cope with and adapt to
complexity and vulnerability and find a path through these life circumstances.
Naturally, the next step in the research process was to describe the experiences and
coping strategies of these patients and families. The experience of being informed of
the diagnosis and of the needed interventions was described as highly emotional and
still affected the lives of the children and their families 10 years later. Parents stated
that the doctors and the approaches they used were important and that, in particular,
receiving the news about the heart defect was central to their experience (Study II).
Doctors and their profession thus came into focus during the research process
(Study III). Interviewed paediatric cardiologists described the challenges and
expectations in dealing with the encountered complexity. For example, the diagnosis
process entailed breaking the news of the heart disease and dealing with the resulting
emotions of the children and parents (as well as the doctors’ own emotions), which
emphasized the dependence on the team doing its job. As part of the research interest
then shifted to the team (Study IV). The team’s challenge was to manage the
increasing complexity at both the family and organizational levels; this required
representatives of several professions and various team-development initiatives,
depending on the conditions of the team in question (Study IV).
Study groups
I. Ninety-seven children/adolescents with CHD, enrolled by means of consecutive
selection, were sorted into three categories with respect to complexity of CHD.
Group I included 42 patients with malformations requiring standardized
operations, group II included 20 patients with more complicated malformations,
and group III included 35 patients with very complex malformations. The patients
were compared with controls without heart disease, matched for age and gender
(Table 2, Fig. 3).
Table 2. The age distribution of the studied patients and of the age- and gender-matched
control group in Study I.
Age (y) n
0–4 42
5–9 29
10–14 10
>15 17
A i m s o f t h e s t u d y | 1 7
Children with CHD and their families Age and gender matched healthy
Children and their families
97
8
97
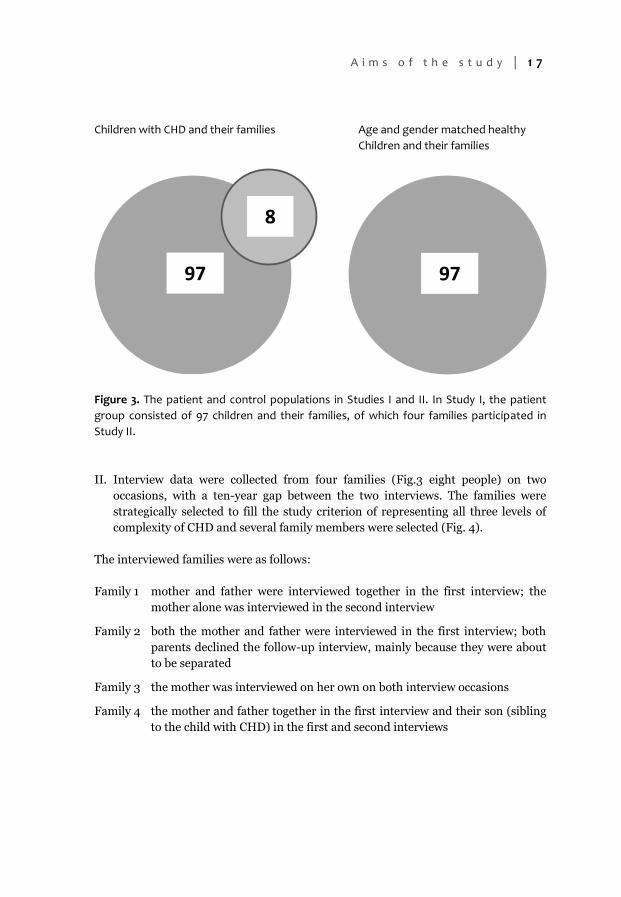
Figure 3. The patient and control populations in Studies I and II. In Study I, the patient
group consisted of 97 children and their families, of which four families participated in
Study II.
II. Interview data were collected from four families (Fig.3 eight people) on two
occasions, with a ten-year gap between the two interviews. The families were
strategically selected to fill the study criterion of representing all three levels of
complexity of CHD and several family members were selected (Fig. 4).
The interviewed families were as follows:
Family 1 mother and father were interviewed together in the first interview; the
mother alone was interviewed in the second interview
Family 2 both the mother and father were interviewed in the first interview; both
parents declined the follow-up interview, mainly because they were about
to be separated
Family 3 the mother was interviewed on her own on both interview occasions
Family 4 the mother and father together in the first interview and their son (sibling
to the child with CHD) in the first and second interviews

1 8 | A n n a - L e n a B i r k e l a n d
F
FB
M
F M
F M
1 1
1
2
2
11
Family 1 Family 2
Family 3Family 4
F = female, M = male, B = child
Figure 4. Illustrates the interviews in Study II. 1 = first interview, 2 = second interview.
III. We interviewed nine experienced paediatric cardiologists working at a tertiary
care centre for paediatric cardiology at a Swedish university hospital,
counselling families of children with CHD. One paediatric cardiologist also
participated in the focus group interviews (Fig. 5).

A i m s o f t h e s t u d y | 1 9
309
6
Figure 5. Paediatric cardiology teams/paediatric cardiologists.
In Study IV, 30 PCTs were involved in an inquiry, of which six teams participated in
focus interviews. Nine paediatric cardiologists were interviewed in Study III, one of
whom participated in the focus interviews.
IV. A national inventory/survey of all 34 PCTs was performed. Qualitative focus
group interviews were conducted in six PCTs selected by size and location
(Fig. 5).

2 0 | A n n a - L e n a B i r k e l a n d
RESULTS
Study I: Complexity
The complexity of the psychosocial situations of children and adolescents
with congenital heart disease
Aim
This study described the psychosocial situation of children/adolescents with heart
disease and their families.
Design and results
This study used questionnaire and quantitative data obtained from a group of 97
children and adolescents with CHD of different degrees of medical complexity and to
a control group.
In the patient group, 20% displayed one or more psychosocial symptoms evaluated as
severe, while in the control group the corresponding proportion was 1%. The three
grades of medical complexity differed regarding number and severity of psychosocial
symptoms: the children with the most complex CHD had the highest number of
moderate and severe symptoms, while those with the least complex CHD had mostly
mild psychosomatic symptoms. The most frequent symptoms in the whole patient
group in terms of the three spheres were healthcare and treatment-related needs in
the external sphere, family symptoms in the interpersonal sphere, and
mental/somatic/psychosomatic symptoms in the personal sphere.
Comparison of the patient and control groups indicated about the same overall
frequency of symptoms in the personal sphere, but that a larger proportion of the
patient group experienced psychological symptoms such as depression, anxiety,
loneliness, behavioural problems, and concentration problems, as well as
psychosomatic symptoms such as headaches and stomach pain, while more
children/adolescents in the control group had allergic, speech, and language
problems. Statistical analysis (Chi2 test, Fisher’s exact test) indicated that the
frequency of anxiety symptoms (p <0.002) and difficulties concentrating (p <0.001)
was significantly higher in the patient group than in the control group (unpublished
data). Headache problems were 15 times more common (p <0.0001) and stomach
pain twice as common (not significant) in the patient group than in the control group
(unpublished data). In the patient group, symptoms in the interpersonal sphere were
much more common (p <0.0001), especially when it came to family symptoms such
as crisis problems, parental desertion, and family interaction problems. Even in the
external sphere, a major difference was observed, with the patient group experiencing
more problems in most areas, including both clearly illness-related matters, such as
medical and rehabilitation needs, and matters relating to finances, insurance,
education, and transportation (p <0.0001).

R e s u l t s | 2 1
In conclusion, Study I elucidates the psychosocial complexity in children and
adolescents with CHD, indicating the need for structured psychosocial care
programme.
Study II: Coping
Facing bad news: a case study focusing on families having a child with
congenital heart disease
Aim
This study explored the experiences among parents and siblings to children with
CHD during the diagnostic phase and how family members dealt with the situation
over time.
Design and results
Interview data were collected from four families on two occasions, with a ten-year
gap between the two interviews. The analysis of the data revealed five main themes
and subsequent sub-themes
Table 3. Teams and subthemes revealed during the analysis.
Themes Sub-themes
Information about the diagnosis evoked overwhelming feelings
Reacting with stress, shock and confusion Feeling shame and guilt Feeling fear and anxiety Considering the situation as unfair Losing control
Ambivalence towards medical interventions and technology
Being dependent of others Lacking trust Feeling powerless and helpless Feeling lonely
Needing medical, social and emotional support and relief
Expecting medical and practical information Processing crises by counselling Asking for continuously support
Finding pathways to new perspectives Gradually getting additional information Well-functioning line of communication Professionals being present and giving time
Outlook of life and future change over time Gaining life experiences Getting increased self-knowledge and self-confidence Getting Increased acceptance Revaluing material conditions Having confidence in the future

2 2 | A n n a - L e n a B i r k e l a n d
Information about the diagnosis evoked overwhelming feelings: Our findings
indicated that receiving news of a child’s disease can be described as a turning point,
with effects persisting even after ten years. Regardless of the severity of the heart
disease diagnosis, the representatives of the studied families said that they were
initially shocked. Parents experienced feelings of guilt, anxiety, diffuse shame and
loneliness, and disappointment in life as such, perceiving the child’s disease as a
punishment. Surgical procedures and associated happenings were described as very
stressful. In addition to structural and relational circumstances, individual factors
proved very significant in shaping the studied families’ ability to cope, and these
factors also changed over time. What was common to our families was the stress this
news entailed, while their reactions and ways of evaluating and dealing with the
problems varied over time.
Ambivalence towards medical interventions and technology: The parents described
it as very stressful and mentally demanding to have to depend on others and not
always to understand what they were experiencing. They said that it was sometimes
difficult to have trust in the consequences of the major therapeutic interventions and
efforts required.
Needing medical, social, and emotional support and relief, finding pathways to new
perspectives, and outlook on life and future change over time: When the initial
shock at the diagnosis had abated and the parents had begun to formulate questions,
they experienced a growing need for contact with health care professions and
information. Access to social support from people outside the healthcare system was
highly variable. In both the short and long terms, well-functioning communication
between the families and medical personnel was essential. PCTs’ willingness to
communicate and to structure information in useful forms gained the families’ trust,
and the doctor’s professionalism in breaking the news was crucial. For all the
children with heart disease, the interviews revealed that the purely medical course of
events over the past decade was more positive than the parents had initially feared.
From a longitudinal perspective, we found effects even after ten years. The
interviewees said that their feelings had changed over time and that they now felt less
anxiety. Despite marked stress, living with and caring for a child with heart disease
proved manageable for the studied families.
Study III: Profession
Breaking bad news: an interview study of paediatric cardiologists
Aim
This study examined the approach of paediatric cardiologist in informing and
communicating with the family of the CHD patient.
R e s u l t s | 2 3
Design and results
Interviews with paediatric cardiologists focused on their encounters with families of
children with CHD. The interviews dealt with parent and patient counselling
throughout the cardiologists’ careers, including the counselling of parents whose
infants were diagnosed with complex CHD requiring some kind of interventional
procedure.
The interviewed doctors unanimously stressed the importance of good
communication when meeting with families, but their strategies for facilitating such
communication varied. Doctors’ strategies for meeting with families varied in terms
of structure, relationship, and degree of formality. Meetings ranged from a very
structured information meeting to a more flexible format, from relying on formal
guidelines to being shaped by the doctor’s personal experience, and from merely
providing factual information to accepting the emotionally charged nature of such
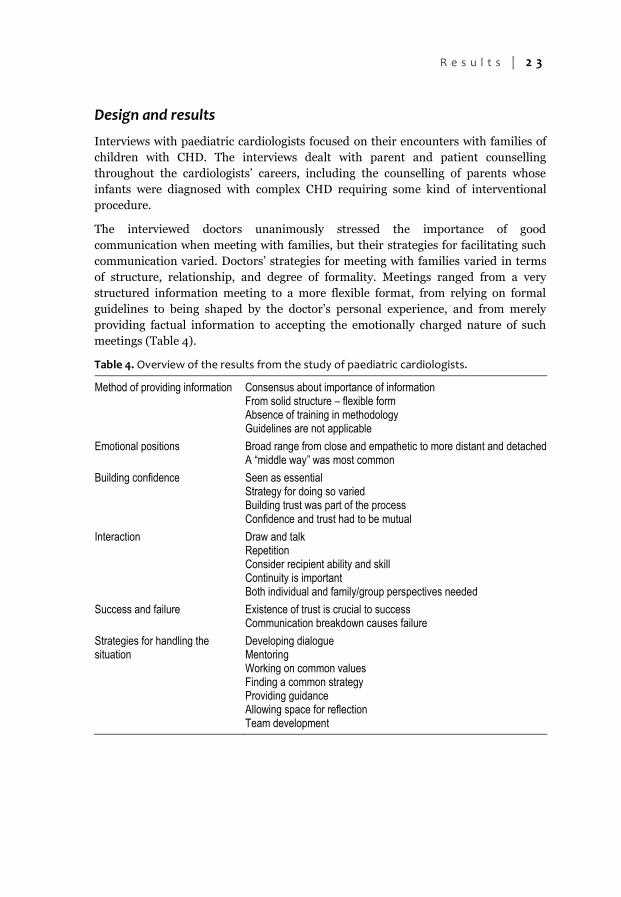
meetings (Table 4).
Table 4. Overview of the results from the study of paediatric cardiologists.
Method of providing information Consensus about importance of information From solid structure – flexible form Absence of training in methodology Guidelines are not applicable
Emotional positions Broad range from close and empathetic to more distant and detached A “middle way” was most common
Building confidence Seen as essential Strategy for doing so varied Building trust was part of the process Confidence and trust had to be mutual
Interaction Draw and talk Repetition Consider recipient ability and skill Continuity is important Both individual and family/group perspectives needed
Success and failure Existence of trust is crucial to success Communication breakdown causes failure
Strategies for handling the situation
Developing dialogue Mentoring Working on common values Finding a common strategy Providing guidance Allowing space for reflection Team development

2 4 | A n n a - L e n a B i r k e l a n d
Method of providing information: There was broad consensus among the
interviewed cardiologists that it was essential to provide complete and accurate
medical information. When it came to information provision, the doctors’ strategies
ranged widely from formally structured to more flexible. The cardiologists agreed
that they lacked training in information provision/conversational methodologies.
There was near consensus that general guidelines were not always applicable.
Emotional positions: Overall, the emotional positions employed ranged widely from
empathetic and close to more distant and detached; most doctors’ chose a “middle
way without being too close”, while some vacillated between closeness and distance.
Building confidence: Creating confidence in the patients and their families was
essential to the doctors’ information provision strategies. There was widespread
agreement that building trust was essential, and the cardiologists used various
strategies for doing so.
Interaction: Most of the doctors drew sketches, and many used repetition in meeting
the information needs of their patients and parents in a stressful situation. Most
considered the recipients’ communication ability when interacting with them.
Continuity between the physician and parents was considered important; likewise, it
was important to consider both individual and group perspectives.
Success and failure: Failure was described as resulting from communication
breakdown, while success arose when doctors and patients/families created mutual
trust.
Strategies for handling the situation: Existence of a common strategy, provision of
guidance, allowing space for reflection, and team development were mentioned as
tools for managing the complexity surrounding the child with CHD.
In conclusion, this study found that paediatric cardiologists stress the importance of
conveying bad news in suitable ways, building mutual trust, and adopting various
emotional positions in relation to the families. All cardiologists wished to improve
their ability to handle such situations and expressed a need to work on common
values, reflection, and education.
Study IV: Teams/PCTs
Teamwork in Swedish paediatric cardiology: a national exploratory study
examining function and dynamics
Aim
This study described the organization and function of PCTs in Sweden, and sought to
deepen our understanding of working in a PCT

R e s u l t s | 2 5
Design and results
A national survey of all 30 PCTs was performed by means of a questionnaire.
Qualitative focus group interviews were conducted with a total of 29 members of six
PCTs selected by size and location. One cardiologist participated in the focus
interviews (Fig. 5).
The questionnaire was answered by nurses in 17 of 26 PCTs, and the nurse was the
coordinator in 17 PCTs. All teams emphasized the need for consistency in dealing
with the child with CHD and the importance of analysing the team’s joint
responsibility for medical and psychosocial care in order to decide on a shared
holistic approach. All PCTs estimated, using a seven-point scale (1 = low estimation,
7 = very high estimation), the degree of teamwork experienced: one team rated the
teamwork at 5 points, eight teams at 6 points, and 17 teams at 7 points.
The complexity of the cases at both the family and system levels obviously required a
team of representatives of various professions. The PCTs tried to work in a structured
way, but team structure and composition differed, and problems arose because of the
working conditions. The cardiologist’s work, time, and interest were essential to case
progress. The complexity and constant change of the children’s cardiac care led to a
need for more cooperation within and between teams, and among the teams, team
physicians, child and adolescent psychiatry (CAP) services, habilitation organizations
(HOs), and school systems. All teams experienced more or less serious problems
communicating constructively with CAP and the HOs.
In conclusion, managing the continuously changing needs of children with CHD and
their families called for organizational alteration and action plans in PCTs. The teams
need to further develop their leadership capacity, resource coordination,
collaboration with organizational support, continuing education, and access to
coaching.

2 6 | A n n a - L e n a B i r k e l a n d
DISCUSSION
Children and young people with cardiac disease, together with their families,
represent a growing and somewhat new diagnostic group for which we cannot draw
generalized conclusions based on experience with other diagnostic groups. The
specifics of this chronic disease group, such as the complexity of their situation,
experience, and the invisibility of their handicap, with various crucial symbolic
implications, has consequences for their psychosocial care and treatment (17).
Emotional consequences, communication, information, and support are essential for
these children, parents, and families as well as for the professionals and PCTs
treating them. In an era of intensifying discussion of priorities and economic
austerity, it is even more important to analyse the consequences of an insufficiently
holistic approach. Provision of necessary resources for the psychosocial needs of
these children and adolescents and their families must be continuously monitored
and developed (2).
Complexity
A growing body of literature addresses questions concerning the QoL and living
conditions of children with CHD (17, 96–98). Latal et al. (17) conducted the first
systematic review of the last 18 years of literature on the psychological adjustment
and QoL of children and adolescents with CHD following cardiopulmonary bypass
surgery, noting methodological variations and restrictions that make it difficult to
compare studies and draw general conclusions. In this respect, there is a complexity
in the literature that must be addressed. As in this thesis, Latal et al. (17) note that
QoL is frequently used as a concept and methodology in understanding and assessing
the psychosocial situation in CHD (99); it represents a multidimensional construct
that includes social dimensions, stress, and emotional and cognitive functions. The
findings of our and other studies from the QoL and HRQoL perspectives can be used
to deepen our understanding of how to develop interventions for children with CHD
and for their families, with the aim of reducing psychosocial morbidity (100).
Neuner et al. (101) demonstrated in a 2011 study that sense of coherence (SOC) was
associated with overall wellbeing and with QoL sub-dimensions for adults with CHD.
Similarly, Moons et al. reflected on the correlations between a well-structured or
“high” SOC and the opportunity to improve QoL (102).
We developed a model illustrating the overall psychosocial situation facing children
with CHD and their families; this model has been useful in analysing and highlighting
various aspects of the psychosocial complexity of this patient population. In Study I
of this thesis research, the complexity of the psychosocial situation of child CHD
patients and their families was illustrated by the high frequency of symptoms in all
areas, i.e., the personal, interpersonal, and external spheres.

D i s c u s s i o n | 2 7
Personal sphere
In the personal sphere, children with CHD had significantly more problems with
depression, anxiety, and concentration as well as more behavioural problems.
Increased internalizing and AD/HD problems are seen in recent studies of children
with CHD (17). In our study, patients with CHD had a statistically significant higher
frequency of mental health and psychosomatic symptoms than did age- and gender-
matched controls.
The study group includes children who have been in a heart-lung machine, which
seems to be a risk factor for AD/HD symptoms (103). The stress of invasive surgical
procedures, hospital care, and the impact of having heart dysfunction are important
both symbolically and in reality and are thus important determinants of mental
health and QoL outcomes (98, 104).
A growing literature that highlights questions concerning the increased frequency of
mental health symptoms in children with CHD, as related to various risk factors,
supports the results of Study I (104, 105).
Interpersonal sphere
The most severe problems experienced by the studied CHD patients and their
families were seen in the interpersonal area, highlighting the family burden of living
with a child with CHD (106). This was even more obvious in comparison with
controls, who experienced significantly fewer family-related problems.
These results indicate, as Sarajuri and Brosig demonstrate (107, 98), that severe
congenital heart defects increase parenting stress. The described family symptoms
can also influence parent–child interaction, making parents less able to care for
children with CHD, rendering the child more vulnerable (16, 108-111). The findings
raised questions about whether the children’s, adolescents’, and families’ QoL has
decreased, but not in all sub-domains (17, 98). Like this thesis, Latal and Brosig’s (17,
98) demonstrate that these children may have behavioural problems. This finding
can mainly be associated with parental descriptions of the situation of the children
and family. Goldbeck and Melches (15, 16) and Solberg (112) find that parental QoL
was less associated with the severity of the child’s illness than with social risk factors,
such as being a single parent.
External sphere
Healthcare and treatment needs were frequent external sphere needs, as were, for
example, social service, financial, and travel/transportation assistance. Connor et al.
reached similar conclusions, examining the level of complexity in terms of the need
for resources and interventions from the healthcare system, the environment, and
society (31). Other authors exemplified this in a study from neonatal care (113). Care
based on a professional approach at all levels has long-term positive consequences for

2 8 | A n n a - L e n a B i r k e l a n d
children/young people with CHD and their families and helps eliminate the risk of
psychosocial sequelae (114, 115).
We identify a complexity of which is supported by the literature (26, 27, 31, 113, 114).
One approach to managing and structuring complexity is offered by the International
Classification of Functioning, Disability and Health (ICF), published in 2001, a
paediatric version of which has been available since 2007 (ICF-CY). The ICF-CY is
based on the diagnosis, but takes account of the “big picture” relating to daily
functions, symptoms, activities, and participation, as well as to household conditions
and social factors (33). The model we developed can be viewed as an earlier attempt
to showcase the psychological complexity of a specific patient population.
Coping – Stress
The difficult situation that the studied parents found themselves in when they
learned the news of their children’s illness changed their lives. We describe this
situation as a turning point (116) in life, but could also have chosen to describe it
using Strauss and Glaser’s (117) concept of “status passage”. It is hardly surprising
that a negative and decisive turning point in life, such as learning that a child suffers
from a serious heart disease, generates problems for the entire family, but our data
also indicate some positive trends, especially from a longitudinal perspective.
As demonstrated in Study II and other studies, being informed of their children’s
congenital heart defects commonly engendered stress and strain for the patients’
families, both at the time of being informed and over time (26–28, 111). Like various
authors (26, 27, 118), we find emotional reactions such as anxiety, fear, and a
changed way of valuing and dealing with problems, as well as a sensed burden of
responsibility and financial uncertainty (31). The present findings can be compared
with those of Menahem and Green (111, 119), who state that healthcare personnel, for
example, PCTs, have to be aware of and identify psychological ill health as a risk
factor for both parents and children. Parental descriptions of how the initial post-
diagnosis period with the child was fraught with anxiety and entailed many life
adjustments coincide well with the results of an interview study of parents of children
with cancer (120).
Arafa (121) found that 98% of parents of children with CHD worried about their
children’s health and future. In our study, especially in the early period of illness, the
parents describe worrying about the future; after 10 years, they still experienced
occasional bouts of worry and concern.
In addition to structural and communicative relationships relevant to the possibility
of dealing with the situation, individual factors relating to the parents and family also
played a role (122). These factors also appeared to change over time. Parental
wellbeing also appears to be related to the psychological adjustment of their children
(17, 123).

D i s c u s s i o n | 2 9
The parents describe finding a pathway when having a child with CHD and
summarize their previous life in terms of major life experiences that can strengthen
the couple’s relationship (122).
As an increasing number of children with CHD survive and require life-long follow-
up (14), it also becomes important to understand the mechanisms underlying the
behaviour of teenagers with CHD and their families (123). Zahmacioglu et al. (124)
believe that specific knowledge of coping strategies is needed for this patient
population and their families. Lazarus’ coping theory (35) underscores the interaction
between problem-oriented and emotion-focused strategies for action, and indicates,
as do our results, that individual factors are often crucial determinants of people’s
ability to orient themselves in situations of extreme stress. The present results are
consistent with Lazarus’ transactional stress model (50), in which emotions play a
dominant role, especially the interplay of emotions with cognitive assessments of the
action context and of the action strategies that therefore become relevant. We have
focused on three aspects of what Lazarus terms secondary appraisal. The first aspect
concerns the evaluation/assessment of who is responsible for the problem and to
what extent, and includes feelings of guilt and shame, as well as positive values such
as pride. Of particular interest here is the parents’ assessment of their own efforts.
The second aspect involves assessing the opportunities for dealing with the problems,
i.e., coping potential. Even here, we focus on the parents’ own opportunities as well
as those of the professionals, mainly doctors, with whom they come into contact. The
third aspect involves future expectations, an approach found to play a major role in
the communication patterns that we described. Secondary appraisal represents an
ongoing cognitive and emotional assessment of the situation in which the families of
children with CHD found themselves during the decade we monitored. This finding is
consistent with those of Lawoko (125), who describes how parents of children with
congenital heart defects initially experience crisis in the first year after being
informed of the diagnosis. Like our subjects, Lawoko’s subjects describe emotions
such as anxiety and anger, but these emotions change and improve. Lawoko’s results
also indicate that parents develop coping strategies and resilience. The families
examined in the present study display “resilience” that may depend on professional
support and networking, as Tak and McCubbin (126) also demonstrated. One
example of the resilience (127) of a family living with a child with CHD is presented
by Wray and Sensky (122), who describe how parents felt that their relationship had
strengthened during the period when their children underwent cardiac surgery.
Before surgery, these parents had stable relationships, which became even stronger
afterwards. Our study demonstrated that, despite marked stress, caring for a child
with CHD proved manageable for the studied families. The studied parents also
described how the shared experience of dealing with their child’s illness positively
developed their relationship.
In line with the results of other studies (17, 19, 128, 129), our results also indicate that
psychosocial complexity creates a need for psychosocial support for children and
adolescents with CHD and their families. Several studies illustrate the impact of this

3 0 | A n n a - L e n a B i r k e l a n d
complexity on daily life, examine mechanisms for coping with the situation, and
emphasize that support is needed and requested (104, 105, 126). Parents described
needing to fight for their children’s and their own rights. They described the
challenges of obtaining information in stressful situations, and said that they felt
responsible for informing others about what it means to live with heart disease in the
family. Parents describe receiving support from grandparents and social networks
(114, 115) and rating the support of healthcare professionals, the PCT, and the
paediatric cardiac clinic as very significant (114, 125, 128). Well-functioning
communication with the healthcare system (in this case, the PCT) in both the short
and long terms provided parents with essential help in managing the situation. As it
is paediatric cardiologists who often break the news of a child’s CHD, the
professionalism of their approach seems to be crucial to the families (130-135).
Profession
A key moment is when the doctor informs parents of their child’s heart problem
(2007). Like Menahem (136), we find that parents view this meeting, which sets the
course of their ongoing interaction with the healthcare system, as crucial and often
prolonged. Against this background, we found it important to study the attitude of
the paediatric cardiologists. The physicians came to play a central role in our study,
but their position in relation to the family could be assumed to be generalizable to
describe the professional aspects of the encounter with children with CHD and their
families.
While the interviewed doctors agreed on the importance of this initial encounter,
their views varied as to the requirements for a good encounter. One important
characteristic of the encounter is the degree of empathy displayed by the doctor, and
the question raised here is whether empathy is consistent with the professional role
of doctor (137). Is sharing how other people (in this case, the parents) experience
events a relevant response to the expectations these people have of the doctor, or
does it fall to other professional roles, such as the social worker or nurse?
Nevertheless, study III focuses on the role of the doctor and how it manifests itself in
the patient encounter. In the preface to their book Profesjonsstudier [Professional
studies], Molander and Terum (138) divide research into professions into three
problem areas. The first relates to qualifications, i.e., how to learn the profession.
While the cognitive conditions of the medical profession are well entrenched in the
education system, its emotional aspects receive much less attention. A second
problem area concerns the status of knowledge, and here we mainly underscore the
needs of theoretical versus clinical knowledge. The third area concerns the practice of
medicine and how to deal with the often conflicting demands and expectations aimed
at the profession by various parties, especially by patients (138).
One difference in attitude regarding the various approaches to the encounter with the
patient/family is the perception of one’s own effort. Conventional theory about
professionals assumes that professionals block their emotions, or at least, in the

D i s c u s s i o n | 3 1
present case, do not allow them to affect encounters with children and families (139).
Here we found significant variation. While some professionals saw themselves as
dominant in the encounter, others viewed the parents as clients and themselves as
providers of what was expected. A difference was even apparent between the
attitudes that the meeting should be characterized either by a firm and stable
structure or by a flexible approach in which the doctor tries to read the parents’
reactions and then adapt to them. However, information and communication
comprised a key concept for all interviewed doctors, and there was a clear
understanding that “communication breakdown” represented failure in their work.
One clear result was that doctors felt that the most important factor contributing to
the sense of a job well done was the creation of trust (140).
By definition, being a doctor means being expected to be professional. The medical
degree and license promises this professionalism and in most cases patients expect a
professional encounter in connection with consultations and treatment (138). What
really provides this legitimacy is the belief that it is based largely on science and
proven experience. Professional practitioners and their experience can be considered
in terms of Carr-Saunders and Wilsson’s (141) classic position on the issue of the dual
role of the professional as mediator and interpreter. In the patient encounter, the
doctor is expected to provide accurate information about diagnoses and risks, and to
translate the scientific language into lay terms so that patients understand what is
involved.
People’s expectations of professionals reflect the idea that a modern society entails
the differentiation and extensive division of duties (59). Being professional requires
objectivity, knowledge, and the attitude that all clients should be treated equally.
Moreover, the status of the professional must be acquired, mainly through education.
All this is expected to make the patient confident that he or she will receive a proper
diagnosis and treatment. Malhotra et al. (142) discuss the ethical issues underlying
the doctor’s professional counselling task, although they focus particularly on ethical
dilemmas in foetal management from a cardiac perspective. Malhotra et al. cite actual
cases to highlight the increasing counselling challenges facing physicians. Here it is a
question of reconciling the expectations that professionals face with their own
personalities (59).
The studied doctors consistently said that medical school spent little time on this
issue and several respondents said they were poorly prepared for their first patient
encounter, which caused them to be nervous and uncertain. All interviewees stressed
the lack of appropriate education in this regard and requested more training rather
than simply guidelines. Rosenbaum (143), in a review study, and Fouron (134) and
Fallowfield (135) discuss aspects of this issue and reiterate the necessity of being
aware of the importance of developing this learning area. Another striking finding
was that many cardiologists emphasized the importance of reflection. In line with
this, many authors have stressed that the practitioner should reflect on current
professional perspectives (136, 144, 145).
3 2 | A n n a - L e n a B i r k e l a n d
It was striking that the cardiologists, besides individual approaches to improving
communication, also emphasized the importance of team meetings and of developing
teamwork, particularly in PCTs.
Teams/PCTs
Earlier studies have demonstrated that both families and cardiologists often value the
local PCT as a key central unit (146), stressing that teamwork needs to be an
important part of the continuum of care to meet the complex needs of children with
chronic disease and their families (147). In study IV, we arrived at the same findings,
i.e., that the knowledge needed to best treat a child with CHD and deal with his or her
family is now so extensive that appropriate treatment requires a team comprising
representatives of various professions. We also found that, although the goal is to
work as a team, there are ambiguities in terms of who is responsible for what aspects
of care and for relationships with other societal actors. There is a need to clarify and
manage the mission of caring for the child with CHD in relation to the increased
complexity and constant change in healthcare and society. Conceptual robustness is
required if a team is to respond to this need at the professional level, with respect to
both the child and his or her family (148, 149). If the professions want to collaborate
in teams to provide the desired holistic approach, the organizational answer is
interprofessional teams (150).
In our study, we identified a great desire to work in teams and a willingness to take
on structural challenges, but the teams nevertheless encountered difficulties and the
discrepancies with ideal ways of working created frustration. For teams to work
efficiently and cope with both current and future missions requires deliberate efforts
to build robust and collaborative cultures, which include further development of
cooperation in workgroups and of workgroup management (151, 152). Factors of
importance for PCT ability to work, as identified in Study IV, were coordination of
team resources, support, continuing education, and access to professional
management consultants.
Dependence on the physician and the necessity of a physician being present in the
PCT were expressed by all interviewees, and it was evident that the physicians’ lack of
availability limited the PCTs’ ability to work smoothly. Thylefors et al. (152, 73)
discuss how lack of time weakens the physician’s ability to participate in the team;
this time pressure means de-emphasizing care conferences, which reduces the
meaning of the interdisciplinary team.
The studied PCTs were formed especially to treat the children with CHD and their
families, and the teams and their internal relationships were built through social
contact within the teams. The teams provided an unexpected description of their
internal communication, presenting an image of integrative cooperation and few if
any internal conflicts. This presentation could be explained in two ways: either the
teams constituted genuinely mature groups, or they sought to project an idealized
group self-image (152). Thylefors also state that conflicts are essential in

D i s c u s s i o n | 3 3
interdisciplinary teams; however, the studied PCTs could constitute properly
functioning working groups, i.e., “trans-professional teams” (75, 76,) in which
conflicts are rare. Earlier studies have demonstrated that lack of organizational
structure, difficulties prioritizing, and poor meeting structure could impede
teamwork (153). Structural and organizational limitations must be exposed at all
levels and eliminated, so that the PCTs’ ability to work in a process and meet
continuously changing needs can develop. Cashman (154) describes this in a case
study of integrated teams in primary care, which stated that organizational structures
and incentive programmes must be related if efficient team function is to be
sustainable.
The studied teams mentioned no explicit leaders. In some teams, the person who
initiated the team meetings served as the temporary leader, while in others, the nurse
and the physician implicitly assumed leadership roles. Like McCallin (155), we want
to raise the question of more directive leadership, and its consequences for PCT
structure and development.
The rapid expansion of this field has led to proliferating knowledge on the part of the
various professions involved in the rehabilitation process, in turn increasing the need
for efficient interaction between experts in different fields (19, 156). The PCTs
evidently had some problems communicating constructively with CAP and the HOs,
which sometimes led to conflicts between individuals, professions, and units.
Cooperation between these entities must be managed and further developed (157).
Dialogue is an important and characteristic cooperation tool in interprofessional
teams (153). Conflict management and constructive communication give a broad
perspective on team functioning, and our results indicate a need to improve team
communication by allowing time for dialogue, problem solving, and knowledge
sharing. As the needs of the children with CHD and their families are increasingly
complex, clinical experience indicates that collective reflection is necessary in PCTs –
there is a need for a “forum for reflection”. Dialogue and discussion concerning
objectives, common understanding, ethics, and collegial support are crucial (157).
There is a need for joint reflection in the local PCT, and in regional and international
paediatric cardiology centres as well. The establishment of an ongoing network of
PCTs may result in national collaboration for research and clinical improvements for
children with CHD.

3 4 | A n n a - L e n a B i r k e l a n d
METHODOLOGICAL CONSIDERATIONS AND LIMITATIONS
Quantitative method
At time of planning this study, we were not aware of any existing instrument
capturing the complexity of psychosocial factors in children/adolescents with heart
disease and their families. Lindström replied positively to the suggestion to put his
theory into practice (34). We found it obvious that more specific disease-adjusted
methods for elucidating psychosocial complexity were needed (158, 159) Drotar et al.
(160) explain how QoL assessments can be used for many purposes, and these
authors describe both the necessity and complexity of understanding and describing
the situation experienced by chronically ill children. In Drotar et al., we found
support for the first study describing the psychosocial situation of these patients,
using a new psychosocial inventory. Guided by previously validated instruments
(161), our aim was to characterize the complexity related to children with cardiac
disease using an assessment instrument to assess/describe their psychosocial
situation (162–164).
As Goldbeck and Melches (15) state in the introduction to their 2005 study, we also
found, at the time of the first study, that many instruments developed for measuring
QoL in children lack the perspective of the child with CHD within his/her family.
In 2001, the International Classification of Functioning, Disability and Health (ICF),
was developed. A paediatric version of this, ICF-CY, has been available since 2007
(33). The ICF-CY is based on the diagnosis, but views the “big picture” relating to
daily functions, symptoms, activities, and participation, as well as to household
conditions and social factors (33). HRQoL scales adapted for children with cardiac
disease are now also available, which was not the case at the time that our study was
planned (39, 40).
One general limitation is that the instruments used in study I and study IV were
developed especially for these studies and have not been psychometrically validated.
The untested reliability of the inventory method could be seen as a weakness, but, in
the method’s defence, most parts of the instrument derive from pre-existing,
validated instruments (16, 164). Comparison with a matched control group and the
relatively extensive material increase the reliability of the instrument’s results. That
the instrument was clearly useful to the well-informed research group that used it,
further attests to its utility. Minor limitations of the method are that it requires an
experienced clinical social worker for its application and that sociodemographic
covariates such as socioeconomic status, education, and profession are not included
in the inventory.

M e t h o d o l o g i c a l c o n s i d e r a t i o n s & l i m i t a t i o n s | 3 5
Qualitative method
The focus of study II was on exploring the experiences of parents and siblings of
children with CHD during the diagnostic phase and on following how family
members dealt with the situation over time. The use of a broad opening question in
the interviews allowed the parents and siblings to choose how to describe their “way
of living” close to a child with CHD. The interviewees were asked to reflect on their
experience of this situation. The judgment of trustworthiness findings should be
based on credibility, dependability, and transferability (165, 166). One aspect of
credibility practiced throughout the thesis work was open dialogue between the
researchers: the authors of the studies discussed the data interpretation to ensure
that judgments about differences and similarities were consistent (94).
We believe that the samples achieved an acceptable level of redundancy, and that the
participants in the constituent studies of this thesis have been sufficiently covered in
the material. Though it could be argued that the numbers of participants in the
studies were small, trustworthiness in a qualitative study is gained more by the
richness of each interview than by the sample size per se (167–169). That being said,
the sample size in Study II did make it difficult to identify differences between
families attributable to the level of disease severity, sociodemographic factors, or
differences in access to resources relevant to their coping behavior.
In Study III, we interviewed a small number of paediatric cardiologists working at the
same Swedish department of paediatric cardiology. Though the results are local and
limited, with the theoretical framework serving as background, we find the
conclusions generally applicable. Another limitation is the lack of gender balance
because, at the time of the interviews, all consultants in the chosen department were
male.
The results of Study IV may also be of limited applicability because Sweden is a small
country; on the other hand, the survey conducted is a national one including a large
proportion of existing Swedish PCTs. As our aim was descriptive rather than
theoretical, we believe the sample achieved an acceptable level of reliability.
Content analysis can be carried out with different levels of abstraction. One approach
is to view the manifest content, i.e., what is overtly expressed in the text, which is the
most common approach in quantitative research. However, we chose a different
option for the constituent studies of this thesis, also analysing the latent content,
which entailed interpretation. Graneheim and Lundman (92) believe that some form
of interpretation is always involved, though its depth may vary, and other authors
describe other similar approaches. It might have been possible to apply an approach
similar to that of Downe-Wamboldt (95), who recommends formulating preliminary
categories after a first, superficial review of the material and then encoding all the
text.
Clearly, there are different ways of thinking and it became ever more apparent over
the course of the research process that it was impossible to go through the process

3 6 | A n n a - L e n a B i r k e l a n d
directly from beginning to end, but that progress was instead iterative between the
various stages (92).
One measure of the reliability of an analysis is to openly describe the analytical
method and how it was implemented, how the data were collected, and the context in
which the data were collected (95). Regarding the follow-up portion of study II, the
material was limited in that interview material was available from only two occasions
involving the same people, which obviously reduces the amount of information
produced by the study.
We established internal validity – i.e., the truthfulness in representing the reality of
the participants – by carrying out a “member check” as suggested by Lincoln and
Guba (165). Member checks do help improve the accuracy, credibility, validity, and
transferability (also known as applicability, external validity, or fittingness) of
research results. In many member checks, the interpretation and resulting report (or
a portion of it) are given to members of the sample (informants) who check the
accuracy of the work. In studies III and IV, we used the member check to obtain
informant feedback or respondent validation. Their comments serve to check the
viability of the interpretation and were described in the studies.
Early in the research process, we found that a combined quantitative and qualitative
approach best suited the overall purpose of the study. Quantitative and qualitative
methods do not need to stand in opposition to each other; instead, we viewed both
approaches as equally valid tools for better understanding the context we wanted to
explore. Combining methods gave a broader database and, consequently, a more
secure basis for interpretation. We saw that combining various methods would
provide benefits such as increased validity and greater confidence in the analysis,
facilitating the development of a nuanced and holistic picture of children with heart
disease and of their general situation (165, 170).

G e n e r a l s u m m a r y | 3 7
GENERAL SUMMARY
In conclusion, the inventory method can differentiate the three grades of medical
complexity, in terms of number and severity of psychosocial symptoms. The
inventory of the personal, interpersonal, and external spheres elucidates the
psychosocial complexity of symptoms and creates a basis for understanding the need
for psychosocial support in children and adolescents with CHD.
Receiving news of a child’s heart disease can be described as a turning point, a central
event in the lives of the affected families. What is common to the studied families is
the stress this news entails, while their reactions and their ways of evaluating and
dealing with the problems vary over time. Despite marked stress, living with and
caring for a child with heart disease proved manageable for the studied families. In
both in the short and long terms, well-functioning communication between the
families and medical personnel was crucial. Staff readiness to communicate by way of
their availability, continuity, manner, structuring of information, and supportive
behaviour created a feeling of security, leading to trust on the part of the families of
the children with heart disease.
Among paediatric cardiologists, we found unanimous emphasis on the importance of
properly communicating bad news: they agreed on the significance of trust and
confidence in relation to the families and on the use of various emotional positions
when breaking the news of the diagnosis. A common aim was to achieve better skills
at handling the situation, by means of education, coordinating efforts through joint
reflection, and sharing experience. To meet these needs, there is a need to develop
teamwork and for medical education programmes to develop the skills of medical
students and residents at delivering bad news.
Swedish PCTs aim and desire to work in a structured way, usually with a nurse or
contact nurse as coordinator, though team structure and composition differs between
units. The challenge is to meet and manage the increasing complexity of paediatric
cardiac cases at both the family and system levels, which requires a team of
representatives of various professions. These teams need leadership, resource
coordination, support, continuing education, and access to coaching. The physicians’
lack of availability limits the PCT’s ability to work smoothly and to meet the
continuously changing needs of children with CHD and their families. Managing this
constant change calls for organizational change and action plans. There is a need for
fora to stimulate dialogue and joint reflection in local PCTs and at regional and
international paediatric cardiology centres as well.

3 8 | A n n a - L e n a B i r k e l a n d
CHALLENGES FOR THE FUTURE
- To meet and manage the increasing psychosocial complexity for children with
CHD and their families.
- To further develop psychosocial care programmes including methods for
describing and assessing the patients’ and their families’ psychosocial needs from
a bio-psychosocial perspective– taking into account the chronicity of CHD.
- To actively participate in the process of developing and apply patient-reported
outcome measures (PROMs).
- Fora for individual and group reflection/supervision/coaching should be offered
to doctors, nurses, and paramedical staff involved in treating and caring for
children with CHD.
- To create conditions for external and national cooperation/collaboration, e.g. by
communicating and taking advantage of a recently introduced national video
system.
- To raise the awareness of the psychosocial complexity of children with CHD, to
stakeholders such as politicians, administrators at various levels, lobbyists,
community and healthcare leaders and the public.

A c k n o w l e d g e m e n t s | 3 9
ACKNOWLEDGEMENTS
First of all, I would like to thank
All the participating children and their families/parents who taught me
something about life and living.
The professions that were available, shared thoughts and professional experiences.
A lot of people have contributed to this work. In particular I would like to thank:
Annika Rydberg My main supervisor for patiently, but firmly, introducing me to
the field of research. With your width of knowledge, common sense and enthusiasm,
you are a role model.
Bruno Hägglöf My co supervisor, for opening a world of research and for valuable
practical support.
Olle Hernell and Magnus Domellöf as previous and present Chairman of the
Division of Pediatrics.
Lars Dahlgren for helping me deepen my understanding of qualitative method and
for valuable discussions over a cup of coffee and a tasty biscuit.
Ulla H Graneheim for sharing your competence in qualitative methods.
Birgitta Bäcklund for turning the word of “kappa” into the substance of a book.
Ina Höjmark, Mona Strid, Barbro Nilsson, and Dag Teien at the Pediatric
Cardiology Clinic in Umeå thank you for lots of laughter and many years of
teamwork.
Kirsi Reijonen my colleague and friend. For long lasting friendship, for listening,
for a dialogue that brought me forward and for cooperation in the research fields “the
art of questioning” and management/leadership agility.
Eva Tingåker Johansson for friendship, a warm heart and encouragement along
the way and for bringing me outside of the academic world reminding me of rest of
life.
Annica Anca Elmberg, for your creativity, for your illustrations filled with
meanings and thank you for patience when I have to “cut” them.
Anneli Kero, Elisabeth Rhodin, Katarina Bergström, Ing-Marie Marklund
colleagues thank you for cooperation and friendship during all years.
Ulla Svensson for providing me a “home away from home”.
Ola, Jacob, Lydia and Pontus My family: The essence of my existence, for love,
support and patience.

4 0 | A n n a - L e n a B i r k e l a n d
This thesis has been supported by grants from: Swedish Heart Child Association
(SHCA), Samaritan Foundation and fundings from the Northern Country
Councils Cooperation Committee.
For funding throughout the years leading up to completion of this thesis I would like
to acknowledge Division of Pediatrics and Division of Child and Adolescent
Psychiatry, Department of Clinical Sciences.

R e f e r e n c e s | 4 1
REFERENCES
1. Tennant PW, Pearce MS, Bythell M, Rankin J. 20-year survival of children born with
congenital anomalies: a population-based study. Lancet. 2010;375:649-56
2. Lundell B. [Pediatric cardiology - a Swedish matter]. Barnkardiologi - en svensk
angelägenhet. Läkartidningen. 2005;102(28-29):2056-9
3. Moons P, Bovijn L, Budts W, Belmans A, Gewillig M. Temporal trends in survival to
adulthood among patients born with congenital heart disease from 1970 to 1992 in
Belgium. Circulation. 2010;122(22):2264-72
4. Somerville J. Management of Adults With Congenital Heart Disease: An Increasing
problem. Annu Rev Medi. 1997;48:283-93
5. Thilén U, Nordenskjöld A, Nordenskjöld M. [Congenital abnormalities require life-long
follow up]. Livslång uppföljning krävs vid medfödd missbildning. Läkartidningen.
2010;107(42):2567-71
6 Oyen N, Poulsen G, Biyd HA, Wohlfahrt J, Jensen PK, Melbye M. National time trends in
congenital heart defects. Denmark 1977-2005. Am Heart J. 2009;157:467-73
7. Boneva RS, Botto LD, Moore CA, Yang Q, Correa A, Erickson JD. Mortality associated
with congenital heart defects in the United States: 1979-1997. Circulation.
2001;103(19):2376-81
8. Marelli AJ, Mackie AS, Ionescu-Ittu R, Rahme E, Plote L. Congenital heart disease in the
general population: changing prevalence and age distribution. Circulation.
2007;115:163-72
9. Griffin T. Supporting families of infants with congenital heart disease. Newborn Infant
Nurs Rev. 2002;2:83-89
10. The Swedish Board of Health and Welfare. The organisation of the Swedish Pediatric
Heart Surgery 1992;3:17-8. Socialstyrelsen. Nationella riktlinjer för hjärtsjukvård.
www.socialstyrelsen.se/Lists/Artikelkatalog/Attachments/8587/2008-102-
2_20081024.pdf
11. McCusker CG, Doherty NN, Molloy B, Casey F, Rooney N, Mulholland C, Sands A, Craig
B, Stewart M. Determinants of neuropsychological and behavioural outcomes in early
childhood survivors of congenital heart disease. Arch Dis Child. 2007;92:137-41
12. Lane DA, Lip GYH, Millanne TA. Quality of life in adults with congenital heart disease. Int
J Cardiol. 2002;86:19-26
13. Berghammer M, Dellborg M, Ekman I. Young adults experiences of living with congenital
heart disease. Int J Cardiol. 2006;340-7
14. Birks Y, Sloper P, Lewin R, Parsons J. Exploring health-related experiences of children
and young people with congenital heart disease. Health Expect. 2007;10:16-29

4 2 | A n n a - L e n a B i r k e l a n d
15. Goldbeck L, Melches J. Quality of life in families of children with congenital heart disease.
Qual Life Res. 2005;14:1915-24
16. Goldbeck L, Melches J. The impact of the severity of disease and social disadvantage on
quality of life in families with congenital cardiac disease. Cardiol Young. 2006;16(1)67-75
17. Latal B, Helfricht S, Fischer JE, Bauersfeld U, Landolt MA. Psychological adjustment and
quality of life in children and adolescents following open-heart surgery for congenital
heart disease: a systematic review. BMC Pediatr. 2009;9:6
18. Alden B, Gilljam T, Gillberg C. Long-term psychological outcome of children after surgery
for transposition of the great arteries. Acta Paediatr. 1998;87:405-10
19. Majnemer A, Limperopoulos C, Shevell MI, Rohlicek C, Rosenblatt B, Tchervenkov C. A
New Look at Outcomes of Infants with Congenital Heart Disease. Pediatr Neurol.
2009;40(3):197-204
20. McCusker CG, Doherty NN, Molloy B, Casey F, Rooney N, Mulholland C, Sands A, Craig
B, Stewart M. Determinants of neuropsychological and behavioural outcomes in early
childhood survivors of congenital heart disease. Arch Dis Child. 2007;92:137-41
21. Hovels-Gurich HH, Konrad K, Wiesner M, Minkenberg R, Herpertz- Dahlmann B,
Messmer BJ, Von Bernuth G. Long term behavioural outcome after neonatal arterial
switch operation for transposition of the great arteries. Arch Dis Child. 2002;87:506-10
22. Miatton M, De Wolf D, François K, Thiery E, Vingerhoets G. Intellectual,
neuropsychological, and behavioural functioning in children with tetralogy of Fallot.
J Thorac Cardiovasc Surg. 2007;133:449-55
23. Spijkerboer AW, Utens EMWJ, Bogers AJJC, Helbing WA, Verhulst FC. A historical
comparison of long-term behavioral and emotional outcomes in children and adolescents
after invasive treatment for congenital heart disease. J Pediatr Surg. 2008;43:534-9
24. Chen CW, Li CY, Wang JK. Growt and development of children with congenital heart
disease. J Adv Nurs. 2004;47(3):260-9
25. Birkeland AL, Rydberg A, Hägglöf B. The complexity of the psychosocial situation in
children and adolescents with heart disease. Acta Paediatr. 2005;94(10):1495-1501
26. Lawoko S, Soares JJ. Distress and hopeless among parents of children with congenital
heart disease, parents of children with other diseases, and parents of healthy children.
J Psychosom Res. 2002;52(4):193-208
27. Lawoko S, Soares JJ. Psychosocial morbidity among parents of children with congenital
heart disease: A prospective longitudinal study. Heart Lung. 2006; 35(5):301-14
28. Menahem S, Poulakis Z, Prior M. Children subjected to cardiac surgery for congenital
heart disease. Part 1 – Emotional and psychological outcomes. J Thorac Cardiovasc Surg.
2008;7:600-604
29. Salonen T. Barnfattigdomen i Sverige. Stockholm: Rädda Barnen, 2011

R e f e r e n c e s | 4 3
30. Köhler L. [Why do children feel worse? Importance of relative poverty, social capital and
status for children's health]. Betydelsen av relativ fattigdom, socialt kapital och status för
barns hälsa. Varför mår barnen sämre än de har det? Läkartidningen. 2007;104(26-
27):1989-91
31. Connor JA, Kline NE, Mott S, Harris SK, Jenkins KJ. The meaning of Cost for Families of
Children with Congenital Heart Disease. J Pediatr Health Care. 2010;24:(5):318-25
32. Lundström NR, Berggren H, Jögi P, Sunnegård J. Centralization of Pediatric Heart
Surgery in Sweden. Pediatr Cardiol. 2000;21(4):353-7
33. World Health Organization. International Classification of Functioning, Disability and
Health (ICF). www.who.int/classifications/icf/en/ 2011
34. Lindström B. The Essence of Existence. Göteborg: NHV-report, 1994:3
35. Lazarus RS. Stress and Emotion: A New Synthesis. London: Free Association Books, 1999
36. Antonovsky A. Health, stress and coping. San Francisco: Jossey-Bass, 1979
37. Bernler G, Johnsson L. Teori för psykosocialt arbete. Stockholm: Natur och kultur,
2001;20-25
38. Eriksson M, Lindström B. Antonovsky's sense of coherence scale and its relation with
quality of life: a systematic review. J Epidemiol Community Health. 2007;61:938-44
39. Downloaded from: www.pedsql.org
40. Uzark K, King E, Spicer R, Beekman R, Kimball T, Varni JW. The Clinical Utility of
Health-related Quality of Life Assessment in Pediatric Cardiology Outpatient Practice.
Congenit Heart Dis. Sep 2012 [Epub ahead of print]
41. Downloaded from: www.disabkids.org
42. Downloaded from: www.kidscreen.org
43. Marino BS, Shera D, Wernovsky G, Tomlinson RS, Aguirre A, Gallagher M, Lee A, Cho CJ,
Stern W, Davis L, Tong E, Teitel D, Mussatto K, Ghanayem N, Gleason M, Gaynor JW,
Wray J, Helfaer MA, Shea JA. The development of the pediatric cardiac quality of life
inventory: a quality of life measure for children and adolescents with heart disease. Qual
Life Res. 2008;17(4):613-26
44. Antonovsky A. Unraveling the mystery of health. How people manage stress and stay
well. San Francisco: Jossey-Bass, 1987
45. Lindström B, Eriksson M. Salutogenesis. J Epidemiol Community Health. 2005;59:440-
442
46. Lindström B. The salutogenic model as a tool for quality of life enhancement for children
with special needs. Exeptionally Educ Can. 1999;9:105-109
47. Karasek RA. Job demands, job decision latitude, and mental strain: Implications for job
redesign. Adm Sci Q. 1979:24:285-308

4 4 | A n n a - L e n a B i r k e l a n d
48. Karasek R, Theorell T. Healthy work: Stress, productivity, and the reconstruction of
working life. New York: Basic Books, 1990
49. Cummings EM, Greene AL, Karraker KH. Life-span Developmental Psychology.
Perspective on stress and coping. Psychology Press, 1991
50. Lazarus RS, Folkman S. Stress, Appraisal and Coping. New York: Springer Publishing
Company, 1984
51. Walsh F. Family resilience: a framework for clinical practice. Fam Process. 2003;42:1-18
52. Gillespie CF, Phifer J, Bradley B, Ressler KJ. Risk and resilience: genetic and
environmental influencies on development of the stress respons. Depress Anxiety.
2009;26:(11):984-92
53. Compas BE, Connor-Smith JK, Saltzman H, Thomsen AH, Wadsworth ME. Coping with
stress during childhood and adolescence: problems, progress, and potential in theory and
research. Psychol Bull. 2001;127(1):87-127
54. Mackay R. Family resilience and good child outcomes: an overview of the research
literature. Social Policy Journal of New Zealand. 2003;20:98-118
55. www.ne.se
56. Gordon H. The Underlying Philosophy of Social Case Work, Family. Theory and Practice
of Social Case Work. 1941;22:139-47
57. Lennéer-Axelsson B. Psykosocialt behandlingsarbete. Stockholm: Natur & Kultur, 2010
58. Bernler G, Johnsson L. Handledning i psykosocialt arbete. Lund: Natur & Kultur, 2010
59. Hansböl G, Krejsler J. Konstruktion af professional identitet – en kulturkamp mellem
styrning og autonomi. In: et markedssamfund. [Construction of professional identity – a
cultural struggle between control and autonomy. In: a market society]. In: L. Moos et. al.
Relationsprofessioner. [Relation professions]. Copenhagen: Danish Pedagogical
University, 2004
60. Larsson EB, Yao X. Clinical Empathy as Emotional Labor in the Patient-Physician
Relationship. JAMA 2005;293(9):1100-6
61. Holm U. Empati. Att förstå andra människors känslor [Empathy: Understanding Other
People’s Feelings]. Stockholm: Natur & Kultur, 2001
62. Hochschild, A. Emotion Work, Feeling Rules, and Social Structure. Am J Sociol.
1979;85(3):551-75
63. Bone D. Dilemmas of emotion work in nursing under market-driven health care. Int J
Public Sector Management. 2002;15:140-50
64. Giddens A. The Consequences of Modernity. Cambridge: Polity Press, 1990

R e f e r e n c e s | 4 5
65. Iedema RA. Medicine and health, inter- and intraprofessional communication. I: Brown,
K. Encyclopaedia of Language and Linguistics (2nd ed). Amsterdam & New York:
Elsevier, 2008
66. Long AF, Kneafsey R, Ryan J, Berry J. The role of the nurse within the multi-professional
rehabilitation team. J Adv Nurs. 2002;37:70-78
67. Belbin RM. Management teams: why they succeed or fail (2nd ed). Oxford: Butterworth-
Heinemann, 2004
68. Katzenbach JR, Smith DK. The Wisdom of Teams: Creating the high-performance
organization. Boston, MA: Harvard Business School Press, 1993
69. Drinka T, Clark P. Health care teamwork: Interdisciplinary practice and teaching.
Westport, CT: Auburn House, 2000
70. King JC, Nelson TR, Blankenship KJ, Turturro TC, Beck AJ. Rehabilitation team function
and prescriptions, referrals and order writing. In: DeLisa JA (ed) Physical medicine &
rehabilitation: principles and practice (4th ed, vol 2). Philadelphia, PA: Lippincott,
Williams & Wilkins, 2005, chapter 46, p. 1051-72
71. D'Amour D, Oandasan I. Interprofessionality as the field of interprofessional practice and
interprofessional education: An emerging concept. J Interprof Care. 2005;19:8-20
72. McCallin A. Interdisciplinary practice - a matter of teamwork: an integrated literature
review. J Clin Nurs. 2001;10:419-25
73. Thylefors I, Price E, Persson O, von Wendt L. Teamwork in Swedish neuropaediatric
habilitation. Child Care Health Dev. 2000;26(6):515-32
74. Kvarnström S. Collaboration in Health and Social Care: service user participation and
teamwork in interprofessional clincal microsystems. Jönköping: School of Health
Sciences, Jönköping University, 2011
75. Hall P, Weaver L. Interdisciplinary education and teamwork: A long and winding road.
Med Educ. 2001;35:867-75
76. Kvarnström S. Difficulties in collaboration: A critical incident study of interprofessional
healthcare teamwork. J Interprof Care. 2008;22(2):191-203
77. Freeth D, Hammick M, Reeves S, Koppel I, Barr H. Effective interprofessional education.
Development, delivery & evaluation. Oxford: Blackwell Publishing Ltd, 2005
78. De Bono E. Creativity and quality. Qual Manag Health Care. 1994;2(3):1-4
79. Leigh A, Maynard M. Leading your team: how to involve and inspire team. London:
Nicholas Brealey Publishing, 2005
80. Meleis AI, Sawyer LM, Im EO, Hilfinger-Messias DK, Schumacher K. Experiencing
transitions: An emerging middle-range theory. ANS Adv Nurs Sci. 2000;23:12-28
81. Kvale S. Issues of Validity in qualitative Research. Lund: Studentlitteratur, 1989

4 6 | A n n a - L e n a B i r k e l a n d
82. Yin R. Case study research. Design and methods. London: Sage Publications, 1994
83. Merriam SB. Case studies as a method of research. Lund: Student literature, 1994
84. Stake ER. The art of case study research. London: Sage Publications, 1995
85. Kvale S. Interviews. An introduction to qualitative research interviewing. London: Sage,
1996
86. Achenbach TA. Manual for the Child Behavior Checklist/4-18 and 1991 Profile.
Burlington VT: University of Vermont Department of Psychiatry, 1991
87. www.aseba.org
88. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV)
American Psychiatry Association. Diagnostic and Statistical Manual of Mental Disorders.
4th edition, 2000; Washington, DC: American Psychiatric Association.
Social and Occupational Functioning Assessment (SOFAS) Scale
Global Assessment of Relational Functioning (GARF) Scale
89. American Psychiatric Association Quick reference to the diagnostic and statistical manual
of mental disorders, 4th edition (DSM-IV). Swedish translation Herlofson J, Landqvist M.
MINI-D IV Diagnostiska kriterier enligt DSM-IV. Stockholm: Pilgrim Press, 1995
90. Sowers KM, Dulmus CN. Measuring the problem behaviour Comprehensive Handbook of
Social Work and Social Welfare. 2008; p. 85-96
91. Krippendorff K. Content analysis. An introduction to its methodology (2nd ed). London,
New Delhi: Thousand Oaks, Sage Publications Inc, 2004
92. Graneheim U, Lundman B. Qualitative content analysis in nursing research: concepts,
procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24:105-12
93. Thomas S, Steven I, Browning C, Dickens E, Eckerman L, Carey L, Pollard S. Focus groups
in health research: A methodological review. Ann Review of Health Social Sciences.
1992;2:7-20
94. MacDougall C, Fudge E. Planning and recruiting the sample for focus groups and in-depth
interviews. Qual Health Res. 2001;11(1):117-26
95. Downe-Wamboldt B. Content analysis: method, applications, and issues. Health Care
Women Int. 1992;13(3):313-21
96. Spijkerboer AW, Utens EMWJ, De Koning WB, Bogers AJJC, Helbing WA, Verhulst FC.
Health-related quality of life in children and adolescents after invasive treatment for
congenital heart disease. Qual Life Res. 2006;15:663-73
97. Spijkerboer AW, Utens EM, Bogers AJ, Verhulst FC, Helbing WA. Long-term behavioural
and emotional problems in four cardiac diagnostic groups of children and adolescents
after invasive treatment for congenital heart disease. Int J Cardiol. 2008;125(1):66-73

R e f e r e n c e s | 4 7
98. Brosig CL, Mussatto KA, Kuhn E M, Tweddell JS. Psychosocial outcomes for preschool
children and families after surgery for complex congenital heart disease. Pediatr Cardiol.
2007;28(4),255-62
99. Koot HM, Wallander JL. Quality of Life in Child and Adolescent Illness: Concepts,
Methods and Findings. Hove, East Sussex: Brunner-Routledge, 2001
100. Landolt MA, Buechel EV, Latal B. Predictors of parental quality of life after child open
heart surgery: a 6-month prospective study. J Pediatr. 2011;158(1):37-43
101. Neuner B, Busch MA, Singer S, Moons P, Wellmann J, Bauer U, Nowak-Göttl U, Hense
HW. Sense of Coherence as a Predictor of Quality of Life in Adolescents with Congenital
Heart Defects: A Register-Based 1-Year Follow-Up Study. J Dev Behav Pediatr. 2011
Feb 15 [Epub ahead of print]
102. Moons P, Norekvål TM. Is sense of coherence a pathway for improving the quality of life
of patients who grow up with chronic diseases? A hypothesis. Eur J Cardiovasc Nurs.
2006;5(1):16-20
103. Bellinger DC, Wypij D, du Plessis AJ, Rappaport LA, Jonas RA, Wernovsky G, Newburger
JW. Neurodevelopmental status at eight years in children with dextro-transposition of the
great arteries: the Boston Circulatory Arrest Trial. J Thorac Cardiovasc Surg.
2003;126(5):1385-96
104. Majnemer A, Limperopoulos C, Shevell M, Rohlicek C, Rosenblatt B, Tchervenkov C.
Health and well-being of children with congenital cardiac malformations, and their
families, following open-heart surgery. Cardiol Young. 2006;16(2):157-64
105. Limperopoulos C, Majnemer A, Shevell MI, Rosenblatt B, Rohlichek C, Tchervenkov C,
Darwish HZ. Functional Limitations in young Children with Congenital Heart Defects
After Cardiac Surgery. Pediatrics. 2001;108(6):1325-31
106. Lawoko S. Factors influencing satisfaction and well-being among parents of congenital
heart disease children: development of a conceptual model based on the literature review.
Scand J Caring Sci. 2007;21(1):106-17
107. Sarajuri A, Lönnqvist T, Schmitt F, Almqvist F, Jokinen E. Patients with univentricular
heart in early childhood: parenting stress and child behaviour. Acta Paediatr.
2012;101(3):252-257
108. Vrijmoet-Wiersma CMJ, Ottenkamp J, Van Roozendaal M, Grootenhuis MA, Koopman
HM. A multicentric study of disease-related stress, and perceived vulnerability, in parents
of children with congenital cardiac disease. Cardiol Young. 2009;19(6):608-14
109. Uzark K, Jones K. Parenting stress and children with heart disease. J Pediatr Health Care.
2003;17(4):163-8
110. Lee A, Rempel GR. Parenting children with hypoplastic left heart syndrome: finding a
balance. J Spec Pediatr Nurs. 2011;16(3):179-89

4 8 | A n n a - L e n a B i r k e l a n d
111. Menahem S, Poulakis Z, Prior M. Children subjected to cardiac surgery for congenital
heart disease. Part 2 – Parental emotional experiences. Interact Cardiovasc Thorac Sur.
2008;7:605-8
112. Solberg O, Grönning Dale MT, Holmström H, Eskedal LT, Landolt MA, Vollrath ME.
Long-Term Symptoms of Depression and Anxiety in Mothers of Infants with Congenital
Heart Defects. J Pediatr Psychol. 2010:36;179-87
113. Fischer AL, Butz C, Nicholson L, Blankenship A, Dyke P, Cua CL. Caregiver Anxiety upon
Discharge for Neonates with Cogenital Heart Disease. Congenit Heart Dis. 2012;7(1):41-5
114. Rempel GR, Rogers LG, Ravindran V, Magill-Evans J. Facets of Parenting a Child with
Hypoplastic Left Heart Syndrome. Nurs Res Pract. Epub 2012 Apr 2.
115. Rempel GR, Harrison MJ. Safeguarding precarious survival: Parenting children who have
life-threatening heart disease. Qual Health Res. 2007;17(6):824-37
116. Strauss AL. Mirrors & masks: the search for identity. London, New Brunswick, NJ:
Transaction Publishers, 2005
117. Glaser B, Strauss A. Status passage. Aldine Transaction, 2009
118. Yildiz A, Celebioglu A, Olgun H. Distress Levels in Turkish Parents of Children with
Congenital Heart Disease. Aust J Adv Nurs. 2009;26(3):9-46
119. Green A, Meaux J, Huett A, Ainley K. Constantly responsible, constantly worried,
constantly blessed: parenting after pediatric heart transplant. Prog Transplant.
2009;19(2):122-7
120. Flury M, Caflisch U, Ullman-Bremi A, Spichiger E. Experiences of Parents With Caring for
Their Child After a Cancer Diagnosis. J Pediatr Oncol Nurs. 2011;28(3):143-53
121. Arafa MA, Zahler SR, El-Dowaty AA, Moneeb DE. Quality of life among parents of
children with heart disease. Health Qual Life Outcomes. 2008;6:91
122. Wray J, Sensky T. Psychological functioning in parents of children undergoing elective
cardiac surgery. Cardiol Young. 2004;14:131-9
123. Cheuk DKL, Wong SMY, Choi YP, Chau AKT, Cheung YF. Parents´understanding of their
child`s congenital heart disease. Heart. 2004;90:435-9
124. Zahmacioglu O, Yildiz CE, Koca B, Ugurlucan M, Gokalp S, Cetin G, Eroglu AG, Oztunc F.
Coming from behind to win - A Qualitative research about psychological conditions of
adolescents who have undergone open-heart surgery for single ventricle between the ages
0-5. J Cardiothorac Surg. 2011;6:155
125. Lawoko S, Soares JJF. Satisfaction with care: a study of parents of children with
congenital heart disease and parents of children with other diseases. Scand J Caring Sci.
2004;18:90-102
126. Tak YR, McCubbin M. Family stress, perceived social support and coping following the
diagnosis of a child´s congenital heart disease. J Adv Nurs. 2002; 39(2):190-8

R e f e r e n c e s | 4 9
127. Luthar SS, Cicchetti D, Becker B. The construct of resilience: a critical evaluation and
guidelines for future work. Child Dev. 2000;71(3):543-62
128. Lawoko S, Soares JJF. Social support among parents of children with congenital heart
disease children: parents of children with other diseases and parents of healthy children.
Scan Journal of Occupational Therapy. 2003;10:177-87
129. Barnett D, Clements M, Kaplan-Estrin M, Fialka J. Building new dreams: supporting
parents’ adaptation to their child with special needs. Infants Young Child.
2003;16(3):184-200
130. Grönning MT, Solberg Ö, Holmström H, Landolt MA, Eskedal LT, Vollrath M E. Mothers
of infants with congenital heart defects: wellbeing from pregnancy through the child´s
first six months. Qual Life Res. 2012;21:115-122
131. Strauss RP, Sharp MC, Lorch C, Kachalia B. Physicians and the Communication of “Bad
News”: Parent Experiences of Being Informed of their Child´s Cleft Lip and/or Palate
Pediatrics. 1995;96(1):82-9
132. Allan LD, Huggon IC. Counselling following a diagnosis of congenital heart disease.
Prenat Diagn. 2004;24(13):1136-42
133. Birkeland A-L, Dahlgren L, Hägglöf B, Rydberg A. Breaking bad news: an interview study
of paediatric cardiologists. Cardiol Young. 2011;21:286-91
134. Fouron JC. The changing and complex relationship between paediatric cardiologists and
life. Cardiol Young. 2000;10:551-6
135. Fallowfield L, Jenkins V. Communicating sad, bad, and difficult news in medicine. Lancet.
2004;363:312-9
136. Menahem S, Grimwade J. Counselling strategies in the prenatal diagnosis of major heart
abnormality. Heart Lung Circ. 2004;13(3):261-5
137. Andersson SO. Mötet och samtalet. In: Bjöörn Fossum. Kommunikation. Samtal och
bemötande i vården. Lund: Studentlitteratur, 2007
138. Molander A, Terum LI. Profesjonsstudier – en introduksjon. In: Molander A & Terum LI
Profesjonsstudier. Oslo: Universitetsforlaget, 2008
139. Hochschild A. Emotion work, feeling rules and social structure. Am J Sociol. 1979;85:551-
75
140. Luhmann N. Familiarity, confidence, trust: Problems and alternative. Trust: Making
and Breaking Cooperative Relations. Department of Sociology, University of Oxford.
Chapter 6, pp 94-107. Oxford: Blackwell, 1990
141. Carr-Saunders MP, Wilson A. The Professions. Oxford: Oxford University Press, 1933
(Reprinted by Frank Cass, London, 1964)
142. Malhotra A, Menahem S, Gillam L. Etichal Issues’ in Fetal Management: A Cardiac
Perspective. Int J Pediatr. 2010;2010:857460

5 0 | A n n a - L e n a B i r k e l a n d
143. Rosenbaum ME, Ferguson KJ, Lobas JG. Teaching Medical Students and Residents Skills
for Delivering Bad News: A Review of strategies. Acad Med. 2004;79(2):107-17
144. Plack M, Greenberg L. The Reflective Practitioner: Reaching for Excellence in Practice.
Pediatrics. 2005;116(6):1546-52
145. Branch WT, Kern D, Haidet P, Weissmann P, Gracey CF, Mitchell G, Inui T. The patient-
physician relationship: teaching the human dimensions of care in clinical settings. JAMA.
2001;286(9):1067-74
146. Kendall L, Sloper P, Lewin RJP, Parsons JM. The views of parents concerning the
planning of services for rehabilitation of families of children with congenital cardiac
disease. Cardiol Young. 2003;13:20-7
147. Yerbury M. Issues in multidisciplinary teamwork for children with disabilities. Child Care
Health Dev. 1997;23(1):77-86
148. Iedema RA. The Discourse of Hospital Communication: Tracing complexities in
contemporary health care organizations. Basingstoke: Palgrave-MacMillan, 2007
149. Batalden P, Ogrinc G, Batalden M. From one to many. J Interprof Care. 2006;20(5):549-
51
150. Reeves S, Zwarenstein M, Goldman J, Barr H, Freeth D, Koppel I, Hammick M. The
effectiveness of interprofessional education: Key findings from a new systematic review.
J Interprof Care. 2010;24(3):230-41
151. Lemieux-Charles L, McGuire WL. What do we know about health care team effectiveness?
A review of the Literature. Med Care Res Rev. 2006;63(3):263-300
152. Thylefors I. Babels torn, tvärprofessionella team. Arbetsgrupper - från gränslösa team
till slutna rum. Stockholm: Natur & Kultur, 2007, pp 86-111
153. Molleman E, Broekhuis M. How working in cross-functional teams relates to core
attributes of professional occupations and the moderating role of personality. Manda
Group Dynamics: Theory, Research, and Practice. 2012;16:(1):50-67
154. Cashman SB, Reidy P, Cody K, Lemy CA. Developing and measuring progress toward
collaborative, integrated, interdisciplinary health care teams. J Interprof Care.
2004;18(2):183-96
155. McCallin A. Interdisciplinary team leadership: a revisionist approach for an old problem?
J Nurs Manag. 2003;11:363-70
156. Boaden N, Leaviss J. Putting teamwork in context. Med Educ. 2000;34:921-7
157. McCallin A, Bamford A. Interdisciplinary teamwork: is the influence of emotional
intelligence fully appreciated? J Nurs Manag. 2007;15:386-91
158. Perrin EC, Stein R, Drotar D. Cautions in using the Child behaviour checklist:
observations based on research about children with a chronic illness. J Pediatr Psychol.
1991;16(4):411-21

R e f e r e n c e s | 5 1
159. Canning EH, Kelleher K. Performance of screening tools for mental health problems in
chronically ill children. Arch Pediatr Adolesc. 1994;148:272-8
160. Drotar D. Measuring Health Related Quality of Life in Children and Adolescents.
Mahwah NJ: Lawrence Earlbaum Associates, 1998
161. Corcoran K, Boyer-Quick J. How clinicians can effectively use assessment tools to
evidence medical necessity and throughout the treatment process. In: AR Roberts & GJ
Green. Social workers´ desk reference. New York: Oxford University Press, 2002, pp.
198-204
162. Bisman CD, Hardcastle D. An Integrating research into practice. Belmont, CA:
Brooks/Cole and Wardsworth, 1999
163. Bloom M, Fischer J, Orme J. Evaluating practice: Guidelines for the accountable
professional (6th ed). Boston: Allyn and Bacon, 2009
164. Chen S. Measurement and analysis in psychosocial research. Brookfield, VT: Avebury,
1997
165. Lincoln YS, Guba EG. Naturalistic Inquiry. Thousands Oaks, CA: Sage Publications, 1985
166. Strauss A, Corbin J. Basics of qualitative research. Grounded theory procedures and
techniques. London: Sage Publications, 1990
167. Sandelowski M. Focus on qualitative methods. One is the liveliest number: The case
orientation of qualitative research. Res Nurs Health. 1996;19:525-9
168. Sandelowski M. Focus on research methods. Whatever happened to qualitative
description? Res Nurs Health. 2000;23:334-40
169. Sandelowski M. What’s in a name? Qualitative description revisited. Res Nurs Health.
2010;33:77-84
170. Repstad P, Fløistad G, Kjeldstadli K, O'Gorman D. Närhet och distans: Kvalitativa
metoder i samhällsvetenskap. Lund: Studentlitteratur, 2007