psycho-social services are an essential componentan
TRANSCRIPT
Psycho-social services are an essential componentan essential component
in Methadone out-patient clinics pin Vietnam
Nguyen To Nhu M.D.; Ph.D.Program Manager
Presenter:g g
Family Health International/Vietnam
Email: [email protected]
Co-authors: Nguyen Thi Huynh (VAAC), Rachel Burdon (FHI), Pham Huy Minh (FHI), Hoang Nam Thai (FHI), Nguyen Thi Minh Ngoc (USAID), Ha Viet Dong (FHI)

Outline
• Overview• Client flowClient flow• Psychosocial services• Contribution of psychosocial services• Discussion• Discussion• Next steps
Why do we need psychosocial services?Why do we need psychosocial services?
• Evidence from many studies shows adding psychosocial support to MMT significantly p y pp g yimproves treatment efficacy:
Reductions in heroin use– Reductions in heroin use– Retention in treatment

Thành phố Hải Phòng
Thủy Nguyên
Hai Phong city
Thuy Nguyen dist
Pilot MMT sitesNgô Quyền
Lê Chân
Ngo Quyen dist
Le Chan distPilot MMT sites Le Chan dist
ố ồ•Decision No Ho Chi Minh cityThành phố Hồ Chí Minh
Quận Bình Thạnh5073/QD-BYT dated Dec 12, 2007
Ho Chi Minh cityBinh Thanh dist
Quận 4
Quận 6
•13 staff in each clinic including 2 counselors
Dist 4Dist 6
•Started in April 08

MMT Vietnam Modelan Integrated Community Based Approachan Integrated Community Based Approach
• Comprehensive Psychosocial support services:• Comprehensive Psychosocial support services:– drug counseling– peer supportpeer support – link to vocational training and job placement
• Address three paradigms of addiction:– Biological Methadone replacement– Psychological Addiction counseling– Sociological social support group for patients
• Linkage with HIV care and treatment
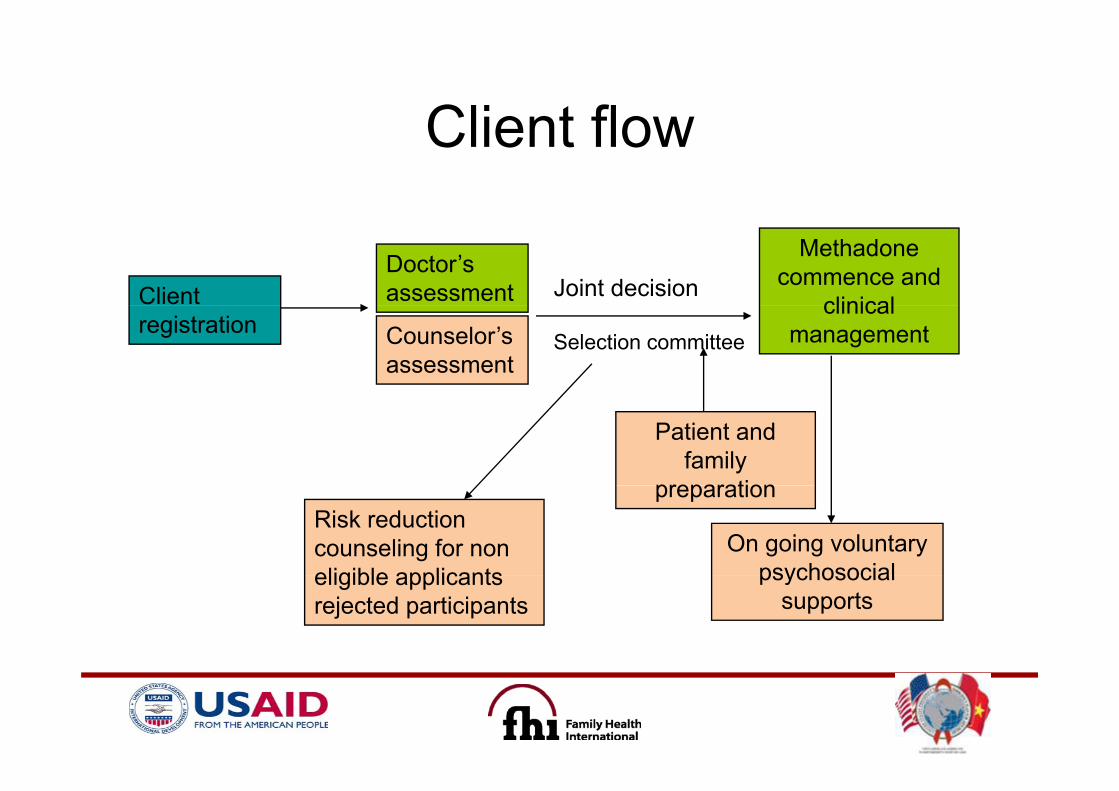
Client flowClient flow
Client Doctor’s assessment Joint decision
Methadone commence and
clinicalregistration Counselor’s
assessmentSelection committee
clinical management
Patient and family
preparation
On going voluntary psychosocial
preparationRisk reduction counseling for non eligible applicants psychosocial
supportseligible applicants rejected participants
Preparation before enter MMT programp p g

Available psychosocial servicesAvailable psychosocial services11 counselors in Assessing the treatment• 11 counselors in 6 clinics
• Assessing the treatment motivation and psycho-social suitability
• 9 peer supporters orgroup leaders
• Prepare patients before entering MMT program
• Providing ongoing individual andgroup leaders
• Involve family
Providing ongoing individual and group counseling (adapted Matrix manual)
• Monthly family meetingso e a ysupport and collaboration
• Monthly family meetings • Social support groups • Case management, linkage andCase management, linkage and
referral

From 3 USAID/FHI supported clinics • Individual counseling: 557/8004
G li 7/167• Group counseling: 7/167• Group education: 52/1446• Family meeting: MonthlyFamily meeting: Monthly
• Adherence to treatment
•Relapse prevention
P iti thi ki d li i•Positive thinking and living
•Referral and linkage services
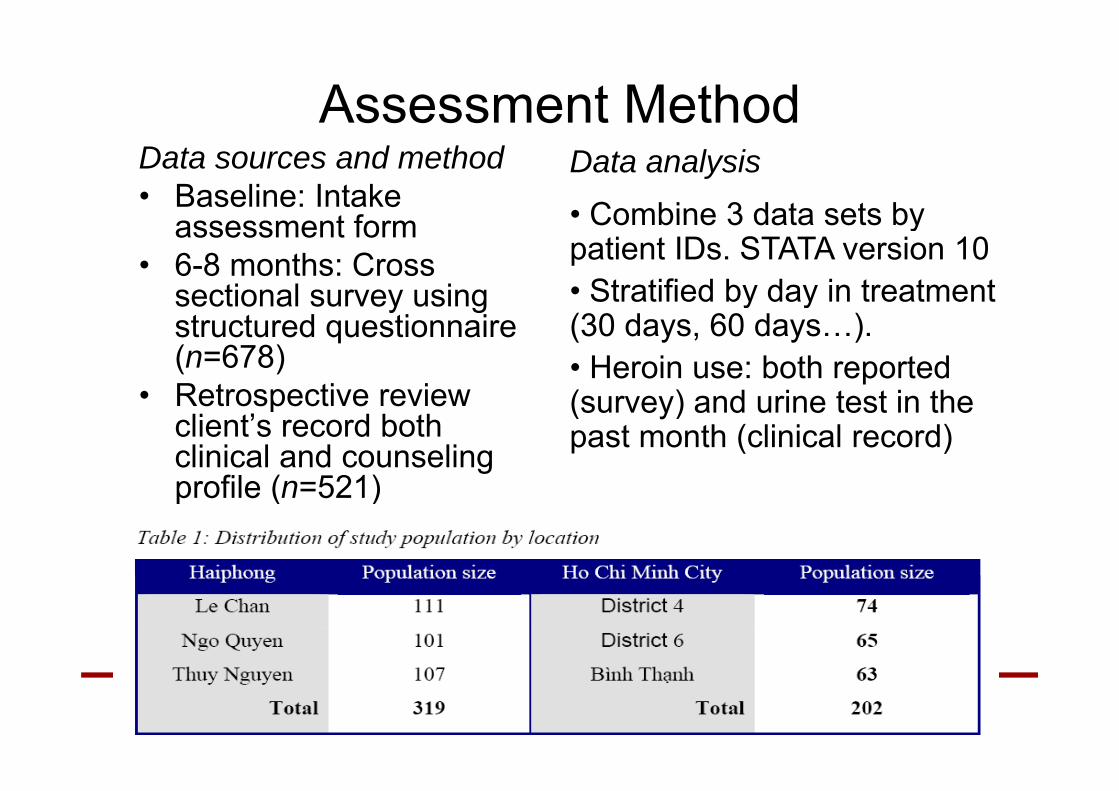
Assessment MethodData sources and method• Baseline: Intake
t f
Data analysis• Combine 3 data sets byassessment form
• 6-8 months: Cross sectional survey using
• Combine 3 data sets by patient IDs. STATA version 10• Stratified by day in treatment sectional survey using
structured questionnaire (n=678)
• Retrospective review
y y(30 days, 60 days…). • Heroin use: both reported ( ) d i t t i th• Retrospective review
client’s record both clinical and counseling profile (n=521)
(survey) and urine test in the past month (clinical record)
profile (n=521)

•1057 patients on MMT(778 on maintenance phase(778 on maintenance phase
87% stopped Heroin use ft 60 d i Tafter 60 days in Tx
Source: MOH report, 2009
• Very good adherence to treatment. <5% drop out rate t eat e t 5% d op out ate(death, jail, rehab center)
• Less risky behaviors of HIV transmission
• 74.8% gained weight and improved appearance

Quotes from the fieldQuotes from the field"the counselors here are more deserving...working hard for us...we see
you here every day with no holiday“you here every day with no holiday
"thank you for saving my children”
"you have informed me of my son’s progress…thank you for my son’s progress"
"thank you to the clinic for helping my son make a lot of progress with your support"your support
"thank you for helping my son stay away from heroin“
Source: Mentoring and supervision report week 7 in Hai Phong. Alan Degilio, Associate Services Clinical Coordinator, Drug and Alcohol treatment center, Adelaide, Australia
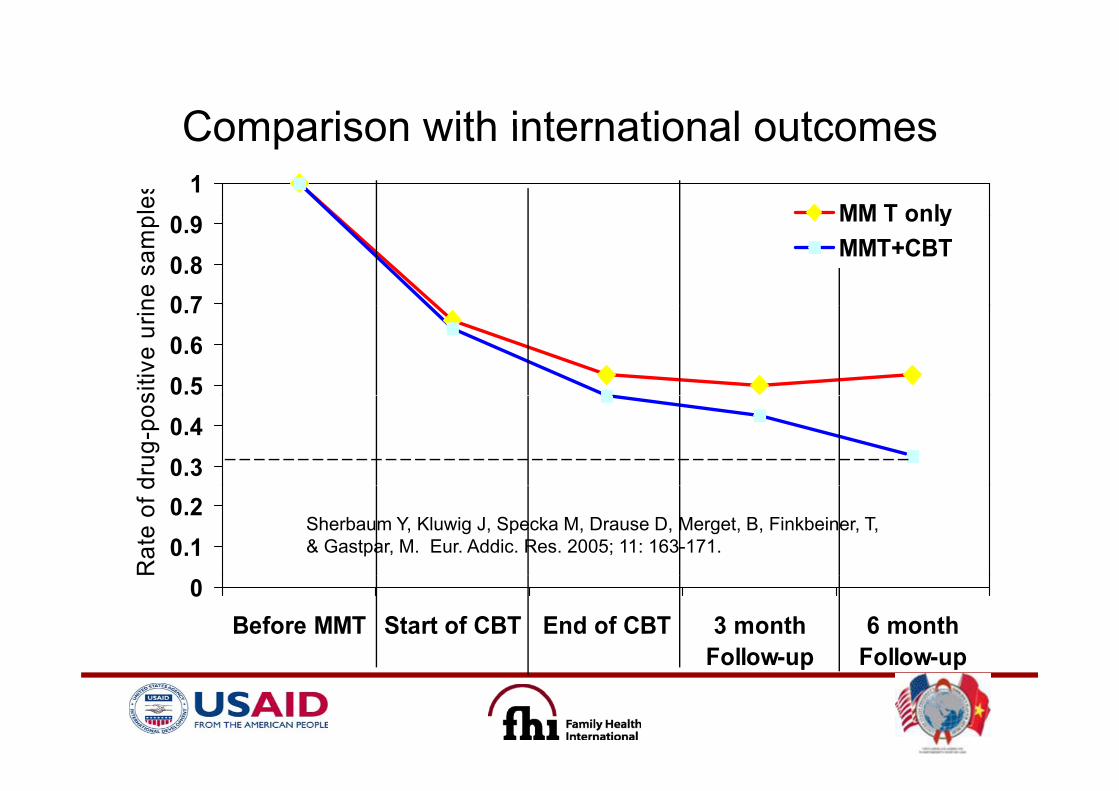
Comparison with international outcomesComparison with international outcomes
0 91
les
MM T only
0 70.80.9
ne s
amp MM T only
MMT+CBT
0.50.60.7
sitiv
e ur
in
0.30.4
drug
-pos
0.10.2
Rat
e of
d
Sherbaum Y, Kluwig J, Specka M, Drause D, Merget, B, Finkbeiner, T, & Gastpar, M. Eur. Addic. Res. 2005; 11: 163-171.
0Before MMT Start of CBT End of CBT 3 month
Follow-up6 month
Follow-upFollow up Follow up

Discussion: possible contributions to good outcomes
Ri ht d i i• Right dose is given• Completely voluntary and good motivation
Positi e effects of co nseling and• Positive effects of counseling and psychosocial support
• Given short follow-up time 6-8 month is “honey• Given short follow-up time, 6-8 month is honey moon” period
• “Hand pick” patients with strict selection criteriaHand pick patients with strict selection criteria• Good attitude from the clinic staff• Good support from family membersGood support from family members• Others?

H.E. Deputy Prime Minister Truong Vinh Trong visited clinic
Source: Ministry of Health, Binh Thanh MMT clinic in HCMC

ROLLING OUT DRUG COUNSELING
TOT Trainers
TOT T i
Training MentorsTOT
T iTrainersTrainersTrainers
PracticePractice
Advanced counselingAdvanced skill based courses
PracticePractice
Basic CounselingBasic Skill based Courses
Implementation Challenges• Voluntary and using adapted international drug
counseling approach is a totally new concept to g pp y pVietnam
• High workload working even in the weekendHigh workload, working even in the weekend and holidays
• High number of drug users with complex• High number of drug users with complex psychosocial needsL k f f l i• Lack of referral services
• Coordination with other agencies and donors in the scaling up plan

Acknowledgmentsg
• Ministry of Health, Vietnam Administration of y ,HIV/AIDS Control
• Dedicated field project staffDedicated field project staff• PEPFAR prevention team
USAID f f di• USAID for funding• Robert Ali, Adelaide University• Kevin Mulvey, former STO/FHI• Dr Stephen J Mills and FHI colleaguesDr. Stephen J. Mills and FHI colleagues