psychiatric toxidromes - wordpress.com
TRANSCRIPT

Jessica L. Goren, PharmD, BCPP Associate Professor, University of RI
Clinical Pharmacist Specialist, Cambridge Health Alliance Instructor in Psychiatry, Harvard Medical School
Psychiatric Toxidromes

Objectives● Introduce common toxidromes !
● Discuss diagnosis of specific psychiatric toxidromes !
● Review prognosis and course for toxidromes
Toxidromes!
● a group of signs and symptoms and/or characteristic effects associated with exposure to a particular substance or class of substances. !
● analogous to groups of symptoms associated with certain medical conditions.

Toxidrome Differential● Neuroleptic malignant syndrome !● Serotonin syndrome !● Anticholinergic toxicity !● Encephalopathy !● Malignant catatonia !
● Heat stroke !
● Delirium Tremens !
● Malignant hyperthermia
Toxidrome Diagnosis● Physical Exam: ●Vital signs and general appearance !●Close attention to neuro exam ● Pupils ●Reflexes ● Posture ●Gait ●Mental status

Toxidrome Diagnosis● Physical Exam: ● Bowel sounds ●Mucous membranes and skin moisture/appearance ●Characteristic odors ●Nosebleeds, needle tracks, blistering !
● Medication History !● Toxicology Screening !● Course of symptoms

Common Psychiatry Toxidromes● Serotonin syndrome !
● Neuroleptic malignant syndrome !
● Anticholinergic toxicity !
● Sympathomimetic toxicity

Serotonin SyndromeSyndrome due to excessive serotonergic tone
Serotonin Syndrome● Hyper stimulation of serotonin receptors 5HT2a +/- 5HT1a
!● Easily confused with NMS !● Triad autonomic hyperactivity MSE changes neuromuscular changes !● Sternbach and Hunter criteria

Hunter Criteria* for SSInitiate 5HT drug + ONE of the following: ● Spontaneous clonus !
● Inducible clonus PLUS agitation or diaphoresis !
● Ocular clonus PLUS agitation or diaphoresis !
● Tremor PLUS hyperreflexia !
● Hypertonia PLUS temperature above 38ºC PLUS ocular clonus or inducible clonus !
*84% sensitive 97% specific

Fig. 1: Mechanisms of serotonin syndrome.
Birmes P et al. CMAJ 2003;168:1439-1442
©2003 by Canadian Medical Association


Serotonin Syndrome● Usually not an issue with one mechanism of action
(although definitely possible) !
● Almost all convincing cases in literature involve MAOIs !
● Beware of non-SRIs with serotonergic activity meperidine linezolid tramadol milnacipran dextromethorphan

Treatment● Discontinue offending agent !
● Supportive care !
● Benzodiazepines (agitation, BP) !
● Fever > 41º C require immediate paralysis, sedation, intubation

SS Antidote● Cyproheptadine (5HT1A,2A antagonist) useful if other measures ineffective 12mg initial dose => 2mg Q2 hr to response ! 12mg => 85% 5HT2 blockade 18mg => 95% 5HT2 blockade

Unique Mechanisms● Vilazodone – 5HT1A partial agonist !
● Trazodone – 5HT2A, 2C antagonist !
● Nefazodone – 5HT2A antagonist !
● Mirtazapine – 5HT2A antagonist !
● Second generation antipsychotics - 5HT2A antagonist

SRI/SNRI + Triptan● 2006 FDA warning 27 => 29 cases no death 13 hospitalizations 10 met Sternbach and 0 met Hunter criteria !● 700,000 visit with co-prescription !● 1/5 patients with triptan get SRI MDD: OR 2.84 CI 1.71 – 4.73 GAD: OR 3.03 CI 1.43 – 6.38

Triptans● triptans 5HT1B, 1D, 1F agonist !
● Short acting (except frovatriptan) !
● Used intermittently !
● American Headache Association combination is reasonable

Neuroleptic Malignant Syndrome (NMS)
Definition● Rare adverse reaction to dopamine receptor antagonists
(blockers) !
● Leading to autonomic dysfunction !
● Can be fatal if not recognized early (10-20%)

More Commonly associated with:● High potency antipsychotics (e.g. haloperidol) !● High dose antipsychotics !
● First generation antipsychotics !
● Young men (possibly due to population at risk of high dose and
high potency antipsychotic use)

Less commonly associated with:Second generation (e.g.) ● quetiapine (Seroquel) ● risperidone (Risperdal) ● olanzapine (Zyprexa) !Non-antipsychotic dopamine receptor antagonists
(e.g.) ● prochlorperazine (Compazine) ● metoclopramide (Reglan) ● promethazine (Phenergan)

Pathophysiology● Not fully understood !
● Probably dopaminergic blockade or depletion in CNS !
● May be a drug induced malignant catatonia (? same underlying pathophysiology) !
● Genetics may be involved
Incidence● 0.5% to 3% of all patients treated with traditional
antipsychotics !
● Recent 0.01% to 0.02% (? due to second generation use) !● Haloperidol implicated in ½ cases (potency, widespread
use)
Risk Factors● previous history of NMS/EPSE !● dehydration !● discontinuation of antiparkinsonian !● withdrawal of benzodiazepines !● catatonia or acute agitation !● use of high potency agents !● iron deficiency
OnsetAt any time - can develop rapidly !Most cases when within 7 days of: ● drug started ● dosage increased ● rapidly titrated !Mild to severe - depending on individual !Dose not a risk factor but more common ↑ dose

Clinical manifestationsSudden change in mental status
FeverMuscle rigidity

Sudden change in mental statusMental state changes precede other signs in 80% of cases !
Clouding of consciousness ranging from: ● confusion to stupor or coma ● agitation, ● delirium, and ● catatonia

Fever● Hyperpyrexia > 38 °C of unknown origin
(? caused by dopamine blockade in hypothalamus causing temperature dysregulation)

Muscle Rigidity ● Dystonia abrupt onset stiffening and rigidity in large
muscles (especially head & neck) !● Severe muscle rigidity produces excess body heat
contributing to hyperpyrexia !● Sometimes difficulty swallowing or a sensation of
tongue thickening that rapidly worsens !● Increased sacroplasmic Ca+ release => muscle contraction/rigidity muscle break down
RigidityAs the syndrome progresses: ● increasing muscle rigidity can lead to diminished chest
wall compliance, hypoventilation, and even respiratory failure !
Other ● EPSEs: parkinsonian tremors, akathisia ● elevated or labile blood pressure ● tachycardia, tachypnoea, tremor, and urinary
incontinence

Autonomic Instability● Tachycardia – 88% !
● Labile or high BP – 61-77% !
● Tachypnea – 73%
Laboratory!● Creatine kinase rises 2 – 4 hours after muscle injury
(indicator degree muscle damage), continued rise may indicate onset !CK is typically more than 1000 IU/L and can be as high as
100,000 IU/L [ !● Rhabdomyolysis releases myoglobin into circulation. !● Once myoglobin in kidneys, it precipitates in renal tubules
causing kidney damage and subsequent renal failure.

Lab: other● proteinuria secondary to stress/tissue damage !
● elevated white blood cell count
Course● Presentation in 70% of cases MS => rigidity => hyperthermia => autonomic !
● Develops over 1 – 3 days !
● Usually resolve in 2 weeks (7 – 11 days norm) !
● Can persist for up to 6 months residual catatonia sx !
● 10-20% fatality rate
Treatment (Not well supported)● Dantrolene – skeletal muscle relaxant up to 10mg/kg/d discontinue after 5-10 days – consider tapering !● Bromocriptine – dopamine agonist 2.5mg Q4-6 hours up to 40mg/day discontinue after 10 days –taper ● Amantadine – DA and Ach effects 100mg Q12H up to 400mg daily
Prevention● Conservative use of antipsychotics !
● Reduction of risk factors !
● Early diagnosis !
● Prompt discontinuation of offending medications !
● Delayed retrial at least 2 wks after resolution recurrence 66% if less 87% ultimately can tolerate AP retrial
Re-challenge Anti-psychotics● 30% risk of developing again !● Check reports on previous episodes for accuracy !● Clearly documented indications for antipsychotics !● Consider alternative medications !● Reduce risk factors use low potency use slow titration consider second generation antipsychotics

Anticholinergic Poisoning

Red as a BeetCutaneous vasodilatation to compensate for loss of sweat
Dry as a Bone

Hot as a Hare
Interference with normal heat dissipation mechanism

Blind as a Bat

Mad as a Hatter

Full as a Flask
Detrusor muscles of bladder and urethral sphincter under muscarinic control
Treatment● Supportive !
● Seizures, agitation => benzodiazepines !
● Prolonged QRS => sodium bicarb

TCA Toxicity● Blockade of cardiac fast sodium channels !
● Antagonism of central and peripheral muscarinic acetylcholine receptors !
● Antagonism of peripheral alpha-1 adrenergic receptors !
● Antagonism of histamine (H1) receptors !
● Antagonism of CNS gamma-aminobutyric acid (GABA) A receptors

TCA Overdose Clinical FeaturesAnticholinergic Plus
● Cardiac Toxicity (quinidine effects) Heart Block Asystole Bradycardia Tachycardia Ventricular Dysrythmias !
● ECG Changes Broadening of QRS complex Widened QT Interval

TCA Overdose- Management 1● Mainstay of initial management is Supportive !
● Try not to give other drugs on top with a few specific exceptions ●A- May need intubation ● B ●C- Give IV fluids if low BP ●D -Control convulsions with Diazepam

TCA Overdose Management 2● Activated Charcoal if more than 4 mg/Kg within 1
hour !
● Correct Hypoxia with Oxygen !
● Correct Acidosis with Na Bic !
● Correct any arrhythmias with Na Bic (i.e. start by controlling the acid base disturbance)

Cyclic Antidepressant Management● Manage A, B, C’s aggressively ● Optimize electrolytes ● Follow serial EKG’s and use Bicarb if: ● QRS >100 or 110 msec
● If bicarbonate and magnesium are not effective, lidocaine is the antidysrhythmic of choice.
● Norepinephrine is the pressor of choice for refractory hypotension.

Is it the Sodium or the Bicarb?● The answer is BOTH! !● Sodium overcomes the
partial blockade from cyclic antidepressants.
!● Alkalinization does
change binding properties.
How does the bicarb work?● Initially thought to increase protein binding thus
limiting free drug in the blood ● Rat study using alpha-1 acid glycoprotein (AAG)
only decreased arrhythmias at massive doses. AAG is a proven TCA binder.
● Current theories is that the ionic form of the TCA binds to the sodium channel causing blockade and the bicarbonate changes the TCA from the ionic form to the neutral form causing less blockade.

Sympathomimetics

Sympathomimetics● Mimics “Fight or Flight” response !
● Alcohol/drug withdrawalà same effects as sympathomimetic drugs !
● Drugs: ●Caffeine, cocaine, amphetamines, ●methamphetamines, Ritalin, LSD, ●Theophylline, MDMA

Sympathomimetics● Tachycardia, dysrhythmias ● Hypertension ● Diaphoresis ● Piloerection (Goosebumps) ● Delusions, paranoia ● Seizures ● Hyperthermia ● Mydriasis (Dilated Pupils)
Caffeine● Toxic dose is >10g (10,000mg) ●Coffee: Tall Starbucks 260mg ●Red Bull: 80mg/can ● Jolt: 72mg/can ●Coca-Cola: 46mg/can ● ‘Wakeups’ (Caffeine pill): 100mg/pill !
● Toxic doses can cause seizure,arrhythmias, respiratory failure, death

Opioids

Opiates / Opioids● Typically present with respiratory depression, altered
mental status, and miosis. !● Address the patient like any other “altered mental
status” !● Key point is to remember to consider an opiate
ingestion.

Naloxone Dosing● Usually start with 0.01-0.1 mg / Kg. !● Repeat as frequently as needed to reverse symptoms. !● If a drip is required, calculate how much naloxone was
used in the first hour and start the drip at 2/3 that dose.

Clonidine and Imidazolines● Clonidine is an alpha-2 agonist that is used for
hypertension. ● Imidazolines, such as oxymetazoline (afrin) are used as
decongestants. ● Symptoms typically present like an opiate overdose ?
Alpha2 Antagonists & Opiate Overdose ● They are NOT structurally related to opiates. !● The alpha-2 receptor targeted by clonidine has significant
functional overlap with the opiate receptor. Both may be located on the same neuron, both coupled by via G-protein to the same potassium channel. !
● May require larger doses of naloxone to reverse symptoms.
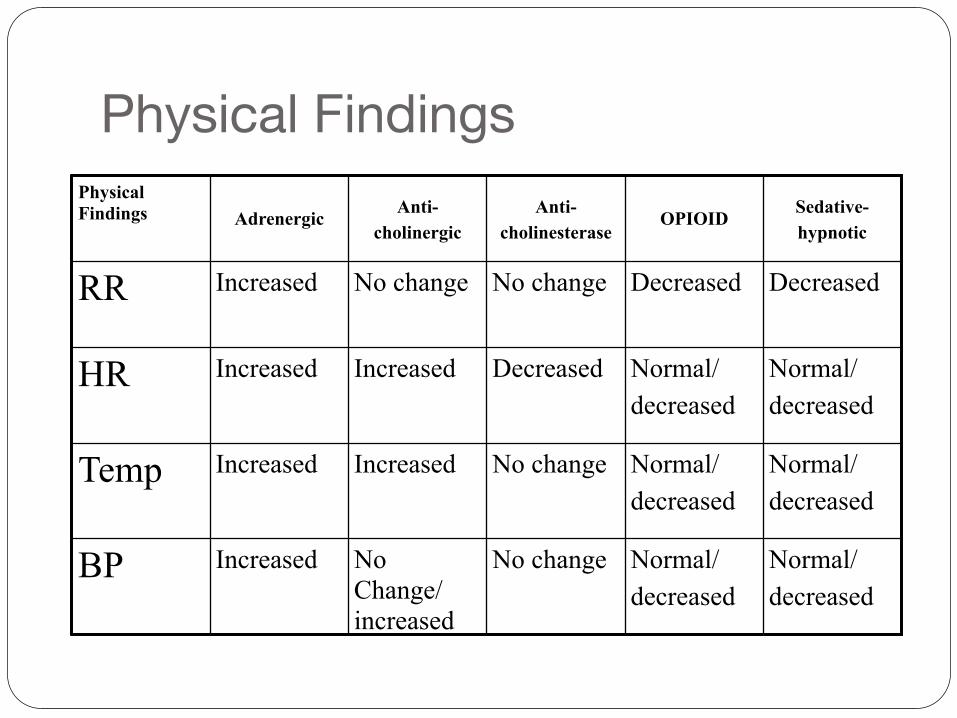
Physical FindingsPhysical Findings Adrenergic Anti-
cholinergicAnti-
cholinesteraseOPIOID Sedative-
hypnotic
RR Increased No change No change Decreased Decreased
HR Increased Increased Decreased Normal/ decreased
Normal/ decreased
Temp Increased Increased No change Normal/ decreased
Normal/ decreased
BP Increased No Change/increased
No change Normal/ decreased
Normal/ decreased

Physical FindingsPhysical Findings Adrenergic
Anti- cholinergic
Anti- cholinestera
seOPIOID
Sedative- hypnotic
Mental status
Alert/ agitated
Depressed/ Confused/ hallucinate
Depressed/ Confused/
Depressed Depressed
pupils Dilated Dilated Constrict Constrict Normal
Mucus membrane
Wet Dry Wet Normal Normal
skin Diaphoretic Dry Diaphoretic Normal Normal

Questions?