psyc 1000 lecture 53. etiology what causes psychological disorders? –for many disorders there is...
TRANSCRIPT
PSYC 1000Lecture 53
Etiology• What causes psychological disorders?
– For many disorders there is no general consensus• Compromises one of the bases of the DSM-IV-TR
classification scheme.
– Major approaches• Psychodynamic – Focus on unresolved conflicts, often
subconscious, and maladaptive defense mechanisms• Behavioural – Understand the conditioning (classical or
operant) that maintains the behaviour and modify.• Cognitive – Target the rationale behind actions and
address incorrect or maladaptive reasoning. Maladaptive processing may also be unconscious.
• Biological – What are the neural substrates that are different in clinical populations? Restore function through pharmacological or physiological manipulation.

Anxiety Disorders
• Anxiety Disorders – Distressing, persistent anxiety– Or maladaptive behaviors that
reduce anxiety
• Generalized Anxiety Disorder– Person is tense, apprehensive, and
in a state of autonomic nervous system arousal
– Unable to identify cause, “free floating”
• Panic Disorder– Minutes-long episode of intense
dread in which person experiences terror and accompanying chest pain, choking, or other frightening sensation
– Perceived as heart-attack, come to fear fear itself

Geneeralized Anxiety Disorder• A. At least 6 months of "excessive anxiety and worry" about a variety of events
and situations. Generally, "excessive" can be interpreted as more than would be expected for a particular situation or event. Most people become anxious over certain things, but the intensity of the anxiety typically corresponds to the situation.
B. There is significant difficulty in controlling the anxiety and worry. If someone has a very difficult struggle to regain control, relax, or cope with the anxiety and worry, then this requirement is met.
C. The presence for most days over the previous six months of 3 or more (only 1 for children) of the following symptoms:
• 1. Feeling wound-up, tense, or restless2. Easily becoming fatigued or worn-out3. Concentration problems4. Irritability5. Significant tension in muscles6. Difficulty with sleep
• D. The symptoms are not part of another mental disorder.
E. The symptoms cause "clinically significant distress" or problems functioning in daily life. "Clinically significant" is the part that relies on the perspective of the treatment provider. Some people can have many of the aforementioned symptoms and cope with them well enough to maintain a high level of functioning.
F. The condition is not due to a substance or medical issue

•Phobia–Persistent, irrational fear of a specific object or situation–Some common and uncommon fears


• Obsessive-Compulsive Disorder– Unwanted repetitive thoughts (obsessions)
and/or actions (compulsions)
Post-Traumatic Stress Disorder
• Four or more weeks of following symptoms
– Haunting memories– Nightmares– Social withdrawal– Jumpy anxiety– Sleep problems
• Associated with– More intense trauma– Closer proximity (e.g., 9/11)
• Concerns about PTSD– Overdiagnosed?– Trauma counseling ineffective
or harmful in some cases– Resilience of survivors

Explaining Anxiety Disorders
• Learning Perspective– Fear Conditioning: 58% of people with social
phobia experienced disorder after traumatic event• Horley et al (2004): Social Phobics avoid looking at eyes
of angry faces (above, early experiences?)
– Stimulus Generalization– Avoidance or Escape behaviors: Negative
Reinforcement– Observational Learning

• Biological Perspective– Natural Selection: predispositions to
fear certain kinds of objects and events (snakes, confinement) and engage in certain ritual behaviors (hand-washing)
– Genes: higher prevalence of anxiety in identical twins
– Reduced GABA levels: GABA is inhibitory neurotransmitter
– Physiology: over-arousal of frontal lobe areas involved in directing attention and impulse control, as in PET Scan of brain of person with Obsessive/ Compulsive disorder (top); high metabolic activity (red) in frontal lobe areas; or over-activity of brain region involved in error checking (bottom)

• Cognitive Perspective– Attentional and other cognitive processes play role in
anxiety (and other psychological disorders)– Emotional Stroop task: name ink color of words that
are either Threatening or Non-Threatening– Study with Adolescents who also completed Beck
Anxiety Inventory (BAI). Measured time (sec) to read Stroop card.
Words Low BAI High BAI
Non-threatening 63.2 68.3
Threatening 65.3 76.6
Difference 2.1 8.3*– Interference index calculated by subtracting time to
read colors of threat words from time to read colors of neutral words: r with BAI = +.42

Mood Disorders
• Mood Disorders – Characterized by emotional extremes– Two variants: Major Depressive
Disorder and Bipolar Disorder
• Major Depressive Disorder – Mood disorder in which person, for no
apparent reason, experiences two or more weeks of depressed moods, feelings of worthlessness, and diminished interest or pleasure in most activities
– Symptoms
• Depression: Five (or more) of following symptoms present during same 2-week period– Depressed mood most of day, nearly every day – Markedly diminished interest in most activities most
of day– Significant weight loss when not dieting or weight
gain– Insomnia or Hypersomnia nearly every day– Psychomotor agitation or retardation nearly every
day – Fatigue or loss of energy nearly every day– Feel worthless or excessive guilt nearly every day– Diminished ability to think or concentrate, or
indecisiveness, nearly every day – Recurrent thoughts of death (not just fear of dying),
recurrent suicidal ideation without specific plan, or suicide attempt or specific plan for committing suicide

• Bipolar Disorder– Mood disorder in which person
alternates between hopelessness and lethargy of depression and overexcited state of mania
– Formerly called manic-depressive disorder
• Manic Episode– Mood disorder marked by hyperactive,
wildly optimistic state
– Symptoms
• Manic Episode: Three (or more) of following symptoms present during same 1-week period– Inflated self-esteem or grandiosity – Decreased need for sleep (feels rested after three
hours sleep) – More talkative than usual or pressure to keep talking– Flight of ideas or subjective experience that
thoughts are racing – Distractibility – Increase in goal-directed activity or psychomotor
agitation – Excessive involvement in pleasurable activities that
have high potential for painful consequences (sexual indiscretions, foolish business investments)

Explaining Mood Disorders• Facts to be explained by theory
– Many associated behaviors and cognitions: lack motivation, recall negative events, negative expectations, …
– Stressful events often precede depression: Incidence of 1% if 0 stressful events, 24% for 3 or more
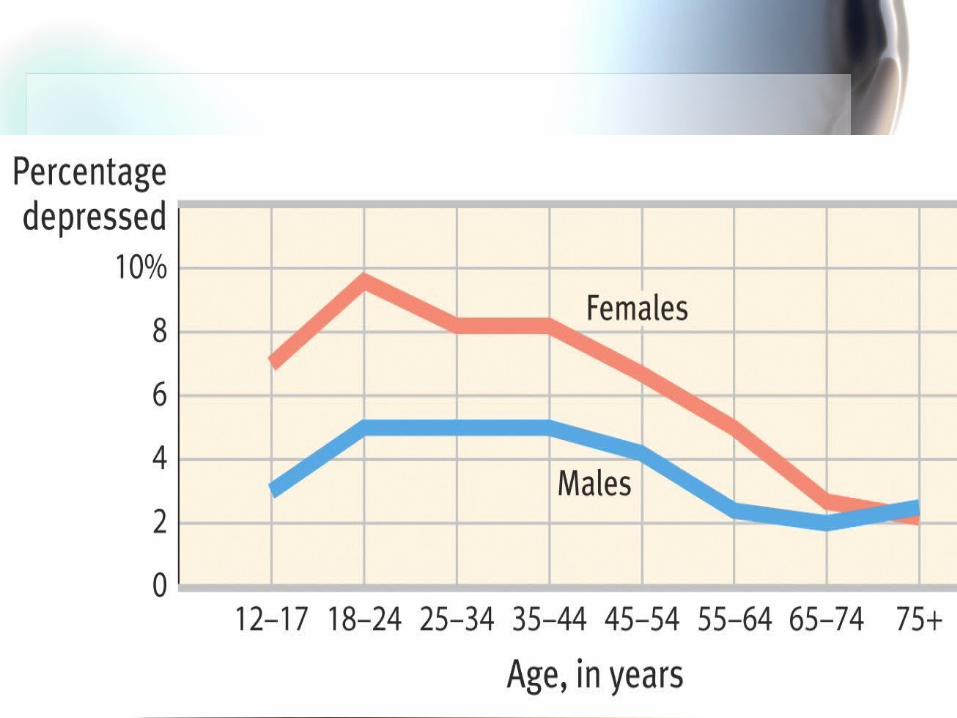
– Major Depressive Episodes often Self-Terminate– Increase in rates of depression (and other
disorders), and also earlier onset– Widespread– More common in women– Affects all ages, but especially young– Also suicide facts (later slides)


Next Class• Suicide
• Personality Disorders